
Abstract
Police staff working in digital forensics, scenes of crime and accident investigators as forensic investigators are exposed to scenes and materials which are highly distressing. Two thousand twenty-eight forensic investigators completed a psychological surveillance survey measuring the proportion of investigators above the cut-off level of anxiety, depression, PTSD, burnout, and secondary trauma. The results showed that forensic investigators had higher symptoms than those found in police officers. Measures of workability and health beliefs were used to identify the most significant hazards and resilience factors for this group. The paper provides recommendations for interventions to reduce the levels of psychological distress.
Introduction
One of the least studied groups in policing is the specialist police staff working in Forensics. While some police officers move into this work, most forensic investigators (FI) are police staff with a specialist degree in one or more branches of forensic science.
In the UK, there are three groupings of forensic investigators: (a) those involved at the scene of a crime or dealing with materials taken from the scene of a crime or disaster, for example, fingerprints, DNA, photographs, CCTV and footprints. (b) Collision Investigators, undertaking surveys, mechanical investigations and reconstructions of road crashes, and (c) Digital Forensic Examiners involved in examining computers and phones for online child abuse, terrorism, financial crime, trading in guns, drugs and people trafficking (College of Policing, 2022).
Every policing role involves hazards; however, the dangers faced by a response officer are very different to that of a forensic scientist and a collision investigator (Cartwright and Roach, 2021). Each police officer or staff member will have unique vulnerabilities and resilience factors dependent on their life experiences, personality, support and training (Tehrani and Piper, 2011). Police forces are required to meet their duty of care (HSE, 2013) to protect their employees’ health and well-being, including the specialist forensic investigators; they must undertake a role risk assessment to identify hazards (College of Policing, 2017). In addition to risk assessments, there is a requirement to undertake regular psychological surveillance of employees engaged in high-risk roles, to identify and deliver effective support (HSE, 2022) educate and train forensic investigators to recognise signs of traumatic stress (NHS Scotland, 2017) and provide management with information and opportunities to reduce hazards and improve support (Hesketh and Tehrani, 2018, DeSmet et al., 2021).
Psychological surveillance is increasingly important in emergency services (Tehrani & Anderson-Cole, 2021); the need to ensure that the questionnaires and other tools are valid and reliable is essential (Hughes, 2018). However, there is a balance to be achieved in the time taken to complete a set of surveillance questionnaires and their usefulness in identifying the health measures, hazards and resilience factors; if the surveillance tool takes too long to complete, it can lead to fatigue and less accurate completion. The Finnish Workability Index (Ilmarinen, 2009) was developed to measure health and functional capacity. It was found to have good predictive ability (Lundin et al., 2017), but due to its comprehensiveness took a long time to complete. Single questions from the Workability Index were identified and found to have comparative results to the longer Workability Index (Alistrom et al., 2010; Thoresen et al., 2012).
Mounting evidence indicates that working in police forensics is stressful, with high levels of burnout (Kelty and Gordon, 2014) and vicarious or secondary trauma (Slack, 2020; Tehrani, 2016). This study examines the results of annual psychological surveillance to establish the levels of clinical symptoms experienced by these three groups of forensic practitioners and how the symptoms compare with those found in police officers. In addition, to identify any resilience factors or significant risks to psychological health. Finally, there are recommendations for improving the psychological well-being of FIs.
