
Abstract
Research into post-traumatic stress disorder (PTSD) and other common mental disorders (CMDs) in police officers is limited, with the majority of research predominately conducted outside the UK, and no study quantitatively examining the role of social support in relation to the mental health of UK police officers working with victims of trauma. Therefore, this study aimed to examine the prevalence and predictors of PTSD and CMD in UK police officers who investigate rape, sexual exploitation and child abuse, along with the potential protective role of social support. Participants were police officers (n = 353) within one police area, who completed self-report measures of PTSD, anxiety, depression and social support. Results showed that 23% of officers had potentially clinical levels of PTSD, 26% had moderate to severe levels of anxiety and 35% had moderate to severe levels of depression. Female officers, those of constable rank, those working with victims of child abuse, and those with lowest levels of social support had poorer mental health. There was tentative evidence that social support statistically moderated the relationship between tenure and depression. These findings suggest the need for bespoke help for the sub-group of officers experiencing mental health problems and for further research into the potential protective role of social support.
Introduction
Policing is unique, as officers have to be a combination of crime fighter, rescue worker, counsellor, psychologist and social worker due to the routine and occupational exposure to violence, danger and traumatic events on a daily basis (Ellrich and Baier, 2017; Paton and Smith, 1999; Waters and Ussery, 2007). For a large number of officers this will also include exposure to secondary trauma through listening to the first-hand accounts of potentially the most traumatic experience of someone’s life, from both adult and child victims of violence and sexual abuse (Cartwright and Roach, 2020; Foley and Massey, 2019; Roach et al., 2018). Those UK police officers who investigate rape, sexual exploitation and child abuse have found to be particularly vulnerable to psychological injury due to the ‘high risk’ nature of their roles and their ongoing exposure to trauma (College of Policing, 2020). This habitual exposure to trauma is seen by some as an occupational hazard of policing (Bonnar, 2000; Huddleston et al., 2007; Wagner et al., 2020), yet clearly, without early identification, help and support, this continued and frequent exposure can in certain circumstances lead to significant mental health disorders such as anxiety, depression and in extreme cases post-traumatic stress disorder (Carlier et al., 1997; Greenberg et al., 2015; Wagner et al., 2020).
Post-traumatic stress disorder (PTSD) has been defined by the World Health Organization Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research, eleventh edition (ICD-11, World Health Organization, 2019) as being a disorder that may develop following ‘exposure to an extremely threatening or horrific event or series of events’. The American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, fifth edition (American Psychiatric Association, 2013) defines PTSD as a potential ‘consequence of exposure to actual or threatened death, serious injury, or sexual violence by either, directly experiencing the traumatic event (A1), witnessing the traumatic event (A2), learning of a violent or accidental traumatic event(s) which have occurred to someone close to them (A3), or experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (A4)’. Criteria (A4) is particularly relevant to policing and this study, as it uses the example of ‘police officers repeatedly exposed to details of child abuse’ as a group at risk of developing PTSD caused by ‘repeated or extreme exposure to aversive details of the traumatic event(s)’ they are exposed to (American Psychiatric Association, 2013). The ICD-11 (World Health Organization, 2019) also introduces Complex Post-Traumatic Stress Disorder (CPTSD). CPTSD is thought to develop in response to repeated exposure to traumatic events and, in addition to other PTSD symptoms, can include greater difficulties in sustaining relationships and controlling emotions, dissociation, feelings of guilt, shame or failure, and risky and destructive behaviours. The literature also refers to Compassion fatigue (Joinson, 1992), Secondary Traumatic Stress (STS) (e.g. Figley 1995; Stamm, 1995) and vicarious trauma (Pearlman and Saakvitne, 1995), which concern the impact of indirect exposure to traumatic material (e.g. police officers hearing victims accounts). Prevalence rates for PTSD in the UK are 3.7% for men and 5.1% for women (Baker, 2020), although rates may be higher amongst police officers, particularly within certain roles (College of Policing, 2019). Brewin et al. (2020) found that almost one in five police officers had symptoms consistent with either PTSD (8%) or complex PTSD (12.6%), although Stevelink et al. (2020) estimated a lower rate of 3.9%.
Anxiety is defined by the ICD-11 (World Health Organization, 2019) as ‘apprehensiveness or anticipation of future danger or misfortune accompanied by a feeling of worry, distress, or somatic symptoms of tension’. Both the ICD-11 (World Health Organization, 2019) and DSM-5 (American Psychiatric Association, 2013) give similar symptoms for diagnosis of ‘General Anxiety Disorder’ (GAD), which give rise to general apprehension or excessive worry, about everyday events which must persist for ‘several’ months for the ICD-11 (World Health Organization, 2019) or at least 6 months for the DSM-5 (American Psychiatric Association, 2013). Generalized anxiety disorder (GAD) is the most common anxiety disorder and one of the most common mental disorders worldwide (Munir and Takov, 2020). There are a number of potential symptoms for GAD that can include difficulty maintaining concentration, sleep disturbance, restless and muscular tension. The symptoms must also result in significant distress or significant impairment in important areas of daily functioning. Prevalence of Generalised Anxiety Disorder (GAD) within the population has been found to be at 5.9% (McManus, et al., 2016), although Stevelink et al. (2020) found higher levels of anxiety (8.5%) within the police officers and staff in their study.
Depression has been identified as the most common mental health disorders worldwide and a major public health issue (Liu et al., 2020), and is linked to suicidal ideation (Barron, 2010; Chopko et al., 2014). There are a number of different types of depressive disorders with the ICD-11 (World Health Organization, 2019) detailing single episode depressive disorder and recurrent depressive disorder, and the DSM-5 (American Psychiatric Association, 2013) detailing major depressive disorder and other types of depressive disorders such as persistent depressive disorder (Dysthymia). Both manuals list similar symptoms of depression, including depressed mood or diminished interest in activities, difficulty concentrating, feelings of worthlessness and hopelessness, recurrent thoughts of death or suicide, changes in appetite or sleep and reduced energy or fatigue, which need to have lasted for at least 2 weeks. Prevalence depression in the general population was found to be at 3.3% (McManus, et al., 2016), although once again Stevelink et al. (2020) found higher levels of depression (9.8%) within their study of police officers and police staff. They also found that exposure to trauma was a significant predictor of PTSD and CMD’s as those exposed to traumatic incidents in the previous 6 months had a six-fold increase in PTSD and a doubling in rates of anxiety or depression compared to those with no recent trauma exposure. Given the relatively high prevalence rates of depression, anxiety and PTSD amongst police officers and their repeated direct and indirect exposure to potentially traumatic events, it is important to understand the risk and protective factors associated with PTSD, anxiety, depression within the population of officers who investigate rape, sexual exploitation and child abuse, not least because this can help inform interventions and systems aimed at reducing and managing this risk.
