
Abstract
Intimate partner violence (IPV)-strangulation is a significant risk factor for lethality, brain injury, stroke, and mental health issues. As first responders, police officers are well positioned to offer life-saving interventions by identifying strangulation and making referrals to healthcare. However, strangulation training is uncommon, and many strangulation incidents are undetected by police. The current study explored what police officers (n = 71) in British Columbia understand about the risks of IPV-strangulation and when they would refer a victim-survivor for a medical-forensic exam. While officers understood strangulation as a high-risk factor, training is needed to enhance understanding of the importance of medical-forensic exams.
Introduction
Strangulation involves external compression of the neck region such that an individual’s blood circulation and/or airflow are impaired (Faugno et al., 2013). Strangulation that occurs in the context of intimate partner violence (IPV) is an intentional act often used as part of an overall pattern of coercive control towards a current or former intimate partner (Edwards and Douglas, 2021; Joshi et al., 2012; Myhill and Hohl, 2019; Stansfield and Williams, 2021; Thomas et al., 2014). IPV-strangulation is one of the strongest predictors of future lethality (Matias et al., 2019; Spencer and Stith, 2020), increasing the likelihood of femicide more than sevenfold (Glass et al., 2008; Spencer and Stith, 2020). Strangulation tends to co-occur with other risk factors that increase the potential for lethal violence, including threats to kill, the presence of weapons, a victim-survivor’s1 belief that their intimate partner will kill them, stalking, and an overall increased level of severity of violence (Bendlin and Sheridan, 2019; Mcquown et al., 2016; Messing et al., 2018; Patch et al., 2023; Shields et al., 2010; Stansfield and Williams, 2021; Thomas et al., 2014). Strangulation also increases the risk of other physical and psychological harms for those who initially survive the incident, including increased risk of stroke, brain injury, miscarriage, post-traumatic stress disorder, anxiety, depression, and suicide (Bergin et al., 2022; Campbell et al., 2018; Clarot et al., 2005; De Boos, 2019; Faugno et al., 2013; Hawley et al., 2001; Joshi et al., 2012; Macgregor et al., 2016; Messing et al., 2018; Monahan et al., 2022; O’Dell, 2007; Patch et al., 2017; Shields et al., 2010; Smith, 2009; Smith et al., 2001; Strack et al., 2001; Strack et al., 2020; Toccalino et al., 2023; Valera et al., 2019; Wilbur et al., 2001; Wilson et al., 2022). Regrettably, few victims-survivors of strangulation seek medical assistance following the incident, as many are unaware of the potential health risks they now face (Brady et al., 2023; Donaldson et al., 2023; Gwinn et al., 2014; Patch et al., 2023; Smith et al., 2001; Strack et al., 2020; Wilbur et al., 2001; Wilkes, 2023).
Given that police officers are typically the first responders to IPV calls for service where strangulation may have occurred, they are in a unique position where they can screen a victim-survivor for strangulation. Identifying when a victim-survivor has experienced IPV-strangulation should factor into subsequent decision making by police officers regarding victim-survivor safety and should result in potentially life-saving interventions through increased access to medical or forensic exams. However, strangulation training for police officers has been relatively uncommon (O’Dell, 2007; Pritchard et al., 2017, 2018; Reckdenwald et al., 2017; Zedaker, 2018). Consequently, the limited available research suggests that many strangulation incidents go undetected or undocumented by police (Garza et al., 2021; Pritchard et al., 2018; Reckdenwald et al., 2017, 2019). Given the overall lack of research on policing and IPV-strangulation, the current study examined the understanding of the risks posed by IPV-related strangulation among a sample of police officers in British Columbia.
Motivation and methods for IPV-Strangulation
IPV-strangulation is a highly gendered form of violence with upwards of 90% of victims-survivors being female, with a similar proportion of those who strangle being male (Leemis et al., 2022; Thomas et al., 2014; White et al., 2021). While strangulation can involve pushing extremities, such as a forearm or knee, against the throat, or constriction of the neck area by ligature, such as by tightening a belt or dog leash around the neck, most IPV-strangulations occur manually, where pressure is placed on the victim-survivor’s neck with one or both hands (Brady et al., 2022; Joshi et al., 2012; Macgregor et al., 2016; Strack et al., 2001; Thomas et al., 2014). This manual act is often a rage-filled overreaction to a perceived insult or loss of control (Brady et al., 2022; Macgregor et al., 2016; Thomas et al., 2014). During the strangulation, threats to kill, degrading or obscene comments, and victim blaming often also occur, and the victim-survivor may be strangled multiple times to demonstrate the power held over them (Brady et al., 2022; Joshi et al., 2012; Macgregor et al., 2016; Messing et al., 2018; Pritchard et al., 2018; Sharman et al., 2023; Stansfield and Williams, 2021; Strack et al., 2001; Thomas et al., 2014; Wilbur et al., 2001; Wilson et al., 2022). It is not uncommon for the victim-survivor to believe in that moment that they are unlikely to survive (Brady et al., 2022; Thomas et al., 2014; White et al., 2021). Strangulation often occurs alongside other tactics of coercive control, including verbal abuse, isolation, and harassment/stalking, all of which serve as strategies to exert power and dominance over the victim-survivor (Joshi et al., 2012; Stansfield and Williams, 2021; Thomas et al., 2014). Jealousy, perceived infidelity, refusal of intercourse, attempts to end the relationship, or disagreements about the victim-survivor spending time with others may precede strangulation by an intimate partner (e.g., Brady et al., 2022; Macgregor et al., 2016; Thomas et al., 2014). Unfortunately, those who have experienced IPV-related strangulation are often exposed to this violence multiple times as on average, victims-survivors report being strangled on five previous occasions (Brady et al., 2022; Messing et al., 2018; Thomas et al., 2014; Wilbur et al., 2001).
