
Abstract
Retired police officers face a heightened risk of suicide compared to the general population, yet research into risk and protective factors is limited. This study investigated relationships between moral injury, self-warmth, self-coldness, and suicidality in 400 retired police officers (M = 62.84, SD = 9.53; 81% male). Higher moral injury and self-warmth and lower self-coldness were associated with greater suicidality. Self-warmth and self-coldness did not moderate the relationship between moral injury and suicidality. Depressive symptoms explained the most unique variance in suicidality. Existing evidence-based depression treatments are likely to have the greatest impact on suicidality among retired police officers.
Police officers have long been identified as at risk of a range of poor mental health outcomes, including suicidality (Jetelina et al., 2020; Violanti et al., 2019). Suicidality is defined by the American Psychological Association (2018) as the elevated risk of suicide, generally indicated by suicidal ideation, intent, and planning. While there is minimal research available that isolates the retired police officer sub-group, there are estimates that this group may have a three to 10 times greater likelihood of completing suicide compared to the general population (Carney et al., 2021; Gaska, 1980). Retired police officers are theorised to differ from serving police officers in their psychological experience, given the frequently cited reduction in supports and connection to their protective policing identity and the contribution of the circumstances within which they left the organisation (Parnaby and Weston, 2020).
Moral injury
Moral injury has received increasing attention in research over the last ten years, exploring its relationship with mental health. Moral injury has been defined as the “…lasting psychological, biological, spiritual, behavioural and social impact of perpetrating, failing to prevent or bearing witness to acts that transgress deeply held moral beliefs…” (Litz et al., 2009: 697). Moral Injury has been associated with high rates of probable anxiety, depression, Post-traumatic Stress Disorder (PTSD) and suicide ideation among healthcare workers (Amsalem et al., 2021) and with PTSD among veterinary professionals (Amsalem et al., 2021; Williamson et al., 2022). Moral injury has been further separated into two factors: self-directed, whereby the individual perpetrated the transgression themselves, and other-directed, where the individual was witness to or experienced the transgression of another (Kelley et al., 2019). However, these factors are not yet empirically validated (Litz and Kerig, 2019).
To date, moral injury has primarily been studied in military populations. Substantial evidence indicates that moral injury and related constructs (e.g., potentially morally injurious events) are associated with increased suicidality. In a recent systematic review, Hall et al. (2022) established that moral injury is positively associated with suicide and related constructs. However, this review highlighted the lack of clarity and consensus in the field regarding moral injury definition and measurement. Only six of the fifteen included studies looked specifically at moral injury, while the remaining measured either exposure to potentially morally injurious events, or a measure conflating moral injury and exposure. Similar conceptual issues were observed in more recent reviews conducted by Khan et al. (2023) and Jamieson et al. (2023).
The construct of moral injury demonstrates clear relevance to the serving police officer population. The policing role involves frequent exposure to potentially morally injurious events, such as exposure to gruesome crimes, death, and moral compromise (Blumberg et al., 2018). In addition, other-directed moral injury caused by institutional betrayal may be particularly relevant for police officers, as evidenced by qualitative research reporting a consistent lack of support from management, and an autocratic leadership style (Carney et al., 2021).
Moral injury may remain relevant to police officers once they end their service. Traumatic incidents, which are also potentially morally injurious, can serve as a tipping point to retirement (Hill et al., 2015). In addition, evidence suggests that retired police officers experience persistent psychological symptoms after exiting the workforce, including those relevant to moral injury, such as guilt and shame (Parnaby and Weston, 2020). In military populations, moral injury appears to persist for years after the end of service (Levi-Belz et al., 2024).
Self-compassion
A significant volume of research indicates that self-compassion is associated with positive mental health outcomes, including for individuals experiencing suicidal behaviours (Cleare et al., 2019). Self-compassion has been identified as both a dispositional trait and a skill that can be taught (Neff, 2003), offering a potential intervention for retired police officers experiencing suicidal behaviours. Broadly, self-compassion involves approaching oneself with kindness and understanding in situations of pain and failure (Neff, 2003). It has previously been identified as having a positive relationship with the well-being of currently serving first responders, including police, fire-fighters, and emergency medical personnel (Lowery and Cassidy, 2022).
Self-compassion has been further separated into two factors; self-coldness (self-judgement, isolation, and over-identification) and self-warmth (self-kindness, a sense of common humanity, and mindfulness) (Muris and Petrocchi, 2017). Self-warmth demonstrates a weak negative association with psychopathology and self-coldness demonstrates a moderate positive association with psychopathology. Given the stronger association between self-coldness and psychopathology, Muris and Petrocchi (2017) advise against using a total self-compassion score, suggesting this results in an inflated relationship to psychological symptoms.
Self-compassion appears promising in the treatment of moral injury, given the inherent contempt, judgement, and criticism contained within moral injury (Farnsworth et al., 2014). Zerach and Levi-Belz (2021) reported that in a sample of health and social care workers, moral injury had a moderate negative association with self-compassion. Davies et al. (2019) found in a large sample of military personnel, that sub-facets of mindfulness (a facet of self-warmth) such as nonjudgement moderated the relationship between moral injury and drug abuse.
