
Abstract
Despite infectious pandemics proving particularly detrimental to those with Obsessive-Compulsive Disorder (OCD), the investigation of analogous experimental paradigms is lacking. To address this gap, we conducted two studies employing vignettes that depicted contamination-related situations commonly experienced during a pandemic (e.g., Coughing into hands and failing to use hand sanitizer). We manipulated the salience of these vignettes across three levels: high contamination, low contamination, and a neutral control condition. Our examination of state anxiety and disgust responses in all participants revealed the successful manipulation of the vignettes’ impact. Specifically, individuals with more severe OCD symptoms reported significantly higher levels of state disgust and anxiety for both high and low contamination vignettes, in contrast to the group with lower symptom severity. No significant differences were observed in the neutral vignette condition between the high- and low-scoring groups. Interestingly, for those with higher OCD symptoms, high salience contamination-focused vignettes resulted in similarly elevated state disgust and anxiety, regardless of whether the vignettes were situated in public (Study 1) or domestic (Study 2) settings. This suggests that the heightened sensitivity to contamination-related scenarios observed in individuals with OCD symptoms in the present study is not confined to a specific context. These findings support the use of contamination-focused vignettes as analogues for studying infectious pandemics and provide valuable insights into OCD models, interventions, and future research.
Introduction
Obsessive-compulsive disorder (OCD) is characterized by recurring, distressing obsessions, such as unwanted thoughts, images, or urges, and compulsions, which involve repetitive actions or mental acts aimed at alleviating associated anxiety (APA, 2013). There are multiple OCD types categorized as up-to-date subgroups of OCD that are also used as diagnostic criteria for DSM-5 in field studies. These groups can be summarized as checking, contamination, hoarding, indecisiveness, and just right (Duradoni et al., 2023; Guazzini et al., 2022; Thordarson et al., 2004). Although the types of OCD resemble each other, all of them have distinctive features that separate one from the others. One of the most prevalent OC (Obsessive Compulsive) symptom pairings involves obsessions centred on contamination and subsequent cleaning compulsions to negate the anxiety (Jalal et al., 2023; Markarian et al., 2010; Rachman, 2004; Stein et al., 2019). Hence, individuals predisposed to OCD exhibit heightened susceptibility to symptom exacerbation during infectious pandemics, surpassing the impact on other disorders (Davide et al., 2020; Fineberg et al., 2020; Fisman & Walsh, 1994; Linde et al., 2022; Nissen et al., 2020; Wagner & Sullivan, 1991).
For example, during the 2009 Swine Flu pandemic, Brand et al. (2013) found that the strength of OCD beliefs and symptoms predicted subsequent fear experiences, with similar patterns observed during the HIV/AIDS crisis in the 1980s and 1990s (Bruce & Stevens, 1992). Regarding the COVID pandemic, a ten- and fourteen-fold surge OC symptoms was observed, both in the general population (Abba-Aji et al., 2020; see also Khosravani et al., 2021) and those diagnosed with OCD (Benatti et al., 2020; Grant et al., 2022). Furthermore, during the COVID pandemic, Alonso et al. (2021) reported that new-onset obsessions occurred in 57.8% of the general population, along with new-onset compulsions in 45.9%, notably featuring heightened obsessions regarding dirt, germs, and viruses. Additionally, 72.4% of the participants reported experiencing moderate to high levels of anxiety (see also Taher et al., 2021). Hassoulas et al. (2021) also noted that those with contamination-related OCD experienced a specific worsening of symptoms compared to other dimensions of OCD during the COVID-19 pandemic.
Banerjee (2020) attributed this increase in OC symptoms during the COVID-19 pandemic to several factors, including the repeated demand for handwashing, fear of unseen viral contamination, social distancing measures, and the proliferation of health-related messages through mainstream and social media (e.g., Stay at Home, Wash Your Hands). These factors collectively contribute to the normalization of OCD symptoms and behaviours during the pandemic and beyond, highlighting an interrelationship between the COVID-19 pandemic, OCD symptoms, anxiety, and specific contamination-related thoughts, in the form of disgust.
Within this context, we identify two factors as notable contributors to the initiation and deterioration of OC symptoms: heightened sensitivity to experiencing disgust and a tendency to undergo temporary shifts in anxiety levels when exposed to contamination (Jalal et al., 2023; Kim et al., 2008; Knowles et al., 2016; Moretz & McKay, 2008; Seçer & Ulaş, 2020; Thorpe et al., 2003; Tolin et al., 2006; Woody & Tolin, 2002). In the present study, our aim to explore the transient shifts in state disgust and anxiety among individuals with high OC scores when exposed to vignettes featuring high-contamination content and contrasting them with individuals scoring lower on OC tendencies. We now elaborate on the interplay between contamination, state disgust and anxiety, their relationship with OC symptoms, and our utilization of vignettes to assess these connections.
Disgust, Contamination and OCD
Disgust is a core concept related to fear of contamination and OCD. Specifically, in regions with an elevated risk and exposure to infectious diseases, individuals typically demonstrate increased sensitivity to disgust, and a heightened perception of potential contamination compared to those in lower-risk areas (Skolnick & Dzokoto, 2013). This suggests that personal disgust is a responsive concept, aligning with alterations in an individual’s immediate environment’s perceived or actual contamination levels (see also Badour et al., 2014). It is therefore no surprise that elevated sensitivity to disgust in relation to contamination are commonly observed in OCD (Athey et al., 2015; Badour et al., 2014; Knowles et al., 2018; Moretz & McKay, 2008; Olatunji et al., 2011; Tolin et al., 2006). Specifically, heightened disgust has been identified as a distinct predictor of fear of contamination (Abramowitz et al., 2003; Moretz & McKay, 2008), with vulnerabilities linked to disgust identified as contributing to the development of OC symptoms at a sub-clinical (Tolin et al., 2006) and clinical level (Knowles et al., 2018).
In the context of OCD, individuals characterized by heightened sensitivity to disgust often perceive aversive situations or stimuli as potentially harmful. This suggests that contamination-based OCD may involve a malfunction in the evaluation process (Abramowitz et al., 2009). The significance of this evaluation process becomes especially apparent during viral pandemics, where uncertainty regarding contamination emerges due to the invisibility of viruses and the uncertainty surrounding the effectiveness of handwashing (Aardema, 2020). This heightened awareness of ambiguity, coupled with an inability to resolve it, encourages, and exaggerates OC symptoms (Harkin & Mayes, 2008). Indeed, a body of research has indicated that sensitivity to disgust contributes to the general fear of contamination (Olatunji et al., 2004), fear of contamination in the presence of disgusting stimuli (Bhikram et al., 2017), fear of contamination in OCD (Rasmussen & Tsuang, 1986; Summerfeldt et al., 1997) and a range of OC symptoms (Muris et al., 2000, 2008; Thorpe et al., 2003).
Anxiety, Contamination and OCD
Anxiety is a core aspect of OCD, driving obsessive behaviours and comorbidity (Abramowitz et al., 2003; Salkovskis, 1999; Salkovskis et al., 2003), with heightened anxiety levels in high-contamination situations leading to washing and checking symptoms (Clauss & Bardeen, 2022; Cougle et al., 2007; Kim et al., 2008). Thus, like disgust, anxiety responds to changes in actual or perceived contamination in an individual’s environment, a response particularly acute in those with OCD. For example, in an ecologically relevant study, Laforest, Bouchard, Crétu and Mesly (2016) examined the potential for a virtual environment (immersion in a disgusting public restroom) to elicit situational anxiety in OCD individuals with a dominant fear of contamination. The result demonstrated that exposure to a “contaminated” virtual environment resulted in more acute anxiety in those with OCD versus the control group, evidenced objectively by biophysiological increases in heart rate and subjective measures of state anxiety (STAI; Spielberger et al., 1983). In addition, a body of literature has identified the relationship between the COVID pandemic, anxiety, and OC symptoms both in the general population and those with OCD (see, Linde et al., 2022).
