
Abstract
Previous research has reported adverse health outcomes for emergency services personnel (ESP), outcomes that research more broadly has shown can be improved using a gamification and mobile health (mhealth) apps approach. We conducted a review of research on gamification and mhealth apps for ESP that had been published in the last 19 years using 6 major research databases. The results demonstrated that virtually no relevant research has been published, suggesting a significant gap in the evidence base of an approach that could potentially have significant benefits for the health of ESP.
Introduction
There is an ever-growing body of research evidence that demonstrates the negative health and well-being of emergency services personnel (ESP) and that suggests that health outcomes for ESP are worse than that of the general population (Arble and Arnetz, 2017; Brooks et al., 2019; Counson et al., 2019; Mildenhall, 2019; Varker et al., 2018). Recently it has become clear that ESPs may experience disproportionate negative outcomes through specific situations, as well as more general working, for example see Mildenhall (2020)’s guidance in the area of psychosocial and mental well-being targeting managers of ambulance personnel during the COVID-19 pandemic and Hesketh et al. (2018) for guidance associated to post-traumatic stress disorder (PTSD) and complex PTSD for police officers in the UK.
Although ‘emergency services’ covers a wide range of agencies, there are important commonalities in terms of the highly demanding nature of the work involved (Peñalba et al., 2008), including exposure to significant psychological (Duran et al., 2018; Milligan-Saville et al., 2018; Petrie et al., 2018) and job-related (Stanley et al., 2016) stressors. These stressors inevitably and understandably result in significant negative health outcomes, including depression (Wild et al., 2018) and PTSD (Ahmed et al., 2017), which can lead to an increased risk of alcohol use (Gulliver et al., 2018) and suicidal ideation and behaviours (Milligan-Saville et al., 2018).
The key question of whether the incidence of these negative health outcomes is higher than in the broader population has been explored through largescale surveys of the health of ESP. This has included a 2019 survey of 5,081 ESP (staff and volunteers) conducted by the UK charity MIND (Mind, 2019), which revealed that 67% of respondents reported they had lived experience of mental health problems (a rise from 55% in 2015), more than double that of the workforce in general. Moreover, the survey revealed ESP were less likely to take time off work as a result of mental health issues than the general workforce. Hesketh, Cooper and Ivy (2014) also noted this issue, describing how it can lead to ‘leaveism’, whereby policing personnel were found to hide health problems by using annual and other leave, rather than sick leave. More recently, an online survey of 16,857 serving UK police officers and staff in 2018 conducted by the University of Cambridge and sponsored by Police Care UK (Miller, 2018) found that 90% of respondents reported being exposed to trauma (98% of which was work related). Worryingly, analysis suggested that of the officers/staff who had experienced trauma, about 20% would be diagnosable as suffering from PTSD (8%) or complex PTSD (12%) yet only 5% will have been told someone and only 1 or 2% clinically diagnosed.
Although PTSD in ESPs has been the subject of research, estimations of incidence have varied greatly and it is not clear how this varies across the various services. For example, one review (Skogstad et al., 2013) reported that PTSD in the police is less than 10%, whereas 20% of paramedics and firefighters are thought to have PTSD. However, Miller (2018) suggests symptoms of PTSD and Complex PTSD are present in as many as one in five police officers and staff in the UK. Whilst this area is contested, and it seems it is not yet possible to estimate accurately how many ESPs are currently experiencing clinical levels of PTSD in the UK, it does seem very likely that the rate is higher than in the general population. The same is true when it comes to the additional three symptoms which would give a diagnosis of Complex PTSD, although a new measure has been developed which is based on ICD-11 criteria and may assist with establishing this (Cloitre et al., 2018).
Given these negative health outcomes, there would seem to be a pressing need to support the health and welfare of ESP. Peñalba et al. (2008) conducted a systematic review of randomised controlled trials (RCT), and quasi-RCTs, aimed at testing interventions for preventing psychological disorders in law enforcement officers. Of the 10 studies included in the review, 3 were on exercise-related psychological interventions and 7 on direct psychological interventions, of which 3 involved comparing a psychosocial intervention (e.g. cognitive behavioural or supportive therapies) to a control group. The authors concluded that there was insufficient evidence to establish the effectiveness of psychosocial interventions and a pressing need for high quality statistically powerful randomized control trial (RCT) studies to address this issue.
