
Abstract
Why did Australia border earlier than most other states in response to the outbreak of COVID-19? Between mid-January and March 2020, the Australian government adopted increasingly restrictive travel bans that led to the country closing its borders to all non-residents, adopting mandatory hotel quarantines for 14 days and a travel ban on Australians travelling overseas. These actions were in contravention of the World Health Organization advice to states on travel restrictions. Australia’s border closure was one of the strictest and, ultimately, longest in the world. In this article, we complement existing explanations on bordering that include critical border studies, securitization and bio/necropolitics with theoretical approaches from public policy literature to examine the domestic conditions that inform border closure policies and practices. We demonstrate that the decision to border, in this case, was not a rejection of World Health Organization advice but a turn towards the domestic pull factors – including domestic expert advice – to border.
Introduction
On 1 February 2020, as the COVID-19 outbreak advanced towards Australia, the country’s Chief Medical Officer (CMO), Brendan Murphy, proposed a solution: close the international border. The closure was gradual but decisive. The Australian government listed COVID-19 as a human disease under the ‘Biosecurity Act 2015’ on 21 January and commenced screening flights coming from Wuhan, China. On 1 February, Australia banned non-residents entering from China, the first of four travel bans which later included Iran (29 February), South Korea (5 March) and Italy (11 March). Between 18 and 27 March 2020, Australia banned international cruise ships, closed its borders to all non-residents, adopted mandatory 14-day hotel quarantine and established a travel ban on Australians travelling overseas, making Australia’s COVID-19 bordering response one of the strictest in the world.
At the time, Murphy’s advice and the Australian government’s actions went against the recommendations of the World Health Organization (WHO): its Director-General had recommended no travel or trade restrictions in response to the COVID-19 outbreak.
1
As a signatory to the International Health Regulations (IHR), Australia’s actions were a clear denial of its international obligations to adhere to WHO advice. However, Australia was not alone in this departure from WHO recommendations. Indeed, it was one of 39 countries that adopted travel bans between January and February 2020.
2
By the end of March, most countries in the world had established bordering measures to respond to the COVID-19 outbreak. Some have since argued that this decision was effective in slowing early transmission (Grépin et al., 2021; Mallapaty, 2020), including CMO Murphy himself (Probyn, 2020). Returning to their 2021 study, Grepin et al. (2024: 11) found:
it seems likely that the border control measures imposed in the early phase of the epidemic (e.g. before March) had some impact on delaying the export of cases out of China and, thus, likely delayed the establishment of outbreaks outside of China, but clearly they were insufficient to stop the pandemic. All the identified studies found that the measures imposed on Wuhan travellers by Chinese officials were likely very effective in reducing exported cases and that the additional targeted measures against Chinese travellers by other countries played some role, but both types of measures became relatively ineffective within a few weeks as other places became the dominant source of imported cases.
Yet this finding, 3 years later, does not explain why states such as Australia bordered so rapidly, decisively and strictly, particularly when the evidence was not clear at the time that bordering would be effective, and international advice recommended against it.
A nascent literature lying at the intersection of Critical Border Studies (CBS), securitization and bio/necropolitics attempts to explain why states implemented border closures during COVID-19 (Bissonnette and Vallet, 2022; Chaulagain et al., 2022; Ferhani and Rushton, 2020; Gülzau, 2021; Hoffman et al., 2022; Lara-Valencia and Laine, 2022; Ozguc, 2021). These works focus on the sovereign decision to border, providing insight into the enforcement and impact of bordering. This work explains the outcome (the sovereign decision) and its impact. In this article, we want to step back and examine the processes that led to the decision to border, including the conflicting practicalities during early responses to the COVID-19 crisis. To properly explain the sovereign decision to border during COVID-19, we contend that it is necessary to open the black box of border policy decision-making. Behind the discrete decision of a powerful ‘sovereign’ actor to border, we conceptualise ‘bordering’ as the accumulation of different actors situated in specific institutional contexts, who are engaging in a continuous process of sense-making and political contestation in response to a crisis. Using a single case study approach, we delve into the domestic conditions that led to Australia’s bordering policy decision.
To open the black box of bordering decisions during COVID-19, we complement and expand insights from CBS, securitization and bio/necropolitics, by drawing on three established theoretical approaches that trace policy processes during crisis – historical institutionalism, expert sense-making, and policy transfer and learning. Through the study of Australia as an archetypal case of sovereign decision-making to border during COVID-19, we seek to understand the complex drivers leading up to a ‘decisive’ act of bordering. We provide new insight into the securitisation framing of crisis to reveal how factors such as history, expert advice and policy transfer/learning informed the bordering sovereign decision. The decision-making process of Australia’s bordering practices during COVID-19 was complex, nuanced and sometimes contested. Most of note, we find expert advice supported this decision despite acknowledgement it was a departure from WHO advice and efforts were made for justification for this departure. It was not an unfettered sovereign process, even if this was the outcome.
This article is structured as follows. First, we consider the dominant theoretical explanations of COVID-19 bordering from Critical Border Studies (CBS) and securitization, arguing that such accounts offer persuasive but incomplete explanations of the domestic processes that input the sovereign decision. We propose to examine three policy processes common in crisis response, historical institutionalism, expert sense-making and policy transfer and learning, to trace the domestic processes involved to border in response to this crisis. In the second section we discuss our methodology and data collection. We then explore the case study of Australia’s bordering practices during COVID-19, analysing the process(es) that led to the decision to border through three theoretical lenses on the policy process. In the discussion, we demonstrate how our findings complement critical theories of bordering and securitization by identifying the historical, policy and expertise-contingent processes that are absent from current explanations of COVID bordering.
Our process-centred contribution provides the field of border studies a framework for examining variation in bordering regimes. Our findings highlight the important role played by domestic experts in Australia’s ‘bordering’ decision-making process, becoming leading sense-makers and supporting the decision to border even against international expert advice, legitimising and justifying government action. Thus, our analysis reaffirms the need to consider the domestic policy process that occurs within the sovereign ‘black box’ and to ground this in the relevant historical, political and institutional context.
