
Abstract
Patient-physician relationship is ideally based on mutual trust. Trust usually takes times to build but can quite instantaneously be destroyed as a result of a single action or a single misperception. This study examined the way patients conceptualize the relationship between trust in a physician and perceived competency, honesty and openness, and personal involvement in care. One hundred sixty-seven patients aged 18–85 years were presented with a set of 27 three-item realistic vignettes that described situations in which participants could find themselves if hospitalized because of illness or accident. These scenarios resulted from the complete crossing of the three factors mentioned above. Participants were asked to assess the level of trust they would feel in each case. Through cluster analysis, three positions were found. For a minority of participants, trust was either unconditionally high (4%) or always quite low (8%). For a majority (75%), however, trust depended interactively on competency and honesty, on the one hand, and involvement, on the other hand; that is, the impact of competency and honesty on trust always depended on the level of involvement in care. In particular, when involvement had a low level, trust was always quite low, irrespective of the levels of both other factors. These findings are fully consistent with the view that, for a majority of patients, trust is inherently brittle: A breach in any one of participants’ expectations regarding physicians’ professionalism is enough to result in a more than proportional reduction in trust level.
Introduction
The patient-physician relationship is, ideally, based on mutual trust (Gilson, 2003). Patients’ level of trust has been repeatedly shown to be associated with positive health behaviors--willingness to consult, sharing of personal information, adherence to treatment, and continuity of care (Broholm-Jørgensen, et al., 2017; Espinosa & Kadić-Maglajlić, 2019; Nguyen, et al., 2009; O’Malley & Forrest, 2002; Rotenberg & Petrocchi, 2018)--and with positive health outcomes, such as timely detection of chronic illnesses and symptom improvement (Lee & Lin, 2009; Mainous, et al., 2004; Thom, et al., 2002).
Lack of trust in physicians has been shown to be associated with higher transaction costs (e.g., time taken to reassure the patient, ordering unnecessary analyses), patients’ disenrollment (Safran, et al. 2001), lower vaccination rates (MacArthur, 2017), medical tourism (Crooks, et al., 2015), costs due to litigation, and even mortality rates (Creed & Miles, 1996; Fiscella, et al., 1999). Physician’s level of trust in the patient has been shown to be associated with provision of information and prescription choices (e.g., willingness to prescribe effective but potentially dangerous drugs) (Moskowitz, et al., 2011).
Trust in a physician depends on many factors that are associated with the physician’s past and present behavior (Hall et al., 2001), the patient-physician congruence in beliefs (Krupat, et al. 2001), the patient’s personality (Sturgis et al., 2010), the patient’s health literacy level (Tsai et al., 2018), the patient’s culture (Kpanake et al., 2013), the patient’s religion (Benjamins, 2006), and also with the recent evolutions in the healthcare system (e.g., the implementation of managed care) (Mechanic & Rosenthal, 1999; Mechanic & Schlesinger, 1996). Among these many factors, the perceived levels of the physician’s technical competency, of the physician’s honesty and openness, and of the physician’s personal involvement in care (fidelity to the patient) have been found to be strongly associated with reported level of patient’s trust (Bashir, et al., 2019; Croker, et al., 2013; Gu, et al., 2019; Hwang, et al., 2017; Thom & The Stanford Trust Study Physicians, 2001). According to Hall et al. (2001), (a) a technically-competent physician produces the best achievable results through accurate diagnosis and appropriate treatment and, as far as possible, avoids hesitancies and mistakes, (b) an honest and open physician tells the truth to patients, is open to suggestions, and provides adequate information, and (c) a physician who is involved in care resolutely places patients’ best interests over any other consideration.
One characteristic of trust that has often been underlined by researchers is that trust between two persons usually takes times to build but can quite instantaneously be destroyed as a result of a single action or a single misperception (McDonald, et al., 2008). Trust “must be viewed as if it were an egg that when treated roughly could shatter” (Blanchard, 2010, p. 5); it is inherently “brittle” (Froud et al., 2012). These conceptualizations of interpersonal trust have led us to inquire into the nature of the cognitive relationship between trust as a global construct and its main components in terms of competency, honesty and openness, and personal involvement in care.