Further, self-compassion and related constructs appear to operate as protective factors by moderating the relationship between moral injury and suicidality in military populations. Levi-Belz et al. (2024) measured self-forgiveness, a construct thought to overlap with self-compassion (Cleare et al., 2019). In their study, self-directed potentially morally injurious behaviour explained 9.7% of the variance in suicidal behaviour, while other-directed potentially morally injurious events explained 7.7%. Self-forgiveness moderated the indirect effects of self-directed and other-directed potentially morally injurious events on suicidality, with the indirect effects only being significant for veterans with low self-forgiveness. Forkus et al. (2019) reported that self-compassion weakened the relationship between exposure to potentially morally injurious events and deliberate self-harm versatility (i.e., number of unique forms of self-harm) but not history of deliberate self-harm among military veterans. Morally injurious experiences were associated with deliberate self-harm versatility only for veterans low in self-compassion., thus acting as a protective factor. Kelley et al. (2019) found that facets of self-coldness (i.e., over-identification) and self-warmth (i.e., mindfulness) acted as risk and protective factors, respectively, on the relationship between moral injury and suicidality in a sample of combat wounded veterans. The association between self-directed moral injury and suicidality was significant for veterans with average and high levels of over-identification. The association between other-directed moral injury and suicidality was significant at low, average, and high levels of mindfulness, but the strength of the association decreased as levels of mindfulness increased. Whether these findings apply in a policing context has yet to be explored.
Current study
Generalised models of suicidal behaviour and prevention indicate that to understand and reduce suicidal behaviour in any population, it is essential to identify and address risk and protective factors (American Psychological Association, 2014). The first aim of this study was to examine the relationships between moral injury, self-warmth, self-coldness, and suicidal behaviours in retired police officers. The second aim was to test whether moral injury, self-warmth, and self-coldness explained unique variance in suicidal behaviours after controlling for sociodemographic factors and depressive symptoms. The third aim was to explore the moderating effect of self-warmth and self-coldness on the relationship between moral injury and suicidal behaviour.
It was hypothesised that higher levels of moral injury and self-coldness, and lower levels of self-warmth would be associated with increased suicidal behaviour in retired police officers. It was further hypothesised that moral injury, self-warmth, and self-coldness would explain unique variance in suicidal behaviour after controlling for demographic factors and depressive symptoms. Finally, it was hypothesised that self-warmth and self-coldness would moderate the impact of moral injury on suicidal behaviour in retired police officers, such that higher levels of self-warmth would weaken the association between moral injury and suicidal behaviours, and higher levels of self-coldness would strengthen the association between moral injury and suicidal behaviours.
Method
Measures
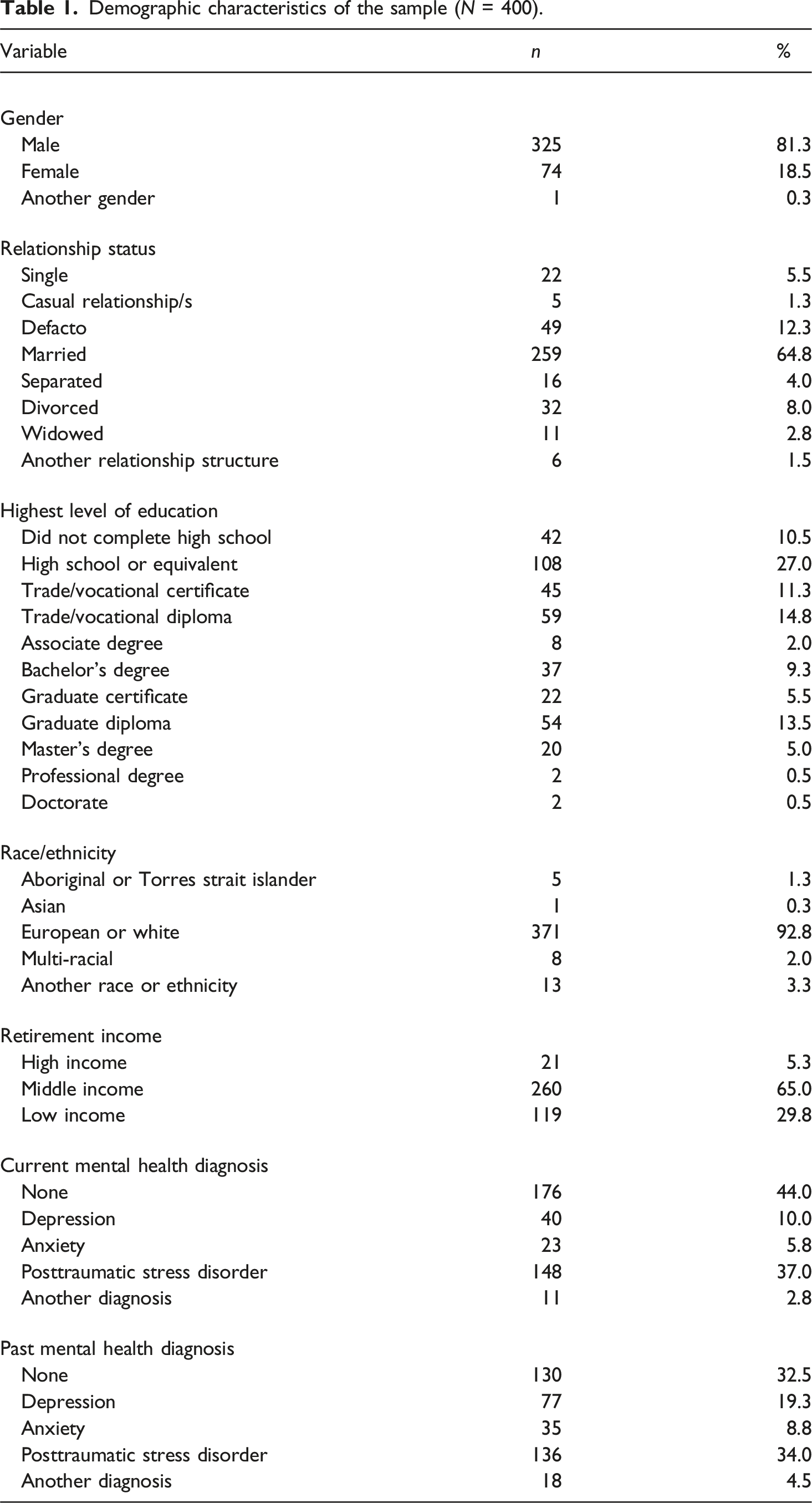
Demographic information collected included age, gender, relationship status, education, ethnicity, income, and self-reported current and past mental health diagnoses (primary diagnosis only).