There has been some research into predictors of officers' mental health, although in general the findings are usually varied. For length of service, Graham et al. (2020) found that levels of PTSD, anxiety and depression increased the longer officers worked in policing with more junior officers (those with less than 1 years’ service) showing the lowest average levels of PTSD, anxiety and depression. They also found that those having the lowest levels of wellbeing were those working in ‘Safeguarding’ (some of whom investigate child abuse, rape and sexual exploitation) as well as CID/local Investigations. These two groups of officers reported lower levels of emotional energy and higher levels of anxiety symptoms in comparison with other role types, although symptoms of depression and post-traumatic stress were found to be relatively similar level across all groups. Brewin et al. (2020) in their study of PTSD and Complex PTSD (CPTSD) also found that CPTSD was more prevalent in those officers with more years of service.
‘Tenure’ is a term used to highlight the length of time a person has remained within a certain role or unit. Burnett et al. (2019) found that tenure was a significant predictor of secondary traumatic stress and compassion fatigue, which was partially supported by Tehrani (2018), who found that increased time in the role was positively correlated with primary trauma, but not with anxiety, depression or secondary trauma. However, Hurrell et al. (2018) found no relationship between amount of time in the unit and levels of secondary traumatic stress. Turgoose et al. (2017) found that although overall levels of compassion fatigue, secondary traumatic stress and burnout were low, higher levels were associated with increased tenure in the role, but not with overall years of police service. They suggested that this may be something particular to those officers working with victims of rape compared to general police duties. Gray and Rydon-Grange (2019) also found that tenure in current role was associated with increased levels of secondary trauma and burnout, but this was not found in relation to overall length of service in policing, which supported the earlier work of Turgoose et al. (2017).
Another predictor that has been studied is gender. There are a number of studies which have highlighted gender differences between officers with being female associated with higher levels of PTSD and CMD’s (e.g. Bourke and Craun, 2014; Bowler et al., 2010; Brady, 2017). Tehrani (2016) found that female investigators suffered from secondary traumatic stress more than their male colleagues, which was replicated in a larger study 2 years later (Tehrani, 2018). Cartwright and Roach (2020) also found that there was a disproportionate number of female police employees being absent from work, compared with their male counterparts. This was supported by Fielding et al. (2018) who found that psychological injury/mental health was the most commonly reported cause of injury in officers, with levels of reported psychological trauma higher in female officers compared to male officers. Collins and Gibbs (2003) also found a significant association between gender and mental ill health with female police officers scoring higher than male officers in their study of stress related mental ill health. In contrast, other studies did not find any gender differences between levels of PTSD or CMDs (e.g. Andrew et al., 2008; Balmer et al., 2014; McCarty et al., 2007; Pole et al., 2001). Gray and Rydon-Grange (2019) and MacEachern et al. (2019) also did not find any significant gender differences in levels of secondary trauma and burnout. Furthermore, Brewin et al. (2020) found that both PTSD and Complex PTSD (CPTSD) were more common in male officers, which was also supported by Burnett et al. (2019) who found that male officers reported higher levels of stress and compassion fatigue than female officers. Therefore, the literature paints an inconsistent picture regarding any association between gender and mental health.
In relation to officer rank, Cartwright and Roach (2020) found constables accounted for the highest percentage of employees taking sick leave compared to other ranks. This was supported by Brewin et al. (2020), Graham et al. (2020) and Houdmont and Randall (2016) who all found that constables had higher levels of PTSD, CPTSD and CMD’s compared to other ranks. This was thought be because constables tended to have greater exposure to traumatic experiences due to the frontline nature of their role.
The concept of social support has been widely examined with a number of studies highlighting its importance for maintaining positive mental and physical health particularly after a traumatic event (e.g. Evans et al., 2013; Jackman et al., 2020; Prati and Pietrantoni 2010). Peer and social support are often described as multifaceted and complex constructs which depend on a number of individual variables such as ‘actual’ support (the network of friends an individual actually has) or ‘perceived’ support such as how satisfied an individual is with the people than can count on if needed (Ferrand et al., 2020; Sarason and Sarason, 2009). High levels of social support are associated with lower levels of PTSD, burnout and CMDs (e.g. Angehrn et al., 2021; Marmar et al., 2006; McCanlies et al., 2017), although a recent literature review (Foley et al., 2021) identified only one paper (Brown et al., 1999) that quantitatively measured the role of social support in a general UK policing population.
In summary, the current literature presents a mixed pattern of findings regarding predictors of PTSD and CMD’s, such as anxiety and depression in UK policing. Given this mixed set of findings and the importance of understanding the risk and protective factors relating to police officers' mental health, further research in this area is needed. Although some literature in other countries exists (e.g. Angehrn et al., 2021; Martin et al., 2009; Santa Maria et al., 2018), caution needs to be exercised when generalising findings between different countries, because of the differences in policing internationally, for example, whether officers routinely carry firearms. Therefore, one particular gap in the current literature is that no research has yet quantitatively examined whether social support acts as a protection against other potential risk factors in the development of PTSD, anxiety and depression in UK police officers. Arguably, this is particularly relevant for officers working in high-risk roles, such as with victims of child abuse, rape and sexual exploitation, given the higher levels of exposure to traumatic material (College of Policing, 2019, 2020; Graham et al., 2020; Hesketh and Tehrani, 2019). Therefore, the current study aimed to explore the predictors and prevalence of PTSD, anxiety and depression within UK police officers who investigate child abuse, rape and sexual exploitation, as well as the potentially protective effects of social support, that is, whether social support moderates the statistical effect of risk factors.
Hypotheses
Given the mixed findings in literature, the following hypotheses were tentatively made: H1 – The longer officers work within policing, the greater the likelihood of increased levels of PTSD, anxiety and depression. H2 – The longer officers work with victims of child abuse, rape and sexual exploitation, the greater the likelihood of increased levels of PTSD, anxiety and depression. H3 – Female officers will show higher levels of PTSD, anxiety and depression than male officers. H4 – Gender will moderate the relationships between length of service and PTSD, anxiety and depression, such that these associations will be weaker in male officers. H5 – Gender will moderate the relationships between tenure in the unit and PTSD, anxiety and depression, such that these associations will be weaker in male officers. H6 –Police and detective constables will have higher levels of PTSD, anxiety and depression, than more senior officers. H7 – Officers with higher levels of social support will have lower levels of PTSD, anxiety and depression. H8 – Social support will moderate the relationships between length of service and levels of PTSD, anxiety and depression, such that the associations will be stronger in those with lower levels of social support. H9 – Social support will moderate the relationships between tenure in the unit and levels of PTSD, anxiety and depression, such that the associations will be stronger in those with lower levels of social support.
