
Abstract
Past research showed that bereaved individuals with higher levels of prolonged grief symptoms report poorer health. However, research addressing the downstream consequences of prolonged grief to physical health and its potential underlying mechanisms is still limited. This study explored whether meaning in life explained the associations of prolonged grief symptoms with mental and physical health outcomes. In a cross-sectional study (N = 332), participants who experienced the death of a family member, a romantic partner, or a close friend 12 months or longer ago completed an online survey. Results showed that higher levels of prolonged grief symptoms were associated with more depression symptoms, higher perceived loneliness, and lower perceived physical health. These associations were explained by the perception of less meaning in life. Our findings offer insights for researchers and mental health professionals that can contribute to improving health among bereaved adults. Implications and suggestions for future research are discussed.
Introduction
The death of an emotionally intimate person has been listed among the most challenging life events (Szuhany et al., 2021). Grief refers to the emotional reactions after such a type of loss, and has been described as a natural and common response to this experience (De Stefano et al., 2021). Although grief reactions tend to become milder over time for most bereaved individuals, a significant minority reports experiencing severe, persistent, and prolonged grief (Boelen & Lenferink, 2022; Eisma et al., 2023). In current editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) and the International Classification of Diseases (ICD-11), severe and prolonged grief symptoms (e.g., identity disruption, sense of disbelief, intense loneliness) have been termed prolonged grief disorder (PGD; Eisma, 2023; Shevlin et al., 2023). Results of a recent cross-national study in 16 countries (e.g., the United Kingdom, Germany, the Netherlands, Nigeria, Kenya) showed that around 13% of the bereaved individuals reported prolonged grief symptoms (Comtesse et al., 2024). Past research showed significant sociodemographic risk factors for prolonged grief, including being an older woman, having fewer years of education, and perceiving lower socioeconomic status (Aoyama et al., 2021; Johnsen et al., 2012; Mason et al., 2020). Some additional risk factors were also found to contribute to experiencing higher levels of prolonged grief symptoms, such as pre-loss grief symptoms (Buur et al., 2024), lack of empathy or social support from close others (Asmat et al., 2024; Sarper & Rodrigues, 2024), having a close relationship with the deceased (Jann et al., 2024), and losing someone after a sudden (e.g., cardiac arrest, Carlsson et al., 2023) or violent death (e.g., suicide, homicide, fatal accident; Doering et al., 2024). Understanding the risk factors for developing prolonged grief symptoms (e.g., closeness to the deceased or the type of death) is particularly crucial, as experiencing these symptoms potentially leads to significant impairment and adverse effects on subjective well-being over time (Prigerson et al., 2021).
Prolonged grief has been associated with poorer mental and physical health outcomes. For example, recent studies showed that bereaved individuals with higher levels of prolonged grief symptoms also reported more depression and anxiety symptoms, higher loneliness, and lower subjective well-being (Eisma & Buyukcan-Tetik, 2025; Peinado et al., 2024). Similarly, experiencing higher levels of prolonged grief symptoms has been associated with poorer physical health outcomes, including pain, heart palpitations, and fatigue (Carlsson et al., 2023; Williams et al., 2021). The associations between higher levels of prolonged grief symptoms and subsequent health outcomes (e.g., depression symptoms, feelings of loneliness, perceived physical symptoms) may be explained by the indirect effect of public stigma (i.e., being a target of negative attitudes, emotions, and behaviors merely for departing from what society considers “normal”; Parcesepe & Cabassa, 2013). Indeed, recent experimental studies have shown strong negative appraisals (e.g., eliciting negative attributions and emotional reactions) of bereaved individuals (e.g.,, being perceived as less emotionally stable and eliciting more anger) not only when they experience prolonged grief symptoms related to the death of an emotionally intimate person (Dennis et al., 2022; Eisma, 2018; Eisma et al., 2019; Gonschor et al., 2020; Zammit et al., 2024), but also when they lack of recognition for their grief experiences (e.g., grieving the death of a companion animal; Sarper & Rodrigues, 2025). Perceiving strong stigma from others, thus, has been shown to decrease help-seeking behaviors (Pattyn et al., 2014), and increase the risk of developing prolonged grief (Heeke et al., 2017) and experiencing psychological distress (Scocco et al., 2017).
