
Abstract
Mental health professionals must contend with the troubling possible outcome of patient suicide death (PSD). Although it has been established that exposure to PSD causes various adverse emotional and cognitive experiences for MHPs, little is known about the actions organizational leaders can take to support them through it. A Delphi consensus study gathered feedback from 17 professionals with workplace postvention experiences to learn what supports are known to exist, which are believed to be important, and what barriers impede this support. The study yielded essential considerations to guide organizational leaders in supporting MHPs. Its fundamental implications are that emotionally supportive, personalized options, provided within the context of a positive working environment with high-quality, cross-level relationships, can benefit MHPs. However, under-response, non-response, and pathologizing or punitive responses from organizations and organizational leaders are significant barriers for MHPs in managing adverse responses after PSD.
Introduction
Postvention, a compassionate response to the needs of those bereaved by suicide, has been a critical consideration since the beginning of the field of suicidology (Shneidman, 1972). Survivors of suicide loss comprise a diverse group experiencing a bevy of adverse psychological, physical, and social consequences, for whom care is both ethical and necessary (Jordan & McIntosh, 2011). Early postvention research focused on supporting immediate kin and attachment figures, but in recent years, the impacts of exposure to suicide have been demonstrated to be extensively more widespread than initially conceptualized (Feigelman et al., 2018; Maple et al., 2019). Consequently, the postvention needs of additional groups, such as second responders, individuals who had a professional relationship with the deceased, have also been considered (Maple et al., 2019). Second responders include mental health professionals (MHPs) who provided treatment to the deceased right before they died, or earlier in life. Prior to being identified as second responders, patient suicide death was already viewed as an occupational hazard impacting MHPs personally and professionally (Chemtob et al., 1989; Litman, 1965). The presence of this hazard presents particular challenges for leaders in organizations planning to equip MHPs for working with patients exhibiting suicidal behaviors (MacGarry et al., 2022).
During their careers, most MHPs are likely to encounter at least one client who expresses suicidal ideation, attempts suicide, or dies by suicide (Schmitz et al., 2012), with some estimating that patient suicide death (PSD) impacts approximately one in four mental health professionals (Foster & McAdams, 1999). Consequently, no matter how diligently or knowledgeably MHPs perform to keep patients experiencing suicidality safe, MHPs and their organizational leaders must face the possibility of losing a patient to suicide (Chemtob et al., 1989; Foster & McAdams, 1999). While in many ways the grief responses of MHPs who lose a client to death by suicide mirror those of other survivors, there are unique characteristics due to the nature of their relationship with the deceased. Current research suggests that MHPs are significantly impacted by PSD (Aldrich & Cerel, 2022; Croft et al., 2023), which affects their professional and personal lives, as well as their mental health and emotional well-being (Lyra et al., 2021). Affective states of MHPs after PSD include grief, guilt, shame, and fear, and distressing subjective experiences of incompetence and helplessness (Downey & Alfonso, 2023). Adverse reactions are particularly prevalent for those previously exposed to suicidality (Van der Hallen, 2023), with higher levels of exposure to suicidality being associated with higher levels of depression, anxiety, and post-traumatic stress (Aldrich & Cerel, 2022). One study determined that 3.8% of psychiatrists experienced clinically significant stress- and trauma-related disorders after exposure to patient suicide (Barman & Kablinger, 2021). The deleterious impact of PSD has caused researchers to consider what kind of support is needed and sought after by MHPs. One study on the need for, search for, and sufficiency of support after PSD determined that almost one in 10 respondents who reported needing and seeking support also reported that the support they received was insufficient, and stress reactions to the event were highest among professionals who needed but did not receive sufficient support (Dransart et al., 2020).
Such challenging experiences may naturally lead to temporary or extended disruptions in an MHP’s functioning in their workplace, especially for those for whom the experience has resulted in post-traumatic stress symptoms (Gutin et al., 2011). Legal and ethical issues may also complicate grief processes for MHPs, because confidentiality considerations, advice from legal counsel to limit sharing about what happened with others, and thoughts about potential liability or actual litigation can produce intense anxiety and prohibit MHPs from openly expressing their experiences.
The impact of patient suicidal behavior varies from one MHP to another based on complex interchanges between personal characteristics and external circumstances. For example, Pisnoli and Van der Hallen (2022) determined that the attitude of MHPs toward suicide plays an important role in understanding individual differences in impact. MacGarry et al. (2022) also concluded that the intensity, duration, and extent of impact are not universal. Instead, key categories of vulnerability factors are responsible for different levels of personal and professional impact, such as personal factors, role-related factors, organizational factors, relationship factors regarding the patient, and other factors related to the incidence of suicidal behavior. The recognition that exposure to PSD will result in MHPs experiencing a bevy of adverse responses varying in duration and intensity, and that vulnerability factors may worsen these responses, has led many researchers to consider the particular postvention needs of MHPs (Dransart et al., 2020; Gutin et al., 2011; Levi-Belz, 2017; MacGarry et al., 2022; Sherba et al., 2019; Tamworth et al., 2022).
If the postvention needs of MHPs are not met, this will disrupt their ability to perform in the workplace (Gutin et al., 2011). Given how common a phenomenon PSD is, organizational leaders can expect such disruptions to exact a significant toll on organizational performance. There are additional concerns that responses to exposure to PSD may lead some MHPs to exit the behavioral health field entirely. For example, in one study, slightly over a third of the respondents said they considered a career change after a PSD or a patient’s non-fatal suicide attempt (Sherba et al., 2019). Such findings suggest that organizational leaders cannot afford to overlook postvention support, because without it, they will likely experience poorer outcomes and higher turnover rates among their mental health workforce. Additionally, organizational leaders need to plan to support the MHPs they employ because organizations themselves are systemic survivors of suicide loss, leading to a challenge best dealt with by organizational leaders (Berkowitz et al., 2011).
Organizations also need to support the postvention needs of MHPs after PSD because their support in such circumstances is crucial to their overall well-being and retention (Sherba et al., 2019). Rich relationships with colleagues, supportive supervisors and managers, and open communication with colleagues and supervisors are among the factors MHPs have identified as particularly beneficial in managing their responses (MacGarry et al., 2022; Sherba et al., 2019). Supporting MHPs after PSD requires that organizational leaders employ individualized, person-centered approaches where individual mental health providers are supported “flexibly based on their level of need” (MacGarry et al., 2022, p. 100). Additionally, this individualized support is strengthened when leaders foster a culture of open communication, as it empowers staff to voice their requests for support appropriately, such as requests for flexible work practices (e.g., facilitating leave or adjusting task demands) to help them manage distressing responses (MacGarry et al., 2022). However, organizations can create additional distress for MHPs if they act in such a way as to imply blame on the part of MHPs if a patient dies (Walter & Pridmore, 2012). Additionally, they may compromise their ability to support staff members who lose a patient due to their concerns about protecting themselves legally (Gutin et al., 2011).