In addition to the above hypotheses, exploratory analysis was planned to investigate whether the nature of officers' work, as indicated by the team each officer was in, predicted PTSD, anxiety and depression over and above the aforementioned predictors.
Method
Design
The study employed a cross-sectional survey design.
Participants and recruitment
Between January and February 2019, the online survey was sent via email to all officers between the ranks of constable and detective chief inspector (n = 908), within a unit that investigates child abuse, child sexual exploitation and serious sexual offences. In total 353 officers completed the survey, which represented a response rate of 39%. Due to the independent and confidential nature of the survey, the third-party server did not record those surveys that were opened, but not started, or started and left incomplete, so any data in this study that is referred to relates to completed surveys only.
In summary, 60.9% (n = 215) of respondents worked in the Rape and Serious Sexual Offences (RASSO) team; 34.3% (n = 121) worked in the Child Abuse Investigation Team (CAIT); and 4.8% (n = 17) worked in the Sexual Exploitation Team (SET). 62.3% (n = 220) of the sample was female and 37.7% (n = 121) were male. 82.2% (n = 290) of the officers were of constable rank, with 17.8% (n = 63) being at sergeant level or above. 3.1% (n = 11) were between 18–25 years old, 29.2% (n = 103) were aged between 26–35 years of age, 36% (n = 127) were between 36–45 years of age and 31.7% (n = 112) were 46 years old and above. For more detailed demographics, see the online supplementary material.
Measures
The survey collected demographic and occupational information (age, ethnicity, marital status, sex, years of service, years on unit, duty type, unit and rank/role) as well as the following measures, which were chosen due to their good psychometric properties and brevity, in order to maximise response rate.
Breslau-7 (Breslau et al., 1999): This is seven-symptom self-report screening scale for PTSD symptoms based on the DSM IV criteria (American Psychiatric Association, 1994), which asks participants to indicate whether they have experienced various symptoms associated with PTSD over the last month. Each of the questions requires a ‘Yes or No’ answer with the participant scoring 1 point for a ‘yes’ and 0 points for a ‘no’. A score of 4 or greater on this scale indicates that someone may be experiencing PTSD (Breslau et al., 1999). This scale has been used in a number of studies and found to have good levels of reliability and validity for identifying current levels of PTSD (e.g. Bohnert and Breslau, 2011; Horvath et al., 2021; Iversen et al., 2005; Kimerling et al., 2006).
Generalised anxiety disorder 7 (GAD-7; Spitzer et al., 2006): This seven-question self-report measure is a screening tool for the severity of GAD symptoms over the previous 2 weeks. The occurrence of each symptom is rated by participants on a 0 (‘not at all’) to 3 (‘nearly every day’) response scale. Total scores of 0–4 are considered minimal severity, 5–9 mild severity, 10–14 moderate severity and 15–21 severe (Spitzer et al., 2006). The GAD-7 has demonstrated high levels of reliability and validity for identifying current levels of GAD (e.g. Delgadillo et al., 2012; Löwe et al., 2008; Seo and Park, 2015a).
Patient Health Questionnaire-9 (PHQ-9; Kronke et al., 2001): This nine-item self-report questionnaire asks participants to rate their experience of symptoms of depression over the past 2 week, using the same response scale as the GAD-7. Total scores of 0–4 are considered minimal severity, 5–9 mild severity, 10–14 moderate severity, 15–19 moderately severe severity and 20–27 severe (Kronke et al., 2001). The PHQ-9 is widely used and has demonstrated high levels of reliability and validity for identifying current levels of depression (e.g. Beard et al., 2016; Kocalevent et al., 2013; Martin et al., 2006; Seo and Park, 2015b).
The Social Support Questionnaire 6 (SSQ-6; Sarason et al., 1983): The SSQ-6 is a short form of the full SSQ (Sarason et al., 1983) and consists of six questions intended to measure perceived availability of and satisfaction with social support, with each question split into two parts. The first part asks the respondent to identify how many people are available to support them in relation a particular context. The second part asks how satisfied they are with the number of people identified in the first part, using a 6-point Likert scale from ‘1 - very dissatisfied’ to ‘6 - very satisfied’. The scores for both parts of all six questions are added together. A total score of 30 and below is taken to indicate minimal social support, 31–60 moderate levels of social support and 61 and above high levels of social support (Sarason et al., 1983). This scale has been widely used and again found to have good levels of reliability and validity (e.g. Friedman et al., 2018; Kneavel, 2020; Tan et al., 2021).
Ethical approval
Ethical approval was granted by the Canterbury Christ Church University Ethics Panel, and occupational approval to conduct this study was granted by the senior leadership team, unit Police Federation, and occupational health services from the police force that the officers worked in. All participants provided informed consent. The survey was completed anonymously and hosted on an independent external server to reassurance the participants that the results could not be traced back to them. To further preserve anonymity, some data such as length of service and age ranges, were requested in bands (e.g. 0–5 years). Participants were advised of the content of the survey prior to consent and had the option of requesting their individual scores and details of organisations, both internally and externally, that they could contact should they need support.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics (Version 26) software. To test the hypotheses various statistical tests were employed including Pearson’s correlation coefficient to measure the association between variables; independent-sample t tests to determine any statistically significant difference in means between groups; Hedge’s g to measure between group effect size; regression analysis to estimate the relationships between predictor variables and PTSD, anxiety and depression. In case of minor violations of t test assumptions, the findings were checked using bootstrapping. Unless otherwise stated, the bootstrapped version gave the same finding as the standard version and so the latter is reported. Moderation analysis was conducted using PROCESS for SPSS Version 3.5 (Hayes, 2017). Finally, where data (e.g. length of service) had been collected in bands to preserve confidentiality, they were converted into a continuous scale by taking the midpoint of the band’s range, for example, 0–5 years was converted to 2.5 years. This enabled such data to be used in the aforementioned analyses.