The study
Role risk assessments
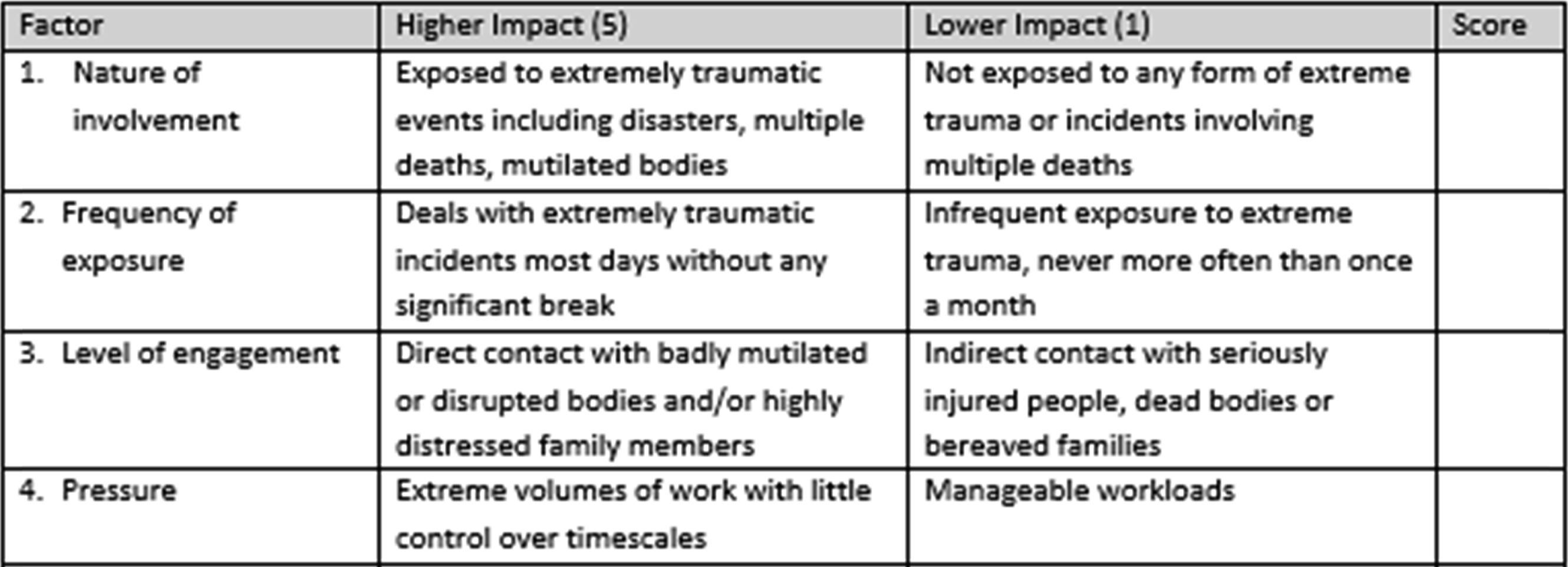
Each of the three forensic roles went through the role risk assessment process. The role risk assessment tool comprises of 10 factors, (1) Nature of Involvement, (2) Frequency of Exposure, (3) Level of Engagement, (4) Pressure, (5) Safeguarding (6) Prosecutions, (7) Team Support, (8) Autonomy, (9) Security/Safety, (10) Media. Each factor had high and low impact descriptors and an opportunity to score the factor within the range of 1–5. Role assessments are undertaken by three independent assessors familiar with the nature and scope of the role. The results were reviewed and scored by an Occupational Health professional to determine the level of risk. The role risk assessments for the three forensic teams confirmed that they all met the criteria for a minimum of annual psychological surveillance and support and that they were eligible to be part of the College of Policing programme of psychological surveillance.
Three factors in the role risk assessment for a Forensic Collision Investigator
College of policing surveillance programme
The College of Policing has funded the psychological surveillance of high-risk roles for police forces in England and Wales (College of Policing, 2017). Twenty-three forces including metropolitan, urban and rural forces have taken up the offer of surveillance for at least one of the three FI groups. The screening questionnaires being administered via a link sent by email directly to the FIs. Completed questionnaires were processed, and the screening reports sent to occupational health practitioners. FIs with clinically significant or borderline scores were referred for an assessment by an occupational health practitioner or psychologist where they were provided with well-being guidance and where appropriate a referral for trauma therapy.
