
Abstract
The development of self-management strategies plays an active role in the recovery process of individuals suffering from mental disorders. The Mental Health Self-Management Questionnaire (MHSQ) was developed to give empirical insight into the construct of self-management. This study aimed to assess the psychometric properties of this recent instrument in a sample of patients meeting DSM-5 criteria for anxiety disorders. Data were drawn from a randomized controlled trial examining transdiagnostic group cognitive-behavioural therapy compared to treatment-as-usual for anxiety disorders. Participants (n = 231) completed a structured interview for anxiety disorders and several self-reported measures, including the MHSQ. Confirmatory factor analysis for the initial three-factor structure showed adequate fit after adding covariances between certain items. The MHSQ had acceptable reliability for the clinical (α = .73, ω = .78), empowerment (α = .80, ω = .80) and vitality (α = .71, ω = .71) subscales. Results showed high correlations with measures of well-being and moderate correlations with measures of disability and depression, especially on the empowerment and vitality subscales. Lower correlations were found between the MHSQ and anxiety symptoms. The linear mixed model examining sensitivity to change showed that the MHSQ score at post-treatment was significantly greater for the experimental condition compared to the control condition for the clinical and empowerment subscales. The MHSQ is a promising measure, and research with other clinical populations and long-term follow-up is warranted to gather further evidence on the validity and fidelity of the instrument.
Introduction
Self-management has been described as the daily practices an individual with an existing physical illness or mental disorder undertakes to reduce or control the impact of such illness on their well-being, manage symptoms, and avoid future relapse (Clark et al., 1991; Lorig & Holman, 2003). Self-management support is an intervention that fosters self-efficacy and empowerment as part of the personal recovery process and is conceptually distinct from clinical interventions such as pharmacotherapy or psychotherapy. Studies have shown the potential of self-management support to improve health outcomes and quality of life, and reduce service utilization in patients with long-term physical health conditions as well as severe mental disorders (Coleman et al., 2009; Lean et al., 2019; Murphy et al., 2013; Panagioti et al., 2014), and studies for patients with depression also appear promising (e.g., Houle et al., 2013). However, research on the added value of self-management support for patients with anxiety disorders remains scarce (e.g., Lauridsen et al., 2022; Zimmermann et al., 2016; Zoun et al., 2019). From a personal recovery perspective, the development of self-management skills for individuals with anxiety disorders warrants more attention as they are the most frequent mental disorders within community settings and often present a chronic or relapsing course, or residual symptoms (Bokma et al., 2019; Kessler et al., 2009; Scholten et al., 2013; Somers et al., 2006).
The assessment of self-management skills is valuable for patients with anxiety disorders as it can help determine the current need for interventions, examine progress in implementing self-management strategies, and explore the potential impact of interventions on clinical outcomes, quality of life, functioning, and health services utilization. A scoping review of generic self-management questionnaires for individuals with chronic conditions identified ten questionnaires published between 1976 and 2019 (Hudon et al., 2021), such as the Patients in Health Scale (PIH; Battersby et al., 2003) and the Therapeutic Self-Care Scale (TSCS; Doran et al., 2002). The self-management strategies examined within these questionnaires mainly focused on behavioural/medical and cognitive/decision-making strategies and, to a lesser degree, on social and emotional strategies (Hudon et al., 2021). As individuals with anxiety disorders use a wide range of self-management strategies based on their needs and preferences in their day-to-day lives to foster their recovery (Villagi et al., 2015), self-management questionnaires developed for long-term physical conditions may not adequately capture the diversity of self-management behaviours that can play an active role in better anxiety management and, consequently, improved outcomes. In response to the lack of validated tools that could quantitatively measure self-management in the mental health domain, Coulombe et al. (2015) developed the 18-item Mental Health Self-Management Questionnaire (MHSQ). This scale, initially developed in French, is based on a previous qualitative study in which 85 self-management strategies were identified from interviews with patients recovering from depression, anxiety or bipolar disorders (Villaggi et al., 2015). A first psychometric validation of the questionnaire identified three factors composing the construct of self-management: 1) clinical, the extent to which an individual seeks help when needed and makes use of available resources (e.g., professional consultation, support group, medication); 2) empowerment, how individuals gain control through a positive self-concept and focus on strengths (e.g., problem-solving, focusing on present moment); and 3) vitality, maintenance of a generally active and healthy lifestyle (e.g., sport, eating habits, exercise). The instrument showed adequate internal consistency, test-retest reliability, and concurrent and convergent validity in the initial validation study with a sample of patients in recovery from depression, anxiety or bipolar disorders (Coulombe et al., 2015). The subsequent Japanese (MHSQ-J; Morita et al., 2019) and Chinese (MHSQ-C; Wang et al., 2022) validations of this instrument have also yielded similar results. To our knowledge, no other studies have yet scrutinized the psychometric properties of the MHSQ.
Our study aimed to examine the psychometric properties of the French version of the MHSQ in a sample of adults with principal anxiety disorders, as a validated questionnaire on self-management behaviours adapted to this population would be valuable to both clinical research and practice. More specifically, we aimed to assess the factor structure, internal consistency, construct validity and sensitivity to change of the MHSQ to appreciate whether our results corroborate previous findings.
Method
Data Source
The study is based on a secondary data analysis from a pragmatic randomized clinical trial of transdiagnostic group cognitive-behavioural therapy (CBT) for anxiety disorders (Roberge et al., 2020). Detailed information on the methodology can be found in the trial protocol (Roberge et al., 2018). The dataset used for this report comprised 231 participants enrolled in the trial and meeting the following eligibility criteria: 1) aged 18–65; 2) fluent in spoken and written French; and 3) meeting principal diagnosis criteria for one of the following anxiety disorders according to the Diagnostic statistical manual of mental disorders (DSM-5; American Psychiatric Association, 2013): panic disorder, agoraphobia, social anxiety disorder or generalized anxiety disorder. Patients having consulted a psychiatrist in the past 12 months or with active suicidal intent, psychosis, cognitive impairment, bipolar disorder, and substance-related or addictive disorders were excluded from the study.