The transitory and responsive nature of state anxiety in relation to environmental stressors was noted in the classic work of Spielberger (1966). Wherein, state anxiety occurs across the two main dimensions of cognitive worry and autonomic-emotional arousal, which are in turn triggered by various threats, including social evaluation, physical danger, ambiguous threat, and threat to daily routines (Endler et al., 1991). During pandemics, particularly when there is a threat of viral contamination, we suggest that all these components are potential targets, especially in individuals with a predisposition to heightened obsessive-compulsive tendencies. As Banerjee (2020) has noted, the increased occurrence of OCD symptoms during the COVID-19 pandemic can be attributed to factors such as frequent handwashing, fear of unseen viral contamination, social distancing measures, and the widespread dissemination of health-related messages through mainstream and social media (e.g., Stay at Home, Wash Your Hands). These factors collectively contribute to the normalization of OCD symptoms and behaviours during the pandemic and reveal an interconnected relationship between the COVID-19 pandemic, specific contamination-related thoughts, changes in disgust and anxiety and symptoms of OCD.
Aims and Hypotheses
Despite evidence indicating the detrimental impact of infectious pandemics on individuals with OCD, the investigation of analogous experimental paradigms remains lacking. In this study, we aim to address this gap by employing specially designed contamination-related vignettes to tap into contamination-related OCD symptoms. By pursuing this approach, we seek to justify the use of contamination-related vignettes as an effective analogue for studying the impact of infectious pandemics on individuals with relevant symptoms.
With these aims in mind, we presented participants scenarios in the form of vignettes that encompassed three distinct levels of COVID-related contamination (high contamination, low contamination, and neutral vignettes). Following their presentation, we then recorded participants’ state disgust and anxiety responses immediately after the presentation of each vignette. In accord, our experimental hypotheses were:
High scoring OCD participants will experience greater state disgust after reading high and low contamination vignettes, but not neutral vignettes, in comparison to low scoring OCD participants. We expect that disgust will be triggered by low contamination vignettes due to the sensitivity of this construct for those scoring higher for OCD but to a lesser degree than high contamination vignettes.
High scoring OCD participants will experience greater state anxiety after reading high and low contamination vignettes, but not neutral vignettes, in comparison to low scoring OCD participants. We expect that anxiety will be triggered by low contamination vignettes due to the sensitivity of this construct for those scoring higher for OCD but to a lesser degree than high contamination vignettes.
Additionally, we will explore the impact of environmental context by presenting the vignettes in two different settings in two studies: public space for Study 1 and domestic space for Study 2. The rationale for this manipulation was that those with OCD often experience their symptoms within the home environment (Rachman, 2002) and “stay at home” directives associated with the COVID-19 lockdown are associated with an intensification of state disgust and anxiety (Hamada & Fan, 2020; Moreira-de-Oliveira et al., 2022). The specific hypothesis for this was:
High scoring OCD participants will experience greater state disgust and anxiety after reading vignettes presented in the domestic versus public space in comparison to low scoring OCD participants.
Study 1
Method
Participants
Forty participants (15 male, 25 female) with a mean age of 21.5 (SD 4.7) were recruited from the university student participation pool and various social media outlets, such as Facebook and Instagram. The ethnic breakdown was 35 white Caucasians (87.5%), 3 Asian (7.5%) and 2 Black or African (5%). The inclusion and exclusion criteria involved individuals over eighteen years of age and not presently enrolled in therapy or treatment for an anxiety disorder or clinical OCD. Fluency in written, spoken, and reading English was also an inclusion criterion for all participants, as it was essential for comprehending the vignettes.
Materials
Vignettes in Research
Vignettes are multidimensional stimuli consisting carefully constructed hypothetical real-world situations that elicit cognitions, perceptions, emotions, and fine-grained feelings (Barter & Renold, 2000; Hughes, 1998). Thus, the subtle details of the design and allocation of the vignette paradigm are necessary to represent a systematic combination of characteristics (Atzmüller & Steiner, 2010). The vignette paradigm has the potential to explore complex psychological and social phenomena in circumstances and situations that are difficult to capture (Gourlay et al., 2014).
Numerous studies have demonstrated the effectiveness of the vignette paradigm in various domains. For example, Lewis et al. (1990) presented psychiatrists with case histories varying in their race and gender to see how this impacted assessment or management of the patient. Sauer (2011) used video-presented vignettes to explore the impact of leadership status and style on leader effectiveness, providing direct evidence that low-to-medium fidelity stimuli can be sufficient to generalize to more realistic contexts. Hine (2019) explored judgements of domestic violence by varying the gender dyadic of the perpetrator versus victim, and type of abuse, physical versus psychological, and Maieron et al. (1996) explored children’s perceptions and acceptance of a hypothetical peer with acquired immune deficiency syndrome. This inherent flexibility of the vignette enables the investigation of sensitive topics, mirroring social reality, and serves vulnerable people or hard-to-research situations (Gourlay et al., 2014). Given the unique advantages of vignettes, it is crucial to tailor each vignette paradigm to the specific contextual properties of the phenomenon under examination. This ensures that participant responses mirror social reality, (Gourlay et al., 2014) and that the narrative fidelity of the vignettes is validated (Finch, 1987; Lanza & Carifio, 1992).
Development of Contamination Vignettes
The importance of vignette development and the concept of validation and methodological rigor is widely promoted in clinical and healthcare literature (McCrow et al., 2013; Paddam et al., 2010; Randhawa et al., 2015). The vignettes employed in this study were developed to reflect real life situations and scenarios, so that they were plausible (Hughes & Huby, 2002); clear, relevant, and real to the phenomenon of contamination during a pandemic (LaFond et al., 2015); and were brief consisting of appropriate language (i.e., in clear English prose) appropriate for the sample tested (Paddam et al., 2010).
Validation and content validity was obtained using a three-phase approach (see Paddam et al., 2010; Randhawa et al., 2015) to the development of vignettes and establish a stronger paradigm for data collection.
Phase one consisted of the initial development of the vignettes by a research team member, which involved brainstorming and drafting a series of potential contamination scenarios based on real-world situations commonly encountered during a pandemic. These scenarios were crafted with the aim of being plausible, clear, and relevant to the research focus on contamination experiences. The research team member drew upon existing literature (e.g., Athey et al., 2015; Badour et al., 2014; Clauss & Bardeen, 2022; Cougle et al., 2007; Kim et al., 2008; Knowles et al., 2018; Olatunji et al., 2011) and expert knowledge within our research team (e.g., Harkin et al., 2011; Harkin et al., 2023; Harkin & Kessler, 2011a, 2012a; Harkin & Mayes, 2008; Persson et al., 2021; Yates et al., 2010) to ensure that these initial scenarios captured key aspects of contamination, aiming to create vignettes that would effectively elicit participants’ emotional responses and engagement. In Phase Two, two members (AY, LD) from our research team assessed each vignette based on four content validity dimensions: clarity, language suitability, real-life applicability, and plausibility. In Phase Three, our expert on OCD (BH) made recommendations for enhancing and modifying each vignette, ultimately, a consensus was reached, with 100% agreement on the proposed modifications (AY, BH, LD).
As a result of this process, and to further ensure the validity and reliability of our vignettes, we incorporated two additional methodological considerations into their design.
First, to ensure that participants engaged deeply with the text, we employed multi-dimensional scenarios (Stolte, 1994) with prose written in first-person prose to subtly influence the reader to interpret each contamination scenario in their own mental space and simulating a real-life scenario that our participants have or could find themselves within (Stolte, 1994). This is why in our vignettes; we chose everyday scenarios, i.e., buying groceries in the supermarket (Study 1: public space); interacting with a builder at home (Study 2: domestic space). Regarding our vignettes being relevant to OCD, our approach is consistent with the observations of Aardema (2020), who noted that fear of contamination is more likely when stimuli are of high personal significance and meaning to an individual, a phenomenon more likely in those with a propensity to OCD. Therefore, each vignette depicted a 51-word contamination scenario which positions the reader at the centre of each vignette in first-person prose. Participants we required to read each vignette twice, in their own time, to fully immerse themselves in its content (Aguinis & Bradley, 2014; Ryan et al., 2010) and then responded to state disgust and anxiety dimensions relative to their experience of the scenario in each vignette.
Our second methodological consideration was the need to construct vignettes with differing levels of contamination to tap into specific vulnerabilities of those with OCD. To achieve this, we developed three English-written vignettes, each varying in the extent of contamination: (a) High Contamination Vignette, (b) Low Contamination Vignette, and (c) Neutral Control Vignette. In study 1, these vignettes located the actor in a public space. The three vignettes were as follows:
Measures
To investigate the role of disgust in anxiety disorders and OCD with precision (Knowles et al., 2018), participants rated their immediate emotional experiences of disgust and anxiety following the contamination vignette, along with their overall OC symptomatology using the following scales.
