
Abstract
This qualitative study explored New Zealand police, paramedic and mental health staff’s experiences of co-response (when these three agencies work together to respond to suicide/mental health-related crises) and how this compared to usual practice. Themes were identified from 24 in-depth interviews using thematic analysis. ‘Dread, fear and failure’ encapsulated the reactions toward usual practice, characterized by fears of inadequate support, coercive measures, risk and poor outcomes. The ‘gamechanger’ co-response model provided police and paramedics with supportive and accessible mental health expertise. Participants felt safer and better able to provide person-and family-centered input. Continuation and extension of co-response models are recommended.
Introduction
Worldwide and in Aotearoa New Zealand (NZ), mental health related 911-calls to first responders have increased significantly (Hodgkinson and Andresen, 2019; NZ Police, 2021; Watson et al., 2021), a demand that often overwhelms emergency services’ capacity to respond. In 2014, New Zealand Police responded to 21,545 emergency calls coded as related to ‘mental health’ and ‘threatened or attempted suicide’ (Williams, 2019). In 2020, this had increased to 70,225 events (NZ Police, 2021), with an estimated 21% of all police callouts relating to mental health issues (Porter, 2021).
Having police as the sole agency attending a mental health related emergency may be detrimental for the person in crisis. In a NZ study, 78% of police callouts resulting in a specialist mental health assessment included the use of force, representing a “coercive pathway to care” for service users often already experiencing social vulnerabilities (Holman et al., 2018: 7). A UK online police discussion forum discussing mental health related callouts found some police respondents judged individuals as ‘scrounging’ and undeserving of police time, and associated mental health callouts with violence and extreme behavior, justifying the use of force (Lane, 2019). Despite increased focus on mental health training of police staff (Fiske et al., 2021), Wondemaghen (2021: 272) posits that as first responders “police cannot be ‘trained enough’ to deal with these calls on their own.” In a New Zealand survey, police reported they were left to manage mental health emergencies on their own, with 89% reporting it was hard to access advice from mental health services when they needed it. Paramedics described similar experiences, and both professional groups found this very stressful (Kuehl et al., 2023).
Exposure to suicide and other mental health-related emergencies can also affect the mental health of the first responders themselves (De Lyra et al., 2021). For example, police officers who respond to suicide-related calls are at an increased risk of developing post-traumatic stress disorder (PTSD), depression, and anxiety (Cerel et al., 2019; Stanley et al., 2016) with repeated exposure increasing the risk of subsequent mental health problems (Aldrich and Cerel, 2022).
Police and ambulance services usually have few other options but to transfer the person in crisis to an emergency department (ED) if a mental health assessment is indicated. Over recent years, EDs have been struggling to manage the growing numbers of mental health/addiction presentations (Australasian College for Emergency Medicine, 2019; Baia Medeiros et al., 2019; Tran et al., 2020). Significant police resources may be expended if officers remain in ED waiting for the person to be assessed. A busy ED may also miss mental health presentations in coding and referral processes (e.g., deliberate self-harm being coded only as a physical injury), meaning an opportunity for future intervention is lost (Werkmeister et al., 2022). For people presenting with mental health/addiction issues to ED, long waiting times (Australasian College for Emergency Medicine, 2018) and experiences of stigmatizing ED staff attitudes (Sacre et al., 2022) are common. In the NZ Government Inquiry into Mental Health and Addiction He Ara Oranga, people stressed their preference for mental health and addiction support in the community, including when experiencing a crisis (Paterson et al., 2018).
With these well-established problems associated with police responding on their own to 911-mental health calls (Crilly et al., 2019; Kirubarajan et al., 2021), first responders have been looking for new ways of working, such as co-response models (Evangelista et al., 2016; Henry and Rajakaruna, 2018; Robertson et al., 2020). Co-response models involve staff from police, ambulance and mental health services jointly responding to 911-emergency mental health/suicide risk calls. In Australia, police-mental health co-response teams (CRTs) were found to often successfully deal with an immediate crisis and reduce ED attendances and inpatient admissions (Meehan et al., 2019). The reduction in ED presentations was partially attributed to service users receiving CRT crisis assessments in the community or police cells, with some being directly admitted to mental health inpatient units bypassing the ED (McKenna et al., 2015). However, a systematic review of CRTs failed to prove their overall effectiveness because of distinct variations in how co-response models were operationalized; though it suggested mental health legislation was used less often and fewer people were taken into police custody (Puntis et al., 2018). Service users have appreciated CRTs providing a quick, supportive, empathetic and calm response that contributed to the de-escalation of a crisis (Evangelista et al., 2016), a view shared by paramedics (Irving et al., 2016).
In NZ, the first tri-agency CRT model was trialled in 2020. This mixed method study presents the frontline staff experiences of this CRT, and how it compares to usual care, contributing to the emerging international evidence on this new way of managing mental health related crises.
Context
The CRT was trialed in an urban region, serving approximately 324,000 people. Thirty-three percent of people in the region were under 25 years old; they were ethnically diverse with a fluctuating proportion of Māori between 11% and 22% depending on the sub-region. (Capital & Coast District Health Board, 2021).
