
Abstract
In the UK, demand for the police has changed, with the majority of calls now vulnerability-related. Police safeguarding notifications (N=3,466) over a one-year period for a local authority in Wales were matched to social care records. Over half (57.5%) of notifications were referred to social services and only 4.8% received social service input (e.g. social worker intervention). Over a third of individuals had repeat notifications in the study year. Findings evidence high levels of police-identified vulnerability and an imbalance in vulnerability-related risk thresholds across agencies. Furthermore, some individuals require more appropriate action to mitigate the risk of future safeguarding notifications.
Introduction
Following international trends, crime rates in the United Kingdom (UK) have been in decline since the 1990s (Tseloni et al., 2010). Incidents classified as non-crime, including vulnerability, public protection and safeguarding, now account for the majority (84%) of calls to the police in the UK (College of Policing, 2015a). This marks, in some respects, a change in the focus of policing from a traditional, crime-orientated reactive approach towards a community focus on prevention, in particular a focus on vulnerability (Bartkowiak-Théron and Asquith, 2012a, 2017; Murray, 2002; O’Neill, 2010). The police are duty-bound to both prevent crime and protect individuals and communities (HMIC, 2015a). With vulnerability thought to be intrinsic in all police encounters (Bartkowiak-Théron and Asquith, 2014, 2017; Paterson and Best, 2016), vulnerable individuals are particularly in need of protection and support from the police and appropriate partnership agencies (for example, health and statutory organisations such as social services). Definitions of vulnerability vary internationally in context and content (Bartkowiak-Théron and Asquith, 2012a, 2012b). In the UK, vulnerability is typically defined by police services using the Ministry of Justice Code of Practice for Victims of Crime definition, which outlines a victim as vulnerable if they are under the age of 18 years or have a mental or physical disability, disorder or significant impairment (Ministry of Justice, 2015). Given the increasing demand placed on police resources by vulnerability issues (Boulton et al., 2017), it is important that the police response is adequate and that a multi-agency response results in those in need receiving the support they require. Globally, police are under scrutiny from the public and other governing bodies in their engagements with, and response to, vulnerable individuals (Bartkowiak-Théron and Asquith, 2012a). UK police services are routinely and independently monitored on their protection of vulnerable people and victims of crime by Her Majesty’s Inspectorate of Constabulary (HMIC). A 2015 inspection highlighted that through an inconsistent response, the majority of services in England and Wales were not meeting the needs of the vulnerable, and that police staff needed training to deepen their understanding of vulnerability (HMIC, 2015a). In response, UK police services are following international models (ACERT, 2017; Equal Justice USA, 2018) and developing trauma-informed training for frontline staff (Ford et al., 2017a; Ford et al., 2017b; North Wales Police, 2017; West Midlands Police, 2017).
Identifying safeguarding needs and onward action
As part of their duty to protect vulnerable individuals, UK police have a statutory responsibility to protect all individuals in need, at risk of abuse, or who have been abused, by making appropriate safeguarding referrals to the local authority (Association of Chief Police Officers, 2012; HMIC, 2015b; Unicef, 2017). Police therefore act as the ‘front end’ actors, whose actions can inform later stages of intervention from services (Asquith et al., 2016; Bartkowiak-Théron and Asquith, 2012b; Herrington and Clifford, 2012; Paterson and Best, 2016). In the UK, police manage safeguarding through public protection units (PPUs) – specialist police departments that review safeguarding notifications submitted by police officers and staff. Where appropriate, PPUs refer safeguarding notifications to other agencies, predominantly child and adult social services. When police feel that a safeguarding referral to these services is necessary, the safeguarding notification must be submitted to the PPU within 24 hours of its occurrence. The referring police officer assigns a vulnerability category/ies to the notification from a pre-defined list of five options: mental health: a mental disorder or disability of the mind (Mental Health Act 1983); domestic violence and abuse (DVA): threatening behaviour, violence or abuse between adults, who are or have been intimate partners or family members (Association of Chief Police Officers, 2008); honour-based violence: violence, or threat of violence, intimidation, coercion or abuse, committed to defend the honour of an individual, family and/or community for perceived breaches of a code of behaviour (College of Policing, 2017a); vulnerable adult: any person aged 18 years or over ‘who is or may be in need of community care services by reason of mental or other disability, age or illness; and who is or may be unable to take care of him or herself, or unable to protect him or herself against significant harm or exploitation’ (Department of Health, 2000: 8); or, child concern and/or child sexual exploitation (CSE): child concern, alarm for an individual who may have been harmed physically or emotionally (College of Policing, 2015b); CSE, the deception, coercion or manipulation of a person under the age of 18 into sexual activity in exchange for financial advantage or status (College of Policing, 2017b).
When safeguarding notifications are shared by the police, the receiving agency risk assesses them to determine service involvement. In the case of social services in the UK, an assessment is made to determine if the named individual(s), or subject(s) of the notification is eligible for intervention, and whether a care and support plan is required (Care Act, 2014). Care and support plans specify the subject’s needs, as identified by a needs assessment, and detail how these are to be met or reduced (Care Act, 2014). Intervention thresholds are set at a local level by local safeguarding children and adult boards (Care Act, 2014; HM Government, 2015). These are often influenced by demand for services and available resources (NSPCC, 2014).
Understanding safeguarding across policing and social services
Research has highlighted the growing volume of safeguarding notifications to social services in the UK (Beadle-Brown et al., 2010; Mansell et al., 2009; National Health Service Information Centre, 2012). In 2010–2011, 5% of vulnerable adult notifications to social services departments in England were submitted by police services (National Health Service Information Centre, 2012). Up to one third of safeguarding referrals in England result in no further action and almost two thirds are for individuals or subjects already known to social services (Stanley et al., 2011). Tensions and conflicting priorities between the police and other agencies in the response to vulnerability have been reported (Leese and Russell, 2017; Paterson and Best, 2016). Commonly reported barriers to effective working between the police and social services include poor communication regarding the outcome of referrals and related court cases (Ford et al., 2017a; Stanley et al., 2011), a lack of understanding about each other’s role (Ford et al., 2017a; Stevens 2013), time constraints (Perkins et al., 2007) and differing priorities (Ford et al., 2017a; Pinkey et al., 2008). Guidance has been produced to help frontline police in the UK identify subjects in need, and to safeguard and put in place appropriate support for them (Waddle and Molloy, 2015). HMIC has highlighted the need for effective partnership working across police and other professionals to risk assess the subject’s situation, address their needs and support individuals (HMIC, 2015a). The majority of studies to date that examine safeguarding referrals are based in England, and primarily examine outcomes for referrals made to children’s services (Stanley et al., 2011). Less is understood about the challenges in identifying and responding to vulnerability elsewhere in the UK, and specifically understanding the level of police-identified vulnerability in adults that results in no further action. As levels of vulnerability-related demand continue to rise, and police are required to do more (Bartkowiak-Théron and Asquith, 2012b), it is important to understand the operating police threshold for action, compared to the response by social services to help identify areas for action. This study adds to knowledge in this field by examining the demand, repeat activity and outcomes (action) taken regarding police safeguarding notifications to both child and adult social services in one local authority area in Wales.