Procedure
Via the Qualtrics online platform (Qualtrics, 2020), we asked participants to read an information sheet, provide informed consent, and informed them that they would be answering questions about their thoughts, feelings, and perceptions on a series of vignettes depicting varying levels of contamination. The presentation order of the vignettes was counterbalanced across the participants, i.e., half completed Vignettes A (high contamination), C (neutral contamination), B (low contamination), and the other half B, C, and A. After reading each vignette, participants completed the DPSS-R, STAI, and the VOCI.
An a priori power analysis was conducted using G*Power version 3.1.9.7 (Faul et al., 2007) to determine the minimum sample size required to test the study hypothesis. Results indicated the required sample size to achieve 80% power for detecting a medium effect .46 (Cohen, 2013), at a significance criterion of α = .05, 2 groups and 6 measurements was N = 40 for a 2 (OCD Group: low vs. high OCD group) × 3 (Vignette Contamination Level: high, low, neutral) × 2 (Emotional Response: disgust, anxiety) repeated measures mixed method design ANOVA. Thus, the obtained sample size of N = 40 is adequate to test the study hypothesis and maintain a type 1 error at an Alpha setting of .05.
Results
Design
A 2 (OCD Group: low vs. high OCD group) × 3 (Vignette Contamination Level: high, low, neutral) × 2 (Emotional Response: disgust, anxiety) repeated measures mixed method design ANOVA was employed with OCD Group as the between- and Vignette Contamination Level and Emotional Response as the within-subject factors. Anxiety and disgust were the dependent measures. In our preliminary analysis of the underlying assumptions of parametric tests, we used a median split of total scores on the VOCI self-report questionnaire to binarize our sample into low-OCD and high-OCD group to support our factorial design. This approach resulted in two groups: low (M = 75.2, SD = 8.9) and high (M = 103, SD = 12) OCD group.
The use of median split is reported to be a legitimate and valuable analytical technique so long as the distribution of scores in the independent variable meet assumptions of normality (Iacobucci et al., 2015; Pscherer et al., 2019). Researchers have used the median split as an empirically based cut off point for high versus low groups in clinical decision-making contexts (Kraemer et al., 2004), OCD (Harkin et al., 2011; Morein-Zamir et al., 2020), trait paranoia and brain activity (Finn et al., 2018) and smartphone addiction (Fabio et al., 2022). The use of the median split in the present study was deemed appropriate because OCD was considered a potential modulator of emotional response (anxiety or disgust) when the participants were exposed to various degrees of contamination salience. Adequate control of a Type I error was assured by means of a preliminary Shapiro-Wilk test that was normally distributed (p > .05). Median splits do tend to give the best results when the variable of origin has a symmetric distribution (see Cohen, 1983). Following a significant main effect or interaction (p < .05), subsequent planned comparisons were examined by means of paired t-tests adjusted at Bonferroni alpha level p .05 where appropriate.
Analyses
A repeated measures mixed method design ANOVA was carried out to examine state anxiety and disgust. As violations of the sphericity assumption (Mauchley’s tests) were observed for the main effect of vignette contamination level, the reported F-value was corrected with Greenhouse-Geisser degrees of freedom (p < .05).
The results of the repeated measures mixed method ANOVA showed that there was a significant main effect of vignette contamination level (F (2, 1.37) = 316.49, p = < .001, ηp2 = .89) on emotional responses (disgust and anxiety) with participants scoring higher for the high contamination vignette (M = 33.01, SD = 6.6) and low contamination vignette (M = 26.53, SD = 4.80) compared to neutral (M = 20.17, SD = 2.59). These results confirm that the content of our contamination vignettes (high and low) successfully increased emotional responses in our participants at a general level.
To determine if our manipulation successfully differentiated high from low OCD participants for state disgust and anxiety, we examined the main effects for OCD group. A significant main effect of OCD group was observed (F (1, 38) = 26.51, p = <.001, ηp2 = .41), indicating that high-OC individuals reported higher levels of disgust (M = 11.68 SD = 2.71) (M = 9.18, SD = 1.33) and anxiety (M = 45.70, SD = 5.48) compared to the low-OC group (disgust: M = 9.18, SD = 1.33; anxiety: M = 39.17, SD = 3.71). There was a significant interaction between OCD group and vignette contamination level (F (2, 76) = 22.61, p = .001, ηp2 = .37), suggesting that the contamination depicted in the vignettes had a different effect on the high OCD group compared to the low OCD group. There was also a significant interaction between OCD group and emotional response (F (1, 38) = 15.54, p = .001, ηp2 = .29), suggesting subclinical OCD (high vs. low) effected on the level of emotional response reported by the participants.
