
Abstract
Introduction
University students are at heightened risk of experiencing mental health problems. Young people commencing university study for the first time may be especially vulnerable (Cleary et al., 2011), and face unique challenges during the early stages of their university experience. Most students start university during the transition from late adolescence to young adulthood—a time when the onset of many common mental disorders peaks (de Girolamo et al., 2012; Kessler et al., 2007). This period is frequently accompanied by significant life changes, including relocation and separation from familial support networks, transition to partial or full financial independence, establishment of new relationships, the need to balance work and study commitments, and responsibility for self-management of physical and mental health (Cleary et al., 2011). Students often have difficulty navigating these transitions, and as many as 75% of students report subjective experiences of stress in multiple areas of life during their first year of university study (Karyotaki et al., 2020). The COVID-19 pandemic introduced additional challenges for students, including the transition to online learning, disruptions to student jobs, and reduced opportunities to participate in social activities due to campus closures and physical distancing mandates (Aristovnik et al., 2020).
Epidemiological research indicates that at least one in three university students meet criteria for one or more mental disorders each year, with mood and anxiety disorders being the most common diagnoses (Auerbach et al., 2016, 2018). Generalised psychological distress is also common (Sharp & Theiler, 2018), and has been shown to be higher among university students than aged-matched non-students (Cvetkovski et al., 2012; Leahy et al., 2010; Stallman, 2010), though there are some exceptions (Burns & Crisp, 2019; Cvetkovski et al., 2019). Untreated mental disorders have been linked to a range of adverse outcomes in later life, including disability (Moussavi et al., 2007), reduced quality of life (Evans et al., 2007), and suicidal thoughts and behaviours (Mortier et al., 2018). Adding to this burden, mental health problems among university students have also been associated with poorer academic performance (Bruffaerts et al., 2018; Stallman, 2010) and early course exit (Mojtabai et al., 2015). There is also evidence to indicate that mental ill-health has increased in this population since the onset of the COVID-19 pandemic (Fruehwirth et al., 2021; Hamza et al., 2021; Lanza et al., 2022), with as many as 30–40% of students estimated to have experienced elevated anxiety or depressive symptoms during the first 2 years of the pandemic alone (Deng et al., 2021; Li et al., 2021; Wang et al., 2021).
There have been very few longitudinal studies assessing mental health symptoms during and before entry to university. Studies conducted prior to the COVID-19 pandemic generally demonstrated that university student mental health is worse during the first year of university study when compared with before or at entry to university (Bewick et al., 2010; Cooke et al., 2006; Duffy et al., 2020). In addition, there is some evidence to suggest that depressive symptoms peak at the end of the first semester before falling in the second semester (Barker et al., 2018). Studies that have examined students longitudinally over the initial stages of the COVID-19 pandemic have also indicated a worsening of mental health among university students in general, with the strongest evidence for an increase in anxiety symptoms, depression, and other mood disorders (Buizza et al., 2022). Though useful, these studies have some important limitations. Most evidence comes from single-institution studies conducted with students attending universities in North America or the United Kingdom, which limits the generalisability of these findings to other contexts. Furthermore, only one known study, conducted at a Canadian university, has specifically examined the mental health experiences of students transitioning to university during the pandemic period (Howard et al., 2022), which showed that the trajectories of depression and anxiety symptoms increased from the beginning to the end of the first semester and remained elevated thereafter.
A range of psychosocial and interpersonal factors are thought to contribute to fluctuations in student mental health during the course of university study. Factors that have been found to be associated with poorer mental health in the first year of study include lower self-esteem, less frequent exercise, drug use, higher perceived stress, and lower levels of social support or university connectedness (Adams et al., 2021; Duffy et al., 2020). Additional factors that may negatively impact on students’ mental health at other times during their university career include loneliness (Moeller & Seehuus, 2019; Weber et al., 2022), low perceived social support (Ma et al., 2020), financial stress, poor diet, or living alone (Tran et al., 2017), substance use (Skidmore et al., 2016), cyberbullying (Lam et al., 2022), and social media use (Haddad et al., 2021). However, few studies have examined these issues collectively among first-year students, with this time identified as ideal for promoting strategies designed to mitigate or prevent mental health problems from developing (Wyatt et al., 2017).
Supporting the mental health of university students is increasingly recognised as a key priority for universities worldwide. In Australia, all universities are required to have an institution-wide mental health strategy and implementation plan (Australian Government: Department of Education and Training, 2018). However, research has identified significant gaps in the available evidence base to inform effective approaches for university student mental health (Fernandez et al., 2016; Worsley et al., 2022), insufficient capacity of counselling services to meet demand (Stallman, 2011), and poor alignment of existing services with student needs (Priestley et al., 2022). The provision of timely, effective, and appropriate support may be aided by identifying the key factors and characteristics of students at increased risk of mental health problems, as well as identifying specific times throughout the academic year that may be associated with elevated risk.
