
Abstract
Although beliefs about the extent to which emotions are amenable versus immutable to control (i.e., implicit theories of emotion) have been linked to various mental health indices, mediators of this relationship remain unclear. This study extends prior research by examining dimensions of emotion regulation (ER) difficulties as parallel mediators in the relationship between emotion controllability beliefs and stress and well-being among university students (n = 483). Higher emotion controllability beliefs were found to be associated with fewer difficulties in emotional clarity, emotional acceptance, effective ER strategy access, impulse control, and goal-directed behaviour. Moreover, the relationship between emotion controllability beliefs and stress and well-being was mediated by emotional clarity and strategy access. Results implicate difficulties understanding one’s own emotions and accessing effective ER strategies as key mechanisms through which lower emotion controllability beliefs may be associated with higher stress and lower well-being. Conversely, better emotional clarity and greater access to effective ER strategies may explain why higher emotion controllability beliefs are associated with better mental health. The present study provides support for the role of implicit theories of emotion in clarifying patterns of adaptive versus maladaptive emotional responding, and sheds light on the cognitive processes underlying individual differences in emotion regulation and mental health. Furthermore, findings offer novel insight regarding the specific emotion regulatory mechanisms through which emotion controllability beliefs may be associated with mental health.
Introduction
The ability to effectively manage emotional responses in everyday life is fundamental to well-being (Berking & Wupperman, 2012; Kraiss et al., 2020). Conversely, difficulties regulating emotion have been linked to mental health disorders (e.g., depression, anxiety; Everaert & Joormann, 2019; Ouellet et al., 2019; Visted et al., 2018). With many formative theories of mental health, stress, and coping rooted in the premise that cognition plays a causal role in emotional responding, significant empirical attention has been paid to the cognitive processes contributing to emotional problems (e.g., Ford & Gross, 2019; Gross, 2015; Hofmann et al., 2013). In the current study, we focus on a particular type of cognition – peoples’ beliefs about the controllability of emotion – and how they relate to emotion regulation, stress, and well-being, so as to further our understanding of the cognitive processes facilitating and hindering mental health.
Emotion controllability beliefs and mental health
Research suggests that people hold varying beliefs about the fundamental controllability of a variety of human attributes and traits (e.g., intelligence, athletic ability, emotion; Burnette et al., 2013; Costa & Faria, 2018). Historically, these beliefs about controllability have been referred to as implicit theories (Dweck, 2000; Dweck et al., 1995). In the domain of emotion, implicit theories refer to the core beliefs people hold about the controllability of emotional experiences (Ford & Gross, 2019; Tamir et al., 2007). Wherein people with higher emotion controllability beliefs (i.e., an incremental emotion theory) believe that everyone can learn to control and change the emotions that they have, people with lower emotion controllability beliefs (i.e., an entity emotion theory) believe that people have relatively little control over their emotions and cannot really change them (Tamir et al., 2007). Notably, empirical work in both clinical and community samples has provided evidence that emotion controllability beliefs are associated with a range of mental health indices. Higher emotion controllability beliefs have been linked to more favorable emotional experiences, greater well-being, and better social and emotional adjustment (Ford & Gross, 2019; King & dela Rosa, 2019; Tamir et al., 2007). Lower emotion controllability beliefs have been associated with higher levels of psychological distress, anxiety, and depressive symptoms (De Castella et al., 2013; King & dela Rosa, 2019; Somerville et al., 2024).
The mediating role of emotion regulation
While researchers have highlighted important associations between emotion controllability beliefs and mental health, more work is needed to clarify why these relationships exist. In terms of potential mediating mechanisms, a leading hypothesis within the implicit theory of emotion literature is that emotion controllability beliefs are associated with differences in key emotion regulation tendencies that, in turn, are associated with more or less adaptive emotional functioning and mental health (Ford & Gross, 2019; King & dela Rosa, 2019; Kneeland et al., 2016). Specifically, scholars have proposed that the more a person believes emotions are controllable, the more likely they are to believe that their own efforts to regulate emotion will be effective (Ford & Gross, 2019). In turn, higher emotion controllability beliefs may prompt individuals to engage in earlier, more active attempts to regulate their own maladaptive emotional responses before their deleterious effects can be fully experienced, facilitating more favorable emotional functioning and better mental health over time (Tamir & Mauss, 2011). Conversely, people who believe emotions to be relatively immutable may be less likely to view their own emotions as amenable to control (Ford & Gross, 2019). From this perspective, lower emotion controllability beliefs may lower one’s engagement in early-stage emotion regulation, making it more difficult to modulate maladaptive emotions as they unfold and increasing the risk of long-term mental health difficulties (Ford & Gross, 2019; Kneeland et al., 2016; Tamir & Mauss, 2011).