From this, we concluded that our contamination vignettes evoked emotional responses in our participants and differentiated high from low OCD participants. We use this to justify subsequent specific analyses between the OCD groups.
Between Group Comparisons
The 2 × 3 × 2 ANOVA revealed a significant three-way interaction between OCD Group × Vignette Contamination Level x Emotional Response measure (F (2, 76) = 17.33, p = .001, ηp2 = .35). This justifies subsequent planned independent comparisons for anxiety and disgust between the high and low OCD groups for each vignette contamination level. Significance values for Levene’s Test indicate that assumptions of equal variances were not assumed for all the independent sample tests on disgust (p < .05), thus the degrees of freedom were corrected on the appropriate t-tests when appropriate.
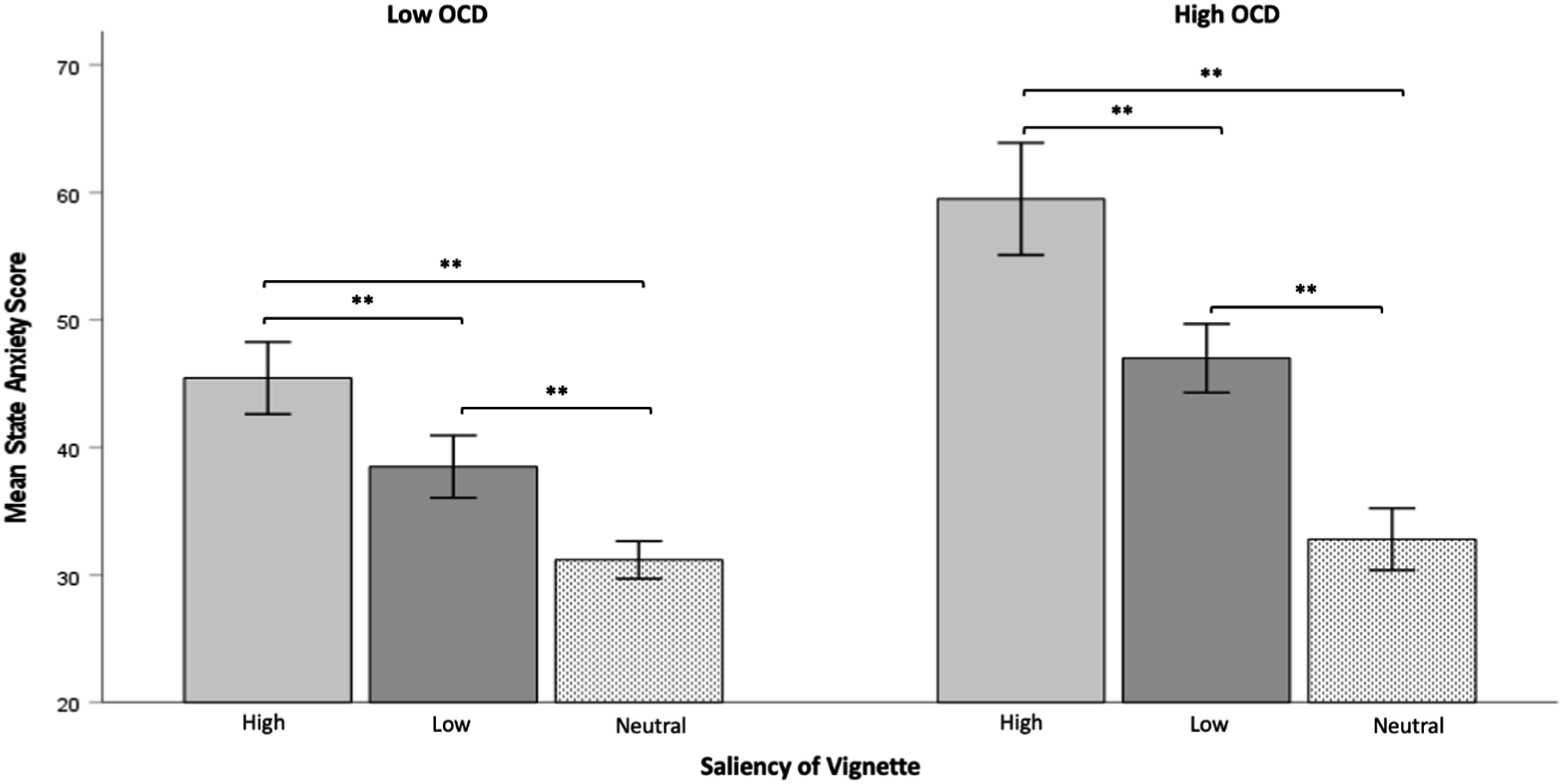
For disgust, the high-OC group exhibited significantly higher levels for both the high contamination vignette (M = 15.85 vs. 11.65, t (23.96) = 3.80, p = .008, g = 1.2) and the low contamination vignette (M = 11.00 vs. 8.70, t (38) = 4.62, p = .001, d = 1.4) compared to the low OCD group (see Figure 1). For anxiety, the high-OC group displayed notably greater anxiety responses for both the high contamination vignette (M = 58.40 vs. 46.20, t (27.53) = 5.62, p = .001, d = 1.7) and the low contamination vignettes (M = 46.95 vs. 39.50, t (38) = 4.80, p = .001, d = 1.5) compared to the low OCD group (see Figure 2). It is important to note that the comparisons between the high and low-OC groups for the neutral contamination vignette did not yield significant differences (p > .05). Means with standard errors for disgust responses for high, low, and neutral contamination vignettes between the low and high OCD groups in a public space. Note. Means with standard errors for state anxiety responses for high, low, and neutral contamination vignettes between the low and high OCD groups in a public space Note. 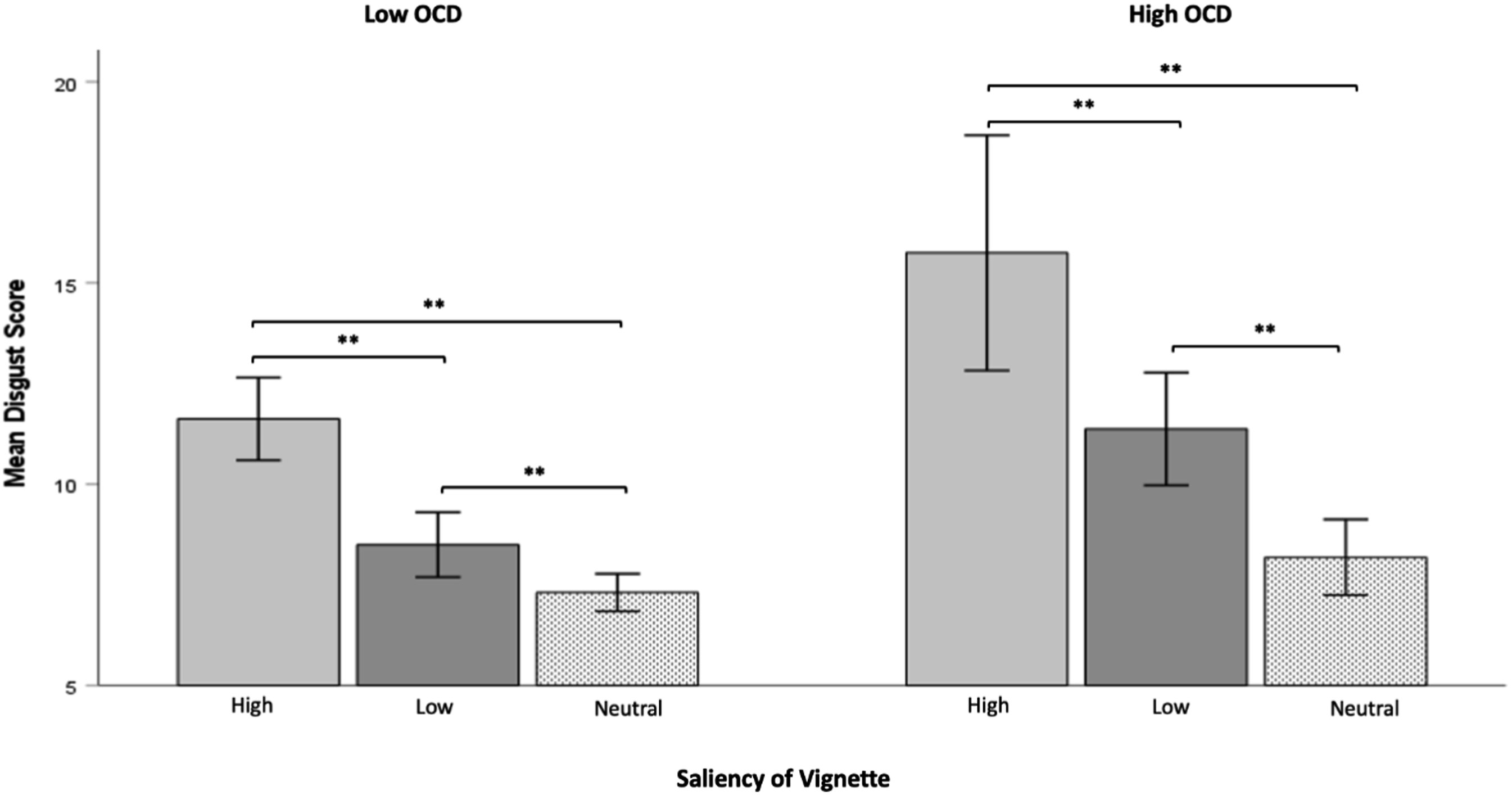
Discussion of Study 1
We found evidence in our disgust and anxiety data that our contamination vignettes successfully induced emotional responses in our participants and differentiated high from low OCD participants. Regarding this latter point, we observed that high-scoring OCD participants experienced greater state disgust and anxiety after reading vignettes with specific contamination-related content versus low-scoring participants. In accord with the specificity of the response of the high OCD group to vignettes that included contamination (i.e., high and low), was that we did not observe group differences (low vs. high OCD group) in the neutral vignettes.
Study Two
Study two served a three-fold purpose. Firstly, it aimed to replicate the effects of our vignette manipulation on the emotional responses of individuals with OCD. Secondly, it sought to assess the extent of the impact of contamination-focused vignettes in a public setting (Study 1) compared to a domestic setting (Study 2). Lastly, it allowed us to examine the effects of vignette location on state disgust and anxiety, specifically the differences between public space (Study 1) and domestic space (Study 2), on individuals with OCD.
Method
Participants
Fifty-two participants (20 male, 32 female) with a mean age of 33 (SD 5) were recruited from the university student participation pool and various social media outlets, such as Facebook and Instagram. The ethnic breakdown was 29 white Caucasians (91%), 1 Asian (3%) and 2 Black or African (6%). Inclusion and exclusion criteria were the same as in Study 1. As in Study 1, we used the median split of total VOCI scores to obtain two groups: low (M = 70, SD = 10.3) and high (M = 114, SD = 20.4) OCD group.
The same a prior power analysis was conducted for Study 2 as was fully reported previously for Study 1. The analysis again justified the sample size of N = 40 is adequate to test the study hypothesis and maintain a type 1 error at an Alpha setting of .05.
Materials and Procedure
The design and structure for Study 2 were the same as Study 1, with the exception that the vignettes presented to the participants depicted a potential contamination scenario in the actor’s domestic space. As in Study 1, we attempted to modulate the experience of contamination across three levels of vignette:
The questionnaires employed and their timing was identical to Study 1; State Trait Anxiety Inventory (STAI; Spielberger et al., 1983); Modified state version of the Disgust Propensity Scale (DPS; Van Overveld et al., 2006); and Vancouver Obsessional Compulsive Inventory (VOCI; Thordarson et al., 2004).
Results
Design
A 2 (OCD Group: low vs. high OCD group) × 3 (Vignette Contamination Level: high, low, neutral) × 2 (Emotional Response: disgust, anxiety) mixed design was employed with OCD Group as the between- and Vignette Contamination Level and Emotional Response as the within-subject factors. Anxiety and disgust were the dependent measures.