The current study reports the results of a longitudinal cohort study that collected data from young people (aged 18–25 years) attending university in Australia for the first time in Semester 1, 2021. The study involved four waves of data collection to assess first-year student mental health, before and during their first semester of study: Wave 1 (baseline, February 2021), Wave 2 (March 2021), Wave 3 (April/May 2021) and Wave 4 (June 2021). The study aimed to estimate initial levels of mental health symptoms prior to commencing university, examine changes in symptoms over the course of the first semester of university study, and identify factors associated with both initial symptom levels and change in symptoms over time. The predictors examined in the current study were selected because they (1) have been previously shown to be cross-sectionally associated with mental health outcomes in university students (e.g. financial stress) and/or (2) are prominent and unique settings-based factors (e.g. pressure to succeed, coping with stress/multiple demands), and/or (3) are developmentally salient adjustment-related factors for young adults undertaking university study for the first time (social support/interactions/loneliness).
Methods
Sample
Participants were 340 Australian first-year undergraduate students transitioning to university in Semester 1 2021. Participants were predominantly female (65%), with a mean age of 18.76 years (SD = 1.61). Participants were recruited via paid social media advertisements (Facebook) to complete an online survey in February 2021. Facebook advertisements targeted 18- to 25-year-olds in Australia who were attending university for the first time and included a link to the study webpage and baseline survey. Emails containing study information were also sent to university administrative and wellbeing staff for distribution to students, and messages were sent to university-affiliated student social media groups and associations.
Procedure
Data were collected via four online surveys delivered at 6-week intervals during the first semester of university study in 2021: Baseline (February 2021), Wave 2 (March 2021), Wave 3 (April/May 2021), and Wave 4 (June 2021). Six-week measurement intervals were chosen to balance participant burden with the ability to detect meaningful fluctuations in mental health symptoms and obtain sufficient measurement points within a single semester of university (which was a pragmatic constraint of the study). The baseline survey was completed prior to the start of the semester. Participants who completed the baseline survey were emailed invitations to complete the survey at each subsequent wave. Participants received an AU$15 e-gift card for completing all survey waves. All students provided written informed consent after reading a study information sheet. Ethical approval for the study was obtained from the Human Research Ethics Committee at the Australian National University (Protocol 2020/651).
Survey Measures
Outcome Variables
Mental health outcomes included in the study were symptoms of depression, anxiety, and psychological distress measured with the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001), Generalised Anxiety Disorder (GAD-7) (Spitzer et al., 2006), and Distress Questionnaire (DQ5) (Batterham et al., 2016) scales respectively.
Depression Symptoms
The PHQ-9 includes nine items to assess the presence of symptoms of major depression according to the Diagnostic and Statistical Manual, Fourth Edition (DSM-IV). Respondents rate the degree to which they have experienced each symptom over a 2-week period on a 4-point scale (0 = Not at all to 3 = Nearly every day). Total scores range from zero to 27, with higher scores indicative of greater severity of depressive symptoms (baseline Cronbach α = .88, W2: α = .88, W3: α = .90, W4: α = .90).
Generalised Anxiety Symptoms
The GAD-7 includes seven items that correspond to the DSM-IV criteria for generalised anxiety disorder (Spitzer et al., 2006). Respondents rate items using the same 4-point scale as the PHQ-9. Summed scores produce an overall severity score ranging from zero to 21, with higher scores indicating greater symptom severity (baseline Cronbach α = .91, W2: α = .91, W3: α = .92, W4: α = .93). Both the PHQ-9 and GAD-7 have been shown to have robust psychometric properties in general population and university student samples and detect change over time (Bernd et al., 2008; Byrd-Bredbenner et al., 2021; Kim & Lee, 2019; Kroenke et al., 2010).
Psychological Distress Symptoms
The DQ5 comprises five items to assess symptoms of common mental disorders experienced in the previous 30 days. Participants rate each item on a 5-point scale ranging from (1 = never to 5 = always). Item scores are summed to produce a total score ranging from 5 to 25, with higher scores indicating more severe levels of general psychological distress (baseline Cronbach α = .88). Scores of 5–7 indicate no distress, scores of 8–17 indicate elevated distress, and scores of 18–25 indicate severe distress. The DQ5 has demonstrated excellent sensitivity and specificity (Batterham et al., 2016, 2018).
Demographic Characteristics
The following demographic characteristics were assessed at baseline: age (in years); gender (male/female/other); student status (international/domestic); intention to live in university residential housing (yes/no); financial stress (1 = not at all to 6 = extremely); relocation from home to attend university (yes/no); and state or territory location of university campus (NSW/QLD/ACT/VIC/SA/WA/TAS/NT). Experience of disadvantage was also assessed using four items that asked participants to endorse (yes/no) whether they were from a low socioeconomic background, the first in their family to attend university, from a refugee background, or had been in foster care. Disadvantage was subsequently re-coded into no disadvantage (defined as experiencing none of the four disadvantages) or some disadvantage (defined as experiencing ≥1 of the four disadvantages listed above). For ease of analysis and interpretation, financial stress was also re-coded into no/minimal financial stress (‘not at all’ or ‘a little’) or some/considerable financial stress (‘somewhat’, ‘quite a lot’, ‘considerably’, or ‘extremely).