In addition to its adverse effects on mental and physical health (i.e., both directly and indirectly), prolonged grief can also be associated with how individuals perceive their lives and construe their future. From an existential perspective, meaning in life refers to the sense and significance felt in relation to one’s own existence, and stems from individuals’ connections with close others (Ivers et al., 2024; Li et al., 2021). As the death of an emotionally intimate person leads to losing a connection with the deceased, bereaved individuals may experience a crisis of meaning later on (i.e., feeling that life is meaningless without the person who died; Steffen, 2019). Past research showed that less meaning in life is associated with lower life satisfaction and self-esteem, poorer mental and physical health outcomes (e.g., lower psychological well-being, physical functioning impairments; Jim & Andersen, 2007; Soucase et al., 2023), more depression symptoms, and higher perceived loneliness (Kleftaras & Psarra, 2012; Macià et al., 2021). Furthermore, meaning in life was found to mediate associations between psychological variables (e.g., anxiety, hopelessness) and poorer mental health outcomes (e.g., depression; Sun et al., 2022; Szcześniak et al., 2022). For example, results of a longitudinal study showed that cancer survivors reported higher emotional distress due to less meaning in life (Jim & Andersen, 2007). Likewise, a recent cross-sectional study showed that meaning in life mediated the associations between symptom distress, and mental and physical components of quality of life among patients with chronic heart failure (Liu et al., 2023). However, research has yet to examine whether the associations between less meaning in life and poorer mental and physical health outcomes are also observable among bereaved individuals. Together with mental and physical health outcomes, bereaved individuals with prolonged grief symptoms may experience significant impairment in other important domains (e.g., social and occupational functioning; Eisma, 2023). Specifically focusing on grief experiences, a lower sense of purpose after the death of a close person was found to be associated with more severe grief reactions (Giang et al., 2024). For example, prolonged grief symptoms include feelings of meaninglessness (i.e., feeling that life is meaningless without the person who died) and identity changes (i.e., feeling that a part of oneself has died; Hilberdink et al., 2023; Prigerson et al., 2021). Hence, experiencing a lack of meaning in one’s life can potentially be associated with greater psychological distress, and negative mental and physical health correlates among bereaved adults (Steger et al., 2006). These results emphasize the importance of examining the role of meaning in life when individuals are coping with grief.
Current Study and Hypotheses