For all these reasons, organizational leaders must plan to support MHPs in the event of PSD. However, few organizations have implemented policies to account for the possibility of these occurrences (Gutin, 2019). Some have claimed that suggestions, guidelines, and protocols already exist to help MHPs employed in organizations navigate the complicated sequelae of suicide bereavement (Gutin et al., 2011). However, scant empirical evidence exists regarding what organizational factors may moderate the impact of MHPs’ responses or the interventions their leaders should select to effectively support employees (Berkowitz et al., 2011; MacGarry et al., 2022; Sherba et al., 2019; Tamworth et al., 2022), and intervention studies to illuminate the acceptability and efficacy of different interventions for second responders like MHPs are almost “completely absent” from the literature (Maple et al., 2019, p. 381). Without knowledge of what approaches and actions will benefit MHPs, it is exceedingly difficult for organizational leaders to plan accordingly. To gain a deeper understanding of how organizational leaders can support MHPs responding to PSD, this study examined existing strategies that support them, identified necessary strategies, and explored barriers that hinder the provision of such support.
Method
Survey Design
A Delphi consensus method (Hsu & Sandford, 2007; Linstone & Turoff, 2002) was selected because it was recommended for developing organizational guidelines and procedures to counteract the impact of patient suicidal behavior on MHPs (MacGarry et al., 2022). The California Baptist University Institutional Review Board approved the study prior to the initiation of recruitment. The study required the opinions of people with occupational exposure to suicide. Informed consent for this study included explaining the potential psychological risks to prospective panelists and informing them that they could withdraw from the study at any time for any reason. Informed consent was obtained for this study from all participants. The study was conducted between December 2024 and March 2025.
Data Collection
The panelists provided qualitative responses and quantitative scores on surveys administered across four rounds. Textual responses were collected in all four rounds of the study, and scores on items coded from the textual responses in the first round were gathered in the second and third rounds. All data was collected electronically via Qualtrics. Dedoose, Excel, and Qualtrics Software were used to sort and code qualitative data, organize and analyze statistical data, and generate anonymized visual representations and summaries of findings to return to panelists in the third and fourth rounds as part of the Delphi group communication process.
Recruitment began using purposive and snowball sampling. Participants in this study were limited to two types of professionals experienced in postvention response. The first type was mental health professionals with lived experience with the death of one or more patients by suicide during their careers. The second category was organizational executives and mid-level organizational leaders who had experience providing support to mental health professionals who had lost one or more patients to death by suicide. After recruitment, potential participants were screened for eligibility and invited to begin the first round. In the first round, the panelists provided textual responses to the Round One Questionnaire (R1Q), which consisted of three questions with fill-in-the-blank options and two open-ended questions to prompt additional answers regarding potential supports and barriers. After the first round, the data from R1Q were coded and used to create the categories and items that comprised the Round Two Questionnaire (R2Q). In the second round, panelists scored the items on the R2Q using 5-point Likert scales and gave explanations for their scores. Their explanations were summarized and anonymized, and nondescript numeric monikers (e.g., Panelist 4, 9, 12, etc.) were randomly assigned to each panelist to reduce bias. These summaries were prepared to display to the panel in the third round. The panel’s scores from the R2Q in the second round were analyzed to determine which items the panelists agreed were most important to consider, and tables and graphs with statistical interpretations were prepared for display along with the summaries to present to the panel in the third round.
The third round began by providing the panel with the tables, graphs, and summaries from the second round. After reviewing this information, panelists completed the R2Q again and gave explanations for why they changed or did not change their scores. Scores and summaries from the third round were aggregated for the panelists to review in the fourth round, following the same procedures as those in the second round.
In the fourth round, panelists viewed the scores and summaries from the third round and gave concluding thoughts on the group’s determinations. Textual responses across rounds were analyzed for themes of agreement that indicated group consensus.
Plan of Analysis
Demographic information for panelists was analyzed to determine the mean, mode, median, range, and standard deviation of characteristics, including age, gender, professional title, and geographic location of work. In the first round, textual data were coded to identify, organize, categorize, and itemize themes for the construction of a quantitative measure (the R2Q), which would be used in the subsequent two rounds. Mayring’s Qualitative Content Analysis approach (2014) was employed to code the first round due to its precedent in other Delphi studies (Gohres & Petra, 2023) and its ability to explore the research problem by reducing textual responses and forming inductive categories that can then be quantitatively analyzed for frequencies and percentages. It was employed to reduce panelists’ written responses into distinct categories using inductive category formation, which were used to construct the Likert scales used in the second and third rounds. The categories were left unweighted when constructing the scales to avoid biasing panelists toward certain categories.
In the second and third rounds, the quantitative scores the panelists provided on the R2Q were analyzed by calculating the median and interquartile range to determine the importance of each item to the panelists and group agreement regarding each item (Giannarou & Zervas, 2014; Hasson et al., 2000; Steinmuller, 2023; von der Gracht, 2012). They were also used to aggregate the data for display to panelists via visual representations and tables in the third and fourth rounds (Trevelyan & Robinson, 2015).
After the third round, the median and interquartile range scores on the R2Q were reanalyzed using the same procedures as in the second round. What remained was to evaluate differences in scores between the rounds and determine if consensus and stability were achieved through the Delphi process. The criteria for successfully determining consensus and stability in a Delphi study are often subjective; therefore, a high threshold for consensus and agreement was established to ensure that the items scored more highly by the group represent the items most relevant to the panel (Binning et al., 1972; Holey et al., 2007). Items rated in the third round with a median of 4 or higher (m
Since the Delphi design is intended to bring together the wisdom of the crowd (Surowiecki, 2004), rigor was ensured through member checking by sharing categories, items, and supporting quotes in the second round with panelists; anonymized feedback from panelists in the third; and asking panelists to provide open-ended feedback on the group’s scores, feedback, and themes of agreements for inclusion in the final study. Finally, rigor was ensured through saturation, as the four iterative rounds of the study invited panelists to share their thoughts multiple times in multiple ways until they had no further insights into the research topic (Creswell & Creswell, 2018).
