
Abstract
Research supports an association between dissociation and elevations in feelings of shame. Yet, some work suggests this connection may be influenced by interpersonal relationship context, with shame heightened when dissociation is experienced with a close friend compared to when alone or with an acquaintance. The current studies sought to further clarify the relational context in which dissociation appears to maximize shame activation. Participants read stories depicting either dissociation or sadness in different relationship contexts, and subsequently responded on measures of emotions, state shame, shame explanations, and perceived behavioral responses. Study 1 (N = 328) revealed that shame feelings were common responses to dissociation, but did not differ when dissociation occurred with an old or new therapist. In Study 2 (N = 345), shame was again elevated in response to dissociation. Additionally, single-item shame ratings were heightened following dissociative experiences with a close friend and doctor compared to when alone, and in these former two contexts showed increased shame with dissociation compared to sadness. Shame appears to follow the experience of dissociation, and this relationship may strengthen when in the presence of another, suggesting that social relationships may be an important variable in the relationship between shame and dissociation.
Dissociation and shame are common responses to traumatic experiences (Bash and Papa, 2014; Dalenberg and Carlson, 2012; Dorahy et al., 2015), yet there may also be a more direct association between the two constructs (Benau, 2020; Benau, 2022; Dorahy et al., 2017; Platt et al., 2017; Thomson and Jaque, 2013). Shame is a painful affect associated with negative appraisals of the self as inadequate, flawed or unacceptable (DeYoung, 2015; Schoenleber et al., 2015). Dissociation is commonly understood to involve disruptions and discontinuities in normally integrated functions (e.g., emotions, cognitions, behaviors) that organize an individual’s personality (Dorahy et al., 2017; Nijenhuis and Van der Hart, 2011; Platt et al., 2017; Schimmenti, 2016). Dissociative symptoms may arise as a response to painful emotions, especially those associated with highly distressing experiences in relationships (DeYoung, 2015; Otis et al., 2012; Platt and Freyd, 2015; Schimmenti and Caretti, 2016). Studies have shown elevations in dissociative experiences as shame feelings mobilize (Dorahy et al., 2017). Recent work also indicates this relationship might be bi-directional, with elevations in shame following dissociative experiences (Benau, 2022; Dorahy et al., 2021). Given the clinical and theoretical implications (e.g., patients feeling ashamed of dissociating), the current study assesses whether shame feelings are associated with a rise in dissociation, and whether this association depends on the relational context in which dissociation occurs.
Using college student participants (study 1) and those living with the psychological impact of trauma exposure (study 2), Dorahy et al. (2021) found those experiencing dissociation via controlled induction or spontaneously, reported elevations in acute feelings of shame. In female students with a trauma history, Platt et al. (2017) found that elevations in dissociation produced increased levels of state shame. Given shame is intimately connected with relational experiences (Benau, 2020; DeYoung, 2015), McKeogh et al. (2018) administered vignettes where dissociation occurred in different relationship contexts (i.e., with a close friend, with an acquaintance, when alone). They found that feelings of shame were higher when dissociating compared to feeling sadness in the presence of a close friend but not when alone or with an acquaintance. Findings from this study indicated that shame may be particularly elevated when dissociation was experienced in the context of more intimate relationships (i.e., a close friend).
The sense of discontinuity and destabilization associated with dissociation may be more threatening when with a close friend as relationally there is more at stake. Specifically, as human beings are social creatures that care deeply about social connection and our sense of self-worth and security is tied to our social belonging (Baumeister and Leary, 1995; Leary and Baumeister, 2000), dissociation may be especially threatening in a relational context that potentially undermines our social relations. Such appraisals of dissociation with a close friend may lead to further appraisals that rejection or exclusion will follow, which activates shame. As a result of these appraisals of dissociation, McKeogh et al. (2018) suggested that “dissociation might have the capacity to act as a natural ‘shamer’ when occurring with close others” (p. 53). However, as these findings were tested in only one specific interpersonal context, it remains unclear the extent to which these appraisals operate in different relationship contexts in which dissociation is experienced. The current set of studies manipulated the relationship contexts to examine the association between dissociation and shame and explored if appraisals associated with dissociation-induced shame were consistently made in different interpersonal situations.
Study 1
Study 1 extended the work of McKeogh et al. (2018) by examining whether dissociation would result in greater shame in a clinical setting where one is with a therapist they have an established relationship with or a new therapist. This allowed an interpersonal context where intimate self-disclosures were likely heightened but familiarity (which was equated in this study with greater closeness) differed. Study 1 also sought to identify what appraisals about dissociation are associated with elevations of shame. Specifically, the study examined whether appraisals around exclusion, loss of control, feeling flawed, fearing rejection, and being exposed would relate to elevated shame in those who dissociate in different contexts.
Method
Participants
Four-hundred and twenty-one participants were recruited from Crowdflower, an online crowdsourcing platform similar to Amazon’s Mechanical Turk (Peer et al., 2017). Of these participants, 93 were excluded for completing the survey in a time period considered impossible for accurate responding (i.e., under 5 minutes), stopping before completing the survey, or failing the two validity checks (detailed below). The final sample of 328 participants were aged between 18–60 years (M = 35.07; SD = 11.09) and were equally divided between male (n = 166; 50.6%) and female (n = 162; 49.4%). The majority were American citizens (n = 310; 95.10%), leaving 16 (4.90%) from countries such as India, Venezuela, and Colombia. Two participants did not complete this question. For race/ethnicity, the majority were White/European (n = 259; 79%), with 29 (8.80%) identified as Hispanic American, and 18 (5.5%) as African American. The remainder (n = 22; 6.6%) were either Asian American, Native American, Multiracial, or identified as “Other” (i.e., not specifically listed ethnicity). Just under half the participants were married (n = 139; 42.4%), 36.30% (n = 119) were single, 20.40% (n = 67) were in a relationship, and a very small number were either separated (n = 2; .6%) or widowed (n = 1; .3%). Almost half the participants had a Bachelor’s degree (n = 148; 45.10%). The remaining reported the following education: 63 (19.20%) tertiary course or diploma, 48 (14.6%) High School, 47 (14.3%) Master’s degree, eight (2.4%) PhD, 10 (3%) ‘not specifically listed other qualification’ and four (1.2%) leaving High School before finishing. Thus, this was overall a well-educated sample.
Seventy-three participants (22.3%) described being diagnosed with a psychological illness (see https://osf.io/z3pwx/ for specific details). A total of 85 participants (26%) indicated having seen a therapist for a mental health difficulty, of which 20 (6.1%) were currently in therapy.
Measures
Demographics
In addition to answering brief demographic questions (gender, age, relationship status, ethnicity, nationality, and highest qualification), participants indicated whether they had been diagnosed with a mental health difficulty, and whether they were ever in therapy (all using “yes/no” items).
Trait Dissociation
The Detachment and Compartmentalisation Inventory (DCI) contains 22 self-report items (α = .96), assessing both types of dissociation (i.e., detachment and compartmentalization) using a 0 (never) to 7 (daily) scale (Butler et al., 2019). Responses exclude experiences only happening under the influence of alcohol or drugs and items 8 and 15 act as validity control items. The DCI demonstrates strong psychometric properties (Butler et al., 2019).
Trait Shame
The Experience of Shame Scale (ESS) measures trait shame across 25 items (α = .96) using a 4-point scale ranging from 1 (“not at all”) to 4 (“very much”) (Andrews et al., 2002). A validity control question was added near the middle of the ESS which read, “If you have read this question, please indicate not at all” (item 17). The ESS has strong psychometric properties (e.g., Andrews et al., 2002; Duran and Lewis, 2012).
Experimental Stimuli
Vignettes
Vignettes offer an analogue for experience rather than capturing the direct experience, but allow control over variables that can be later tested directly. The vignettes used in the current research were based on McKeogh et al. (2018), with changes made to the relationship contexts (e.g., rather than close friend as seen in McKeogh et al., 2018, Study 1 used old therapist). Whilst similar to McKeogh et al. (2018), to ensure understanding and flow between the narratives and measures of shame, the vignettes were piloted on 10 post-graduate psychology students.
Study 1 utilized two independent variables: “Experience” which manipulated dissociation and sadness (control) experiences, and “Relationship context” that manipulated whether the experience was with a new therapist, old therapist, or alone. The “experience” of dissociation was captured by having a flashback, experiencing amnesia, and experiencing depersonalization in line with previous research on the manifestations of dissociation (e.g., McKeogh et al., 2018). For the control condition, sobbing, feeling heavy and being gloomy represented the three comparative sadness experiences.
The second independent variable “relationship context” determined whether the “experience” occurred with an old therapist (i.e., someone you have been seeing for a long time), a new therapist (i.e., someone you have had two previous sessions with), or when alone. This led to the creation of 18 vignettes (dissociation: flashback, amnesia, depersonalization/derealization vs. sadness: sobbing, heavy, gloomy when with old therapist, new therapist, or when alone), whereby nine reflected dissociation in each relationship context and nine reflected sadness in each relationship context (see: https://osf.io/z3pwx/).
For the “experience” independent variable, the flashback condition had the person losing contact with their surroundings and being transported back to an earlier traumatic experience; the amnesia condition had the person feeling disoriented and experiencing a feeling of drifting off such that when they “returned,” they were not aware of what had been happening and why they were sitting in a different position in their chair; and in the depersonalization/derealization condition, the person experienced detachment from their body (depersonalization) and feeling as though the new/old therapist was a long way away (derealization). Regarding the sadness vignettes, the dissociation content in each of the three relationship contexts was replaced with material the same length that reflected sadness-related experiences. Both the sobbing condition (i.e., tears rolling down the person’s face) and the gloomy condition (i.e., feeling gloomy and down) spoke about feeling this way when remembering a recent occurrence, while the heavy condition spoke of a heavy feeling in the person’s body upon remembering people whom contact has been lost. For the relationship contexts, the alone scenario involved being home alone reading a book, the old therapist scenario involved seeing a long-term therapist and talking about a recent experience, and the new therapist scenario involved meeting up with a therapist who had only been seen twice before and discussing current problems.