Theorising Borders
In explaining why states such as Australia implemented border closures during COVID-19, much of the nascent literature has drawn upon the literature of Critical Border Studies (CBS) (Cole and Dodds, 2021; Dodds et al., 2020; Ferhani and Rushton, 2020; Lara-Valencia and Laine, 2022). Such a focus is unsurprising, considering CBS is directly concerned with the question of why states engage in bordering. For CBS scholars, borders must be understood in two intertwined ways. First, rather than a concrete concept of ‘the border’, they focus on bordering practices. Bordering practices are ‘activities which have the effect of [. . .] constituting, sustaining, or modifying borders’ (Parker and Adler-Nissen, 2012: 776). Borders mark out, police and negotiate political space but they do so in myriad ways and in multiple locations, such as traveller pre-screenings (Amoore, 2006), offshore asylum seeker processing (Mountz, 2010), quarantines and detention at hotel sites (Jerrems et al., 2023), the deportation of immigrants (Collyer, 2012) and other practices. This draws attention to the way bordering occurs not just on the edges of a sovereign state, but online, through algorithms, inside the state, outside of it (such as via the practices of commercial and civil society actors), and on the bodies of specific groups and individuals more than others. The second key insight CBS provides to understanding borders is an emphasis on bordering as performance. Borders are ‘continually performed into being through rituals such as the showing of passports, the confessional matrix at the airport, and the removal of clothing’ (Parker and Vaughan-Williams, 2012: 729). Specifically, borders are a sovereign performance: they are entwined with the ‘identity-making activities of the nation-state and other forms of political community’ (Parker and Vaughan-Williams, 2012: 729–730).
This notion of bordering as a performative sovereign practice overlaps with ideas of ‘securitization’. ‘Securitization’ broadly refers to the intersubjective construction of an issue as an existential threat to the population, functioning, or existence of the state, centralising sovereign power and permitting leaders to enact emergency measures that otherwise would be viewed as unacceptable (see Buzan et al., 1998). Within this are two crucial ideas about security. First, security is a construction, one that is centred on the antagonism between the Self and Other (or ‘friend’ and ‘enemy’). This has been a particularly popular way to understand the rise of ‘global health security’, where disease outbreaks are constructed as external security threats to protect the state from (Davies, 2008; McInnes and Lee, 2006; Rushton, 2011). Second, this construction of security enacts a unique political modality, or an ‘exception’ where the sovereign is empowered to act unfettered by normal rules and norms (Huysmans, 1998; Williams, 2003). While some CBS scholars discuss the role of security in bordering or similar ideas, others have made this conceptual overlap between CBS and securitization explicit. Borders are thus understood as ‘intense sites of securitization’ (Côté-Boucher et al., 2014: 196), where this construction of threat results in extreme sovereign practices. This is exemplified by readings of COVID-19 border closures, 3 where they are observed as an ‘archetypal’ emergency measure (Aradau and Tazzioli, 2021: 4–5; Ferhani and Rushton, 2020: 466–467), an ‘extreme’ policy response (Hoffman et al., 2022: 190–191), or a ‘kneejerk reaction to a threat perceived as external’ (Lara-Valencia and Laine, 2022: 665).
In addition to the overlap with securitization, many CBS scholars also highlight the ‘biopolitical’ nature of bordering. Drawing from the work of Michel Foucault, these scholars conceptualise bordering practices as forms of biopolitical management, aimed to regulate the population. Biopolitics is a technology of state power that is fundamentally concerned with regulating biological occurrences at the level of the population, maximising health, optimising economic productivity and controlling risks. Bordering is thus ‘the enhancement of mobility and circulation of populations in order to create new opportunities to sift and cancel out perceived risks within the population’ (Vaughan-Williams, 2015: 7). Some, however, argue that Foucault’s emphasis on the management of life misses the primacy of death in bordering practices. They draw on the work of Achille Mbembe (2019: 66) on necropolitics, which expands Foucauldian biopolitics to focus instead on the sovereign’s power to kill, as well as ‘the practical conditions in which the power to kill, or let live, or to expose to death is exercised’. Bordering practices are thus analysed for their capacity to kill or to create ‘death-worlds’, or ‘new and unique forms of social existence in which vast populations are subjected to living conditions that confer upon them the status of the living dead’ (Mbembe, 2019: 92). Despite their difference in emphasis, however, both biopolitical and necropolitical analyses in CBS highlight an important aspect of bordering, one that infuses the arguments made in relation to COVID-19 border closures. Ultimately, bordering is a blunt sovereign tool, one used to control circulation, manage populations, and consequently, make live and make die.
It is here, at this intersection of CBS, securitization and bio/necropolitics, that analyses of COVID-19 border closures often reside. Ultimately, this work views border closures as an attempt to maintain control over the ‘threat’ or control the ‘bad’ circulation of disease from Others. Border closures and travel restrictions reinforced the ‘perception that the threat is external, foreign’ and provided ‘a form of irrational psychological comfort’ to populations fearing the diseased Other (Bissonnette and Vallet, 2022: 679–680). They reaffirmed the power and authority of the state as the protector of the people, legitimising ‘the agenda of states eager and willing to put surveillance regimes and smart border technologies to ‘work’’ (Dodds et al., 2020: 292). Yet while this may seem a depiction of border closures as mere symbolism, scholars have also highlighted the real and detrimental impacts of these closures, such as the leaving of refugees and ‘irregular’ migrants in ‘permanent quarantine’ (Ozguc, 2021: 63) and the decision to rescue particular citizens while leaving others behind (Ferhani and Rushton, 2020: 471). The focus on border closure provides an incomplete story.
The point of emphasis in CBS, securitization and bio/necropolitics work analysing COVID-19 border closures tends to be on the consequence of bordering, namely, the impact and duration. Bordering is accepted as an executive sovereign decision. 4 We suggest the study of the policy process involved to border is equally important. To what extent the specific domestic policy processes that inform the decision to border is, we propose, underexamined. An appeal for the study of the domestic process does not mean the complete dismissal of the CBS explanation. Indeed, as several scholars have argued, there is a need to evaluate how bordering, securitization and bio/necropolitics explanations overlap with the domestic conditions for bordering. Recent work on ‘border hotels’, for instance, combines bordering and securitization with theories from political geography and analyses of private companies and domestic labour conditions (Burridge, 2023; Jerrems et al., 2023; Lobo and Barry, 2023). This expansion of bordering to study the domestic conditions is one that also fits with CBS and bio/necropolitics and takes us a step closer to grasping the complexity, contradiction and pragmatism behind COVID-19 border closures.