Results
Levels of PTSD, anxiety and depression
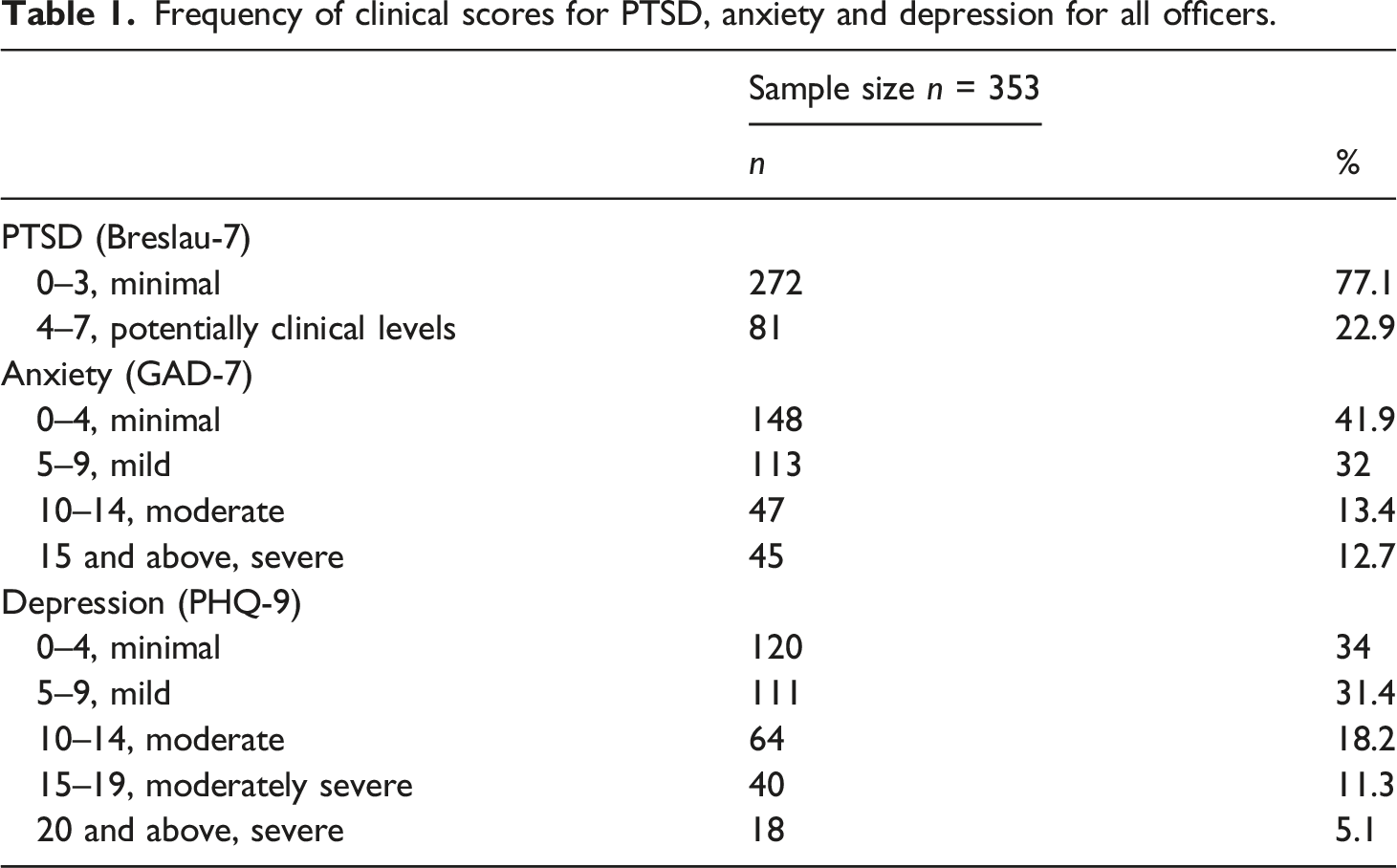
Frequency of clinical scores for PTSD, anxiety and depression for all officers.
Length of service in policing and tenure
H1 – The longer officers work within policing, the greater the likelihood of increased levels of PTSD, anxiety and depression.
The majority of officers had more than 10 years’ service in policing (n = 232, 65.8%), with the largest individual group of officers having between 11–15 years’ service (n = 100, 28.3%), and just over a third having 10 years or less service (n = 121, 34.2%). Contrary to H1, linear regression analyses showed that years of service was not a significant predicator of PTSD (F(1,351) = 0.017, p = 0.897), anxiety (F(1,351) = 0.409, p = 0.523) or depression (F(1,351) = 0.027, p = 0.870).
H2 – The longer officers work with victims of child abuse, rape and sexual exploitation, the greater the likelihood of increased levels of PTSD, anxiety and depression.
The majority of officers had 4 years or less tenure within child abuse, rape and sexual exploitation units (n = 250, 70.8%), with only a small number of officers having tenure of 10 years or more (n = 26, 7.4%). Contrary to H2, linear regression analyses showed tenure was not a significant predictor of PTSD (F(1,351) = 1.301, p = 0.255), anxiety (F(1,351) = 2.904, p = 0.089) or depression (F(1,351) = 3.334, p = 0.069). It is perhaps worth noting that both anxiety and depression came close to being significant predictors, but even if they did become so in a study with a larger sample, the effect size would likely be small.
Gender
H3 – Female officers will show higher levels of PTSD, anxiety and depression than male officers.
Mean, standard deviations (SD),t test and Hedges’ g results for male and female officers in relation to levels of PTSD, anxiety and depression.