The 12-month CRT trial between March 2020 and March 2021 involved a collaboration between the NZ Police, ambulance services and mental health services. The CRT comprised of five staff working Tuesday to Friday between 0800 and 1800. They rotated weekly into two teams. The ‘field’ team consisted of a mental health clinician, police officer, and paramedic. When not on callouts, they joined the ‘home’ team comprising of a mental health clinician and a police officer at the central police station.
Throughout the shift, the CRT police officers and the paramedic checked for incoming 911-mental health/suicide risk related calls on the police and ambulance call systems respectively. Alternatively, frontline staff or Communication Centre staff contacted the CRT for advice and support. For each mental health/suicide risk related 911-call, the name, date of birth and reason for the call were shared amongst the CRT. The mental health clinician scanned for background information on the District Health Board (DHB) platform. Only pertinent information, such as the person being under a community mental health team or an alert on the police system, was shared between CRT members and stakeholders (Ministry of Health, 2021). The CRT information was used to provide advice to frontline police units and to Police/Ambulance Communication staff, e.g. the CRT might advise police officers to initiate an urgent ambulance dispatch for a 911-call that involved a person at high risk of a lethal overdose (as this had occurred in the past). Liaison occurred with mental health clinicians such as case workers who may be asked to assess the service user involved in a 911-call instead of CRT staff. A joined CRT discussion of the information determined if a field team callout was required.
In an unmarked car, the field team responded to 911-emergency police and ambulance callouts involving people in acute distress with often complex health and social challenges. The CRT field team provided timely assistance to police or ambulance staff for callouts that might require the use of the Mental Health Act (MHA). Examples of CRT callouts included a person threatening to jump off a bridge or a person under mental health services being aggressive to the point of needing to be tasered. Outcomes of CRT input included the person staying in the community with GP or mental health follow-up or transfer to the police cells. Service users got transferred to the emergency department if they needed medical input or needed inpatient admission, such as when they were section under the MHA. The CRT did not respond to calls that involved a person who died by suicide.
CRT outcomes using a quasi-experimental design have been reported as successful (Every-Palmer et al., 2022). Over a 1-year trial period, there were 1273 eligible mental health crisis callouts (48% coded as suicide risk, 38% ‘mental health’ emergencies, and 14% as ‘other’). If these crises occurred during a day with CRT availability, they were resolved more rapidly and responses were more likely to be community-based with reduced risks of ED attendance (RR: 0.7, 95% CI: 0.6,0.8). In the following month, service users were less likely to re-present to ED and or be admitted to a mental health unit (p < 0.01 and 0.05 respectively). There were no statistically significant differences in use of force between ‘business as usual’ and CRT responses and few people were detained in police custody.
The views of people in crisis and their families have been canvassed in a companion study. They expressed high levels of satisfaction, viewing the CRT as safe, compassionate, and respectful - providing person-centred care that reduced the risk of adverse outcomes and coercive interventions (Kuehl et al., 2024). However, views about the CRT from the first responders who attend crisis callouts or manage their aftermath have not been reported.
The objective of this study was to ascertain how frontline staff experienced working with a CRT, and how it compared to usual care.
Method
A mixed method design was used. We asked staff from police, ambulance, mental health services and the CRT about their experiences and meaning-making (Crowe et al., 2015) of the CRT, using semi-structured interviews and a Likert scale.
Ethics, consultation, and locality approvals
We undertook consultation with the Research Advisory Group Māori at the local DHB [RAG-M #747] and with the Ngāi Tahu Research Consultation Committee at the University of Otago, aligning with requirements for research involving Māori (the Indigenous people in New Zealand). Ethics approval was received from the Northern B Health and Disability Ethics Committee [20/NTB/150]. We obtained locality consent from the participating DHB and the ambulance service. A memorandum of understanding between the NZ Police, the DHB and ambulance service outlined their commitment to an independent trial evaluation by the University of Otago. The names of the participants and their precise location have been de-identified as per our research protocol and assurance of confidentiality.
Study participants
Participants were frontline staff who were employed by police, ambulance or mental health services in the study region at the time of the CRT trial. Potential study participants were purposively sampled via a sister-study, in which frontline staff’ were surveyed about their experiences of ‘business as usual’ (Kuehl et al., 2023). In the final section of the survey, participants were invited to contact the researcher if they were interested in participating in interviews about the CRT. Snowballing techniques were used to further recruit eligible stakeholders.
Data collection tools
Interview schedule stem questions.