We thus build from the insights provided from CBS, securitization and bio/necropolitics on bordering, to incorporate three established theoretical approaches that could help to explain the policy process that led to the emergence of border closure policies and practices as an option to contain COVID-19.
The first is historical institutionalism, a theoretical lens that emphasises the power of institutions in ‘locking in’ power dynamics and goals, creating a ‘path dependence’ where ‘new’ policy decisions align with historical circumstances (Mahoney, 2000). At a practical level, existing organisational architectures of border security might be repurposed for deployment in crisis situations such as pandemics. Evidence for the impact of policy legacies could include policy makers and public commentators comparing and equating current threats to historical bordering imperatives and the repurposing of existing bordering instruments and infrastructure for the pandemic response (Hajer, 2009). Historical institutionalism also emphasises the importance of timing and sequencing of events and processes. As Pearson and Skocpol suggest, in path dependence processes, the order of events can make a fundamental difference in political developments (Pierson and Skocpol, 2002). Relative timing matters because processes occurring during particular periods can generate irreversibility that removes certain options from the subsequent menu of political possibilities (Pierson and Skocpol, 2002).
Second, in a crisis, the evidence available impacts how events are understood. The impact of expert advice on COVID-19 bordering policy decisions deserves greater attention. Experts can play significant roles in political decision-making processes (Fischer, 1990; Howard, 2021; Pielke, 2007). They have been identified as prominent in much of the domestic policy debate during the pandemic (and for the most part, irrespective of political regime), leading some to argue that COVID-19 has rehabilitated the social and political authority of expertise after period in which the ‘death of expertise’ was proclaimed (Boin et al., 2021; Van Dooren and Noordegraaf, 2020). During crises, policymakers wrestle not only with the gravity of the threat and the enormity of the stakes involved; they also must cope with pervasive uncertainty, governing in a state of sustained ignorance (Boin et al., 2021). One of the key functions of experts during these periods of crisis relates to sense-making, helping decision-makers cope with highly ambiguous contexts such as the one created by COVID-19 (Boin et al., 2021). Sense-making refers to ‘the social and cognitive processes of registering and analysing cues, signals and data about and impending threat and imbuing this information with meaning’ (Boin et al., 2021: 20), the societal struggle to understand what is and what will be happening (Van Dooren and Noordegraaf, 2020). 5
Even though this is mostly a cognitive process that happens in the brains of individuals, it is also a social process, as individuals take into account beliefs, norms and expectations of others when interpreting signals (Boin et al., 2021; Weick et al., 2005). Sense-making is critically important during crises as it directs policymakers’ attention to selected cues, propelling them towards particular interpretations about the development of the crisis, and guiding them towards particular courses of action (Boin et al., 2021). Due to their scientific authority, experts tend to be leading sense-makers. They can also become tools of policy legitimation (Boin et al., 2021; Hodges et al., 2022). While the role of experts in advising governments in relation to domestic responses such as mask mandates and social distancing has been addressed in the current literature (Busse et al., 2022; Capano et al., 2020), the impact of expert sense-making on border policies has not received systematic attention. 6 To address this, this article focuses on their role in bordering decision-making processes.
Finally, a third potential explanation of bordering responses is policy transfer and learning – the deliberate or unconscious drawing of lessons from other jurisdictions in real or delayed time (Dunlop et al., 2020). This typically refers to learning and transfer between states, but it can also occur between states and non-state actors, including international organisations such as the WHO (Stone, 2012; Worsnop, 2017a). As Stone suggests, membership in international organisations can influence policy change in many ways, including through ‘diffusion’ of practices (being learned by ‘osmosis’), by ‘coercion’ (e.g. IMF and conditionalities), or just by participating in conferences and consultations within the organisation (2012). Furthermore, countries can learn not to emulate others, especially where they perceive existing approaches to be failures or unsuited for their own circumstances. A further complicating factor for policy learning and transfer in the early months of the global spread of COVID-19 was the speed of the unfolding crisis, the uncertainty surrounding the behaviour of the virus and the effects of policy responses in other parts of the world, along with the imperative to act quickly to prevent outbreaks (Boin et al., 2021; Lee et al., 2020: 1594). These conditions can actually encourage countries to eschew policy learning in favour of a rapid precautionary bordering response, to gain a kind of ‘first mover advantage’ and prevent any outbreaks (Worsnop, 2017b: 20; Worsnop et al., 2023). Among jurisdictions trying to get ahead of the pandemic we should expect to find a (condensed) process of political ‘sense-making’, drawing on information about existing responses in other countries, with narratives and impressions of the policy performance of other countries playing a role in shaping local responses.
Our aim is to uncover the processes prior to the decision to determine if they can add clarity and nuance to explanations of COVID-19 bordering, and better account for departures from international advice intended to facilitate coordinated action among states (Lee et al., 2020).
Methods and Data Collection
To understand the sovereign decision to border requires a study of the everyday politics that informs policy outcomes (Adler-Nissen and Pouliot, 2014). Domestic policy and political processes, particularly during a crisis, involve multiple actors operating in concert (Boin et al., 2005; Rosenthal and Hart, 1991). These include references to a history of responding to crisis, that is, this is how we manage crises of this kind; deferring to formal policy and legislation that elevates the role of experts as ‘knowledge holders’ to guide policy; and evidence that the decision-making process in real time is responding to feedback mechanisms, which can include opinion polls, editorials, media briefings and study of similar responses to crises in other locations (Boin and ’t Hart, 2010; Cairney and Wellstead, 2021; Hoppe, 2005; Wood, 2019).