Prevalence of IPV-strangulation
There are a wide range of estimates of how common IPV-strangulation is. The Canadian General Social Survey, which asks Canadians aged 15 years and older to self-report victimization experiences, found that approximately 14% of women and girls who had ever been in an intimate relationship reported being strangled by an intimate partner in the previous 5 years (Conroy, 2021). Indigenous women were more than three times as likely to self-report strangulation compared to non-Indigenous women in Canada (Heidinger, 2021; Sorenson et al., 2014). Similarly, according to the 2016/2017 National Intimate Partner and Sexual Violence Survey in the United States, 16.2% of women reported having experienced strangulation or suffocation at some point in the past (Leemis et al., 2022). In contrast, rates among shelter-seeking populations are much higher. In one of the first published studies on this subject, Wilbur et al. (2001) reported that approximately two-thirds (68%) of abused women accessing a shelter or medical centre in the United States had been strangled by their intimate partner. Similarly, in a sample of 17 women accessing a domestic violence shelter in the United States, all 17 reported prior experiences of strangulation (Joshi et al., 2012; Thomas et al., 2014). Similarly, high rates of strangulation prevalence are found among some samples seeking healthcare. In a study conducted in British Columbia with 205 women who received a forensic nurse examination between 2018 and 2020 for an intimate partner related assault or sexual assault, the majority (60%) had been strangled (Adhikari et al., 2023). In a study conducted in a New Zealand hospital setting, King et al. (2023) found that half (49.7%) of the 660 abused women who sought medical services at the hospital had experienced a prior strangulation.
In contrast to samples drawn from shelters or hospital settings, the limited research conducted to date with police data generally tends to identify a lower prevalence rate of IPV-strangulation. In a sample of nearly 10,000 family violence stalking cases in Australia analyzed by Bendlin and Sheridan (2019), strangulation occurred in 16.6% of the files, while a study that used text-mining to scan 182,949 non-sexual assault and non-stalking IPV police reports in Australia reported that only 3.8% of the reports indicated that strangulation had occurred (Wilson et al., 2022). One possible reason for this discrepancy is that police officers do not always detect when strangulation has occurred, particularly when they have not previously been exposed to strangulation training. Pritchard et al. (2018) analyzed nearly 600 IPV calls for service in Brevard County, Florida, and found that police documented strangulation in 11.5% of these files. However, after the researchers reviewed the files for evidence of strangulation, such as if the officer documented that the victim-survivor stated that their partner had grabbed them by the throat, the researchers identified another 17.1% of files where strangulation had potentially occurred but had not been documented by the police. In a similar study, Garza et al. (2021) found that only 6% of IPV files reported to an urban police agency in the United States involved strangulation, but when the researchers reviewed the files, they estimated that 14.4% appeared to involve strangulation. These findings suggest that police officers who are untrained in strangulation are not recognizing the signs or symptoms of a potential strangulation in many cases resulting in missed opportunities for intervention. Unfortunately, few police agencies appear to have provided strangulation training to their officers (O’Dell, 2007; Pritchard et al., 2017, 2018; Reckdenwald et al., 2017; Zedaker, 2018).
Current study
Several studies have now examined police files for the presence of detected or potential strangulation (e.g., Brady et al., 2023; Garza et al., 2021; Pritchard et al., 2018). However, no prior research has been conducted directly with police officers to assess their understanding of strangulation, the degree to which they perceive strangulation as a risk factor for revictimization in an abusive relationship, or their understanding of the importance of medical interventions for a strangulation victim-survivor. Given this gap, whether police appreciate the risk that strangulation poses to a victim-survivor of IPV and how they respond to strangulation once detected is currently unknown. Therefore, the current study explored police officer understanding of the risks posed by IPV-strangulation and identified areas where future training was desired.