Broadening the scope of emotion regulation: a multidimensional approach
Emotion regulation broadly refers to any conscious or nonconscious, intrinsic or extrinsic process involved in the monitoring, evaluation, and modulation of emotional responses (Gross, 2015). To date, empirical work on emotion controllability beliefs has narrowly focused on the use of specific emotion regulation strategies as potential mediators in the relationship between emotion controllability beliefs and mental health. For instance, higher emotion controllability beliefs have been found to be associated with greater use of cognitive reappraisal (i.e., an adaptive emotion regulation strategy that involves actively changing one’s cognitive construal of emotional events so as to alter their meaning and impact; King & dela Rosa, 2019; Kneeland et al., 2016a; Tamir et al., 2007) which, in turn, is linked to greater well-being and lower psychological distress (De Castella et al., 2013; King & dela Rosa, 2019). Similarly, lower emotion controllability beliefs have been linked to greater emotional avoidance, which has been associated with less effective regulation of unwanted affect (Kappes & Schikowski, 2013). Nevertheless, more work is needed to understand how emotion controllability beliefs are associated with broader dimensions of emotion regulation difficulties, and in turn, mental health.
Drawing from key conceptualizations of emotion regulation in clinical psychology (e.g., Berking & Whitley, 2014; McRae & Gross, 2020), we posited that a broader understanding could be developed by considering how emotion controllability beliefs relate to the broader emotion-related skills underlying the effective monitoring, evaluation, and modulation of emotional experiences, as opposed to isolated strategies such as cognitive reappraisal. Specifically, we adopted Gratz and Roemer’s (2004) popular conceptualization of emotion regulation difficulties as a multidimensional construct involving (a) a lack of awareness around one’s emotions, (a) a lack of clarity or understanding around one’s emotions, (c) nonacceptance of one’s emotional responses, (d) limited access to emotion regulation strategies perceived as effective, (e) difficulties controlling impulses when experiencing negative emotions, and (f) difficulties engaging in goal-directed behaviour when experiencing negative emotions. According to this conceptualization of emotion regulation, difficulties in these six areas are indicative of emotion dysregulation, a transdiagnostic risk factor for a range of mental health disorders (Everaert & Joormann, 2019; Ouellet et al., 2019; Visted et al., 2018).
Although difficulties across the multiple dimensions of emotion regulation have not yet been explored in relation to emotion controllability beliefs, their relevance to key mental health outcomes has been well established. For instance, difficulties in emotional clarity, emotional acceptance, strategy access, impulse control, and goal-directed behaviour (but not in emotional awareness) have all been linked to increased reports of insomnia, anxiety, social anxiety and dysfunction, depression, somatic complaints, and negative affect (Helbig-Lang et al., 2015; Saxena et al., 2011). Further, difficulties across all dimensions (including emotional awareness) have been associated with less frequent experiences of positive affect in daily life (Saxena et al., 2011). Despite their commonalities, these six dimensions of emotion regulation difficulties also reveal distinct patterns of associations with other clinically relevant outcomes. For instance, a study by Moriya and Takahashi (2013) found that only difficulties in emotional clarity and strategy access mediated the relationship between interpersonal stress and depressive symptoms, whereby greater interpersonal stress was associated with more difficulty across both dimensions which led, in turn, to greater depressive symptoms. The relevance of specific emotion regulation difficulties may also differ as a function of demographic factors; for example, greater difficulties with nonacceptance and impulse control have been linked to more frequent self-harm in men, while greater difficulties in emotional awareness, emotional clarity, strategy access, and goal-directed behaviour were linked to more frequent self-harm in women (Gratz & Roemer, 2004).
The present study
Research has supported significant associations between emotion controllability beliefs and mental health correlates (Ford & Gross, 2019; Somerville et al., 2024). While scholars have advocated that individual differences in emotion regulation likely mediate these links (King & dela Rosa, 2019; Kneeland et al., 2016), studies investigating this hypothesis have only investigated the mediating role of specific emotion regulation strategies (e.g., cognitive reappraisal). Nevertheless, the literature also points to notable links between dimensions of emotion regulation difficulties as conceptualized by Gratz and Roemer (2004) and indices of mental health (e.g., Helbig-Lang et al., 2015; Moriya & Takahashi, 2013; Saxena et al., 2011), suggesting that these dimensions may also serve as mechanisms in the relationship between emotion controllability beliefs and mental health. Thus, this study extends previous research by first exploring associations between emotion controllability beliefs and multiple dimensions of emotion regulation difficulties. Specifically, we hypothesized that higher emotion controllability beliefs would be associated with fewer difficulties in emotional awareness, clarity, and acceptance, perceived access to emotion regulation strategies, impulse control, and goal persistence when experiencing negative emotions (H1). Additionally, the present study sought to deepen current understanding of the relationship between emotion controllability beliefs and mental health by investigating difficulties in the multiple dimensions of emotion regulation as mediators in the relationship between emotion controllability beliefs and stress and well-being. It was hypothesized that higher emotion controllability beliefs would be associated with lower stress and higher well-being via fewer difficulties across all dimensions of emotion regulation difficulties (H2).
Method
Participants and procedure
This study was conducted following the approval of the institutional ethics review board. Participants were recruited from a large Canadian university via email using contact information from a database of students who had expressed interest in participating in future studies related to stress and coping, as well as through online recruitment flyers posted on student webpages.