Aims of the research
This study aimed to explore the vulnerability-related demand upon, and response from, a police service in Wales, covering approximately 42% of the Welsh population (College of Policing, 2017c). The study also aimed to gain an understanding of the outcome of police safeguarding notifications for vulnerable individuals referred to two statutory agencies, child and adult social services. This article contributes to national and international understanding of the importance of the police response to vulnerability and adversity, through identifying levels of vulnerability in the police safeguarding system and outcomes for vulnerable individuals.
Methods
Data for all safeguarding notifications created by the police service for occurrences (i.e. police incidents) between 1 January 2016 and 31 December 2016 inclusive were extracted by South Wales Police (SWP) Business Intelligence from the police data management system. In collaboration with SWP, a local authority was identified for the sample with a population of approximately 150,000, 18% of residents aged 0–15 years (Welsh Government, 2017) and moderate levels of child poverty (29.8% after housing cost; End Child Poverty, 2016). Social care data for all police safeguarding notifications to the social services within this local authority area, were extracted for the same period, plus an additional month (until 31 January 2017) to allow for a lag in response in the social services dataset. The data were transferred from the police and social services to the research team via secure data transfer and once received, were stored on a secure server with restricted access.
The police safeguarding notification dataset was matched to the social services dataset using: first name and surname; date of birth; police safeguarding notification occurrence date; and the date the notification was referred to social services. To allow for a delay in reporting incidences to the police, records were matched where the date of referral to social services was between five days before and 20 days after the occurrence date listed on the notification. Where multiple records matched on personal information and dates, the police safeguarding notification was matched to the social care record closest in date. Records were matched to safeguarding notifications where either (a) the individual was the main subject of the notification, or (b) the individual was named as an involved subject on another person’s safeguarding notification. As a measure of deprivation, the household postcode of residence for the individual or subject listed in the notification was matched with deprivation quintiles in the 2014 Welsh Index of Multiple Deprivation (WIMD; ONS, 2015). Calculated at the lower super output area (LSOA; geographic areas with a population mean of 1,600) level, the WIMD is a standardised measure used to compare deprivation between areas. The WIMD is a composite measure using a range of domains including: health, education, employment, income, access to services, physical environment and community safety (Welsh Government, 2014). Once data were matched, all personal identifying information was removed and original data files were destroyed. The age of the individual or subject listed in the notification was categorised into four groups for analysis (0–9; 10–17; 18–49 years and aged 50+). During the period for which the data corresponds, the police service operated a four tier system for grading occurrences: grade one, emergency response within 15 minutes; grade two, priority response within the hour; grade three, schedule response incidents within 24 hours; and grade four, resolution without deployment – no attendance required.
Data analysis was undertaken in SPSS v24. Analyses used chi squared for bivariate examination of associations between demographics and multiple notifications, and notification outcomes and subsequent multivariate modelling employed binary logistic regression to identify independent relationships.
Ethical approval for the study was obtained from the National Health Service Research Ethics committee, Public Health Wales Research and Governance Office, and the Confidentiality Advisory Group (CAG; reference 16CAG0123).
Results
Sample description
For the 12-month period (1 January 2016 to 31 December 2016 inclusive), 3,466 safeguarding notifications were created by police for residents in the selected local authority (resident at time of notification submission). Safeguarding notifications recorded individuals as the main subject (62.3%, n=2,161) of the notification or as a person involved in the occurrence for whom the police held a safeguarding concern (thus, an individual named on someone’s notification whom the police also held a safeguarding concern for; 37.7%, n=1,305). The notifications related to 1,600 unique individuals, 38.3% had more than one notification submitted in the period and 13.6% had four or more notifications submitted (range 1–76, average 2; Table 1). A total of 8.5% of individuals accounted for 36% of notifications submitted over the period.
Full sample characteristics (N = 3,466 notifications).