Method
The data for this study was collected through surveys disseminated during in-shift briefings with frontline police officers working in a large urban police agency in British Columbia (BC), Canada. The data was collected by the second author in March 2020.
Participants and procedure
Shortly prior to the onset of the Covid-19 pandemic in 2020, the second author attended four shift briefings where they introduced the study to the police officers as a survey on police responses to IPV. This was intentional to avoid priming the officers to focus on strangulation as a particularly relevant risk factor. The second author distributed a paper copy of the survey and collected the surveys approximately 15 minutes later by passing around a manila envelope for the surveys to be placed into. The surveys were completed anonymously and voluntarily. Those who did not wish to complete the survey were instructed to leave the survey blank and return it when the envelope was passed around. The second author then transferred the four envelopes containing each shift’s surveys to the first and third authors who entered them into an SPSS database for analysis.
At the time the survey was conducted, all police officers in the province were required to complete two online courses on conducting IPV investigations. The first course, Evidence-Based, Risk Focused Domestic Violence Investigations, defined IPV and provided an overview of key investigative steps and the management of IPV files. The second course, Assessing Risk and Safety Planning in Domestic Violence Investigations, reviewed various factors for IPV identified in the literature as increasing the risk for repeat or severe/lethal victimization. These courses took approximately 7 hours to complete and were offered asynchronously online. Together, they prepared the officer for how to use the BC Summary of Domestic Violence Risk Factors (commonly referred to as the SDVR) which, at the time of the study 2 , was the risk review template used by police throughout the province to document risk and inform decision making in response to IPV calls for service. The BC-SDVR was introduced in 2009 as an adapted form of the Family Violence Information Report (FVIR) used in Alberta (see Jung and Buro, 2017 for a detailed description of the FVIR). The BC-SDVR measures 19 risk factors organized into four domains: (1) Relationship History; (2) Complainant’s Perceptions of Risk; (3) Suspect History; and (4) Access to Weapons/Firearms. The BC-SDVR is not a formal, validated risk assessment tool. Instead, it is intended to be used as a job aid, for example, to assist officers in making decisions about whether a suspect can be safely released from custody. Officers are instructed to record summary remarks regarding the 19 risk factors. Given this, the risk factors are not quantitatively assessed either individually or in totality. However, several risk factors, including strangulation, are flagged for police as indicators of increased likelihood of future violence.
Research questions and variables
While the literature has identified strangulation as one of the strongest risk factors for lethality, it is unclear whether police officers are aware of this. Thus, the first research question sought to identify how police officers ranked strangulation among the various risk factors for revictimization contained on the BC-SDVR. The second research question explored police officers’ understanding of the importance of a medical-forensic exam for a victim-survivor of strangulation. As frontline police officers who may be the first point of contact with a recent victim-survivor of strangulation, it is imperative that they recognize the signs and symptoms that may indicate that a victim-survivor of IPV is at risk of significant health consequences resulting from strangulation and act appropriately by connecting the victim-survivor to a health care practitioner, such as a paramedic, emergency room physician, or forensic nurse examiner. To assess whether police officers understood this, the survey presented various signs or symptoms of strangulation that a victim-survivor may exhibit and asked the police officer to indicate the likelihood of referring a victim-survivor for a medical-forensic exam if any of the signs or symptoms were present. By assessing this based on a variety of possible signs and symptoms, this research question also explored areas where future training may be beneficial to improve police officer comprehension about the significance of various indicators as possible signs or symptoms of strangulation. The third research question asked police officers to indicate whether they would like future training on IPV-strangulation, and, if so, in which areas. The key variables analyzed in the current study, therefore, included police officer perceptions of risk for revictimization, understanding of the risks posed by strangulation, and their desired areas for future training with respect to strangulation.
Risk for revictimization
Officers were given a list of 23 risk factors, many of which were drawn from the BC-SDVR, and asked to rate the degree to which each increased the risk of future victimization using a three-point scale (1 = low risk, 2 = moderate risk, 3 = high risk).
Strangulation risks
Officers were provided a series of statements exhibiting common signs or symptoms of strangulation and asked to indicate how likely or unlikely they would be to refer the victim-survivor for a medical-forensic exam if the signs or symptoms were present using a three-point scale (1 = very unlikely, 2 = somewhat likely; and 3 = very likely). Of note, officers were also presented with an option of unsure (4), as lack of certainty about the relevance of different signs or symptoms of strangulation would indicate needed areas for future training.