Following previous work (e.g., McKeogh et al., 2018), the vignettes were written in second person narratives (e.g., “you become upset about something that happened to you recently”) in order to heighten their self-referential nature. Within all the vignettes, certain words and phrases were bolded to further emphasize the dissociation or sadness experience being reported.
Measures of State Shame
Three measures were used to assess whether shame was evoked upon imagining oneself in the vignettes. The first assessed seven separate emotions including shame via individual questions (e.g., “Would you feel”: Angry? Ashamed/Embarrassed? Sad? Surprised? Anxious? Guilty? Relaxed/Calm?). Immediately after reading each vignette, participants rated their feelings using a 5-point scale from 0 (not at all) to 4 (extremely). Different emotions were assessed to determine whether shame in isolation was related to dissociation. Shame and embarrassment were treated as a single emotion as they are considered to both belong to the same affect family (Nathanson, 1992; Tomkins, 2008). Participants who rated themselves anywhere between 1 (a little) and 4 (extremely) for the shame/embarrassment emotion were asked to further rate why they felt ashamed/embarrassed after reading the vignette (i.e., feeling exposed or flawed, as though they had lost control over themselves, isolated/excluded from what is happening inside them, isolated/excluded from what is happening around them, feeling badly if others knew what they were experiencing, and feeling judged/rejected if someone was to see them in this way). Participants rated their reasons for feeling ashamed using an identical 5-point scale of 0 (not at all) to 4 (extremely).
The second shame metric was the 5-item state shame subscale from the State Shame and Guilt Scale (SSGS, Marshall et al., 1994). The wording of the phrases on the original shame subscale were slightly adapted by creating a question for each statement (e.g., “would you feel worthless, powerless?”). Using a 5-point scale, participants rated how much they felt each of the five shame items from “not at all” (1) to “very strongly” (5). The SSGS has sound psychometric properties (Marshall et al., 1994).
Drawing in part on Nathanson’s (1992) Compass of Shame, and the measure developed by McKeogh et al. (2018), the final shame measure assessed seven behavioral responses to shame (e.g., withdraw, attack self and attack other). For both the new/old therapists contexts, the seven behavioral responses were: talk to your new/old therapist about it, quickly leave the room to get away from your new/old therapist, hide your head in your hands or divert your gaze from your new/old therapist, get annoyed with yourself for having this experience in the presence of your new/old therapist, distract attention away from what happened and talk to your new/old therapist about something else, get frustrated with your new/old therapist for being with you, and sit calmly with your new/old therapist. The alone context contained the same seven behavioral responses but was designed to reflect having the experience when alone (e.g., quickly leave the room where it occurred, get annoyed with yourself for having this experience). Again, using a 5-point scale from 0 (never) to 4 (definitely), respondents rated likely engagement in each behavioral responses (for all state measures see: https://osf.io/z3pwx/).
Procedure
Participants were recruited from Crowdflower. They completed the study via Qualtrics, starting with an information and consent forms and demographic questions. After this, in randomized order, participants completed the DCI and ESS. They were then randomly assigned to one of six conditions: alone-dissociation, old therapist-dissociation, new therapist-dissociation, alone-sadness, old therapist-sadness, and new therapist-sadness. Each condition contained three vignettes that reflected either different dissociative experiences (depersonalization/derealization, flashback and amnesia), or comparison experiences (sob, gloomy and heavy). Participants were asked to imagine themselves in the situation and respond to the shame measures after reading each of their three vignettes. Upon completion they redeemed a $1.50 credit. The study was approved by the University of Canterbury human ethics committee (HEC 2017/64).
Design and Analysis
To cover the domain of dissociative and sadness experiences, and to facilitate the interpretation of the analysis, the three dissociation groups (i.e., flashback, amnesia, depersonalization/derealization) and the three sadness groups (i.e., sob, heavy, gloomy) were collapsed to form single experiences of both dissociation and sadness. Thus, the primary analysis was a 2 (Experience: dissociation, sadness) by 3 (Relationship Context: new therapist, old therapist, alone) between-subject design, where the main effect for “experience” assessed if shame increased in the dissociation compared to sadness context and the interaction effect assessed if relationship context was implicated. The dependent variables were: (1) seven separate self-report emotions (e.g., anger, shame, relaxed/calm) assessed by Multivariate Analysis of Variance (MANOVA), (2) seven shame explanations (e.g., feel flawed, exposed, judged) assessed by MANOVA, (3) the state shame scale assessed by univariate analysis of variance (ANOVA), and (4) the behavioral responses (e.g., talk, leave, hide) assessed by MANOVA. Pillai’s trace statistic was interpreted for MANOVA results, while Gabriel’s was used for post-hoc assessments as sample sizes were unequal (Field, 2013). All data are available at https://osf.io/z3pwx/.
Results
Participants did not differ across conditions (Experience x Relationship context) for trait dissociation and shame (see https://osf.io/z3pwx/ for data and analysis; Supplementary Table B1). Although the three different types of dissociation and sadness were averaged to capture a single score for each experience (McKeogh et al., 2018), within group differences did exist (e.g., depersonalization produced less shame generally than amnesia or flashbacks; see https://osf.io/z3pwx/ for statistics).
Chi Squared tests revealed those currently in therapy were evenly distributed across both Experience (dissociation, sadness), χ 2 (1, N = 328) < .00, p = 1.00, V = .00, and Relationship Context (alone, new therapist, old therapist), χ 2 (2, N = 328) = 4.30, p = .12, V = .12 (See Supplementary Table B2 and Supplementary Table B3 at https://osf.io/z3pwx/). Thus, current therapy was not used as a covariate. Regarding the 85 participants reporting having ever seen a therapist, they strongly trended towards being unevenly distributed across Relationship Contexts, χ 2 (2, N = 327) = 5.94, p = .05, V = .14, and had significantly different multivariate scores on the single item emotions, V = .06, F (7, 319) = 3.10, p = .004, η2p = .06, the behavioral responses, V = .06, F (7, 319) = 2.82, p = .007, η2p = .06, and higher state shame scores, F (1, 325) = 19.59, p < .001, η2p = .06 (See Supplementary Table B4 and Supplementary Table B5 at https://osf.io/z3pwx/). Thus, having ever seen a therapist was used as a co-variate in the analysis.
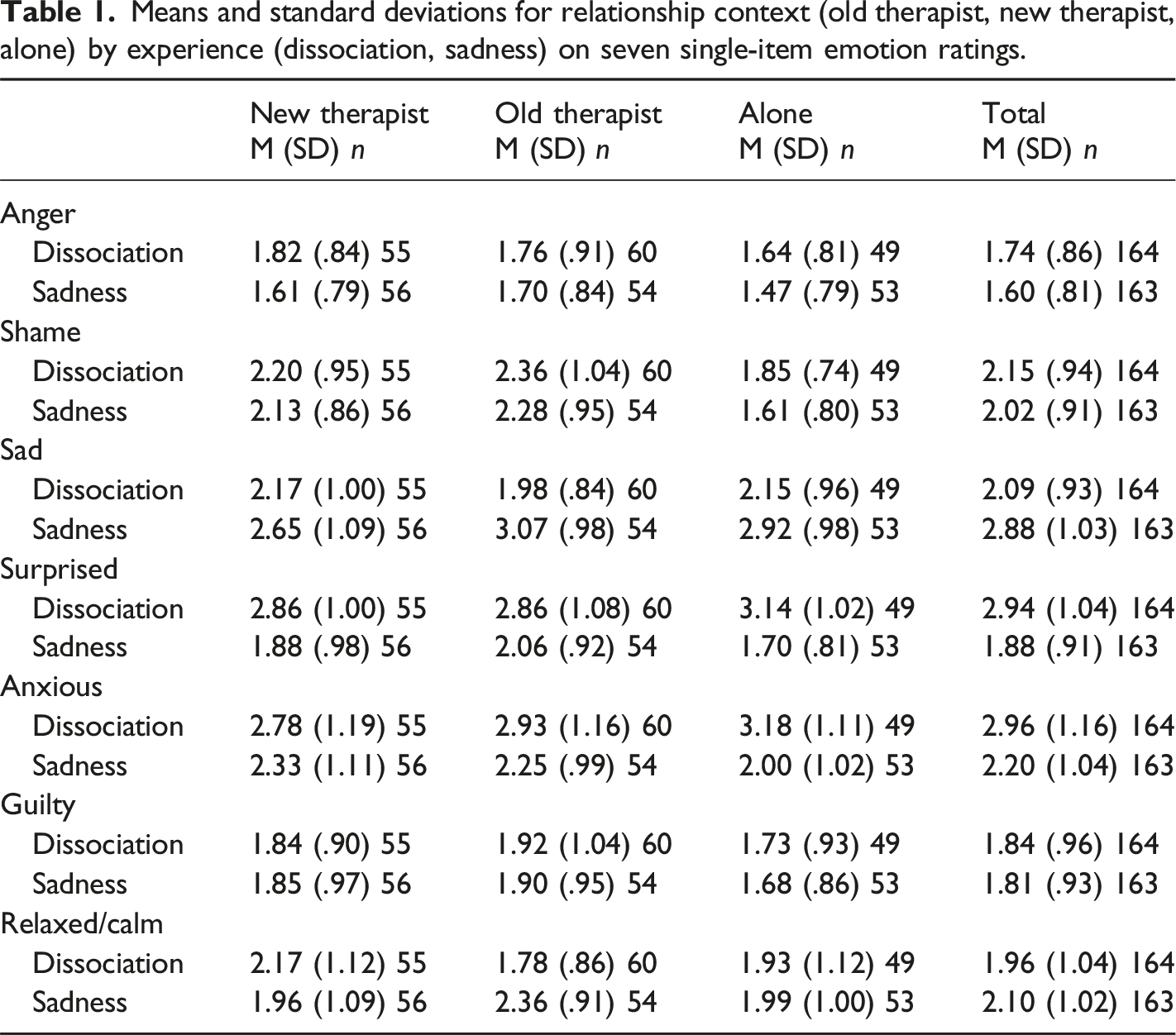
Single-item Emotions
Means and standard deviations for relationship context (old therapist, new therapist, alone) by experience (dissociation, sadness) on seven single-item emotion ratings.