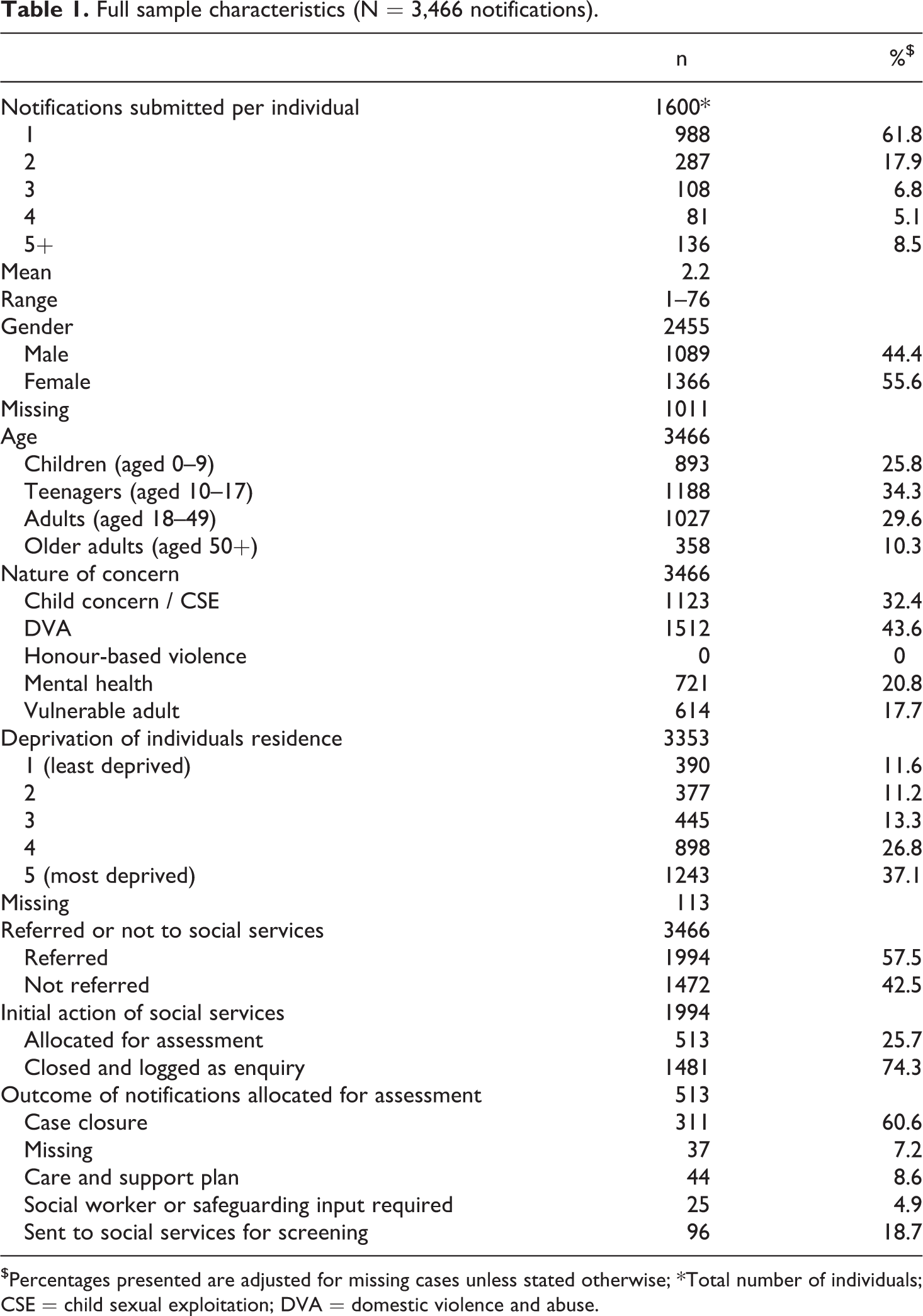
$Percentages presented are adjusted for missing cases unless stated otherwise; *Total number of individuals; CSE = child sexual exploitation; DVA = domestic violence and abuse.
Gender is recorded only for the main subject of the safeguarding notification and is not recorded for other individuals named on a notification. Where gender was documented, over one half (55.6%; n=1,366) of notifications were for females (gender was not available for 29.2% of notifications; Table 1). Individuals aged under 18 years represented 60.1% of the sample and more than one third (37.1%) related to subjects who were resident in the most deprived quintile.
Safeguarding notifications were predominately submitted by police constables (91.3%) and were in relation to high-grade response occurrences (90.1%; grade one and two). The vast majority (86.2%, n=2,987) of notifications recorded one nature of concern (NOC; see introduction for the five types of NOC which can be applied), while 13.1% recorded two concerns. The most common NOC recorded was DVA (43.6% of notifications), followed by child concern/CSE (32.4% of notifications). There were no notifications for honour-based violence. Aggravating factors (i.e. drugs, alcohol and/or mental health in relation to the incident) were poorly recorded but were documented in 18.2% of notifications, and of these 51.5% reported drugs and/or alcohol misuse.
In 32.2% (n=1,115) of the sample, information on the date and/or time of the PPU risk assessment were missing. Where data were available for analysis, 41.2% of safeguarding notifications were risk assessed within 24 hours of the occurrence being reported.
Safeguarding notification to child and adult social services
Of the 3,466 safeguarding notifications submitted by police officers and staff, 57.5%, (n=1,994) were referred to child (69.9%) or adult (30.1%) social services. For children, 546 (39%) matched to notifications where the child was the subject and 848 (61%) to notifications where the child was a named individual on another individual’s notification. For adults, this was 586 (98%) and 14 (2%) respectively.
Of the 1,600 individuals in the sample, 69.4% had all of their safeguarding notifications referred. All individuals who had only one safeguarding notification recorded during the study period were referred to social services compared to 40.6% of those with multiple notifications during the time period (p<0.001). First safeguarding notifications during the time period were more likely to be referred than subsequent notifications (first, 80.4% referred; subsequent, 37.9% referred; p<0.001; Table 2). Notifications were most likely to be referred to social services when the subject was a child aged under 10 (79.8% referred) and least likely when the subject was an adult aged 18–49 (36.2% referred; p<0.001). Notifications were also more likely to be referred when multiple concerns were recorded (63.3% referred compared with 56.6% with one concern; p<0.05). The association with deprivation was not clear, but notifications for subjects who lived in the least deprived quintile were more likely to be referred (65.1%) than the most deprived (55.1%; p<0.001). There were no significant associations found in relation to the gender of the subject. Notifications for children that recorded child concern/CSE as a nature of concern were less likely to be referred (61.5%) than those with no CSE recorded (73.2%; p<0.001) and notifications for adults were less likely to be referred when vulnerable adult was recorded as a NOC (Table 2).
Characteristics of notification by outcomes.