Suppose that, in patients’ minds, the relationship between these terms is simple and additive, so that the higher the physician’s competency level, the higher the physician’s level of honesty and openness, and the more the physician seems to involve himself or herself in care, the more this physician deserves to be trusted. In this case, any increase or decrease in only one of these aspects would result in a proportional increase or decrease in global trust level. If, for example, the perceived level of competency passes from “high” to “average” as a result of recent observations or in the light of new information, the overall level of trust would diminish but trust would not be completely destroyed all at once.
Suppose now that the relationship between these terms is complex and interactive and could be expressed using the following multiplicative mental equation:
Level of trust = Competency × Honesty and Openness × Involvement in Care.
In this case, any increase or decrease in only one aspect would result in a disproportional increase or decrease in trust. A decrease from “high” to “average” in any component would result in an abrupt fall in the level of trust. This kind of interactive relationship would be compatible with suggestions made by authors arguing that trust is, by nature, fragile (Froud et al., 2012; McDonald, et al., 2008).
The Present Study
The first aim of the present study was to examine the way patients conceptualize the relationship between trust and competency, honesty and openness, and personal involvement in care. The simulation technique was similar to that already used in analyzing people’s views about health issues involving complex relationships between constructs (Kpanake et al., 2018, 2019; Vera Cruz et al., 2019). The second aim of the study was to examine the extent to which patient’s views differ regarding the degree of trust that physicians deserve.
Our hypothesis was that (a) most patients would conceptualize the relationship between trust, on the one hand, and competency, honest and openness, and involvement, on the other hand, in a complex, interactive way that would be consistent with McDonald et al.’s views (McDonald, et al., 2008), although (b) a small number of patients would express principled positions of unconditional trust or of unconditional distrust (Gupta et al., 2014).
Method
Participants
Demographic Characteristics of the Sample. Composition of the Clusters.
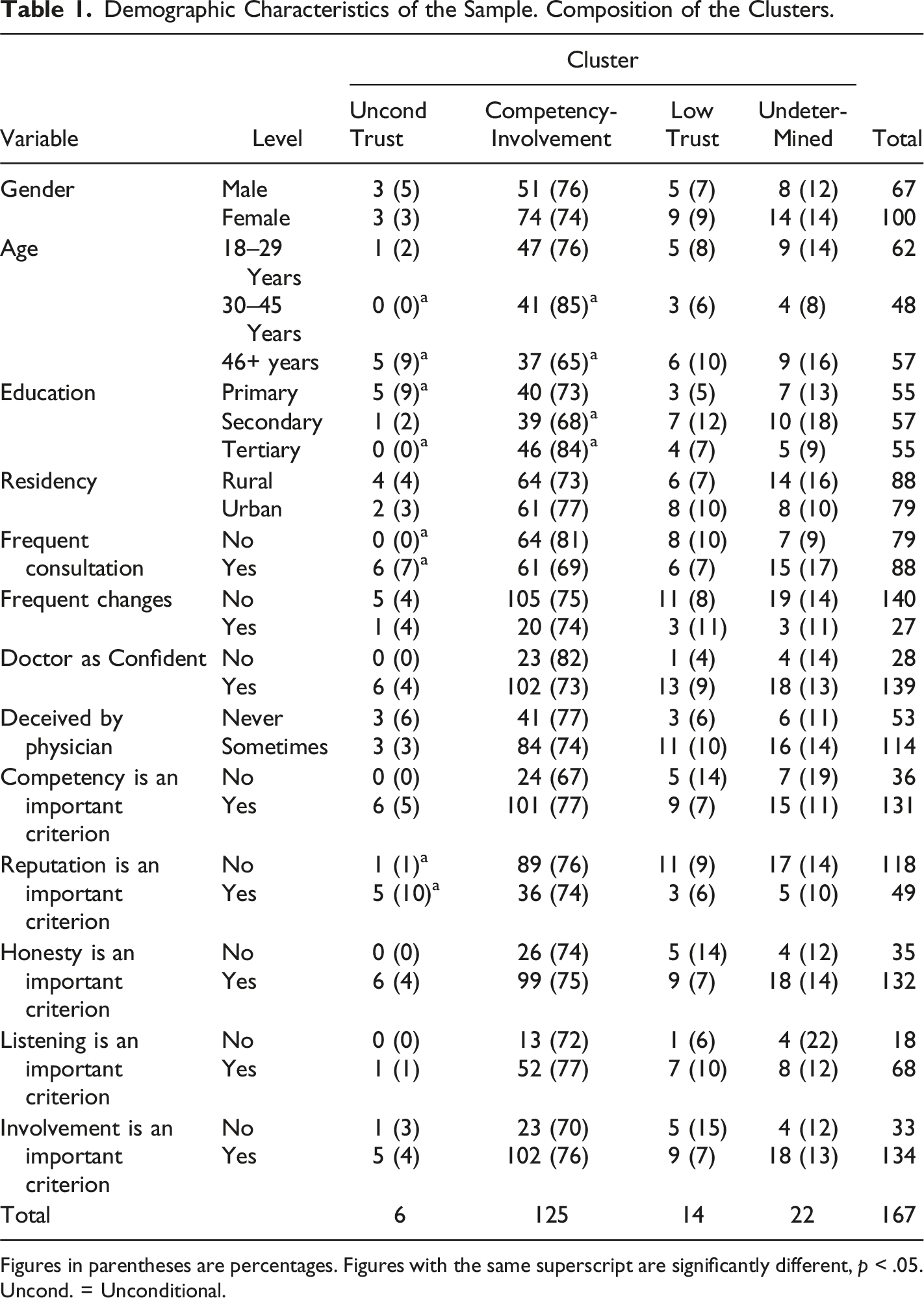