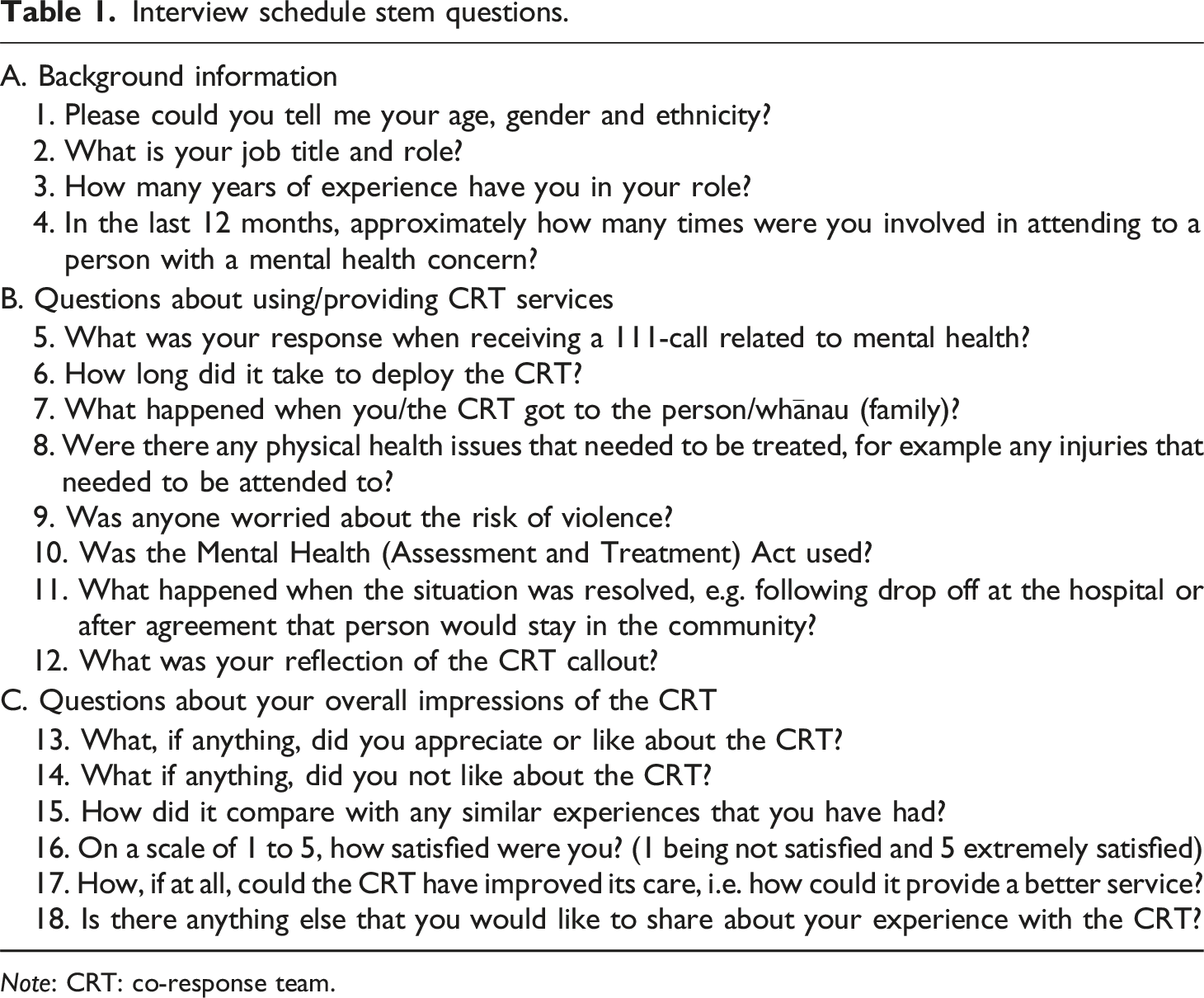
Note: CRT: co-response team.
Interviews
After obtaining informed consent, SK interviewed 24 participants between September 2020 and February 2021. Depending on participant preferences and COVID-19 pandemic restrictions at the time, fourteen face-to-face interviews occurred at a police station, emergency department or community mental health service; 10 interviews occurred via telephone. All interviews were recorded and transcribed verbatim. Demographic information was separated from the transcriptions and linked only by secure key code. All participants were assigned pseudonyms to preserve anonymity.
Analysis
For the qualitative analysis, thematic analysis was conducted in accordance with Braun and Clarke’s (2006) approach. Patterns were identified iteratively through processes of data familiarisation, data coding, theme development, and review (Braun and Clarke, 2006). We used an inductive, realist approach to data analysis, describing how participants experienced and made meaning of the CRT.
Two researchers (SK and LC) independently coded interview transcripts; codes were examined and iteratively consented into groups capturing similar themes, each with several subthemes. Using a reflexive approach (Braun and Clarke, 2021b), these themes and subthemes were considered by the wider team (SK, LC, and SEP) to sense-check ideas and achieve richer interpretations of meaning. Early interviews informed subsequent data collection. Moving back and forth between data collection and analysis enabled us to refine, define and name the themes (Braun and Clarke, 2021a). We defined our conceptualization as ‘themes’ not as topic summaries (Braun et al., 2022). Data saturation was achieved when we had reached the provisional sample size of at least three participants from each of the four stakeholder subgroups and when regular review of data quality confirmed we had “rich, complex, ‘messy’ data” (Braun and Clarke, 2021c: 210). SK used NVivo Qualitative Data Analysis software (version 12, QSR International, Doncaster, Victoria, Australia) to assist with data organization and analysis, LC manually coded the data. NVivo analysis was shared across the research team.