All participants were provided a personalized link to an online survey. Upon opening the survey link, participants viewed a description of the study and provided their informed consent. Compensation included entry into a raffle for a chance to win one of ten $30 gift certificates. At the end of the survey, participants were also offered online feedback about their current stress and a list of mental health resources. Participants were included in the primary analyses if they correctly responded to all three attention items dispersed throughout the survey, indicated that they were currently registered in university, and were between 18 and 25 years old. Of the 573 participants who submitted survey responses, 483 met these criteria (Mage = 20.20 years, SD = 1.46; 80.95% women). Self-reported ethnicities were as follows: 59.01% White, 15.53% East Asian, 8.07% mixed, 3.73% Southeast Asian, 3.52% South Asian, 2.48% Arab, 1.66% Latin American, 1.24% Black, 0.21% Indigenous, and 3.52% other (1.04% preferred not to answer).
Measures
Emotion controllability beliefs
Emotion controllability beliefs were measured using the four-item Implicit Theories of Emotion Scale (ITES; Tamir et al., 2007), which includes two incremental theory items (e.g., “if they want to, people can change the emotions that they have”) and two entity theory items (e.g., “the truth is, people have very little control over their emotions”), rated on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). Entity theory items were reverse-scored and an average was calculated such that higher scores reflected higher emotion controllability beliefs (range: 1–5). The ITES has demonstrated acceptable internal consistency (α = .77 – .78) in university student samples (De Castella et al., 2013; Tamir et al., 2007) and was also acceptable in the current study (α = .75).
Dimensions of emotion regulation difficulties
The Difficulties in Emotion Regulation Scale Short Form (DERS-SF; Kaufman et al., 2015) was used to measure dimensions of emotion regulation difficulties. This 18-item measure adapted from the original 36-item DERS (Gratz & Roemer, 2004) assesses difficulties in six areas of emotion regulation: emotional awareness (e.g., “I pay attention to how I feel”, reverse-coded), emotional clarity (e.g., “I have difficulty making sense out of my feelings”), emotional acceptance (e.g., “when I’m upset, I become embarrassed for feeling that way”), access to strategies perceived as effective in regulating negative emotion (e.g., “when I’m upset, I believe there is nothing I can do to make myself feel better”), impulse control (e.g., “when I’m upset, I become out of control”), and goal persistence when experiencing negative emotion (e.g., “when I’m upset, I have difficulty getting work done”). Items are rated on a five-point Likert scale (1 = never, to 5 = almost always). Both the original DERS and the DERS-SF can be used in terms of the total emotion dysregulation score that they yield and/or their individual subscale scores (Gratz & Roemer, 2004; Kaufman et al., 2015). Accordingly, in the present study, ratings for each subscale were summed to produce scores for each of the six dimensions, such that higher values indicated greater difficulties within that emotion-related competency (range: 3 – 15), and subscale ratings were summed to produce a total emotion dysregulation score (range: 18 – 90). In the initial validation study of the DERS-SF using a college student sample, the total scale demonstrated excellent internal consistency (α = .89) and a correlation of .97 with the original DERS (Kaufman et al., 2015). The subscales also demonstrated strong psychometric properties, with internal consistencies ranging from .78 to .91. This measure had good internal consistency in the present study as well (awareness α = .75, strategies = .80, clarity = .81, acceptance = .84, impulse control = .89, goals = .93; total scale = .90).
Stress
Stress was measured using the Perceived Stress Scale (PSS-4; Cohen et al., 1983). This four-item measure assesses the extent to which individuals appraise their life as having been stressful over the past month (e.g., “in the past month, how often have you felt difficulties were piling up so high that you could not overcome them?”). Participants rated the frequency with which they endorsed each item on a four-point Likert scale (0 = never to 4 = very often). After reverse-scoring two items, a sum score was calculated such that higher scores indicated greater stress. The PSS-4 has demonstrated acceptable psychometric properties in previous studies, even when administered across cultures and in different languages (Lee, 2012; Warttig et al., 2013), and also yielded good internal consistency in the present study (α = .83).
Well-being
Well-being was measured using the Mental Health Continuum-Short Form (MHC-SF; Keyes, 2005, 2009). This 14-item measure asks participants to indicate how often during the past month they have experienced various aspects of emotional (e.g., “during the past month, how often did you feel happy?”), social (e.g., “during the past month, how often did you feel that people are basically good?”), and psychological (e.g., “during the past month, how often did you feel that your life has a sense of direction or meaning to it?”) well-being on a six-point Likert scale (1 = never to 6 = every day). A sum score was calculated, such that a higher sum score indicates higher overall well-being (range: 0 – 70). The MHC-SF has demonstrated good psychometric properties in samples of varying ages and nationalities (see Keyes, 2009) and demonstrated excellent internal consistency in the present study (α = .92).