Participants were randomly assigned to either receive a 12-week group CBT program (n = 117) in addition to treatment-as-usual (TAU) or TAU only (n = 114). The CBT program was a 12-week group intervention led by two psychologists or psychotherapists and focused on education and self-monitoring, specific cognitive restructuring, graduated exposure, response prevention, and generalized cognitive restructuring (Norton, 2012).
Measures
Each potential participant completed a screening questionnaire and an initial face-to-face interview, which included the Anxiety and Related Disorders Interview Schedule for DSM-5 (ADIS-5; Brown & Barlow, 2014), a structured interview guide designed to diagnose current anxiety, mood, obsessive-compulsive, trauma, and related disorders. If meeting eligibility criteria, they also completed a booklet of self-reported symptom measures widely used in clinical trials for anxiety disorders and generally validated in both English and French.
The following self-reported assessment scales were drawn from the dataset to examine construct validity between the three MHSQ subscales and other self-report assessment scales assessing related constructs of anxiety, depression, well-being and functioning. For convergent validity, the MHSQ would be expected to have a negative correlation with anxiety and depressive symptoms (clinical recovery) but positive correlations with measures of well-being (personal recovery). No hypothesis was formulated for functioning as it relates directly to both clinical and personal recovery. Given that the data for this article was derived from a secondary data source, no other measure for self-management was available for the study to examine criterion validity.
Anxiety Symptoms Measures
The Beck Anxiety Inventory (BAI; Beck et al., 1988; Freeston et al., 1994) is a 21-item self-reported generic measure of anxiety symptoms with high internal consistency (α = .92; α = .88 in our sample), test–retest reliability over 1 week, r(81) = .75 and including established significant reliable improvement and clinically significant change cut-points based on normative data and comparable samples of multiple anxiety disorders (Oei & McAlinden, 2014). Items are scored on a scale between 0 and 3, with a maximum score of 63 interpreted as minimal (0–7), mild (8–15), moderate (16–25) or severe (26–63) anxiety levels.
Participants also completed diagnostic-specific self-reported measures of anxiety disorders. The Penn State Worry Questionnaire (PSWQ; Gosselin et al., 2001; Meyer et al., 1990) is a 16-item questionnaire that measures worry as a trait observed in generalized anxiety disorder, with high internal consistency (α between 0.93 and .95; α = .74 in our sample) and test-retest reliability (test-retest r of 0.92 and .93). Items are scored on a scale between 1 and 5, with a maximum score of 80 interpreted as not anxious or a worrier (0–29), below clinical range (30–52), problems with worry (52–65) or chronic worrier (66–80).
The Social Phobia Inventory (SPIN; Connor et al., 2000; Radomsky et al., 2006) is a 17-item questionnaire assessing the experience of fear, avoidance, and physiological discomfort in social anxiety disorder, with good internal reliability (α between .87–.94; α = .91 in our sample), test-retest reliability (r = .78), and convergent validity. Items are scored on a scale between 0 and 4, with a maximum score of 68 interpreted as none (0–20), minimal (21–30), moderate (31–40), severe (41–50) or very severe (51–68) anxiety severity.
The Panic Disorder Severity Scale - Self Report (PDSS-SR; Houck et al., 2002; Roberge et al., 2022) examines seven dimensions of panic disorder, such as panic symptoms and avoidance, and shows good internal reliability (α = .92; α = .91 in our sample), test-retest reliability (ICC = .81) and sensitivity to change with a mean decrease of 7.3 (SD = 5.1). Items are scored on a scale between 0 and 4, with increasing values corresponding to increasing severity of panic symptoms.
The Mobility Inventory for Agoraphobia (MIA; Chambless et al., 1985) assesses agoraphobic avoidance behaviour in 27 places or situations when alone or with a companion and shows excellent internal consistency (α between .91–.97; not available in our sample due to low sample size with agoraphobia symptoms) and construct validity. Items are computed as an average of items from 1 (never avoid) to 5 (always avoid) for two subscales - alone and accompanied - and users can skip items if they do not apply to their lives.
Depressive Symptoms
The Patient Health Questionnaire (PHQ-9; Arthurs et al., 2012; Kroenke et al., 2000) is a commonly used instrument that assesses the frequency of depressive symptoms with good reliability (α between .86–.89; α = .82 in our sample) and validity. Items are scored on a scale between 0 and 3, with a maximum score of 27 interpreted as none/minimal (0–4), mild (5–9), moderate (10–14), moderately severe (15–19) or severe (20–27) depression severity.
Functioning and Well-Being
The Sheehan Disability Scale (SDS; Sheehan et al., 1996; Leon et al., 1997) measures functional impairment in the three domains of work, social life and family life, and shows good internal reliability (α = .89; α = .80 in our sample) and good sensitivity. Items for each scale are scored between 0 (not at all) and 10 (extremely) to reflect impairment levels.
The Mental Health Continuum-Short Form (MHC-SF; Lamers et al., 2011) is a 14-item scale measuring emotional, psychological, and social well-being, and has shown excellent internal consistency (α between .74-.89 between scales; α = .90 in our sample), construct and discriminant validity. Items are scored on a 6-point scale of frequencies ranging from never to every day. Scores are categorized as “flourishing mental health” when at least one of the three signs of hedonic well–being and at least six of the eleven signs of positive functioning are scored as ‘every day’ or ‘almost every day’ during the past month.
Mental Health Self-Management Questionnaire (MHSQ)
The MHSQ was initially developed in French and validated by Coulombe et al. (2015) and comprises three subscales: clinical (5 items), empowerment (9 items) and vitality (4 items), with 5-level Likert scales ranging from 0 (never used) to 4 (very often used). The three subscales comprise the average score for each item, and a higher score should be interpreted as better self-management. In the initial study by Coulombe et al. (2015), a confirmatory factor analysis (CFA) supported a three-factor solution. The reliability was satisfactory for each subscale (clinical: α = .69, empowerment: α = .81, vitality: α = .75), with adequate test-retest reliability over two weeks (ICC ranging from .76 for empowerment to .85 for vitality). For criterion validity, results supported convergent validity with self-management measures and concurrent validity with diverse clinical and personal recovery measures. Coulombe et al. (2015) used a back translation process to ensure the conceptual equivalence of the items in both languages, and the MHSQ items presented in this article are drawn from that reference.