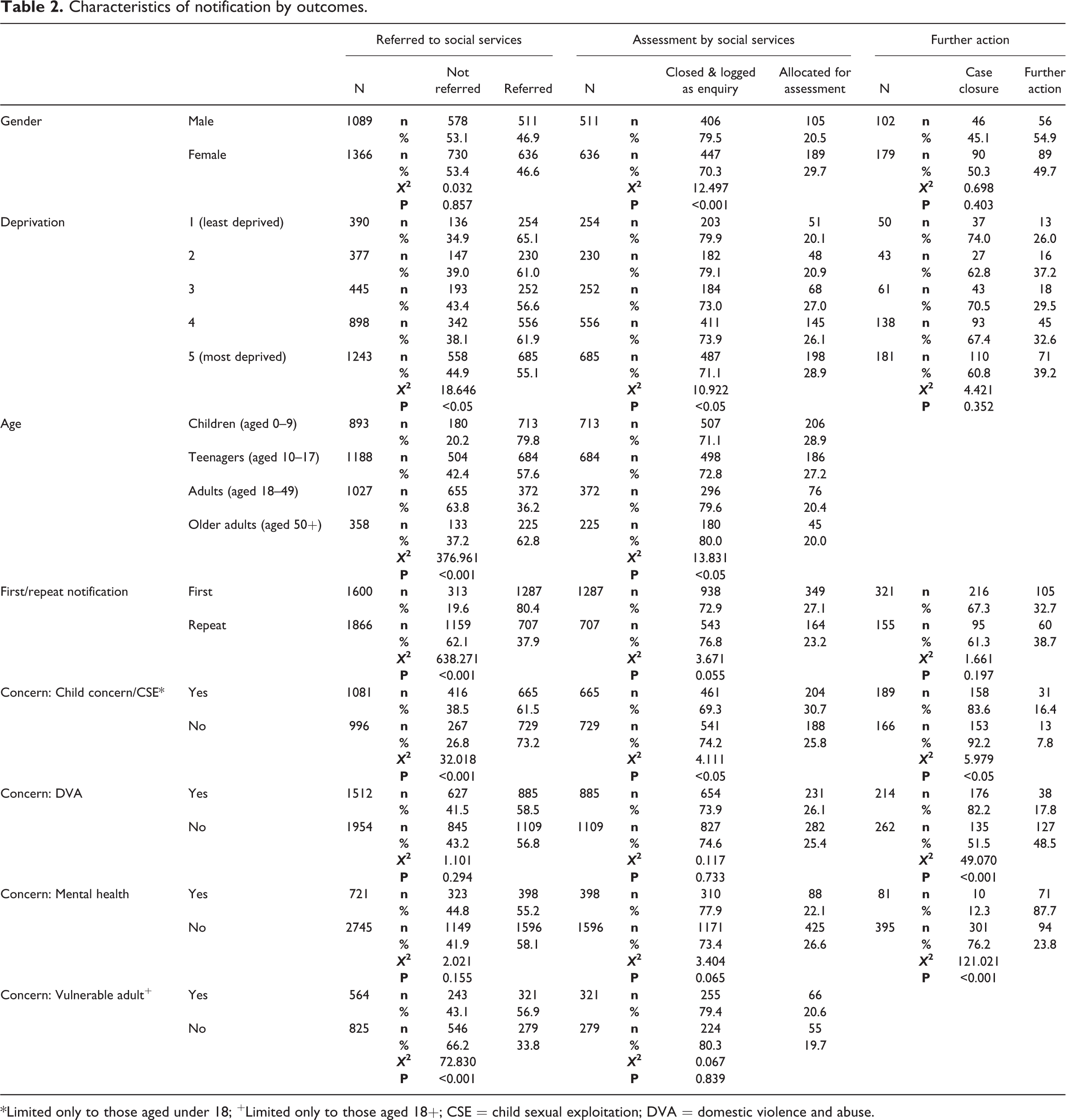
*Limited only to those aged under 18; +Limited only to those aged 18+; CSE = child sexual exploitation; DVA = domestic violence and abuse.
In logistic regression, children aged less than 10 years were seven times more likely to be referred than adults aged 18–49 (OR 7.0, 95% CIs 5.67–8.58; p<0.001). Individuals resident in the least deprived quintiles were 1.5 times more likely to be referred than those resident in the most deprived quintile (Table 3). Notifications with multiple NOCs were more likely (OR 1.3, 95% CIs 1.08-1.61; p=0.006) to be referred than those with only one NOC and the first notification in the time period was over six times more likely to be referred than subsequent notifications. After adjusting for demographics (age, deprivation and gender), the independent associations for age and deprivation remained (Table 3), with children under ten years of age three times more likely to be referred than adults aged 18–49 years. After adjusting for repeat NOC and notification frequency (first/repeat notifications in the time period), the odds of having a first notification referred remained 4.8 times higher, and age remained a strong predictor (Table 3).
Unadjusted and adjusted odds of a safeguarding notification being referred to social services by demographic factors.
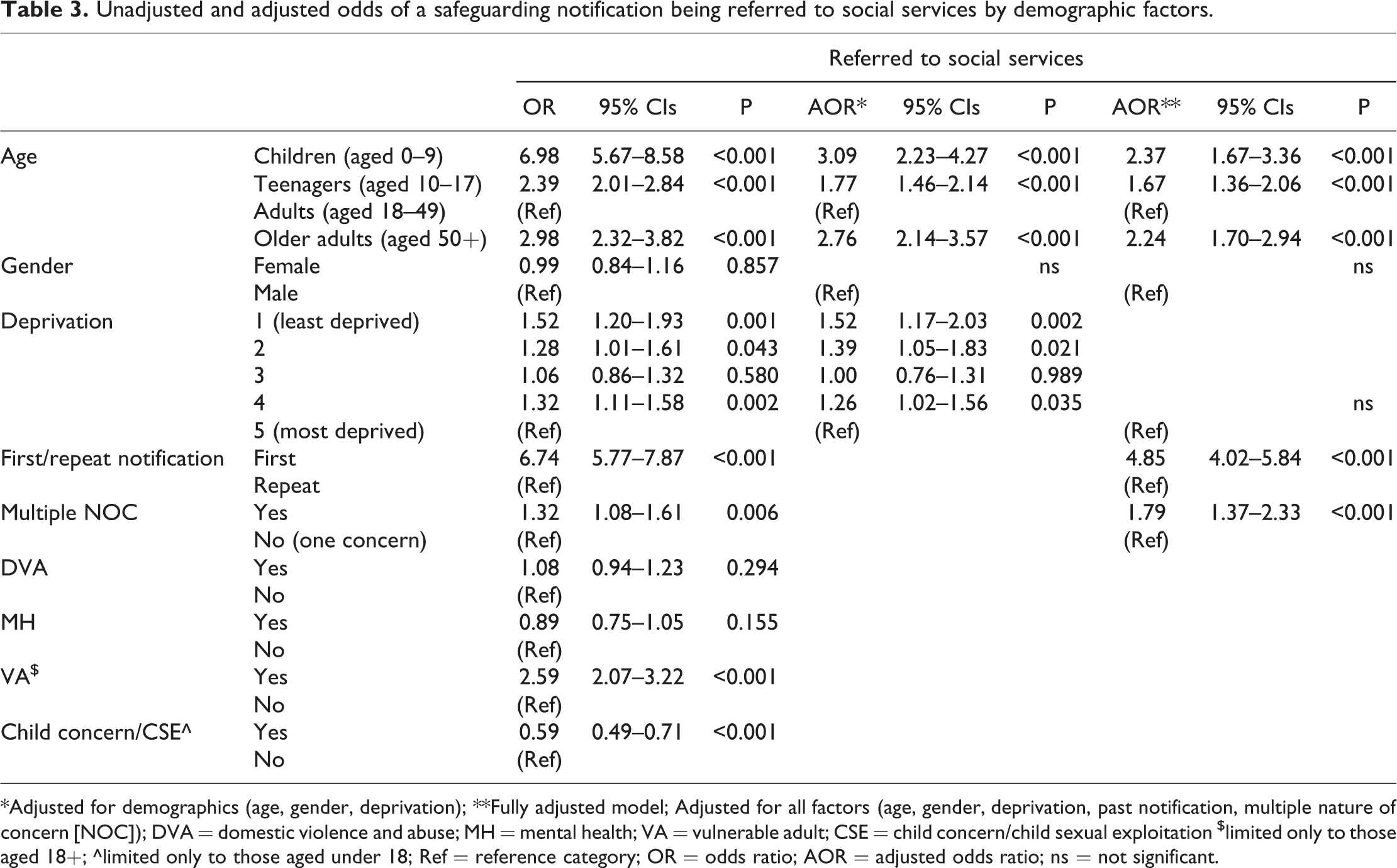
*Adjusted for demographics (age, gender, deprivation); **Fully adjusted model; Adjusted for all factors (age, gender, deprivation, past notification, multiple nature of concern [NOC]); DVA = domestic violence and abuse; MH = mental health; VA = vulnerable adult; CSE = child concern/child sexual exploitation $limited only to those aged 18+; ^limited only to those aged under 18; Ref = reference category; OR = odds ratio; AOR = adjusted odds ratio; ns = not significant.
