
Abstract
In spite of the importance of emotion regulation for nurses’ well-being, little is known about which strategies nurses habitually use, how these strategies combine in order to regulate their emotional distress, and how these are related to their caregiving orientations. The current study aimed to explore the emotion regulation repertoires that characterize health-care providers and to investigate the association between these repertoires and caregiving orientations in a sample of nurses. Firstly, a confirmatory factor analyses was run to test the suitability of the Regulation of Emotion System Survey for the assessment of six emotion regulation strategies among health-care providers. Subsequently, the latent profiles analysis was employed to explore emotion regulation repertoires. Three repertoires emerged: The Average, the Suppression Propensity and the Engagement Propensity profiles. The participants of the last two groups relied on Expressive Suppression and Engagement, respectively, more often than others. Nurses were more likely to be placed within the Engagement Propensity group when compared to the first responders, and higher levels of hyperactivation of the Caregiving System were associated with this repertoire. A greater reliance on Expressive Engagement among nurses was discussed in terms of the fact that nurses usually have a longer and more care-oriented relationships with patients than first responders.
“Care is both a practice and a disposition”
[Tronto, J. C. (1993). Moral boundaries: A political argument for an ethic of care. New York, NY: Routledge, p. 132].
Introduction
The ability to regulate negative emotions that arise from exposure to the suffering of others is at the core of caring. Indeed, it is only through the regulation of unpleasant feelings (i.e., emotional distress) that individuals can effectively take care of someone who is in pain or is suffering. Most attempts at modifying individual feelings requires significant costs (in terms of physical and/or psychological energy; Suri et al., 2015), especially when these attempts are frequently demanded and the subject has to face intense emotional arousal. Therefore, the consistent need to regulate emotions in response to the distress elicited by the physical and emotional suffering of others may have consequences for caregivers.
The work of many health-care providers involves frequent and recurring exposure to patients’ physical and emotional pain, trauma, and even death (Watson, 1997). In addition, in the case of nurses compared to other health-care providers (e.g., first responders), the relationships with patients are more care-oriented and last a long time. This often results in compassion fatigue (Figley, 1995), which, related to nurses’ job, was defined by Joinson (1992) as a feeling of deep sympathy and sorrow for another who is stricken by suffering or misfortune, accompanied by a strong desire to alleviate their pain or remove its cause. Bearing witness to these difficult situations requires the implementation of strategies for regulating emotional distress. As a consequence, any nurse who wants to take care of their patients, needs to integrate his/her technological/technical competencies with “ontological caring competencies” (Watson, 1997, p. 50) that means focusing on the ability to be present, to be reflective, to attend to mutuality of being and centering one’s consciousness and intentionality towards caring, healing, wholeness and health. These competencies require the ability to regulate emotions and develop effective repertoires of emotion regulation strategies. Indeed, the ability to regulate emotions seems to characterize a nurse’s job more than other work roles (Kovács et al., 2010) as a consequence of some facets of nurse-patient relationship (i.e., an empathic, more care-oriented and often prolonged relationship with patients that involves multiple interactions). However, at the expense of these professionals’ well-being, the ways that nurses typically regulate their distress is a subject that is still underexplored. Very little is known about the emotion regulation strategies that they habitually use, how these strategies might co-occur, their effectiveness to regulate unpleasant feelings, and how their use relates to nurses’ caregiving orientations (i.e., preferred individual modalities in the functioning of the Caregiving System). In this study, the emotion regulation repertoires of a large group of healthcare professionals were analyzed, focusing on how emotion regulation strategies are associated with the caregiving orientation of nurses.
Background
The Tendency to Care for Others: The Caregiving System
According to Bowlby (1969/1982), the propensity of human beings to care for others is governed by an inborn behavioral system, the Caregiving System. This system is what motivates the caregiver to provide help and care to those who are in a state of difficulty and suffering, and presumably emerged over the course of evolution because it increased humans’ inclusive fitness. While the Caregiving System may have initially promoted the provision of care for others with whom the subject was closely related, today, through the cultural and educational elaboration of caregiving tendencies, it may be activated by genuine concern for anyone in need (Shaver et al., 2010).
Individual differences in the functioning of the Caregiving System depend on a person’s previous experiences with his/her attachment figure during infancy (Bowlby, 1969/1982). Indeed, repeated security-restoring and security-enhancing experiences with attachment figures, what Mikulincer and Shaver (2016) called a “broaden-and-build” cycle of security, favour the development of an optimal Caregiving System functioning in adulthood (Colledani et al., 2021). Throughout life, the mental representations of care are progressively defined starting from these subjective experiences (Shaver et al., 2010; Mikulincer & Shaver, 2016). If caregiving works adequately, individuals develop a positive image of themselves and others, which strengthens the trust in the Caregiving System (i.e., they feel empathic concern for others in need). In these situations, individuals perceive themselves as effective caregivers and others as worthy of help and consideration. On the contrary, recurring failures in providing adequate assistance to others may cause discomfort and negative mental representations of themselves and others (Mikulincer & Shaver, 2016). This frequently occurs for people with anxious or avoidant attachment orientations who, having serious difficulties identifying others’ emotions (Mikulincer & Shaver, 2019), often rely on inadequate distress regulation. For instance, attachment anxiety and attachment-related avoidance orientations often lead the insecure person to put in place inadequate distress regulation processes (Mikulincer & Shaver, 2019). For example, individuals with a preoccupied or anxious-ambivalent attachment orientation show upregulation of negative emotions in some contexts (Tamir, 2016). Conversely, avoidant people may experience reduced sensitivity and responsiveness, which can increase the risk of providing non-effective care.
The goal of the Caregiving System is to reduce other people’s suffering, protect them from harm, and foster their growth and development (Mikulincer & Shaver, 2016). Its activation transforms the person into an attachment figure and motivates him/her to provide protection, proximity, and security. There are two categories of situations that activate the system: 1) when the other is in a state of need, stress, or danger and needs help; 2) when the other has exploration/growth opportunities but needs help to do so. In either case, once the Caregiving System is activated (whether appropriately or not), the caregiver relies on a repertoire of behaviors aimed at restoring or enhancing the other person’s welfare. This implies: a) the suspension or postponement of actions aimed at achieving personal goals to synchronize and coordinate one’s behavior with that of the person in need; b) knowledge of how to develop appropriate action plans for the solution of the problem; and c) the ability to deprioritize any individual priorities and interfering actions or feelings. In sum, the Caregiving System activation requires empathy, sensitivity, and responsiveness to others’ needs and, consequently, the ability to regulate distress that is elicited by dealing with another person’s suffering.