Psychosocial and Lifestyle Stressors
The following data on psychosocial and lifestyle risk factors were collected at baseline: alcohol consumption, loneliness, thwarted belongingness, social support, social media use, pressure to succeed, and trouble coping.
Alcohol Consumption
Alcohol consumption over the past month was measured with the 3-item Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) (Bush et al., 1998). Each item is rated on a 5-point scale, with total scores ranging from zero to 12. Higher scores indicate higher levels of alcohol consumption. In men, a score of 4 or more is considered positive for hazardous alcohol consumption; in women, a score of 3 or more is considered positive. The AUDIT-C has demonstrated adequate specificity and sensitivity among young people (García Carretero et al., 2016; Liskola et al., 2018), and reliability was acceptable in the present study (baseline Cronbach α = .82).
Loneliness
Loneliness over the previous two weeks was assessed using the 6-item De Jong Gierveld Loneliness Scale (de Jong Gierveld & van Tilburg, 2006). Items are rated on a 5-point scale (No!, No, More or Less, Yes, Yes!) and for this study, responses of No! and No were coded as 0, and More or Less, Yes, and Yes! Were coded as 1. Responses are summed, and total scores range from zero to 6, with higher scores indicating greater feelings of loneliness. The internal consistency of the scale was adequate (baseline Cronbach α = 0.78).
Thwarted belongingness
Thwarted belongingness was measured with the 9-item thwarted belongingness subscale of the Interpersonal Needs Questionnaire-15 (INQ-15) (Van Orden et al., 2012). Items are rated on a 7-point scale (1 = Not at all true for me to 7 = Very true for me) and averaged to produce a total score after reverse-coding of selected items. Higher scores indicate greater levels of thwarted belonging. The INQ-15 has demonstrated robust psychometric properties in university student samples (Li et al., 2015; Van Orden et al., 2012), and internal consistency was high in the present sample (baseline Cronbach α = .89).
Social Support
Perceived social support was assessed using the 5-item version of the Schuster Social Support Scale (Schuster et al., 1990). Participants were asked to rate how often they had supportive and negative interactions with their friends (5 items) and family (5 items) on a 4-point scale (0 = Never to 3 = Often). Of the 5 items, 2 indicate positive interactions (e.g., My friends make me feel cared for) and 3 items indicate negative interactions (e.g., My friends make too many demands on me). Support from family and friends were combined to produce two scores, one for supportive social interactions and one for negative social interactions. Higher scores indicate more frequent supportive or negative social interactions. The Schuster Social Support scale has previously demonstrated acceptable reliability (Schuster et al., 1990). However, internal consistency was marginal in the current sample at baseline (supportive social interactions: Cronbach α = .68; negative social interactions: Cronbach α = .76).
Social Media Use
Social media use was measured with the 6-item Bergen Social Media Addiction Scale (BSMAS) (Andreassen et al., 2017), which is a modified version of the Bergen Facebook Addiction Scale (Andreassen et al., 2012). The scale assesses the symptoms of social media addiction (i.e., salience, conflict, mood modification, withdrawal, tolerance, and relapse), with each item rated on a 5-point scale (1 = Very rarely to 5 = Very often). Scores range from 6 to 30, with higher scores indicating greater social media addiction. The original version of the scale has demonstrated sound psychometric properties (Andreassen et al., 2012), and internal consistency of the BSMAS in this study was acceptable (baseline Cronbach α = .83).
Participants were also asked single item bespoke measures assessing experiences (yes/no) of any of the following over the past year: feeling too much pressure to succeed or having trouble coping.
Statistical Analyses
Descriptive statistics and estimated means for the outcome variables at each time point were obtained using SPSS 28 (IBM Corp, 2021). Latent growth curve models were used to estimate initial levels (intercept) and change over time in PHQ-9, GAD-7, and DQ-5 scores. This approach is highly suited to identifying predictors of both level and change in outcomes based on longitudinal data, as all available data are retained in the analysis. Latent growth models were estimated using Mplus 8.1 (Muthén & Muthén, 2017). The intercepts of the outcome variables at the four time points were fixed at zero, with subsequent time points treated as equidistant for estimating linear slope, using a maximum likelihood estimator (see, e.g., (Geiser et al., 2013)). All available data were incorporated into the models irrespective of whether participants missed one or more follow-up assessments, under the assumption that missingness was unrelated to unobserved variables (missing-at-random), using a maximum likelihood estimator. Separate models were estimated for the three mental health outcomes (PHQ-9, GAD-7, DQ5), with an identical set of putative predictors of mental health included as independent variables of both intercept and slope for each latent growth model (refer to measures section).
Power
Our sample of n = 340 was sufficient to detect a small-medium effect size for a change in R2 (f2 = 0.07) with 80% power and up to 20 predictors in the regression model. Accounting for attrition, the completer sample (n = 190) remained sufficient to detect a small-medium effect size for a change in R2 (f2 = 0.12) under the same assumptions, although noting that we used all available data in the latent growth model such that power would have been greater than this estimate. Smaller changes in R2 would be unlikely to have clinical or public health significance.