Moral injury was measured using the 10-item Moral Injury Symptom Scale – Military Version – Short Form (Koenig et al., 2018) that asks participants to rate their experience of moral injury on a 10-point variable Likert scale. The wording of the measure was altered to reflect a non-military experience. For example, “I feel guilt over failing to save the life of someone in war” was changed to “I feel guilt over failing to save the life of someone while on duty”. Such changes were not expected to alter the psychometric properties of the scale, consistent with findings of an adjusted version of the long form of the scale used for health professionals (Mantri et al., 2020). A total score was calculated by reverse scoring negative items and then summing all items. Scores on the measure range from 10 to 100, with higher scores indicating greater moral injury. The scale demonstrated an acceptable level of internal consistency in this sample, Cronbach’s α = 0.72.
Self-compassion was measured using the Self-Compassion Scale (Neff, 2003). Participants rate each of the 26 items on how they typically behave towards themselves in difficult times using a 5-point Likert scale (1 = Almost Never; 5 = Almost Always). The two factor scores of self-warmth (e.g., “I try to see my failings as part of the human condition”) and self-coldness (e.g., “I’m disapproving and judgemental about my own flaws and inadequacies”) were used consistent with Muris and Petrocchi (2017). Both subscales range from 13 to 65, with higher scores on self-coldness indicating lower levels of self-compassion, while higher scores on the self-warmth subscale indicate greater self-compassion. In this study, the scales demonstrated excellent internal consistency, with α = 0.93 for self-warmth and Cronbach’s α = 0.94 for self-coldness.
Depressive symptoms were measured using the 20-item Centre for Epidemiological Studies Depression Scale (Radloff, 1977). Participants rated their experience of depressive symptoms over the preceding week on a 4-point Likert scale (0 = less than 1 day; 3 = 5–7 days). Items include “I was bothered by things that usually don’t bother me” and “I felt I was just as good as other people”. Scores range from 0 to 60, with higher scores indicative of greater depressive symptoms. Scores of 16 or above indicate the individual is at risk of developing depression. In the present sample, the Centre for Epidemiological Studies Depression Scale demonstrated excellent internal consistency with Cronbach’s α = 0.96. The Centre for Epidemiological Studies Depression Scale was used as a covariate, to separate the influence of depression on suicidal behaviour from the other variables of interest. This is a generally accepted practice in suicidal behaviour research and aligns with Australian research suggesting that depression is the most common mental health diagnosis amongst police officers (Muir et al., 2022; Rogers et al., 2018).
Suicidal behaviours were measured using the 4-item Suicidal Behaviors Questionnaire-Revised (Osman et al., 2001). Participants rated their experience on a variable Likert scale, which varied for each item. Items included “Have you ever thought about or attempted to kill yourself?” and “How likely is it that you will attempt suicide someday?”. A total score ranging from 3 to 18 is calculated by summing the scores on each item, with a cut-off of 7 indicating that the individual is at-risk (Osman et al., 2001). The Suicidal Behaviors Questionnaire-Revised has been validated in both clinical and non-clinical samples. In the present sample, the Suicidal Behaviors Questionnaire-Revised demonstrated good internal consistency with Cronbach’s α = 0.82.