Data analytic plan
All analyses were conducted using SPSS version 29 (IBM Corp, 2022). To assess the associations between emotion controllability beliefs, emotion regulation difficulties, stress, and well-being, Pearson correlations coefficients were computed. Subsequently, path analysis was conducted to assess the indirect relations of emotion controllability beliefs to stress (Model 1) and well-being (Model 2) through the dimensions of emotion regulation difficulties (i.e., emotion awareness, acceptance, clarity, strategy access, impulse control, and goal persistence) using the SPSS add-on, PROCESS (Model 4; Hayes, 2013). In particular, a non-parametric bootstrap resampling procedure with 10,000 resamples was used to estimate the total and specific indirect effects and their associated 95% bias-corrected confidence interval (CI).
Results
Identifying covariates
Data were first examined to identify potential covariates. Age and race were unrelated to the study variables and are not discussed further. Point-biserial correlations revealed that gender was significantly associated with emotional awareness and acceptance, such that women tended to report greater difficulties accepting their negative emotions and men tended to report greater difficulties in emotion awareness. Point-biserial correlations also revealed that recruitment source (i.e., email or website) was significantly associated with pertinent study variables, such that individuals recruited via webpages reported greater difficulties in emotional clarity, acceptance, and strategy access, higher stress, and lower well-being than individuals recruited via email. As such, partial correlations controlling for gender and recruitment source were computed. Fisher’s r-to-z transformations indicated no significant differences between the partial and Pearson correlations (all p’s > .05). Moreover, controlling for gender and recruitment source did not alter the significance of the mediation analyses; reported results thus exclude covariates.
Associations between emotion controllability beliefs, dimensions of emotion regulation difficulties, stress, and well-being
Descriptive Statistics and Correlations Among Study Variables.
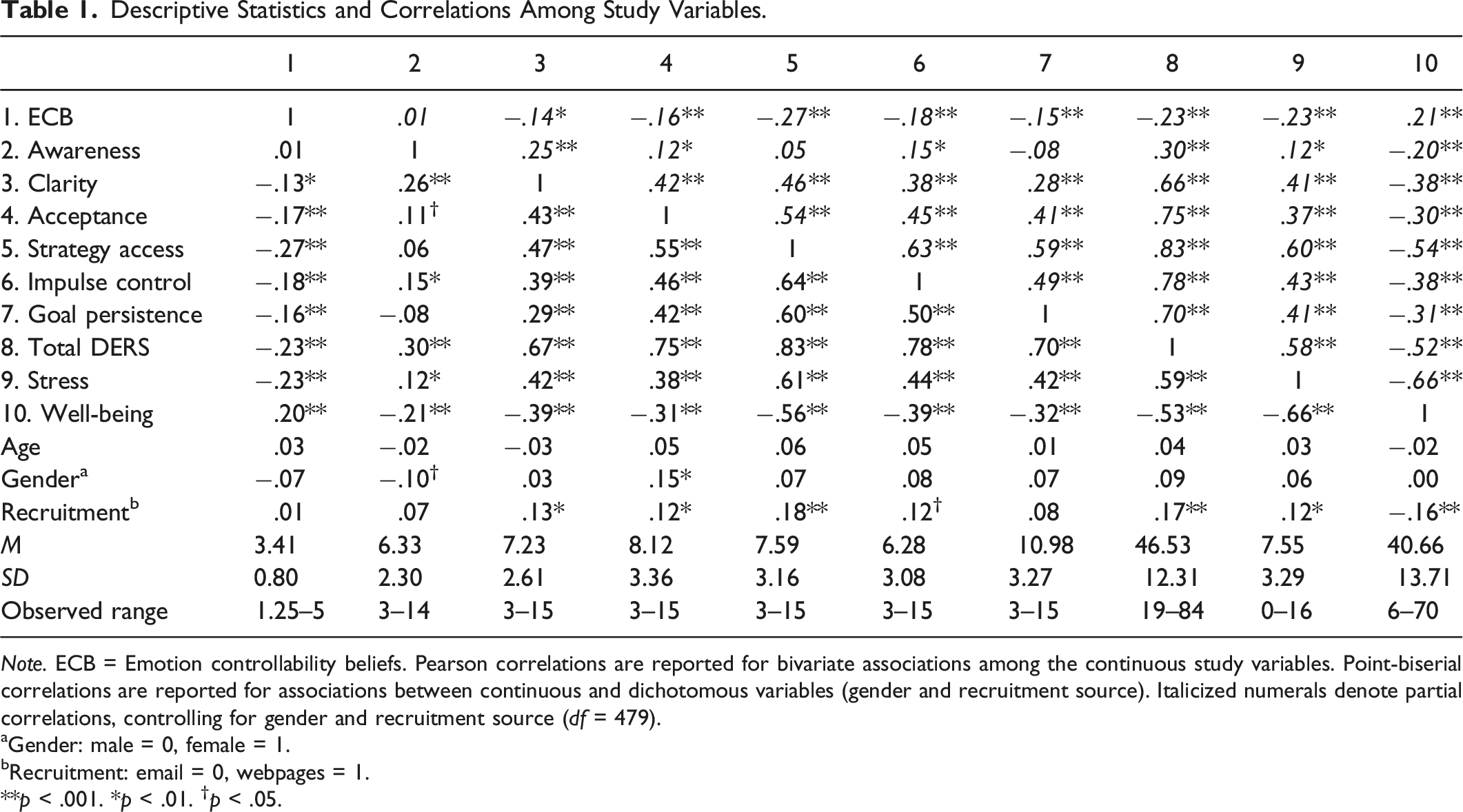
Note. ECB = Emotion controllability beliefs. Pearson correlations are reported for bivariate associations among the continuous study variables. Point-biserial correlations are reported for associations between continuous and dichotomous variables (gender and recruitment source). Italicized numerals denote partial correlations, controlling for gender and recruitment source (df = 479).
aGender: male = 0, female = 1.
bRecruitment: email = 0, webpages = 1.