Results
Baseline Characteristics of the Study Participants (N = 340).
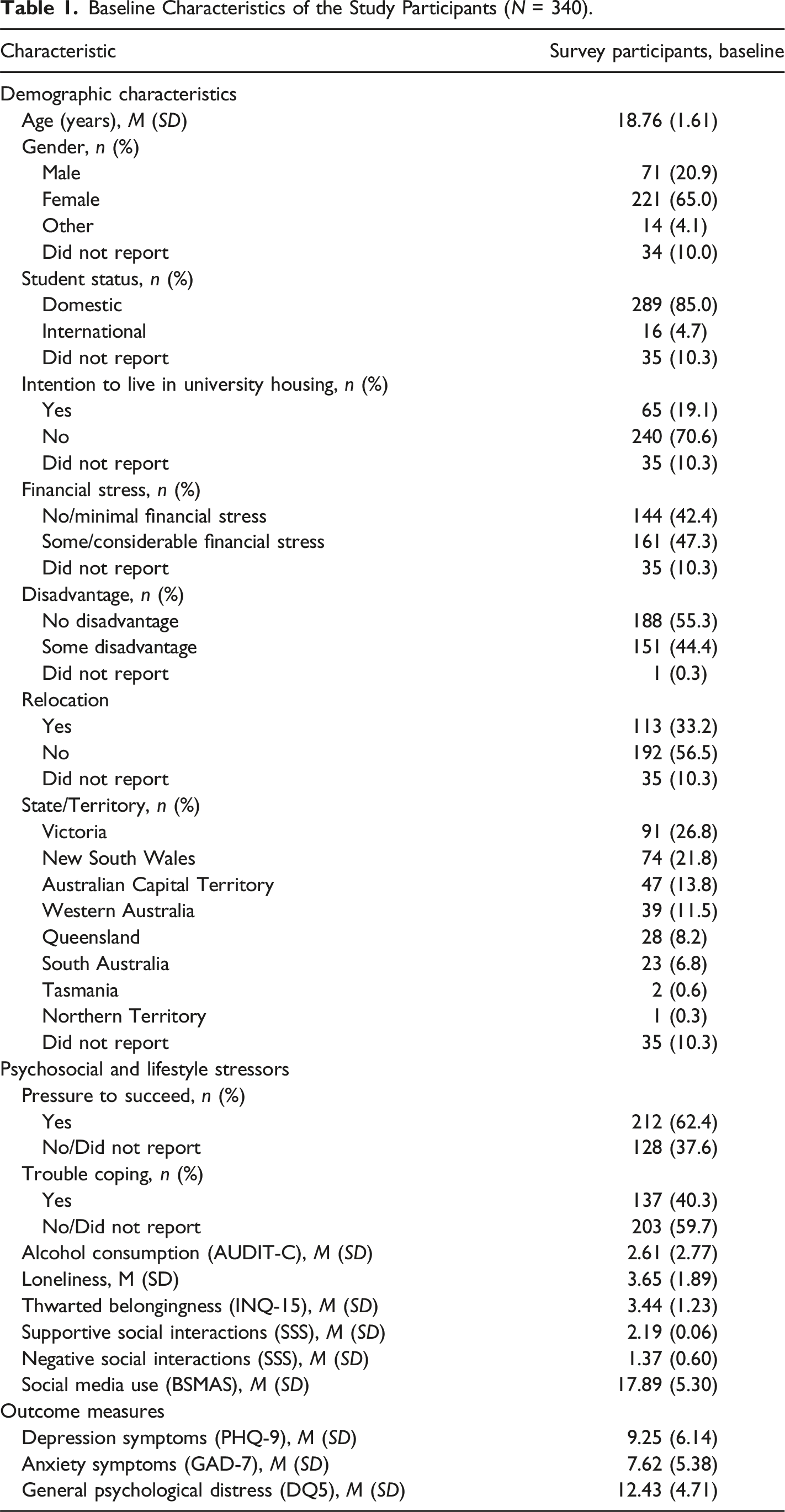
The sample reported an average level of alcohol consumption under the cut-offs for hazardous levels of drinking. On average, participants had mild levels of depression and anxiety symptoms at baseline, and elevated symptoms of psychological distress.