Participants
The sample consisted of retired police officers previously employed in an Australian policing context. Australian policing is delivered through state, territory, and federal agencies, with structures and operational demands comparable to the UK, Canada, and the US. Unique features include Australia’s vast geography, dispersed population, and low rates of gun violence. Officers serve an average of nine to 14 years and may retire early, often due to service-related injury, with access to defined benefit pensions or superannuation (ACT Policing, 2024; Parliament NSW, 2021; WA Police Union, 2023).
Demographic characteristics of the sample (N = 400).
Procedure
Ethical approval was obtained from the Charles Sturt University Human Research Ethics Committee (reference number H22416). The study used a quantitative, cross-sectional, and correlational design. Participants were recruited through email sent via retired police organisations and support groups, and social media advertisement to relevant organisations and Facebook groups. The survey link presented participants with an information statement that detailed the requirements and nature of the study, along with support service information. Informed consent was obtained before proceeding with the survey. Participants answered demographic questions and completed all measures at one-time point, via an anonymous online survey using the Qualtrics platform. The survey took on average 26 minutes to complete. Presentation of scale order was counterbalanced to control for order effects. The study concluded with a debriefing statement which summarised the aims of the study, and reiterated support service information. Withdrawal was possible at any time by closing the web browser.
Data analysis
A priori power analysis (Faul et al., 2007) was conducted for multiple regression with 12 predictors (incorporating demographic items), with power (1 - β) set at 0.95 and α = 0.05, two-tailed. A total sample size of at least 89 participants was required to complete analyses with appropriate power.
Age, gender, relationship status, education, and mental health diagnoses were controlled for in the analyses due to evidence suggesting these variables are linked to suicidal behaviour in police officers (Barron, 2010). In addition, depression scores were controlled for due to the overlap with suicidal behaviour (Rogers et al., 2018). Gender, relationship status, education, and mental health status were transformed into dichotomous variables (i.e., male, female; partnered, unpartnered; diploma and below, above diploma level; present, absent, respectively).
Descriptive statistics for the sample were calculated. Bivariate and partial correlations between the key variables of suicidal behaviour, moral injury, self-warmth, and self-coldness were analysed. Hierarchical regression analyses tested whether moral injury, self-warmth, and self-coldness explained unique variance in suicidal behaviour, after controlling for the sociodemographic variables and depressive symptoms.
The moderation model was tested using the PROCESS macro (Model 1) (Hayes, 2014) in SPSS. The model was tested separately for self-warmth and self-coldness. In each model, the covariates, moral injury, a factor of self-compassion, and the interaction term were entered simultaneously into the regression analysis. Centred scores were used in the analyses. The model used 5000 bootstrap samples and a bootstrapped 95% confidence interval (CI) was used. A 95% CI that did not include zero for the interaction terms was used to infer significance.
Results
Data cleaning
A total of 473 participants consented to and commenced the survey. Nine participants were excluded based on their answers to initial screening questions assessing inclusion criteria. An additional 64 participants were excluded due to at least one full scale being incomplete.
Missing data were analysed using Little’s Missing Cases at Random (MCAR) test, and as a result of the small percentage of total missing data (< 2%), were replaced using the Expectation-Minimisation Imputation method (Tabachnick and Fidell, 2014).
Assumption of normality testing was completed for all variables, with moral injury, self-warmth, self-coldness, and depression scores meeting assumptions of normality. Scores on the Suicide Behavior Questionnaire-Revised did not meet assumptions of normality, which was expected given the nature of the construct as occurring infrequently in the general population (Tabachnick and Fidell, 2014). Bootstrapping accounts for the assumption of normality violations (Preacher et al., 2007).
Preliminary analyses
Half (50.5%, n = 199) of the sample scored 7 or above on the Suicidal Behaviors Questionnaire-Revised, which indicates a clinically significant risk of suicide. In addition, most of the sample (81%, n = 320) scored 16 or above on the Centre for Epidemiological Studies Depression Scale, which indicates clinically significant levels of depressive symptoms.
Descriptive statistics
Descriptive statistics and Pearson’s correlation coefficients between variables.