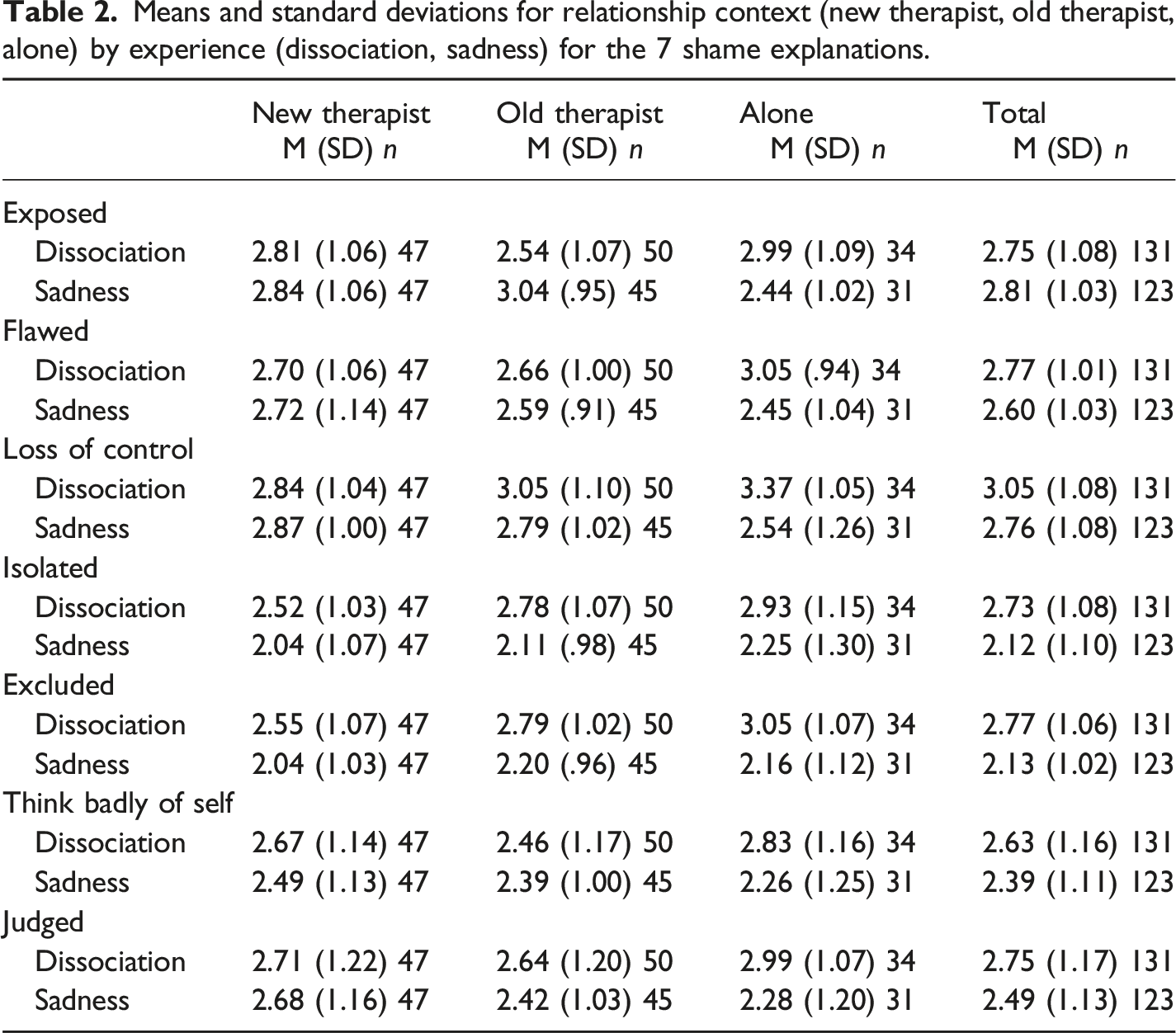
Shame Explanations
Means and standard deviations for relationship context (new therapist, old therapist, alone) by experience (dissociation, sadness) for the 7 shame explanations.
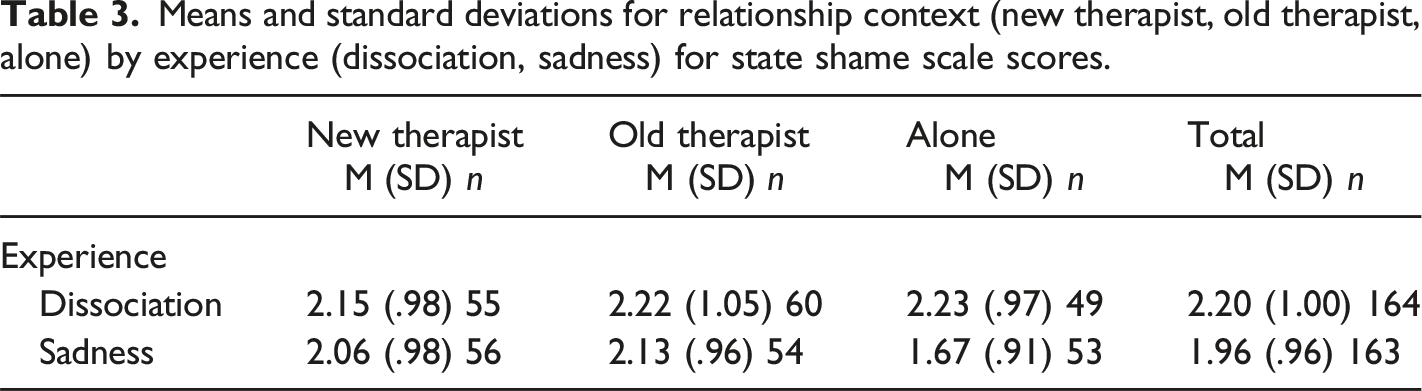
State Shame
Means and standard deviations for relationship context (new therapist, old therapist, alone) by experience (dissociation, sadness) for state shame scale scores.
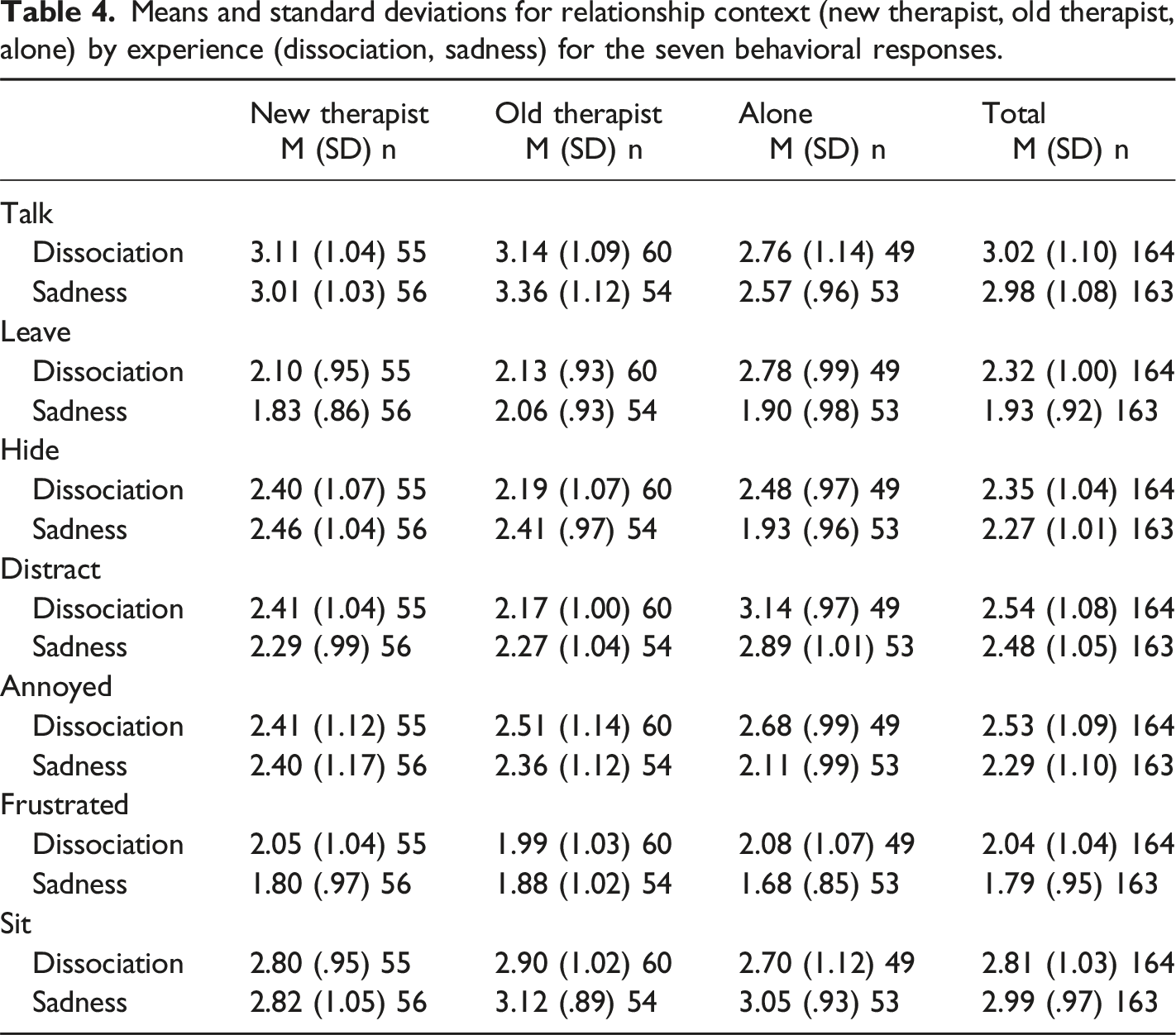
Behavioral Responses
Means and standard deviations for relationship context (new therapist, old therapist, alone) by experience (dissociation, sadness) for the seven behavioral responses.