For the quantitative analysis of the Likert Scale, the mean was used for measuring the central tendency (Amidei et al., 2019).
Findings
Demographic and work background
Demographic information of interview participants from Police, Ambulance, Mental Health Services and the CRT.
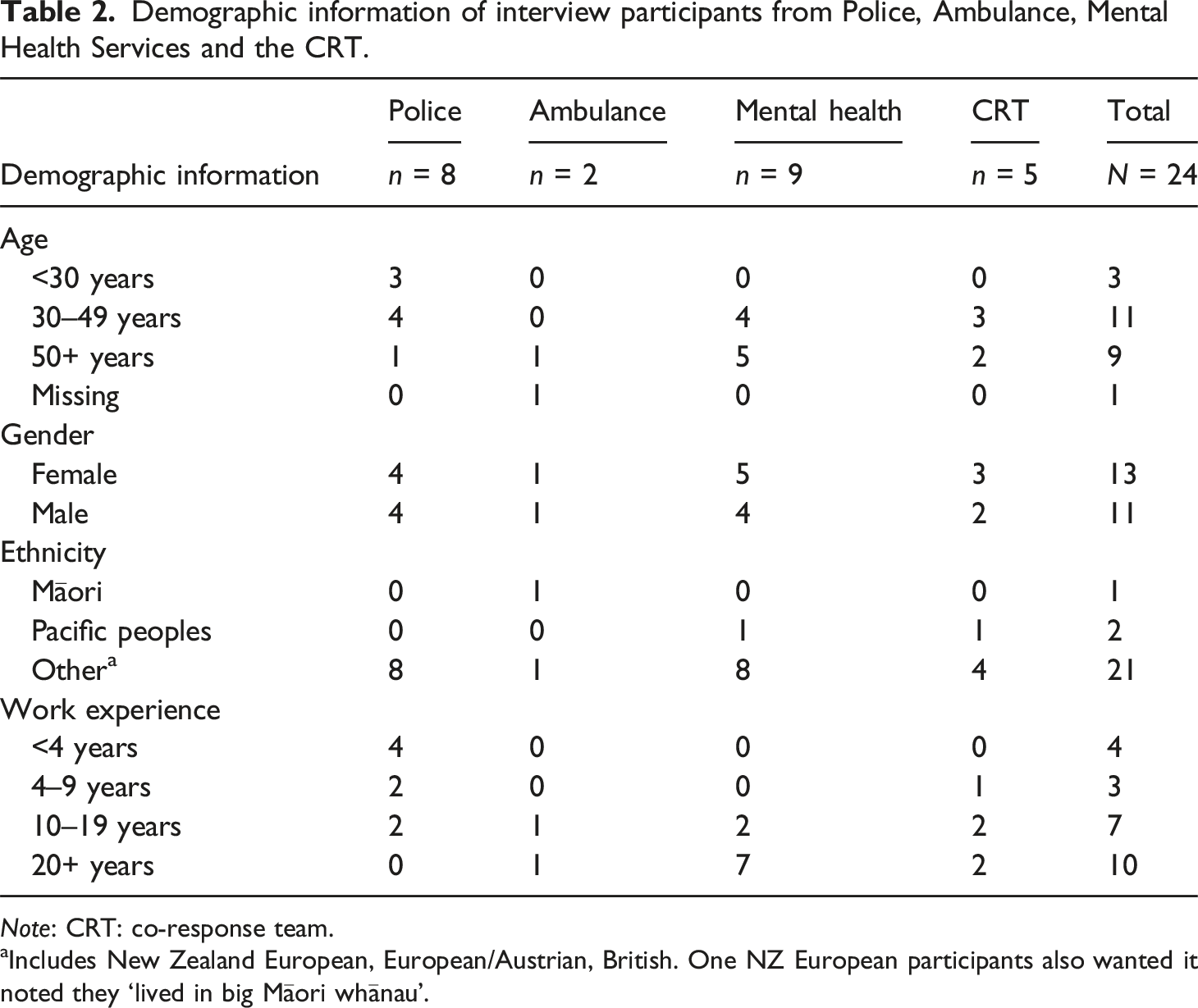
Note: CRT: co-response team.
aIncludes New Zealand European, European/Austrian, British. One NZ European participants also wanted it noted they ‘lived in big Māori whānau’.
Of the eight participating police staff, two were sergeants, four constables and two were police station employees. Of the nine mental health professionals, four were community mental health nurses, two mental health crisis nurses, one an ED mental health liaison nurse, one a forensic liaison nurse, and one a psychiatrist. Both ambulance staff were senior paramedics. The CRT consisted of two police sergeants, two mental health professionals (a nurse and occupational therapist), and a paramedic.
