
Abstract
Self-Practice/Self-Reflection (SP/SR) is an aspect of therapist training and professional development aimed at enhancing therapy skills, empathy, wellbeing, and resilience in the ultimate furtherance of client outcomes. For many decades, intensive SP/SR has been a required part of therapist training in many countries but relatively little is known about the effect of SP/SR. Studies have found cognitive-behavior therapy (CBT) therapists trained under a Beckian CBT paradigm benefitted from more time limited Beckian SP/SR. Mindfulness-based CBT is a more recent third-wave CBT paradigm with psychological process aims similar to those of SP/SR. While training in mindfulness-based CBT often has prominent SP/SR aspects, and mindfulness practice has been shown to benefit health care providers personally and professionally, to date no evaluations have been reported specifically of effects of participation of CBT trainees in stand-alone mindfulness-based SP/SR that meets regulatory requirements for more intensive SP/SR. A study on SP/SR training meeting German requirements is reported here. Post-graduate CBT trainees (N = 95) were assigned to delayed or immediate SP/SR with those in the delayed SP/SR condition crossing-over into SP/SR training after two baseline evaluations on a variety of reflective skill, wellbeing, and resilience measures spaced six to 9 months apart before participating in 120–150 hours of stand-alone mindfulness-based SP/SR followed by a third reevaluation on all study measures. Participants assigned to the immediate SP/SR condition underwent identical SP/SR training with pre/post assessments. Results indicate participation in intensive stand-alone mindfulness-based SP/SR resulted in favorable changes in measures operationalizing all variables. Findings are discussed in terms of their implications for training and professional development of CBT therapists.
Keywords
Introduction
Practitioners of Cognitive-Behavior Therapy (CBT) develop competencies as they progress throughout their training and later in their careers. These have been conceptualized as having declarative, procedural, and reflective components (Bennett-Levy, 2006). Declarative knowledge is factual information whether subject matter related or personal. Procedural skills are knowing how to do therapy, whether implicit or rule based. Reflective competencies are essentially a “… metacognitive skill which encompasses the observation, interpretation, and evaluation of one’s own thoughts, emotions and actions, and their outcomes.” (Bennett-Levy, 2006, p. 60). While training programs have traditionally placed considerable emphasis on declarative and procedural skills, attention on reflective skills has been more variable.
Several countries, including all Scandinavian countries, Germany and Austria have long legally required Self-Practice/Self-Reflection training (SP/SR) as part of training of therapists of various schools of psychotherapy including CBT to improve both professional competency and personal resilience (cf. Laireiter & Willutzki, 2003). In Germany, as of 2022, the requirement is for 120 hours SP/SR training for psychologists and counselors becoming licensed CBT therapists (cf. Laireiter & Willutzki, 2003). Similarly, 150 hours of CBT SP/SR training is mandatory for physicians choosing CBT training to qualify for independent practice in several mental-health-related medical subspecialties including psychiatry, psychosomatic medicine, and neurology (Bayrische Landesärztekammer, 2020).
SP/SR is a form of experiential learning (cf. Morris, 2020) with therapists-in-training as actively involved participants. Therapeutic techniques are self-practiced during workshops and home practice by applying them to common real-world psychological problems which trainees are themselves facing. This exposes trainees to novel experiences as they personally experience therapeutic techniques. As with other experiential learning, trainees may experience SP/SR as demanding and somewhat psychologically risky. This is why conducting SP/SR training typically requires prior disclosure and participant consent as, for example, called for under Section 7.04 of the Code of Conduct of the American Psychological Association (American Psychological Association, 2017). In addition to self-practice, SP/SR strategically employs critical self-reflection to engender and deepen meaningful learning (cf. Bennett-Levy, 2019; M. L. Davis et al., 2015; Laireiter & Willutzki, 2003).
Self-reflection is a critical element of SP/SR not only because it supports the development of procedural and declarative knowledge (Bennett-Levy et al., 2003; Rønnestad et al., 2019; Skovholt & Trotter-Mathison, 2016, p. 197), but more importantly because self-reflection is thought to be key to the development of the empathic skills underlying a strong therapeutic alliance which is the strongest non-specific determinant of psychotherapy outcome (Flückiger et al., 2018). SP/SR’s specific focus on reflective skills (cf. Bennett-Levy, 2019) has been associated with improvement in these skills among both early career and experienced CBT therapists (Bennett-Levy et al., 2003; M. L. Davis et al., 2015). However, due to lack of experimental control conditions, studies showing these effects often do not allow for such improvements to be unambiguously attributed to SP/SR participation versus general professional development factors (McGillivray et al., 2015; McGinn, 2015).
In addition to reflective and empathic skills, therapists’ own wellbeing and resilience have been shown to affect the quality of their therapeutic work (Nissen-Lie et al., 2013, 2017). While wellbeing always appears to have a positive effect on therapeutic competencies (Nissen-Lie et al., 2013), the role of resilience-related coping skills is less straight forward. Here, a certain amount of self-doubt (Nissen-Lie et al., 2013), including an ability to tolerate uncertainty appears to be beneficial (Strout et al., 2018; Turner et al., 2014). However, while SP/SR training has well documented benefits for CBT therapists’ reflective (McGillivray et al., 2015) as well as declarative and procedural skills (M. L. Davis et al., 2015), its effects on general wellbeing and tolerance of uncertainty are less known.