Strangulation training
At the end of the survey, officers were told that one of the areas where research suggests more training may be necessary is on strangulation. They were then asked whether (0 = no, 1 = yes) they thought they were in need of training regarding the warning signs or symptoms of a non-fatal strangulation in the context of IPV. Officers were also provided with a checklist of four areas where they may may want to receive future training on strangulation. Again, responses were collected using a binary measure (0 = no, 1 = yes).
Analytic strategy
Given that this was the first research study to measure police officer understanding of the risks posed by IPV-strangulation, the exploratory research questions were primarily answered using univariate analyses. Bivariate analyses (e.g., chi-square, independent samples t-tests) were also conducted to explore whether any of the results varied by police officer characteristics.
Results
Sample description
In total, 71 police officers participated in the survey. Most participants were male (88.4%). Participants ranged in age from 24 to 54 years of age with a mean of 35.1 years old (sd = 7.6). On average, participants had 4.9 years of service (sd = 9.3) ranging from less than 1 year to 18 years of service.
Perceptions of strangulation as a risk factor for revictimization
Police officer ratings of risk factors for revictimization as high risk (n = 67).
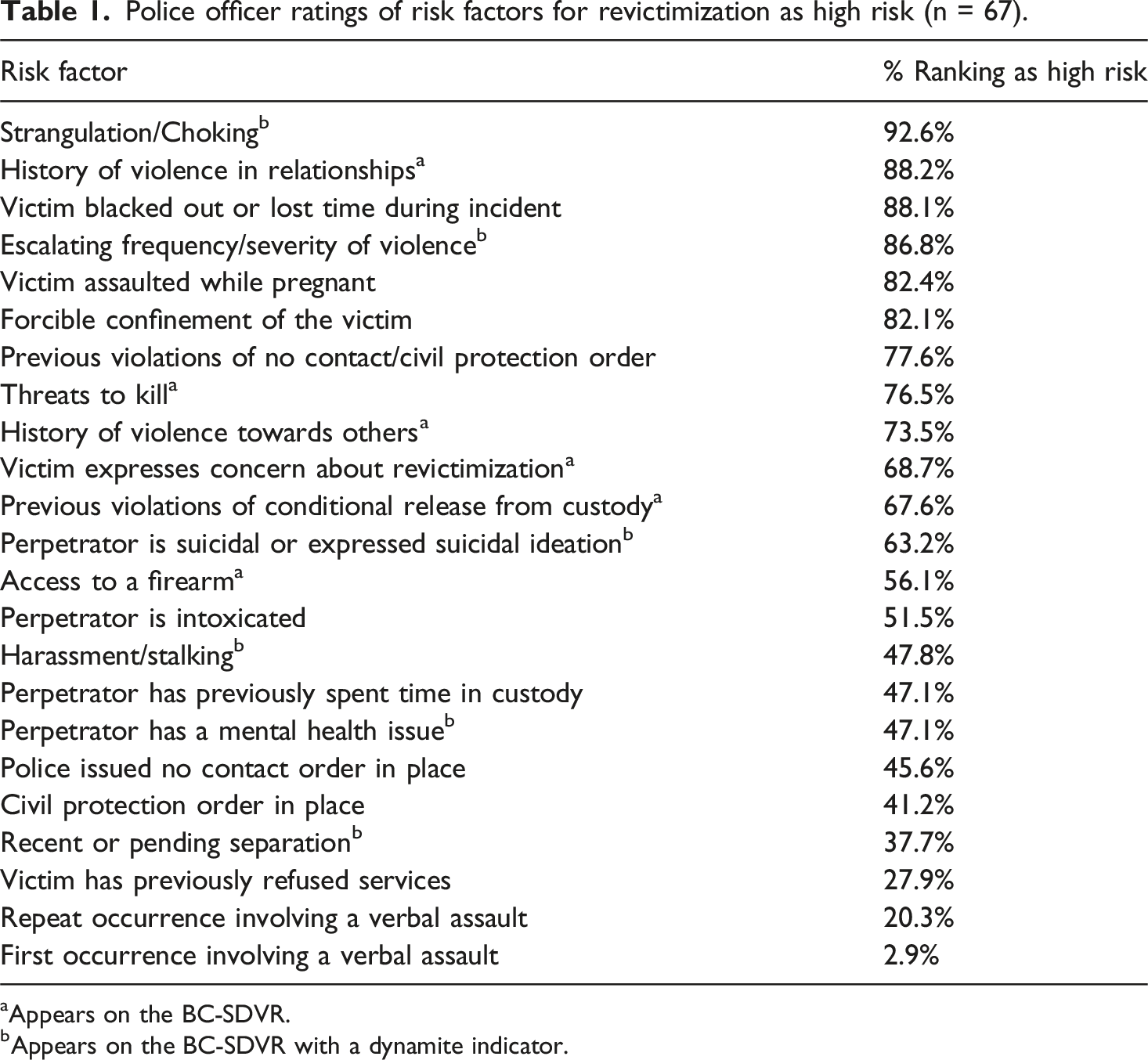
aAppears on the BC-SDVR.
bAppears on the BC-SDVR with a dynamite indicator.