Discussion
The primary hypothesis that shame would heighten following experiences of dissociation was partly supported, with higher state shame scale ratings, regardless of relationship contexts, when imagining dissociating compared to feeling sadness. The single-item shame measure did not yield similar findings. The five-item state shame measure, where the word “shame” is not directly mentioned, is considered more opaque and more psychometrically sound than the single item shame measure (Turner, 2014) and findings were consistent with Dorahy et al. (2021), who used a dissociative induction technique. Yet, McKeogh et al. (2018) used the same outcome measures and found effects for dissociation on both the single-item and state shame measures. The close friend condition used by McKeogh et al. (2018) may be more potent for producing shame when dissociation occurs than the old and new therapist contexts, where such symptoms might be deemed a little more acceptable.
Anxiety was an emotion of importance, with higher scores in the dissociation compared to sadness experience. More specifically, dissociation when with an old therapist produced more anxiety and less relaxation than sadness. In addition, anxiety was higher when dissociating alone than when feeling sadness alone. Dissociation experiences alone or in more intimate contexts seem to be associated with anxiety, where McKeogh et al. (2018), amongst others (Dorahy et al., 2017; Simeon et al., 2003) also reported higher anxiety with dissociation and concluded that anxiety may be a ubiquitous response to experiences of dissociation.
Neither the single item nor state shame measures were different for shame in the dissociation compared to the sadness condition in different relationship contexts. Thus, there was no support for experiences of dissociation in a therapeutic relational context (i.e., new, old therapist) increasing feelings of shame compared to when alone. Single item shame was heightened in the new and old therapist context compared to when alone, but this was not specifically related to the dissociation condition. Elevated shame feelings across experiences were evident with a close friend or acquaintance in McKeogh et al.’s (2018) study. Seemingly, having dissociative experiences or feelings of sadness in the presence of another, regardless of the level of intimacy, is shame evoking, at least as assessed with the single item shame measure. Given shame is in essence a relational affect (Benau, 2020; Benau, 2022; DeYoung, 2015; Dorahy et al., 2013), it is perhaps not surprising that regardless of whether experiencing sadness or dissociation, people felt more ashamed when in the presence of another as opposed to when alone.
Regarding the shame explanations, participants who felt shame while imagining dissociating attributed this as due to them feeling isolated from what was happening inside and around them, being judged negatively, and as though they had lost control over themselves. Different drivers may be involved in why shame might occur following dissociative experiences including (1) the shame-inducing experiences of feeling alienated from self and others (see DePrince et al., 2015), (2) being appraised negatively, and (3) losing control of psychomotor functioning (Benau, 2022). Therefore in the clinical context, careful exploration of the specific appraisals relevant for dissociation-associated shame with each client may heighten therapeutic precision. For the interaction, the alone context showed a loss of control and feeling exposed being higher when dissociating than when experiencing sadness. This is consistent with Gilbert’s (2000) internal shame where the individual makes negative appraisals of their self as defective, out of control and exposed (e.g., defectiveness is being exposed to the self; Moore and Fine, 1990).
Results from the behavioral responses showed unique findings for dissociation. Regardless of the relationship context, participants imagining dissociation reported having a greater desire to leave the room where it occurred and feeling frustrated at the therapist or another person. These comprise the withdrawal and attack-other scripts, respectively, in Nathanson’s (1992) compass of shame responses. Thus, experiencing dissociation in general may give rise to similar behavioral responses as shame.
In sum, this study found dissociation increased shame, but only when assessed with the state shame measure and not the single-item shame measure. There was evidence based on the single item measure that shame was elevated when experiencing dissociation and sadness with an old or new therapist than when alone. Thus, the relational context seems to be important to shame feelings when experiencing dissociation or sadness. However this finding was not specific to dissociation, and is also in contrast to those from Dorahy et al.’s (2021) induction study, where relationship context was not related to the dissociation-shame association. The same was true in the current study for the state shame measure where the main effect of relationship context along with its interaction with experience were not significant.
Taken together, this study further supports dissociation commonly giving rise to negative affective states such as shame across different interpersonal contexts. Yet, the study used seeing a therapist to manipulate intimacy in a design that required participants to imagine themselves in that scenario. However, only a quarter of participants actually had the experience of seeing a therapist and intimacy in such contexts was not assessed. Consequently, it was unclear how much intimacy the two therapy contexts elicited given the apparent lack of familiarity participants had with the chosen contexts and that time in therapy may not equate well with increased intimacy.
Study 2
In an effort to overcome the possible lack of intimacy in the relationship contexts used in study 1, this study used both close friend and being with a doctor, along with the alone context. Most participants would have the experience of being to a doctor and have to a greater or lesser extent some form of relationship with them. The close friend context previously demonstrated a relational effect between dissociation and shame (McKeogh et al., 2018). To further address the issue of intimacy, a single control question was included in Study 2 assessing how comfortable participants felt sharing personal information with either their close friend or doctor. Additionally, based on previous work (e.g., Wu et al., 2022), two personality control questions were included to control for any differences in shame responding associated with having a personality style more concerned with rejection in relationships (consistent with an anaclitic personality style) or more prone to engage in self-criticism (consistent with an introjective personality style). These two personality characteristics have been associated with shame (Dorahy and Hanna, 2012; Wu et al., 2022), so controlling them allowed greater assessment of the specific relationship between shame and dissociation.
It was predicted that dissociative experiences would produce increased feelings of shame. Second, experiences of dissociation were hypothesized to produce elevated feelings of shame when with a close friend and when with a doctor compared to when alone.
Method
Participants
Four hundred and forty three participants started the survey using Cloud Research (previously called Turk Prime; Litman et al., 2017), a crowd sourcing data acquisition platform built on Amazon’s Mechanical Turk (MTurk) (Buhrmester et al., 2011). Of these, 98 did not complete the study or were excluded for failing at least one of the five validity checks, including robot questions (verbal and pictorial), an absurd question and completing the survey in less than 5 minutes,. The final sample comprised 345 adults with an age range of 21–61 years (M = 39.09; SD = 10.7), where 187 identified as male (54%), 157 as female (46%) and 1 as gender neutral (.3%). No significant difference between the included and excluded samples were evident for age, F (1, 437) = 3.36, p = .07, η2p = .008, or gender, χ 2 (1, N = 436), = .31, p = .58. Ethnic composition was similar to Study 1, with the majority identifying as White/European (n = 253; 81%). In addition, both relationship status and education had a very similar break down to Study 1 with the largest group being married (n = 147; 43%) and having a Bachelor’s degree or above (n = 197; 57%), respectively. Mental health difficulties were reported by 67 (19%) participants, with the majority of these (90%) reporting anxiety and/or mood disorders.
Measures
Demographics
The same demographic and mental health questions from Study 1 were used. The questions about seeing a therapist were replaced with, “do you currently have a close friend?” and “do you have a doctor whom you see at least occasionally?”
Trait Dissociation and Trait Shame
The DCI and ESS were again used to assess trait dissociation and shame respectively. These once again showed high internal consistency (DCI: α = .95; ESS: α = .97).
Intimacy and Personality Control Questions
To address intimacy comfort, participants in the doctor and close friend contexts across both experiences rated on a five-point scale from 0 (not at all) to 4 (extremely), “how comfortable do you feel sharing personal information with your doctor/close friend?”. Regarding personality, two questions drawn from the Depressive Experiences Questionnaire (DEQ, Blatt et al., 1976) were chosen as they most fully captured anaclitic personality orientation (“I am very sensitive when around others for signs of rejection,” Question 28) and introjective personality orientation (“I tend to be very critical about myself,” Question 64) (Riley and McCranie, 1990). Responses were made from 1 (strongly disagree) to 7 (strongly agree).
Experimental stimuli
Vignettes and Measures of Shame
The same 18 vignettes used in Study 1 were adapted so new and old therapist were substituted for doctor and close friend respectively. For example, rather than having an appointment with a therapist whom one had been seeing for a long time (Study 1, old therapist context), participants in the close friend context met up with a very close friend they have known for a long time (https://osf.io/z3pwx/). The dependent variables were the same as Study 1.
Procedure
The procedure of Study 2 mostly mimicked Study 1 with the addition of participants in the doctor and close friend contexts answering the intimacy control question, and all participants answered the two personality control questions.