Past research showed that prolonged grief is associated with less meaning in life (Hilberdink et al., 2023; Ivers et al., 2024; Prigerson et al., 2021), and lacking meaning in life is associated with more depression symptoms, higher perceived loneliness, and lower perceived physical health (Jim & Andersen, 2007; Kleftaras & Psarra, 2012; Macià et al., 2021). Building upon this evidence, we hypothesize that meaning in life is a potential underlying mechanism for the associations between higher levels of prolonged grief symptoms, and poorer mental and physical health outcomes. Replicating past research (Carlsson et al., 2023; Eisma & Buyukcan-Tetik, 2025; Peinado et al., 2024), we expected participants who report higher levels of prolonged grief symptoms to also report more depression symptoms (H1a), higher perceived loneliness (H1b), and lower perceived physical health (H1c). Aligned with recent studies (Hilberdink et al., 2023; Ivers et al., 2024; Prigerson et al., 2021), we also expected participants who report higher levels of prolonged grief symptoms to report less meaning in life (H2). Lastly, we expected meaning in life to mediate the associations between prolonged grief symptoms and depression symptoms (H3a), perceived loneliness (H3b), and perceived physical health (H3c). A depiction of our hypothesized model is shown in Figure 1. Mediation theoretical model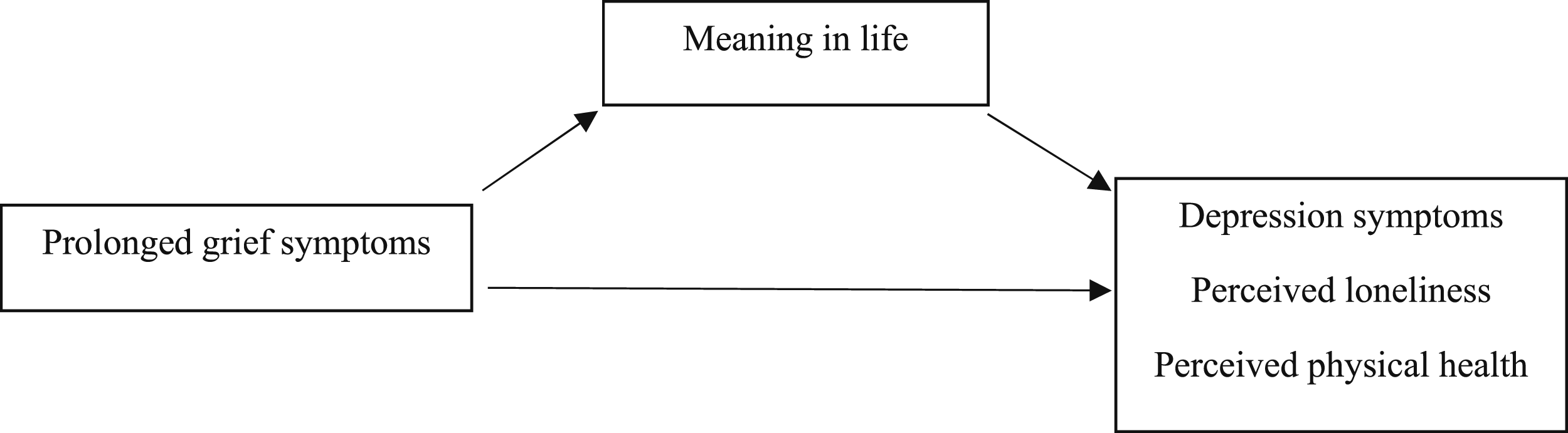
Moreover, research has shown an increased risk of developing prolonged grief among older women, and bereaved adults with fewer years of education and lower socioeconomic status (Aoyama et al., 2021; Johnsen et al., 2012; Mason et al., 2020), or individuals who lost a close family member (Holland & Neimeyer, 2011; Lobb et al., 2010) to a violent death (Hardison et al., 2005; Wilson et al., 2022). Given their importance to our main variables under examination—and particularly to grief experiences—, we explored if our theoretical mediation model remained significant after controlling for these risk factors (i.e., sociodemographic variables, the relationship with the deceased, and the type of death).
Methods
Participants and Procedure
This study was part of a larger project examining how bereaved individuals differ in their grief experiences (“Understanding the antecedents and implications of prolonged grief for psychosocial adjustment, health, and well-being”). Prior to the data collection, the study was approved by the Ethics Council at Iscte-Instituto Universitário de Lisboa (Ref.: #22/2021). Data collection was completed between April 2021 and June 2022. Prospective participants from four European countries—Portugal, Cyprus, Turkey, and the United Kingdom—were recruited on Clickworker, a crowdsourcing platform used for online data collection with users from around the world. The survey was hosted on Qualtrics and made available in Portuguese, Turkish, and English so participants could select the language they felt most comfortable with. The informed consent presented a detailed description regarding the main aim of the study, the estimated duration of the survey, the potential distress participants might experience while responding to the grief-related questions, and their rights to abandon the study without providing any justification.