Symptoms of Depression, Anxiety, and Distress
Figure 1 shows the estimated means for depression, anxiety and distress across all time points based on latent growth curve models. There was no significant linear change observed over time for depression (F(1,3) = 1.35, p = .261) or anxiety (F(1, 3) = .296, p = .828) symptoms. However, a significant effect of time was observed for psychological distress (F(1,3) = 3.05, p = .03). Posthoc contrasts revealed that distress was significantly higher at wave 3 compared to baseline (t = 2.91, p = .004). Estimated marginal means (and standard errors) for depression (PHQ-9), anxiety (GAD-7), and distress (DQ-5).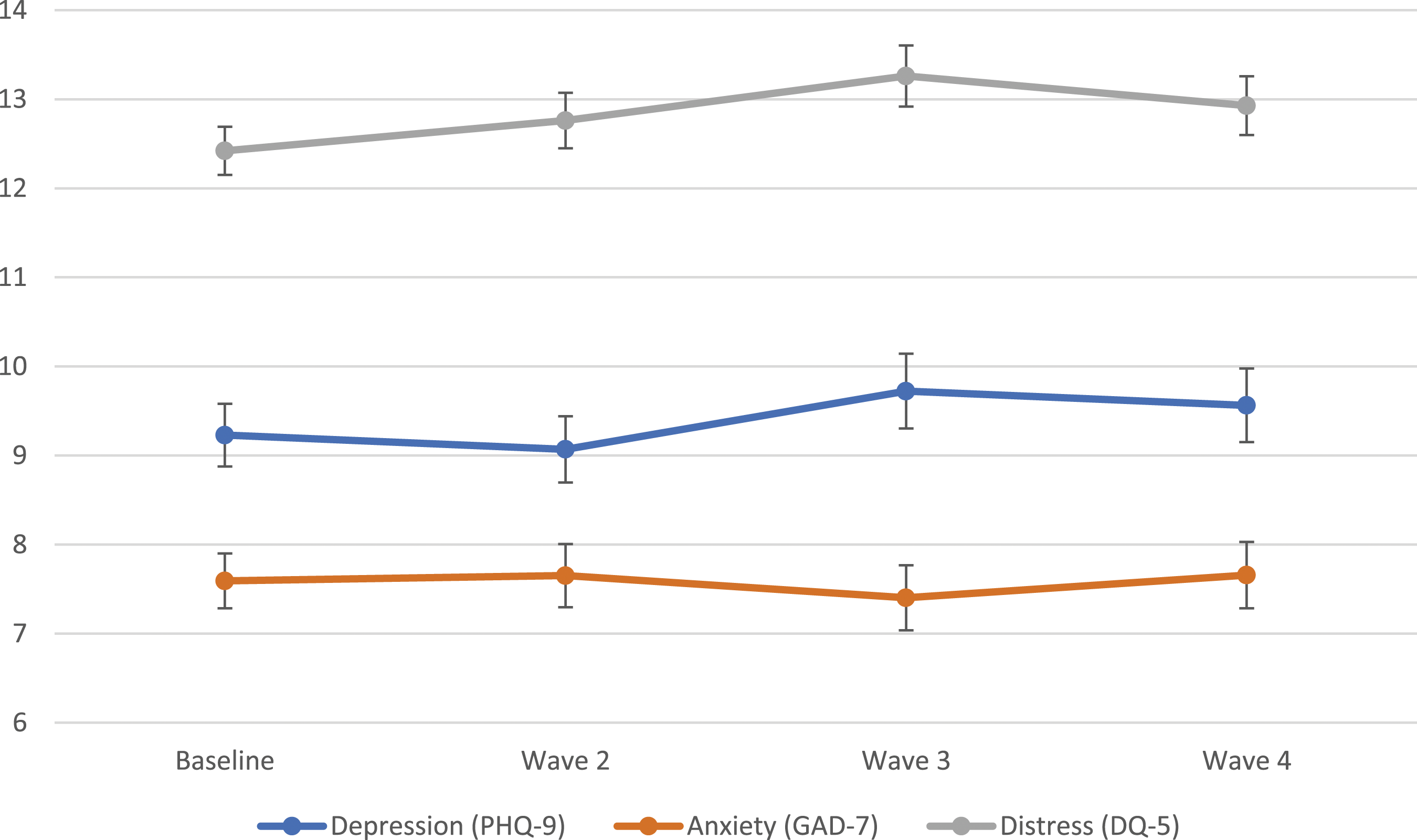
Predictors of Initial Symptoms and Change in Symptoms Over Time
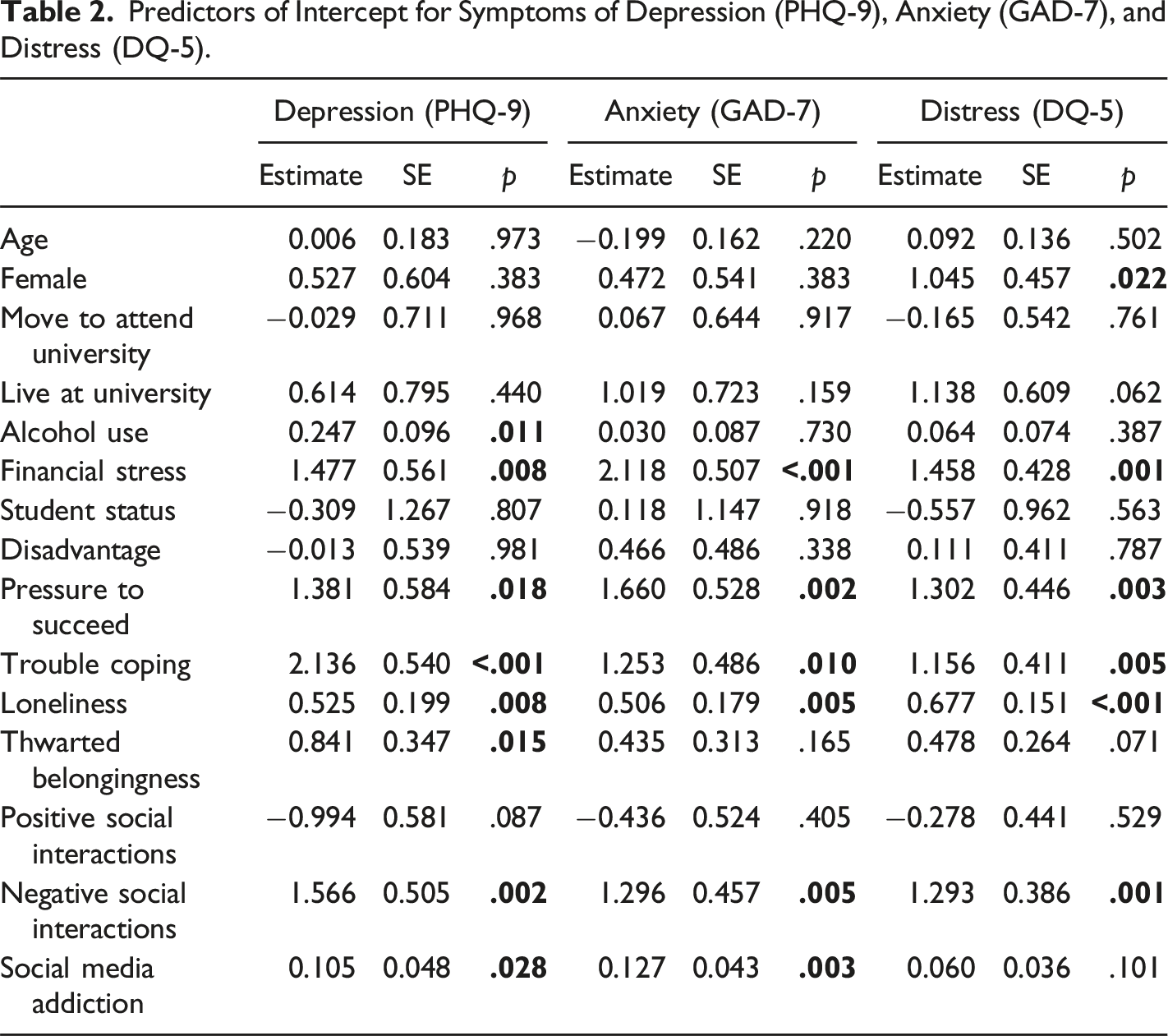
Predictors of Intercept for Symptoms of Depression (PHQ-9), Anxiety (GAD-7), and Distress (DQ-5).
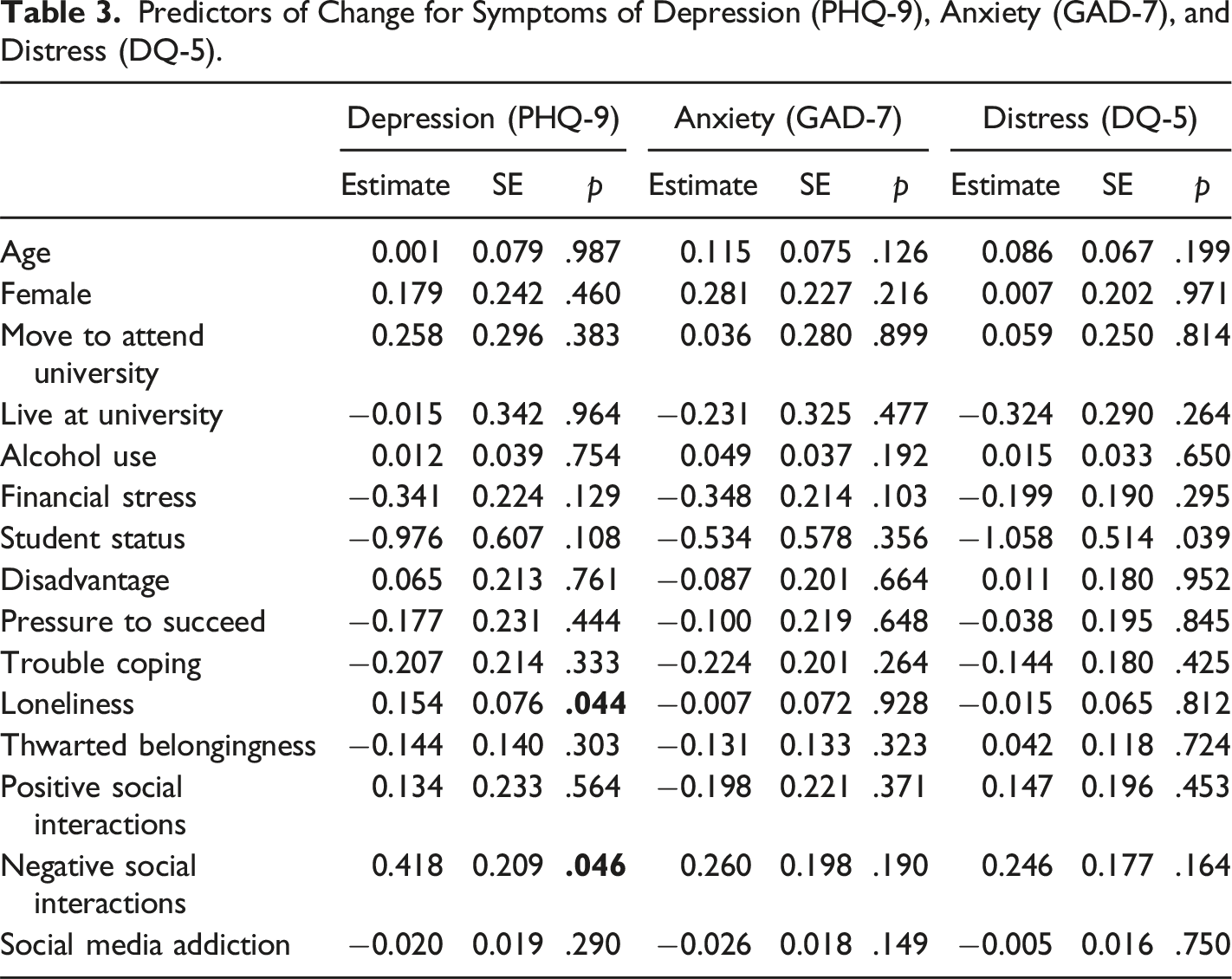
Predictors of Change for Symptoms of Depression (PHQ-9), Anxiety (GAD-7), and Distress (DQ-5).
Discussion
Transition to university represents a key time of vulnerability for young people’s mental health. The results of this study showed there were a range of demographic, psychosocial, and lifestyle factors related to the likelihood of experiencing depression, anxiety, and psychological distress at initial university commencement. These included greater alcohol use and financial stress, greater loneliness, increased negative social interactions, thwarted belongingness and problematic social media use, as well as feeling