Questionnaires
The screening questionnaires in the online screening were selected and had been validated within an occupational setting (Tehrani & Hesketh, 2018). The questionnaires included four self-assessment measures for anxiety, depression, primary and secondary trauma. The questionnaires were the Goldberg Anxiety/Depression Scale (Goldberg et al., 1988), with the anxiety and depression scores ranging from 0 to 9. The Professional Quality of Life (Stamm, 2009) measured compassion satisfaction, burnout and compassion fatigue. Higher scores on ‘burnout’ and ‘compassion fatigue’ and lower scores on ‘compassion satisfaction’ indicate adverse outcomes. The last clinical questionnaire was the Impact of Events-Extended (Tehrani et al., 2002), which measured the symptoms of avoidance, arousal and re-experience where total scores of 50 or more were indicative of PTSD. Cut-off levels to indicate clinically significant results had been calculated by the questionnaire developers and were:
Personal resilience was measured using the Sense of Coherence Scale (Antonovsky, 1987) with three subscales: meaningfulness, comprehensibility and manageability. Lower scores for a sense of coherence indicate a lower level of personal resilience. An eight-item lifestyle questionnaire based on well-being guidance from the National Health Service scored as either good, average or poor. The Emotional Literacy Questionnaire (ELQ) (Steiner and Perry, 1999) assessed emotional resilience and somatic sensitivity to traumatic events. The ELQ consisted of seven subscales with scores ranging from 0 to 6. The brief Cope questionnaire (Carver, 1997) measures active and passive coping styles. Adverse childhood experiences (Felitti et al., 1998) included emotional, physical, sexual, and domestic abuse exposure experienced by the FI in their childhood. Questions regarding other personal factors such as age, exposure to recent traumatic events, other traumas and addictive behaviours, together with questions on manager support and mental health stigma, were included. The two single item workability and health beliefs (Alistrom et al., 2010; Thoresen et al., 2012) “What is your current workability compared with your lifetime best?” and “In general, what would you say is your current state of health?” both questions were scored on a 5 point Likert scale ranging from poor to excellent.
The data was gathered as part of a psychological health surveillance programme. Where surveillance identified FIs with marginal or clinical scores, follow-up assessments, support and counselling were provided. The statistical analyses were performed using SPSS statistical software version 27.
Results
The data was gathered between 2017 and 2021. In total, 2028 FIs went through the surveillance process, of which 1018 were of Scene of Crimes Investigators, 702 Digital Forensic Investigators, and 308 Forensic Collision Investigators. 43.4% of those screened were female and 56.6% male. The average time in the role was 5.96 years (SD 3.1) and the maximum time in the role was 9 years. 12% of forensic investigators had experienced four or more adverse childhood experiences (Felitti et al., 1998). 80% of the FIs said they had good, very good or excellent support from their supervisors, and 90% said there was little or no mental health stigma in their team. The average number of sick days taken was 6.9 days, FIs had 28 h of untaken overtime. 87% of FI reported high or very high exposure to trauma, and 38% had intentions of leaving their role. The period of the study included the COVID pandemic years, inspection of the clinical results showed no significant difference between years.
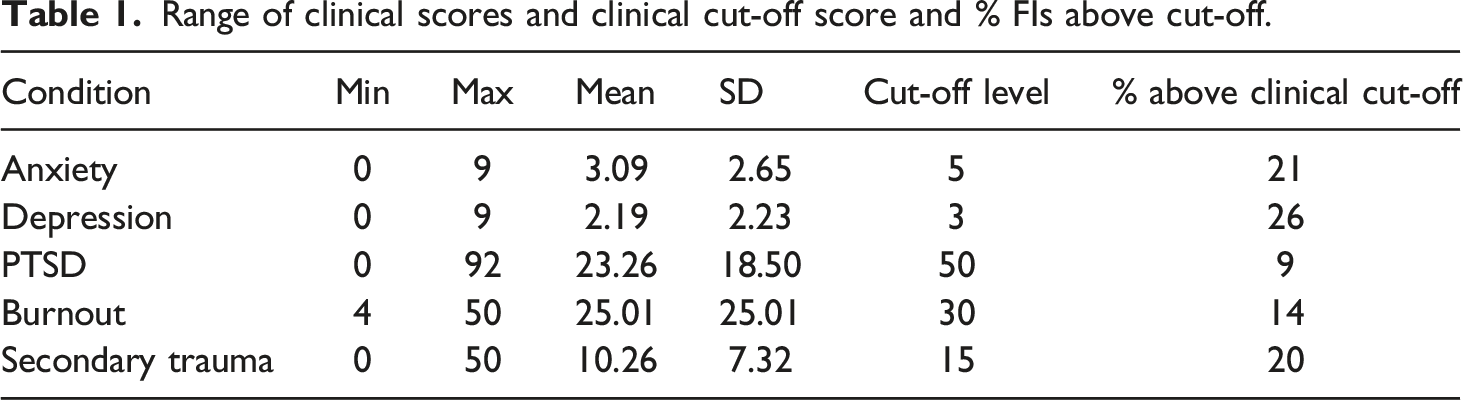
Range of clinical scores and clinical cut-off score and % FIs above cut-off.