Results
Seventeen panelists participated in the first round. In the second round, the R2Q items regarding recommended supports were completed by 14 of the first-round participants (82.3%), and the items regarding barriers to support were completed by 12 of the first-round participants (58.8%). Eleven panelists gave explanations for their scores regarding supports, and nine gave explanations for their scores regarding barriers. In the third round, 10 participants rated R2Q items regarding recommended supports (58.8%). Post-hoc testing for these items using the Wilcoxon matched-pairs signed-rank indicated reliability between rounds (n = 27, Z = −0.5766, p = .56). Nine panelists completed the R2Q items regarding barriers to support in the second round (52.9%). Post-hoc testing using the Wilcoxon matched-pairs signed-rank test revealed low reliability for the items in the barriers to support categories, presumably due to attrition in participation (n = 31, z = −2.2144, p = .0271). The items in the barriers to support categories were analyzed again, this time excluding the responses of participants who did not complete the third round, and under these conditions demonstrated reliability across rounds (n = 39, Z = 0, p < .05). Consequently, the scores presented regarding items of barriers to support are from the data collected from the nine panelists who completed both the second and third rounds. Eight panelists (47) gave explanations for their scores in the third round. Seven panelists (41.1%) provided final thoughts in the fourth round regarding supports and barriers.
Characteristics of the Panelists
Characteristics of Panelists
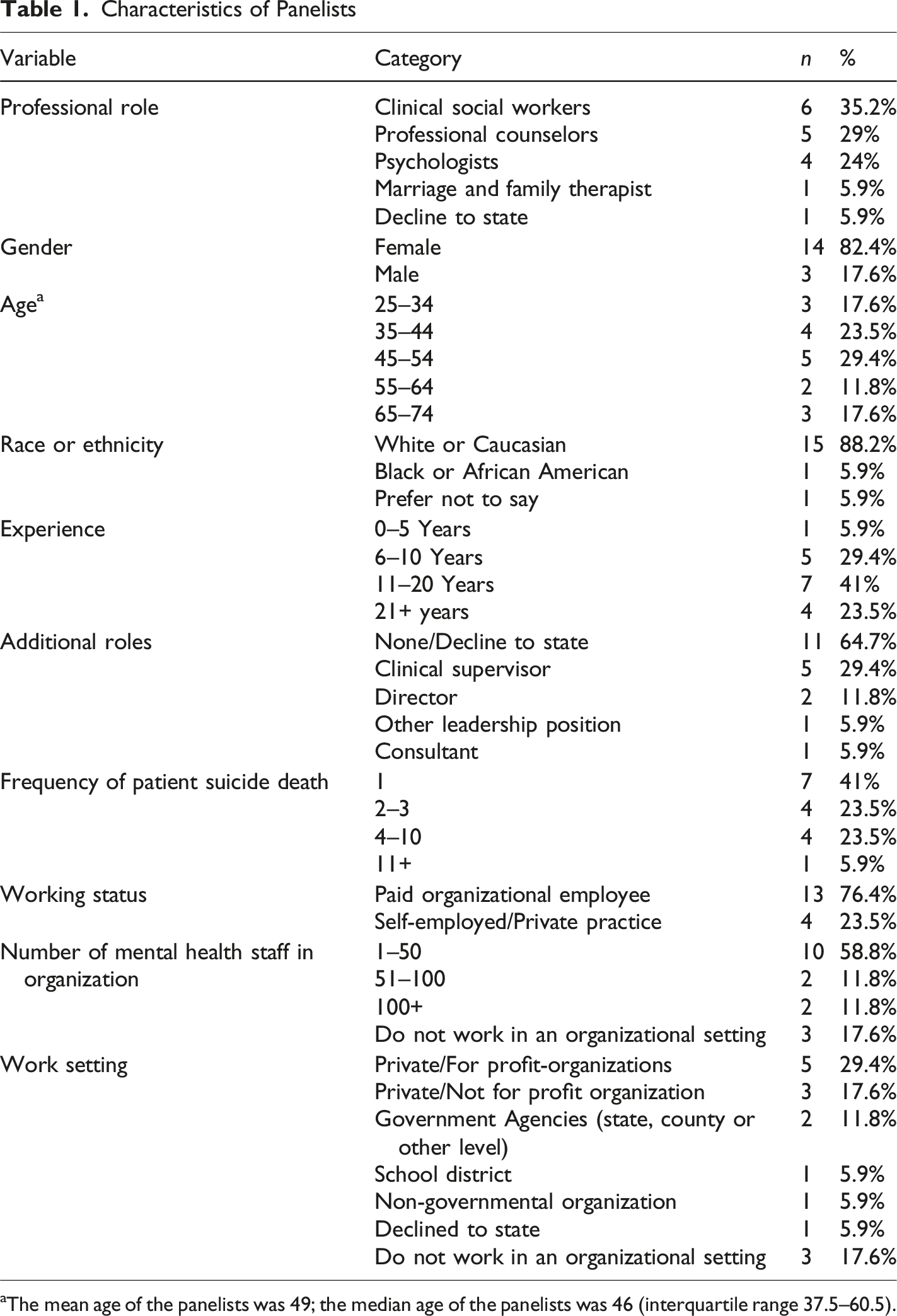
aThe mean age of the panelists was 49; the median age of the panelists was 46 (interquartile range 37.5–60.5).