We selected Australia as an ideal case study for three reasons (Bengtsson and Hertting, 2014). The first reason for selection is that Australia, unlike some other early movers, is not an authoritarian regime or a country with a low-capacity health system, which are usually the features identified (to date) for states to be more likely to exhibit non-compliance with the IHR (Worsnop, 2017b, 2019). Second, like other early movers such as Japan and New Zealand, Australia has an established reputation for securitization practices that include adopting border restrictions. In the case of public health emergencies, Australia adopted border restrictions that exceeded the Temporary Recommendations for PHEICs (Public Health Emergency of International Concern) on Swine Flu/H1 N1 in 2009, Ebola in 2015 and Zika in 2016. Likewise in COVID-19, Australia was one of a small number of democratic, high-income countries that support WHO yet moved first (in February) to impose a raft of border restrictions that well exceeded WHO advice. Third, despite Australia’s early sovereign decision to border (and previous practice of bordering), it is not clear that Australia is against the IHR or WHO. Australia was a key player in the revised IHRs process and is invested in regional diplomacy to promote the IHR core capacity requirements (Davies et al., 2015).
This case leaves open a variety of domestic actors – experts, politicians, bureaucrats and the public – whose preferences need to be captured to trace and reconstruct the processes that informed the decision to border. It is not physically possible to interview all of these groups on their views concerning the border decision. Therefore, we decided to rely on primary sources for qualitative content analysis of the political, administrative and policy processes. This required us to collect diverse sources of non-numerical data to capture the knowledge and views held by experts, politicians, bureaucrats and the public in Australia in the lead up to the initial decision to border in January and apply further border restrictions over February and March. Our qualitative content analysis thus covers the period of January to April 2020.
Content analysis can be defined as a research method or technique that uses a set of procedures to make replicable and valid inferences from texts (Krippendorff, 2008; Weber, 1990). Qualitative content analysis involves the systematic analysis of textual information, including a variety of texts from official (e.g. government reports and administrative records) to cultural (e.g. newspaper articles or editorials) and personal (e.g. letters or diaries) documents (Halperin and Heath, 2020). Being an unobtrusive method of data collection, qualitative content analysis reduces bias – vis-à-vis more obtrusive methods such as surveys and interviews – and allows the systematic analysis of a larger number of documents than would be possible through either interviews or direct observation (Halperin and Heath, 2020). We analysed a large number of texts (official and cultural documents), tracing Australia’s ‘bordering’ decisions made during the period of analysis, along with the justifications being made for those decisions, and the persistence of those decisions overtime (do they endure when the public hears about them). This approach allowed us to study the decision-making and the policy process in Australia in sufficient depth. Through analysing texts, we made sure we captured the persons involved in the process (official documents) as well as the responses (cultural documents), and the interactions between decision-makers, experts, commentators and the public in real time.
This data collection involved sourcing multiple texts. First, we wanted to establish it was the case that Australia’s border decision contravened WHO’s guidance. We sourced all WHO travel advice published as statements for the period of analysis, and we compared Australia’s bordering timeline with the data on ‘international travel controls’ for all countries between January and April 2020 from the Oxford COVID-19 Government Response tracker (secondary source). Second, we collected 159 official documents from the Australian government, including 91 Chief Medical Officer’s media communications (statements, press conference and media appearances transcripts), 19 National Cabinet statements and communications, 38 Australian Health Protection Principal Committee (AHPPC) statements, 10 parliamentary discussions transcripts and one Australian National Audit Office (ANAO) Auditor-General Report. These documents capture the practice of expert advice provided to the Australian government, the bureaucratic practice of communicating policy to politicians, and the practice of communication on decisions made by politicians to the public during the crisis. Third, we sourced media articles, editorials and opinion polls available through Factiva, ProQuest and EBSCOhost databases to discern domestic public views on bordering. These sources were identified as evidence of feedback mechanisms from the public and experts who were outside of the formal policy process. We used the search terms (virus or corona or covid) and (flight or travel or border) to capture both articles that mention COVID
We then coded all the primary source texts. Coding can be understood as the ‘operations by which data are broken down, conceptualized, and put back together in new ways’ (Strauss and Corbin, 1990: 57). It involves the identification of passages of text and the application of labels to them that indicate they are examples of a particular thematic idea (Halperin and Heath, 2020). We followed an inductive coding process considering existing explanations from public policy literature. 7 Our inductive coding process involved two steps. First, we coded all texts for policy recommendations that referred to any mentions of ‘travel restrictions’, ‘travel bans’, ‘border measures’ and similar combinations. Second, we then coded all texts with the following existing explanations for bordering practice in mind: legacy/historical institutionalism, experts’ advice, and policy transfer and learning, in order to assess the justifications provided for Australia’s bordering decision-making process during COVID-19, and community responses to those decisions. Once the two-stage coding was completed, we looked for patterns between the recommendations and explanations relevant to our research question.
Case Study: Australia’s Bordering Practices During COVID-19
Why did Australia adopt bordering practices during COVID-19? If we analyse Australia’s response through the CBS and securitization theoretical lenses, we seem to have a clear answer: this is an archetypical securitization case, a sovereign performance of a decision to border through an established pattern of strict bordering practices to protect the country from an external threat. Indeed, if we adhere to the securitization framework, border closures can be easily read as the ‘emergency measure’ enabled by successful ‘securitizing moves’. The key components of a securitizing ‘speech act’ are all apparent: the referent object, the (external) threat and the resulting logic of exceptionalism.
Australia was clearly and repeatedly positioned as the referent object in need of ‘protection’. Throughout the analysed statements and communications, Australia’s stringent measures (including its bordering practices) were represented as necessary to ‘protect the community’, to ‘keep Australians safe’, to ‘save our vulnerable Australians’, to ‘protect Australian lives’ and to ‘protect Australia’s health’. Australia’s Health Minister Greg Hunt used these concepts regularly in press conferences and official statements when explaining Australia’s border response (see, for example, Department of Health and Aged Care, 2020f, 2020g).