As described above, the Caregiving System can be optimally activated (using optimal or primary modality) or can be activated in two non-optimal ways (secondary modalities, i.e., hyperactivation and deactivation). In the first case (optimal activation), helpers perceive themselves as effective caregivers and others as worthy of help, and this strengthens their trust in the system. However, distress-eliciting mental events may lead individuals to think that the primary modality of the Caregiving System should be substituted by one of the secondary modalities (Shaver et al., 2010). In the case of anxious hyperactivation (secondary modality), the caregiver insists on providing care at all costs, intensifying his/her efforts that are intrusive, anxious, and poorly timed. He/she is motivated by the desire of feeling competent and admirable as a caregiver, and forces the needy person to accept help even if it is not required or not provided in a sensitive way. These efforts are perceived by the person in need as controlling and the caregiver is experienced as intrusive or aggressive. The other secondary modality implies the avoidant deactivation of the Caregiving System to prevent the caregiver from suffering from anxiety and frustration resulting from failing to provide effective care. When escaping from the role of caregivers is not possible, deactivated caregiving orientation involves the tendency to provide only uncertain assistance, and emotional distance from people seeking for care and comfort. As a consequence, a caregiver’s efforts are drastically reduced and sensitivity and responsiveness to the needs of others are inhibited. If the individual experiences systematic failures in attaining the goals of the Caregiving System and consistently uses one of the secondary modalities, he/she could develop a recurrent tendency (i.e., personal caregiving orientation) to hyperactivating and deactivating the system.
Overall, it can be assumed that the Caregiving System functioning is associated with the caregiver’s regulatory efforts and individual differences in the Caregiving System orientations (anxious/intrusive caregivers and avoidant caregivers) may influence the type of emotion regulation strategies that people use to regulate the generation, experience, and expression of their negative emotions arising from the relationships with suffering others. For instance, the deactivation of the Caregiving System may lead a nurse to dismiss from relationships and to reduce his/her expression of care and feelings. On the contrary, a hyperactivated orientation of the Caregiving System may predispose a nurse to be excessively distressed by the relationships with his/her patients and the resulting distress may be associated with difficulties in regulating his/her negative emotional reactions. In both cases, the functioning of the system takes shape as the nurse manages the relationship and this, together with his/her ways to regulate emotions, may help to explain the potential failure of caring in job distressing situations.
The Regulation of Negative Emotions
“Emotion regulation refers to shaping which emotions one has, when one has them and how one experiences or expresses these emotions” (Gross, 2014, p. 6). People may regulate their emotions to attenuate, maintain, amplify, or change them, depending on their goals. Interest and knowledge of emotion regulation have grown exponentially in the last 20 years (Gross, 2014). This growing interest is due to the fact that emotions and their regulation processes are essential elements of each human relationship. Currently, competent emotion regulation is recognized as a fundamental component of well-being and optimal psychological and social functioning. On the contrary, difficulties in emotion regulation have been identified as a key factor in the development and maintenance of many psychological disorders (Aldao et al., 2015).
While the downregulation of negative emotions is not the sole purpose of emotion regulation (Tamir, 2016), researchers have especially investigated the strategies that people use in a deliberate way to diminish unpleasant emotional arousals due to the strong associations between negative emotion dysregulation and mental health symptoms or reduced well-being (Aldao et al., 2010). Emotion regulation strategies are commonly divided into two separate groups: theoretically “more adaptive” and “less adaptive” strategies. However, mounting evidence has shown that each emotion regulation strategy is not “good” or “bad” in itself, but may be more or less successful, depending on the tendency to rely on a given strategy in proportion to other strategies and depending on the circumstances (De France & Hollenstein, 2017; 2019; Lougheed & Hollenstein, 2012). For example, reappraisal (i.e., a positive re-evaluation of a negative situation) may help the person to face his/her negative feeling; however, a heavy reliance on reappraisal in the face of controllable events may also prevent individuals from taking actions to modify the situation. Thus, using one “adaptive” strategy all the time is not as beneficial as having a wide range of strategies (i.e., a repertoire) to apply as needed to fit the situation (Aldao et al., 2010; Bonanno et al., 2004).
Emotion regulation repertoires are “the range of emotion regulation strategies an individual employs, and the proportional degree to which they rely on them” (De France & Hollenstein, 2017, p. 204). A limited emotion regulation repertoire is a risk factor for experiencing difficulties in individual functioning (Adao et al., 2015; Bonanno & Burton, 2013). Conversely, a broad emotion regulation repertoire, is associated with fewer mental health difficulties (Aldao et al., 2010; De France & Hollenstein, 2017; 2019; Lougheed & Hollenstein, 2012). In summary, it can be expected that a broad repertoire and a flexible use of emotion regulation modalities are, for nurses, crucial to coping effectively with their distressing work conditions.
Nurses and the Regulation of Caregiver’s Distress
Nursing is a stressful profession that constantly requires coping with high cognitive, physical, and emotional demands. Research on various samples of nurses has highlighted that prolonged exposure to these demands is associated with stress, burnout, and compassion fatigue (Hunt et al., 2017). Nevertheless, caring for patients is a source of challenge, satisfaction, and motivation (Morgan & Lynn, 2009), since some positive outcomes (e.g., work engagement, creativity, work motivation) have been observed only when emotional demands are high (Bakker & Sanz-Vergel, 2013; De Jonge et al., 2008) and when these demands are associated with more competent emotion regulation abilities (Donoso et al., 2015; Mauno et al., 2016). For example, while the ability to empathize is fundamental for nurses, an empathic response to suffering can result in emotional distress. These feelings can be alleviated by different behaviors, such as helping or escaping the situation (Mikulincer & Shaver, 2016), that in turn are associated with individual differences in well-being (Hunt et al., 2017). Thus, nurses need emotion regulation skills that allow them to respond effectively to the emotional distress that arises from their relationships with suffering patients.
Few studies thus far have analysed the emotion regulation strategies that health-care providers (nurses in particular) use in regulating their negative emotions. These few studies have mainly focused on the association between organizational factors and emotion regulation. For example, Bamonti et al. (2019) investigated health care workers’ levels of burnout and the emotion regulation strategies associated with them. From the theoretical perspective of emotional labour (Delgado et al., 2017), some studies have also focused on the interaction between the attempts of nurses to regulate emotions at work, work engagement and job satisfaction (Djediat et al., 2020).