Police and ambulance staff reported attending “countless” suicide/other mental health crises (Lucy–P, Rita–P, Olaf–P), “with some shifts solely consisting of mental health” (Gilly–P). Police officers estimated attending between 50 and 200 mental health crises/year, whilst paramedics attended approximately one mental health/suicide related crisis a fortnight.
Themes
We identified three overarching themes. Firstly, ‘dread, fear and failure’ represented participants’ feelings towards mental health crises before the CRT’s introduction. ‘Game changing’ signified participants’ appreciation of the co-response model. Lastly, the theme ‘room for improvement’ included aspects of the CRT that could be further developed.
Dread, fear and failure
Dread
Police officers described high levels of anticipatory trepidation about attending suicide/mental health related crises; “every frontline cop dreads mental health” (Travis-P). A normal police officer on a response team does not want to go to a mental health incident. A normal frontline young cop has joined the Police to help people, save lives, and drive fast cars. (Martin–P)
Much of this dread related to uncertainty as how to manage complex situations. Universally, police participants described expecting little support available from mental health services in the field. As a result, police officers often felt obliged to detain distressed or suicidal people under mental health legislation and transport them to ED to await specialist support. Police dreaded the amount of time this might take, rendering them unavailable to respond to other emergencies. They resented having to “sit there for six hours [waiting for mental health services] and babysit someone who 50% of the time just falls asleep” (Travis–P).
Fear
Both police and paramedics reported a fear of being hurt during suicide/mental health-related crises, which were viewed as dangerous and ‘unpredictable [as] there are often weapons’ (Stan–P). Though police felt better trained to manage potentially volatile situations, the paramedics felt exposed and vulnerable, describing past instances in which they had been hurt. One participant said he and his colleagues had bought their own stab-resistant body armor that they wore under their uniform as protection during mental health crises callouts. I've been assaulted three or four times on the job. Every single instance of an assault has been from … a patient suffering a mental health crisis in some form or another… [and so] I've purchased and wear my own stab-proof vest … there are several of us who have gone as far as purchasing our own (Fin-A)
Failure
Police officers and paramedics felt they often failed service users and their families, and they carried responsibility for this. If it all goes … wrong, it's [on] us. (Stan–P)
The ambulance service’s medically driven approach was viewed as inadequate in addressing a person’s mental health needs. [We are] operating from a platform of medical assessment, not mental health assessment. We've got some tools and things, but in the end ... I can't offer them ... the expertise. (Nina–A)
Getting people help, support and providing safety was challenging, and sometimes unsuccessful with devastating outcomes for the person and their family. This could be traumatising for staff. We found him [deceased] 24 hours later, it's just not nice for us. We expect a certain degree of that in our job, but ... (Stan–P)
Police and paramedics were frustrated that transferring distressed people to ED was not always necessary and sometimes had adverse consequences. Due to the long waits, some people self-discharged before being assessed. ED staff might re-contact Police requesting they search for the person, but sometimes this was not possible. They feared without support the person would die of suicide, and some had experienced this (as illustrated above).