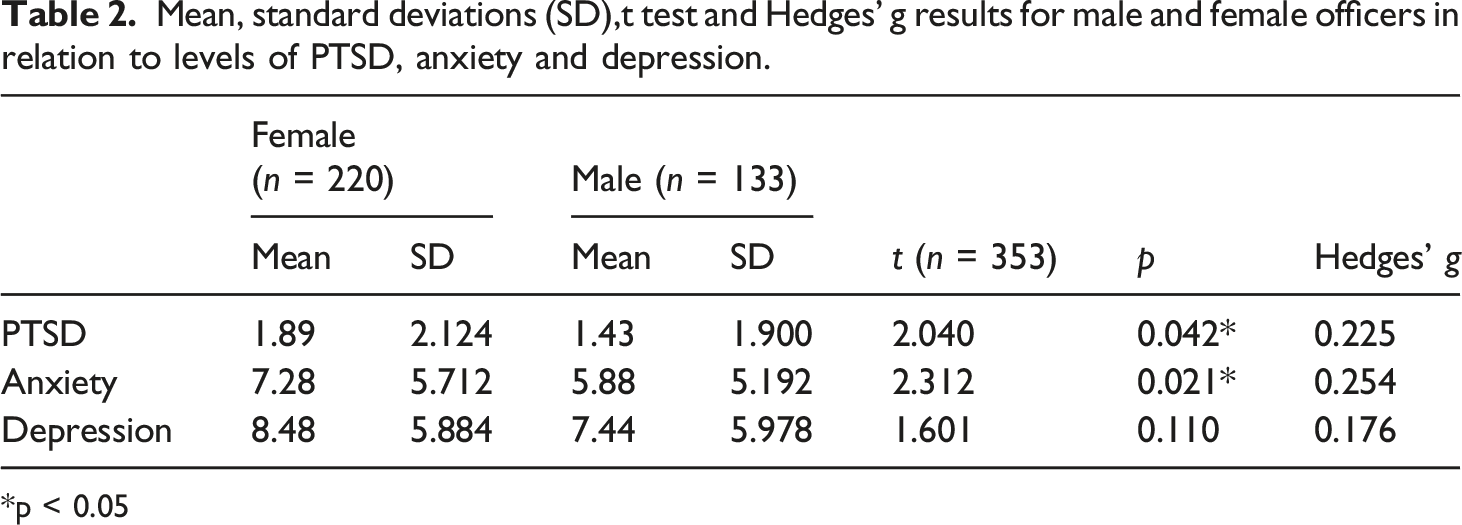
*p < 0.05
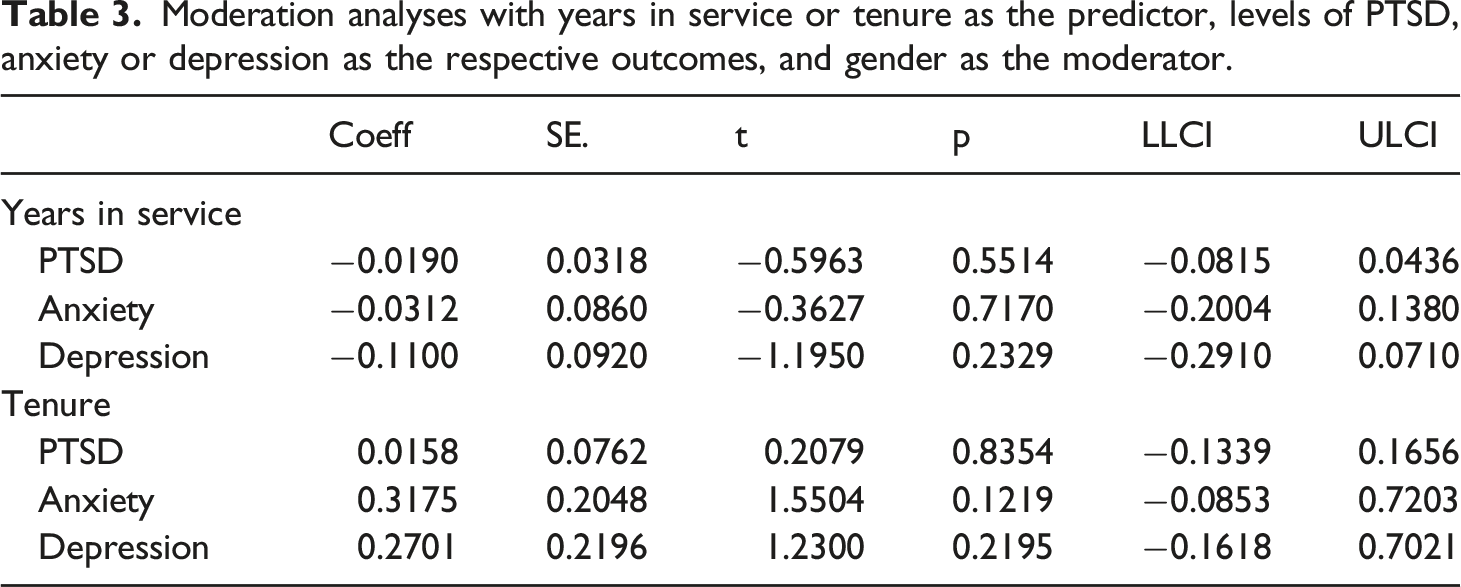
H4 – Gender will moderate the relationships between length of service and PTSD, anxiety and depression, such that these associations will be weaker in male officers.
H5 – Gender will moderate the relationships between tenure in the unit and PTSD, anxiety and depression, such that these associations will be weaker in male officers.
Moderation analyses with years in service or tenure as the predictor, levels of PTSD, anxiety or depression as the respective outcomes, and gender as the moderator.
Rank
H6 – Police and detective constables will have higher levels of PTSD, anxiety and depression, than more senior officers.
Mean, standard deviations (SD), t test and Hedges’ g results for constables and managers in relation to levels of PTSD, anxiety and depression.
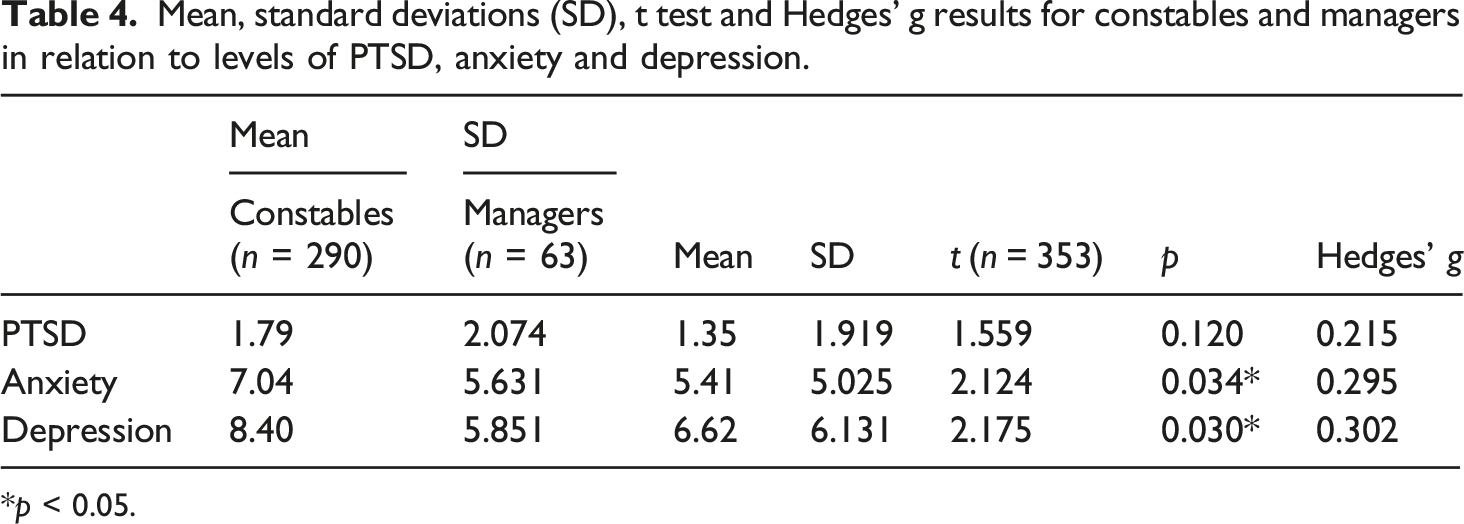
*p < 0.05.