Although a large amount of research has been conducted on the health and well-being of ESP since the Peñalba et al. (2008) review, there has been a relative paucity of RCT studies on possible interventions. Moreover, some of the interventions that have been evaluated appear not to be effective. For example, Skeffington et al. (2016) conducted an RCT to assess the effectiveness of an intervention for trainee firefighters based on the Mental Agility and Psychological Strength Training Program (MAPS) but did not find evidence that the intervention prevented mental health issues compared to a no treatment control group. As Arble and Arnetz (2017) note, there are multiple pathways that could be used by ESP to increase well-being, and an integrative philosophy using physical health behaviours, both approach and avoidance coping strategies and social support might be a beneficial approach. It follows that that more limited, uni-dimensional interventions might not be sufficiently nuanced or comprehensive to make an appreciable difference.
In terms of contemporary approaches at the time of writing, the National Police Well-being Service (NPWS), developed by the College of Policing, has been particularly prominent and covers eight core elements to deliver tailored support and guidance for policing.
The eight elements begin by providing workshops, materials, toolkits and an online network to build the skills and abilities of executives, senior, middle and first-line managers. An overview of these eight facets are as follows:
This focus on leadership is essential to facilitate the other elements of the service. The second key part is concerned with personal resilience. Here the service establishes a positive psychology approach, utilising the work of Seligman (e.g. Seligman and Csikszentmihalyi, 2014). A further area is that of effective peer support and networks. These are particularly important in high risk roles, such as counter terrorism, firearms, child abuse work and homicide investigations. These are factored into the next element of the service, which addresses psychological screening and support. This risk management strategy will be embedded into most of the areas across UK policing and is seen as a key initiative to monitor officer and staff well-being and have an effective way of prioritising interventions, clinical medical and supervisory. Trauma and post incident support also feature as one of the eight live service offerings, with optimum policing models being developed in cooperation with Public Health England (PHE) and other specialists. A final offering is that of an outreach service, taking well-being to the front line by means of a fleet of vehicles that can be utilised by service providers to reach all elements of the policing population. The entire NPWS is performance managed by way of a robust benefits realisation programme.
Although the NPWS offers a broad approach to supporting the health and well-being of policing personnel it tends to rely on reasonably traditional, e.g. face- to- face, mechanisms of support and does not, at least explicitly, incorporate more contemporary, digital solutions. Serious games are a popular phenomenon within the field of Game Studies and the sub-field of Games for Health (Bean, 2018) with a great deal of research aimed at benefiting and improving the lives of various populations, in particular stroke rehabilitation and fall prevention (Bleakley et al., 2015; Hall et al., 2012; Marston and Smith, 2012; Marston and McClenaghan, 2013; Miller et al., 2013). Respective reviews (Bleakley et al., 2015; Hall et al., 2012; Marston and Smith, 2012; Miller et al., 2013) have illustrated digital gaming can have a positive benefit on one’s health, be it cognition, physical activity (Duplàa et al., 2017; Pyae et al., 2016), or engagement (De Schutter and Brown, 2016; Gerling et al., 2015; Marston, 2013; Marston et al., 2016; Wiemeyer and Kliem, 2012). Gamification (Deterding et al., 2011) has become an area of game studies that facilitates users to be rewarded for reaching specific goals or completing a series of tasks (Marston and Hall, 2016). Regarding videogames and online environments (e.g. Second Life), there is a growing body of work surrounding the design approaches to videogames and PTSD (Macleod and Sloan, 2017; Holloway and Reger, 2013). Macleod & Sloan (2017) discuss and present a prototype to understand the potential benefits of using such an environment for PTSD self-help, and online virtual environments such as Second Life have been used as a means of facilitating interactive learning environments to educate ‘visitors’ about military/combat-related PTSD (Holloway and Reger, 2013). The T2 Virtual PTSD Experience (Holloway and Reger, 2013) offers various actors (e.g. veterans, family members, peers and military personnel) the opportunity to learn and understand the causes and symptoms surrounding PTSD, and the respective authors note how the positive responses from the various actors who are engaging with the virtual environment, has resulted in greater understanding of PTSD, and the greater need for the provision of resources via offering additional care, advice and help (Holloway and Reger, 2013).
A systematic review by Callejas-Cuervo et al. (2017) presents 15 articles focused on emotional recognition and videogames, concluding that active engagement within such environments can offer direct rehabilitation for PTSD via physiological signal measurement. Colder et al. (2018) explored how videogames are used by U.S. veterans positively in their respective recovery in behavioural and PTSD health. This qualitative study interviewed 20 participants who reported the positive benefits of engaging with videogames to alleviate and manage their change in mood, and stress levels. Furthermore, data analysis suggested videogames offered participants additional strategies to coping with PTSD, including adaptive coping, eudaimonic well-being and socialising, leading the authors to conclude that videogames offered some veterans a ‘form of personal medicine that can promote recovery’ (Colder et al., 2018: 2).