**p < .001. *p < .01. †p < .05.
Indirect Effects of Emotion Controllability Beliefs on Stress Through the Dimensions of Emotion Regulation Difficulties
Model 1 (Figure 1) was used to assess the relation between emotion controllability beliefs and stress via the dimensions of emotion regulation difficulties. Results revealed that greater emotion controllability beliefs were associated with fewer difficulties in emotional clarity, Indirect Effects of Emotion Controllability Beliefs on Stress Through the Dimensions of Emotion Regulation Difficulties.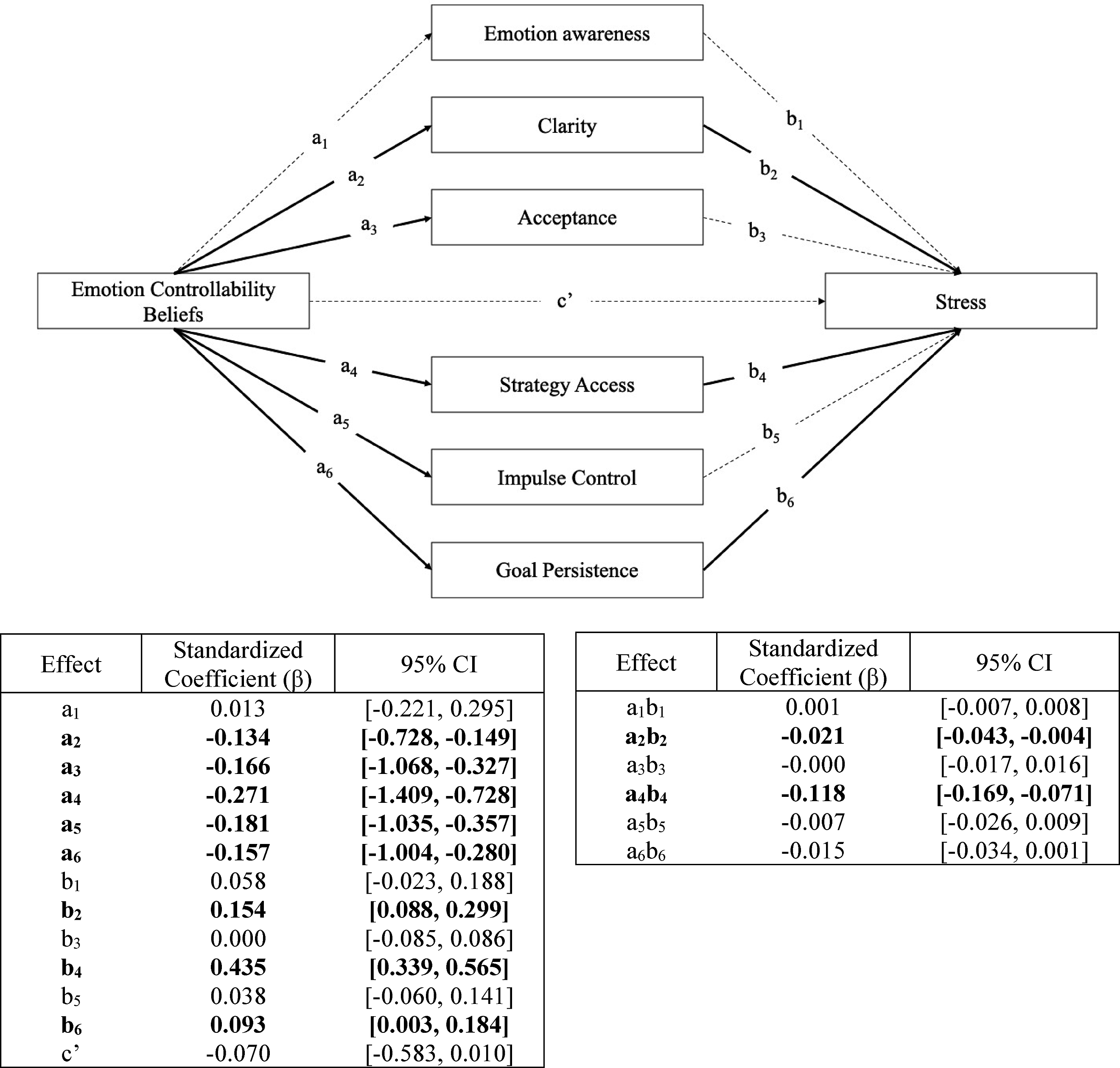
emotional acceptance, strategy access, impulse control, and goal persistence when experiencing negative emotions. However, only difficulties in emotional clarity, strategy access, and goal persistence were positively associated with stress. Inspection of the 95% CIs indicated significant negative indirect effects of greater emotion controllability beliefs on stress through fewer difficulties in emotional clarity and strategy access (95% CIs [−0.043, −0.004] and [−0.169, −0.071], respectively).