The ‘threat’, of course, was COVID-19, but the construction of this threat was striking in its emphasis on the external nature of the danger. From January to March 2020, the government’s official narrative focused on the ‘external’ nature of the danger and the returning citizen or visitor as the main source of risk to the country: National Cabinet statements tended to highlight that most cases in Australia were ‘overseas acquired’ or ‘imported’ from overseas. Accordingly, as Deputy CMO Paul Kelly mentioned in early March 2020, the Australian government tried to ‘contain it [the virus] beyond our borders’ (Department of Health and Aged Care, 2020c). This aligns with the framing from securitization, particularly that within global health security work which has highlighted how disease outbreaks tend to be represented as external threats to protect the state from (Davies, 2008; Rushton, 2011, 2019).
Finally, these constructions of threat and referent object were grounded in a logic of exceptionalism. COVID-19 was repeatedly referred to as an ‘emergency’ requiring ‘extraordinary’ measures that would otherwise not be justifiable. Australia’s Chief Medical Officer (CMO), Dr Brendan Murphy, for instance, acknowledged in June 2020 that these measures were ‘not normal public health policy’, but insisted that they were necessary due to the threat of importation (Probyn, 2020). We can see within this the idea that COVID-19 invoked a unique political modality – the exception – that enabled the sovereign to act unfettered by normal rules and norms (Kenwick and Simmons, 2020).
Yet, as has been argued elsewhere, there are some gaps in this reading of the Australia case, namely, questions concerning just how ‘sovereign’ this process was (Kirk and McDonald, 2021: 7). While CBS can account for the sovereign decision to border, it does not account for the process that led to the decision to border – the domestic factors that influenced and informed the decision-making policy process. Hence, we must delve further into the specifics of practices behind the decision, and probe to what extent there was variation and contestation. In this section, we complement and expand the insights from CBS with three additional theoretical approaches to explain the option to border as a policy practice in one domestic context.
Historical Institutionalism
Australia is often noted for its history of ‘strong bordering’: the Australian settlement of the early twentieth century institutionalised trade protectionism and racially selective immigration programme (the ‘White Australia Policy’) geared around the nation’s biopolitical needs (‘populate or perish’, expansion for national defence and economic growth), and explicitly cast certain overseas populations as threats to national security (Devetak, 2004). While the White Australia Policy was officially disbanded in the second half of the twentieth century, some see its institutional and political legacy in Australia’s more recent practice of offshore detention and overseas resettlement of asylum seekers, as well as Australia’s strict biosecurity border regime designed to protect agricultural industries from imported pests (Bashford, 2002). More specifically to our case study, Australia has a pattern of using borders to manage disease outbreaks, as the country’s response to the Ebola outbreak of 2013–2016 shows. Two months after WHO’s declaration of the Ebola outbreak in West Africa as a PHEIC in August 2014, Australia had adopted one of the strictest bordering practices in the world. By the end of October 2014, the Australian government had enhanced border screenings and temporarily suspended visa applications for citizens of Ebola-affected countries. These restrictions were soon extended to cover all individuals that were not Australian citizens or permanent residents (Gilbert, 2016; Rhymer and Speare, 2017).
There is a policy apparatus necessary for the functioning of bordering and historical institutionalism played a significant role shaping Australia’s bordering during the COVID-19 crisis, particularly in terms of path dependence and in the sequencing of events that occurred immediately before Australia’s COVID-19 response begun in January 2020. In terms of path dependence, in addition to a history of strong bordering, several already-existing institutions and plans shaped the decision-making process (Fenna, 2021). Emergency frameworks had been developed over decades, including the National Health Security Act 2007, the National Security Health Agreement (2011), the National Health Emergency Response Arrangements (2011) and the Emergency Response Plan for Communicable Disease Incidents of National Significance (2016). Disease-specific plans had also been established, most notably the Australian Health Management Plan for Pandemic Influenza (2019, AHMPPI), which became the basis for the Covid-19 Plan (Australian National Audit Office, 2021).
Besides providing a framework for roles and responsibilities during a health crisis, these plans propose principles, approaches and policy instruments that can shape government bordering responses to threats such as COVID-19. Bordering practices such as closing borders and quarantining people arriving to the country were options suggested in the National Action Plan for Human Influenza Pandemic of 2006 and in the FLUBORDERPLAN of 2009, although only for ‘some situations’ and to be implemented for a limited duration, considering economic, political and social factors. Not all elements of bordering policy recommendations were planned. In fact, as the ANAO audit of 2021 states, at the onset of the COVID-19 Pandemic ‘Australia did not have any current planning in place to support the implementation of travel restrictions or mass quarantine of arrivals in response to a communicable disease pandemic’, as the AHMPPI 2019 did not include these measures, and the FLUBORDERPLAN, which did include them, was decommissioned in 2019 (Australian National Audit Office, 2021). 8 But there was prior record of the policy option to border and, indeed, the practice. The question then turns to what did science recommend on bordering for a government exploring this as an option in response to the crisis.
The Formal Inclusion of Expert Advice
The Australian government relied openly and heavily on expert advice during the COVID-19 crisis. There were four key expert bodies assembled to inform the Australian government – or the National Cabinet–from January 2020. Public health, medical and scientific experts were represented on the Australian Health Protection Principal Committee (AHPPC), the Communicable Diseases Network Australia (CDNA), the Public Health Laboratory Network (PHLN) and the Australian Technical Advisory Group on Immunisation (ATAGI). All were presented in media briefings and policy statements as playing a central role in federal and state governments’ decision-making. Expert advice and appearances were increasingly brought into the government’s press conferences throughout the pandemic response. The experts’ role was made explicit in the government’s narrative, with constant praising of their ‘frank and fearless’ medical advice. Minister Hunt often highlighted their centrality in the decision-making process by claiming that ‘where they have advised, we have adopted’ (Department of Health and Aged Care, 2020g). Experts played a significant sense-making role in Australia’s bordering decision-making process during COVID-19 in two main ways: establishing the nature of the threat and determining the best way to respond.