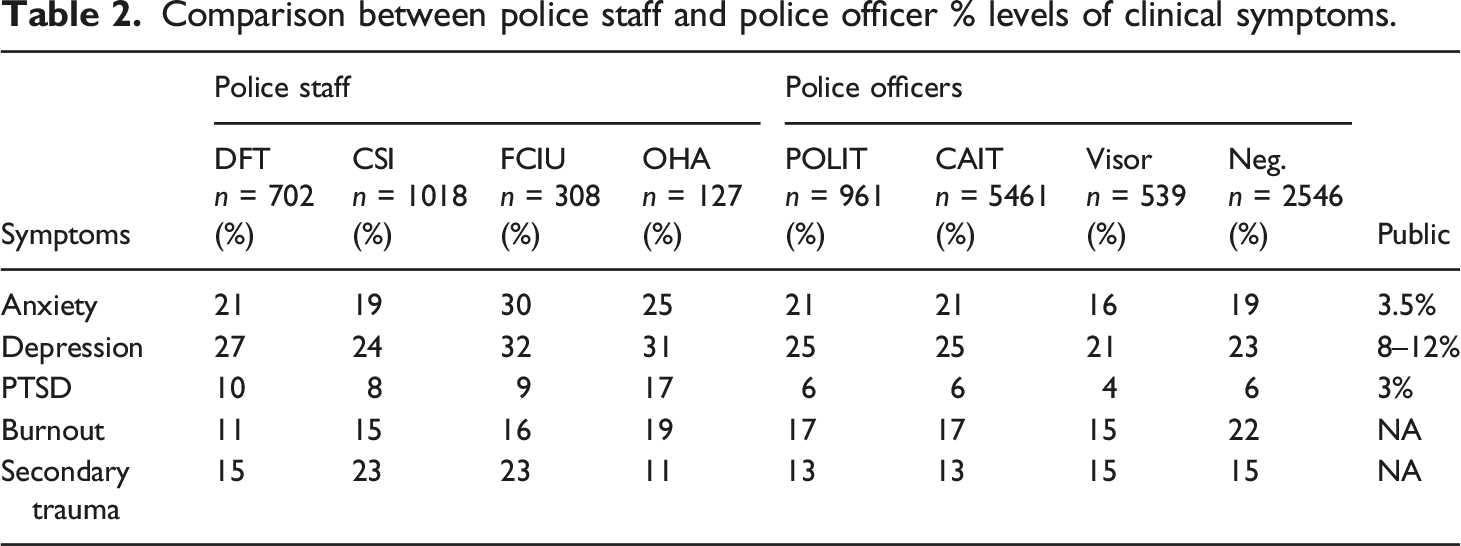
Comparison between police staff and police officer % levels of clinical symptoms.
Relationship between FI’s health beliefs and workability correlations with clinical symptoms.