Participants felt with usual care, services users were disadvantaged by different agencies working in silos, making the provision of integrated support difficult. Mental health services were commonly unaware of clients’ crisis calls. A CRT clinician explained how on one occasion, a distressed service user came to the attention of Police and ambulance 17 times in a month, with their mental health team oblivious to this until contacted by the CRT: “That came as quite a shock” (Nick-C).
Game changing
Twenty-three participants were very satisfied with the CRT (one score missing) (Figure 1). Mean overall satisfaction with co-response team scores by affiliation. Note: *5 = extremely satisfied, 4 = very satisfied, 4 = moderately satisfied, 2 = slightly satisfied, 1 = not at all satisfied.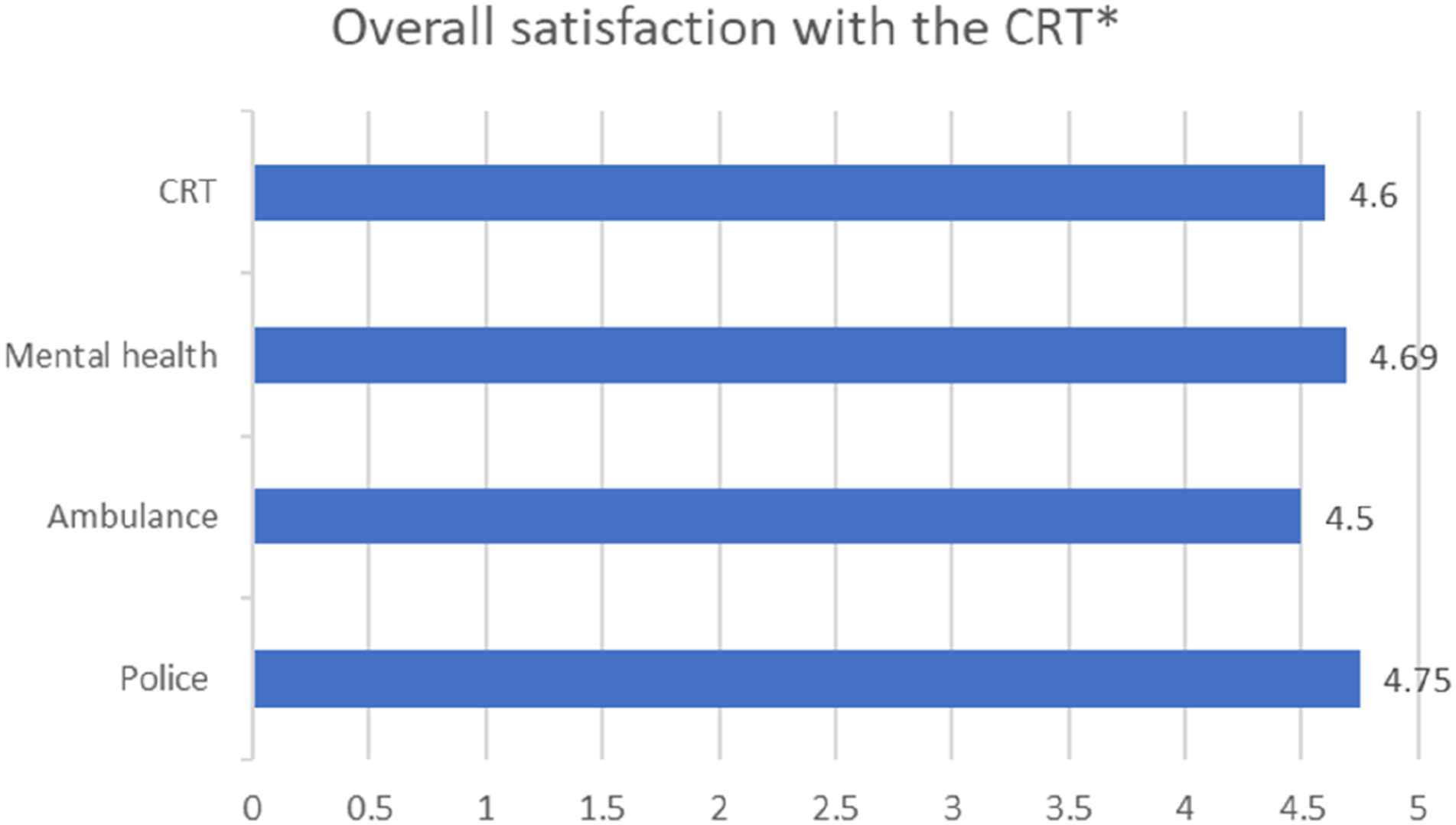
Timely access and support
All eight police participants were unreservedly enthusiastic about the CRT, describing being able to access “fantastic” (Lucy-P, Martin-P, Rita-P, Olaf-P), approachable, expert crisis assistance. Mental health clinicians similarly praised the model as providing “proactive” help (Logan–MH, Michael–MH), such as being “happy to go and look for somebody” when significant concerns existed about suicide or other risks (Moni–MH). When police officers contacted the CRT, their advice was “really invaluable” and it was “never a hassle” to obtain support, which contrasted dramatically with the usual model (Lucy-P). Every time I’ve contacted [the CRT], they’ve been willing to help … [on the other hand] when I’ve contacted the mental health team … it’s like trying get blood out of a stone. (Martin- P)
Frontline staff’s ability to access timely support from the CRT resulted in better use of resources. Without [the] CRT working, I would easily say there would be a [officer] at the hospital every day, waiting with a mental health patient … that constable that was being paid to serve the hospital isn't having to do that anymore. (Lucy–P)
The CRT was considered instrumental in reducing the requirement for ambulance transports. The CRT paramedic could contact key stakeholders directly and frequently arranged alternative transportation to ED or to a GP, freeing up scarce ambulance resources.
For CRT staff, being split between field and home teams meant they could support multiple callouts simultaneously. When the field team could not attend in person, the home team provided ‘liaison services’ giving frontline police officers “a little bit more information” so they could manage the crisis effectively instead of going in “blind” (Nick-C). Participants found this configuration effective. If the home base team was not operational because staff were sick or on leave, colleagues commented it felt “like your superpowers are taken away” (Analise-C).
The CRT’s expertise and access to background information supported the development of service-wide, individualized plans for repeat crises. Such plans might include involving trusted case workers or organizing reviews at community mental health bases instead of ED. Mental health staff receiving information about their clients directly from the CRT was viewed as “really helpful” as it allowed them to act promptly to support the client (Luke–MH).
Safer
The CRT’s ability to respond quickly and effectively to “tense situation[s]” (Matt–MH) made frontline staff feel safer and better supported. Matt thought if the response to a person on a bridge had been mental health led, it might have been slower and the threatened suicide may not have been averted. “[Mental health services] are able to respond quick to acute situations, but CRT are able to respond faster” (Matt–MH).