Notification outcomes
Figure 1 outlines the outcomes for notifications received by social services. A quarter (25.7%) were allocated for assessment by the social services assessment team, the remainder (74.3%, n=1,481) were closed and logged as an enquiry, i.e. no further action was taken. Of those closed, 5.5% were already known to social services or safeguarding.
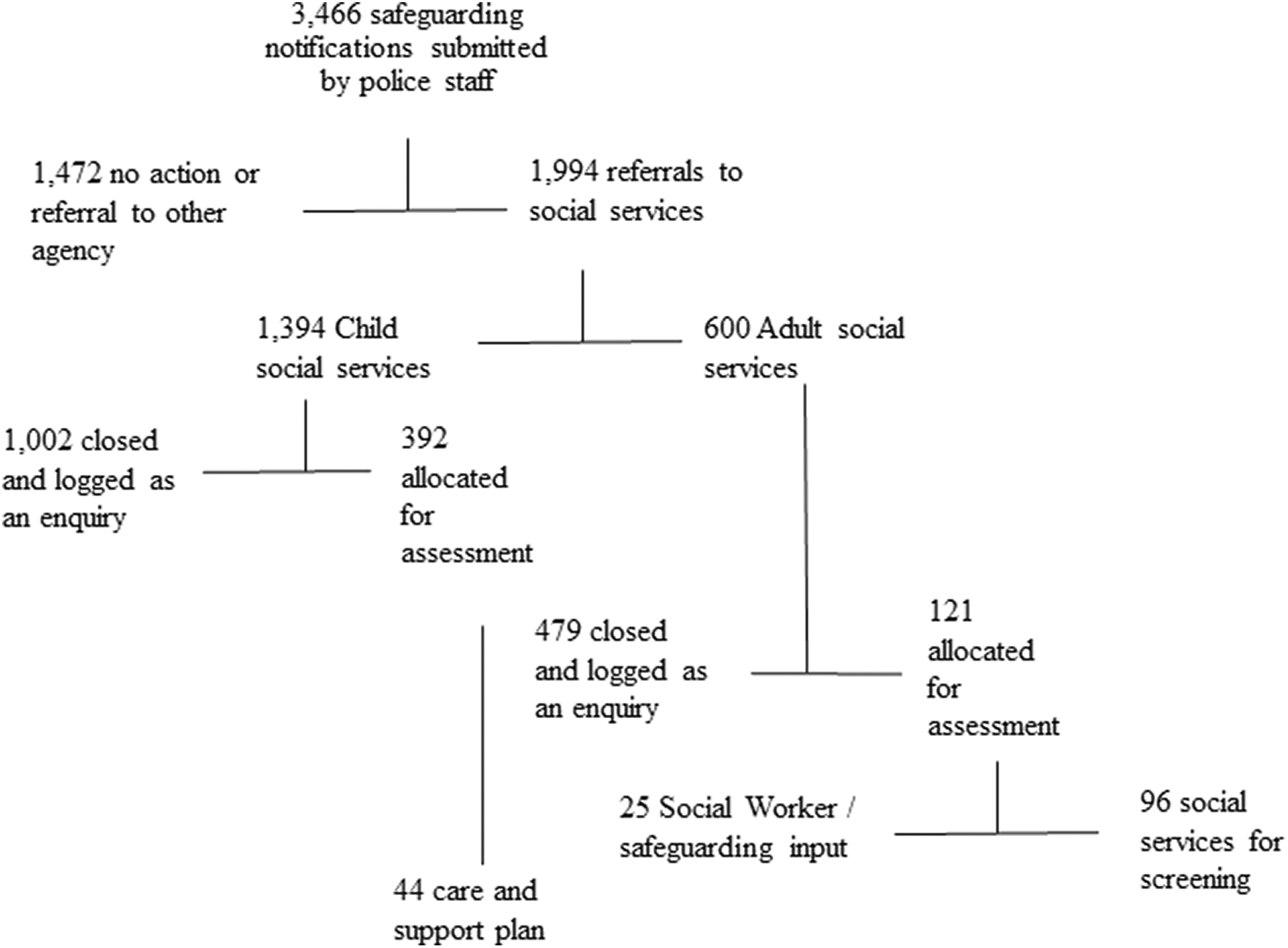
Notification outcomes.
In bivariate analysis, safeguarding notifications were significantly more likely to be allocated for assessment where the individual was a child (aged 0–9; 28.9% compared to 20.4% adults aged 18–49; p<0.05; Table 2); female (29.7% versus male, 20.5%; p<0.001) or from the most deprived quintile (28.9% most deprived, 20.1% least deprived; p<0.05). The notification was also more likely to be allocated for assessment where multiple concerns were recorded (30.4% compared with one concern, 24.9%; p<0.05) and where child concern/CSE was identified (30.7% with child concern/CSE compared with 25.8% no child concern/CSE; p<0.05). There were no significant associations with outcome and other NOCs.