Another addition in Study 2 was increased validity checks to ensure the data obtained were reliable. To help address the issue of “bots” (Dreyfuss, 2018), participant ticked a box stating, “I am not a robot,” answered an absurd question, “would you feel like wearing socks on your head?” (responses other than “not at all” were excluded), and indicated the second and fourth letters of the capital city of the USA (i.e., a, h). To further prevent bots responding, this latter question was inserted as a picture rather than typed out. Similar to Study 1, participants completed all of the questionnaires online via Qualtrics survey software. Participants received $2 US towards their Amazon account upon completion of the survey. The Human Ethics Committee at the University of Canterbury approved all procedures (HEC 2018/21).
Design and Analysis
The design of Study 2 was identical to Study 1. Experience (dissociation, sadness) and relationship context (close friend, doctor, alone) were the key independent variables, while state shame, shame explanations, and behavioral responses were the dependent variables. Pillai’s trace statistics was again shown for MANOVA results and Gabriel’s used for post-hoc analysis. All data are available at https://osf.io/z3pwx/.
Results
Similar to Study 1, no differences were evident for trait dissociation across Experience and Relationship Context. For trait shame there was no experience main effect or interaction, but the relationship context effect was significant, with those in the doctor context having more trait shame than the close friend and alone contexts (see Supplementary Table B6 https://osf.io/z3pwx/). Thus, trait shame was used as a covariate in the analysis. The majority of participants reported currently having a close friend (92%) and seeing their doctor at least occasionally (79%) and scores on these measures did not differ across experience or relationship context (see Supplementary Table B7 and Supplementary Table B8 https://osf.io/z3pwx/). No differences across conditions were evident for anaclitic or introjective personality orientation (see Supplementary Table B10 https://osf.io/z3pwx/). As in Study 1, scores from the three dissociation experiences (i.e., amnesia, depersonalization, flashbacks) and the three sadness experiences (i.e., heavy, sob, gloomy) were respectively collapsed into single scores (see https://osf.io/z3pwx/ for specific within experience differences). For the intimacy manipulation question (comfort sharing personal information) across the four conditions (excluding alone), there was a main effect for Experience, with those in the dissociation experience reporting greater comfort sharing personal information, and trends towards significance for relationship context and the interaction (see Supplementary Table B9 https://osf.io/z3pwx/). Participants felt less comfortable sharing sadness experiences with their Doctor compared to sadness with their close friend or dissociation with a close friend or their doctor.
Single-item Emotions
Means and standard deviations for relationship context (doctor, close friend, alone) by experience (dissociation, sadness) on seven single-item emotion ratings.
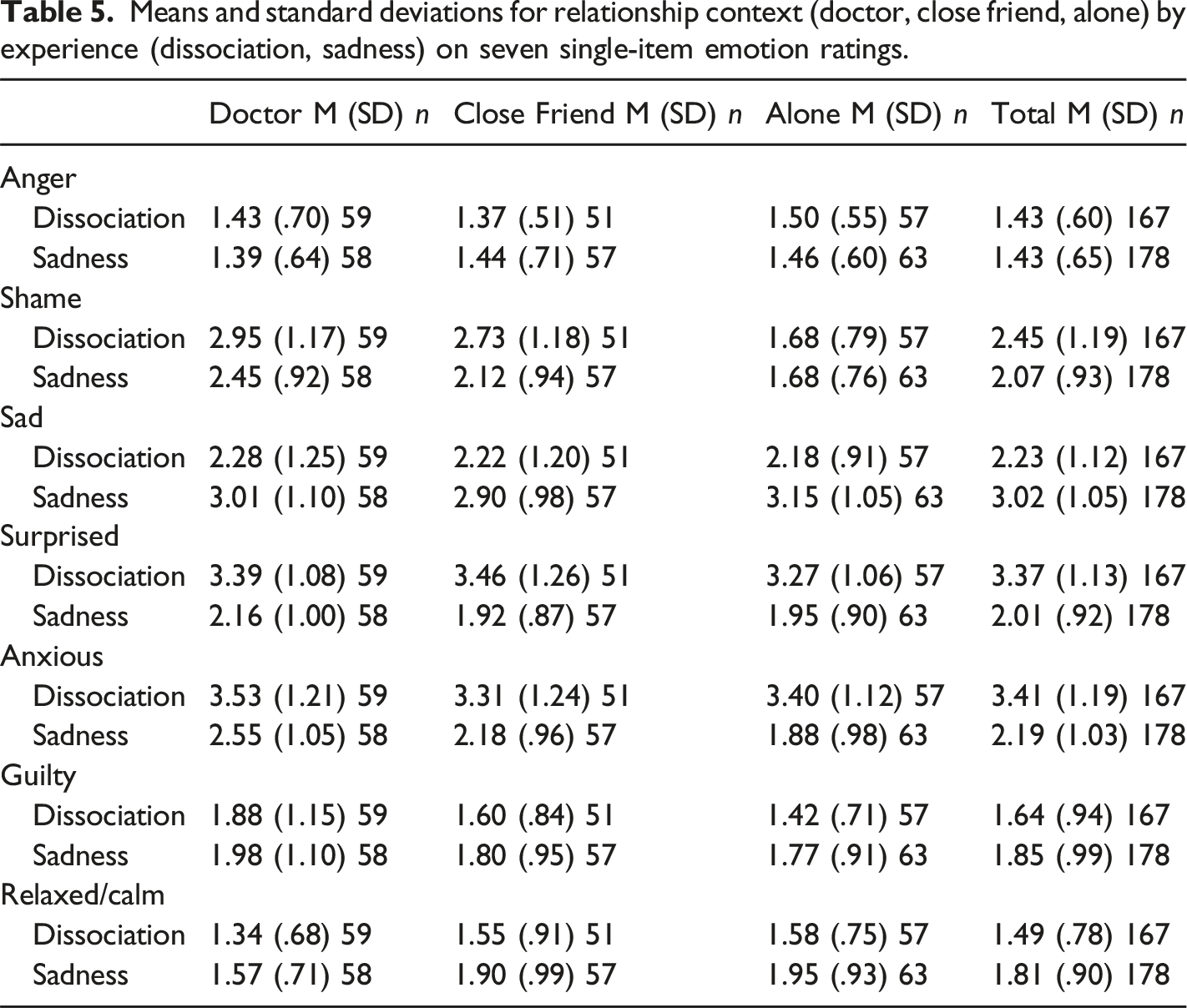
Regarding experience, ANCOVA with trait shame controlled showed higher ratings for shame, F (1, 338) = 19.59, p < .001, η2p = .06, surprise, F (1, 338) = 155.49, p < .001, η2p = .32, and anxiety, F (1, 338) = 150.61, p < .001, η2p = .31, in the dissociation compared to sadness experience. In contrast, the sadness compared to dissociation experience had elevated scores for sad, F (1, 338) = 52.89, p < .001, η2p = .14, and relaxed, F (1, 338) = 13.43, p < .001, η2p = .04, while trending in that direction for guilty feelings, F (1, 338) = 3.83, p = .05, η2p = .01. For Relationship Context controlling for trait shame, there was a significant univariate effect for shame, F (2, 338) = 35.79, p < .001, η2p = .18, and relaxed, F (2, 338) = 3.25, p = .04, η2p = .02. Post-hoc analysis showed that regardless of whether exposed to sadness or dissociation, respondents felt more shame when with a doctor, F (1,234) = 63.47, p < .001, η2p = .21 or close friend, F (1,225) = 44.78, p < .001, η2p = .17, compared to when alone. No differences were found for shame between doctor and close friend, F (1,222) = .60, p = .44, η2p = .003. Regarding ratings for relaxed, scores were lower in the doctor context compared to when with a close friend, F (1,222) = 4.18, p = .04, η2p = .02 or alone, F (1,234) = 7.82, p = .006, η2p = .03, with the latter two groups not differing, F (1,225) = .16, p = .68, η2p = .001.
For the multivariate interaction, the only significant univariate interaction was for shame, F (2, 338) = 4.49, p = .01, η2p = .03. Simple effects analysis showed higher shame in the dissociation compared to the sadness experience when with a doctor, F (1, 14) = 11.40, p = .001, η2p = .09, or close friend, F (1, 105) = 12.81, p < .001, η2p = .11. No difference was evident when alone, F (1, 117) = .02, p = .89, η2p < .001. Thus, compared to sadness, dissociation elicited more shame feelings in intimate contexts but not when alone.
Shame Explanations
Means and standard deviations for relationship context (doctor, close friend, alone) by experience (dissociation, sadness) for the seven shame explanations.