The study
The present study explores these topics by investigating the emotion regulation repertoires that relate to caring relationships, focusing on two groups of people (first responders and nurses) who, for their work or voluntary activities, frequently interact with individuals who are suffering (i.e., who are in physical and emotional pain). Specifically, this study considers whether the emotion regulation repertoires that these health-care providers rely on may vary depending on the features of the relationships with suffering patients that characterize their work. On the one hand, we assessed emotion regulation repertoires in voluntary first responders whose service implies time-limited and technical interactions with suffering people, mostly in emergency situations. On the other hand, emotion regulation repertoires and caregiving orientations were assessed in nurses for whom “the caring” is the core of their job. Reliance on six conscious self-reported strategies, included in the Regulation of Emotion System Survey (RESS) by De France and Hollenstein (2017) has been measured. Three of these have directly impact the cognitive component of emotion: Distraction (the withdraw of one’s attention away from the emotional situation), Rumination (a pervasive focus on an emotional experience, its causes and consequences) and Reappraisal (an alteration of the emotional experience by changing the thoughts about it). Two strategies included in the RESS directly impact the behavioral component of emotion: Expressive Suppression (active attempts to eliminate the behavioral manifestation of an emotional experience) and Expressive Engagement, (amplifying expression). Finally, the sixth strategy impacts the physiological arousal component of emotion: Arousal Control (De France & Hollenstein, 2017).
The differences in the ways people behave in response to requests for support and care from others may depend on the personal modalities to regulate emotional distress, but also on the individual dispositional level of activation of the Caregiving System, which in turn is shaped by personal experiences in caring situations. Individuals with a hyperactivated caregiving orientation tend to engage to a higher extent in the relationships with suffering others and this may lead them, even though they may feel more intense distress, to try to regulate it by means of more active and less avoidant emotion regulation strategies. Thus, assuming that the individual orientation of the Caregiving System may affect personal use of and reliance on some strategies rather than others, we investigated in the nurses who took part in this study their caregiving orientations and tested how these relate to emotion regulation repertoire differences. We focused on nurses since, in work situations, they are usually called to engage in long and less occasional caring relationships than first responders who, as explained extensively above, have time-limited and “technical” interactions with suffering people.
Aims
We explored the suitability of the 24-item version of the Regulation of Emotion System Survey (RESS; De France & Hollenstein, 2017) for the assessment of emotion regulation strategies consciously used by health-care providers to regulate their negative emotions. As preliminary analyses, the factor structure of the scale and the reliability of its subscales were verified. Subsequently, Latent Profile Analyses (LPA) were used to identify the profiles that characterize the emotion regulation repertoires used by health-care providers. The latent profiles that emerged from the analysis were also analyzed in relation to gender, age classes, and professional role (first responders versus nurses). With reference to the professional roles, our expectation was that the profiles that entail greater engagement in the relationship would be more typical of nurses than of first responders. In fact, compared with first responders, who typically have time-limited and “technical” interactions with suffering people, nurses are involved in long lasting and care-oriented relationship with patients. Thus, taking into account the different demands of the two roles, we hypothesized that they had different ways to cope with them.
Moreover, we also explored among nurses how the different emotion regulation profiles interact with differences in caregiving orientations (i.e., hyperactivation and deactivation). We anticipated that those nurses who report higher scores in terms of hyperactivation of the Caregiving System, would be also those who rely more heavily on strategies indicative of greater engagement in the relationships.
Participants
A total of 462 health-care practitioners were recruited for the study through convenience sampling (Mean Age = 35.75; SD = 12.30); 61.38% were females. Four participants did not provide details concerning age and five concerning genders. Of the total participants, 212 were nurses (Mean Age = 39.22, SD =12.12; 80.1% were females) and 250 were first responders of a first-aid organization (Mean Age = 32.12, SD = 11.45; 44.7% were females).
Data Collection
The participants were recruited between November-December 2018. The nurses were contacted in various hospitals located in the North of Italy, whereas the first responders were approached through the organization they were part of. Questionnaires were distributed to participants in sealed envelopes, in collaboration with the human resources departments of their organizations. The envelopes included the questionnaire and an instruction letter, where it was explained that participation in the study was voluntary and anonymous. Participants were informed about the aim of the study, the duration of the task, and the possibility of withholding their consent to participate in the research without being penalized. Completed questionnaires were picked up in sealed envelopes by participants and returned to researchers.
All participants completed the Italian 24-item version of the RESS (Meneghini et al., 2019). The participants in the sample of nurses also filled out the Italian version of the Caregiving System Scale (CSS; Meneghini et al., 2015).
Materials and Procedure
The 24-item version of the RESS (Meneghini et al., 2019) was used to evaluate how frequently participants implemented six strategies commonly used to regulate negative emotions: Distraction, Rumination, Reappraisal, Expressive Suppression, Expressive Engagement, and Arousal Control (four items for each scale). The first three strategies mainly impact the cognitive components of the emotion. Expressive Suppression and Engagement directly affect the behavioral component. Finally, Arousal Control acts on the emotional experience by means of the autonomic arousal component. For each item, respondents are required to evaluate how often in their life they use the described strategy to moderate their negative feelings (e.g., “Keep busy” for Distraction; “Continually thinking about the event” for Rumination; “Thinking of alternate ways to see the situation” for Reappraisal; “Hiding feelings” for Suppression; “Telling others one’s own feelings” for Engagement; and “Slow heart rate and breathing” for Arousal Control). Answers were recorded on a five-point Likert scale ranging from 1 (never) to 5 (always).
The Italian version of the CSS (Meneghini et al., 2015) was used to investigate the caregiving orientations of the nurses who participated in this study (N = 212). The CSS includes twenty items aimed to assess the secondary strategies of the system. Ten items evaluate deactivation, and ten assess hyperactivation. The Deactivation scale (DE) is unidimensional and describes the inhibition of sensitivity and the tendency to exhibit emotional distance when someone seeks care and comfort (e.g., “I don’t often feel an urge to help others”). The Hyperactivation scale (HY) includes two different but related facets (Colledani et al., 2021): the first representing effortful, intrusive, and coercive attempts to help others (HY_Intrusive; four items; e.g., “I sometimes feel that I intrude too much while trying to help others”) and the second describing self-focused anxiety and distress related to worries about one’s ability to provide effective care and support (HY_Anxiety; six items; e.g., “I often worry about not being successful when I try to help others who need me”). Together, these two aspects of excessive activation of the Caregiving System can create a self-amplifying cycle of distress and awkwardness in trying to provide sensitive and responsive support, which augments worries about one’s ability to provide effective help and care. In filling out the questionnaire, respondents were required to focus on the way they usually (i.e., in working and non-working situations) feel, think, and behave when they provide help to others and to rate the extent to which each item is self-descriptive. Answers were recorded on a 7-point scale (4 was the mid-point), ranging from 1 (not at all) to 7 (very much). In the Italian context, the scale showed adequate psychometric characteristics (Meneghini et al., 2015).
Ethical Considerations
All ethical standards for research with human subjects were respected following the principles in the Declaration of Helsinki.
Data Analyses
The internal consistency of the six scales of the RESS was evaluated using composite reliability (CR). This index is conceptually similar to Cronbach’s α (i.e., it represents an estimate of true variance relative to total variance) but it is considered to be a better index of internal consistency (Raykov, 2001).