Few officers selected the low risk category, which resulted in violations of chi-square assumptions due to insufficient cell counts. As such, the data was collapsed into two groups (low and moderate = 0, high = 1) to enable comparisons of risk ratings by police officer demographics, including self-identified gender, age, and years of policing experience. Chi-square analyses interpreted using Fisher’s Exact Test because of low cell counts did not detect any gender differences for 22 of the 23 risk factors. The one exception concerned the risk factor of forcible confinement where male police officers (86.0%) were significantly more likely than female police officers (50.0%) to identify forcible confinement as high risk [x2 (1) = 6.03, Fisher’s Exact Test p = .033]. Older officers (Mage = 37.7 years, sd = 8.1) were significantly more likely than younger officers (Mage = 33.2 years, sd = 7.0) to view a civil protection order being in place as high risk, t (60) = −2.3, p = .025. There were no other significant differences based on police officer age, and no statistically significant differences considering police officer years of experience.
Understanding the importance of medical-forensic examinations for survivors of strangulation
Police officer perceived likelihood of referring victim-survivor of IPV strangulation for a medical-forensic exam (n = 70-71).
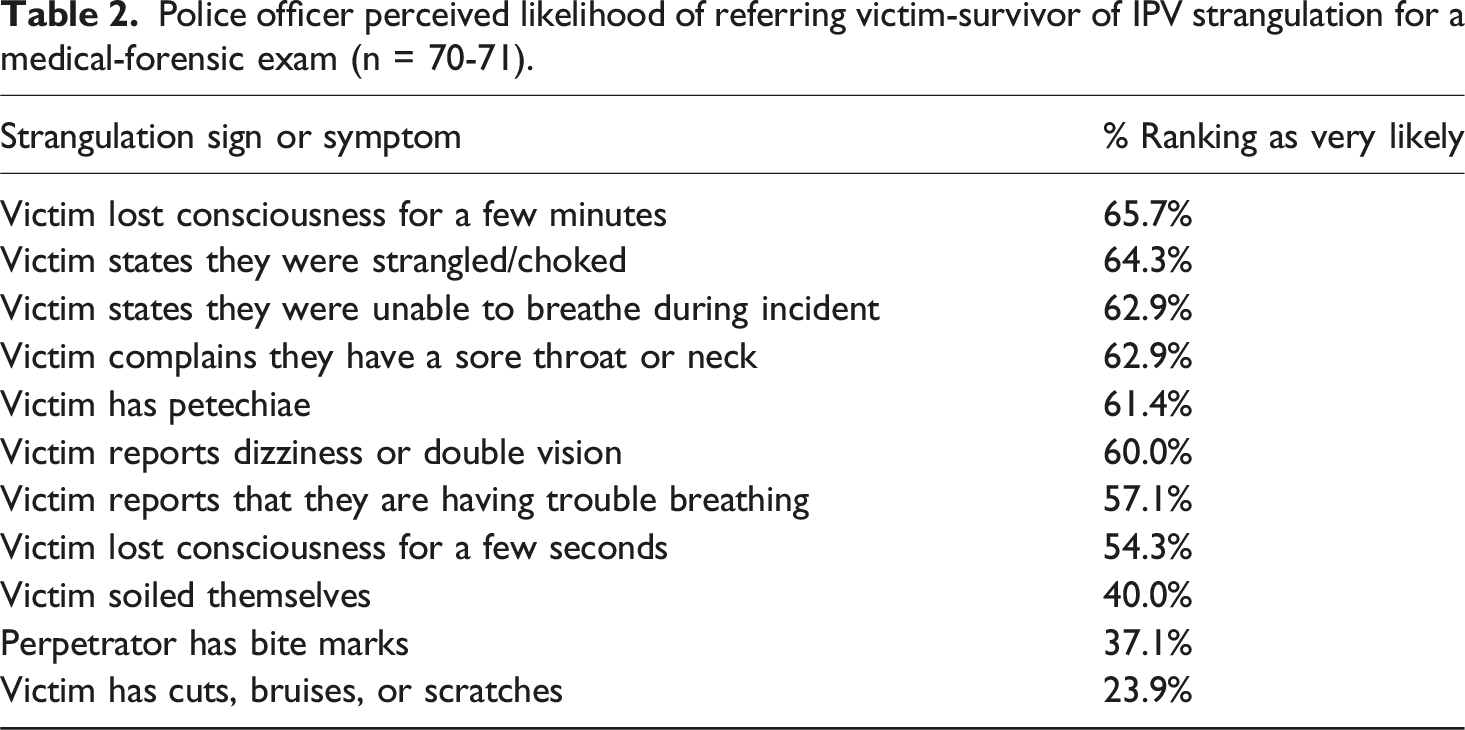
The unsure responses were removed and the remaining responses collapsed into two groups (0 = Very Unlikely or Somewhat Likely; 1 = Very Likely) to assess whether there were any demographic variances in these trends. Female officers were significantly less likely (25%) than male officers (67.9%) to state they would be very likely to refer the victim-survivor for a medical-forensic exam if the victim-survivor reported having trouble breathing, x2 (1) = 5.5, Fisher’s Exact Test p = .044. There were no other differences according to gender. Older officers (M age = 37.4 years, sd = 8.5) were significantly more likely than younger officers (M age = 31.3 years, sd = 4.9) to state they would be very likely to refer the victim-survivor for a medical-forensic exam if the victim-survivor stated that they had been strangled or choked, t (52.1) = −3.5, p < .001. Older officers (X = 37.9, sd = 8.3) were also significantly more likely than younger officers (M age = 33.7 years, sd = 7.6) to state they would be very likely to refer the victim-survivor for a medical-forensic exam if the victim-survivor had soiled themselves, t (55) = −2.1, p = .045. Similarly, officers with more years of policing experience (M age = 5.8 years, sd = 4.3) were significantly more likely than officers with fewer years of policing experience (M age = 2.9 years, sd = 2.7) to state that they would be very likely to refer the victim-survivor for a medical-forensic exam if the victim-survivor stated that they had been strangled or choked, t (52.1) = −3.2, p = .003. There were no other statistically significant differences according to police officer years of experience.