Antle et al. (2019) designed a mobile app comprising of six different relaxation games, accessible via a tablet to facilitate children aged between 5 and 8 years old to engage with the respective games while been connected to an EEG headset. Results showed improvements by the children who were able to self-regulate anxiety and cortisol levels in some children were reduced. Furthermore, children who received support from their teacher surrounding learning transfer and who were able to make multimodal connections responded positively to the intervention.
As online interventions and video games require accessible (often mobile) devices, it could be that there are aspects of the working environment of ESP that are barriers to their use. However, similar technology is being increasingly used in training of ESP, for example mental practice virtual reality games (Bauerle et al., 2016) for coal mine first responders, and a mental calculation App (using elements of game design and gamification) for paramedic students (Hall et al., 2018).
Given the increasing use of digital devices in the work of ESPs and their potential for supporting health and well-being interventions that has been demonstrated in other domains, the purpose of this review was to ascertain and identify literature surrounding the use of digital devices and games within the field of health and well-being, directly associated to ESPs. We believe this is the first such review covering this area.
Materials and methods
Search strategy (identification of relevant studies)
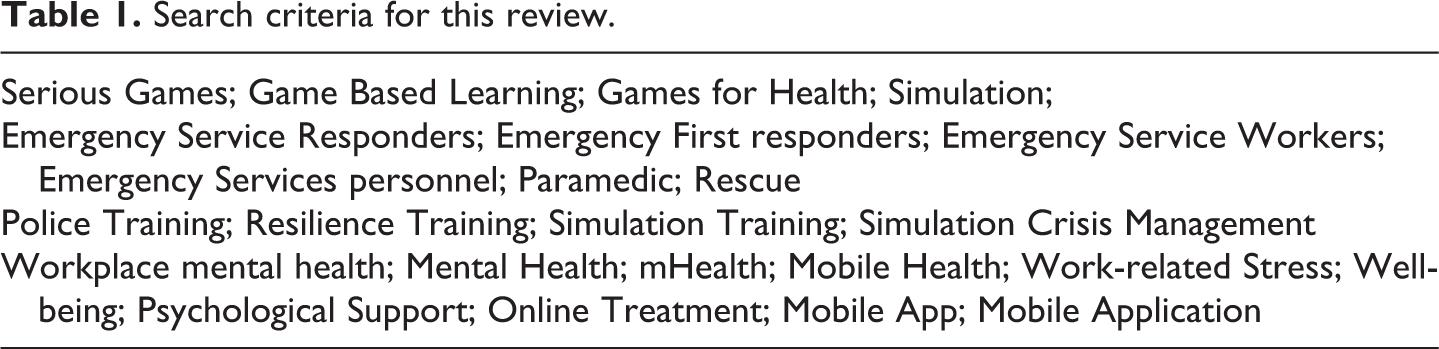
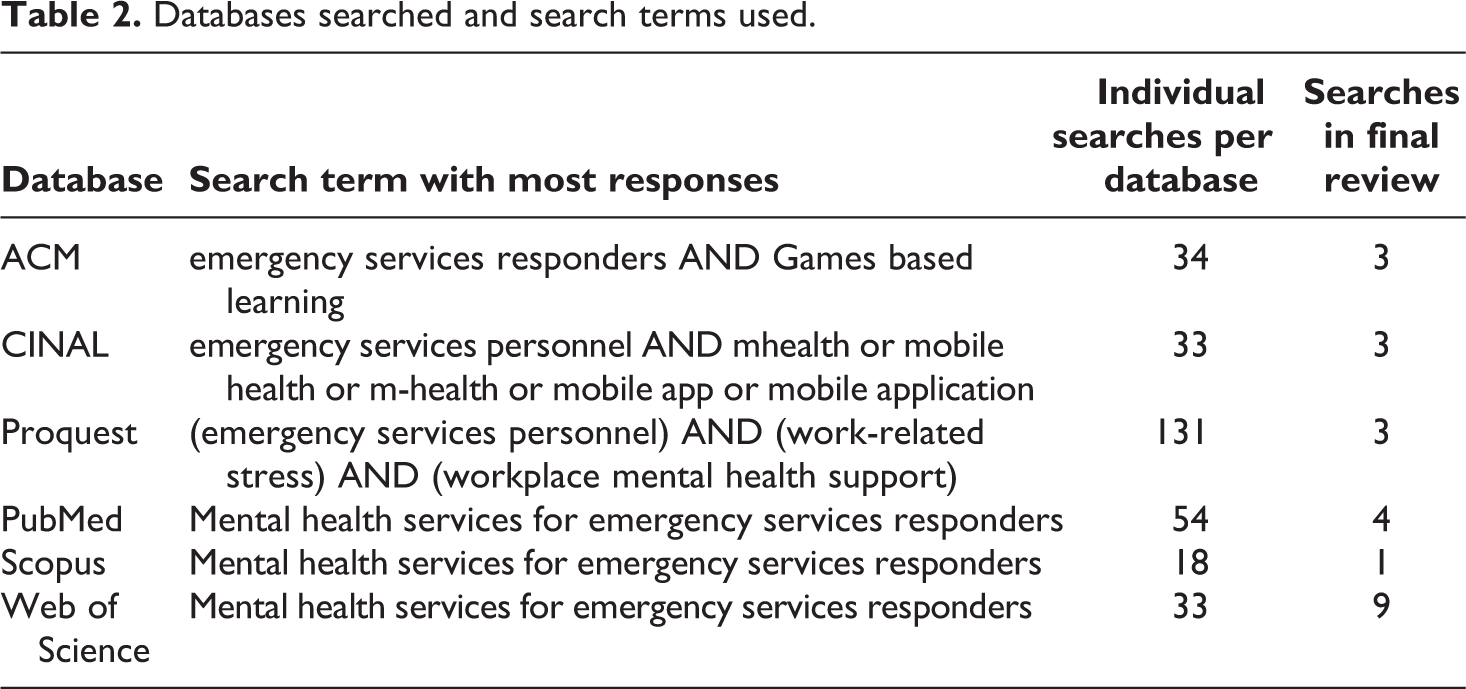