During the first months of 2020, experts played a vital role in defining COVID-19 as ‘serious’ but ‘external’ and ‘containable’. In terms of determining the ‘seriousness’ of the threat, the first significant action in this regard was the listing of COVID-19 as a human disease under the ‘Biosecurity Act 2015’ on 21 January, before WHO declared COVID-19 a PHEIC on 30 January, activating the country’s response mechanisms. The decision was communicated directly by CMO Murphy to Minister Hunt on 20 January through a phone call, expressing his concerns about the potential of COVID-19 becoming a major health crisis (Margo, 2020). CMO Murphy explained the process in more detail in Parliament on 23 April, stating that at the time he considered the evidence coming from China between 19 and 20 January regarding significant human-to-human transmission as ‘game-changing’ and a ‘significant risk’ that needed to be addressed. From January onwards, the AHPPC and the CMO Murphy – and deputy CMOs – played an active role communicating the level of risk and preparing the population for the actions that would follow.
The second sense-making element regarding the nature of the threat, highlighted in most experts’ public communications between February and March 2020, was the ‘external’ character of the risk. As previously mentioned, the AHPPC and the CMO Murphy narrative in the first months of 2020 focused on the ‘importation’ of cases as the main source of risk in the country, recommending bordering measures to ‘deal with’ or to ‘reduce’ the external ‘traffic’. Australians coming back from overseas were presented as the main threat for the country (Department of Health and Aged Care, 2020a). In April 2020, CMO Murphy reaffirmed this in Parliament stating that the ‘greatest risk’ to uncontrolled transmission had been in ‘imported cases’ since January 2020.
Finally, along with being ‘serious’ and ‘external’, the health experts believed that the virus was ‘containable’: an assessment that would directly influence the bordering measures recommended at the time. On 2 February 2020, CMO Murphy addressed this issue explicitly, justifying the approaches taken by then which included screenings and a travel ban against China, and suggesting with further bordering actions the virus was ‘capable of containment’. Deputy CMO Paul Kelly corroborated this idea in early March, stating that their efforts were focused on containing the virus ‘beyond our borders’. Geography was identified as significant for reinforcing the idea that containment was an ‘effective’ option for Australia, as later reflected on by CMO Murphy in April 2020 stating that as an island, the country was in a position ‘of perhaps doing border measures more effectively than other countries’ (Parliament of Australia, 2020d).
The experts’ sense-making role was crucial in defining the best way to respond to the threat. Under the AHPPC, the role of the assembled experts led by the CMO was to assess the data and recommended to government advice to inform the policy instruments. Notably, of all the recommendations offered by the AHPPC, bordering measures were considered the most important policy instruments adopted in the early response according to CMO Murphy while answering questions in Parliament on 23 April 2020 (Parliament of Australia, 2020d).
Indeed, as Table 1 shows, it was health experts who advised on major bordering decisions (with exception of the decision to ban outward travel) adopted by government in the first months of 2020:
Public Health Advice to the Australian Government for Australia’s COVID-19 Travel Restrictions, January–March 2020.
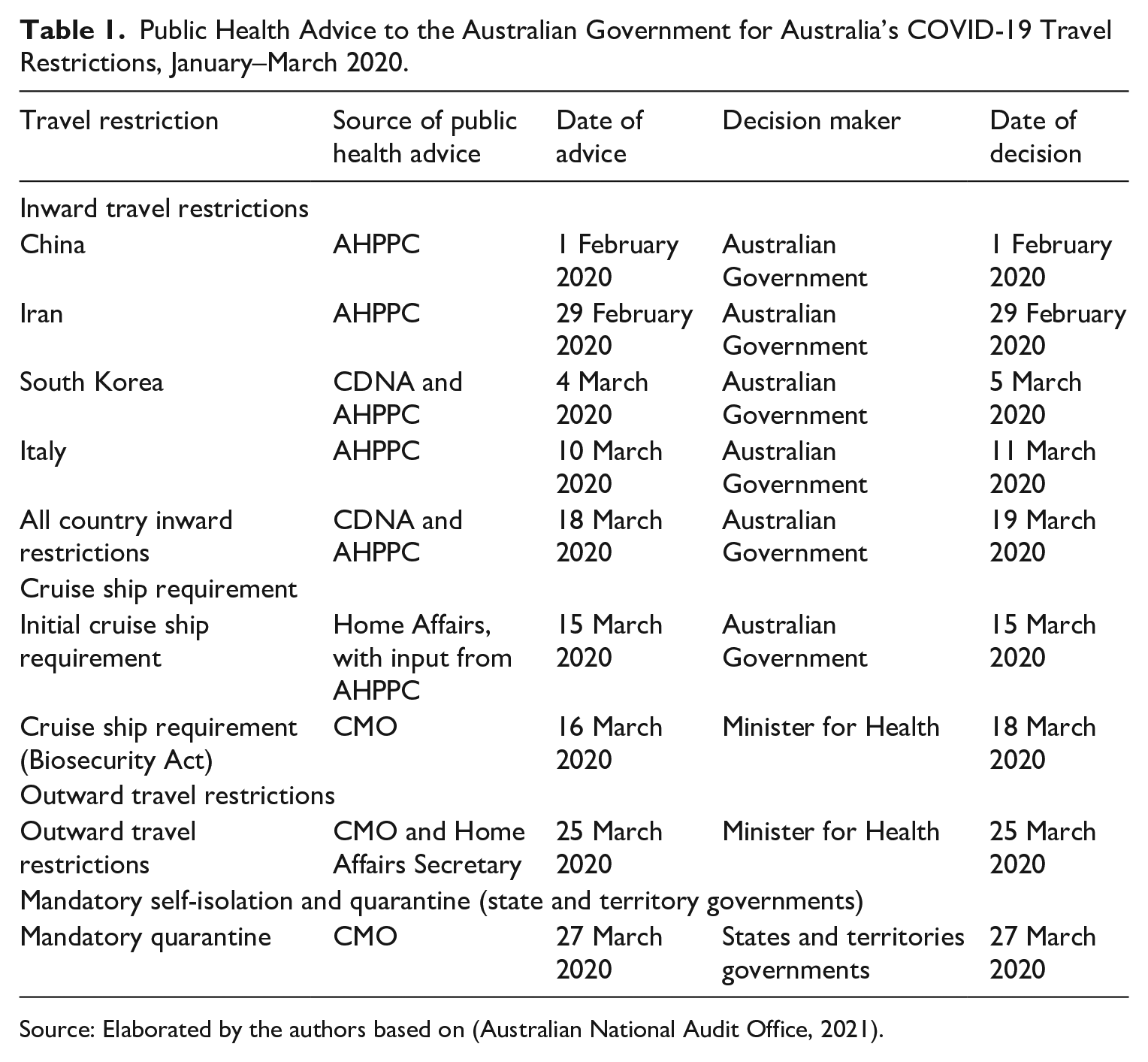
Source: Elaborated by the authors based on (Australian National Audit Office, 2021).