Ethical Considerations
The trial protocol was approved by the ethics review boards of the Integrated Health and Social Services Centers in Estrie (#MP-22- 2016-570), Québec City (#2017-166), and Laval (#2016-2017-C54). All participants provided written informed consent.
Statistical Analyses
The factor structure of the MHSQ was examined with CFA, with maximum likelihood estimation algorithms (MLR), following the method used by Coulombe et al. (2015). Analyses were conducted with the entire sample without any imputation method. The CFA was run to test the fit of the three-factor final model obtained by Coulombe et al. (2015). Correlations between constructs were analyzed with CFA analysis, but only significant correlations were presented in the path diagram. Model fit was assessed with the standardized root mean square residual (SRMR), the root mean square error of approximation (RMSEA), comparative fit index (CFI) and Tucker–Lewis index (TLI). The RMSEA is an absolute adequacy index evaluating the distance between hypothetical and perfect models. CFI and TLI are incremental adequacy indices that compare the adequacy of a hypothetical model with that of a model with the worst fit. The following criteria indicate a good model fit: SRMR below .08, RMSEA below .07, CFI and TLI higher than .95 (Hooper et al., 2008). Other iterations of the initial CFA model were also conducted to account for covariance and to examine the improvement in adequacy for indices following the removal of items based on internal consistency and clinical pertinence.
Internal consistency was assessed using Cronbach’s alpha and McDonald’s omega, and individual items were examined through corrected item-total correlations. An estimate >.70 was considered adequate for internal consistency, and an item-total correlation >.30 cut-off was adopted (Rattray & Jones, 2007).
Construct validity was assessed through bivariate correlations between the MHSQ subscales and other self-report assessment scales of generic anxiety symptoms, specific anxiety symptoms, depressive symptoms, well-being and functioning. Spearman correlations were used as some measures were not normally distributed (i.e. MIA, PDSS, PSWQ).
Sensitivity to change was examined through a linear mixed regression model at baseline and post-treatment, using the maximum-likelihood method and the variance components correlation matrix on the MHSQ considering the treatment group, time, and evolution between groups (i.e., the interaction). The intra-group therapy variance was less than 5%, and only a random effect on the patient was added. Results were adjusted for comorbid depressive symptoms (PHQ-9), psychotropic medication and principal anxiety disorder (ADIS-5) at baseline. There was no bootstrap resampling, given that residuals were normally distributed. MPlus 7 version 1.31 was used for factor analysis, IBM SPSS Statistics version 25 was used for all other statistical analysis, and figures were created on GraphPad Prism version 7.
Results
Participants
Sociodemographic Characteristics, Clinical Profiles and Service Utilization at Baseline.
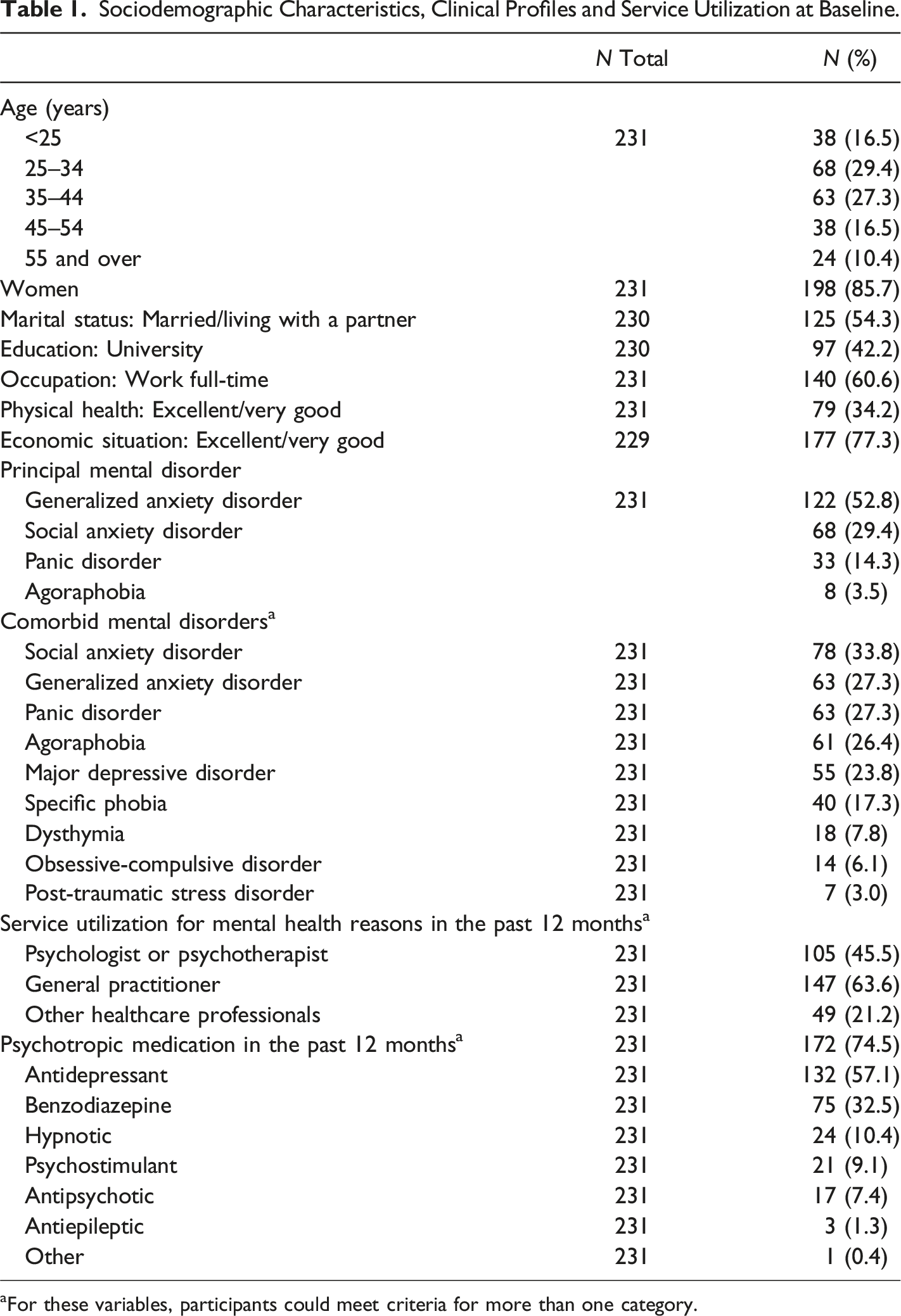
aFor these variables, participants could meet criteria for more than one category.