Electronic databases ACM, CINHAL, ProQuest, PubMed, Scopus, Web of Science (WOS) were searched for articles published since January 1, 2000. Limiters were ‘Adults’ (>18 years), ‘English’ and ‘humans. Individual search strategies were adapted for each database (Table 1). For example, in CINAHL provision is made to filter by age group whereas this not facility is not available in ACM. The broad range of the search criteria (Table 1) led to multiple individual searches per database. Consequently, with the exception of Scopus, the selection of papers per database was drawn from more than one search (Table 2). In a small number of searches, full text records were not available. In such circumstances the abstract or preview was assessed.
Search criteria for this review.
Databases searched and search terms used.
Study selection
The eligibility of each article was reviewed using the inclusion and exclusion criteria (Table 3). The inclusion criteria consisted of five elements. First, the study examined the material as identified in the search criteria (Table 1), since January 2000 and March 2019, published in the English language and conducted on humans. The ACM, CINHAL, ProQuest, PubMed, Scopus or World of Science databases were searched.
Inclusion and exclusion criteria.
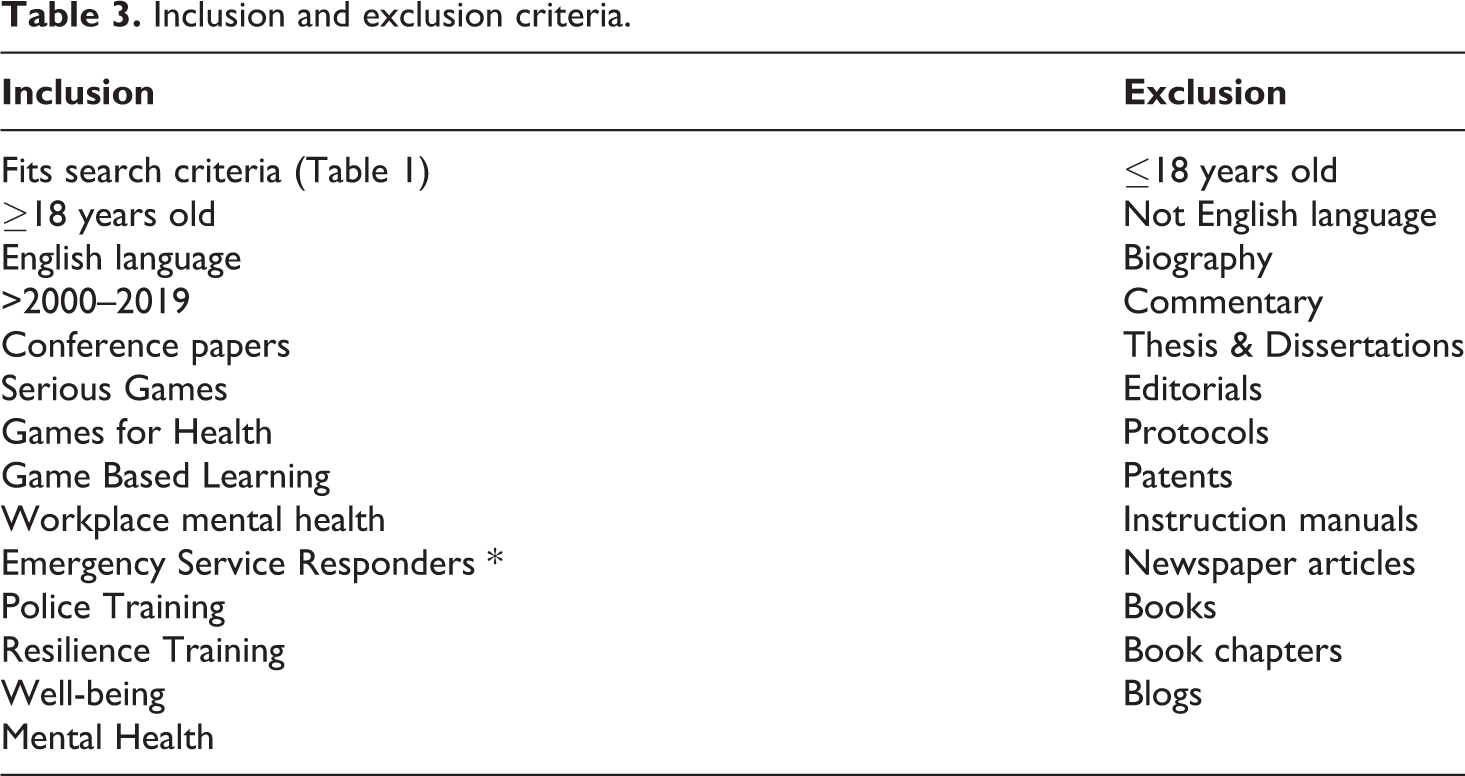
The exclusion criteria were framed by three factors. First, studies that did meet the inclusion material. Second, studies that did not report original results. For example, blogs and other commentaries, letters to the editor, research proposals, and study protocols. Third, citations or patents and finally, material reporting technical details. For example, details of hardware or device program architecture.
The initial database search identified 1131 records. Table 3 details the databases used, number of searches per-databases and terms used, number of searches included in the final review. The total number of duplicates amounted to 112. Once the duplicates had been removed, 1019 records were reviewed. After due process, two (2) records met the criteria for inclusion and form this scoping review. Figure 1 shows the review