Figures in parentheses are percentages. Figures with the same superscript are significantly different, p < .05. Uncond. = Unconditional.
Material
The material consisted of 27 three-item scenarios that described a situation in which participants could find themselves in case of illness or accident. It was composed according to the principles established by Norman H. Anderson (2008). Since it was the judgment process itself that was being studied, the levels of the factors (the pieces of information) were combined orthogonally. This enabled us to study the main effects, but above all to characterize the interactions between factors. The 27 scenarios resulted from the complete crossing of three factors, each with three levels: (a) the treating physician’s perceived technical competence: he doesn’t look very competent and your family physician refuses to give you his opinion; he looks normally competent and your family doctor says he is a good physician; he looks very competent and your family physician says he is one of the best specialists in the field (as in the example); (b) the treating physician’s perceived level of openness and honesty: he doesn’t seem to be very honest with you and he doesn’t seem to be very open to discussion (as in the example); he seems to be normally honest with you and to be open to discussion; he seems to be very honest with you and is apparently very open to discussion, and (c) the treating physician’s perceived level of personal involvement in your cares: he doesn’t seem to be very involved in care; he seems to be normally involved in care; he seems to be very involved in care (as in the example).
The response scale – of sufficient breadth to avoid, as far as possible, floor or ceiling effects – was a 20-point scale with a left anchor labeled “Not at all” (1) and a right anchor labeled “Completely” (20). An example of a scenario is the following: “Suppose you have been hospitalized for one week. Your treating physician seems to be very competent in his field. According to your family’s doctor, this physician is one of the best experts in the field. You have, however, the impression that this physician is not very honest with you; in addition, he does not seem to be open. Nevertheless, he seems to be very interested in your case, and very involved in the care that is provided. To what extent would you feel inclined to trust this physician?” As shown in the example, only terms and expressions that were fully familiar to the participants were used. Another scenario in shown in Appendix A.