Despite having been required for many decades in many countries, specific therapist and therapy-related outcomes of SP/SR training have only recently been put to empirical tests, at least in English language publications (cf. Bennett-Levy, 2019; examples are: M. L. Davis et al., 2015; Haarhoff et al., 2011). Furthermore, the extant empirical literature, SP/SR has been mostly approached from a traditional Beckian approach (M. L. Davis et al., 2015, p. 182). A more recent third-wave CBT treatment paradigm with a considerable evidence base employs mindfulness-based interventions such as Mindfulness-Based Stress Reduction (MBSR; Kabat-Zinn, 2013; Santorelli et al., 2017) and Mindfulness-based Cognitive Therapy (MBCT; Segal et al., 2002, 2013). Mindfulness-based meditation interventions have been shown to improve emotion regulation skills, resilience, and psychological well-being (Birtwell et al., 2019; Godfrin & van Heeringen, 2010). Specific mechanisms of action responsible for its effects likely include improved self-reflective skills (Gu et al., 2015, 2016; Lutz et al., 2016), improved resilience by way of enhanced tolerance of cognitive and emotional processes (Farb et al., 2012; Herwig et al., 2010), and improved self-esteem (Morley & Fulton, 2020). Of these the role of self-esteem as a mechanism of action in mindfulness is least well understood because self-acceptance but not self-esteem is specifically targeted the practice of mindfulness (Thompson & Waltz, 2008). However mindfulness practices have often been found to result in increased self-esteem (Morley & Fulton, 2020; Pepping et al., 2013) and may mediate its beneficial effects (Bajaj et al., 2019).
Study Aims
The study aimed to examine quantitative evidence of effects of comprehensive mindfulness-based SP/SR on self-reflection, empathy, psychological wellness, and resilience, among CBT trainees of various health service professions.
Hypotheses
Based on the prior literature on the benefits of SP/SR training for CBT therapists and the effects of mindfulness-based interventions on psychological wellbeing and resilience, participation in mindfulness-based SP/SR training was hypothesized to be associated with improvements in (i) self-reflection and empathy and (ii) psychological wellbeing and resilience.
Method
Design
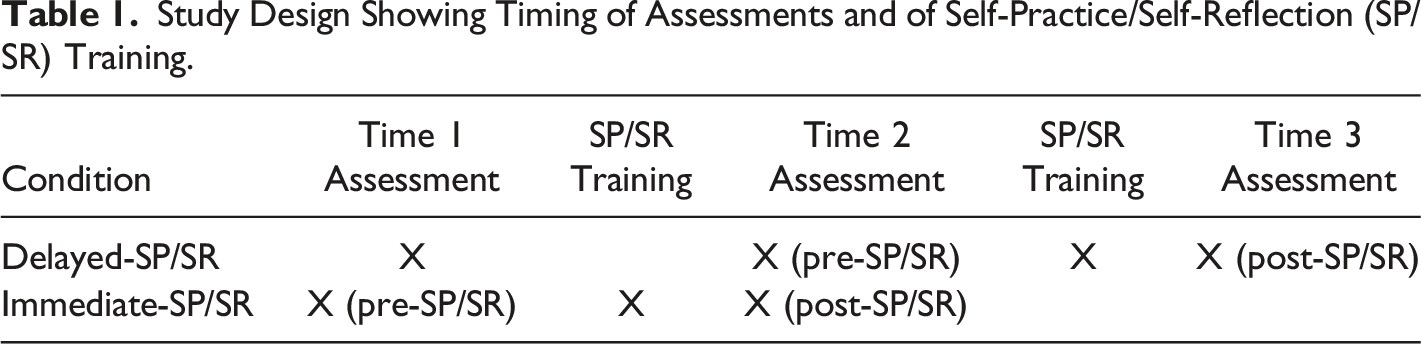
Study Design Showing Timing of Assessments and of Self-Practice/Self-Reflection (SP/SR) Training.
Participants
Participant (N= 95) Demographics.