Analyses
ANOVAs for the 2 × 3 × 2 design were carried out for disgust and anxiety. As violations of the sphericity assumption (Mauchley’s tests) were observed for the main effect of vignette contamination level and the interaction between vignette contamination level and emotion, the reported F-values were corrected with Greenhouse-Geisser degrees of freedom (p < .05).
The results of the repeated measures mixed method ANOVA showed that there was a significant main effect of vignette contamination level (F (1.24, 61.74) = 140.37, p = .001, ηp2 = .74) on emotion responses (disgust and anxiety) with participants scoring higher for the high (M = 25.81, SD = 6.12) and low contamination vignette (M = 20.21, SD = 4.36) compared to the neutral (M = 16.61, SD = 2.86). As in Study 1, this again confirms that the content of our contamination vignettes (high and low) successfully increased emotional responses (disgust and anxiety) in our participants at a general level.
To determine if our manipulation successfully differentiated high from low OCD participants for disgust and anxiety, we examined the main effects for OCD group. There was a significant main effect of OCD group (F (1, 50) = 28.01, p = .001, ηp2 = .36), with the high OCD group (M = 22.93 SD = 3.94) reporting higher levels of emotion than low OCD group (M = 18.82, SD = 3.60). There was a significant interaction between OCD group and vignette contamination level (F (2, 100) = 15.02, p = .001, ηp2 = .23), suggesting that the contamination depicted in the vignettes had a different effect on the high compared to the low OCD group. There was also a significant interaction between emotion and OCD group (F (1, 50) = 12.76, p = .001, ηp2 = .20), suggesting subclinical OCD (high vs. low) effected on the level of emotional response reported by the participants.
From this, we conclude that our contamination vignettes evoked emotional responses in our participants and differentiated high from low OCD participants specifically. This justifies subsequent specific analyses comparing the high and low OCD group.
Between Group Comparisons
The 2 × 3 × 2 ANOVA revealed a significant three-way interaction (F (2, 100) = 9.24, p = .01, ηp2 = .16) between OCD Group x Vignette Contamination Level x Emotional Responses (disgust and anxiety). We use this to justify subsequent planned independent comparisons for disgust and anxiety between the high and low OCD groups for each of the three vignettes. Significance values for Levene’s Test indicate that assumptions of equal variances were not assumed for all the independent sample tests on disgust (p < .05), thus the degrees of freedom were corrected on the appropriate t-tests when appropriate.
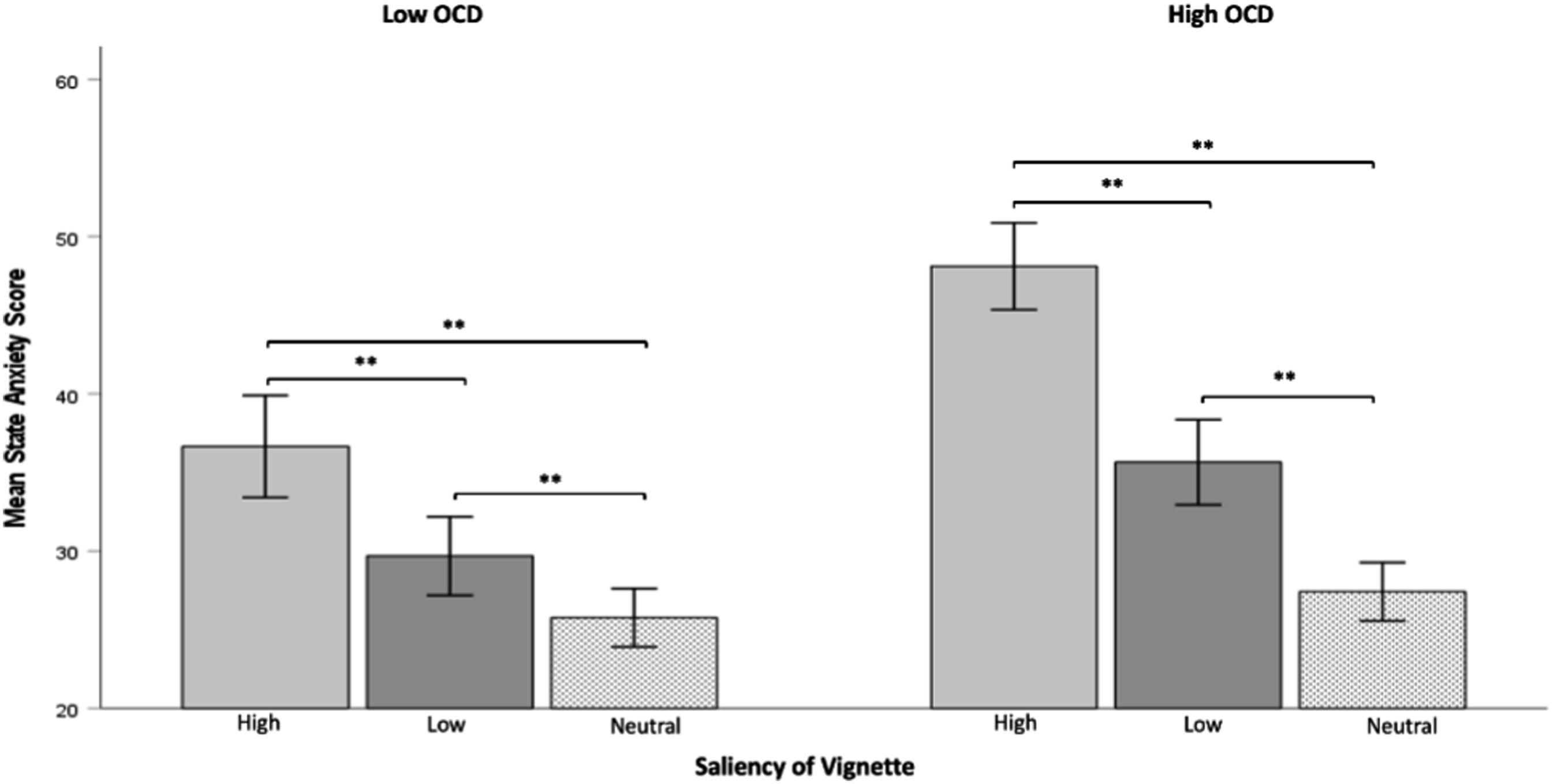