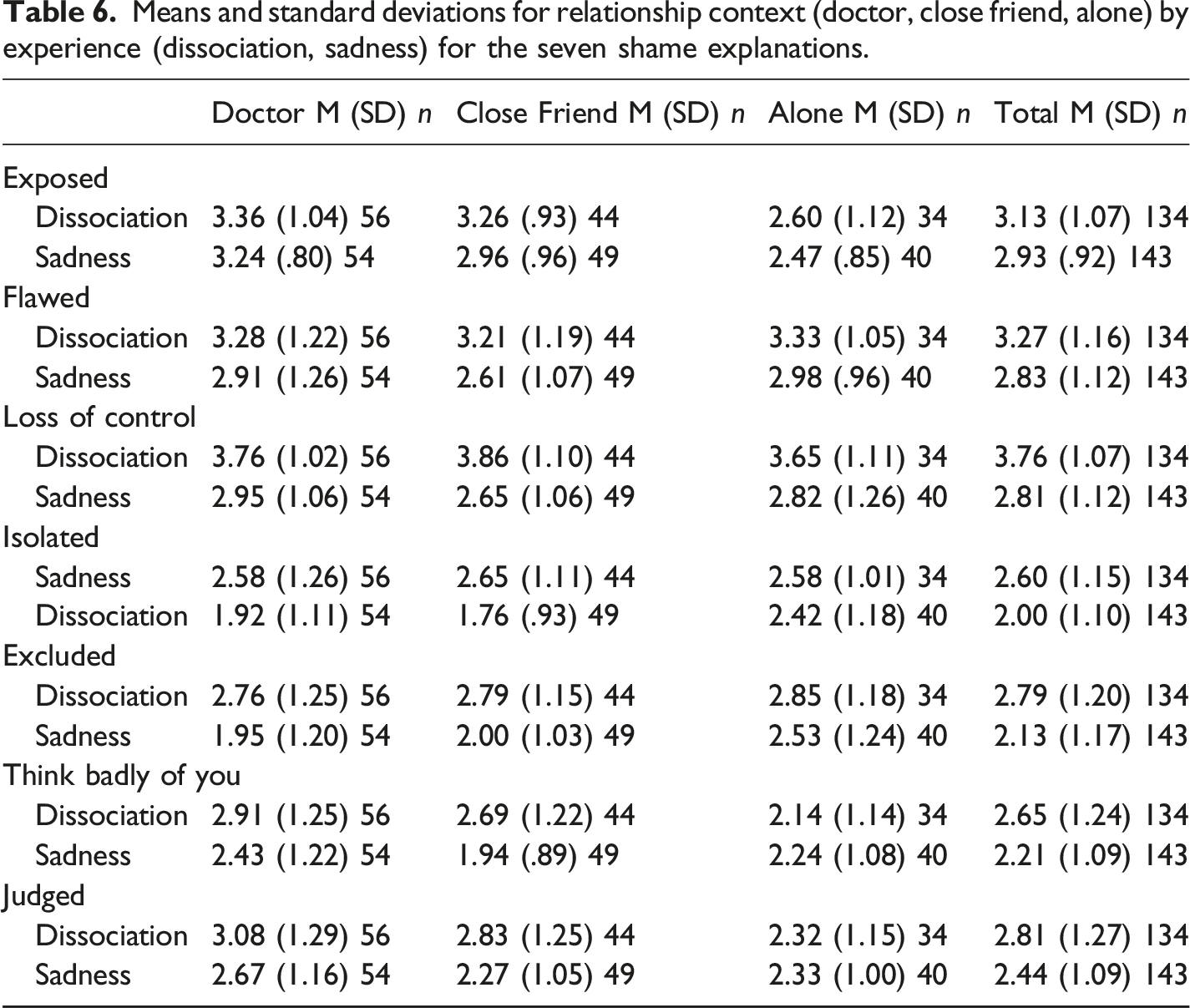
The Experience main effect showed higher ratings in the dissociation compared to sadness conditions for flawed, F (1, 270) = 17.16, p < .001, η2p = .06, out of control, F (1, 270) = 60.98, p < .001, η2p = .18, isolated, F (1, 270) = 21.98, p < .001, η2p = .08, excluded, F (1, 270) = 25.52, p < .001, η2p = .09, feeling badly that others know of the experience, F (1, 270) = 12.44, p < .001, η2p = .04 and feeling judged, F (1, 270) = 9.38, p = .002, η2p = .03. Additionally, there was a trend for exposed, F (1, 270) = 3.41, p = .07, η2p = .01. Regarding Relationship Context, univariate analysis showed significant effects for exposed, F (2, 270) = 15.78, p < .001, η2p = .12, excluded, F (2, 270) = 3.50, p = .03, η2p = .03, feeling badly, F (2, 270) = 3.24, p = .04, η2p = .02, and feeling judged, F (2, 270) = 4.73, p = . 01, η2p = .03. Post hoc analysis controlling for trait shame showed that shame when dissociating or experiencing sadness was more likely associated with feeling exposed when with a doctor, F (1,181) = 28.17, p < .001, η2p = .14, and close friend, F (1,164) = 21.41, p < .001, η2p = .12, compared to when alone. No difference was evident between doctor and close friend, F (1,200) = .37, p = .54, η2p = .002. For feeling excluded, the doctor context was higher than being alone, F (1,181) = 5.64, p = .02, η2p = .03, and there were no differences between being with a close friend and alone, F (1,164) = 1.78, p = .18, η2p = .01, or being with a doctor and close friend, F (1,200) = 1.06, p = .30, η2p = .005. Post-hoc tests showed that regardless of whether dissociating or feeling sadness, participants were significantly more likely to feel badly that others know of the experience when with a doctor compared to when alone, F (1,181) = 5.92, p = .02, η2p = .03. No differences were evident for close friend versus being alone, F (1,164) = 1.81, p = .18, η2p = .01 or with a doctor, F (1,200) = 1.36, p = .25, η2p = .007. For feeling judged, scores were higher when with a doctor, F (1,181) = 8.95, p < .003, η2p = .05, and close friend, F (1,164) = 4.83, p = .03, η2p = .03, compared to when alone. No difference was evident between doctor and close friend, F (1,200) = .61, p = .44, η2p = .003.
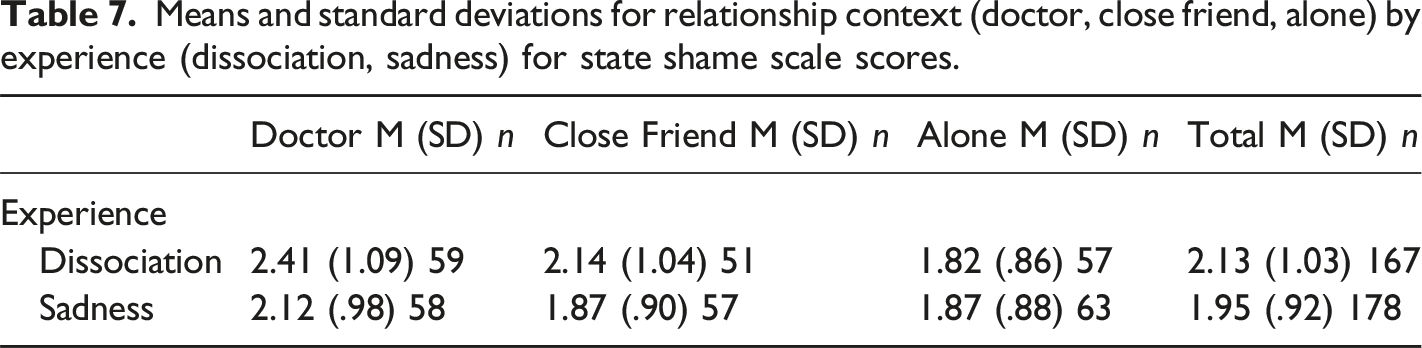
State Shame
Means and standard deviations for relationship context (doctor, close friend, alone) by experience (dissociation, sadness) for state shame scale scores.
Behavioral Responses
Means and standard deviations for relationship context (doctor, close friend, alone) by experience (dissociation, sadness) for the seven behavioral responses.
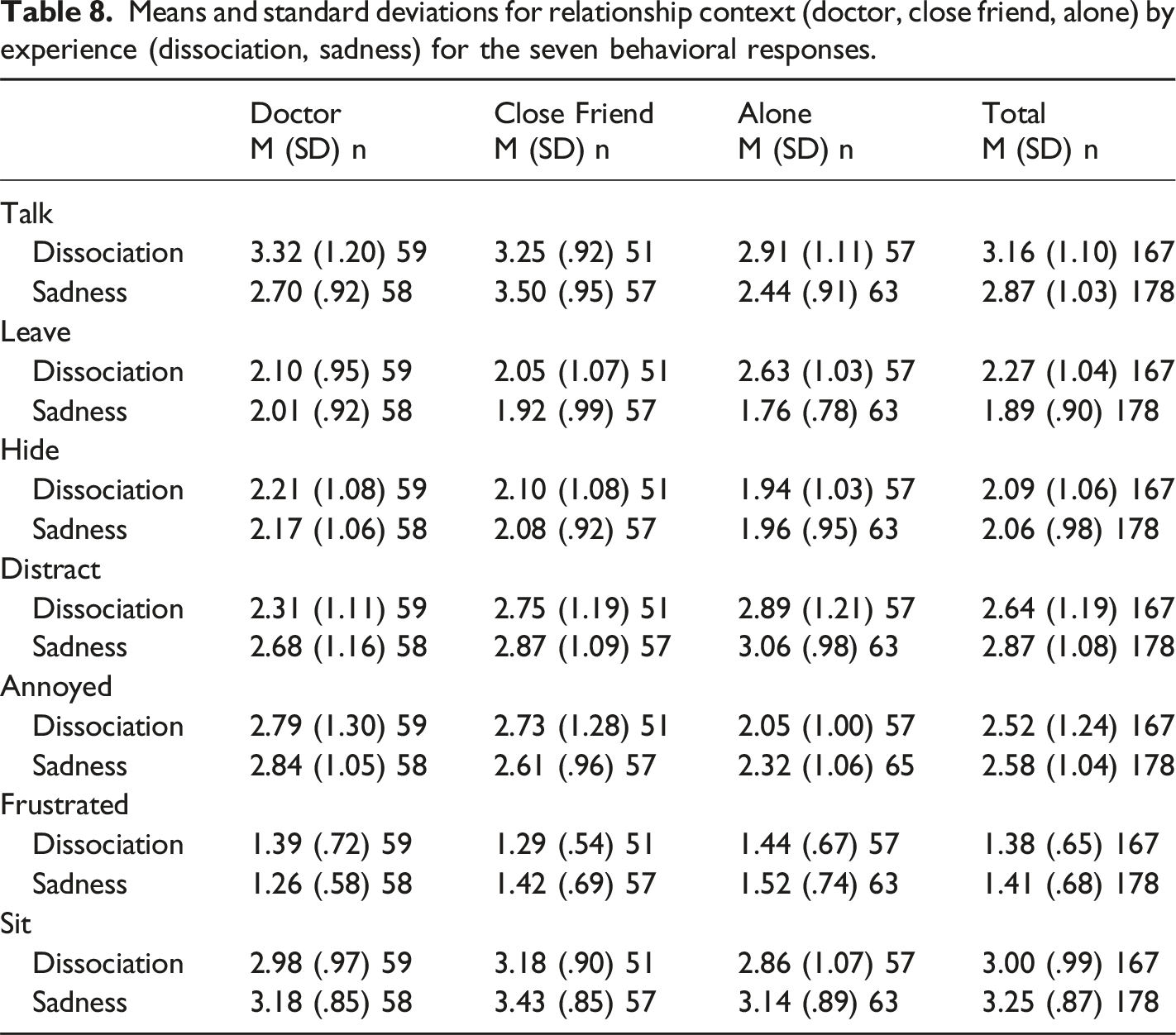
For Experience, in the dissociation compared to the sadness condition participants reported a greater desire to talk, F (1, 338) = 6.43, p = .01, η2p = .02, and leave, F (1, 338) = 15.56, p < .001, η2p = .04. Wanting to sit was elevated when experiencing sadness compared to dissociation, F (1, 338) = 6.30, p = .01, η2p = .02. For Relationship Context, ANOVA showed significant ratings for talk, F (2, 338) = 13.66, p < .001, η2p = .08, distract, F (2, 338) = 10.51, p < .001, η2p = .06, annoyed, F (2, 338) = 9.72, p < .001, η2p = .05 and sit, F (2, 338) = 3.10, p = .046, η2p = .02. There was a trend towards significance for frustrated, F (2, 338) = 2.73, p = .07, η2p = .02. Post-hoc analysis with trait shame controlled showed that, regardless of the experience, participants were more likely to want to talk when with a close friend than when alone, F (1, 225) = 29.51, p < .001, η2p = .12, or with their doctor, F (1, 222) = 7.65, p = .006, η2p = .03. They had a greater desire to talk when dissociation or sadness were experienced with their doctor than when alone, F (1, 234) = 5.08, p = .03, η2p = .02. There was less of a desire to distract attention away from the experience when with a doctor compared to when alone, F (1, 234) = 19.08, p < .001, η2p = .08, or with a close friend, F (1, 222) = 10.35, p = .001, η2p = .05, with the latter two not differing, F (1, 225) = 1.15, p = .29, η2p = .005. For getting annoyed at oneself for having the experience, significantly higher ratings were found when with a doctor, F (1, 234) = 12.19, p = .001, η2p = .05, and close friend, F (1, 225) = 18.46, p < .001, η2p = .08, compared to when alone. The doctor and close friend contexts did not differ, F (1, 222) = .18, p = .67, η2p = .001. Participants experiencing dissociation or sadness had a greater desire to sit calmly with a close friend than when alone, F (1, 225) = 5.93, p = .02, η2p = .03. There was no difference when with a doctor compared to when alone, F (1, 234) = .44, p = .51, η2p = .002, or with a close friend, F (1, 222) = 2.75, p = .10, η2p = .01. The trend for frustration at another was produced by lower scores when with a doctor than alone, F (1, 234) = 5.16, p = .02, η2p = .02, with no differences between close friend and either alone, F (1, 225) = 1.69, p = .20, η2p = .007, or with a doctor, F (1, 222) = .59, p = .44, η2p = .003. In short, when experiencing dissociation and sadness when alone, with a close friend or with their doctor, participants were more likely to talk to a close friend, distract when alone or with a close friend, get annoyed with themselves when with another (i.e., doctor or close friend) and sit calmly with a close friend.
For the interaction, significant results were evident for talk, F (2, 338) = 5.89, p = .003, η2p = .03, and leave, F (2, 338) = 6.59, p = .002, η2p = .04. Post-hoc analysis controlling for trait shame showed that wanting to talk about the experience was significantly higher when dissociating than when sad in the presence of a doctor, F (1, 114) = 10.95, p = .001, η2p = .09, and when alone, F (1, 117) = 6.17, p = .01, η2p = .05. In contrast, when with a close friend, there was no difference in a desire to talk when experiencing dissociation or sadness, F (1, 105) = 2.07, p = .15, η2p = .02. Regarding the desire to leave the context they were in, participants reported significantly higher ratings when dissociating compared to being sad when alone, F (1, 117) = 31.83, p < .001, η2p = .21. No differences for a desire to leave were found across experiences in the close friend, F (1, 105) = .70, p = .41, η2p = .007, and doctor, F (1, 114) = .41, p = .52, η2p = .040, contexts.
Discussion