The CRT further enhanced safety through their multidisciplinary expertise. The multifactorial nature of complex presentations could often be addressed immediately, including physical, mental health and risk containment needs. [He] often presents with multiple issues - mental health and physical health, so it’s great that the paramedic is there and there is a mental health person. (Matt–MH)
Both paramedic participants felt having access to the CRT meant they could perform their job better and more safely. Being informed about people’s past mental health crises and behaviour enabled paramedics to predict “how they are going to react” (Fin–A) and to anticipate any risks on re-presentation. Nina appreciated that on a recent dispatch, the CRT (via ambulance communication) informed her of some signature risks, enabling her to take precautionary steps.
Better for the person
The CRT was praised for their de-escalation expertise. Police officers identified the CRT had advanced skills “talk[ing] with people who are at the higher ends [of distress or self-harm risk]” (Olaf–P) and to defuse these situations. The advantage of [CRT response] is that we've been able to stop things from escalating ... the runaway train is just leaving the station and we are just on time to put the brake on. If we got there half an hour, an hour later, the train will be away, and it'd be a whole different scenario. (Nick-C)
This approach often avoided the use of coercive interventions and could “resolve the incident within minutes to an hour, which is really great for us” (Martin–P). A police-only response, while rapid, could escalate an emergency situation resulting in the use of force. I was told that [before the CRT intervened] the person was about to be tasered [and the CRT prevented this]. (Matt–MH)
Participants thought people in crisis were less frightened with CRT involvement. A non-uniformed CRT mental health clinician was considered less threatening than a uniformed police officer. This assisted with engagement and potentially averted escalation. We had a job where a chap was having paranoid hallucinations, had assaulted [a family member] quite badly. The parents were reluctant to engage with mental health because they didn't want the son to be sectioned …[The CRT were] able to spend some extra time with the family, talk through the options… put a plan in place for their son ... For me, that particular job was one that …[had] potential to turn into something more serious … So, they [CRT] really do make a real difference. (Lucy–P)
The CRT was viewed as being sensitive to cultural needs. A Cook Island Māori CRT member shared how she was able to utilise her cultural background as a common ground at times, which enhanced rapport building (Analise–C). From the perspective of a Māori participant, a callout involving a Māori service user may have been culturally enhanced. A Māori representative may have been something she [the distressed person] would appreciate, or help keep us culturally safe, as long as this did not interfere with patient and crew physical safety. Support for any ethnicity would of course be amazing in this setting. (Nina–A)
However, non-Māori CRT staff were viewed to have “excellent communication skills” that allowed to “break those barriers anyway” (Analise–C), with Māori service users being treated with “dignity and respect that everyone deserves” (Nina–A).
Room for improvement
Not enough CRT
Few participants had negative experiences with the CRT. However, nearly all lamented insufficient CRT coverage. Participants regretted that the CRT did not work night shifts nor weekends despite “a high element of callouts during hours of darkness” (Martin-P). CRT staff could not attend every job and “don’t always get the opportunity to intervene as quickly [as we would like]” (Nicola-C), something viewed as “hard” by police (Gilly-P). We [mental health services] have had it today. The Police had been with a person who was threatening suicide … and they requested us to go, and we just literally don't have the people [available to attend]. But [if] it's in the time where the CRT is [rostered on, it’s] great. Really awesome to have them to be able to go out and respond immediately. (Moni–MH)
CRT staff disliked there only being one paramedic on the team compared to two CRT police officers and two CRT mental health clinicians. This was viewed as unmanageable, unfair and potentially “gonna break someone” (Nick-C). Moreover, the paramedic’s involvement in every callout meant that incoming ambulance calls were not well monitored by the CRT.
Unsatisfactory interface with services
Crisis mental health clinicians were dissatisfied with how the CRT linked up with their service. Firstly, they resented completing mental health assessments when the CRT clinician had already completed an assessment; it was viewed as an unnecessary duplication. Secondly, crisis mental health clinicians preferred the usual care approach where police waited in ED with people involved in 911-mental health/suicide risk calls (although not police, as covered earlier) as it ensured the person stayed in ED until assessed. Lastly, sometimes CRT service users had expectations that were difficult for crisis mental health services to meet, e.g., timely assessment or admission. [If] people get dropped off at ED, they still wait a long time to see us. (Moni–MH)
Discussion
Frontline staff considered the CRT a game changer. Usual care responses to emergency mental health/suicide risk callouts evinced feelings of dread, fear and a sense of failure. In comparison, the CRT enabled first responders to access better support, increase safety, and lead to better outcomes for the person. All participants wanted more CRT availability.
Similar to other studies (Boyd and Kerr, 2016; Sacre et al., 2022) and inquiries (Paterson et al., 2018), the business-as-usual 911-emergency mental health response was viewed as unsatisfactory and unsafe by participants. Police participants dreaded 911-mental health callouts, as they were often unable to access help from mental health services, findings that aligned with survey results (Kuehl et al., 2023). Consequently, the risk of violent incidents increased, police powers under mental health legislation were enacted more frequently and officers spent many hours in ED with a person sectioned under the MHA. This risk has been identified nationally (Paterson et al., 2018), with the outdated and over-used Mental Health (Compulsory Assessment and Treatment) Act (MHA) 1992 (Office of the Health and Disability Commissioner, 2018), currently being overhauled to create a shift towards recovery and a wellbeing approach (Ministry of Health, 2021). Using mental health legislation is a serious undertaking that may have significant impact on the individual and their family and should not be used “in case” to mitigate risk. The CRT provided timely support that offered alternatives to the use of coercive interventions.