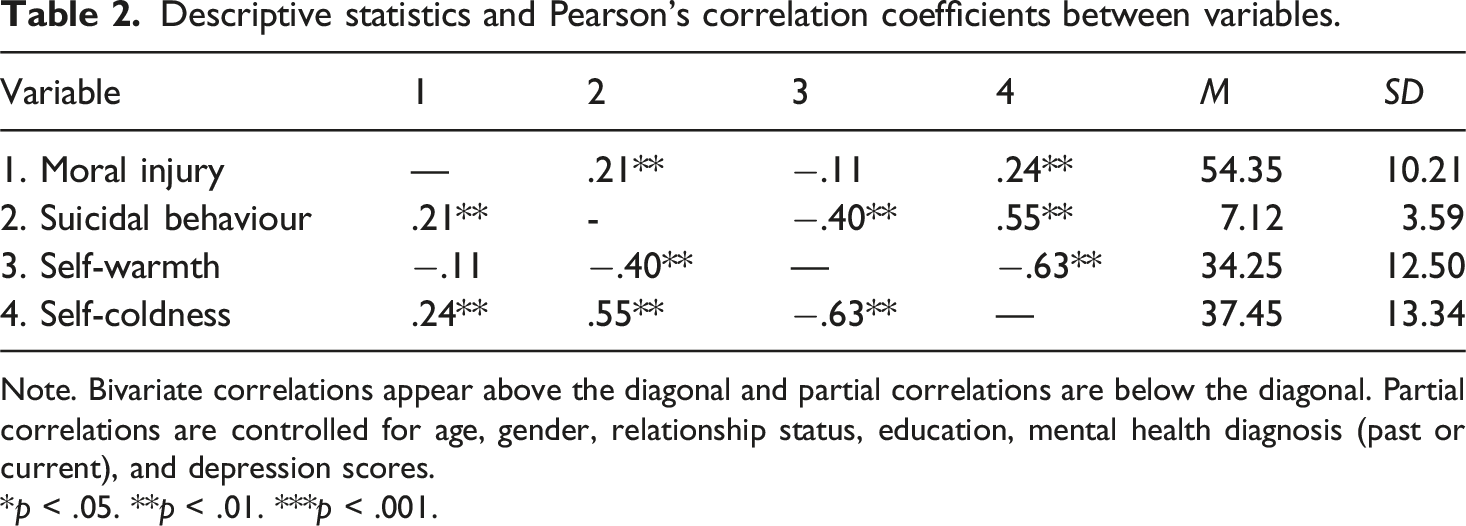
Note. Bivariate correlations appear above the diagonal and partial correlations are below the diagonal. Partial correlations are controlled for age, gender, relationship status, education, mental health diagnosis (past or current), and depression scores.
*p < .05. **p < .01. ***p < .001.
Hierarchical regression analyses
Analysis for the hierarchical regression model for demographics (Model 1), depressive symptoms (Model 2) moral injury (Model 3) and self-warmth and self-coldness (Model 4) predicting suicidal behaviour.
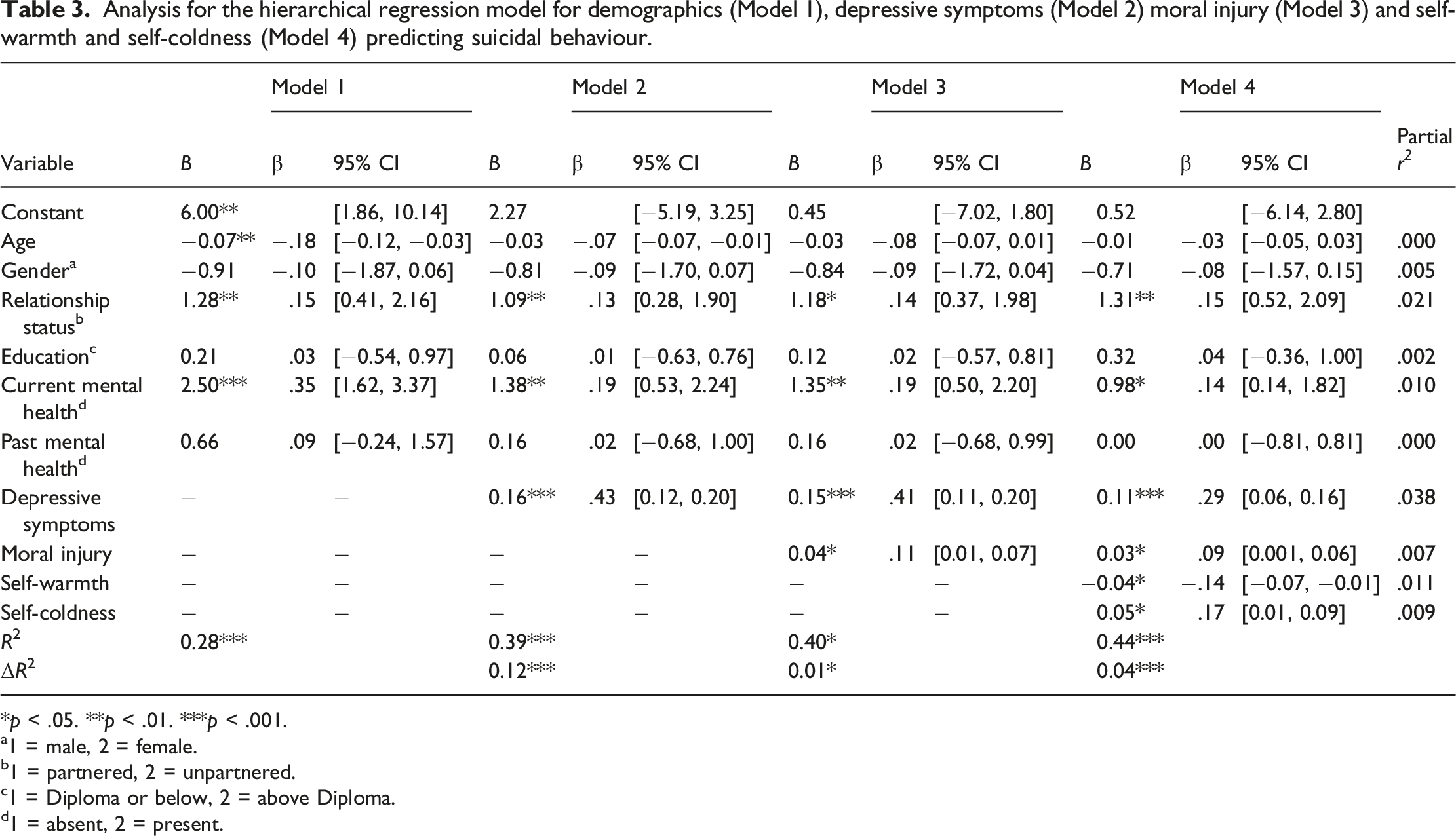
*p < .05. **p < .01. ***p < .001.