Indirect Effects of Emotion Controllability Beliefs on Well-being through the dimensions of emotion regulation difficulties
Model 2 (Figure 2) was used to assess the relation between emotion controllability beliefs and well-being via the dimensions of emotion regulation difficulties. Once again, results revealed that greater emotion controllability beliefs were associated with fewer difficulties in emotional clarity, emotional acceptance, strategy access, impulse control, and goal persistence when experiencing negative emotions. However, only difficulties in emotion awareness, emotional clarity, and strategy access were negatively associated with well-being. Similar to the pattern observed for stress, inspection of the 95% CIs indicated significant positive indirect effects of greater emotion controllability beliefs on well-being through fewer difficulties in emotional clarity and strategy access (95% CIs [0.003, 0.038] and [0.080, 0.186], respectively). Indirect Effects of Emotion Controllability Beliefs on Well-Being Through the Dimensions of Emotion Regulation Difficulties.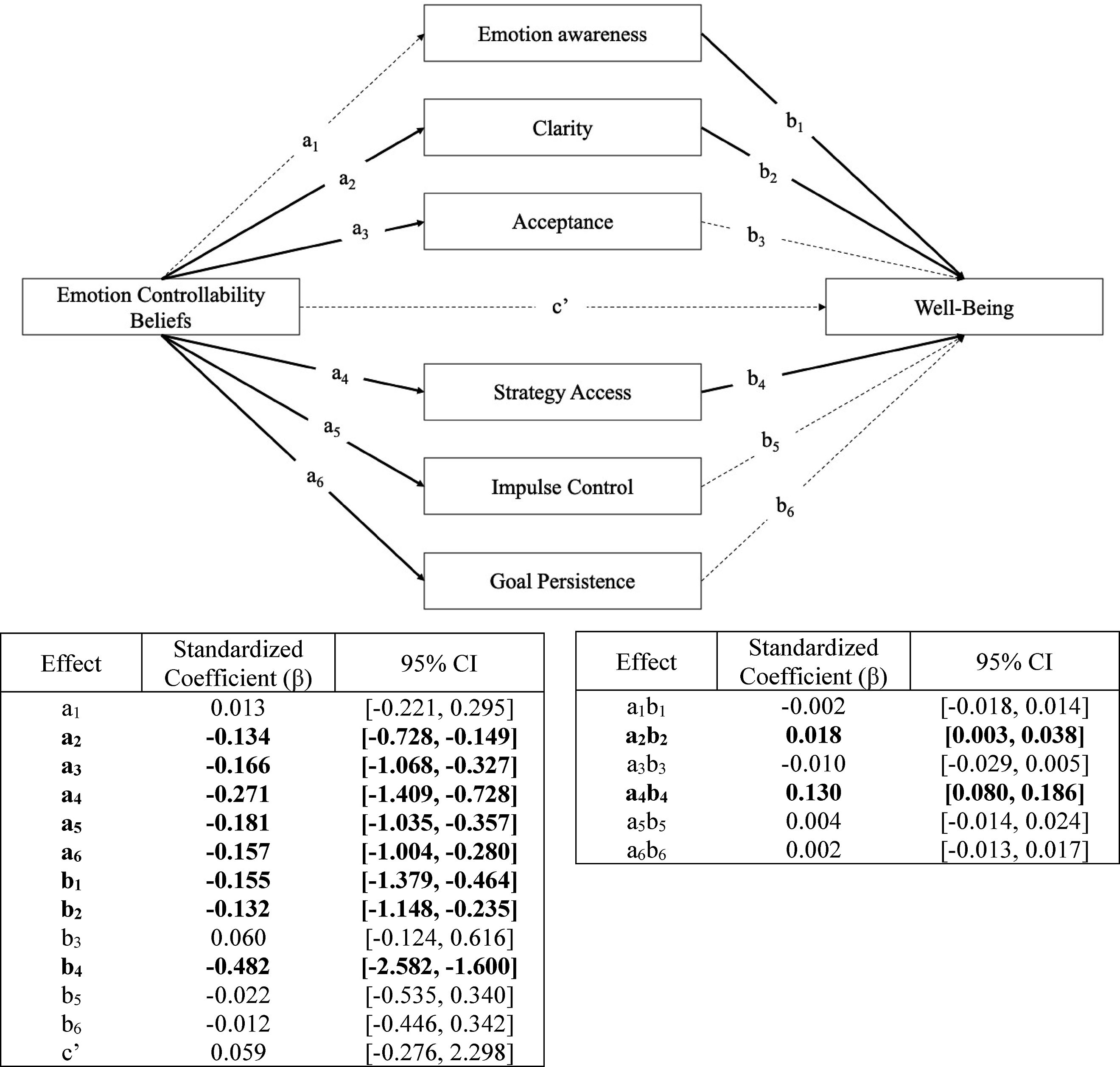
Discussion
Consistent with previous research (e.g., De Castella et al., 2013; Kraiss et al., 2020), higher emotion controllability beliefs were correlated with lower stress and higher well-being. Extending previous research, results indicated that emotion controllability beliefs were also correlated with multiple dimensions of emotion regulation. Specifically, the lower one’s emotion controllability beliefs, the more likely they were to have difficulty making sense out of their own feelings (low clarity) and to report guilt, embarrassment, and irritation with themself when experiencing negative emotion (non-acceptance). Additionally, low emotion controllability beliefs were correlated with greater difficulties modulating the intensity and duration of one’s own negative emotions (poor access to emotion regulation strategies), as well as greater difficulties controlling one’s behaviors (impulse control) and concentrating on important tasks (goal persistence) when experiencing distress. Taken together, findings support significant associations between emotion controllability beliefs and trait-level difficulty in important dimensions of emotion regulation.