The factor structure of the scale was assessed by running a confirmatory factor analysis (CFA) using the Mplus7 package (Muthén & Muthén, 2012), and the robust maximum likelihood as the estimator (MLR; Muthén & Muthén, 2012). In the model, six factors were defined, each measured by four items. The goodness of fit of the model was evaluated using several fit indices: χ2, Standardized Root Mean Square Residual (SRMR), Comparative Fit Index (CFI), and Root Mean Square Error of Approximation (RMSEA). A solution fits the data well when χ2 is non-significant (p ≥ .05), SRMR values are less than .08, CFI indices close to .95 (.90 to .95 for reasonable fit), and RMSEA smaller than .06 (.06 to .08 for reasonable fit; Marsh et al., 2004). A-priori analysis recommended a minimum sample size of n = 200 to obtain adequate power in a model with 6 latent factors and 24 observed indicators (α < .05, effect size = .30, power = .90; see Soper, 2020). Missing data (.21%) were completely at random (MCAR; Little MCAR test χ2(250) = 280,777, p = .09) and were dealt with using Full Information Maximum Likelihood (FIML) in Mplus7 (Muthén & Muthén, 2012).
LPA was employed to explore latent profiles deriving from the scores in the six RESS scales. LPA is a person-centered approach that can be used to classify individuals into a series of groups that are defined by a similar pattern of scores in a set of variables (Collins & Lanza, 2010). The profiles that can be derived through this method represent a useful approach to evaluating the effects of individual differences in applied research since they give a holistic interpretation of individuality that allows for describing individuals better than through single dimensions (Ferguson & Hull, 2018).
In this work, mean scores of the six RESS scales were used to run seven models (with 1 to 7 latent classes). To identify the best-fitting model several statistics were used: Akaike Information Criterion (AIC; Akaike, 1973), Bayesian Information Criterion (BIC; Schwarz, 1978), Sample- Adjusted BIC (SABIC; Sclove, 1987), and Entropy. The latter ranges from zero to one and high values indicate a better fit. In contrast, for AIC, BIC, and SABIC, lower values are indicative of a better fit (Nylund et al., 2007). In the evaluation of models, two comparative tests were also considered: The Vuong–Lo–Mendell–Rubin likelihood ratio test (VLMR; Nylund et al., 2007) and the Lo–Mendell–Rubin likelihood ratio test (adjusted LMR; Lo et al., 2001). These tests compare adjacent models (with C latent classes and C – 1 classes). When the results of these tests are non-significant, this indicates preference of the more parsimonious model. According to the suggestions in the literature (Collins & Lanza, 2010), the interpretability of the solution was also taken into account to select the better solution.
The latent profiles that emerged from the six scales of the RESS were analyzed in relation to individual characteristics (i.e., gender, age classes, and professional role) through χ2 test and standardized residuals. In addition, for nurses, differences in the Caregiving System orientations between the different latent profiles were explored through one-way ANOVAs (with Bonferroni-corrected post-hoc pairwise comparisons).
Results
Reliability and Construct Validity of the RESS
Results of the Confirmatory Factor Analysis and Reliability Indices.
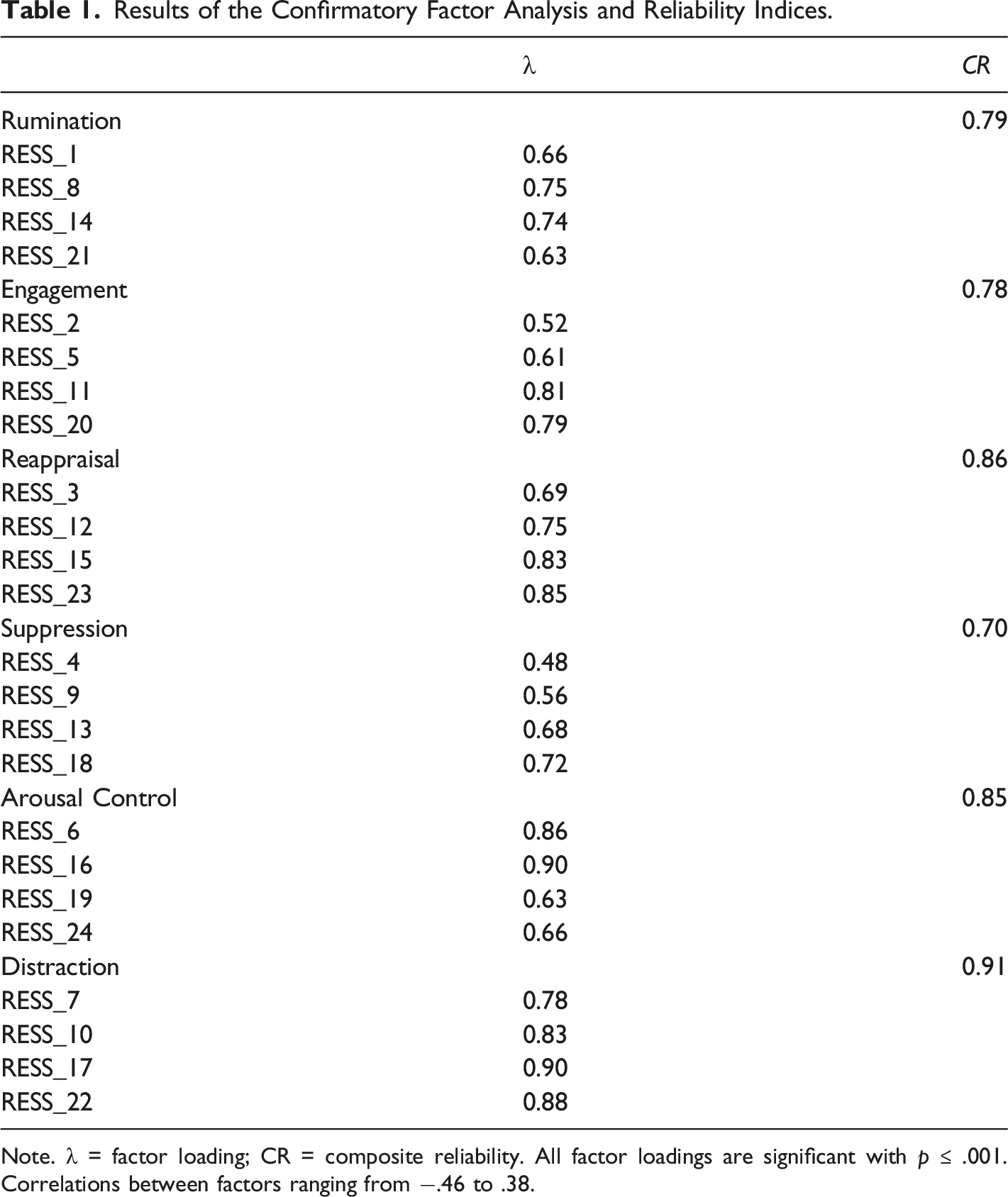
Note. λ = factor loading; CR = composite reliability. All factor loadings are significant with p ≤ .001. Correlations between factors ranging from −.46 to .38.