a1 = male, 2 = female.
b1 = partnered, 2 = unpartnered.
c1 = Diploma or below, 2 = above Diploma.
d1 = absent, 2 = present.
Moderation models
Analyses for Self-warmth and self-coldness moderating the relationship between moral injury and suicidal behaviour.
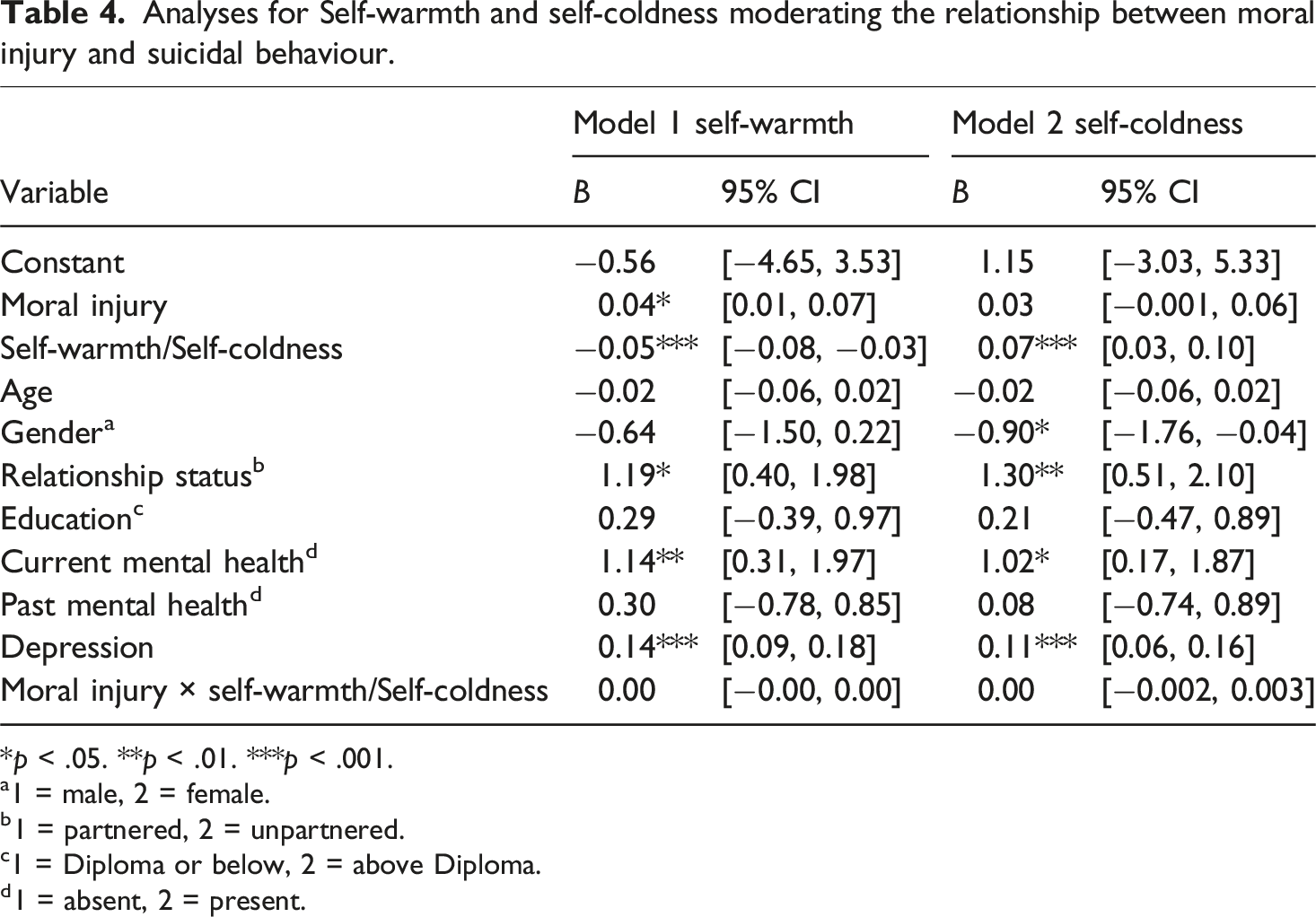
*p < .05. **p < .01. ***p < .001.
a1 = male, 2 = female.
b1 = partnered, 2 = unpartnered.
c1 = Diploma or below, 2 = above Diploma.
d1 = absent, 2 = present.