Factor Structure
Model Fit From Confirmatory Factor Analysis.
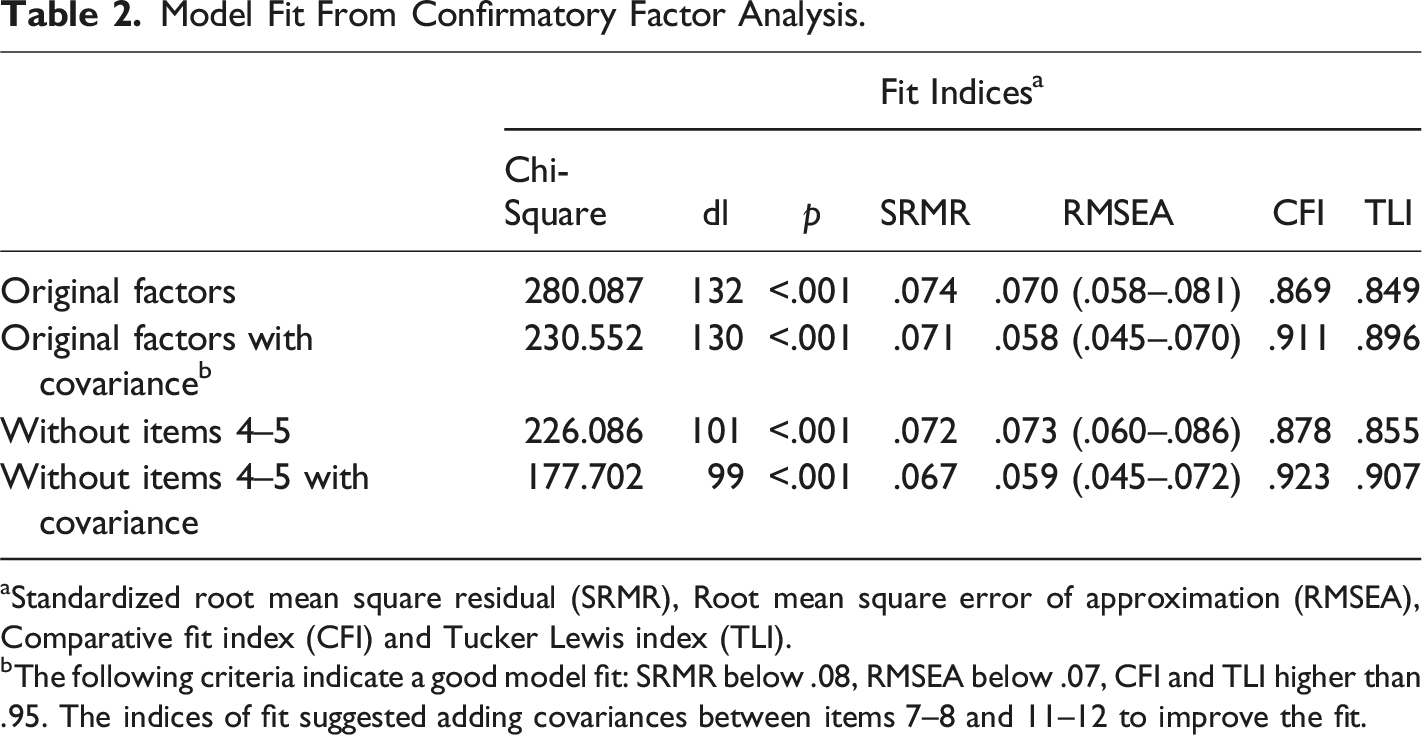
aStandardized root mean square residual (SRMR), Root mean square error of approximation (RMSEA), Comparative fit index (CFI) and Tucker Lewis index (TLI).
bThe following criteria indicate a good model fit: SRMR below .08, RMSEA below .07, CFI and TLI higher than .95. The indices of fit suggested adding covariances between items 7–8 and 11–12 to improve the fit.
Cronbach’s Alpha and Correlations Between Each Item of the MHSQ.