process. Two of the authors—HM and GP, independently assessed all records for inclusion and conducted the review of the records. Studies were only included if they met the full inclusion criteria (Table 3). Initially, the titles of papers and abstracts were screened for suitability and if necessary, the full paper was then reviewed. Both HM and GP reviewed all records from each database separately and then collectively compared their selections. Discrepancies were discussed and reviewed by HM and GP before a final decision was made. Full texts were retrieved to determine if they met the inclusion/exclusion criteria. HM and GP jointly decided the final selection of papers for inclusion.
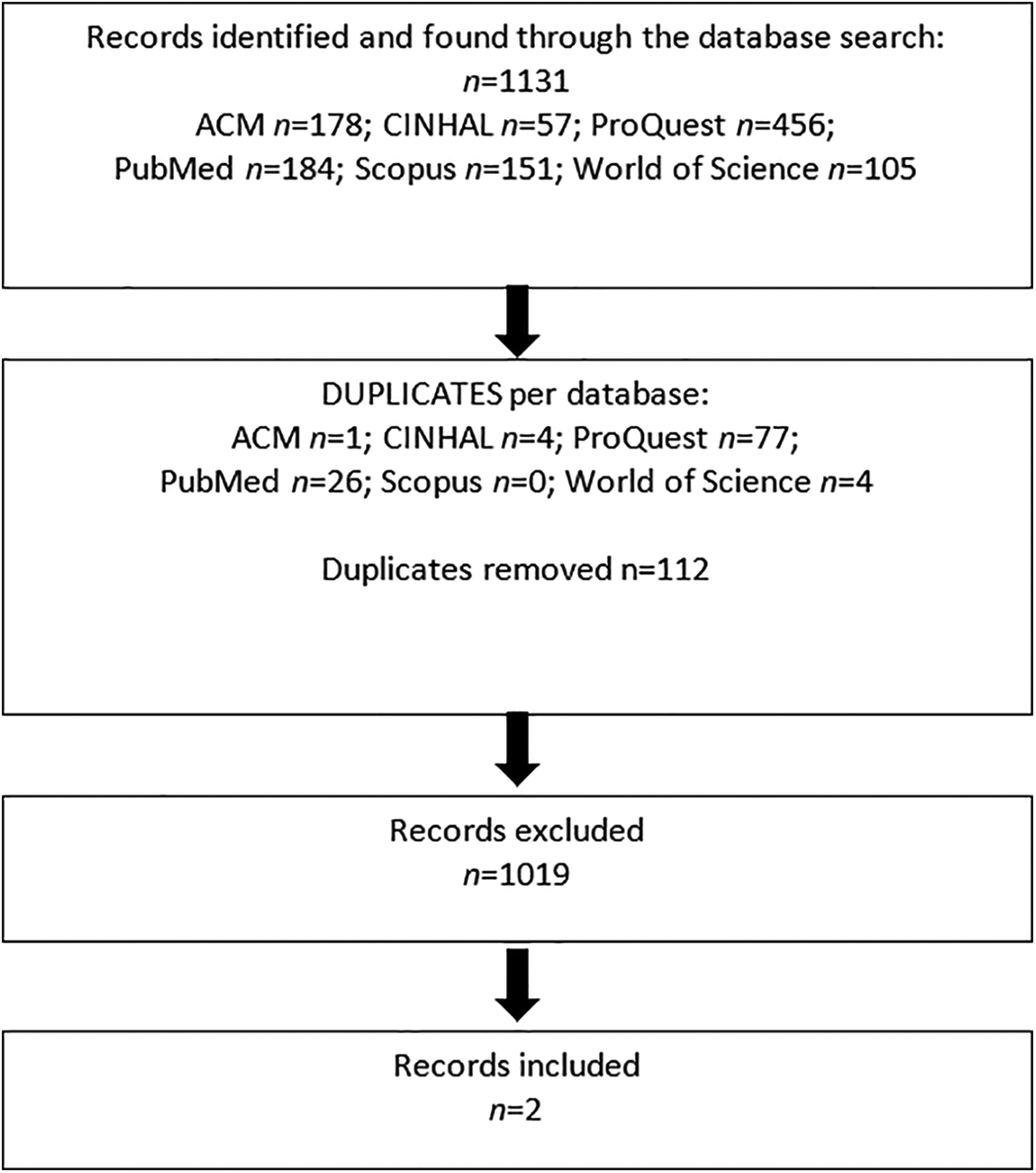
Search process and eligible studies.
The rejected papers by the two independent reviewers included areas that were deemed to be irrelevant, completely out of scope and did not align with the inclusion criteria (e.g. cyber security, personalised computing and trust, e-procurement, adaptive brain computer interfaces, and robotic communication). Additional paper rejections related to content that included emergency service personnel which did not include the specific technology outlined in the inclusion criteria (mobile apps/serious games), and websites providing health and well-being information to ESPs were not in the scope of this paper, as the focus here was on mHealth Apps and serious games.
Results
Table 4 provides a detailed overview of the two articles reviewed (n = 2). The first study was published in 2017 by Deady et al. (2017), who recruited participants (n = 106) from four fire service departments located in the metropolitan area of New South Wales, Australia. The second study, published by Seligman et al. (2015), recruited eight participants (specific details were not reported). The latter conducted a user-centric process during