First Round
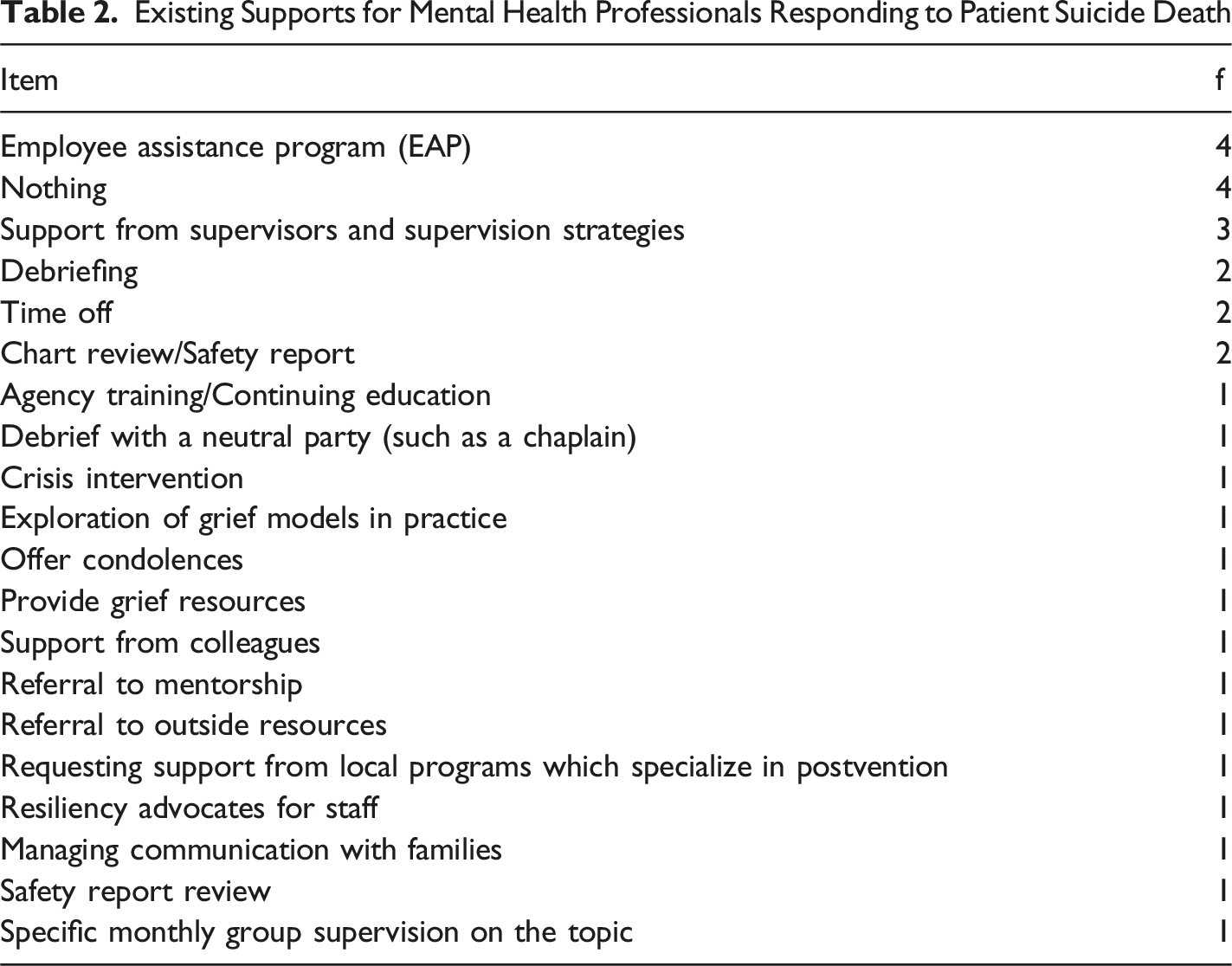
Existing Supports for Mental Health Professionals Responding to Patient Suicide Death
Second Round
In the second round, panelists completed the RQ2. They rated 44 out of 73 (60.2%) items regarding postvention support recommendations as rather important or essential. They rated 46 out of 72 (63.9%) items regarding postvention support barriers as moderate or severe barriers. Textual explanations were prepared for display to panelists in the third round.
Third Round
In the third round, panelists reviewed the scores and rationales of other panelists and repeated the R2Q. The panelists rated 42 out of 73 (57.5%) items regarding support as important or essential. The panel’s scores on all items related to supports are displayed in Appendix A. The panel rated 61 out of 72 (84.7%) items regarding barriers as severe or moderate. The panel’s scores on all items related to beliefs are displayed in Appendix B. This resulted in a total of 42 recommended strategies and 61 barriers to be considered by organizational leaders seeking to support MHPs after PSD. Textual explanations were prepared for display to panelists in the fourth round.
Final Results
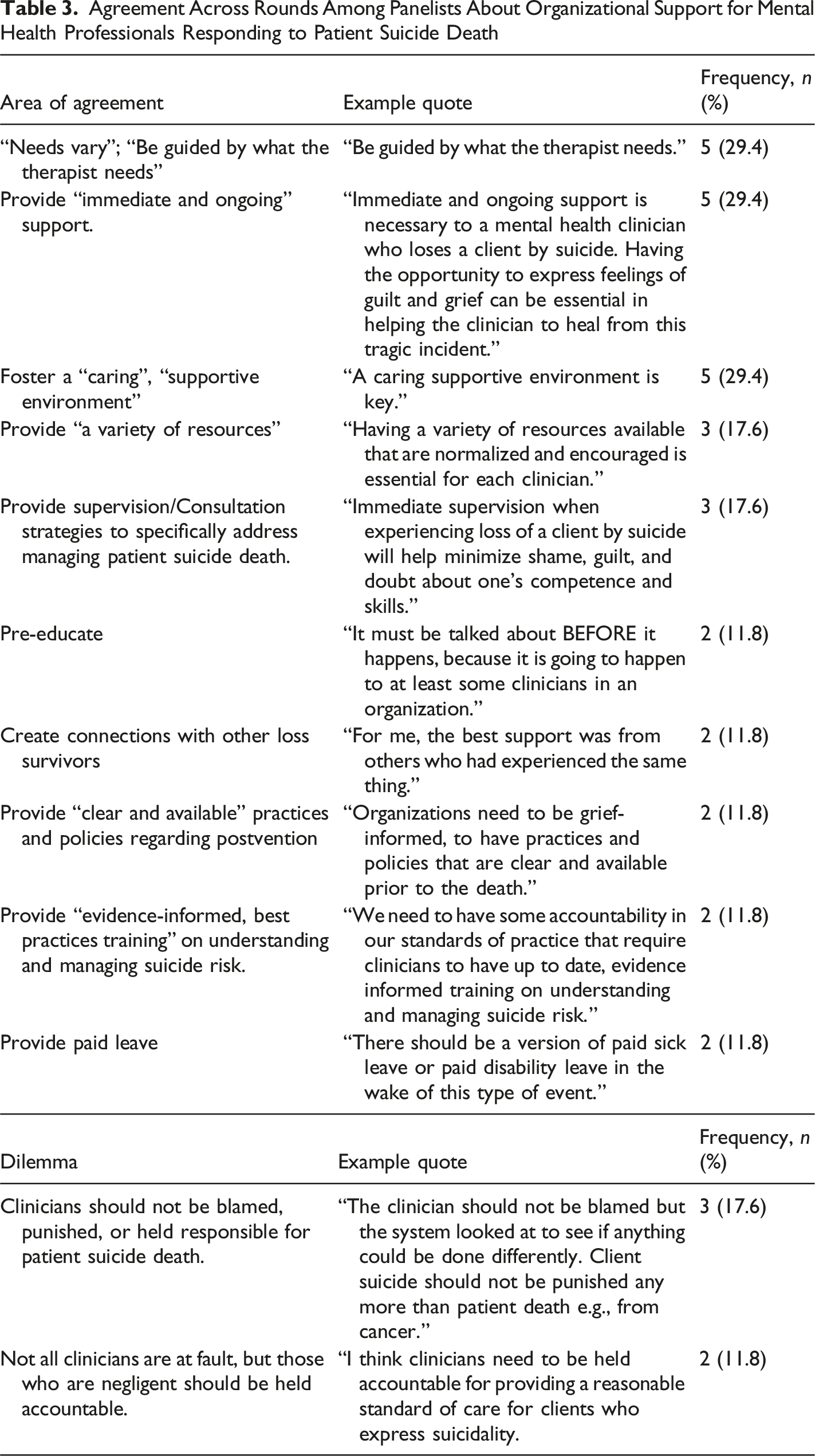
Agreement Across Rounds Among Panelists About Organizational Support for Mental Health Professionals Responding to Patient Suicide Death
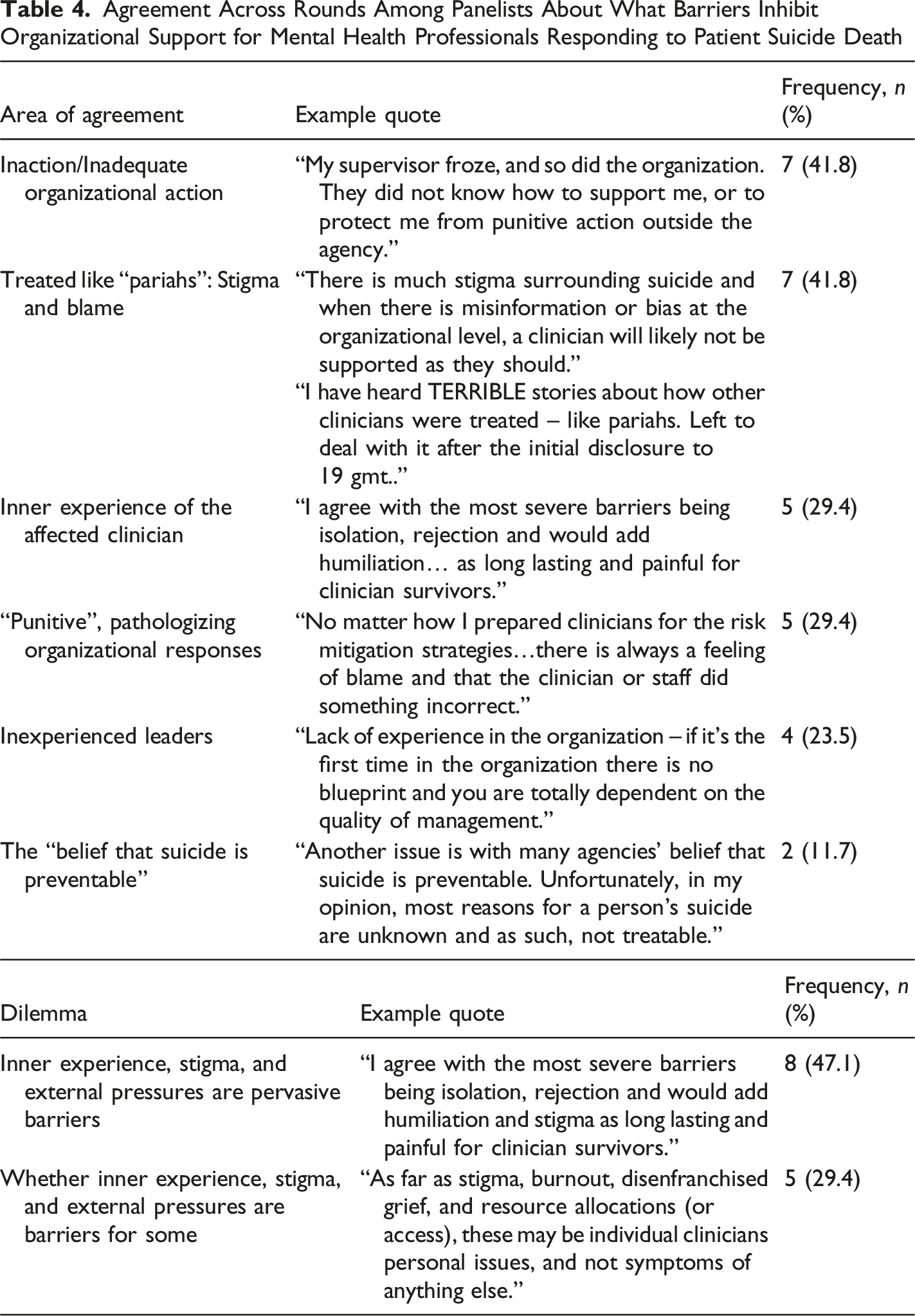
Agreement Across Rounds Among Panelists About What Barriers Inhibit Organizational Support for Mental Health Professionals Responding to Patient Suicide Death
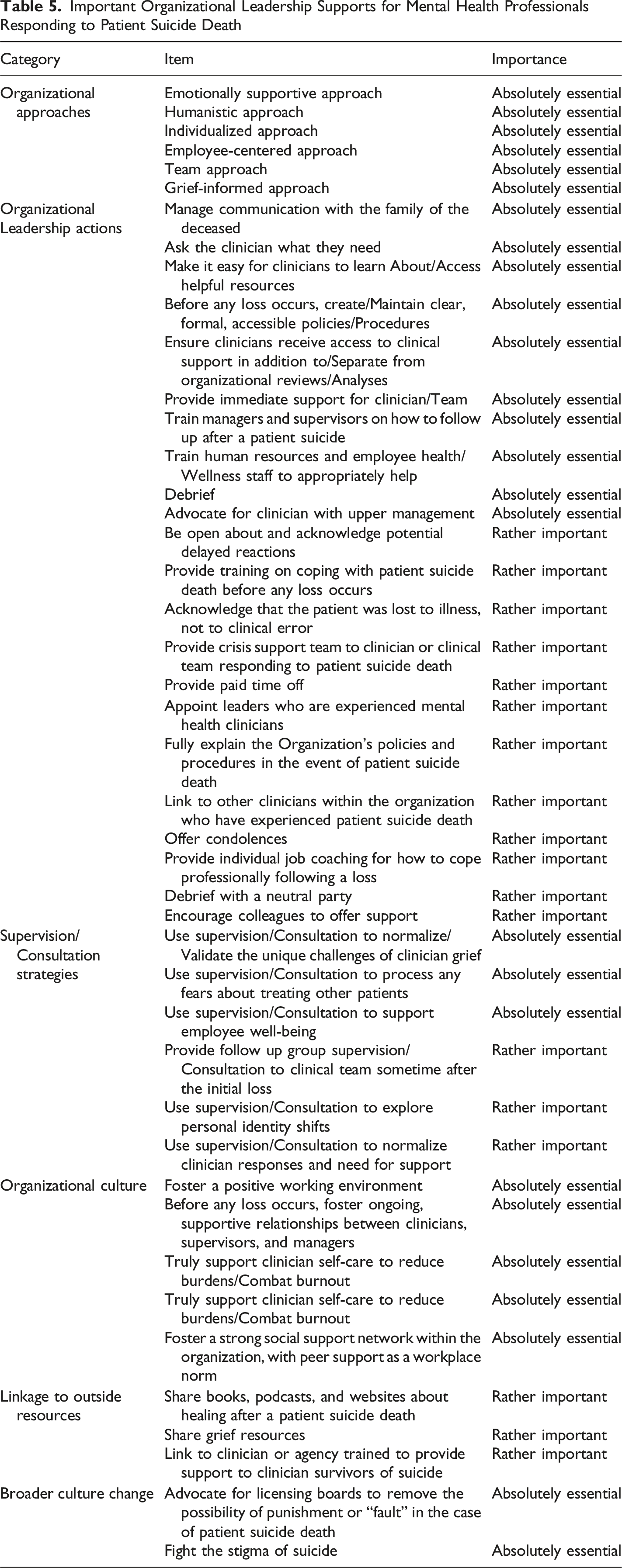
Important Organizational Leadership Supports for Mental Health Professionals Responding to Patient Suicide Death
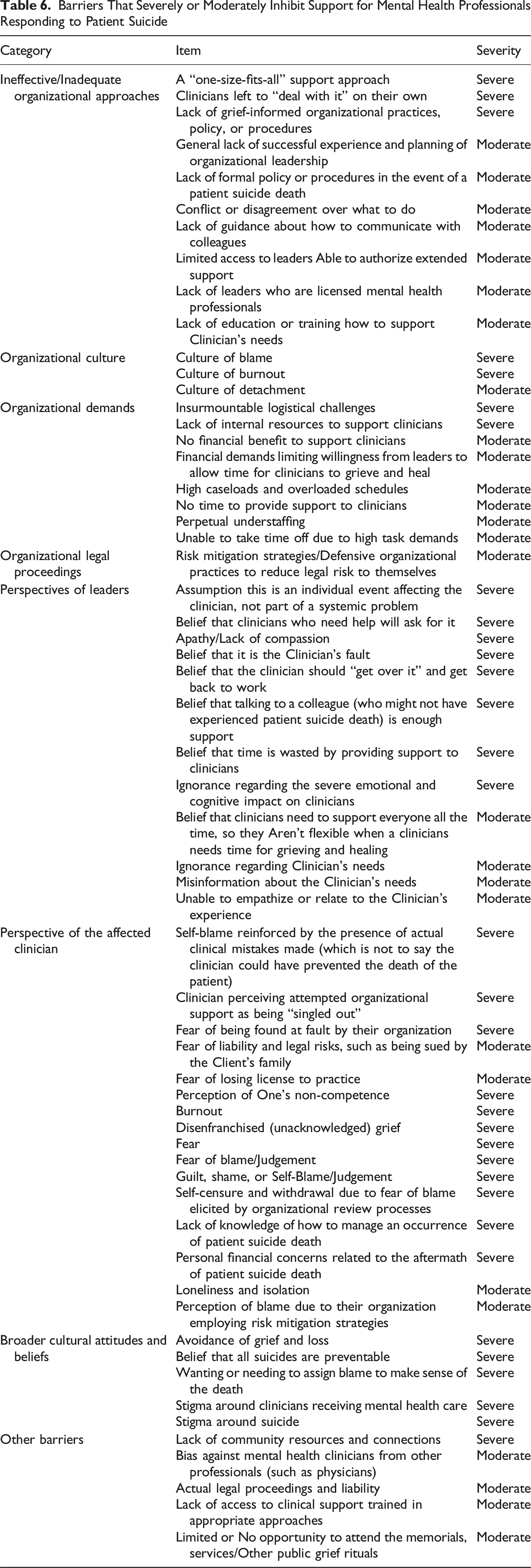