Whereas previous studies have investigated specific cognitive emotion regulation strategies as mediators in the relationship between emotion controllability beliefs and mental health (e.g., cognitive reappraisal), the present study extends current literature by examining dimensions of emotion regulation difficulties as parallel mediators in the relationship between emotion controllability beliefs and stress and well-being. Results revealed significant indirect effects of emotion controllability beliefs on stress and well-being through difficulties with emotional clarity and strategy access. Furthermore, the direct effects of emotion controllability beliefs on stress and well-being were both non-significant; these results differ from those of previous studies which reported significant direct effects of emotion controllability beliefs on stress and well-being, even in the presence of indirect effects through emotion regulation (De Castella et al., 2013; King & dela Rosa, 2019). However, it should be noted that these studies only examined one emotion regulation strategy as a potential mediator (i.e., cognitive reappraisal), whereas in the present study, six dimensions of emotion regulation difficulties were explored as potential mediators. The discrepancy between our findings and those of previous studies thus highlights the utility of adopting a multidimensional conceptualization of emotion regulation when attempting to elucidate mechanisms that explain the relationship between emotion controllability beliefs and mental health outcomes. The inclusion of multiple dimensions of emotion regulation as potential mediators, rather than a single emotion regulation strategy such as cognitive reappraisal, appears to improve our ability to explain variability in stress and well-being. As a result, direct effects of emotion controllability beliefs on stress and well-being may no longer be observed.
Current findings implicate emotion processing as a novel pathway through which emotion controllability beliefs may be linked to mental health. Specifically, higher emotion controllability beliefs were associated with fewer difficulties understanding one’s own emotions (i.e., fewer difficulties in emotional clarity), which in turn, mediated the relationship between emotion controllability beliefs and stress and well-being. Although this is the first study to investigate the relationship between emotion controllability beliefs and emotion processing variables such as emotional clarity, we draw from research on anxiety in relation to implicit theories of emotion and emotion processing to explain the current findings. Specifically, a systematic review by Somerville et al. (2024) recently noted that higher emotion controllability beliefs are generally associated with fewer anxiety symptoms through greater use of adaptive emotion regulation strategies (e.g., cognitive reappraisal). Similarly, it is possible that the more an individual believes that emotions are amenable to control, the greater their propensity to actively make sense of their emotional experiences, thereby improving their mental health outcomes (such as their stress and well-being). Indeed, several studies have documented significant positive relations between difficulties with emotional clarity and anxiety-related outcomes (e.g., panic disorder, social anxiety; Oussi et al., 2023; Thompson et al., 2017), supporting the notion that emotional clarity is highly implicated in mental health outcomes.
The findings in this study also highlight the importance of general beliefs regarding one’s ability to access strategies perceived as effective in modulating the duration and intensity of one’s own negative emotional experiences as a primary mechanism through which emotion controllability beliefs may be associated with mental health. Specifically, higher emotion controllability beliefs were associated with fewer difficulties accessing strategies perceived as effective in regulating one’s own emotion, and in turn, were associated with lower stress and higher well-being. These results might also mean that lower emotion controllability beliefs are associated with poorer expectations regarding one’s own ability to access effective emotion regulation strategies which, in turn, is associated with higher stress and lower well-being. Drawing on previous research in the area of implicit theories within the academic domain, holding the view that intelligence is fixed and unchangeable may lead an individual to adopt a mindset of helplessness in the face of challenges (Costa & Faria, 2018; Dweck et al., 1995). In the context of emotions, an individual with an entity theory might feel a similar sense of helplessness in the face of emotional challenges, perhaps believing that there is nothing they can do to make themselves feel better because they perceive effective emotion regulation strategies to be inaccessible or ineffective. By contrast, the more a person believes emotions are controllable, the greater their sense of self-efficacy may be during challenging emotional situations in terms of their ability to employ effective strategies to reduce the discrepancy between their current and desired emotional states (Ford & Gross, 2019). It is suggested that future research more closely investigate the different profiles of emotion regulation strategy use that may be associated with emotion controllability beliefs. Indeed, investigating emotion regulation strategy use from a multivariate perspective (e.g., through cluster analysis) may help to further our understanding of whether higher emotion controllability beliefs are associated with an increased likelihood of engaging in adaptive (vs. maladaptive) emotion regulation strategies, or greater attempts to regulate emotions overall.