Procedure
Data were gathered in accordance with Anderson’s recommendations for this kind of study (Anderson, 2008). Each volunteer was tested on an individual basis, in a quiet room, usually in the volunteer’s home. Some participants were interviewed in an unused classroom at the university. Scenarios were presented in random order, varying from participant to participant. Participants took 20–40 minutes to complete the session. None of them complained about the number of vignettes they were required to evaluate or about the credibility of the proposed situations. After having completed the judgment task, participants were invited to answer some questions about what they consider important in the patient-physician relationship (see Table 1).
Ethical approval for the study was granted by the Ethics Committee of the Federal University of Toulouse, France. All participants signed a consent form before completing this survey, and responses were anonymous.
Results
Main Results of the ANOVAs.
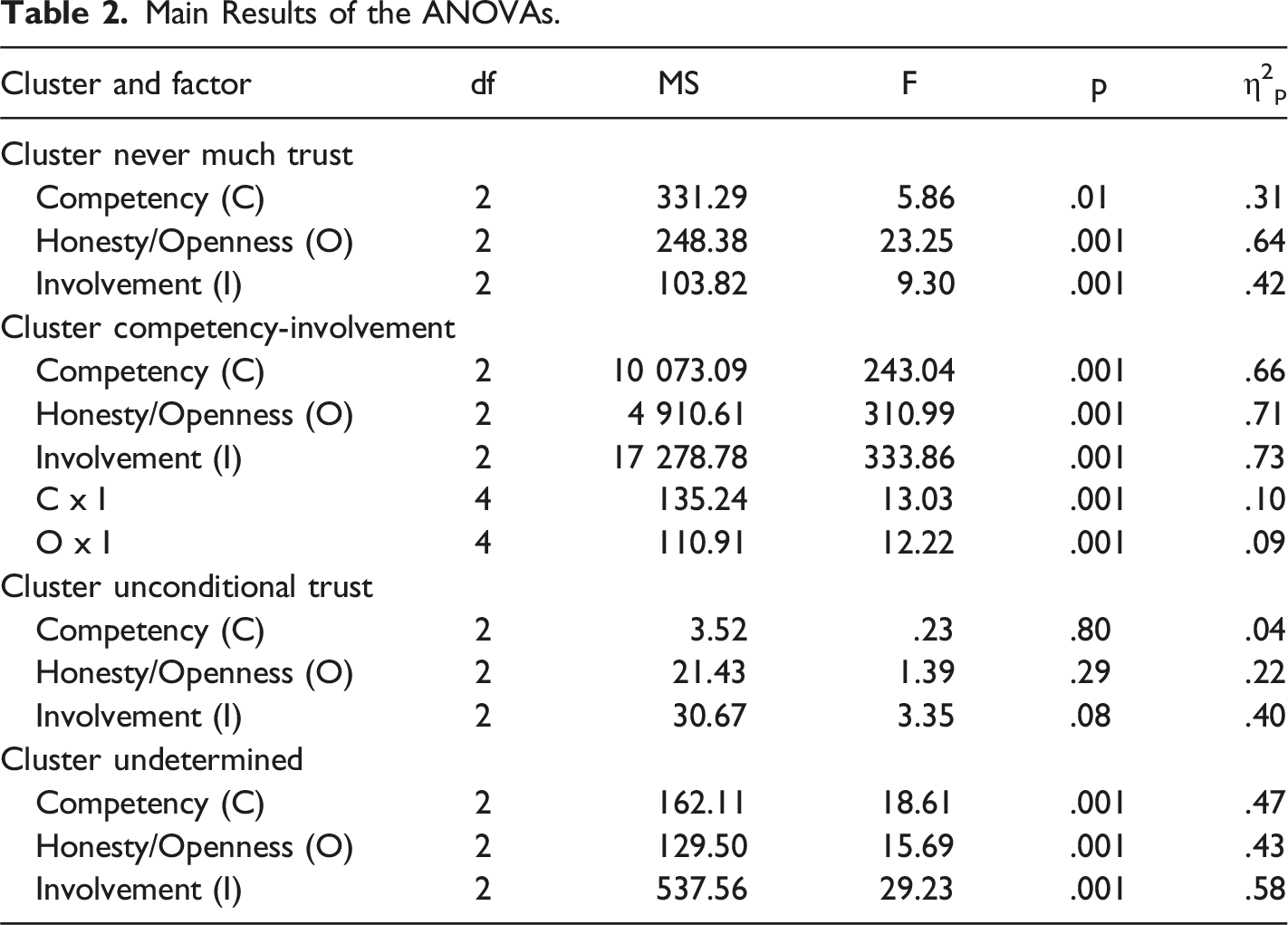
The first cluster (N = 6, 4%) was the expected Unconditional Trust cluster. As can be observed in Figure 1 (top row), trust ratings were always close to the positive end of the response scale (M = 18.01). As shown in Table 1, participants aged 46+ years, participants with only primary education, participants who frequently consulted a physician, and participants for whom physician’s reputation was an important criterion were more often in this cluster than participants aged 20–45 years, participants with tertiary education, participants who did not consult frequently, or participants for whom reputation was