Barriers That Severely or Moderately Inhibit Support for Mental Health Professionals Responding to Patient Suicide
Discussion
This study identified consensus recommendations on what types of support MHPs need from organizational leaders after a patient suicide death, as well as what barriers organizational leaders need to overcome for such support to be effective. The following discussion will be organized around the panel’s three types of findings: existing supports, recommended supports, and barriers to support. They will be compared with existing literature regarding organizational and leadership support, leading to inferences about effective practices that organizational leaders can undertake to support MHPs responding to PSD.
Existing Supports
Of the existing supports known to the panelists, referrals to employee assistance programs (EAPs) were frequently identified. However, this panel did not consider these referrals important for supporting MHPs, suggesting that, when available, this support offered little consistent benefit. These findings need close consideration because referrals to EAPs have been recommended previously as “a valuable resource in the aftermath of suicide death” for organizational employees (Berkowitz et al., 2011, p.165). It may be that the unique professional relationship MHPs had with their patients who died by suicide renders this support less helpful to them than it does to other organizational employees. Thus, organizational leaders cannot expect referrals to an EAP to sufficiently support an MHP after a patient suicide.
One troubling finding of this study is that many panelists knew of no existing supports at all for MHPs responding to PSD. Combined with the ineffectiveness of referrals to EAPs, this demonstrates that many panelists experienced no support, or support so generic and ineffective that