For disgust, the high OCD group showed greater disgust for the high (M = 10.73 vs. 7.50, t (35.66) = 4.46, p = .001, g = 1.2) and low contamination vignette (M = 8.69 vs. 6.88, t (36.92) = 4.80, p = .001, g = 1.3) compared to the low OCD group (see Figure 3). For anxiety, the high OCD group also had greater anxiety for the high (M = 48.12 vs. 36.88, t (50) = 5.56, p = .001, d = 1.4) and low contamination vignette (M = 35.65 vs. 29.62, t (50) = 3.37, p = .001, d = .93) compared to the low OCD group (see Figure 4). Importantly, comparisons between the high and low OCD groups on the neutral contamination condition revealed that disgust and anxiety did not reach significance (both t-tests, p > .05). Means with standard errors for disgust responses for high, low, and neutral contamination vignettes between the low and high OCD groups in a domestic space. Note. Means with standard errors for state anxiety responses for high, low, and neutral contamination vignettes between the low and high OCD groups in a domestic space. Note. 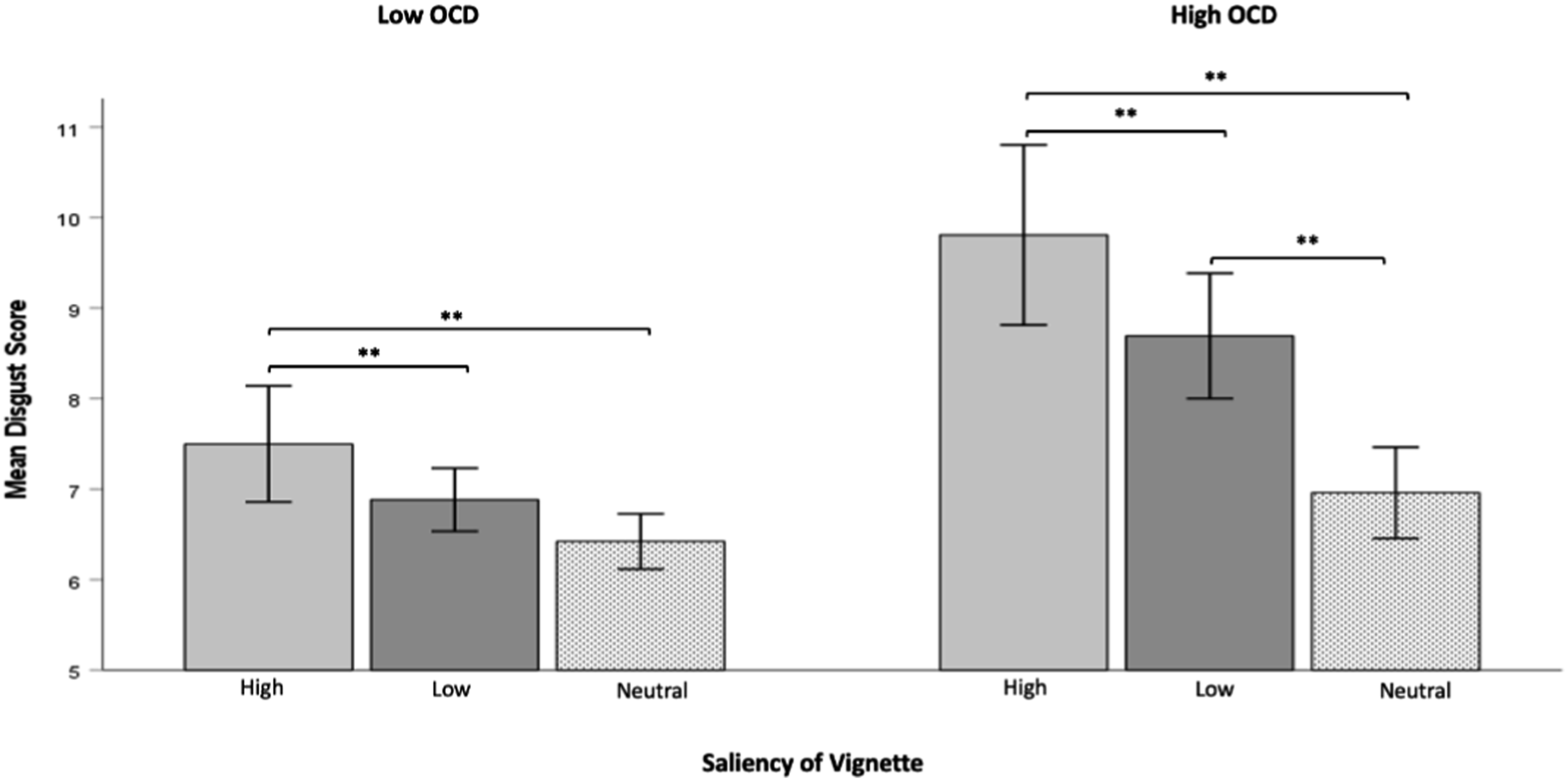
Discussion of Study 2
Disgust and anxiety responses to the vignettes in Study 2 replicate the main findings of Study 1. These data indicate that high-scoring OCD participants experience greater disgust and anxiety when confronted with contaminated-related vignettes.
Public Space versus Domestic Space Comparisons
To assess the impact of different environmental spaces on high- and low-scoring OCD participants, we compared disgust and anxiety responses across Studies 1 (public space) and 2 (domestic space). Therefore, we conducted a 2 (OCD Group: low vs. high OCD) × 2 (Environmental Space: public vs. domestic) ANOVA, with disgust scores for the high salience vignettes as the dependent variable. We focussed on the high-salience vignettes as these evoked the most acute responses in high-scoring OCD participants. The result showed that there was a significant main effect of OCD group (F (1, 88) = 34.05, p = .001, ηp2 = .28), with the high OCD group showing higher disgust scores (M = 12.96, SD = 4.7) compared to the low OCD group (M = 9.3, SD = 2.6) for the high salience vignette. There was also significant main effect of Environment (F (1, 88) = 52.97, p = .001, ηp2 = .38), with public space showing higher disgust scores (M = 13.75, SD = 4.06) compared to domestic space (M = 9.12, SD = 3.06) for the high salience vignette (see Figure 5). The interaction between OCD Group and Environment was not significant (F > .05). Means with standard errors for state disgust responses for public and domestic spaces between the low and high OCD groups.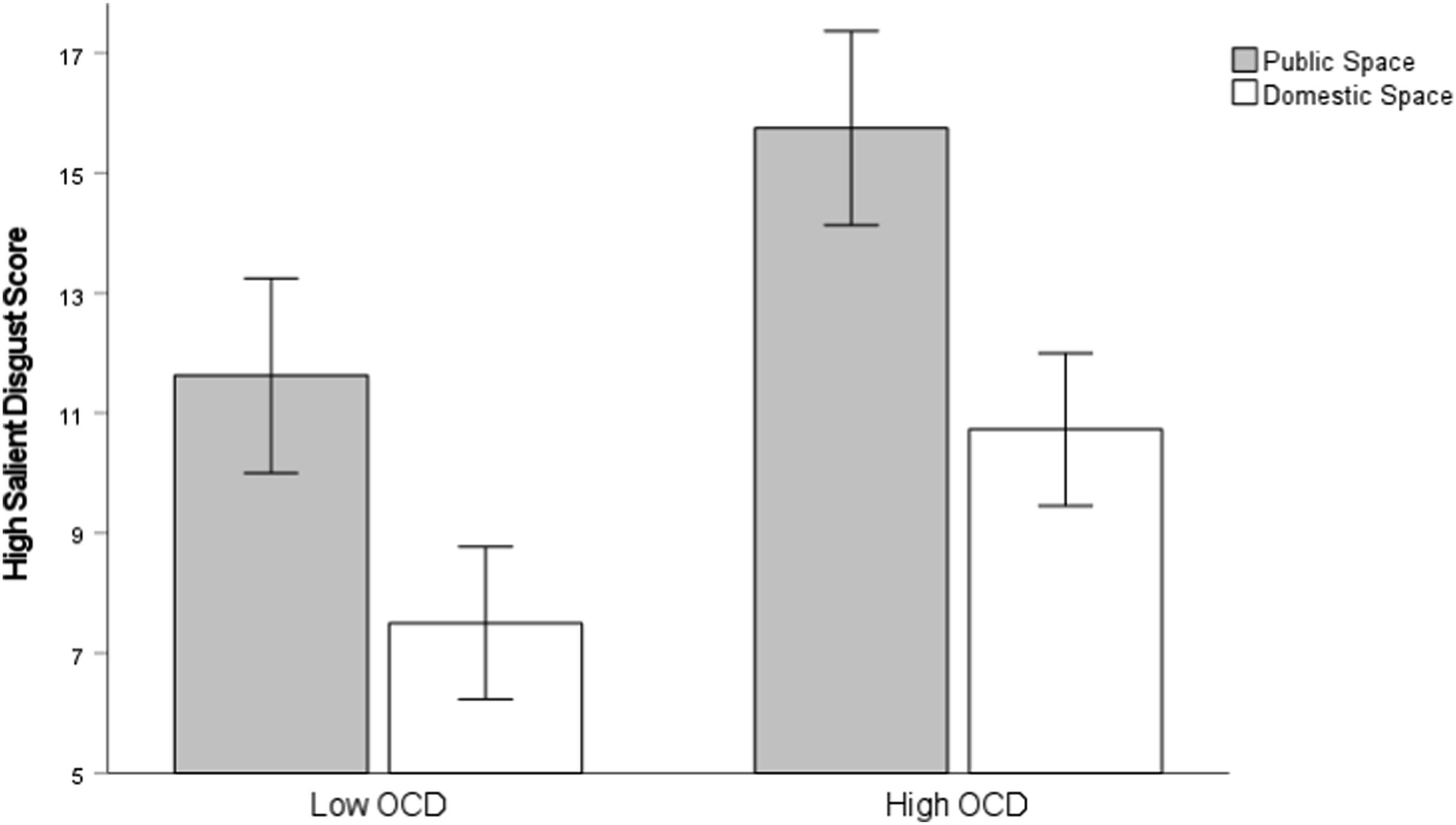