Findings supported the first hypothesis with elevated feelings of shame for dissociative compared to sadness experiences, when assessed on both single item and state shame measures, despite those in the dissociation experience reporting more comfort sharing personal information with a doctor or close friend. Thus, results were more unequivocal than in Study 1 where only the state shame measure produced this result, and demonstrate that even when individuals report a degree of comfort sharing personal experiences, dissociation elevates shame feelings. This further supports dissociation as shame-inducing, perhaps on account of the alienation and loss of control it brings. Replicating Study 1, anxiety was also elevated in the dissociation experience, as was surprise, suggesting shame was not a unique emotional response to dissociation and speaks to the emotional storm dissociative experiences usher forth. The sense of experiencing a loss of control with dissociation may be particularly triggering of not only shame but also anxiety and surprise.
Regardless of whether participants were exposed to dissociation or sadness, shame scores were elevated on the single item measure when with a doctor or close friend compared to when alone, and strongly trended in this same direction for the state shame measure (i.e., p = .06). These findings suggest more intimate contexts may be relevant to reactive shame following dissociative or emotional experiences, perhaps because they heighten risk of being viewed as inferior or being rejected. The second hypothesis of heightened shame when dissociating in the presence of a close friend or doctor compared to when alone speaks more closely to this issue and was supported using the single item shame measure. The state shame measure showed only a modest trend towards elevated shame when dissociation occurred in more intimate contexts (p = .09). The findings suggest some evidence that intimate relationships, whether in the form of an emotionally (friend) or professionally (doctor) close other, are associated with feelings of shame upon experiencing dissociation compared to sadness. McKeogh et al. (2018) found higher reports of single item shame and state shame when dissociation compared to sadness occurred with a close friend. There was no difference across experiences in the less intimate contexts of being with an acquaintance or alone. Intimacy may further heighten the relationship between shame and dissociation, and thereby have a regulating effect on it, such that greater intimacy strengthens the connection (where dissociation may heighten the risk of rupture in meaningful relationships leading to shame) and less intimacy reduces it (where dissociation has less severe relational consequences).
With reference to shame explanations, as seen in Study 1, regardless of the relationship context, the shame of dissociating was associated with several different explanations: Feeling flawed in some way, having a loss of control over oneself, feeling isolated and excluded from what was happening inside and around them, and that others would think badly of them if they knew what they were experiencing and being judged. Feeling exposed and judged were more likely given as explanations for shame while dissociating or feeling sadness in the close friend and doctor contexts than when alone. While feeling excluded and thought badly of was elevated in the doctor versus close friend condition. In short, the context involving personal and professional relationships drew on different explanations for shame, where being excluded/rejected and thought badly of were particularly pertinent when in a relationship associated with seeking expertise for one’s health.
Turning to behavioral responses, regardless of relationship context, when dissociation was experienced, participants had a greater desire to talk about it. This was especially the case when with a doctor or alone, suggesting a sense that in these contexts the feelings associated with dissociation could be helpfully addressed through sharing one’s experience with a doctor, or another person when it occurs alone. However, there was also a greater desire to leave the context where dissociation compared to sadness occurred. The seemingly opposing desires to leave and talk in the presence of dissociation-related feelings like shame, suggests either individual differences in responding or some conflict about whether to reduce the feelings associated with dissociation by taking the risk of sharing in order to unburden oneself, or dealing with them outside the relational context by exiting it. Trait shame was controlled in these analyses, so other variables may determine the path a person takes if faced with that internal dilemma (e.g., relational dynamics in the moment, including immediate personal comfort; intensity of state feelings and the capacity to tolerate them so sharing can be facilitated). Regardless of whether experiencing dissociation or sadness, compared to when alone participants reported a greater desire to sit and talk with a close friend while also feeling annoyed at themselves for having such experiences. These seemingly dissimilar responses speak again to possible individual differences or the internal response conflict that dissociation- and sadness-related feelings bring.
Regarding the contextual findings of wanting to talk in the presence of a close friend about dissociation or sadness experiences, or talk to a doctor more pressingly for dissociation than sadness experiences, these contexts also heightened state shame. Thus, being in these relational contexts not only activated shame, but also came with a preference to talk about the experience. Indeed, McKeogh et al. (2018) found experiencing either dissociation or sadness when in the presence of a close friend evoked shame and brought forth the desire of wanting to have a discussion about the occurrence. This is consistent with DeYoung’s (2015) view that interpersonal engagements can both activate shame feelings and also heal them. A desire to leave the room when dissociation occurs alone, may reflect an adaptive withdrawal response in the absence of other effective ways to manage the experience.
In sum, dissociation heightened shame when assessed by the single-item and state shame measures, and using the single item measure dissociative experiences increased feelings of shame comparative to sadness experiences when with a close friend and doctor. Further, when both sadness and dissociation were experienced in the presence of a doctor or close friend, it elevated shame feelings on the single-item instrument compared to being alone. In short, these findings support shame as a response to dissociative experience and highlight the potential importance of an intimate relational context in increasing the link between dissociation and shame. Being in an interpersonal engagement with either a more emotionally (close friend) or professionally (doctor) connected other may amplify the shame associated with experiencing dissociation, at least when measured with a single shame item.