In logistic regression analysis (Table 4), females, those from younger age categories (aged 0–9 years, or 10–17 years), or notifications for individuals resident in more deprived areas were more likely to have their notification allocated for assessment. The frequency of notification (first or subsequent) was less important for assessment than it had been for notification, as was having multiple NOCs (Table 4). When demographic factors were adjusted for, only age remained significant, with individuals in the youngest age groups three times more likely to be allocated for assessment (AOR 3.1, 95% CIs 2.00–4.91; p<0.001). After accounting for other factors (repeat NOC and notification frequency; see Table 4), the only significant difference remained for age, with individuals under 10 years old nearly three times more likely be allocated for assessment than adults, irrespective of sex or deprivation (AOR 2.7, 95% CIs 1.72–4.33; p<0.001).
Unadjusted and adjusted odds of a safeguarding notification being allocated for assessment to social services by demographic factors.
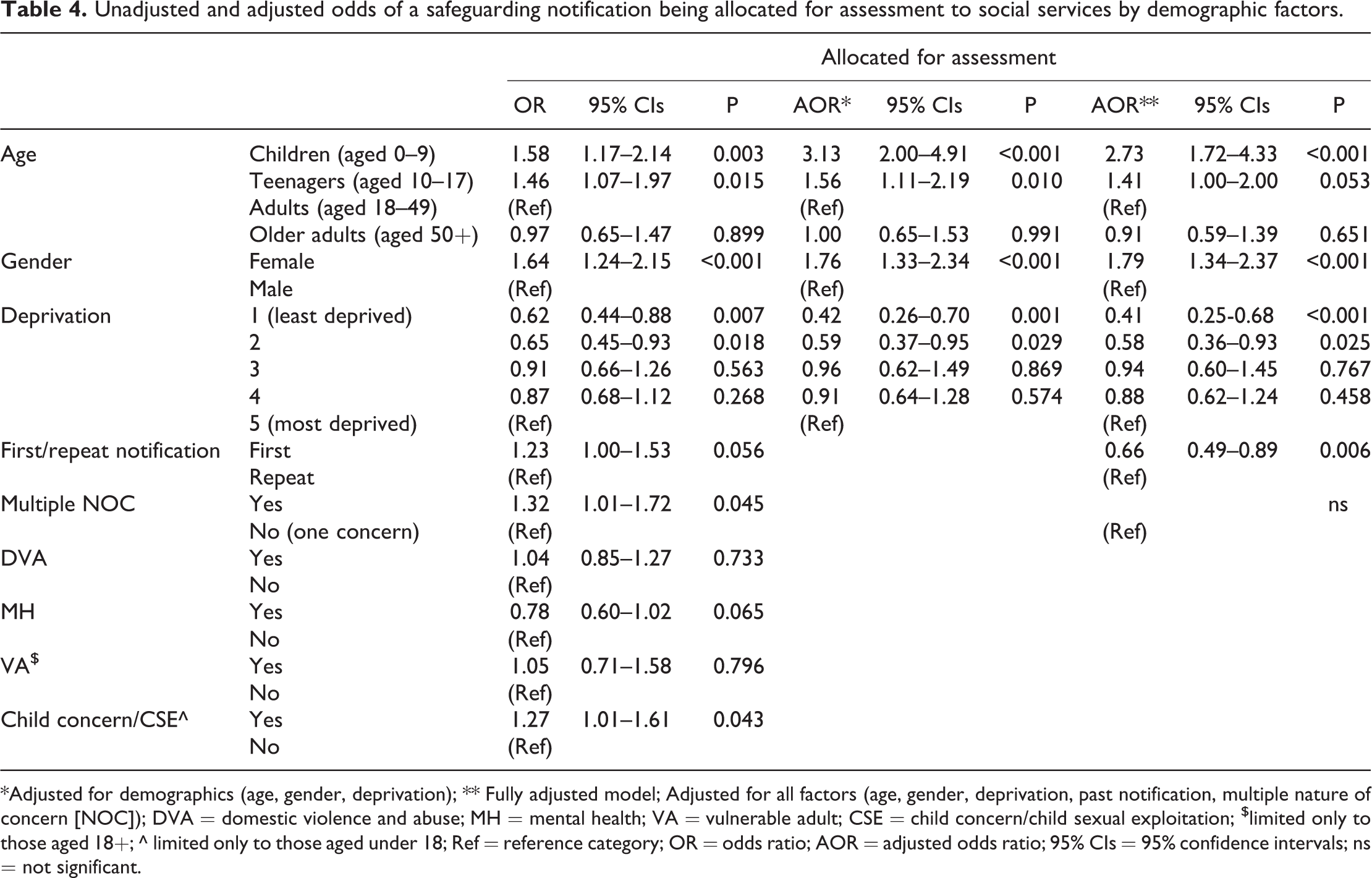
*Adjusted for demographics (age, gender, deprivation); ** Fully adjusted model; Adjusted for all factors (age, gender, deprivation, past notification, multiple nature of concern [NOC]); DVA = domestic violence and abuse; MH = mental health; VA = vulnerable adult; CSE = child concern/child sexual exploitation; $limited only to those aged 18+; ^ limited only to those aged under 18; Ref = reference category; OR = odds ratio; AOR = adjusted odds ratio; 95% CIs = 95% confidence intervals; ns = not significant.
Of the 513 safeguarding notifications allocated for assessment, 65.3% were closed following assessment by the social services assessment team (see Figure 1). Further action was taken for 165 safeguarding notifications, including: implementation of a care and support plan (9.2%); input from a social worker or safeguarding team (5.3%) and shared with social services for additional screening (20.2%). Therefore, only 4.8% of total safeguarding notifications submitted by police resulted in an action from social services. In bivariate analysis, safeguarding notifications were more likely to have further action following assessment when there were multiple concerns recorded (50.6%; one concern, 31.2%; p<0.001), where child concern/CSE was recorded as a concern (limited to children only; 16.4%, no child concern/CSE, 7.8%; p<0.05); or mental health was recorded as a concern (87.7%; no mental health concern, 23.8%; p<0.001). Notifications were less likely to have further action when DVA was recorded (17.8%; not DVA NOC, 48.5%; p<0.001). However, this may be because they were referred to an alternative appropriate agency (for example, domestic violence support services).