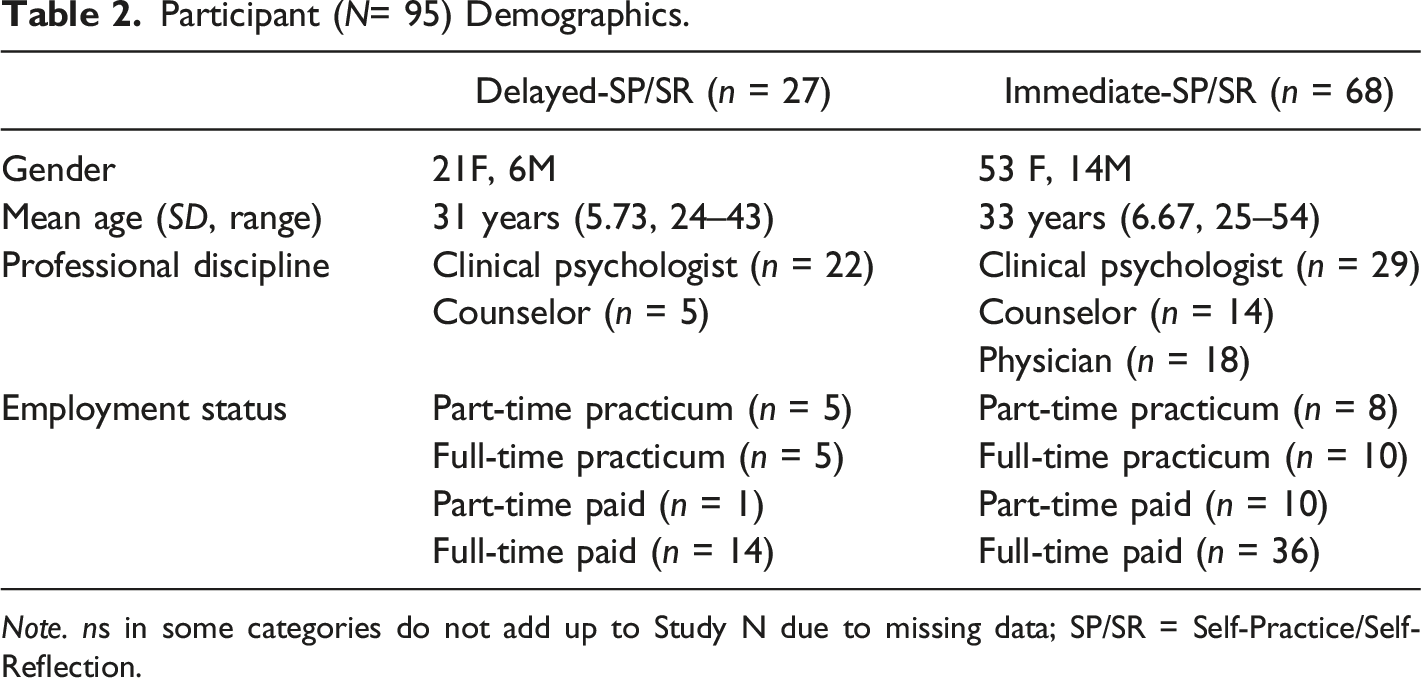
Note. ns in some categories do not add up to Study N due to missing data; SP/SR = Self-Practice/Self-Reflection.
Mindfulness-Based Self-Practice/Self-Reflection Training
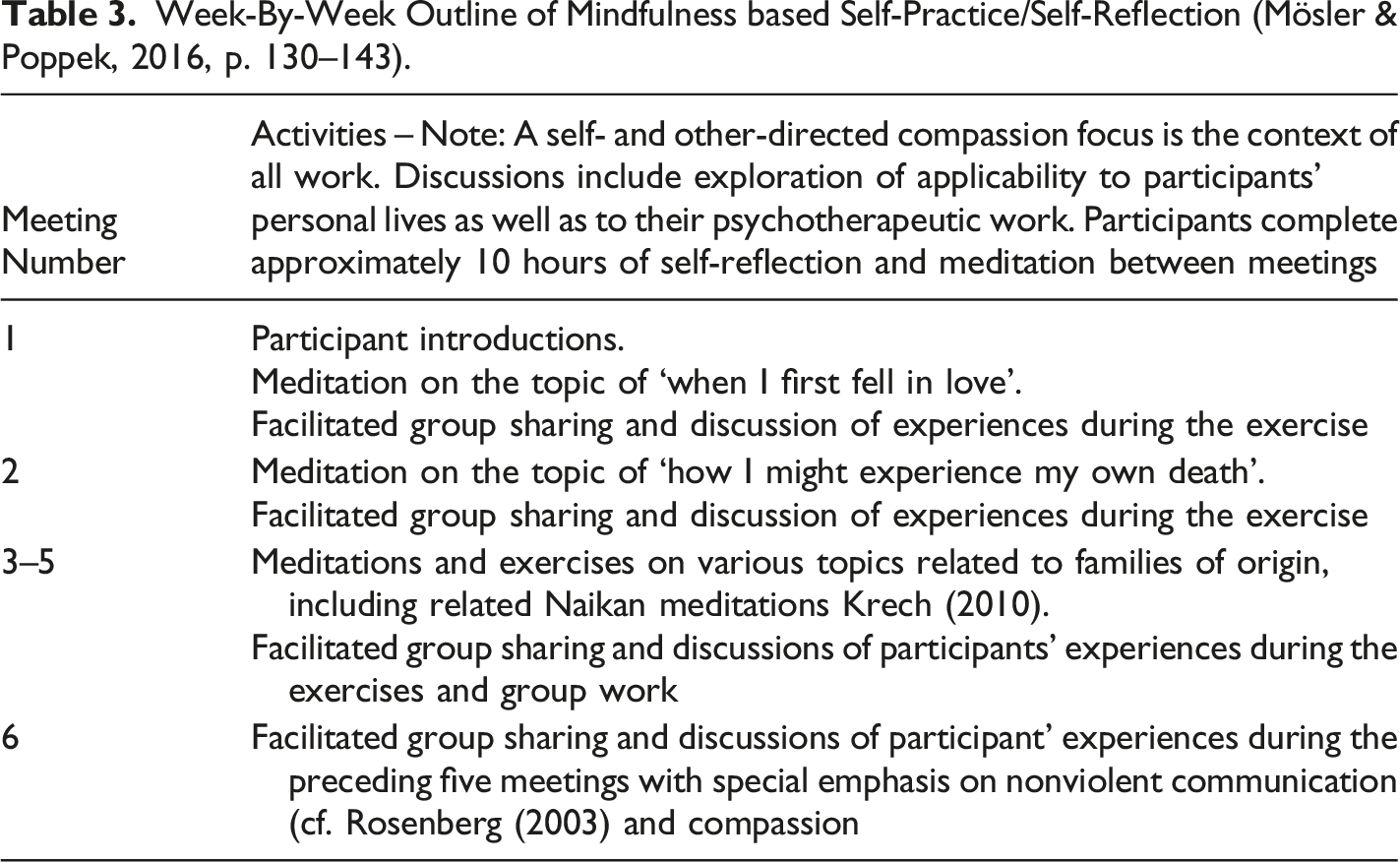
In compliance with German regulations, mindfulness-Based SP/SR was delivered over a 120–150 hours broken into a series of six or seven two-to three-day workshops spaced one to 3 months apart with participants required to spend approximately 10 hours between workshops for written self-reflection and meditation exercises. Throughout all workshop and home exercises, equal emphasis was placed on the personal and professional practice dimensions of SP/SR (cf. Bennett-Levy, 2019).