Interestingly, emotion controllability beliefs were found to be unrelated to emotional awareness in the present study. A possible interpretation of this finding is that an individual may similarly pay attention to and care about their emotional experiences, regardless of whether or not they believe they ultimately have control over them. For example, an individual who believes they have control over their emotions may notice and care about their feelings of stress or anxiety and set out to address (or “control”) them in some way, just as someone who does not believe they can control their emotions may also notice and care about their feelings of stress or anxiety, albeit from a different perspective of controllability. This is consistent with previous research on controllability beliefs in the area of academic achievement which, as noted earlier, has demonstrated that although individuals holding entity versus incremental views of intelligence are equally aware of academic challenges, they understand and approach these challenges in very different ways (Costa & Faria, 2018). Applying this logic to the current finding, an individual may be equally aware of their emotions independent of the extent to which they believe those emotions are controllable, thereby explaining the non-significant association between emotion controllability beliefs and emotional awareness in the present study.
In demonstrating consistent links between emotion controllability beliefs and emotion regulation correlates, these findings point to the prospect that lower emotion controllability beliefs are associated with an increased risk of emotion regulatory problems, and conversely, that fostering higher emotion controllability beliefs may aid in improving clinical treatments. While the cross-sectional nature of this study restricts inferences regarding the causal link between emotion controllability beliefs and emotional problems, such an idea is consistent with the tenets of existing cognitive therapies suggesting that maladaptive cognitions form the core of psychopathology and that restructuring these maladaptive cognitions is key to decreasing emotional distress (Hofmann et al., 2013). The potential causal link between emotion controllability beliefs and emotion regulation is further supported by experimental studies demonstrating that inducing different emotion controllability beliefs is associated with greater use of different emotion regulation strategies (e.g., Kneeland et al., 2016b). Moreover, studies in clinical samples of patients with social anxiety disorder have suggested that increasing emotion controllability beliefs may be an important mechanism through which therapy-related changes in psychological symptoms may occur (De Castella et al., 2013). As such, a potential avenue for future research is to investigate how emotion controllability beliefs might be enhanced in clinical settings, and to further examine the role of emotion controllability beliefs as potential mediators of treatment-related changes in mental health.
Limitations
While the present study indicates that emotion regulation is an important mechanism through which emotion controllability beliefs may be associated with mental health, there are several methodological limitations. To begin, our sample consisted of predominantly White university students who identified as women, and so individuals of varying gender identities, ethnicities, ages, and sociodemographic backgrounds are not well represented. As such, the present findings are not generalizable to more diverse adult samples and future studies using more diverse samples are necessary to solidify the present findings. This is particularly important in light of previous research findings that have demonstrated that age, gender identity, and socioeconomic status each play a role in the types of emotion regulation difficulties that individuals tend to report (e.g., Mankus et al., 2016). Another key limitation relates to the correlational nature of our study. Throughout, we have presented a model in which emotion controllability beliefs temporally precede dimensions of emotion regulation difficulties and mental health. Although this approach is consistent with previous studies on emotion controllability beliefs (e.g., King & dela Rosa, 2019) as well as prominent cognitive theories of mental health (Hofmann et al., 2013), current findings cannot rule out the possibility that difficulties in emotion regulation or mental health issues precede emotion controllability beliefs. For example, it is possible that the repeated experience of stress and emotion regulation difficulties orient individuals to view their emotions as generally immutable to control. Moreover, the cross-sectional nature of this study cannot eliminate the possibility of reciprocal interaction. For example, it may be that lower emotion controllability beliefs lead to greater emotion regulation difficulties and increased distress, which in turn, strengthen the view that emotions are fundamentally immutable. Carefully implemented experimental and longitudinal studies are needed to confirm the chronological precedence of emotion controllability beliefs in the prediction of emotion regulation and mental health.
Conclusion
To conclude, the present study offers new insight regarding the specific emotion regulatory mechanisms through which emotion controllability beliefs may be associated with mental health. In line with broader implicit theory models of self-regulation, emotion controllability beliefs appear to be linked to distinct affective, cognitive, and behavioural responses to emotional challenges. Although individuals with high versus low emotion controllability beliefs may be equally aware of their emotions, individuals with lower emotion controllability beliefs are more likely to report difficulties understanding, accepting, and regulating their emotions. These difficulties are characterized by lower emotional clarity and acceptance, poorer access to effective emotion regulation strategies, and greater problems controlling maladaptive impulses and engaging in goal-directed behaviours when experiencing negative emotion. In turn, emotional clarity and perceived access to effective emotion regulation strategies may be two unique mechanisms through which emotion controllability beliefs are associated with emotional functioning. Findings suggest that implicit theories of emotion may help to clarify broad patterns of adaptive versus maladaptive emotional responding, as well as shed light on the cognitive processes underlying individual differences in emotion regulation and subsequently, mental health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on reasonable request.