On the decision to recommend bordering, the experts’ narratives reveal some initial unease to be going against international expertise, and particularly, against WHO recommendations and rules. Most of the AHPPC’s public communications during January 2020 mentioned that WHO’s recommendations were against any travel bans concerning China. At the time, Australia’s Deputy CMO Dr Paul Kelly suggested in an interview on 30 January that Australia’s approach did ‘technically’ follow the International Health Regulations (IHR), because the IHR allowed sovereign states to ‘make their own rules’ and their ‘own approaches’ (Department of Health and Aged Care, 2020d). Later, CMO Murphy acknowledged that his advice was against WHO’s rules, but he justified Australia’s decision to take a different approach on several grounds including expert advice he received at the time. On the question of travel restrictions, he acknowledged that Australia ‘took a very different position’ considering the nature of the virus and its epidemiology, but he felt Australia’s decision was still the ‘right one’ in retrospect, having become ‘one of the most forward-leaning countries in the world in border measures’ (Parliament of Australia, 2020d).
The official narrative was thus open about Australia’s ‘very different position’ to the WHO and accompanied with significant efforts to justify the bordering decisions as informed by expert advice. The measures taken before the total border closure at the end of March were often described as ‘proportionate’ in public communications (see, for example, Department of Health and Aged Care, 2020b, 2020d). The use of the word ‘proportionate’ was a deliberate practice intended to trigger recognition that decision-makers consulted with and drew information from experts before settling on policy or course of action (Rubin and De Vries, 2020). Indeed, the authority of expertise and the centrality of their advice in the decision-making process rapidly intensified, a situation that was acknowledged by CMO Murphy on several occasions by stating that ‘both federal and state, have at all times been advised by the consolidated national advice from the AHPPC’ (Parliament of Australia, 2020d).
Once it was established that bordering was the course of action and it was openly supported by experts, the government’s bordering approach enjoyed support across parliament for the entire period of analysis, 9 with only a few exceptions such as brief comments from Senator Faruqi (from the Australian Greens Party) denouncing the government’s ‘alarmist’ and ‘xenophobic’ China travel ban. The main opposition party, the Australian Labour Party (ALP), was at the time explicit in their support, with ALP Senator Green’s intervention on 26 February stating that ‘Labour recognise that the government’s travel ban is based on medical advice, and we support those measures to protect Australians’ (Parliament of Australia, 2020e).
Rare criticism from the Opposition focused only on the specific implementation of some measures, rather than the overall bordering approach. For instance, on 5 March, the Shadow Minister for Foreign Affairs, ALP Senator Penny Wong, questioned the government’s repatriation of Australian unaccompanied minors stranded in Hubei (Parliament of Australia, 2020b, 2020c). Indeed, the most contested decision in the period of analysis was where the travel bans applied. Several MPs questioned the reasoning behind the decision to establish travel bans for some countries and not others. On 2 March, 9 days before WHO declared COVID-19 a pandemic and the recommendation on no travel restrictions was still in place, Senators Jacqui Lambie and Penny Wong questioned government officials about the decision to adopt a travel ban to Iran and not a similar one to South Korea, considering that the latter had more reported cases than the former at the time (Parliament of Australia, 2020a, 2020c). Notably, no politician objected to the bans or raised Australia’s contravention of WHO’s advice. The lack of challenge to the government’s bordering approach could be seen as indicative of an effective use of discursive coercion (Schmidt, 2022), having been able to persuade potential opposing actors of the necessity and appropriateness of the measures with a discourse/narrative legitimated by the experts.
The media held a generally positive view on the border restriction policies being adopted by the Australian government. Editorials between January and March 2020 placed great faith in experts and Australia’s ‘solid’ institutions (The Australian, 2020b). Journalists agreed that restrictions were necessary, framing compliance as part of the ‘Australian Spirit’, described as possessing qualities of ‘acts of kindness, self-control and patience’ (The Australian, 2020a). The tone towards border closures was generally optimistic from January to early March, with the government praised for being proactive and responsive. Indeed, the only criticism in this period was whether experts recommended the adoption of travel restrictions fast enough (Clun, 2020; Holden, 2020).
In terms of public opinion, Australians were surveyed on several occasions in the reference period about their attitudes towards COVID-related border restrictions. Support for bordering policies grew with awareness of the severity of the crisis. Australia was an outlier. 10 A 24 March Ipsos poll found Australian responders ‘Agreement with closing our borders has increased substantially, up from 69% from the last survey on a week ago to 83%’ (IPSOS, 2020b). Another Ipsos international survey conducted between March and April asked if people believed travel and self-isolation would be ineffective (IPSOS, 2020a). Australians started out with a majority feeling it would be ineffective, but had the largest shift, consistently towards greater belief in the effectiveness of restrictions. This contrasts with other countries, where the numbers supporting effectiveness of border closures moved up and down throughout the period (IPSOS, 2020a).
Expertise lay the early groundwork that legitimated the policy option (which was historically path-dependent) for Australia to border. This was not a knee-jerk sovereign decision justified ad hoc. Expert advice served to validate Australia’s bordering practices given they played a major role in sense-making during the early stages of COVID-19, both defining the nature of the threat and the best way to respond to it. Expertise was referred to by the government, opposition and media to justify the bordering approach. Indeed, experts themselves justified the need to contravene the international expert body – WHO – advice on the grounds of ‘effectiveness’. Historically, as established above, the policy option to border was available to Australia, but what evidence existed at the time to presume border closures were effective enough to defy WHO’s advice? We now turn to the final process of bordering–policy transfer and learning practices.