Week-By-Week Outline of Mindfulness based Self-Practice/Self-Reflection (Mösler & Poppek, 2016, p. 130–143).
Measures
Participants completed a brief sociodemographic survey to indicate their age, gender, professional discipline, and employments status.
The German version of the
The German version of the
The German version of the
The German version of the
The German version of the
Finally, participants answered three
Procedure
After providing consent, participants in both conditions completed the sociodemographic survey and all study measures. Participants in the immediate SP/SR condition then commenced 120–150 hours mindfulness-based SP/SR training over six to seven two-to three-day long workshops followed by post-SP/SR assessment on all study variables. Participants in the delayed-SP/SR condition waited 6–9 months before completing all measures again followed by immediately commencing identical SP/SR training followed by a third completion of all study measures. Total duration of SP/SR training in both conditions was dependent on availability of staff to run workshops and on participants’ personal issues, such as birth of a child or illness and averaged 15.03 months (SD = 4.50).
Results
Plan for Analyses
Data were analyzed in two phases. In Phase I, to see if SP/SR conditions affected study variables while controlling for threats to internal conclusion validity of history and maturation (Kazdin, 2017, p. 17), the interaction of time (Time 1 vs. Time 2) and condition (Delayed-SP/SR vs. Immediate-SP/SR) was analyzed using a mixed within-between two-way ANOVA. In the Phase I analysis delayed-SP/SR participants served as the no-intervention control and their post-SP/SR scores did not participate. Power to find a small to medium time by condition effect
For the subsequent Phase II analysis, groups were combined to take advantage of the additional power due to delayed-SP/SR participants crossing over into the SP/SR intervention after Time 2. Only study variables found to be significantly impacted by treatment in Phase I were examined as outcome variables in Phase II to examine if effects found in Phase I would replicate when delayed-SP/SR participants were included in the analysis and to examine possible moderation of SP/SR effects by participants’ professional discipline. These analyses employed mixed within-between two-way ANOVAs using pre-SP/SR/post-SP/SR score pairs as the within subjects’ independent variable and SP/SR condition (delayed vs. immediate) as the between subjects’ independent variable. The first baseline measurement in the delayed-SP/SR condition did not participate. Power was equivalent to that in Phase I. A significant interaction of time by condition in Phase II would mean that SP/SR groups did not respond to SP/SR in the same fashion. A significant main effect for condition would mean a failure of group assignment to conditions to yield equivalent groups. A significant main effect for time would mean that participation in SP/SR training affected outcome variables in both groups and would thus potentially replicate Phase I results.
Finally, because professional discipline of participants varied across SP/SR conditions because there were no physicians in the delayed-SP/SR condition, mixed within-between two-way ANOVAs were run with pre-SP/SR/post-SP/SR as the within subjects’ independent variable, professional discipline (psychologist, counselor, physician) as the between subjects’ independent variable, and all outcome variables that showed replicated effects as dependent variables. In this analysis a significant time by professional discipline interaction would signify that members of different professions responded differently to SP/SR training.
Phase I Analysis: Empathic and Reflective Skills
Phase I Analysis: Means Standard Deviations, and Two-Way ANOVA Statistics for Empathic and Reflective Skills Variables.