Social support
H7 – Officers with higher levels of social support will have lower levels of PTSD, anxiety and depression.
Overall, 32% (n = 113) of officers indicated high levels of social support, 49.6% (n = 175) indicated moderate levels of social support and 18.4% (n = 65) indicated low levels of social support. Social support had significant, medium to large, negative Pearson’s correlations with PTSD (r = −0.349, n = 353, p = <0.001), anxiety (r = −0.416, n = 353, p = <0.001) and depression (r = −0.489, n = 353, p = <0.001). Thus, as hypothesised, there was a negative association between social support and all three variables.
H8 – Social support will moderate the relationships between length of service and levels of PTSD, anxiety and depression, such that the associations will be stronger in those with lower levels of social support.
H9 – Social support will moderate the relationships between tenure in the unit and levels of PTSD, anxiety and depression, such that the associations will be stronger in those with lower levels of social support.
Moderation analysis between years’ service in policing and levels of PTSD, anxiety and depression where social support is the moderator.
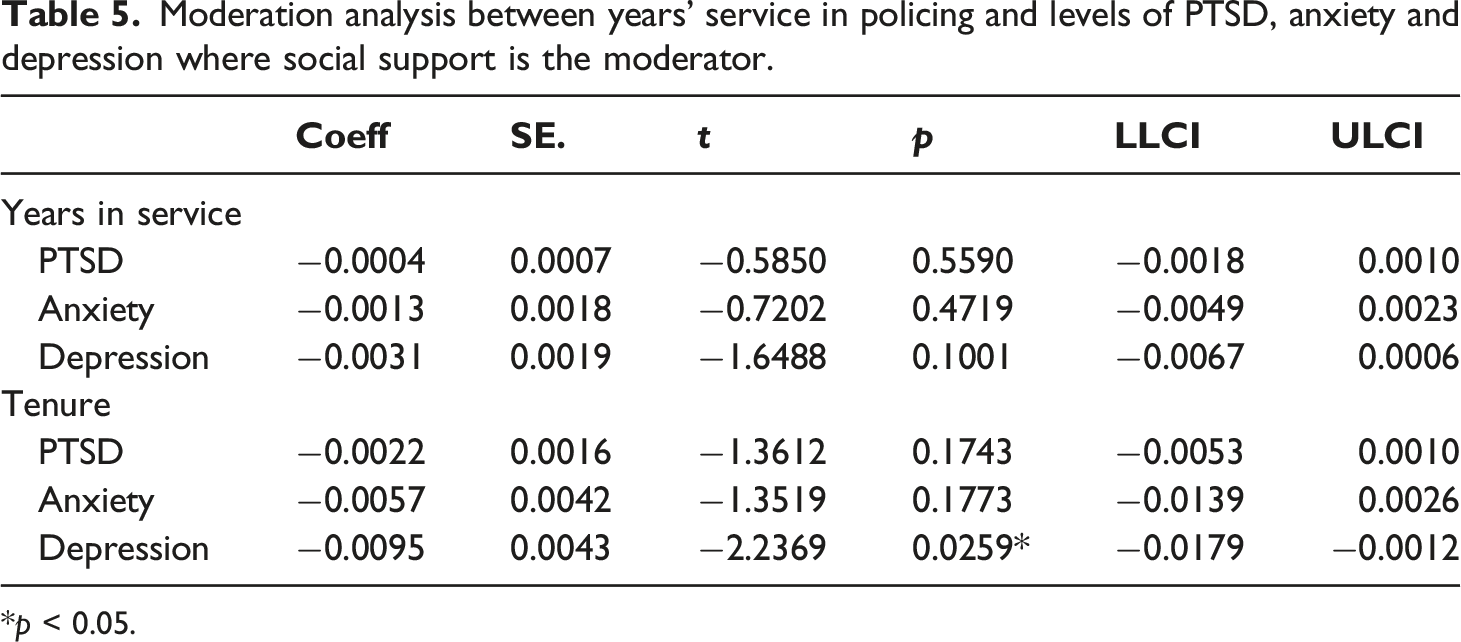
*p < 0.05.
Conditional effects of the years on unit on depression, for different values of the moderator, social support.
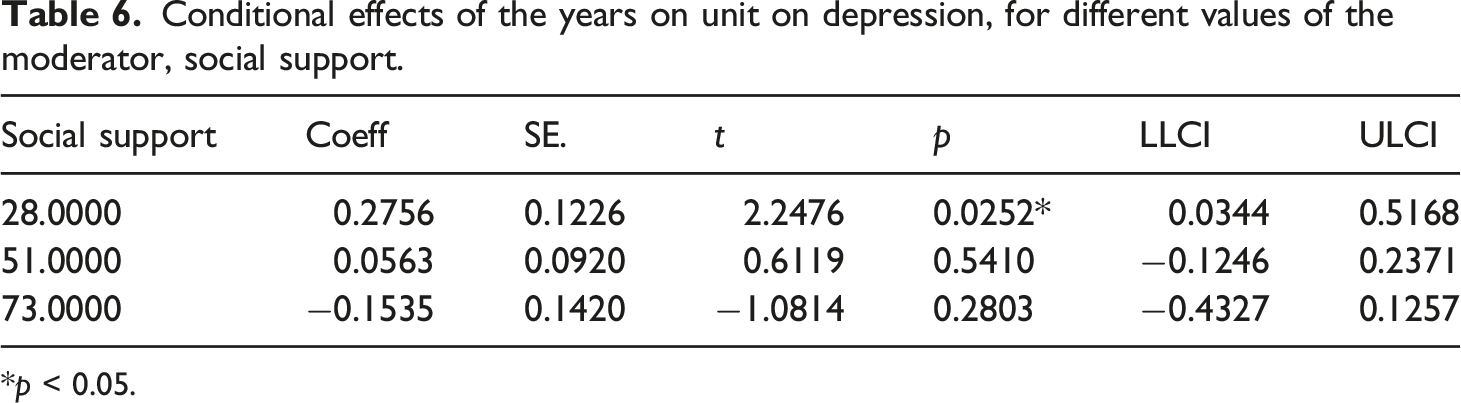
*p < 0.05.
Teams
Levels of PTSD, anxiety and depression between RASSO and CAIT teams.