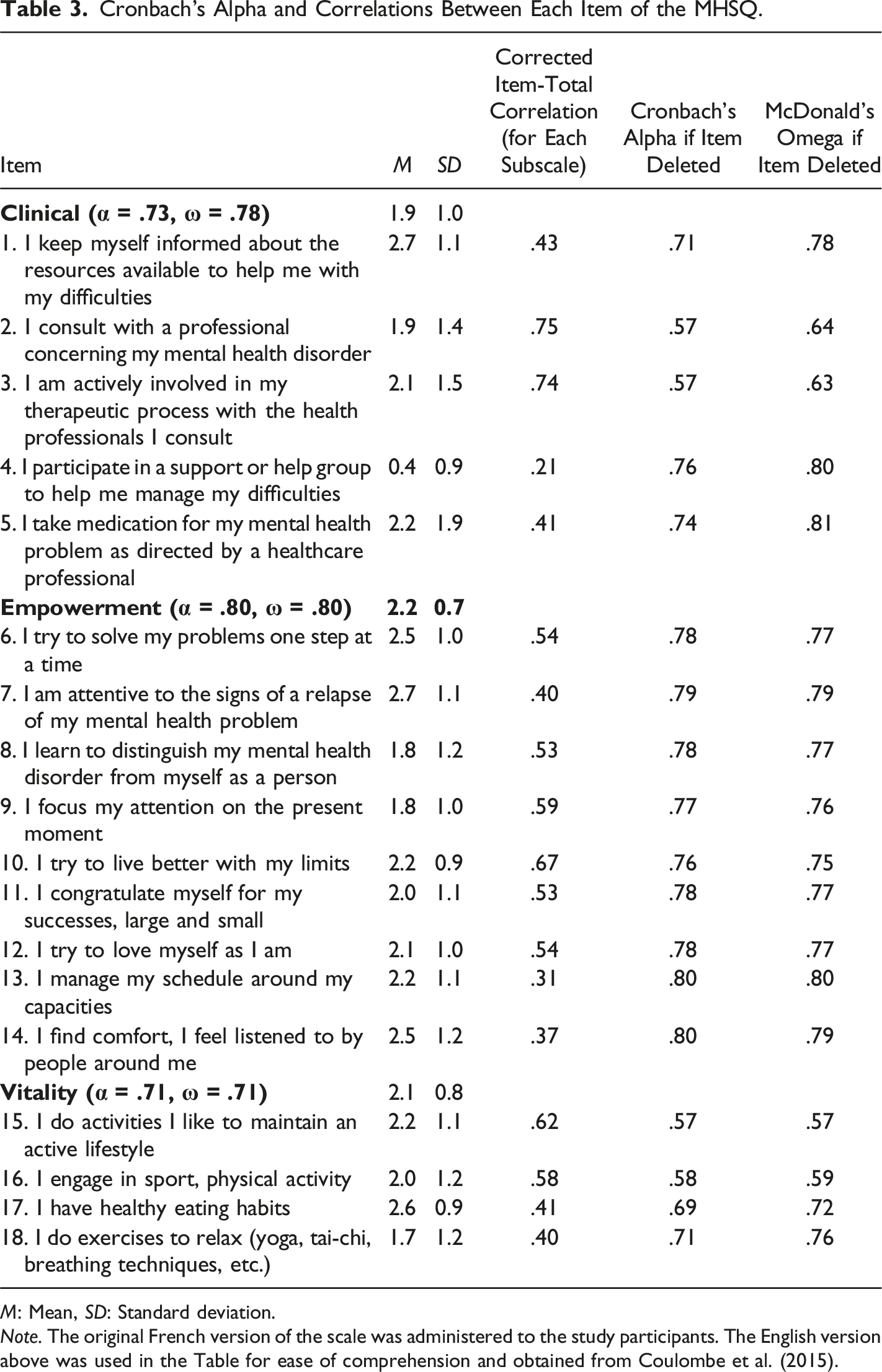
M: Mean, SD: Standard deviation.
Note. The original French version of the scale was administered to the study participants. The English version above was used in the Table for ease of comprehension and obtained from Coulombe et al. (2015).
Two participants were excluded from the CFA analysis as they had missing data on the MHSQ. Scores were normally distributed with a linear association. Considering correlations between scales with CFA analysis, there was no significant correlation between the clinical and empowerment subscales (r = .13, p = .13) and between the clinical and vitality subscales (r = .008, p = .92). There was a significant correlation only between the empowerment and vitality subscales (r = 0.42, p < .001). Figure 1 shows the path diagram for the CFA without items 4 and 5. Path diagram for the confirmatory factor analysis. All coefficients are standardized coefficients. Only coefficients that were significant at p ≤ .05 are represented.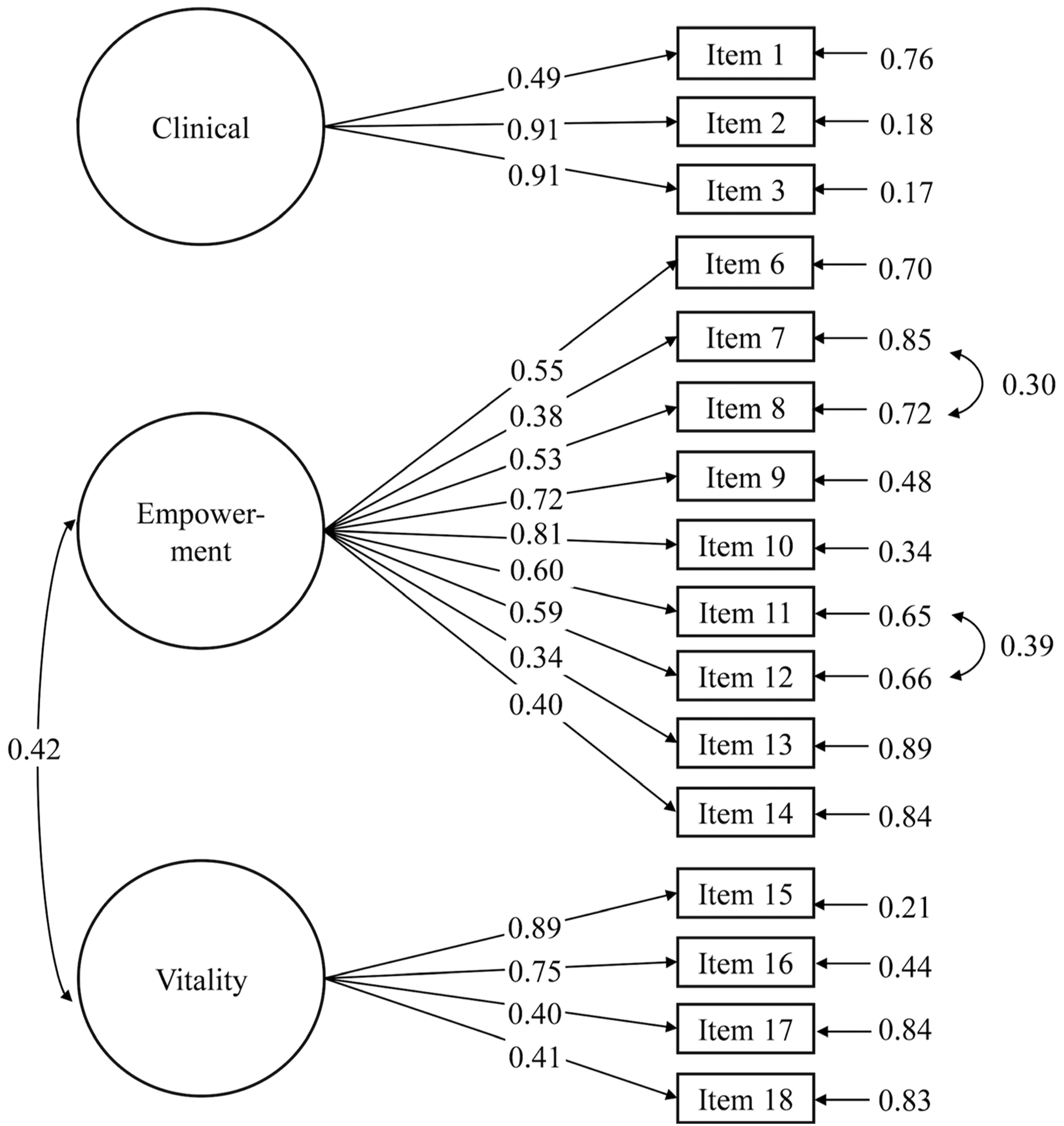
Internal Consistency
Cronbach’s alpha (α) and McDonald’s omega (ω) showed adequate internal consistency for the clinical (α = .73, ω = .78), empowerment (α = .80, ω = .80) and vitality (α = .71, ω = .71) subscales of the MHSQ. Baseline mean scores (±SD) were 1.9 (±1.0) for the clinical, 2.2 (±0.7) for the empowerment, and 2.1 (±0.8) for the vitality subscales. Mean scores for individual items, corrected item-total correlations, Cronbach’s alpha and McDonald’s omega (ω) if the item was deleted are