Emotion Regulation Repertoires and Work Roles
Fit Statistics for LPA Models with 1 to 7 Latent Classes.
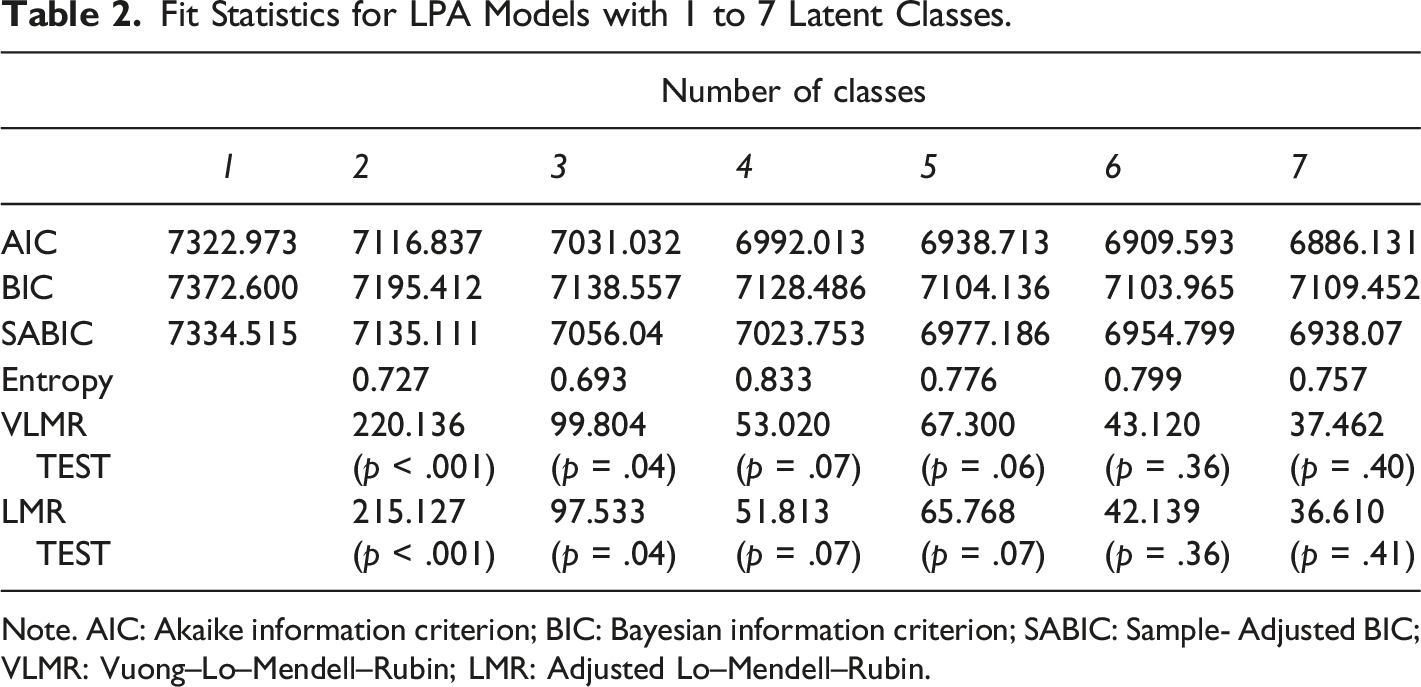
Note. AIC: Akaike information criterion; BIC: Bayesian information criterion; SABIC: Sample- Adjusted BIC; VLMR: Vuong–Lo–Mendell–Rubin; LMR: Adjusted Lo–Mendell–Rubin.
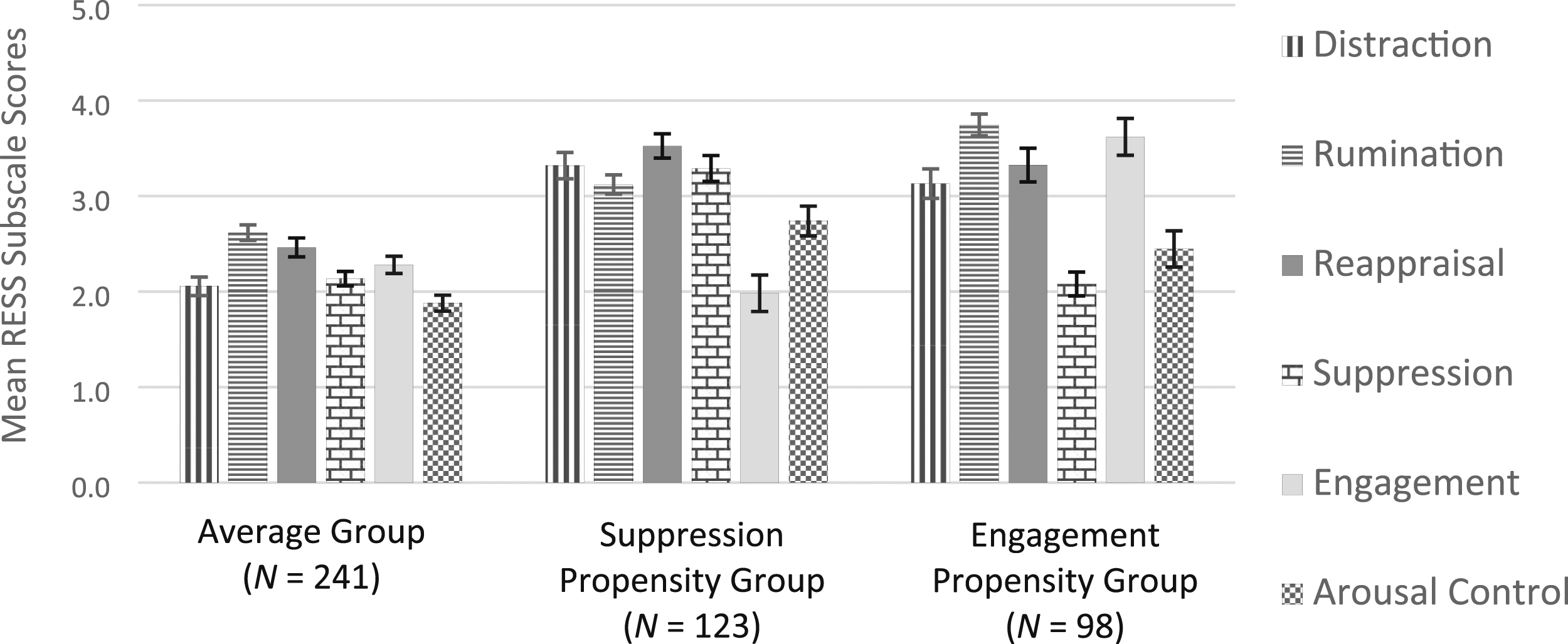
Figure 1 depicts the standardized mean scores on the six RESS scales for the participants belonging to the three classes, whereas Figure 2 displays the three profiles using the raw scale means to facilitate the interpretation of each group’s emotion regulation repertoire, i.e., it allows for identification of the relative frequencies of the six strategies assessed. Standardized mean scores in the six RESS scales for the three classes resulting from the Latent Profile Analyses. Raw scale means in the six RESS scales for the three classes resulting from the Latent Profile Analyses.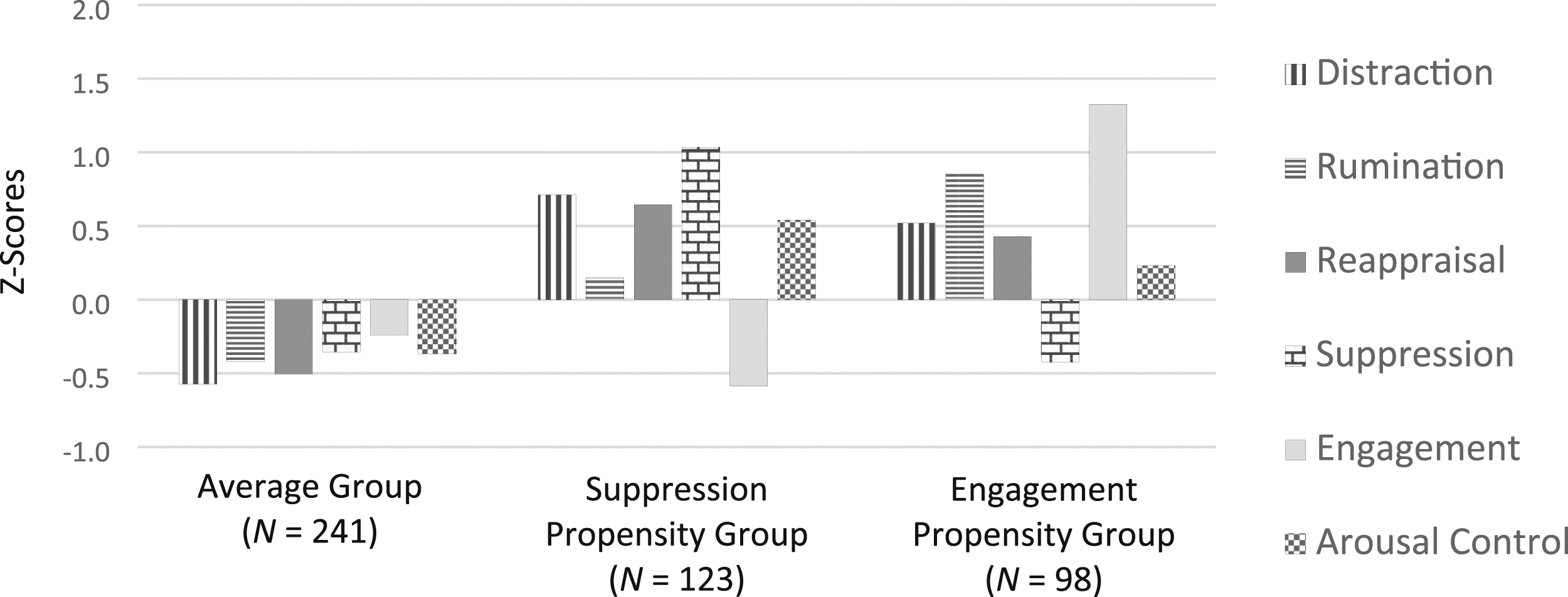
As shown in Figure 1, the health-care providers belonging to the first class reported scores near to the sample mean (within 0.5 SD below the sample mean) for all the RESS scales. This class is the largest in size (52.2% of the participants) and was labelled the Average group. The other two classes were labelled Suppression Propensity (26.6% of the participants) and Engagement Propensity groups (21.2% of the participants). Individuals falling into the Suppression Propensity group reported high scores on the Suppression scale (more than 1.0 SD above the sample mean), relatively high scores (more than 0.5 SD above the sample mean) on the Distraction scale, and low scores on the Engagement scale (more than 0.5 SD below the sample mean). In contrast, the participants belonging to the Engagement Propensity group, showed high scores on the Engagement scale (more than 1.0 SD above the sample mean), relatively high scores (more than 0.5 SD above the sample mean) on the Rumination scale, and scores below the sample mean (within 0.5 SD) on the Suppression scale.