In Model 2 the moral injury x self-coldness interaction was not significant. The moderation model was again unsupported. Model 2 explained a significant 44% of the variance in suicide risk. In this model, higher levels of self-coldness and depressive symptoms were associated with higher rates of suicidal behaviour. In addition, male gender, being unpartnered, and having a current mental health diagnosis were also associated with suicidal behaviour.
Discussion
This study aimed to examine the relationships between moral injury, factors of self-compassion (i.e., self-warmth and self-coldness), and suicidal behaviour in retired police officers. Overall, results supported the assertion that retired police officers are at risk of poor mental health outcomes, with 50.5% of the sample presenting with a clinically significant risk of suicide and 81% with scores indicating clinically significant depressive symptoms. The high rates of depressive symptoms were surprising given a relatively lower report of formal depressive diagnosis (10%) and may be reflective of a reduced likelihood of help-seeking and, therefore, formal diagnosis, characteristic of policing populations (Grumley Traynor and Rydon-Grange, 2024).
The first aim of this study was to examine the relationships between moral injury, self-warmth, and self-coldness with suicidal behaviours in a retired police officer population. Results supported the hypotheses that higher levels of moral injury and self-coldness would correlate with higher levels of suicidal behaviours, and that higher levels of self-warmth would be associated with lower levels of suicidal behaviour in retired police officers.
Results from this study suggest that moral injury, and not just exposure to events, is associated with increased suicidal behaviour. Previous research into the relationship between moral injury and suicidal behaviour has primarily used measures that conflate exposure to potentially morally injurious events with the psychological outcome of this exposure (Litz and Kerig, 2019).
The strength of the relationship between moral injury and suicidal behaviour in this study was less robust than that demonstrated by Ames et al. (2019), who reported a moderate positive correlation between moral injury and suicidality, using the long-form of the Moral Injury Symptom Scale. However, the measurement of suicide risk in the Ames et al. (2019) study was estimated using secondary data identifying risk factors for suicide. This method may have overestimated the presence of suicidal risk, and thus the relationship between moral injury and suicidal behaviour.
The strength and direction of the association between the factors of self-compassion (i.e., self-warmth and self-coldness) and suicidal behaviour was as expected. These results were consistent with meta-analysis by Cleare et al. (2019) which looked at these variables across populations.
The second aim of this study was to test whether moral injury, self-warmth, and self-coldness explain unique variance in suicidal behaviours after controlling for sociodemographic factors and depressive symptoms. Results supported the hypothesis that moral injury, self-warmth, and self-coldness would each explain unique variance in suicidal behaviours.
Whilst statistically significant, the unique variance in suicidal behaviour accounted for by moral injury was small. Self-warmth and self-coldness similarly contributed only a small amount of unique variance in suicidal behaviour, however this was consistent with a recent meta-analysis which established that self-compassion has a primarily indirect relationship with suicidal behaviour (Cleare et al., 2019). Of the variables studied, depression scores explained the largest unique variance of suicidal behaviours. Depression was also highly prevalent in the sample, with 81% of scores suggestive of clinically significant depressive symptoms.
The results of this study suggest that self-warmth and self-compassion contribute a similar amount of unique variance in the suicidal behaviour of retired police officers. This finding contrasts with previous research, which suggested that self-coldness has a stronger relationship with psychopathology. The Muris and Petrocchi (2017) meta-analysis and the factor analysis conducted by López et al. (2015) included studies that investigated various psychopathology, including depression, anxiety, and stress. However, none of the studies included suicidal behaviour as an outcome measure, which may explain the difference in results to the present study. In this sample, neither self-warmth nor self-coldness is more strongly associated with suicidal behaviour in retired police officers.
The third aim of this study was to explore the moderating effect of self-warmth and self-coldness on the relationship between moral injury and suicidal behaviour. It was hypothesised that self-warmth and self-coldness would moderate the relationship between moral injury and suicidal behaviour. The moderation models were not supported. This finding was unexpected given previous research using total self-compassion scores that suggested that self-compassion moderates the relationship between the impact of exposure to potentially morally injurious events and the versatility of deliberate self-harm (Forkus et al., 2019).
More specifically, Kelley et al. (2019) demonstrated that one of the three subcomponents of self-warmth (i.e., mindfulness) and one of the three subcomponents of self-coldness (i.e., overidentification) moderated the relationship between moral injury and suicidality. There are several possible reasons for the difference in results. Firstly, factor analysis conducted by López et al. (2015) has demonstrated that only the two-factor (i.e., self-warmth and self-coldness) and not a six-factor model using the Self-Compassion Scale is supported (López et al., 2015). Secondly, Kelley et al. (2019) used a measure of moral injury that includes a two-factor model of self- and other-directed moral injury. Preliminary evidence evaluating a new moral injury measure in a first responder population including police, provides initial support for using the bifactor model of moral injury in this population (Tappenden et al., 2023). These differences in the measurement of both key constructs of self-compassion and moral injury may explain the difference in results.