the design process of the SAMHSA Disaster App. The sample included representatives from the Federal Emergency Management Agency (FEMA), the Department of Defense, the American Red Cross, the Assistant Secretary for Preparedness and Response, the Uniformed Services University of the Health Sciences.
Summary of articles (n = 2) included for this scoping review.
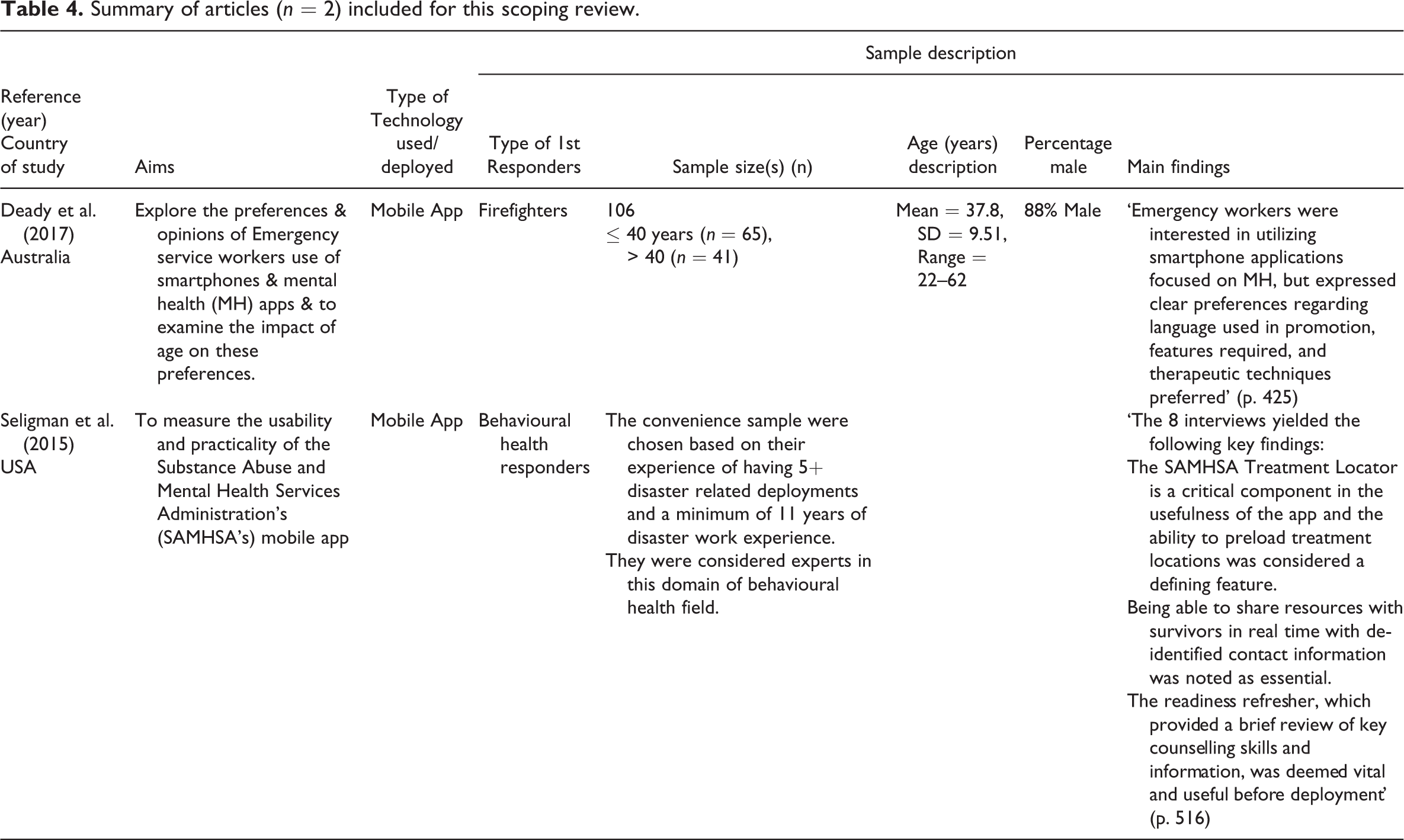
Over a 4-day period, Deady et al. (2017) collected data comprising of smartphone use, design preferences of mobile apps (mApps) content focusing on the likely use by users; in conjunction with a series of mental health words and associated descriptions. Respective participants recruited reported positively to using a tailored emergency mApp, with 74% of participants reporting they would use a specific mental well-being app on a daily basis, especially if they were feeling low. Similarly, 60%noted they would use an app for at least 5 minutes a day. However, 42% would prefer face-to-face support, and 17% noted a preference for an app format. Several terms were highlighted by respondents including well-being (54%), mental fitness (54%), followed by resilience (36%), and stress (30%). However, least popular terms included emotional well-being (21%), mental health (19%), and psychological health (16%).
Seligman et al. (2015) report the SAMHSA Disaster App contains several functionalities to assist first responders during an incident. Features including preplanning for deployment, identifying and facilitating locations as suitable sites for clinics and treatment centres.
Discussion
This review has primarily highlighted the paucity of specific mApps aimed at supporting the health and well-being of ESP. The results section (n = 2) show the different approaches which were undertaken by the respective research teams and some of the possibilities afforded by using this innovative technology.