Figure 2 supports the interpretations drawn by Figure 1 and allows for identifying some similarities in the strategies used by individuals belonging to the three profiles. For instance, the individuals of the Suppression Propensity and Engagement Propensity groups, while being markedly different in the Suppression and Engagement scores, showed a similar use of Distraction and Reappraisal.
χ2 tests were run to investigate the relationship between the three latent profiles and gender, age classes (18–30 years vs 31–45 years vs 46–65 years), and professional role (nurses vs first responders). Even if, compared with the group of volunteers, the group of nurses includes more females (χ2(1) = 59.7, p = .001) and older individuals (t(430) = 6.50, p < .001), results showed that the three repertoires were not associated with age (χ2(4) = 6.27, p = .180) or gender (χ2(2) = 3.73, p = .155); however, they were associated with professional role (χ2(2) = 13.21, p ≤ .001). In particular, the analysis of standardized residuals showed that Engagement Propensity was more frequent for nurses (z = 2.24, p < .05) and less frequent for first responders (z = - 2.06, p < .05).
Nurses’ Emotion Regulation Repertoires and Caregiving Orientations
Analyses indicated that the scores of the non-optimal caregiving orientations (HY_Intrusive, HY_Anxiety, and DE) were rather low (i.e., below the mid-point, ps < .001). The lowest score was for DE (Mean = 1.80, SD = .73), whereas the highest was for HY_Intrusive (Mean = 2.96, SD = 1.24; F(2,210) = 83.91, p < .001, η 2 p = .44).
Bonferroni-Corrected Post-Hoc Pairwise Comparisons.