not an important criterion. Clusters of Trust Judgments. Trust judgments are on the vertical axis, the three levels of personal involvement are on the horizontal axis, the three curves correspond to the three levels of competency, and the three panels correspond to the three levels of honesty/openness. Each row corresponds to a cluster: Unconditional (top row), Competency-Involvement (middle), Never Much (bottom).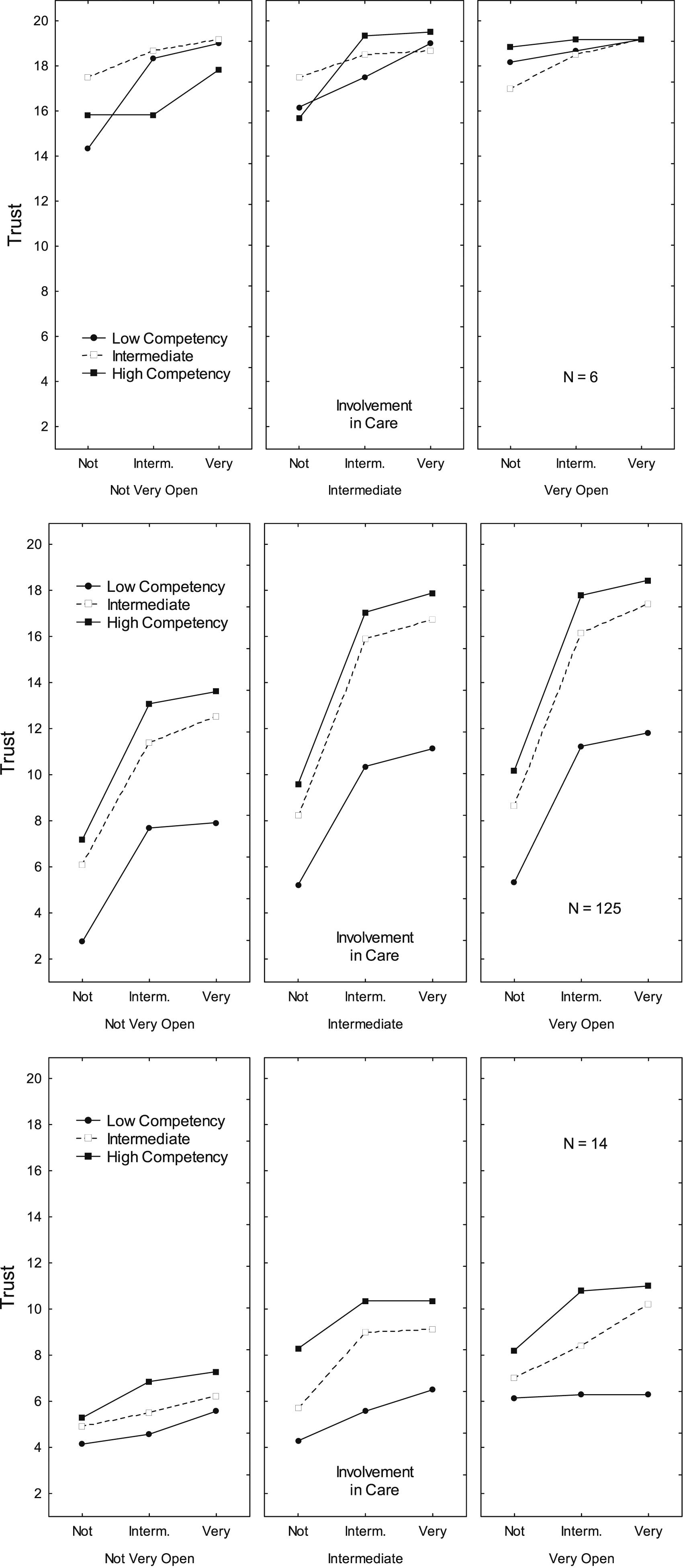
The second cluster (N = 125, 75%) was the expected interactive cluster. It was called Competency-Involvement because, as can be observed in Figure 1 (center row), these two factors were the ones with the strongest impact. Ratings were considerably higher (a) when the physician’s technical competency was high (M = 13.87) rather than low (M = 8.16) and when the physician’s involvement in care was very high (M = 14.17) rather than low (M = 7.03). In addition, the effect of competency on trust was stronger when the level of involvement was high (16.65 – 10.29 = 6.36) rather than low (8.99 – 4.43 = 4.56). Ratings were higher when the physician’s honesty and openness were very high (M = 13.00) rather than low (M = 9.14), and in the same way, the effect of honesty on trust was stronger when the level of involvement was high (15.90 – 11.35 = 4.55) rather than low (8.06 – 5.35 = 2.71). Participants aged 30–45 years and participants with tertiary education were more often members of this cluster than participants aged 46+ years or participants with secondary education.