After giving their consent, participants were asked to complete the eligibility criteria items. Only participants who indicated being at least 18 years old and having experienced the death of a family member, a romantic partner, or a close friend 12 months or longer ago were considered eligible for the study. The time criterion was based on the prolonged grief diagnosis presented in the DSM-5-TR (Eisma, 2023). Individuals who failed to meet these criteria were directed to the end of the survey, informed they were not eligible for the study, and thanked for their interest. Eligible participants were then presented with the standard demographic information form, followed by the remaining measures. In the end, participants were thanked, informed about the main goals of the study, given the contact information of the researchers, and provided with detailed information on public health services in case they considered to have felt distressed or anxious after their participation, or wished to learn more about how to seek professional help in these services. Participants who successfully completed the survey received €1.50 on their Clickworker account.
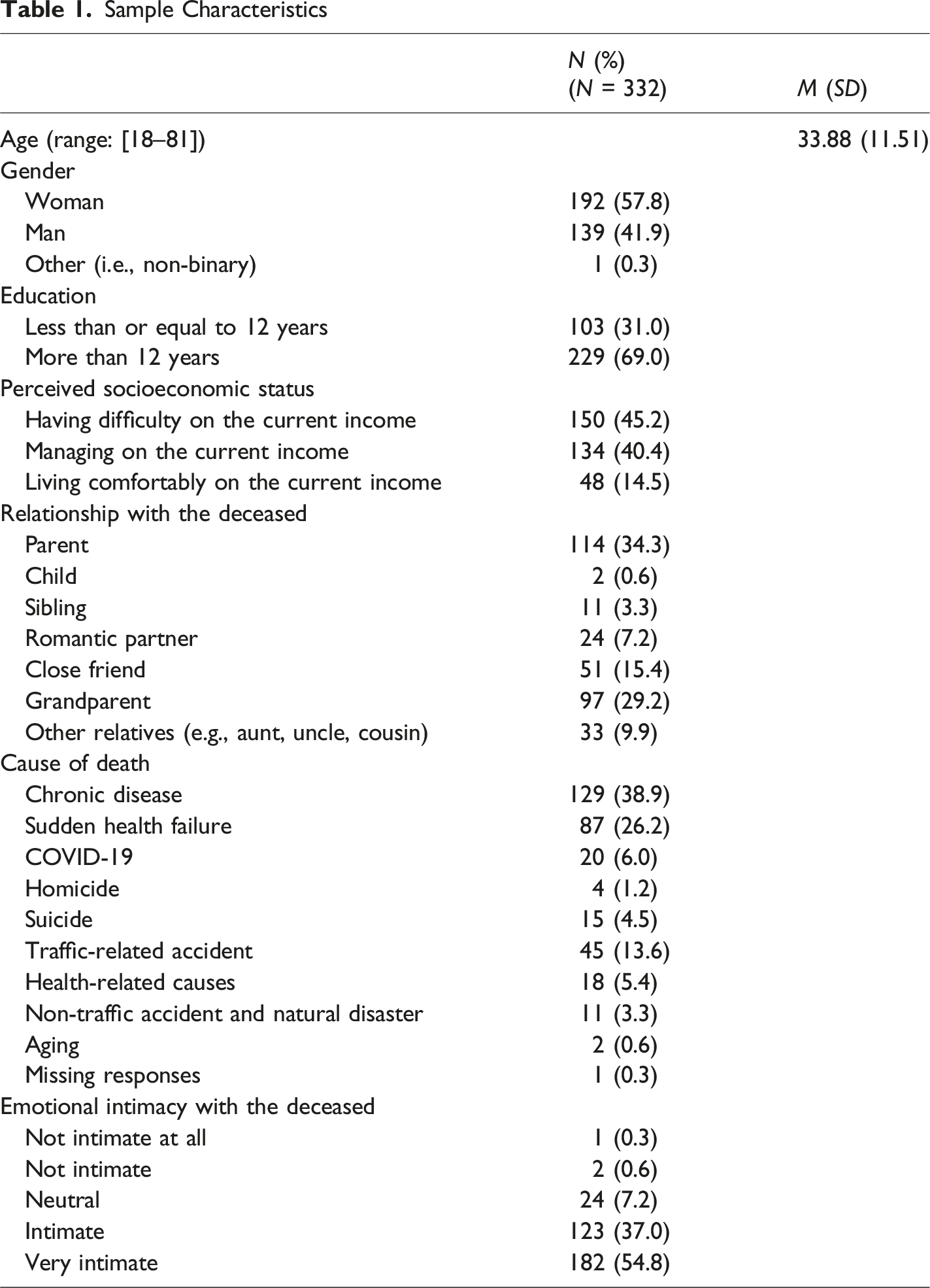
Sample Characteristics
Measures
For the Portuguese and Turkish versions of the survey, we used previously validated measures. For the measure that was not previously validated in our target samples—the Three-Item Loneliness Scale—, we followed the procedure of translation and back-translation (Titlestad et al., 2017). Specifically, both researchers, who are native in either Portuguese or Turkish and fluent in English, translated the original items and response scale into their languages. These items were then back-translated into English with the help of colleagues from the same research group. Final translations were then reviewed by the team, and discrepancies were resolved through discussion until the translated items reflected their original meaning. Apart from the Inventory of Complicated Grief, none of the measures herein reported have been used elsewhere. Notably, the measures assessing meaning in life, depression symptoms, perceived loneliness, and perceived physical health have been previously used among bereaved samples (Al-Mamun et al., 2025; Arnoldy et al., 2023; Lenger et al., 2020; Linley & Joseph, 2011).
Demographic Information