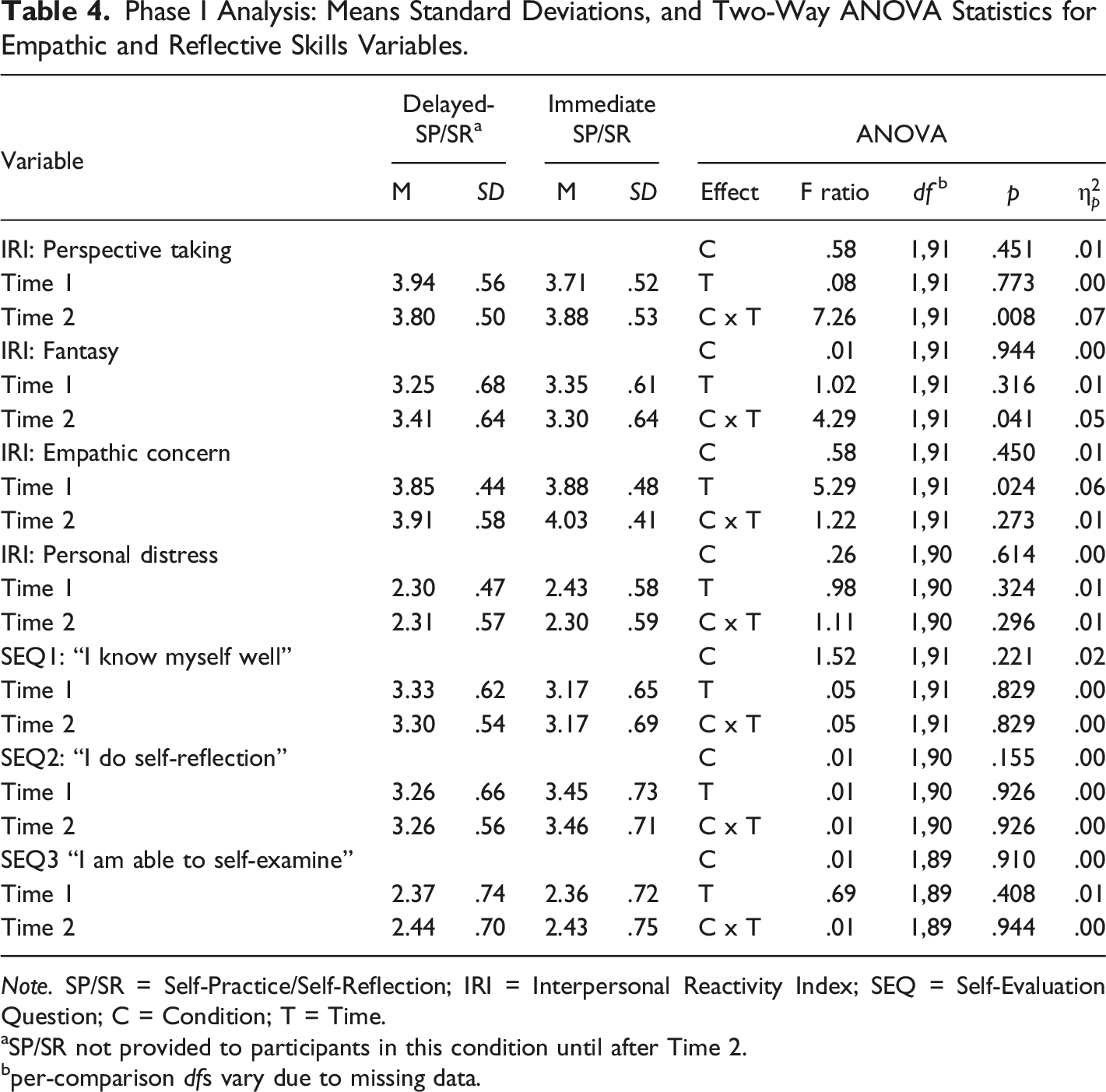
Note. SP/SR = Self-Practice/Self-Reflection; IRI = Interpersonal Reactivity Index; SEQ = Self-Evaluation Question; C = Condition; T = Time.
aSP/SR not provided to participants in this condition until after Time 2.
bper-comparison dfs vary due to missing data.
Phase I Analysis: Psychological Wellness and Resilience
Phase I Analysis: Means Standard Deviations, and Two-Way ANOVA Statistics for Psychological Wellbeing and Resilience Variables.
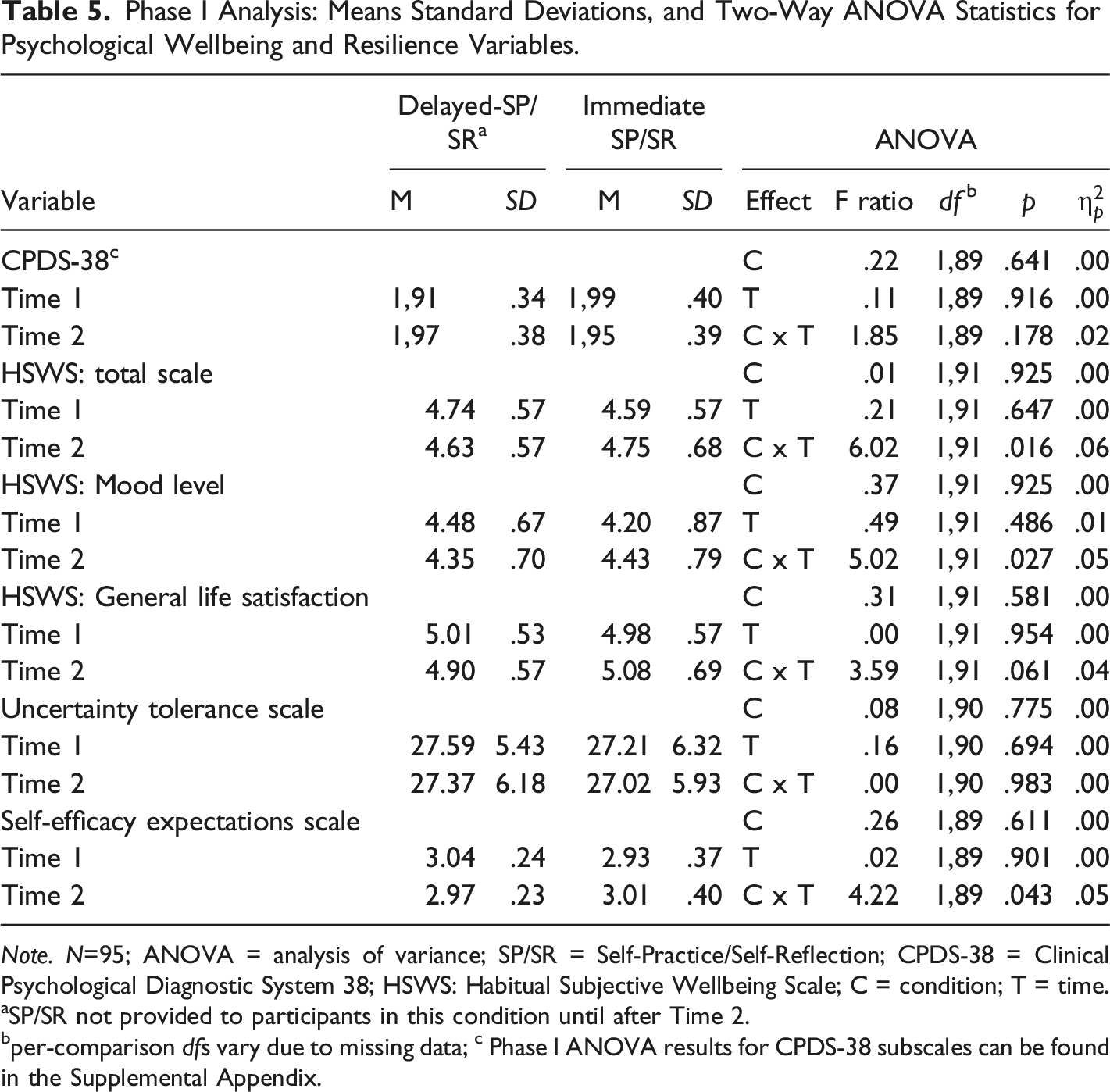
Note. N=95; ANOVA = analysis of variance; SP/SR = Self-Practice/Self-Reflection; CPDS-38 = Clinical Psychological Diagnostic System 38; HSWS: Habitual Subjective Wellbeing Scale; C = condition; T = time.