Policy Transfer and Learning Practices
Australia’s bordering decision-making process did not occur in a vacuum. It was informed and influenced by international developments. We found that policy transfer and learning practices were another significant driver of Australia’s bordering response during COVID-19. Several bordering decisions adopted by the government came from observing other countries’ decisions in real-time. The China travel ban, the first and one of the most significant bordering measures adopted by the Australian government, was informed by observing then mimicking the actions of other governments. On 27 January, when asked about the possibility of quarantining the passengers of the 43 flights coming from China that day, Murphy dismissed the option suggesting that he was ‘not aware of any first world country that’s doing that’ (emphasis added, Department of Health and Aged Care, 2020b), stating that there was not sufficient evidence of the risk. This approach was revised on 1 February when the travel ban was adopted.
An audit by the Australian National Audit Office of the country’s management of international travel restrictions during COVID-19, published in December 2021, suggests that Australia may have changed its approach after the United States decided to adopt their travel ban on 31 January. The audit shows that CMO Murphy’s advice to federal government on 31 January did not support ceasing flights from China (Australian National Audit Office, 2021). Later that day, the United States introduced their travel ban. The following day, the AHPPC met and changed their approach, recommending additional border measures to deny entry to Australia to people who had left or transited through mainland China. The timing of the change to the AHPPC advice regarding a travel ban suggests that Washington’s decision might have influenced the experts and the Australian government perception that it was ‘ok’ to defy WHO advice. Almost two weeks after the decision, CMO Murphy added more evidence to the policy learning factor in their decision, stating during a press conference that Australia was ‘not alone in the travel ban’ mentioning the United States and New Zealand as examples of developed countries that adopted ‘very similar arrangements’ to Australia (Department of Health and Aged Care, 2020e). 11 Indicating a limited approach to policy learning however, CMO Murphy did not refer to countries such as Japan, Taiwan and South Korea, all of which had also adopted bans.
These events set the course for Australia to ultimately not follow IHR recommendations on travel restrictions but not without careful effort to justify and explain Australia’s position with respect to WHO. As previously mentioned (see ‘expert advice’ section), public communications by government and health authorities often referred to the WHO recommendations and position regarding travel restrictions, justifying Australia’s approach vis-à-vis the IHR on several occasions as ‘proportionate’, and claiming that ‘technically’ Australia did not break any WHO rule (Department of Health and Aged Care, 2020d).
Policy learning can be mimicry, adaptation or rejection. It is important to acknowledge that Australia had time to learn the impact of policy decisions on bordering and these decisions were being remade within the space of hours. Policy transfer and learning practices were another driver of Australia’s bordering response that, in this instance, served to legitimate the practice. Australia looked to other countries for ‘permission’ when considering bordering options. Indeed, the Australian government – and the health experts – used other countries’ actions to legitimate their own bordering choices. Paradoxically, presentation of the decision to border was often communicated as not a rejection of Australia’s effort to coordinate with the WHO, with reference to acceptance of the diffusion of practices and rules within the organisation (e.g. IHR) and active consultation with WHO in the early stages of the COVID-19 pandemic.
Discussion and Conclusion
This article opened with a simple question: Why did Australia border earlier than most other states in response to the outbreak of COVID-19? To date, the nascent literature on COVID-19 border closures, drawing ideas from Critical Border Studies (CBS) and securitization theory, has tended to focus on the sovereign decision to border and its political (and health) impacts. These studies have provided important insights into the role of collective fear, sovereign power, and the effects on those both outside and within borders, but what about the policy processes through which the decision to border was made and legitimated? As we have demonstrated through an examination of the archetypal case of Australia, the policy process to border is shaped by historical legacies and timing, expert guidance, and policy learning from other states. WHO’s advice not to border factored little into the decision-making process (including expert advice) until after the decision to border had been made.
Of course, this argument is not necessarily contradictory to CBS and securitization. While the burgeoning COVID-19 literature has tended to focus on the arguments considering borders as a sovereign performance and a biopolitical or necropolitical tool, other scholars using these theories have explored bordering and securitization as a more nuanced and contested process (see Côté-Boucher et al., 2014; Jerrems et al., 2023; Salter, 2008). Our analysis here thus reaffirms the need to consider the domestic policy process that occurs within the sovereign ‘black box’, and to ground this in the relevant historical, political and institutional context. This may not be as neat or parsimonious an explanation as that provided by sovereign decisionism, but it permits us to better understand how and why particular states such as Australia border at particular times and to particular degrees. It also highlights the possibilities of further fruitful engagement between CBS, securitization and the policy process.
While our focus on a single case study problematizes generalisability, this article still provides important insights concerning bordering and pandemic policymaking. COVID-19 represented a departure from the normal ‘siloed’ structure of expert advice because multiple policy subsystems were implicated in the policy response, involving experts from public health, economics, trade, migration, aged care and social policy. Nonetheless, the historical practice of ‘bordering’ as a policy solution reappeared within the first month of the outbreak and quickly gained public currency. While the importance of historical institutionalism in the Australian response could have been expected, the lack of political contestation – considering that Australia’s bordering approach was one of the strictest in the world – and the centrality of experts in the decision-making process – as leading sense-makers and as ‘policy legitimation tools’ – was a surprising finding. Domestic experts played a central role in the bordering decision-making process. This role was crucial to legitimate government action and Australia’s consequential departure from international expert advice. We found minimal effort was made by both experts and politicians to justify departure from international advice. This justification was accepted by the political opposition and the domestic population. Moreover, we found significantly strong support from the Australian population – increasing overtime – despite the evident negative effects of the bordering measures for sectors of the population (e.g. families of Australians stranded overseas) and the economy (e.g. tourism).
In sum, our policy process-centred contribution provides the field of border studies with a framework to examine conditions for variation in bordering regimes. The Australian government made a decision based on a history of expediency to border, domestic expert advice consensus and learning from watching other situations. Bordering in this case was not an expedient sovereign rejection of international advice but an outcome due to domestic priors that informed how to best control the crisis.
Footnotes
Acknowledgements
The authors thank the Australian Government for the support provided to this research through the Australian Research Council. The authors thank the reviewers and colleagues who provided useful feedback for the different versions of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was fully funded by the Australian Government through the Australian Research Council (DP220100587).