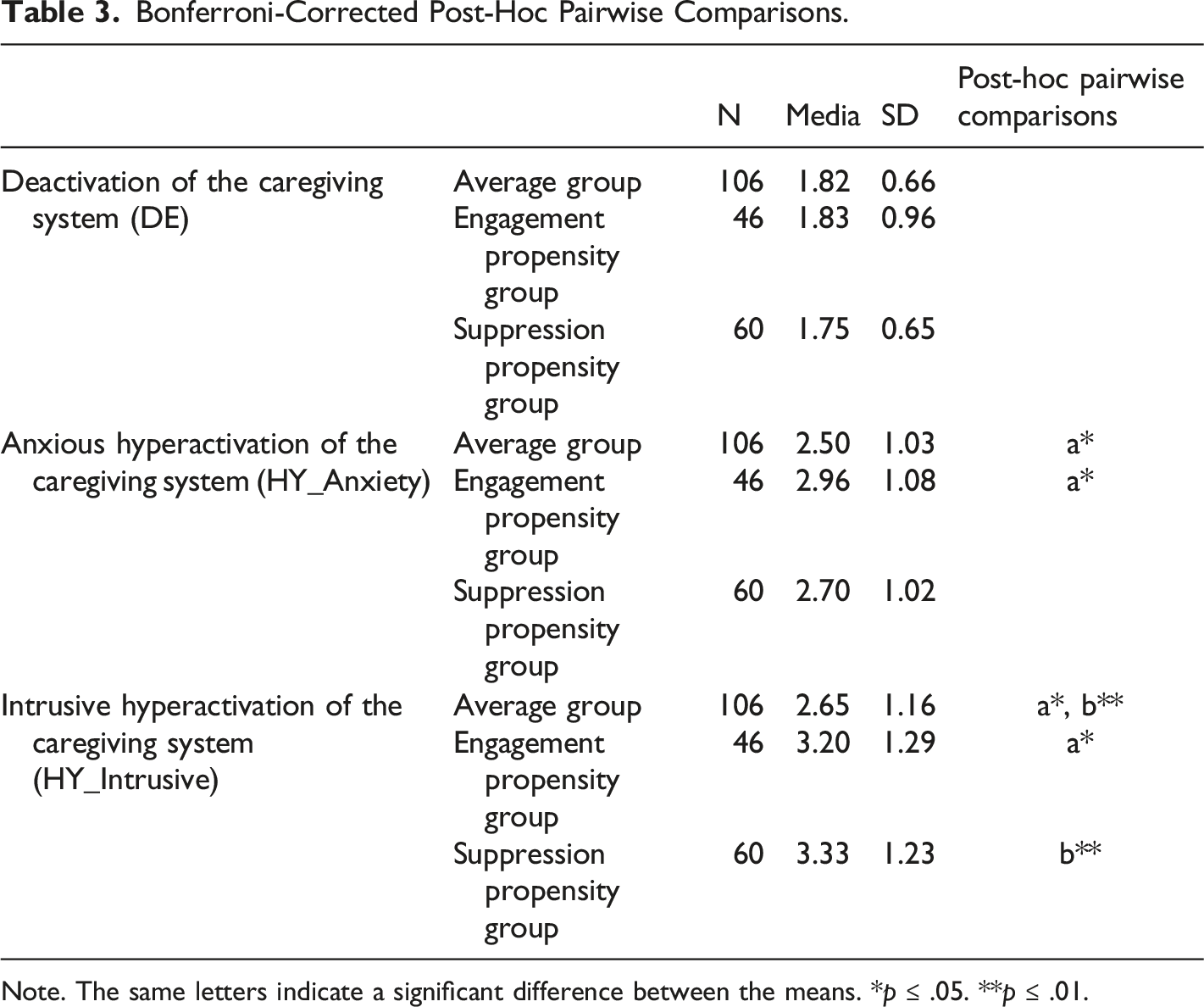
Note. The same letters indicate a significant difference between the means. *p ≤ .05. **p ≤ .01.
Discussion
The work of health-care professionals involves a heavy emotional load related to high physical and psychological costs. For instance, nurses use a lot of energy to regulate their emotions in order to be calm and competent. However, this is often taken for granted and, sometimes, underestimated by others in their working environment (Mauno et al., 2016). Research has paid little attention to these complex dynamics and the few investigations carried out have mostly used a qualitative method. In this study, we explored, in a group of health-care practitioners, how six emotion regulation strategies used to manage negative emotions (Distraction, Rumination, Reappraisal, Expressive Suppression, Expressive Engagement, and Arousal Control), combine to shape emotion regulation repertoires. First, we tested the suitability of an instrument for the assessment of these strategies among health-care providers. In the past, studies on this topic among health-care practitioners have been limited by the unavailability of questionnaires that detect the use of different emotion regulation strategies in a comparable way (i.e., comparing multiple strategies together and investigating how these interact). Data analyses showed that the abbreviated version of the RESS is a suitable instrument for the assessment of emotion regulation repertoires among first responders and nurses. Reliability indices showed satisfactory fit for all the sub-scales of the RESS and construct validity was supported, as indicated by the results of the CFA. Therefore, the 24-item version of the RESS can be used to outline the health-care practitioners’ repertoires of conscious emotion regulation strategies in individuals and groups, with research and/or diagnostic purposes.
The LPA indicated that, among health-care providers, three main profiles (i.e., emotion regulation repertoires), resulting from the combination of the emotion regulation strategies assessed were the best fit for the data. These are consistent with the profiles delineated in the literature (De France & Hollenstein, 2017). The Average profile characterizes people who report average use of all the strategies. On the contrary, the Suppression Propensity group showed using (and relying on) Expressive Engagement less often and Expressive Suppression more often than people of other groups. Finally, the Engagement Propensity group showed using (and relying on) Expressive Suppression less often and Expressive Engagement more often than others. According to previous studies (De France & Hollenstein, 2017; Meneghini et al., 2019), the Average profile is the most common, and is also the most common among participants in our study. It is conceivable that individuals in this repertoire group tend to use the six strategies assessed with greater flexibility, i.e., “the ability to implement emotion regulation strategies that are synchronized with contextual demands” (Aldao et al., 2015, p. 264). On the contrary, individuals who belong to Engagement Propensity and Suppression Propensity group seem to use Expressive Engagement or Suppression in most situations when they want to regulate their unpleasant arousals. As literature suggests (Aldao et al., 2015), people who have large and flexible repertoires have the fundamental elements to develop adaptive and effective emotion regulation processes in various situations. On the contrary, repertoires that are characterized by heavy reliance on a limited number of strategies may be risk factors for mental disorders. However, Aldao (2013) highlighted that only those individuals who endorse using high (but not low) levels of maladaptive strategies are at risk of reduced well-being.