it might as well have been absent. This finding gives credence to Gutin et al.’s conclusion that MHPs are often “left to cope with the consequences of this difficult loss on their own” in “less than optimal conditions” (2011, p.94). While the results of this study were limited by the boundaries of the panel’s knowledge, it appears that, despite decades of PSD being recognized as an occupational hazard (Chemtob et al., 1989), MHPs remain under-supported. Consequently, organizational leaders will need to proactively plan to support them, expecting to do so with a limited repertoire of resources and limited supportive infrastructure at their disposal.
Nevertheless, several additional, effective existing supports for MHPs were identified by panelists, specifically debriefing, support from supervisors, supportive supervision strategies, time off, and aspects of chart review and safety report processes. The panel agreed that debriefing was highly important; however, some stated that the quality of the debriefing and its purpose (e.g., support rather than organizational risk mitigation) influence its supportive value. These findings highlight the efficacy of previous recommendations that targeted supervision practices should be provided to unlicensed clinicians after a suicide that focus on grief reactions, exploratory questions, and professional impact (Schulz, 2005). The panel’s recommendations on time off for affected MHPs also echoed earlier recommendations (Weiner, 2005). Consequently, organizational leaders should ensure MHPs receive supportive debriefing in addition to and separate from organizational risk mitigation practices, and that they receive supervision directly related to the death of the patient. Additionally, they need to provide (or advocate for) short-term paid time off options.