Discussion
This study presents unique data on the levels of vulnerability-related demand encountered by the police. In a Welsh local authority with a population of approximately 150,000, nearly 3,500 safeguarding notifications were submitted by the police during a one year period, of which over one half (57.5%) were referred to a statutory agency (child or adult social services). Despite the identification of vulnerability as the mechanism for activating responses such as social services intervention for individuals (Bartkowiak-Théron and Asquith, 2014), our findings indicate that only a small proportion (4.8%; 8.7% of adult safeguarding notifications and 2.1% of those submitted for children) of safeguarding notifications created by the police result in a direct action or input from social services (for example, further screening by the social services team, case and support plan or social worker input). Thus, over three quarters of safeguarding notifications created by the police were not referred to social services, or were immediately closed by social services, resulting in no action for the vulnerable individuals involved. Although these figures are low, they are not dissimilar to attrition rates in safeguarding notifications documented elsewhere (Parton, 2006). The findings of this study reveal a large volume of police safeguarding notifications that do not meet the intervention thresholds of statutory agencies, indicating that the risk thresholds across services for intervening with matters related to vulnerability are not in alignment. However, the activity driving the volume of police safeguarding notifications remains unknown and it may be that inappropriate notifications are being submitted by the police, the impact of which is reported elsewhere (e.g. strains between multi-agency working, see Ford et al., 2017a). The identification of vulnerability by the police as part of their assessment of risk of harm (Williams et al., 2009) is subjective, and based on both the willingness and capacity of individual police staff to assess vulnerability as part of their role (Asquith et al., 2016; Ford et al., 2017a). Research has identified that in cases of vulnerability, how police apply their discretion can impact on the care that people receive (Bartkowiak-Théron and Asquith, 2012b). Current models for responding to vulnerability may prevent police using discretion in activating relevant processes such as safeguarding referrals when working with vulnerability (Bartkowiak-Théron and Corbo Crehan, 2012). Furthermore, assumptions of who is ‘at risk’ (see Stanford, 2012) may encourage risk-averse behaviour by the police (Paterson and Best, 2016), as possibly evidenced through the high number of safeguarding notifications identified in this study. These findings have implications for policing, social services and multi-agency working, raising questions on differences across agencies in the identification of vulnerability, risk management, and thresholds for action. The proportion of police referrals that do not receive social services intervention highlight a need for co-ordination across agencies to deliver a more effective and efficient service for early identification and collective action to address the needs of vulnerable individuals.
A small proportion of individuals accounted for a high proportion of the notifications submitted during the one year period studied, with less than one in ten individuals accounting for over one third of the demand. This finding suggests a need for change in the current system with a large proportion of vulnerable individuals repeatedly being identified on police safeguarding notifications, and thus known to social services, but falling below the threshold for action. These vulnerable individuals require more effective intervention and appropriate action to protect them from harm and mitigate the risk of future notifications. This will also help to alleviate the burden that receiving a large amount of notifications poses on social services. It is problematic when vulnerability is not identified, as it can allow vulnerable individuals and those at risk to fall through the cracks (Asquith et al., 2016). Previous literature has discussed issues in the categorisation of vulnerability (Asquith et al., 2016; Bartkowiak-Théron and Asquith, 2012, 2017), including the assumption that if someone has a certain characteristic (e.g. mental illness) they are automatically vulnerable – what Bartkowiak-Théron and Asquith (2014: 94) term the ‘checkbox approach’ for categorising vulnerability. This approach potentially results in an over focus of those at risk, resulting in individuals designated at low-risk being denied access to services (Stanford, 2012). Identifying groups of individuals with increased risk of multiple safeguarding notifications is useful for the development of guidelines for the investigation of notifications so that the police are able to effectively target early intervention. Given that the majority of notifications made and assessed were for children aged under 10 years, these findings are similar to others which have found children to be at increased risk of re-referrals to children’s services (on average, 55% re-referred in 6 years; Troncoso, 2017). Additionally, due to the potential trauma that re-referral may cause to both subjects and families, the high levels of demand and its associated cost (Bilson and Martin, 2017), it is appropriate that effective practices for services to mitigate these negative effects are developed.
Despite more safeguarding notifications arising from individuals living in the most deprived quintile, the proportion of notifications resulting in referral was 50% higher in those resident in the most affluent areas. Whether this reflects a ‘real’ difference in the type of cases seen in wealthier versus poorer areas or just in how vulnerability is processed, requires further study.
Further, this study found clear differences in the characteristics of the individuals whose safeguarding notifications were referred to social services and those whose notifications go on for assessment. Thus, notifications for individuals in the youngest or oldest age groups and those from less deprived areas, were more likely to be referred regardless of their gender. However, referred notifications for individuals from more deprived areas and females were more likely to proceed to assessment. The first notification for the time period was also important for referral to social services by the police but not in the assessment of the referral made by social services. This finding suggests that repeat or multiple notifications may not necessarily equate to high levels of risk for the individual concerned, as although they are referred to social services they do not go on for assessment. This may be indicative of assessment for intervention being dependent on other information held on that individual by social services (e.g. a recognition that not everyone who may be categorised by the police as vulnerable is, or a consideration of individual resilience [Bartkowiak-Théron and Asquith, 2014]). Alternatively, multiple referrals for individuals not assessed as requiring intervention could indicate system fatigue or compassion burnout for that individual, meaning that individuals who regularly have a safeguarding notification and are repeatedly being referred may be seen as problematic, and not receive the attention and hence the support they need. Consequently, there may be no benefit in submitting multiple notifications for individuals, but further research should explore the outcomes for individuals with repeat referrals. More longitudinal research is needed with larger samples to examine police safeguarding referrals and their outcomes in more detail, as these findings have implications for how services risk assess individuals.