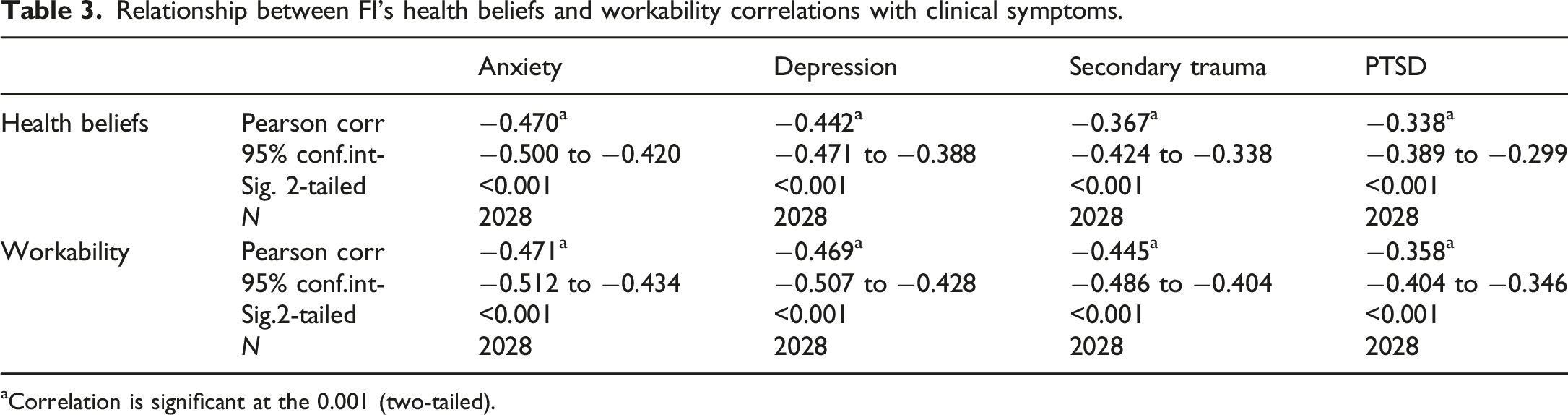
aCorrelation is significant at the 0.001 (two-tailed).
The next stage of the analysis used stepwise regression. A regression looks at the strength of the relationship between hazard and resilience factors, in this case, Workability and Health Beliefs. As the Workability and Health Beliefs measure similar FI attitudes, two separate stepwise regressions were undertaken to identify any shared variables and those unique to one of the outcomes. The correlation process occurs several times in the stepwise regression, each time removing the weakest correlated variable. At the end of the process only the variables that explain the distribution best remain.
Showing the seven shared predictive variables, seven additional predictive variables for health beliefs and eight additional predictive variables for workability.
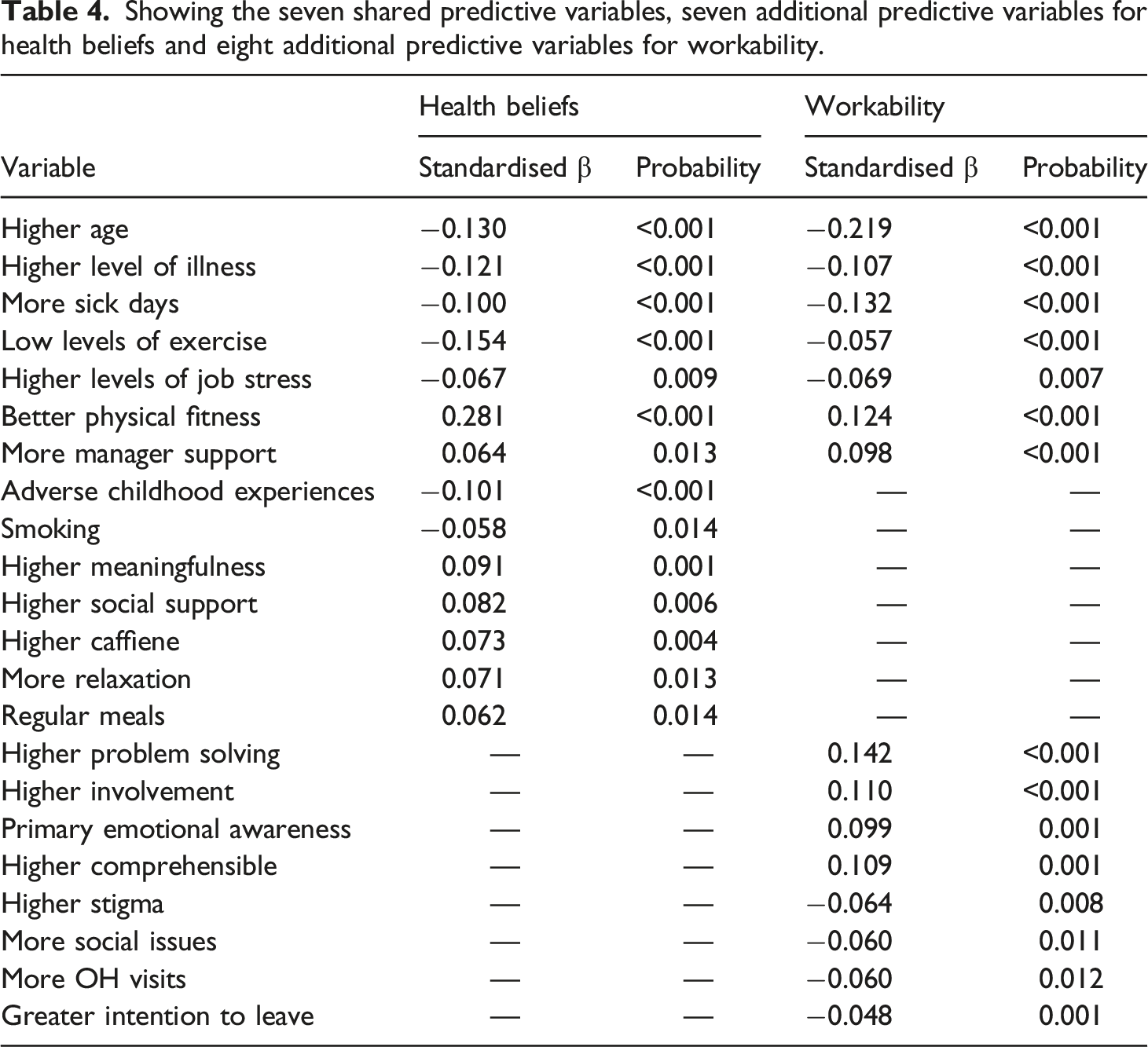
Several variables positively accounted for variance, including a meaningful role (9%), social support (8%), caffeine (7%), relaxation (7%) and regular meals (6%). The variables predicting positive workability were: problem-solving (14%), involvement (11%), higher comprehensibility (10%) and primary emotional awareness or “gut feelings” (9%). Variables predicting negative workability were: stigma (6%), social issues (6%), OH visits (6%) and intention to leave (5%).
Discussion