presented in Table 3. Corrected item-total correlations ranged between .21 and .75, indicating that one or more items have a poor relationship with their respective subscale. Item 4 had the lowest item-total correlation in the entire scale, and internal consistency coefficients would increase (α = .76, ω = .80) with removal from the clinical subscale. If item 5 were removed, internal consistency coefficients would also increase slightly (α = .74, ω = .81). With the removal of both items 4 and 5, internal consistency coefficients were improved further (α = .81, ω = .86). No other item was found to increase Cronbach’s alpha if deleted. However, if deleted, two additional items in the vitality subscale would increase McDonald’s omega coefficient: items 17 and 18. For item 4, the majority have never (80.4%) or very rarely (8.3%) participated in a support or help group. For item 5 on medication, the responses were in the extremes. Either the participant was taking medication for mental health problems as prescribed by the healthcare professional (47.6%), or the participant reported having never used medication (38.1%). As items 17 and 18 were well distributed, they were not deleted. As an additional consideration, a minimum of three or more items is generally recommended within a factor (e.g., Marsh et al., 1998), and only two items would remain for this scale if they were removed.
Construct Validity
Spearman Correlations Between MHSQ and Other Self-Report Measures.
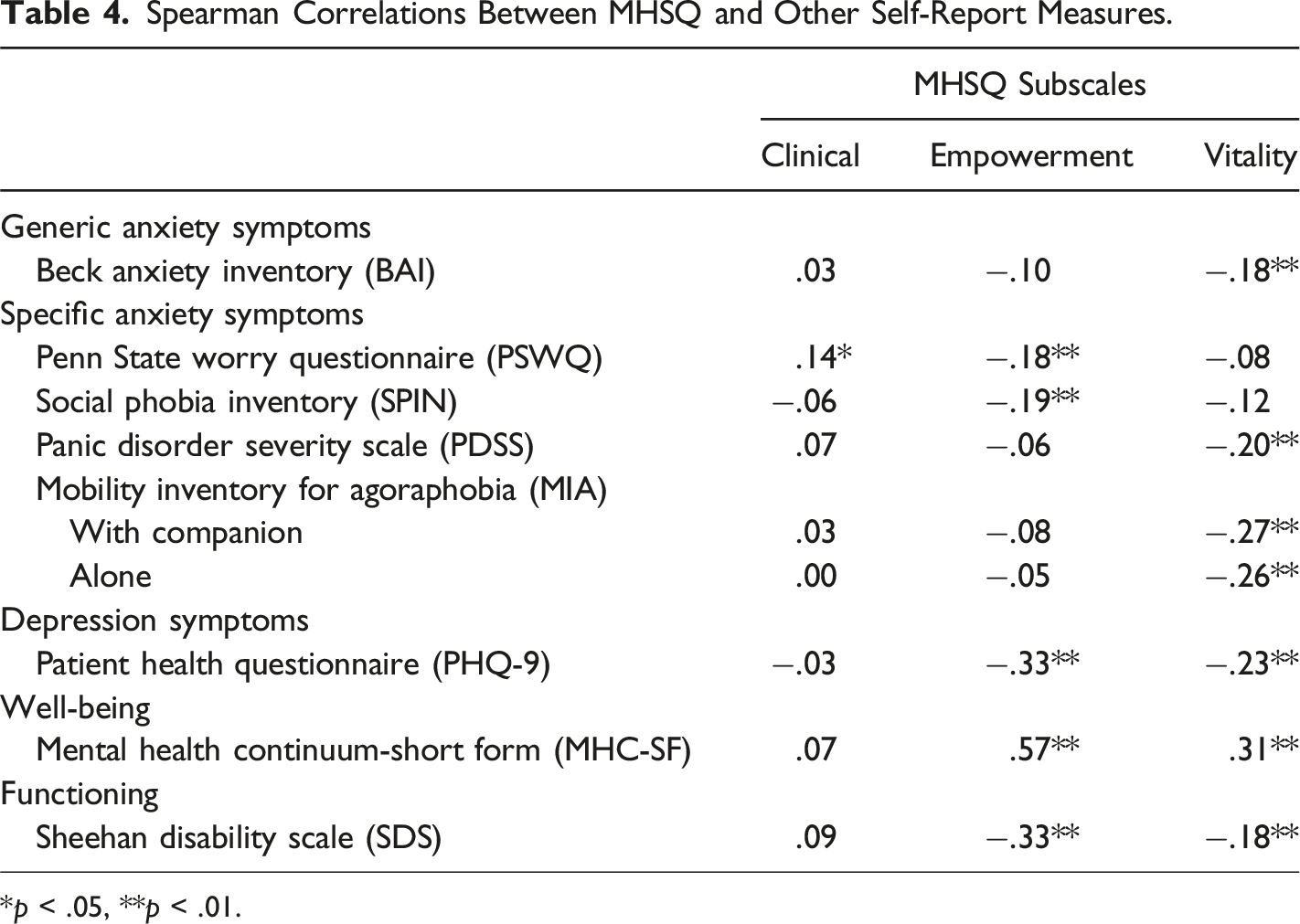
*p < .05, **p < .01.