The current results suggest that self-warmth is not a protective factor, and self-coldness is not a risk factor in the relationship between moral injury and suicidal behaviour. It is hypothesised that the small contribution of moral injury in explaining suicidal behaviour, along with the absence of a moderating effect of self-warmth and self-coldness on the relationship between moral injury and suicidality may be accounted for by issues with the measurement of moral injury.
Due to the recent and rapid expansion of research interest in moral injury, a lack of conceptual clarity and consensus with this construct warrants consideration. Moral injury is a relatively new construct with no gold-standard measure of assessment. Most available moral injury measures have been developed in the last five to 10 years, including the scale used in this study, the Moral Injury Symptom Scale – Military Version – Short Form (Koenig et al., 2018). The psychometrics of this and many available tools for measuring moral injury have recently been questioned due to poor study quality and inconsistent demonstration of reliability and validity across studies (Houle et al., 2024). This may impact the reliability of moral injury scores in the current study and therefore the confidence which with conclusions can be drawn from results.
The Moral Injury Symptom Scale – Military Version – Short form uses a total score and includes only one question that addresses other-directed moral injury. Other-directed moral injury is likely relevant to a policing context, as evidenced by research that emphasises the moral impact of witnessing gruesome crimes, ineffective institutional leadership, and organisational betrayal within police organisations (Simmons-Beauchamp and Sharpe, 2022). Other-directed moral injury is also theorised to be closely associated with suicidality (Hamrick et al., 2022). The Moral Injury Symptom Scale – Military Version – Short Form may be primarily measuring self-directed moral injury and therefore not be the most suitable measure for the policing population.
Additional limitations were identified in this study. While the large sample size enhanced the reliability of the findings, the sample was homogenous, primarily white, married, and male. While reflective of the current retired policing population in Australia (McKernan, 2008), as this population becomes increasingly diverse and representative of the broader Australian population, the findings outlined here should be generalised with caution. In addition, the sample, primarily sourced through advertisement via an organisation with a significant focus on providing mental health support for retired police, may be skewed towards those experiencing mental health and wellbeing-related concerns.
The study was cross-sectional. As a result, we cannot interpret when psychopathology, moral injury, and suicidal behaviour developed and how this interacts with retirement and aging. Longitudinal research will help us to better understand the mental health and treatment needs of retired police officers. Given the novel application of moral injury within this population, it was beyond the scope of the current study to examine the influence of variables such as policing role, length of service, or time since retirement. Future research could explore these factors to better identify individuals at heightened risk of moral injury and inform tailored prevention strategies.
This study, while preliminary, provides much-needed clarification on the psychological treatment of retired police officers at risk of suicide. Despite a small contribution of moral injury, self-warmth, and self-coldness in this study, moral injury and self-compassion would still be considered viable treatment targets, particularly for those presenting without depressive symptoms. This is because of the seriousness of the outcome (i.e., suicide risk), where any reduction in suicide risk is of value (Ferguson, 2009). However, given the larger variance accounted for by depression, as well as the availability of efficacious assessments and treatments for depression across adults and older adults, the presence of depressive symptoms would be a higher priority target (Werson et al., 2022).
Given this is the first study of its kind in a sample of retired police officers, and the proportion of the variation in suicidal behaviour unaccounted for, other variables impacting suicidality warrant exploration. Risk factors that have recently been linked to suicide by police officers, such as substance abuse, anxiety, burnout, and social support may be worth exploring (Talavera-Velasco et al., 2024). Further research exploring these additional risk factors for suicide will advance the psychological treatment of retired police officers.
With increasing research interest, several measures of moral injury developed in the last two years show promise and may address some limitations outlined in this study. The Expressions of Moral Injury Scale (Tappenden et al., 2023) has been validated in a sample of first responders, and includes a bifactor model of moral injury. The Houle et al. (2024) meta-analysis recommends the Moral Injury Outcome Scale (Litz et al., 2022) as having superior psychometric properties. Further research using improved measurement will increase the confidence with which conclusions can be drawn and test the hypothesis that the absence of a moderation effect, along with the small contribution of moral injury to suicidal behaviour, is impacted by conceptual and measurement issues with moral injury.
In conclusion, the results of this study demonstrated that moral injury and self-coldness have weak positive associations with suicidality and self-warmth has a weak negative association with suicidality in a retired police officer population. All three constructs explain a small amount of unique variance in suicidality. However, depression was most strongly associated with suicidality. There was no interaction effect between self-coldness and moral injury or between self-warmth and moral injury in predicting suicidality. Further research is required to determine other relevant risk and protective factors for suicidality in retired police officers and to utilise increasingly refined measures of moral injury. While further research is required, this study provides preliminary guidance into the psychological treatment of at-risk retired police officers.
Footnotes
Ethical statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author is employed by Victoria Police in a public service role. However, the results of this research would have no financial or other benefit to the author in this capacity. We have no other known conflict of interest to disclose.
Data Availability Statement
The data that support the findings of this study are available to be shared with other researchers by request.