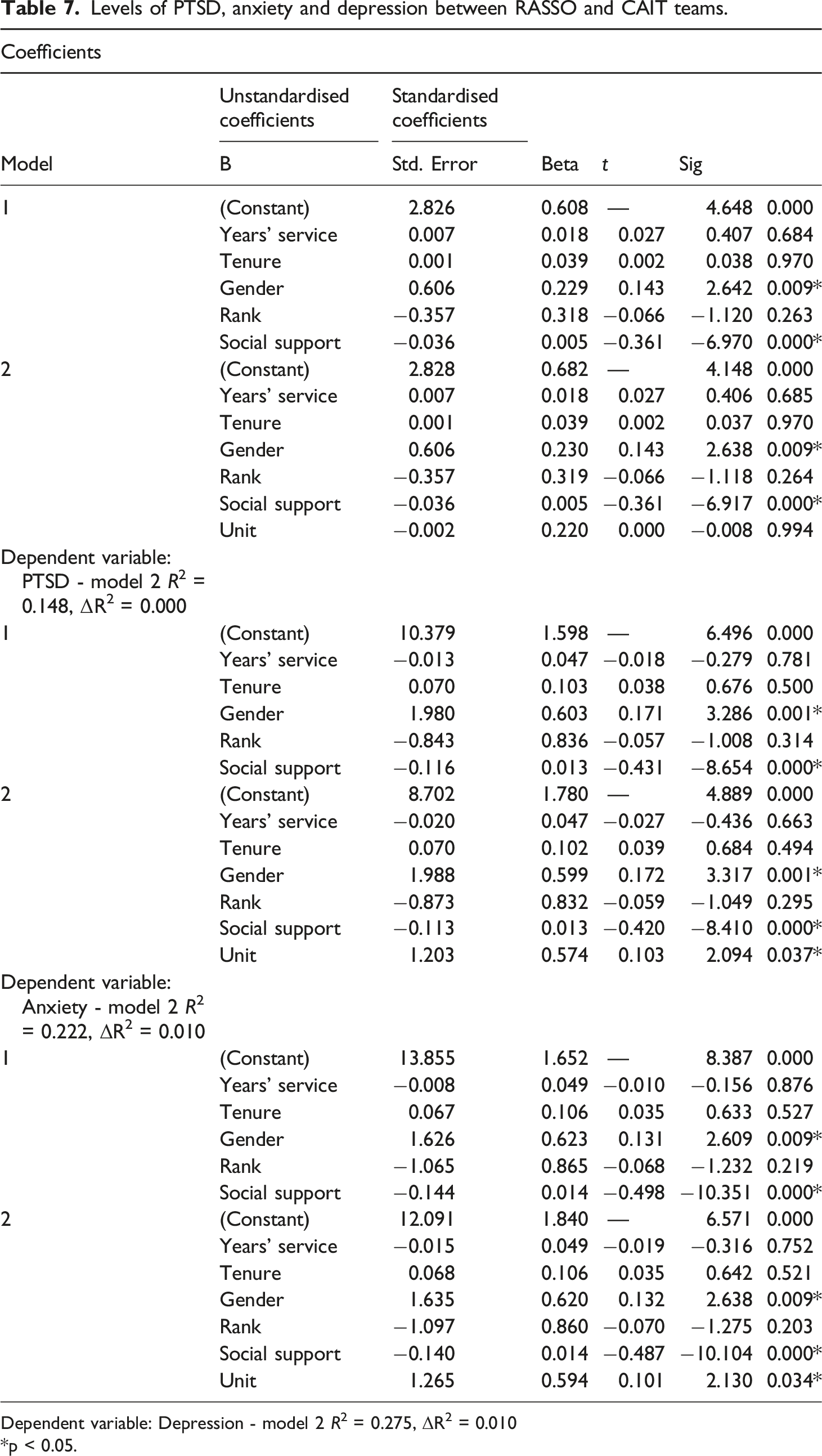
Dependent variable: Depression - model 2 R2 = 0.275, ΔR2 = 0.010
*p < 0.05.
Discussion
The aim of this study was to explore the predictors and prevalence of PTSD, anxiety and depression within UK police officers who investigate child abuse, rape and sexual exploitation, as well as the potentially protective effects of social support. The study found that the average levels for the whole sample were in the minimal range for PTSD, and the mild range for both anxiety and depression. However, it estimated that that 22.9% of officers had potentially clinical levels of PTSD, 26.1% had moderate to severe levels of anxiety, 34.6% of officers had moderate to severe levels of depression and 12.7% were potentially experiencing clinical levels of all three.
There have been limited quantitative studies that have been conducted with similar populations of UK police officers. Turgoose et al. (2017) found that, in 142 RASSO officers, average levels of STS were within the normal range, but there was a sub-group of 26% of officers with moderate, high or severe levels of STS. Similarly, Hurrell et al. (2018) found that 35% of their sample of officers who investigated child abuse met the criterion for probable PTSD on the STS scale, though only 12% had clinical levels of anxiety and 6% for depression. Gray and Rydon-Grange (2019) in their study of 78 staff from specialist sexual and violent offending teams, found that levels of secondary trauma were low or mild within their sample and MacEachern et al. (2019), in their study of 63 officers primarily engaged in child abuse investigations, again found that overall, 51% (n = 32) experienced little or no STS, although as seen in similar studies, some officers (11%, n = 7) were found to be in the high and severe range. Thus, both the current and previous studies suggest that, overall, most officers working with victims of child abuse, rape and sexual exploitation on average have little or mild levels of PTSD, anxiety or depression, but that a sub-group of officer’s experience clinical levels of difficulty. The current study adds to the existing prevalence literature by specifically examining the levels of PTSD (not STS), as well as anxiety and depression, in a large sample of officers (n = 353) that investigate both child abuse, rape and sexual exploitation.
Predictors of PTSD, anxiety and depression
It was initially hypothesised that the longer an officer worked with victims of child abuse, child sexual exploitation and rape the greater the levels of PTSD, anxiety and depression that officer would be experiencing. This hypothesis were based on the likely increased level of exposure to trauma and traumatised victims, which was measured in terms of years of service in policing and years of service within the unit (tenure). However, neither years in policing or tenure were significant predictors of PTSD, anxiety or depression. One possible explanation of this could be that years in policing and tenure are not sufficiently good for trauma exposure, as the amount, nature and severity of exposure can vary substantially between officers within such commands. It is also worth noting that most officers had 4 years or less tenure within their teams. It is possible that longer serving officers who were experiencing PTSD, depression or anxiety had left these teams and/or the police service, attenuating the predictive strength of length in policing and tenure. The findings in current study contrast with those of some other studies have that found that that longer time in the role may predict greater secondary trauma and CMD’s (Burke, 1989; Harman, 2019; Perez et al., 2010). However, it is worth noting that these finding tend to be from policing outside the UK and/or different types of policing, where the context is different.