aSP/SR not provided to participants in this condition until after Time 2.
bper-comparison dfs vary due to missing data; c Phase I ANOVA results for CPDS-38 subscales can be found in the Supplemental Appendix.
Phase II Analysis: Replication of Significant Interaction Effects from Phase I
Phase II Analysis: Means Standard Deviations, and Two-Way ANOVA Statistics for Variables Found to be Affected by SP/SR in the Phase I Analysis.
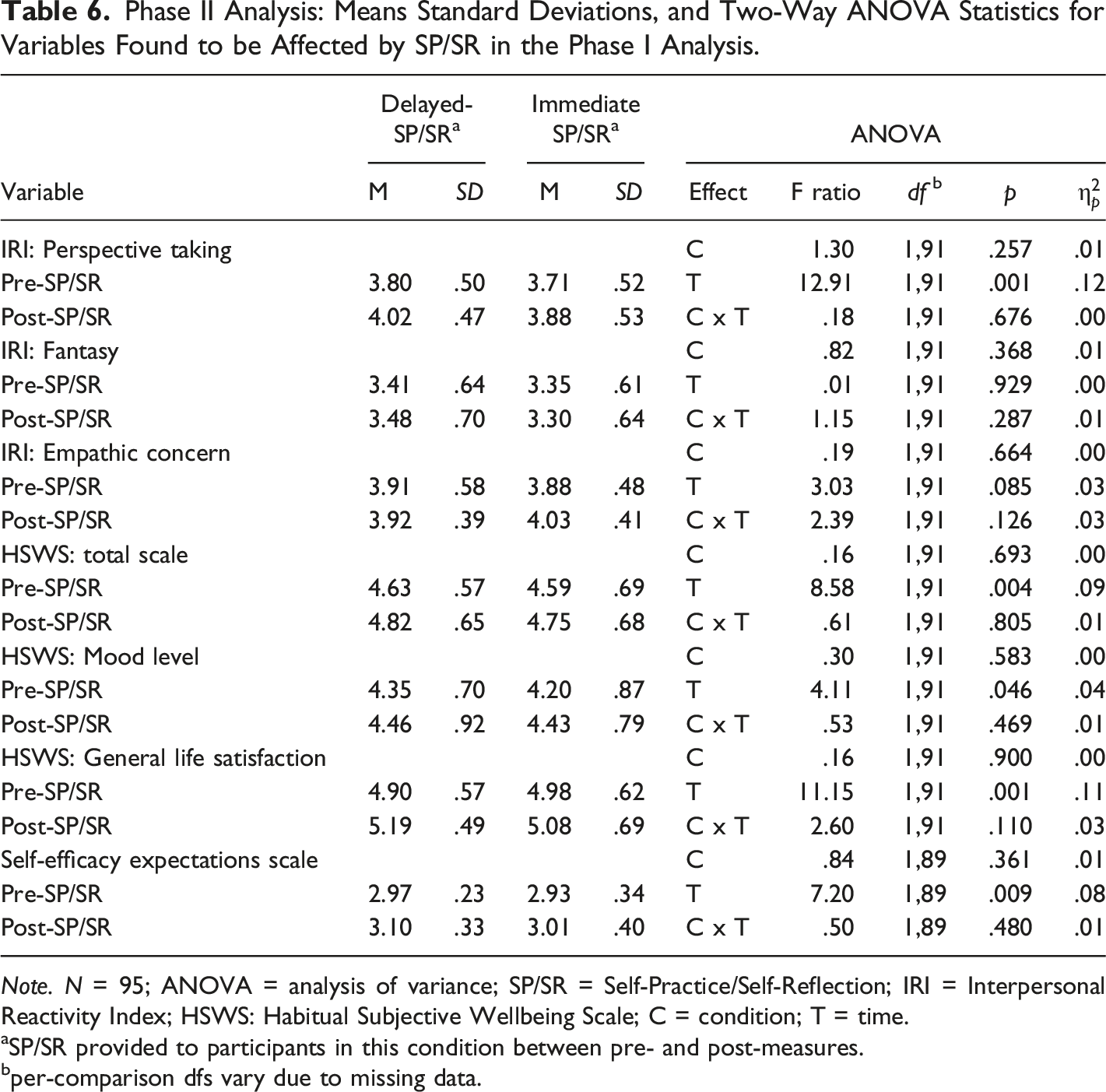
Note. N = 95; ANOVA = analysis of variance; SP/SR = Self-Practice/Self-Reflection; IRI = Interpersonal Reactivity Index; HSWS: Habitual Subjective Wellbeing Scale; C = condition; T = time.