Sensitivity to Change
A comparative analysis was initially conducted between participants in the intervention (n = 117) and the control conditions (n = 114; TAU). As shown in Figure 2, there was no significant difference in the mean ±SD score of the MHSQ at baseline between the two conditions. When evaluating the clinical subscale, the linear mixed model indicated a significant difference in time (p < .001) and for the interaction (between-group difference of 0.57; 95% CI [0.34, 0.80], p < .001), suggesting that the tCBT intervention condition was associated with a significatively larger increase in the MHSQ score over time. Similar results were encountered when evaluating the empowerment subscales (difference in time, p < .001; between-group difference of 0.44; 95% [CI 0.29, 0.60], p < .001). The vitality subscale showed no significant differences in time (p = .192) nor for the interaction (p = .233). Sensitivity to change according to the CBT condition on total and subscale scores of the MHSQ. CBT, cognitive behavioural therapy; TAU, treatment-as-usual.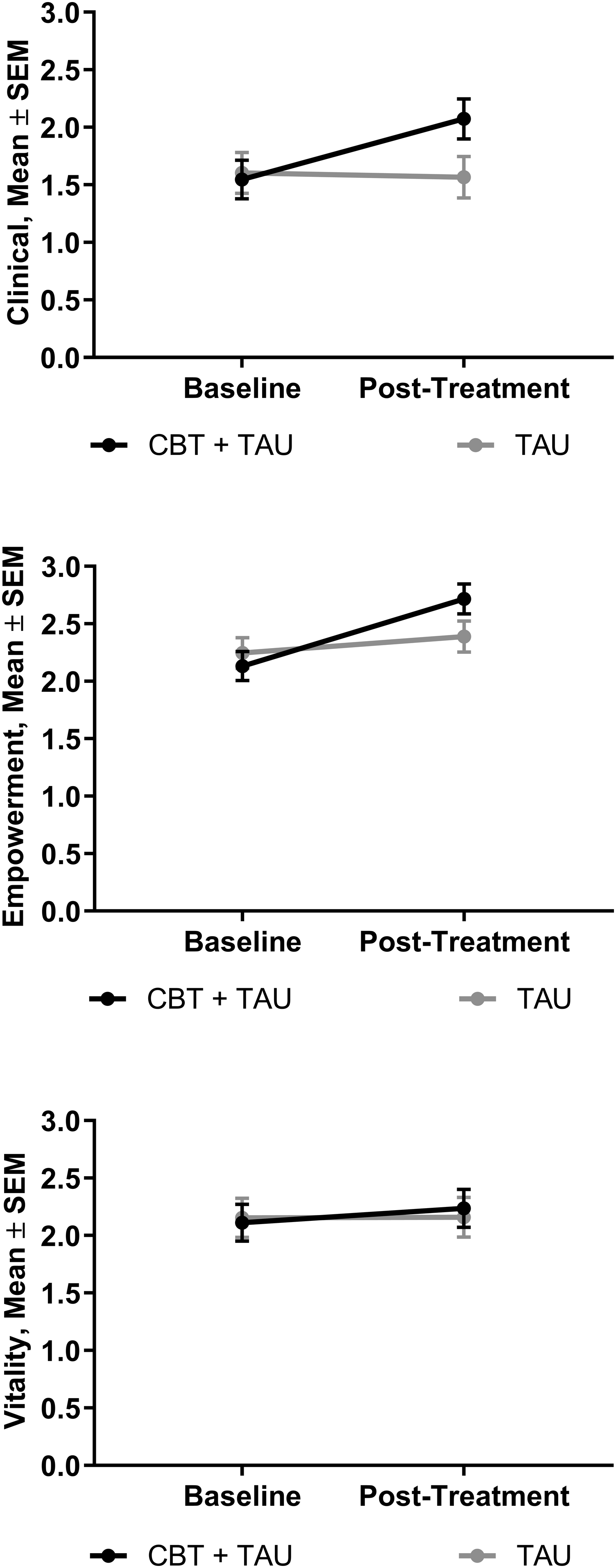
Discussion
This study aimed to evaluate the psychometric properties of the MHSQ in a sample of participants with principal anxiety disorders drawn from a randomized controlled trial on transdiagnostic group CBT. Psychometric properties were generally supportive of the applicability of the self-reported MHSQ scale in the recovery process of individuals with anxiety disorders, both from research and clinical standpoints. Interestingly, our secondary dataset also highlighted potential areas for improvement that appear predominantly associated with the distinct characteristics of our sample.
As in the original validation study conducted by Coulombe et al. (2015), a three-factor model was found adequate in our sample with the same item distribution corresponding to each clinical, empowerment and vitality subscale. The initial CFA showed a marginal fit after adding covariances between items 7–8 and 11–12 within the empowerment subscale, with the CFI and TLI index being slightly below the expected thresholds. From a clinical angle, items 7 and 8 were conceptually related as they refer to having a personal identity independent from one’s mental health condition. Items 11 and 12 emphasize self-compassion and self-acceptance, foundational to a non-judgmental perspective in personal recovery. Coulombe et al. (2015) also employed this method to improve the original model, but covariance was added for item 1 (i.e., resources available) with items 7 and 18 on relapse signs and exercise, respectively. A possible hypothesis is that since our participants were enrolled in a clinical trial at the time of completing the MHSQ and were also high users of mental healthcare resources and medication, this may have directly influenced their knowledge about resources available and perception of relapse prevention.