pressure to succeed and difficulty coping during the past year. These factors impacted depression, anxiety, and distress almost uniformly, with some exceptions. Alcohol use and thwarted belongingness was associated only with depression, whereas female gender was associated only with psychological distress, and problematic social media use was associated with symptoms of depression and anxiety but not distress. However, the transition to university itself did not appear to have a major impact on mental health symptoms more broadly, as we did not identify significant changes in depression or anxiety symptoms across the study waves, and there was only a limited increase in psychological distress, which was significant only at one time point, from baseline (measured in February 2021) to Wave 3 (measured in April/May 2021).
The finding that symptoms of anxiety and depression generally remained stable over the course of the first semester is at odds with previous research that has found a small deterioration in mental health among first-year students during this time (Bewick et al., 2010; Cooke et al., 2006; Duffy et al., 2020; Fruehwirth et al., 2021; Howard et al., 2022). These previous studies have typically recruited larger samples (ranging from 419 to 24,234) and collected data over longer timeframes (e.g., prior to university and throughout the first year of study), suggesting that our analysis may not have been sufficiently powered to detect relatively small changes in students’ mental health symptoms over a shorter period of time. In addition, earlier studies conducted during the COVID-19 pandemic collected data during the initial stages of the outbreak (Fruehwirth et al., 2021; Howard et al., 2022), at a time when students were still adjusting to disruptions in their daily lives due to pandemic-related measures (Aristovnik et al., 2020). There is some evidence to indicate that coping improved over the course of the pandemic (Weber et al., 2022), and our findings are in line with a growing number of studies that have indicated that mental health symptoms either remained stable or, in some cases, improved as the pandemic progressed (Goh et al., 2023; Stamatis et al., 2022). This might suggest that students had already developed coping strategies during the early pandemic period (in 2020), which may have prepared them for some of the challenges and changed circumstances faced by young people during the transition to university study in 2021 (i.e. an increased emphasis on autonomous learning and the need to develop alternative ways of forming and maintaining social connections). Additionally, improved awareness of mental health and increased access to remote support as a result of the pandemic could have better equipped students to manage their mental health during the transition to university. The increase in psychological distress observed at Wave 3 may be attributable to the timing of this assessment. Wave 3 data collection occurred just before the start of the end of semester examination period for most universities in Australia, a typical time of increased stress for students.