aSP/SR provided to participants in this condition between pre- and post-measures.
bper-comparison dfs vary due to missing data.
Phase II Analysis: Examination of the Effect of Professional Discipline SP/SR Training Outcomes
Mixed within/between two-way ANOVAs were run with professional discipline (psychologist, counselor, physician) as the between subjects’ variable, pre-SP/SR/post-SP/SR as the within subjects’ variable, and dependent variables IRI perspective taking (F (2,84) = 1.51; p = .23), HSWS total scale (F (2,84) = .35; p = .71), HSWS mood level (F (2,84) = .07; p = .93), and HSWS general life satisfaction (F (2,84) = .92; p = .40), and SEES (F (2,82) = .21; p = .81). These were the outcome variables where SP/SR effects found in Phase I, were replicated in Phase II. Because none of these effects were significant, participants’ professional discipline did not significantly impact how they responded to SP/SR training.
Discussion
As hypothesized, mindfulness-based SP/SR training had beneficial effects on empathy, reflective skills, wellbeing, and resilience of CBT trainees. Improvements in empathy and reflective skills were evident on the IRI subscale “perspective taking” but not on other IRI subscales or on the three SEQ items. Positive effects on wellbeing and resilience were found on HWBS, its mood level and general life satisfaction subscales, and on the SEES. There were no effects on CPDS-38 total scores, any CPDS-38 subscales, or on the UTS.
Changes in study variables were not evident due to time alone or due to whether SP/SR training was provided immediately or after a 6–9 months delay. This provides a good counter argument to threats to internal conclusion validity of natural psychological maturation across time or of extraneous events that may have coincidentally occurred while SP/SR was ongoing. This is important because these confounding factors might otherwise account for the observed changes rather than SP/SR training. However, alternative accounts for why changes were seen cannot be entirely ruled out, as participants had many other training experiences throughout the approximately one to two-year duration of the study which may have impacted study variables. For example, participants’ professional responsibilities and demands on their time typically increase later in CBT training, though it is unclear whether this might support or tax wellbeing and resilience. Similarly, CBT training and supervision may have primed the development of empathy late in training to potentiate the impact of SP/SR training. To control for these confounds, an extended no-SP/SR control group would be ideal, but such a group could not be formed due to the legal requirement in Germany that all CBT trainees participate in SP/SR training. Owing to these circumstances, obtaining a Time 1 measurement from the delayed-SP/SR group was a good way to address maturation and history threats to improve internal conclusion validity.
Similarly, threats to external validity could be ruled out reasonably well and results can be considered generalizable due to the low participant attrition rate and finding that training effects could not be attributed to participant’s professional discipline (psychologist, counselor, or physician) or to whether SP/SR began immediately or after a delay. The heterogeneous composition of both samples in terms of professional background, age, and gender further speak in favor of the generalizability of the present findings.
A limitation of the study was the lack of an implementation check. While all participants completed SP/SR training, it is unknown if all benefitted equally. Future studies may want to include a measure of mindfulness such as the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006). Variations in FFMQ scores may also relate to individual differences in participant motivation and engagement, variables also not assessed in the present study which have previously been found to relate to the benefit of SP/SR (M. L. Davis et al., 2015). Inclusion of such measures may be particularly relevant when studies are conducted in countries such as Germany where SP/SR training is legally required.