Recommended Supports
In this section, the panel’s recommendations for essential or highly important supports after a patient suicide will be discussed. First, they strongly agreed on the importance of rich workplace relationships across levels, specifically determining that organizational leaders can best provide support when they adopt emotionally supportive, individualized, employee-centered approaches within positive working environments with ongoing, supportive relationships between MHPs, supervisors, and managers. There was also agreement that hiring organizational leaders with experience in mental health care would enhance their ability to support MHPs, as they would bring a personal perspective to guide their actions.
The panel also recommended preemptive actions that leaders can take before any actual loss to prepare all MHPs in the event of PSD. They suggested that these leaders generate and maintain clear, formal, and accessible policies and procedures for PSD and ensure that managers, supervisors, human resources staff, and employee wellness staff receive training on managing this psychological hazard. Guidelines for generating policies and procedures that leaders may find useful are Sample Agency Practices for Responding to Client Suicide (Sung, 2016) and Guidelines to Assist Clinical Staff After the Suicide of a Patient (Grad, 2012).
An additional preemptive action recommended by the panel was to educate MHPs on crucial information in case of patient suicide, such as it being a possibility, common responses to it, organizational policies and procedures regarding it, and resources available to MHPs to help them manage their responses. Taking an educational approach would not only help prepare MHPs in case of PSD, it could also help reduce stigma around suicide itself, an issue identified by Gutin et al. (2011), lessening the possibilities of isolated, disenfranchised grief. Educating staff ahead of a patient suicide could also reduce the likelihood that they will accrue undeserved organizational blame, because it might counteract prevailing social messages implying that if a suicide occurs, it necessarily follows that someone caring for the patient failed (Walter & Pridmore, 2012). Incorporating these pre-training recommendations could be accomplished by sharing resources such as What to do if a Patient Dies by Suicide: Guidelines for Professionals (Quinnet, n.d) within the course of routine training or supervision activities.
The panel also recommended actions that should be taken after an instance of PSD. In these tragic cases, organizational leaders should prioritize giving immediate support to affected MHPs and affected treatment teams. Several recommendations were that organizational leaders should offer condolences, directly ask what the MHP needs, provide access to relevant internal or external resources for clinician survivors, and, if possible, connect them with another MHP in the organization who has lived experience with PSD and a willingness to share their experiences. Organizational leaders should also manage communication with the deceased’s family, clarify organizational policies and procedures regarding the event, and encourage colleagues to offer support. Along with providing direct, immediate support, leaders should acknowledge potential delayed reactions and continue tending to the needs of MHPs over an extended period. Although several of the actions recommended by the panel have been described elsewhere (Berkowitz et al., 2011; McGann et al., 2011a, 2011b; Weiner, 2005), this study is the first to assemble them into a single list of meaningful actions.
After a patient suicide death, the panel also recommended supportive supervision and specific supervision and consultation strategies. The panel’s recommended strategies had several objectives, all of which should culminate in the overall goal of providing high-quality patient care. The objectives included normalizing and validating the unique challenges of clinician grief, their need for support, and their responses, processing fears about treating other patients, and exploring personal identity shifts and how they relate to professionalism. Several panelists cautioned that supervisors must carefully consider their dual role as both a professional mentor and guide for MHPs and as an employee beholden to an organization. Although the panel agreed upon many supervision strategies as essential or important for supporting MHPs, previous researchers have noted that MHPs may hesitate to engage in supervision regarding their reactions after PSD due to a sense of systemic and emotional vulnerability (Schulz, 2005). Nevertheless, supervisors have a responsibility to assist MHPs in working through the professional and personal issues following a suicide (Schulz, 2005). The panel’s supervision recommendations may guide supervisors in this responsibility.
Barriers to Support
As might be expected based on findings in previous literature (Aldrich & Cerel, 2022; Croft et al., 2023; Lyra et al., 2021), some of the barriers to support mentioned by the panel were their distressing affective and cognitive experiences. These experiences, by themselves, were a barrier to receiving support in an organizational setting, especially during reviews of the incident or other circumstances when MHPs might withdraw or self-censure to protect themselves. These internal barriers are best addressed by providing a menu of options to affected employees, including options outside the organization for confidential support, such as individual counseling with a therapist trained in postvention support, or sharing resources such as cliniciansurvivor.org, and by ensuring that MHPs have a clear understanding of what will be done with the information they provide to leaders after a patient suicide, including what they share in the course of clinical supervision with supervisors employed by the organization. These recommendations underscore those of MacGarry et al., who urged organizations to “endeavor to move from generalized or standardized responses to the event, such as case reviews, to more person-centered approaches where the mental health provider is supported flexibly based on their level of need” (2022, p.100).
Along with the internal experiences of affected MHPs, the panel also asserted that organizational leaders’ viewpoints could be barriers to support. They emphasized that invalidating viewpoints from their leaders, ranging from outright apathy or lack of compassion and understanding due to ignorance or judgment, were in themselves barriers to receiving support. Panelists who did not feel safe or understood by their leaders naturally struggled to perceive they were being supported, regardless of their actions. It may be that practices such as those taught in Emotionally Engaged Leadership (Stedman & Andenoro, 2015) could help organizational leaders better connect with their employees’ perspectives and needs. Hence, actions intended to be supportive may be more likely to be perceived as such.
The contributions of the panel also supported the assertion of Tehan & Thompson (2012) that ignoring or failing to plan for the effects of any grief and loss issues in the workplace will undermine the organization’s efficiency, effectiveness, and reputation. Leaders who do not consider the bereavement-related needs of their followers can expect increased stress, anxiety, and depression, relational strain with coworkers and managers, reduced performance and reliability in daily tasks, and physical health problems. Such neglect will be viewed by staff as a trust-eroding “failure of leadership,” especially if leaders of organizations communicate values of care and support for patients without demonstrating the same care and support to their staff (Tehan & Thompson, 2012, p.272). Applying these values within the organization requires consideration of individual employees’ needs and overall support strategies that the whole organization can utilize. Their conclusion that neglecting grieving staff members after this type of patient death has a deleterious impact, combined with the panel’s contributions specific to MHP responses to PSD, establishes non-responses and under-responses as some of the most severe barriers to employee support.