Participants were asked to complete the standard demographic information form and indicate their age, gender, education, perceived socioeconomic status, relationship with the deceased, cause of death, and emotional intimacy with the deceased.
Prolonged Grief Symptoms
We used the Inventory of Complicated Grief (PT version: Frade et al., 2009; TR version: Erdem Atak et al., 2012; EN version: Prigerson et al., 1995) to assess prolonged grief symptoms. Participants were asked to think about the most important person they lost and answer 19 items (e.g., “I feel disbelief over what happened”) using 5-point rating scales (0 = Never to 4 = Always). We computed a mean score by averaging responses (PT version: α = .90; TR version: α = .93; EN version: α = .91), with higher scores indicating higher levels of prolonged grief symptoms.
Meaning in Life
We used the Presence subscale of the Meaning in Life Questionnaire (PT version: Portugal, 2017; TR version: Boyraz et al., 2013; EN version: Steger et al., 2006). This subscale includes five items (e.g., “My life has a clear sense of purpose”) and assesses the presence of meaning in life (i.e., understanding the meaning, purpose, and significance of one’s own life) on 7-point rating scales (1 = Absolutely untrue to 7 = Absolutely true). We computed a mean score by averaging responses (PT version: α = .92; TR version: α = .90; EN version: α = .89), with higher scores indicating more presence of meaning in life.
Depression Symptoms
We used the Patient Health Questionnaire-2 (PT version: Torres et al., 2013; TR version: Sari et al., 2016; EN version: Löwe et al., 2010) to assess depression symptoms. Participants were asked to indicate how often (0 = Not at all to 3 = Nearly every day) they experience “Little interest or pleasure in doing things” and “Feeling down, depressed, or hopeless” over the last two weeks. We computed a mean score by averaging responses (PT version: r = .77; TR version: r = .53; EN version: r = .61), with higher scores indicating more depression symptoms.
Perceived Loneliness
We used the Three-Item Loneliness Scale (Hughes et al., 2004) and asked participants to indicate how often (1 = Hardly ever to 3 = Often) they feel lonely in their daily lives (e.g., “How often do you feel that you lack companionship?”). We computed a mean score by averaging responses (PT version: α = .85; TR version: α = .83; EN version: α = .85), with higher scores indicating higher perceived loneliness.