Turning to gender, as predicted, female officers had higher levels of PTSD and anxiety than male officers. However, contrary to the hypotheses, the two groups did not significantly differ in levels of depression, and gender did not interact with years in service or tenure when predicting PTSD or CMDs. The finding of greater levels of PTSD and anxiety in female officers, but no difference in depression, fits with the pattern reported in the DSM-5 manual for the general population (American Psychiatric Association, 2013). It is perhaps unsurprising that gender did not moderate the relationship between length of service/tenure and mental health, as no such relationship was found.
With regard to rank, due to increased levels of exposure, and contact with traumatised victims, it was hypothesised that constables would have greater levels of PTSD and CMDs compared to their managers. This is indeed what was found for anxiety and depression, though not for PTSD. The findings regarding anxiety and depression fit with previous UK policing research (e.g. Cartwright and Roach, 2020; Graham et al., 2020; Houdmont and Randall, 2016). Furthermore, it is possible that the failure to find a difference in PTSD is a Type II error because some previous research has found higher levels in lower ranks (Brewin et al., 2020) and there was a (non-significant) trend in that direction in the current study.
Peer and social support
The results highlighted that overall, perceived availability and satisfaction with social support within the command was generally at a relatively high level, with almost 82% of officers evidencing ‘high to moderate’ levels of social support. Those with higher levels of social support had significantly lower levels of PTSD and CMDs. Furthermore, social support statistically moderated the relationship between tenure in unit and depression, such that for those with the lowest levels of social support, longer tenure predicted higher depression, while for those with higher levels of social support, this relationship no longer existed. To the best of the author’s knowledge, this is the first study to have quantitatively examined the moderating effect of social support in UK policing. While it is possible that this finding is a Type I error, and hence should be examined in a replication, it is nevertheless consistent with research from outside policing that suggests social support can protect against depression (Gariepy et al., 2016).
Differences between units
Exploratory analysis was conducted in order to examine whether the different types of work being conducted by officers (e.g. rape or child abuse investigation) was a potential predictor of PTSD, anxiety or depression. This study found that working in child abuse investigation predicted higher levels of anxiety and depression, but not PTSD, when compared to those working in rape investigation. Furthermore, these effects were not due to any differences in gender, tenure, years of service, rank or social support between the two units, as these were controlled for in the analysis. While this finding is consistent with previous literature that has suggested high levels of CMD in CAIT officers (College of Policing, 2019, 2020), this is the first study to compare differences between those who investigate child abuse and rape.
Strengths and limitations
Strengths of the current study include the relatively high response rate of 39%, which was likely supported by using a confidential, anonymous third-party server to host the survey; the use clinically validated measures of PTSD, anxiety, and depression, and the comparison of investigators working with different types of vulnerable victims of crime.
Study limitations include the possibility that the sample is biased in some way, given that 61% of officers did not respond; the possibility that participants may still have had some doubt over anonymity and hence that the findings may have been influenced by social desirability bias; the cross-sectional nature of the design meaning that causal conclusions could not be drawn nor trends over time examined; the possibility that common method variance may have inflated associations, given that all variables were measured by self-report questionnaire; the fact that the study was based in only one police area, potentially limiting generalisation; the small sample size for the sexual exploitation team (due to the small size of this team) meaning that it was not possible to include them in the comparative analysis; and the fact that this survey could not differentiate between external stressors (such as factors impacting on officers which were occurring outside of policing) or take into account any information about previous mental health problems, which was intentionally not collected in case doing so impaired participant recruitment and because historic mental health is not easy to accurately assess using online surveys. It may be worthy of note that familywise error (alpha) may have been inflated due to the multiple statistical tests conducted. Therefore, there is the potential that some of the significant findings within this study may be Type I errors, so it would be useful for future studies to attempt to replicate this findings.
Finally, whenever conducting studies in policing, researchers need to be mindful of police culture and the impact of stigma regarding officers admitting they are struggling with going sick with stress or CMDs as it can been seen as a weakness, requiring officers to hide their illness (e.g. Angiolini, 2015; Bell et al., 2022) which may have impacted on these results. Marshall et al. (2021), highlights the impact of stigma and under-reporting of CMD’s in police officers when they sent out two identical mental health screening questionnaries for completion. One of which was sent to officers by their employer, and one was from an independent third-party organisation. The results showed that even though the questionnaries were identical, some officers under-reported symptoms of mental health disorders to their employers with only 76.3% of symptoms declared. This was regardless of gender or symptom type, with those with more severe symptoms including PTSD and other CMD’s being significantly more likely to under-report their symptoms.
Implications for practice and future research
Together with previous research, the results of this study indicate that there is a sub-group of officers working with traumatised victims who themselves are suffering from significant mental health problems and are therefore in need of support. Thus, it is important to continue with efforts to eradicate the stigma of mental health in policing and normalise officers' help-seeking for CMD and PTSD. The current findings also suggest that female officers; those of constable rank; those working with victims of child abuse, and those with lowest levels of social support may be in greater need of help. Furthermore, the study tentatively suggests that social support may be a protective factor that helps protect against the effect of greater exposure to traumatic material as tenure increases. Given the tentative nature of this finding, it will be important to examine further, including in longitudinal research. Should such research confirm this, interventions to improve social support amongst officers who have low levels would be worth developing.
Conclusions
This study reinforces and extends our knowledge of the prevalence and predictors of CMD and PTSD in UK police officers working with victims of child abuse, rape and sexual exploitation. Similar to previous research, it has identified a sub-group of officers with mental health difficulties, with higher levels being observed in female officers, those of constable rank, those working with victims of child abuse and those with lowest levels of social support. To the best of the authors' knowledge this is the first study to have quantitatively examined the protective role of social support in UK police officers working with victims of child abuse, rape and sexual exploitation. If the tentative finding that social support statistically moderates the relationship between tenure and depression is confirmed by future research, then interventions to increase social support would be worth trialling. Regardless, it is evident that there is a need to provide help to the sub-group of officers with clinical levels of PTSD and CMDs. It will be valuable for future research to examine whether the mental health difficulties experienced by this sub-group arise because some officers are ‘holding onto trauma’ from working with victims of child abuse, rape and sexual exploitation, or whether there may be other causes.
Supplemental Material
Supplemental Material - ‘Holding onto trauma?’ The prevalence and predictors of PTSD, anxiety and depression in police officers working with child abuse, rape and sexual exploitation victims
Supplemental Material for Prevalence and predictors of PTSD, anxiety and depression in police officers working with child abuse, rape and sexual exploitation victims by Jim Foley, Fergal Jones, Alex Hassett and Emma Williams in The Police Journal
Footnotes
Acknowledgements
The author would like to personally thank Dr. John Durkin for his support in developing the portal, which allowed officers to respond to this survey knowing that their answers would remain confidential.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.