The CRT involved community mental health clinicians from the outset of the 911-mental health crisis call, freeing up police officers. It was eye-opening for mental health clinicians to be privy to a holistic view of their clients. Despite complex health and social challenges of many mental health clients (Gibb and Cunningham, 2018), case managers are restricted to sole access of health information. The CRT changed this silo approach by sharing pertinent information with them (Ministry of Health, 2021). As a result, the person received support from somebody they knew during or following shortly after the 911-callout, enabling safe and effective support.
The CRT home team was able to provide timely advice and support to stakeholders irrespective of the field team’s dispatch status. Discussed elsewhere (Every-Palmer et al., 2022), within a 12-months period 65.1% of 911-mental health callouts were resolved by the CRT home team compared to 34.9% callouts attended by the field team. E.g. in another study, the ratio was 24.3% for telephone advice only and 75.7% for callouts (Meehan et al., 2019). Similar to a CRT ride along and control room support model where police officers are assisted remotely via telephone or police radio by a mental health worker (Puntis et al., 2018), our model included a designated CRT. What distinguishes this CRT is their proactive approach, actively monitoring incoming calls, discussing each callout, and reaching a team decision. As a result, stakeholders experienced timely person- and family-centred support.
Innovations on how to improve the management of 911-mental health crisis calls also need to benefit frontline staff. Our participants explained that the CRT’s proactive approach and expertise often defused tense situations, with the person being promptly referred/transferred to appropriate services. Participants believed that these strategies prevented escalation, and in some cases, a suicide. As police officers are at high risk of PTSD from exposure to suicide and other traumatic callouts (Cerel et al., 2019; Stanley et al., 2016), CRTs could support the wellbeing and retention of police officers and other frontline staff as well as benefiting service users and their families.
Clinical recommendations include increased access to the CRT and improved interface with crisis mental health services. For people requiring transport to ED for medical or psychiatric assessment and treatment, a location near ED that is like a ‘living room’ (peer support, welcoming and non-clinical furniture) (Shattell et al., 2014) instead of a waiting room would likely enhance people’s crisis experience. A follow-up evaluation on the planned national roll-out of the CRT, including interviews with service users and family members, is recommended.
Strengths and limitations
International literature about co-response models usually involves the views of a single professional group. A strength of this study was the combined perspectives of three professional groups, achieving saturation of themes. Results can be triangulated with quantitative data showing the co-response model had clear benefits in increasing the likelihood of crises being resolved in the community and reducing hospitalisations, ED response time, and repeat presentations (Every-Palmer et al., 2022).
It is imperative that the lived experience voice is privileged in terms of evaluating the CRT. In a companion study, we conducted qualitative interviews with 23 people who received CRT intervention or supported family members receiving intervention (Kuehl et al., 2024). Overall, there is a high concordance of themes from service users and professional staff, albeit from different perspectives. The majority of all stakeholders interviewed (89.4%, n = 42) were satisfied with the CRT, rating themselves as ‘extremely satisfied’ or ‘very satisfied’ (Kuehl et al., 2023). This, alongside the quantitative data, gives confidence in the validity of themes.
There was likely self-selection bias, a usual limitation in qualitative research. Individuals commonly participate in qualitative research if they have strong feelings about the subject, disproportionately attracting those with polarised views. There may have been others who had more humdrum CRT experiences who did not participate.
Furthermore, in the catchment area, like many other places, the demand for mental health services was high and services were overstretched. Police and ambulance staff had come to expect little help managing suicide/mental health emergencies. Because stakeholders had low expectations, it was not difficult for the CRT to exceed them. The ‘honeymoon’ period of high satisfaction and appreciation may degrade over time as people start to take the CRT for granted.
Conclusion
The CRT model was seen as game-changing, providing much-needed assistance to emergency staff managing suicide/mental health crises. The results of this study, alongside the data reporting better outcomes for service users, suggest the need for wider adoption of collaborative responses to manage mental health and suicide related crises.
Footnotes
Acknowledgements
Thank you to Director Simon Williams and Inspector Simon Welsh of the Evidence-Based Police Centre and to staff from the Police National Headquarters, particularly Inspector Brett Callander, Dr Melissa Smith, Ms Meredith Cole, and Ms Nicole Martin-Lupp, for supporting the study. Thank you to the three agencies who sponsored the CRT intervention: Wellington mental health services (MHAIDS 3DHB), Wellington Free Ambulance (WFA), and the Wellington District Police, and to the CRT team leader Senior Sergeant Matthew Morris.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NZ Police.