The panel also lent credence to Gilbert’s statement that, in times of trial, leadership is an “essential attribute” in maintaining a culture of meaning and humanity (2007, p. 219). Without leadership effectively maintaining cultures of meaning and humanity, trials such as encountering PSD become more devastating when they occur in an unsupportive or rejecting environment. The panel’s discussion of organizational cultures of blame, burnout, and detachment accentuates the importance of maintaining a culture that supports employees by carefully cultivating organizational values and respectful communication standards. Recommendations from (Sansbury et al., 2014) on developing a culture of resiliency for staff encountering psychological hazards might assist leaders in preparing to support MHPs after a patient suicide. They recommend focusing organizational goals on teaching and reinforcing trauma recovery concepts such as safety, empowerment, collaboration, choice, and trust, and asking employees, “what, if any, changes are needed to ensure these concepts are weaved into the agency culture?” (Sansbury et al., 2014, p. 119). They can also help promote resiliency by providing ongoing growth opportunities, teaching employees to periodically self-assess for adverse responses to psychological hazards, and developing structures for employees to meet to foster a supportive, self-care environment. However, for self-assessment and meeting structures to be effective, organizations must be perceived as safe, empowering, and collaborative environments. Otherwise, staff are unlikely to feel safe enough to share openly, and thus cannot benefit.
Sansbury et al.'s (2014) recommendations that leaders create structures wherein staff can foster a supportive self-care environment also echo the sentiments of the panel in this study, when they recommended that leaders promote peer support networks as a workplace norm so that, in the case of PSD, MHPs would have a rich community network to draw on, reducing perceptions of isolation and fear. To enhance the benefit of these relationships within these environments, the panel also recommended that leaders promote clinician self-care to reduce burnout. The panel’s views also aligned with those of other researchers, who found that strong relationships and strong communities of support are essential for managing personal responses (McGann et al., 2011a).
The barriers presented by the panelists are also echoed in previous literature on postvention experiences in organizations. For instance, Gutin et al. (2011) emphasized that stigma, fear of legal reprisal, and concerns about risk management have created barriers to support from organizational leaders. Reactive responses to these challenges may impede receptive, sensitive communication with staff. Creating clear policies and procedures ahead of any instance of patient suicide may help to reduce stress on the part of leadership that causes them to show up less receptively or sensitively in the moment with staff. Leaders may also find that being prepared ahead of time allows them to dispel fears of judgment and blame more easily than if they respond reactively in the moment. Additionally, by developing and discussing policies and procedures related to patient suicide, organizational leaders acknowledge that patient suicide, while never desired, is not always preventable. Rather, it is possible, even when MHPs are following the standard of care and performing excellently. Making this difficult truth discussable will assist leaders in supporting MHPs in such an instance without them immediately feeling blamed, regardless of the level and type of care the patient received prior to their death.
Panelists varied in their views on the role of accountability in supporting MHPs. Despite differing views presented at the beginning of the study, the group’s consensus by the third round was that advocacy should be directed at licensing boards to remove the possibility of fault in PSD cases. The drop in participation from panelists completing the second and third rounds may have inflated the agreement between panelists on this item. Alternatively, the arguments of some panelists may have persuaded others to change their opinion
Along with organizational barriers, the panel agreed that extra-organizational cultural attitudes and beliefs, as well as external pressures such as stress from actual legal proceedings, deficiencies in community resources, access to appropriately trained therapists to help them heal, and limited opportunities to attend public grief rituals, could all present barriers to support. These challenges make the work that can be done within an organization to support MHPs even more important, especially that of advocacy and linking with additional resources when they are unavailable within the organization.
This study provides building blocks for empirical research on postvention organizational leadership support for MHPs responding to PSD, in the form of lists constructed using the joint knowledge of experienced panelists, which can be empirically examined. The result of these insights includes a series of recommendations, based on group consensus, that organizational leaders can implement in cases of patient suicide. These insights, along with a vignette generated for practical application, are described in an additional document intended for distribution to organizational leaders. See Supplemental materials to view this document.
Limitations
Despite this study’s strengths, several limitations should be considered. First, the Delphi design employed is based on the assumption that a panel of knowledgeable individuals assures a high-quality outcome in addressing a complex problem (Dalkey, 1969; Linstone & Turoff, 2002). Additionally, the design gathers the opinions of knowledgeable persons, but it does not evaluate whether their views are accurate. This study also experienced a reduction in panelists across rounds, which reduced the reliability of some findings, especially those with a wider variance between scores, as well as in portions of the questionnaires that were not completed by all panelists. The length and psychological impact of the study may also have deterred the participation of other eligible individuals with valuable insights. Finally, purposive and snowball sampling limited recruitment to people known to the researcher or professional groups associated with the researcher, which may have falsely amplified consensus due to homogeneity factors. Due to these limitations, empirical research with larger representative population samples is needed to confirm the study results.
Directions for Future Research
Several directions for future research can confirm the accuracy of its meaningful findings. First, the lists of the recommended organizational leadership supports and barriers to support for MHPs responding to PSD generated by the panelists in this study require empirical research to determine content validity. Second, since several panelists recommended pre-training or education for MHPs to enable them to manage responses to PSD, more research is needed to determine the impact and optimal nature of such a program. Third, the emergence of clinician accountability and individual factors dilemmas presents philosophical questions that need further exploration. Further exploration of these dilemmas would help identify the underlying issues driving them and determine what, if anything, can be done to resolve them.
Conclusion
Organizational leaders must carefully plan how to support their staff so they can continue to provide high-quality mental health care after an event of PSD. This study explored the opinions of a panel of knowledgeable individuals who identified existing supports for MHPs responding to PSD, recommended supports organizational leaders can provide, and identified barriers to their implementation. A compassionate, flexible, and individualized approach from organizational leaders, incorporating essential actions such as managing communication with the family of the deceased and providing a menu of available support options to affected clinicians, was determined to be an excellent starting point for organizational leaders seeking to assist MHPs in their grief journey.
Supplemental Material
Supplemental Material - Supporting Mental Health Professionals After a Patient Suicide: A Delphi Consensus Study
Supplemental Material for Supporting Mental Health Professionals After a Patient Suicide: A Delphi Consensus Study by Carolyn Michelle Cummings in OMEGA - Journal of Death and Dying.
Footnotes
Acknowledgements
I sincerely thank Dr. Jason Kiker for his invaluable guidance throughout this research, as well as the fellows of the Dr. Paul and Annie Kienel Leadership Institute for their unwavering support and expertise. I also thank the Coalition of Clinician-Survivors of Suicide for their postvention resources and references, which made this work possible. Finally, I honor the bravery and honesty of the panelists who shared their grief experiences in this study for the good of others.
Ethical Considerations
Ethical approval for this study was obtained from the California Baptist University Ethical Review Board (052-2425-EXP).
Consent for Publication
Written informed consent was obtained for anonymized patient information to be published in this article.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.