General Discussion
Using similar samples sizes, both studies showed strong though not wholly consistent evidence that exposure to a dissociation vignette elevated shame. In Study 1, the more psychometrically sound state shame measure showed this results, but not the single item measure. In Study 2, both single item and state shame scale measures indicated elevations in shame when exposed to dissociation versus sadness vignettes. Thus, shame does appear generally associated with dissociative experience, rather than dependent on the presence of another or the level of intimacy in that connection as McKeogh et al. (2018) proposed. However, there may be some variation depending on how it is measured, with the state shame tool showing consistent elevations in the dissociation compared to sadness experience in both studies, but the single item measure showing this pattern only in Study 2. The single item measure used the word “shame,” so draws on a predominantly cognitive understanding of what this term means for each individual and thus draws on their willingness to directly identify with it (DeYoung, 2015). The state shame measure is more visceral, asking participants to determine whether they are experiencing the desire to disappear or are feeling small, worthless or disgraced. Thus, it is more experiential in nature.
It has been noted that hearing the word “shame” connected with one’s own experience can be shaming in and of itself (e.g., DeYoung, 2015; Herman, 2011). In this regard, scores on the single item measure in Study 1, especially for dissociation, were lower compared to Study 2, which may suggest participants were less willing to identify explicitly with the term “shame” when with a therapist (e.g., dissociation in Study 1 for new and old therapist merged = 2.28 vs. Study 2 for doctor and close friend merged = 2.84). The alone context in study’s 1 and 2 showed little difference (e.g., dissociation Study 1 = 1.85 vs. Study 2 = 1.68), nor did the state shame scale (dissociation in Study 1 new and old therapist merged = 2.18 vs. Study 2 merged doctor and close friend = 2.28). Thus, one explanation for no effect between dissociation and sadness on the single item measure in Study 1 was participants were reluctant to identify too strongly with the term “shame” after experiencing dissociation with an old or new therapist, even though it was experientially felt, as evident in state shame scale scores. Thus, while both studies 1 and 2 showed evidence for shame being heightened in the dissociation vignette compared to the sadness vignette, the state shame measure, which does not explicitly mention shame, is not impacted on by any effect direct exposure to the term “shame” may have on responding.
Despite evidence that shame was elevated with imagining experiencing dissociation compared to sadness, indications of a contextual effect were somewhat more equivocal. Four interaction analyses across both studies (one for single item shame and one for state shame in each study) assessed if shame was elevated with dissociation compared to sadness in more intimate contexts. Only one interaction, single item shame in Study 2, showed significant results. Here, as hypothesized, increased shame was evident in the dissociation experience compared to the sadness experience in the doctor and close friend contexts, but not when alone. The other three interactions failed to show that shame was more related to dissociation than sadness in the interpersonal versus alone contexts. McKeogh et al. (2018) found more consistent findings with higher single item and state shame scores in the dissociation compared to sadness experience when with a close friend, but not when with an acquaintance or alone.
The current studies anticipated a greater felt sense of intimacy in Study 2 because most participants had the experience of seeing a doctor or having a close friend, which was not the case in Study 1, where new and old therapists were used. Thus, the results seem consistent with McKeogh et al. (2018) that increased intimacy may be a moderating factor in elevating shame associated with dissociation, and again the close friend context produced heightened dissociation-related shame, at least on the single item measure. Yet, Dorahy et al. (2021) found no evidence that relationship context produced different associations between shame and dissociation, with elevated shame in the dissociation condition regardless of whether the person was alone or with another. However, whilst this study induced dissociation it only asked participants at the start of the procedure to remember times when dissociation occurred with a close friend or when alone. After this, the induction was initiated and no further mention was made of the relationship situation. Thus, it was not a sensitive assessment of the relationship context hypothesis. There is some suggestion in the current findings that dissociation-related shame is further heightened in intimate relationships, as McKeogh et al. (2018) noted. The presence of another, especially someone with more emotional ties, when dissociation is experienced, may expose aspects about oneself wished to remain hidden and heighten fears of unacceptability or rejection. Future work needs to examine if heightened intimacy moderates the relationship between dissociation being experienced and shame rising. This might include manipulating the nature of intimacy and the degree to which it brings safety and security. The impact of intimacy on the relationship between shame and dissociation may differ in those with and without a relational trauma history (Platt et al., 2017), and this requires further exploration.
Contexts with greater intimacy did seem to be related to shame when experiencing dissociation or sadness. Two of the four analyses examining changes in shame across relational context regardless of experience found elevated shame when with another compared to when alone, while a third trended in that direction. The single item measure in both studies showed less shame in the alone condition compared to the two relational contexts (Study 1 new and old therapist; Study 2 doctor and close friend). The trended state shame measure in Study 2 was significantly higher for doctor over being alone when dissociation or sadness were experienced, and fell marginally short of significance for close friend than when alone. It seems intimacy may heighten shame when displays of sadness or dissociation are evident.
Participants in Study 2 generally said they felt comfortable sharing personal information with their doctor or close friend, despite still responding that they would feel ashamed when experiencing dissociation in those relationships. Sharing personal information and having a dissociative symptom may reflect two different classes of experience, the former being more under the agency of the person (e.g., what is shared and what is not), the latter seemingly more uncontrollable. Participants reported a loss of control being the most predominant reason for feeling ashamed when dissociation was experienced, followed by feeling flawed and exposed. Loss of control was also the highest rated reason for shame following dissociation in Study 1. Yet, Dorahy et al. (2021) found an appraisal of being flawed was given as the predominant account for why dissociation leads to shame. Loss of control, exposure and perceiving oneself as flawed are dominant cognitions associated with shame (Garfinkle, 2012; Gilbert, 2000; Nathanson, 1992), and seemingly intimately connected with dissociation.
Anxiety was consistently associated with dissociation across studies, which was also evident in other work (e.g., McKeogh et al., 2018). Anxiety and self-conscious emotions such as shame do not occur in isolation (Gilbert and Andrews, 1998; Polivy, 1981), and in fact, share many similarities (e.g., fearing exposure or negative evaluation; Gilbert, 2000). Thus experiences like dissociation that activate shame are also likely to activate anxiety. Moreover, anxiety is considered a reaction to internal or external threat (Nathanson, 1992; Shill, 2004), with the loss of control, and sense of being flawed or exposed associated with dissociation in these studies creating that threat. Future work should investigate whether shared and unique pathways link dissociation to both shame and anxiety.
Results from the behavioral responses show some variation across studies and conditions, but desiring to talk or to leave were often associated with dissociation. The desire to leave is a withdrawal behavior designed to reduce elevated distress (e.g., shame) by vacating the situation where that distress is felt (Elison et al., 2006; Nathanson, 1992). In opposition to leaving, the desire to talk about the experience is an approach behavior. A growing body of literature shows that if damage to the self created by shame can be overcome, approach behaviors will be desired and that participants in research studies of healthy adults preferred to be with another rather than alone upon experiencing shame (e.g., De Hooge et al., 2018; De Hooge et al., 2010). DeYoung (2015) argues that responding to shame in a manner that seems most natural (e.g., hiding from the experience) is also considered to be one of the most toxic, with the person’s least likely response (e.g., allowing the shame to be exposed) also being ultimately the most healing. As she notes, “shame needs light and air” for healing (p. 116). Indeed, when investigating the usefulness of therapists’ responses to disclosures of shame, participants from clinical and non-clinical samples favor approaching rather than avoiding shame feelings (Dorahy et al., 2015; Dorahy et al., 2017).
Taken together, the findings have implications. First, therapists should be aware that dissociative experiences (and also to a lesser extent sadness experiences) have the propensity to activate shame, which may be elevated in more intimate contexts. Appraisals associated with this link, like feeling flawed, exposed and out of control can be explored and reappraised. In addition, the competing desires to leave and want to talk about dissociation-related shame may be present, such that psycho-education and increasing tolerance to avoid leaving may assist soothing via interpersonal connection which builds the therapeutic relationship more broadly (DeYoung, 2015).
Both studies had several limitations. First, it remains uncertain how generalizable the results are. Both studies used crowd sourcing platforms to recruit participants and while they are more diverse than other sampling methods like the use of college students (Buhrmester et al., 2011), they still represent a distinct group (i.e., those registered on the platform) that may differ from the general population. In addition, experiences of dissociation were created in the form of vignettes where participant were asked to imagine having the experience as opposed to experientially having dissociative experiences. But the findings were generally consistent with a study where dissociation was induced (Dorahy et al., 2021). The samples were non-clinical, thus replicating the findings in individuals attending therapy for dissociation would add strength to the current body of research examining the relationship between shame and dissociation.
Conclusions
Collectively, the current studies support the theory that dissociative experiences give rise to acute shame feelings (Platt et al., 2017). More tentative evidence was found for this relationship being elevated in contexts where intimacy was most heightened (i.e., doctor, close friend), suggesting intimacy may modulate the connection between dissociation and shame. Thus, the relationship between dissociation and shame may be influence by the context the person is in, and possibly their own history of relational trauma. Appraisals about dissociation signifying a loss of control or a sense of oneself as flawed or exposed seem to be associated with elevated shame. There now exists a growing body of evidence supporting the bi-directional relationship between dissociation and shame, where shame seems to trigger dissociation, and dissociation (potentially regulated by intimacy) seems to produce elevated shame feelings (Benau, 2022; Dorahy et al., 2017; McKeogh et al., 2018).
Supplemental Material
Supplemental material - The Impact of Relationship Context on Dissociation-Induced Shame Using Vignette Scenarios
Supplemental Material for The Impact of Relationship Context on Dissociation-Induced Shame Using Vignette Scenarios by Martin J. Dorahy , Kate McKeogh and Kumar in Psychological Reports.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.