Desired areas for strangulation training
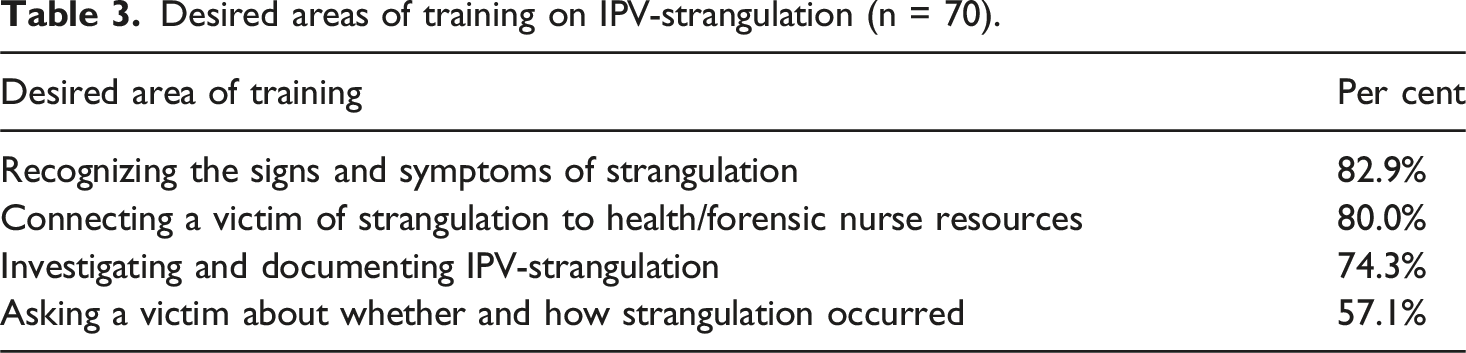
Desired areas of training on IPV-strangulation (n = 70).
Discussion
This study was the first to examine police officer understanding of the risk posed by strangulation relative to other risk factors for revictimization, and to explore police officer recognition of the importance of medical-forensic care following an incident of strangulation. Moreover, it was the first study to examine IPV-strangulation in the context of Canadian policing. The findings of this study suggest that police officers in British Columbia appear to recognize strangulation as a significant risk factor for victimization but would benefit from – and indeed desired – training on conducting IPV- strangulation investigations, documenting evidence of the strangulation, and referring victims-survivors for medical-forensic exams.
It was not altogether surprising that police officers in the current study recognized strangulation as a significant risk factor for revictimization, as it is one of the “dynamite” indicators flagged on the BC-SDVR. However, the risk factors presented included five other dynamite indicators, some of which were not commonly perceived by the officers as particularly high risk despite their flagged status on the risk review tool. This suggests that the police officers in the current study were particularly aware of the risks posed by strangulation, although how they understood it to increase risk to the victim-survivor was not specifically measured. Interestingly, while there were no differences by officer demographics in terms of how participants interpreted the risks posed by strangulation, there were two main differences when examining officers’ response to these cases. Compared to those who were younger or less experienced, police officers who were older and who had more years of policing experience were significantly more likely to agree that they would be very likely to refer a victim-survivor for a medical-forensic exam if they explicitly stated that they had been strangled. One possible explanation for this finding may involve training. While all police officers in British Columbia are required to complete the two IPV-related courses, it is possible that younger or less experienced officers have yet to complete the training resulting in less awareness about the health consequences posed by strangulation. Unfortunately, completion of prior training on IPV generally or strangulation specifically was not measured in the current study.