The results of this review highlight how mHealth Apps can be used by ESPs in differing contexts and environments. However, neither paper primarily focused nor reported on how such an App could be used within an intervention. Furthermore, when using mApps it is important to ascertain whether functionality and usability is positive, but also such Apps could be used within an RCT intervention.
As noted in the introduction, there is a growing body of evidence in the UK investigating the health and well-being of ESPs including and by the national charity Mind, as well as related phenomena, such as ‘leaveism’ (Hesketh and Cooper, 2014) which illustrates this ongoing and growing concern for the health and well-being of ESPs. The work by Peñalba et al. (2008) note there is still a lack of evidence-based interventions within the domain of health and welfare of ESPs. While Arble and Arnetz (2017) suggest various approaches to dealing with the health and welfare of ESPs.
From the sole standpoint of policing, the National Police Well-being Service (NPWS) and the Blue Light Well-being Framework (Hesketh and Williams, 2017), aims to support police personnel and staff in the domain of health and well-being. Oscar Kilo (OK), the web portal for the NPWS, offers organisations an opportunity to audit and benchmark against a set of independent standards, which are specifically aimed at both the police and other emergency service responders. The framework was developed with various actors (e.g. practitioners at all levels, professionals and academics). The OK framework comprises of five segments, (1) strategic and tactical planning templates, (2) psychological risk management guidance (Hesketh et al., 2017), (3) responding to trauma guidance (Hesketh and Tehrani, 2018), (4) the GAIN pyramid (Hesketh et al., 2017), and (5) a series of real stories presented in animations.