The third cluster (N = 14, 8%) was the expected Low Level of Trust cluster because, as can be observed in Figure 1 (bottom row), ratings were nearly always on the left side of the response scale (M = 7.18). Ratings were, however, slightly higher (a) when physician’s technical competency was high (M = 8.71) rather than low (M = 5.48), (b) when physician’s honesty and openness were very high (M = 8.26) rather than low (M = 5.60), and (c) when physician’s involvement in care was very high (M = 7.89) rather than low (M = 6.16).
A fourth cluster (N = 22, 13%) was also found. It was called Undetermined because ratings were always close to the center of the response scale (M = 11.36) and were not affected by any of the three factors.
Discussion
As expected, three qualitatively different positions regarding patient’s trust in physicians were found. For a minority of patients, trust was either unconditionally high (4%) or always quite low (8%). Unsurprisingly, trust was always high particularly among older patients with only primary education who consult their physician on a regular basis. These findings were consistent with previous views (Gupta, et al., 2014).
For a large majority of patients, however, trust depended on information about technical competency, honesty and openness, and involvement in care. The importance attributed to each factor in the judgment process was, however, not equivalent. Involvement explained roughly half of the variance in trust judgment, followed by competency and honesty. This is consistent with the results reported by Thom and The Stanford Trust Study Physicians (2001). It supports the view expressed by most authors that trust depends not only on perceived technical competency but also on relational issues (Hall, et al. 2001).