This study has demonstrated that the levels of clinical symptoms experienced by the three groups of forensic practitioners confirmed the view of Cartwright and Roach (2021) that more attention should be given to the wellbeing of police staff. Forensic investigators should be regarded as being at a similar, if not higher, level of risk compared to their police officer colleagues. This increased recognition of the psychological burden carried by FIs increases the need for this group of investigators to be included in psychological surveillance and support programmes. Police forces need to be alerted to their duty to these groups and to ensure they are regularly monitored and supported. Management information from the psychological surveillance could also help identify hazards and resilience factors that could be addressed in tailored primary, secondary and tertiary interventions (Holman et al., 2018).
The study confirmed the value of using the single workability and health beliefs measures to identify the hazards and resilience factors within a working group as a proxy for clinical symptoms. Unsurprisingly there was an overlap between workability and health beliefs; however, there were some crucial differences in the factors contributing to these attitudes to work and health in the FIs.
In the shared area, the common factors were that lower levels of workability and health were found in the older FIs; illness and sick days during the previous year was also a strong predictor of lower workability and health. Physical fitness and taking more exercise was also significant in supporting both measures. One paper (Almarzrouei et al., 2021) has indicated that manager support was not associated with stress in FIs; this study and others (Kelty et al., 2021) have found management support to be vital to workability and psychological well-being.