Furthermore, DVA was shown to be a major concern evident in just under one half of all police vulnerability notifications. The importance of early intervention to address DVA has been highlighted by the police service that this data corresponds to, and nationally police services are routinely inspected on their handling of DVA cases (HMICFRS, 2017; South Wales Police & Crime Commissioner, 2016). This study found no clear association between the nature of concern listed on notifications and if they were either referred to social services or assessed as needing intervention. If the NOC does play a factor in the processing of notifications and their outcomes, it is unclear why. The lack of any association between the nature of concerns and notification referrals or outcomes of assessment by social services demonstrates a possible disconnect between the police, who drive the notifications, and social services, who control the assessment of them. It is important for the management of this system that the practices of these two agencies are aligned. Research has found difficulties among police in identifying vulnerability (Dehaghani, 2017) and the NOCs in this study may be reflective of the way in which police understand, identify and approach vulnerability categories in the field (Bartkowiak-Théron and Asquith, 2012a). Researchers have argued that normative lists of who is defined as vulnerable (Asquith et al., 2016; Bartkowiak-Théron and Asquith, 2012) may not cover all vulnerabilities (Williams et al., 2009). Further, categories of vulnerability are not discrete, as individuals may fall into a number of categories over time and these may change with police contact (Asquith et al., 2016; Bartkowiak-Théron and Asquith, 2012, 2017). These issues may be reflective of the lack of association between the NOC of notifications and their outcomes, and have implications for how the police recognise and categorise vulnerability (Asquith et al., 2016).
This article contributes to the national and international understanding of the importance of the police response to vulnerability and adversity, through its identification of high levels of police-identified vulnerability and the outcomes for such individuals following identification. Its findings are of relevance to policing systems internationally as trends show a continuing rise in levels of police incidents that are not categorised as crime, but rather as vulnerability-related. Given the increasing levels of vulnerability-related demand for the police, there is a need for police to take proactive action using an early intervention approach to vulnerability to help prevent problems before they escalate (Waddell and Molloy, 2015). Effective partnership working is an essential part of early intervention to support the vulnerable. In the Welsh context, the Social Services and Well-being (Wales) Act 2014 and Well-being of Future Generations (Wales) Act 2015 promote partnership working with a focus on consideration of long-term preventative approaches that improve the well-being of individuals and address problems before they escalate. These Acts provide a context to support the development of a preventative and early intervention approach to vulnerability, on the part of the police and other agencies. In England and Wales, late intervention has been estimated to cost nearly £17 billion per year (Chowdry and Fitzsimons, 2016).
Currently in the UK the police response to vulnerability is managed through safeguarding notification submissions to the PPU. The findings of this research indicate that the police safeguarding referral system faces a large level of vulnerability-related demand with little resulting intervention from statutory partners. Research elsewhere has highlighted the need for police staff training and awareness to enable the identification of vulnerability (including that of victims), and guidance on when and how to interact and connect with partner agencies (Bartkowiak-Théron and Asquith, 2014; Bartkowiak-Théron and Layton, 2012; Ford et al., 2017; Williams et al., 2009). The application of a trauma-informed approach to policing may allow officers to better understand the demands of complex welfare cases, and enable them to work in a more supportive and preventative way. Research has identified that individuals exposed to childhood trauma are less likely to report support from the police during childhood and more likely to report as adults that the police are not supportive (Hughes et al., 2018), highlighting a challenge for how the police engage and support individuals in need. However, the police, alongside other agencies such as social services, may be well positioned to offer support or formal interventions, which can assist in the development of community resilience (Ungar, 2013). The need for policing to become trauma-informed is internationally recognised (Ko et al., 2008; Pinals, 2015; Webb, 2016). Research in the USA has found benefits from collaborations between police officers, mental health professionals and social workers (Compton et al., 2014; Greater Manchester Police and Crime Commissioner, 2017; The Vancouver Police Department, 2017).
Limitations
The present findings should be considered in light of several important limitations. Analysis is limited to outcomes of police safeguarding notifications shared with social services. It therefore does not examine the outcome of all police notifications made to other agencies during this period, or other notifications made to social services during this timeframe. Some of the notifications in this analysis may have also been shared with other organisations (e.g. wider health services, such as specialised mental health services or charities for instance Women’s Aid) and therefore may have received input from these. However, due to data limitations wider interventions for the notification and their outcomes is unknown.
The research team worked closely with the police and social services, who provided the data for this research, to seek only appropriate data items and try to minimise missing data (i.e. avoiding free-text fields). However, a number of data items were poorly completed and were consequently not used in analysis. For the one year in which the data corresponds, the police reference number for the occurrence that the safeguarding notification was related to was not recorded on the social services data system with the notification. No other unique identifier was used by both the police and social services for the notifications. To understand outcomes for individuals, the two datasets (police data and social service data) were matched on personal information provided in both datasets using the fields: surname, first name and date of birth. Data matching is subject to bias due, for example, to differences in the spelling of names or the use of aliases. Different data files were provided by child and adult social services due to the different systems used. Finally, it is important to acknowledge that this data represents a snapshot of time, and thus the individuals that the data corresponds to are likely to have had notifications before and after the period used for this analysis. Expanding the one year (1 January 2016 to 31 December 2016 inclusive) time frame used in this study was not possible due to the police using a different database to store records prior to this period, preventing data extraction. The fields collected on police safeguarding notifications were also different prior to 2016.
Conclusion
Over the past 10 years there has been an increasing focus on how the police in the UK can respond effectively to the rising demand of vulnerability and public protection. This study has demonstrated the extent of vulnerability-related demand that the police respond to, of which only a small percentage is acted on by social services. Our findings suggest that risk thresholds in relation to vulnerability and safeguarding across agencies are not in alignment. In turn, this has implications for how the police and other agencies respond to vulnerable individuals. A proactive early intervention approach from the police and other services is required to respond to, and support, vulnerable individuals. Processes for the identification and management of vulnerability by the police should be reviewed where only a small number of individuals are responsible for a large number of notifications, as this indicates that the current system does not adequately support those in need. The potential to improve the police safeguarding notification system is apparent. It is important that systems and processes that prioritise early intervention are in place to support vulnerable individuals who may not meet social service involvement thresholds. Supporting individuals before their level of vulnerability escalates, may prevent them from reaching thresholds for intervention. Such a system should also enable systems to accurately and quickly identify those who do need further input from social services. Any changes to the processes for dealing with vulnerability should be made in conjunction with further staff training and awareness raising to allow the police to effectively and efficiently identify vulnerability and offer appropriate support.
Footnotes
Acknowledgements
The authors would like to thank Public Health Wales, South Wales Police, The South Wales Police and Crime Commissioner and partners at Bridgend County Borough Council for their assistance with this research project.
Data availability statement
Datasets and other materials used in this article are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Home Office Police Innovation Fund and the South Wales Police and Crime Commissioner (Reference 2016-039).