In addition, the relationship between factor levels and trust judgments was not linear. A high level of trust was associated not only with the highest levels of all of the three factors, but also with “normal” levels of technical competency, honesty and openness, or involvement in care. This finding supports the idea that the “average” physician—who has adequate although not exceptional levels of all three factors—may, in participants’ views, be trusted as much as the “exceptional” physician. Finally, the impact of competency and honesty depended on the level of the physicians’ involvement in care. In particular, when involvement had a low level, trust judgments were always quite low, irrespective of the levels of both other factors.
The following equation is an attempt to synthesize the complex relationship between the four constructs:
Trust = Involvement (Competency + Honesty)
For most participants, judged trust depended on a multiplicative combination of Involvement on the one hand, and Competency and Honesty in additive combination on the other hand. This equation is consistent with the finding that a breach in any one of participants’ expectations regarding physicians’ professionalism (which is in some way a composite of the three factors) is enough to reduce notably the level of trust, especially if this breach is about the physician’s perceived involvement in care (Froud et al., 2012; McDonald et al., 2008). Nevertheless, the level of trust attributed to situations in which one factor has a low level is never nil; it is usually close to the center of the trust scale. This means that, even in these not fully satisfying cases, a certain level of trust can be achieved for a majority of patients, and more importantly, suggests that trust can probably be rebuilt if a positive change is observed in the aspect that was not optimal.
Some participants gave a middle-of-scale rating to all scenarios, i.e., they did not have strong feelings for or against the physician’s trustworthiness in any situation, and they gave no indication of what quality in a physician was of greater importance. The scenario-based methodology allowed us to separate these participants from the others and to realize that their ratings indicated not mild views regarding trust, but indecision or even indifference. Small groups of undetermined participants have often been found in health-related studies (Kpanake et al., 2019).
Limitations
The first limitation of this study is that it is a convenience sample of lay people living in one region of France who were willing to complete a time-consuming judgment task. The second limitation is that only a small number of factors could be studied. An orthogonal design requires a multiplicative increase in the number of scenarios as additional pieces of information, such as the doctor’s gender, are considered. Such an increase quickly becomes too burdensome for participants.
Future studies should, therefore, investigate the degree to which the relationships between trust, perceived competence, perceived honesty and openness, and perceived involvement in care are affected by the doctor’s demographic characteristics (e.g., age and gender), and by the participant’s state of health or psychological state. Despite its limitations, this study is, to our knowledge, the first to empirically investigate the cognitive reasons why trust is so difficult to build and so easy to destroy.
Conclusion
This study showed empirically that people’s trust in their doctors is a function of multiple important elements, namely their perceptions of competence, honesty and above all the doctor’s involvement in their care. To gain patients' trust, doctors sometimes have to devote a great deal of time and effort. A breach in any one of these elements can significantly, and sometimes instantaneously, reduce the level of this trust, although a certain amount of confidence may nonetheless remain.
These findings are probably not limited to trust in physicians (Rotenberg, 2018). In business or in international relationships, for example, trust is also a precious good without which it is difficult to achieve anything of importance: A single breach (e.g., whether, in the case of a company, a delivery cannot take place or whether, in the case of peace negotiations between two parties, an unexpected movement of troops has been detected) can be enough to alter considerably the quality of relationships between parties.
Footnotes
Acknowledgements
We would like to thank the people who tested early versions of the material used in this study or conducted the pilot studies: Karine Chevalier and Katia Schaller.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the University of Toulouse Jean Jaurès and the Canada Research Chairs program (Grant number: 950–230745). The funding bodies had no role in the design of the study; in the collection, analysis, and interpretation of data; in the writing of the manuscript; or in the decision to submit the paper for publication.
Data Availability Statement
Appendix
A second example of the material used You’ve been in hospital for a week. The doctor treating you doesn’t seem to be very competent in his field. Your family doctor has refused to share his opinion. You don’t feel that he’s being very honest with you, nor does he seem to be very open. However, he does seem interested in your illness and your care. You have the impression of being followed normally. To what extent do you feel inclined to trust this doctor? Not at all o---o---o...... o---o---o Completely