Although police officers exhibited a strong level of recognition of strangulation as a significant risk for revictimization, they appeared less likely to understand the importance of a medical-forensic exam when victims-survivors presented with possible symptoms of strangulation. A medical-forensic exam is of the utmost importance for a strangulation survivor, as strangulation can cause injuries within seconds and death within minutes (Bichard et al., 2022; De Boos, 2019; Faugno et al., 2013). Whereas the average male handshake can grip approximately 90 pounds of pressure, it takes only 11 pounds of pressure to compress the carotid artery, and 4.4 pounds of pressure to compress the jugular vein (Faugno et al., 2013). The carotid artery transports oxygenated blood from the heart to the brain, therefore, pressure on the carotid artery can result in the brain either being fully or partially deprived of oxygen (Faugno et al., 2013). As the brain does not store reserves of oxygen, loss of consciousness can occur within approximately 15 seconds and death can occur within four to 5 minutes (Faugno et al., 2013). Conversely, the jugular vein returns the deoxygenated blood from the brain to the heart (Faugno et al., 2013; Hawley et al., 2001). Pressure on the jugular vein prevents this blood from leaving the brain resulting in a build-up of pressure and potential petechial hemorrhaging where blood vessels burst, resulting in a pattern of red dots appearing on the skin (De Boos, 2019; Faugno et al., 2013). Impaired blood circulation via the carotid artery or jugular vein compression both increase the risk for death during strangulation and in the days or weeks following the strangulation incident (Douglas and Fitzgerald, 2022; Faugno et al., 2013; Smith, 2009; Smith et al., 2001; Strack et al., 2020). For example, a subset of those who initially survive strangulation may develop a carotid dissection, which increases the risk for a stroke and death (Clarot et al., 2005). Police officers should be made aware of symptoms (reported by the victim-survivor) or signs (observed by the police officer) that may indicate that strangulation has occurred, including the victim-survivor reporting dizziness or light-headedness, experiencing a headache or sore throat, having difficulty speaking or experiencing changes to their voice, experiencing changes to vision, losing control over their bladder or bowels, or reporting loss of or altered consciousness.
In the current study, two-thirds of participants agreed they would be very likely to refer a victim-survivor for a medical-forensic exam if the victim-survivor had lost consciousness for a few minutes. However, this finding suggests that one-third of the officers were only somewhat likely or not likely to refer the victim-survivor for an exam in this instance. Whether a victim-survivor lost consciousness for a few seconds or a few minutes, it is critical that they receive medical attention as this is a sign that blood circulation and breathing were impeded, which increases the risk for serious consequences, such as a brain injury, stroke, or death. Some police officers appeared to differentiate between the significance of losing consciousness for a few minutes compared to a few seconds, as only 54% of officers indicated that they would be very likely to refer a victim-survivor for a medical-forensic exam if the victim-survivor had lost consciousness for a few seconds. However, many victims-survivors will not be able to reliably report how long they lost consciousness for, and that is assuming they even recall losing consciousness at all (White et al., 2021). Victims-survivors may instead report that they lost track of time or ended up in a different location from where the incident began and not being able to remember how they got there. These statements may all indicate that the victim-survivor lost consciousness or experienced an altered state of consciousness during the incident, which increases the risk for subsequent physical and mental health consequences and should result in a recommendation to access a health care provider.
Of concern, less than half (40%) of participants in the current study agreed that they would be very likely to refer a victim-survivor for a medical-forensic exam if the victim-survivor had soiled themselves. Losing control of one’s bowels because of strangulation is relatively rare, estimated to occur in less than 10% of victims-survivors (Mcquown et al., 2016; Shields et al., 2010; White et al., 2021) but it may indicate that the victim-survivor was close to death. In the strangulation timeline, pressure on the carotid artery can result in loss of consciousness after as little as six to 10 seconds, loss of control over bladder after around 15 seconds, and loss of control over bowels after approximately 30 seconds (Carter et al., 2024; Midttun, 2021). Given that these outcomes indicate that the assailant continued to strangle the victim-survivor well past the point of apparent loss of consciousness (White et al., 2021), loss of control over bowels should be considered a significant risk factor for future lethality. However, in the current study, as participants were not instructed to consider these signs and symptoms in light of strangulation, it is possible that the majority of officers were not very likely to indicate that they would refer a victim-survivor for a medical-forensic exam if they had lost control over their bowels because this might have been considered an outcome of something else, such as substance misuse or abuse. Still, given its significance to potential lethality in the context of strangulation, police officers should be trained that if a victim-survivor of strangulation lost control over their bowels, this is a significant risk factor that should quickly result in the provision of medical care. Moreover, police officers should be trained that victims-survivors may be embarrassed about losing control over their bladder or bowels (White et al., 2021). As a result, they may change their clothes before speaking to a police officer. Given this, it is important for police officers not only to ask about whether the victim-survivor experienced incontinence but also to ask whether they changed their clothes following the incident and, if so, to allow the officer to examine the clothes.