The variables significantly correlated with health beliefs included Adverse Childhood Experiences (ACE); this finding is consistent with Tehrani (2018) which identified ACE scores as a significant factor in increased PTSD symptoms in child abuse investigators. The results also showed that several lifestyle factors were also related to higher health beliefs, including not smoking, caffeine consumption and regular meals. The results also emphasised the importance of engaging in a meaningful role and having social support from colleagues.
Attitudes to work are important in maintaining an effective forensic team. Higher levels of problem-solving and willingness to get involved in problem-solving and make decisions were highly significant factors. Almazrouei et al. (2021) found that decision making was adversely affected by work-related stress, a finding that has been found in many settings (Regehr and LeBlanc, 2017). The personal capacities of being able to comprehend or understand where work fits into the larger objectives of the team and organisation and the ability to use intuition (primary emotional awareness) were also protective, as well as the ability to talk about mental health issues without the fear of being stigmatised by colleagues. Unsurprisingly, FIs not experiencing positive workability were more likely to need occupational health support and to want to leave the organisation.
Recommendations
The recommendations from this study have been divided into three groups: the primary recommendations related to policies and strategies, secondary recommendations involving training and development, and tertiary recommendations concerning individual interventions and support.
Primary interventions
Police Forces should introduce psychological surveillance for the three groups of forensic investigators, particularly those directly involved in dealing with the death and abuse of vulnerable people. They should consider the needs of FI as they age and, where possible, identify adjustments to the role to reduce the levels of exposure to traumatising material and ensure that workloads are reasonable. Particular attention needs to be given to monitoring sickness absence and making referrals to occupational health whenever there are signs that a FI is struggling. Recruitment should take account of the impact of adverse childhood experiences (ACE) on the resilience of the FI, ensuring that where an FI applicant had high levels of ACE scores, they were aware of the hazards within the role and alert them to the support available should they experience any symptoms of anxiety, depression or trauma.
Secondary interventions
FIs and their supervisors should be stress and trauma aware and recognise signs of psychological distress in themselves and others. Supervisors need to provide positive leadership and interpersonal skills to respond to personal and work-related issues and distress. There should be training in the resilience-building sense of coherence skills, including being fully committed to their work where their role is aligned with their personal values and they are able to articulate their purpose and role within wider investigations. This will require greater interactions with other policing groups to ensure FIs are always informed of the cases’ developments and outcomes. The FIs also would benefit from training in problem-solving, emotional regulation and intuitive thinking.
Tertiary interventions
There should be support for FIs, which may involve having peer wellbeing supporters in their teams. They need to be encouraged to improve their physical fitness and lifestyles through education sessions from occupational health or others on the importance of eating regular healthy meals, stopping smoking, reducing caffeine consumption and talking about their mental health.
Limitations and future opportunities
The study did not look at the impact of the actual work undertaken by the FIs. However, qualitative data was collected as part of the surveillance process; this could be analysed and augmented with interviews to understand better the impact of working in forensics. Factors involving particular incidents and crimes may influence anxiety, depression, and traumatic stress, as well as workability and health beliefs. Future studies could look for the aspects of s of the FI role and work which may pose increased hazards, such as time spent at the scene of a crime or the vulnerability of the victim.
Stepwise regression was used due to the study’s many potential predictors of mental health problems. Stepwise regression whilst valuable in narrowing down multiple variables in exploratory studies; miss some critical variables. Future studies need to build on these results and undertake a more focused analysis.
The study was cross-sectional which cannot establish causality, however the study provides an opportunity for police forces to introduce interventions including policy or procedural changes, training or support for FIs. The ongoing psychological surveillance programme could therefore be used to evaluate these interventions in longitudinal studies.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Noreen Tehrani is a director of NTA Psychological Screening Ltd, which undertook the surveillance programme adopted in this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.