Perceived Physical Health
We used a single item from the physical health subscale of the 36-item Short Form Health Survey (PT version: Ferreira, 2000; TR version: Koçyiğit et al., 1999; EN version: Ware et al., 1995) and asked participants, “In general, would you say your health is…”. Responses were given on a 5-point rating scale (1 = Poor to 5 = Excellent), with higher scores indicating higher perceived physical health.
Data Analytic Plan
We conducted a secondary data analysis by using data previously collected for the larger project (Sarper & Rodrigues, 2024). First, we computed descriptive statistics and overall correlations between our main variables (i.e., prolonged grief symptoms, meaning in life, depression symptoms, perceived loneliness, perceived physical health). We then tested our hypotheses through separate mediation models using the PROCESS macro for SPSS (Model 4) with 10,000 bootstrap samples and 95% confidence intervals (Igartua & Hayes, 2021). In all models, prolonged grief symptoms scores were the predictor variable and meaning in life scores were the mediator variable. Outcome variables were depression symptoms scores (Model A), perceived loneliness scores (Model B), and perceived physical health scores (Model C).
Lastly, we tested the robustness of our results considering potential risk factors. For the loss-related questions, we relied on past research (Buur et al., 2024; Holland & Neimeyer, 2011) and categorized the relationship with the deceased as close family (parent, child, sibling, romantic partner), close friend, and extended family (grandparent, other