Several key interpersonal factors were shown to be associated with levels of depression, anxiety, and distress. Loneliness, lack of social support from family and friends (characterised by negative interactions), and lack of belongingness were of particular importance for initial symptom levels. Importantly, interpersonal factors were also the only factors shown to be associated with change in mental health symptoms, with increased levels of loneliness and greater negative interactions with family and friends at baseline predicting a greater increase in depression over the course of the semester. This is consistent with previous research (Moeller & Seehuus, 2019), particularly studies conducted during the COVID-19 pandemic (Ma et al., 2020; Weber et al., 2022). It is likely that loneliness and lack of social support were particularly challenging during the pandemic, when opportunities to develop supportive social connections through traditional methods such as university orientations, social, and networking events may have been limited by social distancing measures. Social support has an established theoretical and empirical association with mental health (De Silva et al., 2005; Wang, 1998). Theoretical models suggest that social support has both a direct positive effect on wellbeing (Cohen & Wills, 1985), and also plays a role in helping individuals cope with stressful life events. As transition to university can be a stressor, particular focus should be placed on increasing connections for students who arrive at university without strong social networks or support, as well as those who move away from existing support systems to attend university.
Disadvantage was not significantly associated with mental health during the first semester of university. Many universities have initiatives that provide targeted support to students from disadvantaged backgrounds, due to increased risk of difficulty transitioning to the university environment. Our results suggest that it was not these factors per se that impacted mental health, with other factors like social support and belongingness explaining greater variance in mental health difficulties. However, financial stress emerged as a robust predictor of initial depression, anxiety, and distress. This is in line with previous research, which has found that subjective measures of financial concern may be more reliable predictors of mental health outcomes than objective indicators (McCloud & Bann, 2019). Several factors may account for this relationship, including concerns about future financial stability, the need to prioritise work over academic study, reduced participation in social and recreational activities leading to feelings of loneliness and isolation, as well as elevated overall stress and reduced self-esteem (Frankham et al., 2020; Moore et al., 2021). Consequently, one approach to managing this risk would be to screen students early to identify who may be at risk of, or already exhibiting, poor mental health, and targeting services to these students to ensure they are well supported and able to develop and thrive in the university environment.
Similar to past research (Beiter et al., 2015; Farrer et al., 2016), pressure to succeed and difficulty coping were shown to be consistent predictors of initial symptom levels. University study places new challenges, pressures, and demands on young people, who may embody strong internal and external expectations to succeed, while adjusting to an unfamiliar environment where they are expected to juggle multiple competing demands. Many students, both in this study and in previous research, have indicated that they struggle with these pressures, and there is evidence to show that psychosocial factors such as pressure to succeed represent a major source of student stress (Beiter et al., 2015). Providing students with accessible skills training, such as managing expectations and coping with stress and academic workloads, may help to reduce distress and improve student mental health. Higher alcohol use at baseline was also associated with higher depression symptoms. It has been established that students with elevated depressive symptoms face escalated risk of negative alcohol-related consequences (e.g. academic problems, withdrawal from study, interpersonal problems, suicidality) (Kenney et al., 2018). Given that excessive drinking behaviour can be emphasised at the start of university, it is important to target known factors that increase risk of adverse outcomes among students with elevated depressive symptoms who engage in hazardous drinking (Fredman Stein et al., 2022; Kenney et al., 2018).
Limitations
There are several limitations to this study. Firstly, this study included a cross-sectional component, meaning that we were unable to tease out causal relationships between initial symptoms and baseline predictors. In addition, although we considered a range of demographic and psychosocial predictors, there are likely to be other factors not examined here that may also be relevant, such as the impact of other lifestyle factors such as diet, sleep, and physical activity on mental health outcomes. Moreover, the relatively short time frame of the study may have limited our ability to detect subtle changes in symptoms over time and capture complex symptoms trajectories. A study with a longer time frame would provide a more robust analysis and enable dips and troughs in symptoms to be observed. Furthermore, limited change in symptom outcomes observed over the course of the study may have influenced the strength and reliability of the identified predictors of change. Further, multiple comparisons mean that type I errors for small effects are possible. Males and international students were underrepresented in the sample. This is typical of participation in mental health research (Woodall et al., 2010), but may limit the generalisability of the findings to these groups. Finally, study attrition was also relatively high.
Conclusion
In this study, no overall increases in symptoms of depression, anxiety, and distress were observed among first-year university students throughout their first semester of study. This suggests that the transition to university may not generally lead to a decline in mental health. Poorer mental health upon entering university was predicted by a range of factors, most of which had a similar impact on symptoms of depression, anxiety, and distress. Only baseline loneliness and negative social interactions were identified as predictors of symptom change over the course of the semester, with both factors predicting a greater increase in depressive symptoms. The findings suggest that addressing pre-existing risk factors like loneliness and negative social interactions may be especially important for first-year students to prevent an increase in depressive symptoms during the first year. Additionally, interventions aimed at helping students to manage financial stress, fostering social connections, and promoting effective coping strategies may further support students’ mental health during this period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Australian Foundation for Mental Health Research and the John James Foundation. LMF is supported by an ARC DECRA DE190101382. AG is supported by an ANU College of Health and Medicine TRANSFORM Career Development Fellowship. ALC is supported by NHMRC Fellowship 1173146.
Ethical Statement
Data Availability Statement
The data are available from the lead author upon request.