Despite good power, SP/SR training effects were not found in uncertainty tolerance on the UTS, on the CPDS-38 and its subscales, and on the self-reflection items of the SEQ. As mindfulness practice is well known to improve distance from own thoughts and emotions (Herwig et al., 2010; Lutz et al., 2016), the lack of findings on the UTS is somewhat puzzling. This may have been due to this particular operationalization of tolerance of uncertainty (Dalbert, 2002b) which, while popular in Germany, may not be sensitive to changes in affect management due to mindfulness practices. However, it may also reflect variability in degree to which participants mastered mindfulness skills which is unknown due to the lack of an implementation check. Lack of findings on the CPDS-38 may be because the CPDS-38 is a pathology focused measure. With observed CPDS-38 scores in this study toward to bottom end of the scale, a pathology-oriented measure may have lacked the measurement sensitivity to detect more subtle changes in wellbeing among this group of overall psychologically well-adjusted CBT trainees. SEQ items were pilot tested in this study to see if these items with their good face validity could give a reliable read of participants’ self-rated reflective skills. However, it did not appear that merely asking participants self-reflection questions is a feasible way to detect any impact of SP/SR.
Findings of the present study regarding wellness and resilience replicate the prior literature on the personal benefits of mindfulness-based practice among a variety of health service providers (Conversano et al., 2020; Spinelli et al., 2019). Importantly, SP/SR equally emphasizes the application of self-practice and self-reflection to professional competencies (cf. Bennett-Levy, 2019). Here prior findings have also shown benefits, for example for increased empathy and reduced compassion fatigue among a variety of health care providers (Conversano et al., 2020). In contrast to the present study, however, efficacious mindfulness protocols from prior studies often only take just a few hours (Kriakous et al., 2021) or may be delivered virtually (e.g., Pflugeisen et al., 2016; Wen et al., 2017) versus the SP/SR protocol employed here which takes 120–150 hours plus additional time for home-based self-reflection and meditation. Future research may thus want to investigate what the optimal dose/response relationship for mindfulness-based SP/SR to engender both personal and professional outcomes.
For better comparability between present findings and prior work on the effects of Beckian-based SP/SR as developed by (Bennett-Levy et al., 2015), it would have been desirable also to include in this study outcome measures used in previous SP/SR research, such as the Cognitive Therapist Self-Monitoring Scale (CMSMS) (Thwaites et al., 2003) as cited in M. L. Davis et al., (2015) and the Cognitive Therapist Empathy Scale (CTES; (Thwaites et al., 2003) as cited in M. L. Davis et al., (2015). It is entirely possible, that despite the differences in paradigms between Beckian and mindfulness-based SP/SR, effects on therapists’ reflective competencies, wellbeing and resilience might be comparable. Present findings that self-efficacy improved following mindfulness-based SP/SR would be consistent with this. On the other hand, because mindfulness-based SP/SR does not include practice of specific cognitive-therapy (CT) skills, a mindfulness-based approach may not lead to improvements in CT-specific technical skills seen after Beckian SP/SR (cf. Haarhoff et al., 2011; Schneider & Rees, 2012). Such measurement of declarative and procedural CBT skills would also have been desirable to see if improvements seen here in empathy translate into better declarative and procedurals skills as prior research and theory would suggest (Bennett-Levy, 2006). Though it is possible there are paradigm specific SP/SR effects with mindfulness-based SP/SR specifically benefiting declarative and procedural skills related to mindfulness-based CBT but not to Beckian CBT.
Regardless of the paradigm they follow, all therapists aim to improve their clients’ mental health. However, similar to prior SP/SR studies (cf. McGillivray et al., 2015), the effect of SP/SR on ultimate client outcomes was not measured in this study and is therefore unknown. Because prior research has shown that when therapists’ empathy and skills improve, their well-being, coping skills, and reflective abilities also increase, it stands to reason clients would also benefit. Nevertheless, it would be desirable at least to show effects of SP/SR on clients’ experience while undergoing CBT, for example by evaluating possible changes the quality of the Helping Alliance (Luborsky et al., 1996) as their therapists participate in SP/SR.
Conclusion
SP/SR based on Beckian principles has been shown to have many promising benefits for the training and later professional development of CBT therapists practicing Beckian CBT. While empirically supported mindfulness-based therapies such as MBSR and MBCT have prominent experiential aspects that are also used in training therapists to implement them, there would not appear to have been prior studies on the effects of an organized course of mindfulness-based SP/SR training. Because SP/SR training is not only promising benefits for CBT trainees and their clients but is a legal requirement in many countries, the availability of empirically supported mindfulness-based SP/SR training as documented in this study is of benefit to training programs in such countries and elsewhere that seek an additional option to engage CBT trainees in SP/SR. The present findings are an important step in showing mindfulness-based SP/SR benefits CBT trainees’ self-reflective and empathic development, wellbeing, and resilience.
Supplemental Material
Supplemental Material - Reflective Skills, Empathy, Wellbeing, and Resilience in Cognitive-Behavior Therapy Trainees Participating in Mindfulness-Based Self-Practice/Self-Reflection
Supplemental Material for Reflective Skills, Empathy, Wellbeing, and Resilience in Cognitive-Behavior Therapy Trainees Participating in Mindfulness-Based Self-Practice/Self-Reflection by Thomas Mösler, Sandra Poppek, Christoph Leonhard, and Wilfried Collet in Psychological Reports
Footnotes
Author Contributions
TM and SP: Conceptualization, implementation, and manuscript editing. WC: Conceptualization, data analysis, and manuscript editing. CL: Conceptualization, data analysis, and manuscript preparation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TM and SP participate financially in book sales of the Self-Practice/Self-Reflection program that is the subject of this research and in workshops implementing the program.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available for reanalysis contingent on IRB approval of proposed research.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.