In line with our hypothesis, data indicated that Engagement Propensity characterizes more nurses than first responders. Increased use of Expressive Engagement among nurses, i.e., an emotion regulation strategy that imply an accentuation of emotional expression to regulate the emotional experience, can be explained by the fact that nurses usually have a longer, less occasional and more care-oriented relationships with patients than others (i.e., physicians or first responders, as assessed in this study) and strong emotional expressions could be functional in supporting these relationships. In addition, a profession like that of the nurse places great value on being genuine in the interactions with patients (Diefendorff et al., 2011). Even if according to the Caregiving System theory (Shaver et al., 2010), the differences in the ways people behave in response to requests for support and care from others depend on the individual dispositional level of activation of the system (HY vs DE), these may be shaped by personal experiences in caring situations. Habitual reliance on Expressive Engagement strategies in job relationships may affect the way these professionals manage their negative emotions in many situations, including outside of the workplace. In fact, previous research (Diefendorff et al., 2011) has found that the person-level affectivity, in conjunction with display rules, motivates the extent and type of emotional management in nurses. As a consequence, it is conceivable that a frequent use of Expressive Engagement in the working contexts influences how, in general, the person regulates his/her negative emotions, even in non-work situations. Especially when the nurse’s negative emotional activation elicited in the workplace is inadequately managed, the resulting distress can affect his/her entire life.
More involvement in the relationship with the patient may also encourage in nurses a slight hyperactivation of the Caregiving System. Most nurses who were involved in this study reported low scores of the caregiving system secondary modalities (DE and HY). However, those who were more intrusive and anxious in caring relationships also showed more frequent use of Expressive Engagement. Consequently, it could be affirmed that, in the case of nurses, higher levels of hyperactivation of the Caregiving System (even at a moderate degree) are associated with a greater tendency to regulate negative emotions by means of a strategy that acts on the expressive component of emotion, especially the Expressive Engagement. As hypothesized by De France and Hollenstein (2017), people showing Average and Suppression Propensity emotion regulation profiles may have lower emotional awareness than people who use, to a larger extent, Expressive Engagement. As Expressive Engagement and emotional awareness may have reciprocal influences, nurses belonging to the Engagement Propensity group may perform, to a greater extent, behaviors that characterize hyperactivated helpers, i.e., putting more intense efforts to provide care. In turn, these behaviors may reinforce nurses’ tendency to use Expressive Engagement strategies. Indeed, increased caregiver’s anxiety and intrusiveness may induce a greater need to regulate the distress elicited by the relationship. From this perspective, a greater reliance of nurses on habitual engagement strategies seems to imply negative consequences for them. However, research on emotion regulation has clearly shown that each strategy is not “good” or “bad” in itself, but may be more or less successful, depending on the characteristics of the situation (Aldao et al., 2010; Bonanno et al., 2004). For instance, the use of Expressive Engagement, under some circumstances, may favor feelings of personal and professional accomplishment in nurses, making the relationship with the patient more genuine and satisfying (Diefendorff et al., 2011). These circumstances may be particularly frequent in nursing job.
Study Strengths and Limitations
This is the first study that attempted to describe the emotion regulation repertoires that characterize nurses, and to link these with the individual caregiving orientation. This is an important issue because how the conscious emotion regulation strategies combine, their association with automatic emotion regulation processes, the frequency with which each strategy is usually used are all facets related to individual and workplace well-being. Our study offers an effective self-report instrument to develop research on the emotion regulation in care environments.
One limit of the study is that, as a result of its exploratory nature, we did not take into account any additional dispositional variables that could affect the emotion regulation repertoires (e.g., personality traits, empathic responsiveness, etc.). Moreover, in many everyday situations some emotion regulation processes take place automatically and unconsciously and, even if a deliberate management of one’s emotional arousals occurs, the result may be affected by unconscious, implicit regulatory processes (Koole & Rothermund, 2011). Further research, in larger and more various samples, may investigate these relationships and also shed light on how the emotion regulation repertoires may depend on organizational conditions such as organizational and professional display rules, the length of service of the nurse, etc. Assessing variability in contextual characteristics (e.g., specific job situations), it will be also possible to evaluate which are the most adequate emotion regulation modalities that prevent phenomena such as burnout and compassion fatigue in nurses. We compared nurses and first responders focusing on the different type of caring that they provide to patients in their work. This because our assumption was that prolonged caring as opposed to caring that is limited in terms of time of contact with the patient, might be a characteristic that influences how these health professionals regulate emotions. However, there may be other differences (e.g., length of service, nurses are paid for their work and would not find it easy to quit, while volunteers can quit any time they want if they got burned out) that influence an individual’s behavior and consequently have an effect on individuals’ emotion regulation processes. Future research may also measure the effects of these variables. Finally, as ways and goals of emotion regulation are strongly linked to culture (Djediat et al., 2020), future studies should examine whether the use of emotion regulation strategies and repertoires vary depending on the nurse’s cultural background.
Conclusions
This study offered a self-rated instrument to evaluate emotion regulation repertoires and, in a comparative way, the use of some conscious emotion regulation strategies of health-care providers. The 24-item version of the RESS allows clinicians and researchers to assess the use of conscious emotion regulation strategies of these workers at individual and/or group level, for research and diagnostic purposes. We hope that this will stimulate investigations that shed light on the emotion regulation processes of nurses and on their adequacy in different contexts. Specifically, our data showed that three different profiles are distinguishable, i.e., three emotion regulation repertoires that result from the combination of six of the main strategies that people consciously use to regulate their negative emotions: Average, Suppression Propensity and Engagement Propensity. The latter characterized the nurses and showed to be related to greater (even if at moderate levels) hyperactivation of the Caregiving System. We hypothesized that this association is explained by the greater involvement in the relationships that these professionals have with their patients in comparison with first responders. For example, nurses who are considered to be more compassionate and empathic are genuinely therapeutic for patients (Kinman & Grant, 2016). This means that they need to continually develop and maintain effective resources and emotion regulation strategies to face distressing work conditions. When regulation skills are poor, the risk is that relationships with patients are characterized by excessive emotional detachment or, conversely, hyperidentification with the suffering other. Further research will be able to evaluate how much each strategy or repertoire is functional in the different working situations of the nurses. Indeed, increased knowledge of how these professionals regulate negative emotions, both outside and inside work contexts, can be useful to develop trainings that help them to improve their emotion regulation abilities. The RESS can be the starting point to develop research on the levels of adequacy of nurses’ emotion regulation repertoires to promote satisfying relationships. For instance, if some nurses’ emotion regulation repertoires showed to be not adequate or tend to change over time, a suggestion could be to help nurses to strengthen their job self-efficacy (even in terms of emotion regulation skills) and empathic abilities (Cunico et al., 2012; Meneghini et al., 2016; Schipper & Petermann, 2013) to reduce anxiety and hyperactivation of the Caregiving System that, in turn, may influence their use of emotion regulation strategies.
Footnotes
Acknowledgments
Thanks are due to all the participants. In addition, the authors wish to thank Professor Laura Cunico for commenting on earlier versions of the manuscript and Dr. Gaia Carbon for her support in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.