Police officers seemed to recognize that they would benefit from receiving more training on IPV-strangulation. Participants wanted training about how to recognize the signs and symptoms of non-fatal strangulation, and when and how to connect a victim-survivor to a medical exam. Police officers were least likely to desire training on when and how to ask an IPV victim-survivor about experiencing strangulation. This is likely because police officers in British Columbia already ask victims-survivors about strangulation as part of the BC-SDVR tool. However, it is important to study this further as officers are not necessarily guided about what questions to ask victims-survivors. For example, it would be helpful from both a healthcare and legal perspective to establish how many times the strangulation occurred in the current incident and whether strangulation has occurred in the past, what the method of strangulation was in the current incident, what else was said or done during the strangulation (e.g., threats to kill, verbal abuse, slapping), what ended the strangulation, whether the victim-survivor lost track of time during the incident, if they recalled experiencing incontinence and whether they changed their clothes, whether they were able to breathe during the strangulation, whether the victim-survivor’s feet left the floor during the incident, how much pressure they estimated was placed on their neck, whether they believed the assailant was going to kill them, and what signs and symptoms they are experiencing now. Critically, officers should be trained that all victims-survivors who report experiencing strangulation or possible strangulation be immediately referred to a health care practitioner, such as a forensic nurse examiner or emergency room physician.
While this study was the first to examine IPV strangulation in the context of policing in Canada, the sample was drawn from a single police agency in British Columbia. Consequently, it is not representative of police officers in other jurisdictions throughout Canada. While all police officers in British Columbia complete the same IPV training courses and use the same risk review tool when investigating IPV files, the participating agency may differ in important ways from those elsewhere in the province, such as agency size and location, police officer characteristics, exposure to IPV calls for service, or department focus on the relevance and importance of strangulation in IPV files. Still, the study findings revealed important areas for future training with respect to conducting strangulation investigations and the importance of obtaining medical-forensic exams for victims-survivors. However, it did not examine police officer familiarity with the different signs and symptoms of strangulation. This is an important area for future research because existing studies (i.e., Garza et al., 2021; Pritchard et al., 2018) suggest that police officers are not detecting a substantial number of potential strangulations, likely due to lack of training about what to look for and victim-survivor tendencies to not remember or report experiencing strangulation.
Frontline police officers are in a critical position where they can identify strangulation and offer interventions that address victim-survivor safety from both a healthcare and legal perspective. Police officers should be trained to recognize the signs and symptoms of strangulation, and should receive further training on how best to investigate and document these cases with the goal of supporting strangulation-specific criminal charges that are now available in many jurisdictions (Douglas and Fitzgerald, 2022; Edwards and Douglas, 2021; Laughon et al., 2009; McCormick and Cohen, 2024). Moreover, police officers should be trained about the significant risk for physical and mental health outcomes following strangulation, including the increased risk for brain injury, stroke, miscarriage, anxiety, depression, and suicidality, and the importance of referring victims-survivors for medical interventions. While there are many barriers to accessing medical services post-strangulation, research suggests that one such barrier is the lack of understanding among victims-survivors about the serious risks posed by strangulation, not only during the incident but also over the following days, weeks, and months. By educating police officers about these risks, they will be in a better position as frontline responders to communicate this information to victims-survivors and offer to facilitate access to healthcare, such as a medical-forensic exam. Providing training to police officers about strangulation is an imperative step towards supporting the safety and wellbeing of victims-survivors.
Footnotes
Ethical considerations
This study received ethical approval from the University of the Fraser Valley Human Research Ethics Board (HREB# 100419) in March 2020. Participation was voluntary. Participants gave passive consent by completing and returning the survey at the conclusion of the data collection period.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time the study was conducted, the second author, who administered the survey, was a Sergeant with the Royal Canadian Mounted Police (RCMP), which may have resulted in some of the police participants perceiving pressure to participate in the study. To mitigate this concern, the survey data was collected anonymously, participants were informed of their option to decline participation without penalty, and the police officers placed their own copy of the survey into the envelope, preventing the second author from knowing which officers in the room participated in the study. The authors declare no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.