We also conducted a 2 (OCD Group: low vs. high OCD) × 2 (Environmental Space: public vs. domestic) ANOVA, with anxiety scores for the high salience vignettes as the dependent variable. The result showed a significant main effect of OCD group (F (1, 88) = 61.40, p = .001, ηp2 = .41), with the high OCD group scoring higher in anxiety (M = 52.59, SD = 9.20) compared to the low OCD group (M = 40.93, SD = 7.9) for the high salience vignette. There was also significant main effect of Environment (F (1, 88) = 42.97, p = .001, ηp2 = .33), with public space showing higher anxiety scores (M = 52.30, SD = 9.17) compared to the domestic space (M = 42.5, SD = 9.18) for the high salience vignette (see Figure 6). However, the interaction between OCD Group and Environment was not significant (F > .05). Means with standard errors for state anxiety responses for public and domestic spaces between the low and high OCD groups.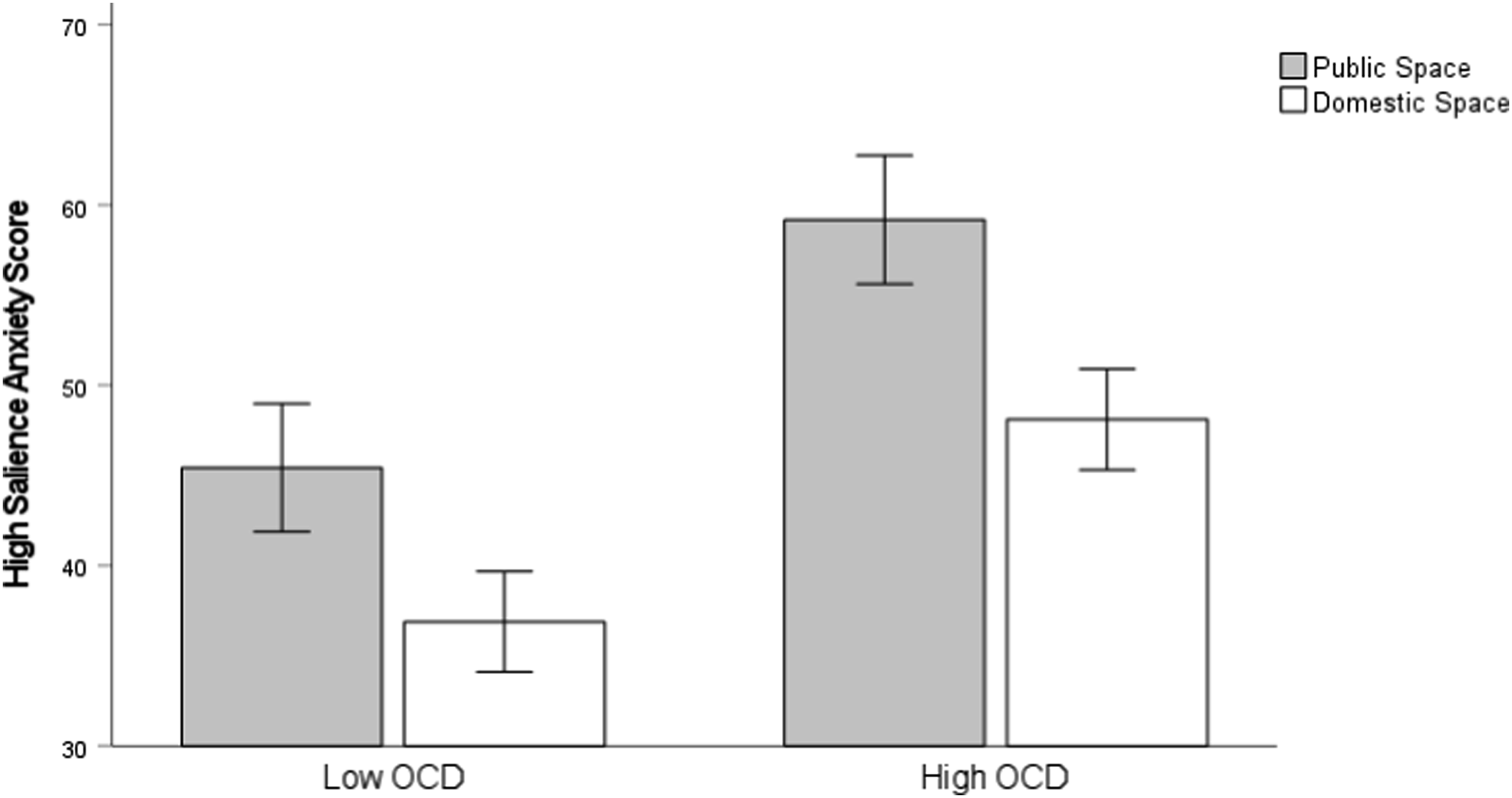
We conclude from these analyses that for high-scoring OCD participants, the salience of the contamination vignettes (i.e., high vs. neutral) is more emotionally meaningful to them than the actual location (public vs. domestic) of contamination in our studies.
Discussion
The present study aimed to show that state disgust and anxiety are sensitive to the presentation of contamination-related vignettes, a pattern we expected to be most pronounced in high-scoring OCD participants. Our results corroborated our hypotheses (H1 and H2), with the most pronounced effect observed in participants with high OCD scores compared to those with low scores. Specifically, individuals with high OCD scores exhibited significantly greater levels of state disgust and anxiety after reading contamination-related vignettes (both high and low) when compared to the neutral control vignette. The reliability of these between-group effects is bolstered by the replication of the Study 1 findings in Study 2.
Nevertheless, it is important to note that we did not find support for hypothesis three (H3). Our observation revealed that the location of contamination scenarios in the vignettes (Study 1: public space vs. Study 2: domestic space) did not result in significant variations in state disgust and anxiety among high-scoring OC participants. These findings underscore the fact that contamination-related vignettes consistently evoked heightened feelings of disgust and anxiety in individuals with high OCD scores, which superseded whether the scenarios were situated in a public or domestic setting. In other words, what holds significance for high-scoring OC participants is the presence of contamination per se, in any form.
We conclude that our vignette manipulations resonated with OC symptoms at a sub-clinical level and with the exacerbation of these symptoms over the COVID-19 pandemic. The current research focus serves to improve measurement and development of novel methodological paradigms for experimental investigation, with a specific emphasis placed on understanding the mechanisms that may account for the role of disgust in OCD and related symptoms (for review; Olatunji et al., 2017).