The model’s fit was also significantly improved by removing items 4 and 5 from the model. Internal consistency data and clinical relevance supported the reason for withdrawing these items. Looking at corrected item-total correlations for each subscale, two sets of items initially emerged as a concern in both the clinical subscale (item 4 – support or help group; item 5 – medication) and the vitality subscale (item 17 – eating habits; item 18 – exercise). We determined that it would not be advantageous to remove items 17 and 18 as they showed a normal distribution and, conceptually, they were highly concordant with vitality in self-management. A consultation process with patients with lived experience of anxiety disorders could help explore improvements in the formulation of these concepts and potentially include new and meaningful items for that vitality subscale. However, items 4 and 5 from the clinical subscale items raised a red flag for the fit of the model and were withdrawn. We hypothesize that this finding could be related to sample characteristics in each study. Our sample was composed of individuals with principal anxiety disorders and excluded individuals with bipolar disorder and developmental disorders. In the Coulombe et al. (2015) study, 36% of the sample had a bipolar disorder. In the Morita et al. (2019) study, 13% of participants had a bipolar disorder, and 14% had a developmental disorder. In the Wang et al. (2023) study, 16% of the sample had a bipolar disorder. Altogether, these sample differences may alter the response patterns of the clinical portion of the MHSQ. Clinical recommendations for the management of anxiety disorders do not systematically encompass pharmacological treatments or the participation in support/help groups, and the bimodal distribution of data for these variables supports the assertion that the items may simply not be relevant as a self-management strategy for numerous individuals with anxiety disorders. Eliminating these items from the CFA showed an improved model fit, particularly considering covariance and a better internal consistency. An improvement to the scale could be to recommend the use of these two items as optional as they are appropriate, but not essential, clinical self-management strategies for anxiety disorders. A “non-applicable” response choice would be offered to participants for items 4 and 5, and consequently, they would not be included in the subscale average scoring; this modification could benefit diverse clinical samples.
Construct validity was predominantly supported for the MHSQ. Consistent with Coulombe et al. (2015) and the concept of personal recovery that includes the goal of living a fulfilling life even in the presence of a mental disorder, the measure of emotional, psychological, and social well-being showed positive moderate-to-large correlations with the empowerment and vitality subscales. We had expected that functioning would also present a correlation with MHSQ, but without specifying the direction. An interpretation of the positive finding is that functioning, as an inherent part of a mental health diagnosis with symptomatology, is more closely related to symptom reduction in a clinical recovery perspective. Most findings for anxiety and depressive symptoms were also negatively correlated with the empowerment and vitality subscales. Considering measures of symptom severity, depressive symptoms (PHQ-9) correlated negatively and moderately with the empowerment and vitality subscales, as expected based on previous findings (Coulombe et al., 2015). However, the clinical subscale did not show a positive association with self-report measures, apart from a slight correlation with worry (PSWQ). It is to be noted that Coulombe and colleagues (2015) did not hypothesize that result, but they reported positive correlations with GAD-7 and PHQ-9. There is a possibility that differences could be related to using the BAI scale instead of the GAD-7 in our study, but it would not explain the results for the PHQ-9 as we used the same depression measure. We hypothesize that these differences are more likely to be related to the more diagnostically diverse clinical population in the Coulombe et al. (2015) study, compared to our sample, composed exclusively of patients suffering from an anxiety disorder, which would predispose BAI scores to lie at the higher end of the scales. A striking difference between samples is probably related to depressive symptoms. In Coulombe’s study, most participants experienced predominant mood disorders, either a diagnosed depressive disorder (55.7%) or bipolar disorder (36.2%). In our sample, only 23.8% of participants met the criteria for a depressive disorder, and depression was always a comorbidity rather than the principal diagnosis. Contrary to Coulombe et al. (2015) and Wang et al. (2022), we could not measure criterion validity with our dataset as we did not have another concurrent measure available specifically for the concept of self-management.
This is the first study to examine sensitivity to change for the MHSQ scores. There was evidence of a significant increase in the MHSQ scores of participants between baseline and post-treatment for the clinical and empowerment subscales. It should be noted that this change represented less than a unit in the score of the MHSQ, which ranges from 0 to 4, and that a statistical difference may not necessarily reflect a clinically meaningful change. A threshold of clinical significance would need to be defined. Further studies on responsiveness and sensitivity to change will need to draw on theoretical frameworks and empirical clinical data from trials of self-management support interventions, combined with patient perspectives on meaningful change in self-management strategies. Another aspect to consider is that the clinical subscale refers to service demand and utilization (e.g., information about resources available, consulting a professional, therapeutic process, support or help group). Participants in the tCBT condition were exposed to a group intervention focusing on psychoeducation, group support, and a therapeutic process that cannot be entirely disentangled from self-management strategies in the clinical subscale of the MHSQ. Similarly, other types of clinical interventions, such as individual psychotherapy or pharmacotherapy, would also face a similar overlap, which may indicate that the MHSQ questionnaire addresses treatment as well as self-management.
Some strengths and limitations should be considered in the interpretation of the findings. The characteristics of the sample may influence the generalizability of the results. Overall, participants were experiencing anxiety disorders and multiple comorbidities, and even though they frequently sought mental health care in the past year (e.g., 45.5% psychotherapy, 74.5% medication), they were meeting DSM-5 criteria for anxiety disorders and were motivated to enroll in a clinical trial. They reflect a wide range of clinical profiles in the community. However, from the sociodemographic standpoint, they were predominantly French-speaking women with a favourable economic situation, which may limit the generalizability of findings. By broadening the range of clinical samples in the validation studies of the MHSQ, the study provides valuable new information about the instrument’s psychometric properties and recommendations for improvement. As a limitation of a secondary analysis, we did not have the necessary data to assess fidelity, and the lack of other self-reports measuring self-management or coping strategies limited our ability to establish criterion validity. Further studies are needed to examine test-retest fidelity and criterion validity and investigate the clinical significance of change in self-management.
Overall, the MHSQ is a promising tool for the measurement of self-management strategies among individuals living with an anxiety disorder, and the results of our study are generally concordant with the three previous validation studies (Coulombe et al., 2015; Morita et al., 2019; Wang et al., 2022). Furthermore, as the first study to examine the evolution of the MHSQ score across two time points, there is some evidence that an intervention involving a certain degree of SMS, like tCBT, can show an increase in the frequency of self-management strategies used by an individual. Further research could be conducted alongside the delivery of self-management support interventions to investigate the clinical usefulness of the instrument for patients and health care professionals in clinical trials as well as routine care in the mental health field. As mentioned by Coulombe and colleagues (2015), it would also be interesting for future research to conduct a longitudinal investigation over several years to estimate further the influence of self-management on the evolution of recovery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Canadian Institutes of Health Research (334091, 340410).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to ethical reasons but are available from the corresponding author upon reasonable request.
Author Biographies