Additionally, Hesketh and Tehrani (2019) discuss the existing psychological approaches to trauma risk and management across UK policing. They highlight the ongoing need for intensive efforts by various police personnel (e.g. senior managers, and supervisors) and support staff (e.g. occupational health) to ascertain respective risks. Further recommendations are also noted relating to reducing harm, provision of protective training and education, and where appropriate the provision of post-trauma interventions and treatment need to be offered. Hesketh and Tehrani (2019), highlight three categories of policing personnel; (1) responders, (2) specialists, and (3) personnel involved in major disasters, and their recommendations support the appropriation and provision of post-trauma intervention and treatments; while continuing to differentiate and administer appropriate solutions for police personnel and staff alike.
As documented in the introduction, there is a growing body of work surrounding the use and deployment of videogames by military veterans to combat behavioural change and PTSD. However, there is still a paucity in the literature surrounding the use and deployment of videogames by first responders/emergency services as noted by Holloway and Reger (2013), who have constructed a purpose-built environment in Second Life to educate various actors in the various issues and factors surrounding PTSD. The field of Games for Health has embraced the design, use, and development of videogames/environments for multiple health conditions, (Colder et al., 2018; Macleod and Sloan, 2017; Callejas-Cuervo et al., 2017; Holloway and Reger (2013). Yet, there is very little research indeed that has explored the use of mHelath Apps, videogames, and virtual environments to support and combat PTSD and related issues by police personnel and emergency responders.
We would like to propose several recommendations for moving this work forward: Future work should examine how mApps can be integrated and used by different ESPs organisations. Future work should consider a framework for the design, development and deployment of a mHealth Apps targeting ESPs, associated to their health and welfare. A consortium comprising of ESPs, researchers, stakeholders, users, designers and developers would facilitate key information to be developed, revised, shared and evidenced. This framework could be both national/country specific and/or accessible on an international landscape. Future work should consider an intervention comprising of multi-methods which uses different technologies (i.e. mHealth Apps, digital games) both on a national and international scale. This would offer greater insight into the suitable approaches for supporting, managing and potentially treating health and welfare. a. Taking an international study design would offer insight into different ESP organisational practices, and may offer different approaches, feedback (via workshops and 1-to-1 interviews) into the needs and requirements of mHealth Apps and video game engagement, functionality and features. As the evidence grows in this domains, further scoping/systematic reviews will have to be conducted to ensure all evidence from this multi-disciplinary arena is captured and documented. Therefore, utilizing a protocol such as the recent PRISMA extension for scoping review (PRISMA-ScR) (Tricco et al., 2018), or the PRISMA framework(s) (Moher et al., 2009) would minimise bias. a. We propose a suitable virtual environment/videogame should be co-designed, co-created, tested and evaluated by a myriad of actors (e.g. designers, police/emergency responders, family members, health and well-being practitioners and academics) to ascertain the benefits of engaging with such an environment as a means of rehabilitation, education and as a support mechanism. Furthermore, if such a development was to be conducted, there is the potential for various environments to accommodate the diverse needs, requirements and similarities from the various emergency services (e.g. police, fire service, paramedics, forensic investigators). Evaluating such a prototype could take the form of including a minimum of two police forces (located across the UK) who have diverse geography (e.g. city vs rural) needs and issues, who would then provide feedback and insights prior to rolling out across various police forces with a view to implementation within police related resources.
Conclusions
The work presented in this paper is distinctive because it intersects across the fields of game studies, psychology, mental health, organisational behaviour, and public services. Furthermore, this work contributes to the fields of psychology, health and well-being, public services, in addition to having a real-life impact not only on police officers and staff, but also other emergency services personnel. To the knowledge of the authors, this is the first piece of work to examine mApps used by first-line responders and PTSD. Given the paucity of literature surrounding both police and emergency service personnel, the work presented here highlights an area that is ripe for development.
Finally, this work is a call for action from the fields of academe, policy makers, respective training colleges, police and emergency service personnel (at all levels) to ensure appropriate measures, interventions and provision of suitable support and resources are available to access.
Footnotes
Author Disclosure Statement
No competing financial interests exist. Funding was received from the <Institution – Redacted for Reviewing Purposes>.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support for the research and authorship from the Centre for Policing, Research & Learning, The Open University, UK; £5103.06.