Models of OCD, Interventions and Future Research
Building upon our research, we aim to contribute to the development of OCD models, interventions, and future investigations. In the first instance, a central aspect of a pandemic is that viruses are invisible, with the success of protective measures (e.g., handwashing) often uncertain. Consequently, this places a person with a propensity towards disgust in a position of ambiguity (e.g., “I have washed my hands for 20 seconds but is that enough?”), which potentially induces a form of thought-action fusion (TAF; Shafran et al., 1996): the extent that people believe a thought is equivalent to action. Moreover, this uncertainty surrounding contamination amplifies the likelihood of contamination-related thoughts (e.g., “Am I still contaminated with a virus?”), narrows the gap between thoughts and actions, and increases the likelihood of subsequent compulsive actions (e.g., excessive handwashing and its success) (Harkin & Mayes, 2008). In other words, excessive handwashing (action) only highlights the ambiguity and futility of trying to wash away the fear of being contaminated by an invisible virus (thought). An assertion supported by the work of Mertens et al. (2020) who reported that intolerance of uncertainty, anxiety and worry were predictors of fear of COVID-19. These points are consistent with previous research, which has demonstrated that reducing disgust propensity results in improvements in washing/contamination symptoms in those with OCD (Athey et al., 2015). Additionally, studies have highlighted the association between mental contamination and mental TAF (Coughtrey et al., 2013; Fergus & Rowatt, 2018); and how repetitive staring, attention, and checking reduces memory accuracy, confidence, and increased likelihood of further checking (Harkin & Kessler, 2011a; van den Hout et al., 2008; van den Hout et al., 2009; van den Hout & Kindt, 2003; van den Hout et al., 2019). Figure 7 provides an overview of a potential relationship between infectious pandemics, contamination-related vignettes, mental contamination, disgust, OC symptoms, and potential targets for intervention. Proposed relationship between pandemics, contamination-related vignettes, disgust propensity and the development and maintenance of obsessions and compulsions.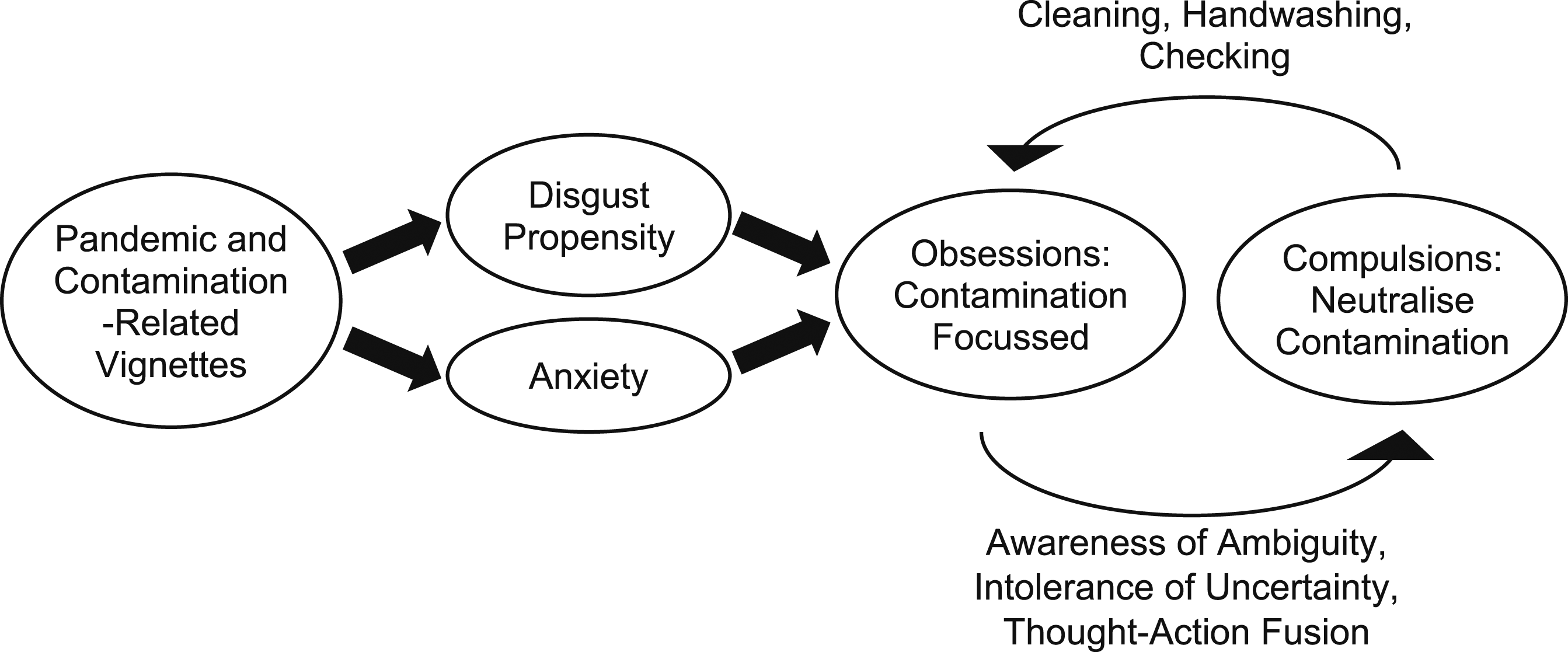
Regarding future research, we propose the following. First, in the context of contamination-related vignettes frequency of disgust could be combined with other established metrics known to drive OC symptoms; e.g., TAF (Shafran et al., 1996), memory (Harkin et al., 2011; Persson et al., 2021), confidence (Tolin et al., 2001), a desire to physically check and recheck (van den Hout & Kindt, 2003), cognitive fatigue (Pasquini et al., 2015), anxiety and avoidance (Abramowitz, 2006) and awareness of ambiguity (Harkin & Mayes, 2008). For example, concerning TAF, it would be interesting to examine if disgust propensity influences the distance between thoughts and actions and if this mediates the severity of OC symptoms or vulnerability to contamination-related vignettes or infectious pandemics.
Second, as questionnaires are the traditional method to record responses to vignettes, a more ecologically valid approach is to present contamination-related vignettes and then provide participants with the option of interacting with the content of the vignettes. For example, an update to the classic vignette paradigm is the ‘choose your own story’ task (Green & Jenkins, 2014), which provides participants with the opportunity to make decisions that impact subsequent outcomes and the option to return to previous decisions to change them (Freedman et al., 2018). Such an approach will improve the depth that participants engage with the text and provide researchers with more nuanced hypotheses and additional data to analyse (Stolte, 1994). We suggest that such an interactive and iterative approach lends itself naturally to measuring the symptoms of those with OCD via text, video, or virtual-reality-based contamination-focused vignettes. For example, in the context of our vignettes, when confronted with a source of viral contamination, participants could choose between (a) washing their hands, (b) asking the person if they feel unwell, (c) wearing a mask, or (d) leaving. After this, participants could be assessed qualitatively in terms of why they engaged in these behaviours and quantitatively by providing immediate emotional responses along dimensions of disgust, anxiety, TAF and OC symptoms. Such an approach would help identify those with a specific vulnerability to infectious pandemics and provide interventions with a means to assess the success of interventions (e.g., attention bias modification for threatening stimuli in OCD; see Amir et al., 2009) in a safe and controlled setting.
Our research has certain limitations that can be classified into two categories. First, our use of subclinical OC participants limits the extent that we can extrapolate our findings to clinical groups. However, we argue that subclinical groups tend to have fewer comorbidities and pharmacological interventions, making it easier to attribute our observed effects to OC symptom severity and disgust responsivity (Mataix-Cols et al., 1999). Second, we failed to find meaningful differences in disgust and anxiety responses for high-scoring participants in our public (Study 1) versus social space (Study 2) comparison. These findings are contrary to research showing more acute OC symptoms in the context of greater personal responsibility (Lopatka & Rachman, 1995; Moritz et al., 2007; Radomsky et al., 2001) and in settings of familiarity (Rachman, 2002). We posit that among high-scoring individuals with OCD, the emotional impact of the contamination vignettes (i.e., high vs. neutral) surpassed the influence of the physical location (public vs. domestic) of contamination in our studies. Future research is required to unravel the intricate relationship between locations, vignette content, and emotional responses in individuals with OCD. This multidimensional exploration will contribute to a deeper understanding of how these factors interplay and shape the emotional experiences of individuals with OCD.
Finally, the present study employed a vignette experimental design, featuring a vignette set size of 3 and a participant sample size of 40. In total, 120 vignettes were evaluated, each prompting two subjective emotional responses for state anxiety and disgust. To ensure statistical robustness, a priori power analysis for a repeated measures analysis of variance was conducted, revealing that a minimum sample size of 40 participants would yield greater than 80% power (α = .05) to detect an effect size of d = .46 (Cohen, 2013) across two groups for the dependent variables. The result of the study was evaluated together with the effect size, study efficiencies and confidence intervals to provide sufficient powered effects on main hypotheses, with most p-values returning less than .001. A properly powered study can often return p < .001 on a sample test that truly represents population level, just like 20% of tests can potentially return non-significant results (Brysbaert & Stevens, 2018). So, we propose that the results of the current study and its theoretical motivation to pursue the main effects with explicit predictions in terms of directional hypothesis, justify the sample size recommended in our G*Power analysis.
However, Brysbaert and Stevens (2018) suggest that an effect size of .4, and a sufficient sample size should be maintained to obtain a Type I error as low as 0.05 or 0.01 and a power as high as 0.8 or 0.9. It is also worth noting that an average effect size of .4 means that over 50% of the expected effect sizes are smaller, and that the probability of successful replication with an alpha value of p < .05, is around 50% (Vankov et al., 2014). Thus, significant results obtained from smaller sample sizes may represent an underpowered study. Stanley et al. (2018) argue that the sample size required for 80% powered studies are considerably higher than current practice, with replication studies often exceeding the minimum sample sizes produced from G*Power analysis (Szucs & Ioannidis, 2017). Therefore, we accept that a potential limitation for the present study is the smaller sample, and we embrace the challenge to keep informed with current trends in scientific voice. Replication is an important characteristic in statistical analysis (LeBel et al., 2018), so a future focus could be to determine meaningful research with smaller samples that would benefit replication with a larger sample size. A replication of the current study could increase in predictive power to .9 and increase the sample size to 100, which can potentially represent a more high-powered study of this important phenomena.
Conclusion
In conclusion, our study contributes to the existing knowledge on contamination-related OCD symptoms and highlights the emotional reactivity of individuals with OCD to specific stimuli. These findings have implications for interventions and future research, emphasizing the importance of addressing the salience of contamination cues in therapeutic approaches.
Footnotes
Acknowledgments
We would like to thank Isabel Sparks and Milly Killeen for data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.