relatives), and the type of death as natural/anticipated (chronic disease and other anticipated health-related causes, aging), natural/sudden (sudden health failure and other sudden health-related causes), related to COVID-19, and unnatural/violent (homicide, suicide, traffic-related accident, non-traffic accident and natural disaster). We started by computing separate one-way ANOVA to explore if scores in our main variables differed according to age (i.e., 18–24 vs. 25–44 vs. 45 and older; Steger et al., 2009), perceived socioeconomic status (i.e., having difficulty vs. managing vs. living comfortably), the relationship with the deceased (i.e., close family vs. close friend vs. extended family), and the type of death (i.e., natural/anticipated vs. natural/sudden vs. COVID-19 vs. unnatural/violent). Post-hoc comparisons with Bonferroni adjustment were computed when significant differences were observed. We also computed independent samples t-test to compare scores according to gender (i.e., women vs. men) and education (i.e., less than or equal to 12 years vs. more than 12 years). Then, we computed the mediation models including these variables as covariates.
Results
Preliminary Results
Descriptive Statistics and Correlations Between Measures
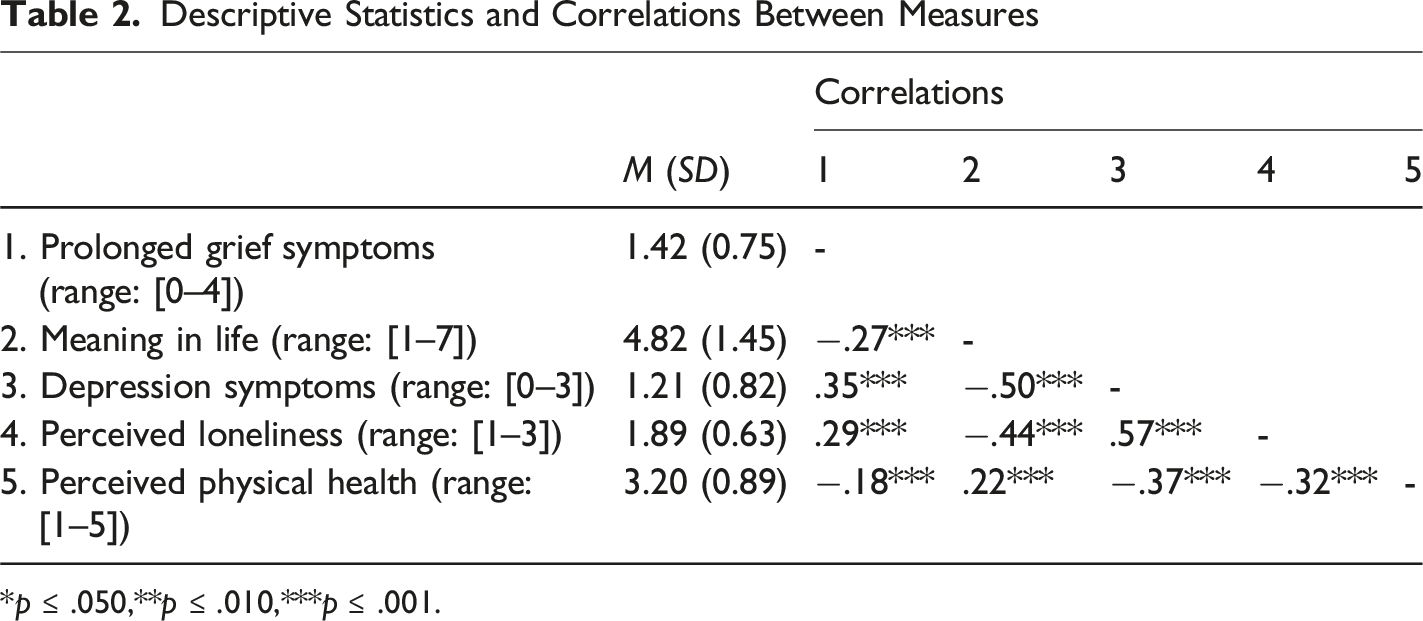
*p ≤ .050,**p ≤ .010,***p ≤ .001.
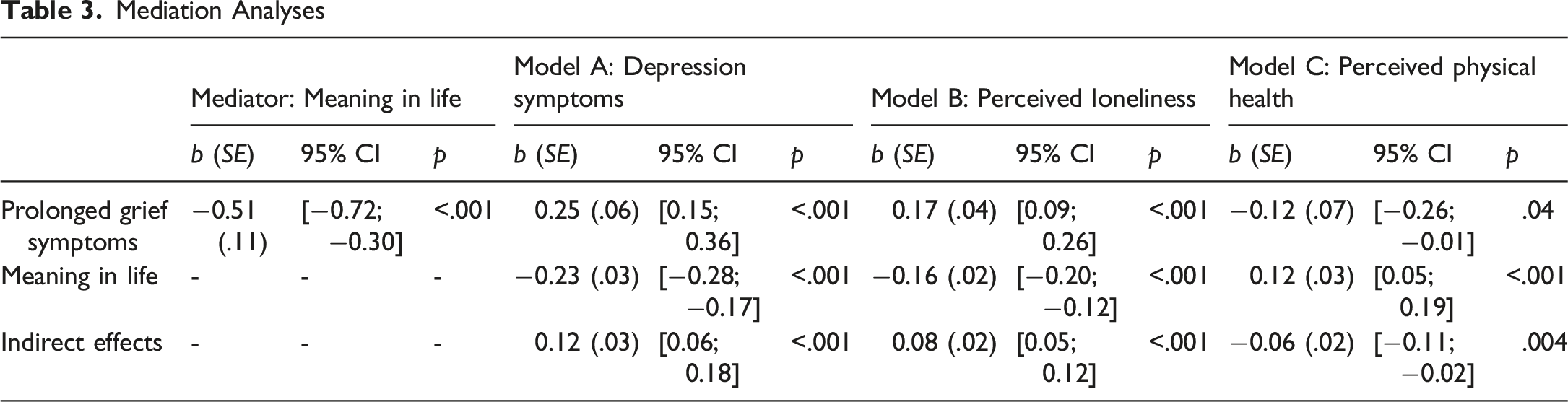
Mediation Models
Mediation Analyses
Controlling for Risk Factors
Descriptive Statistics for Prolonged Grief Symptoms, Meaning in Life, Depression Symptoms, Perceived Loneliness, and Perceived Physical Health According to Age and Gender
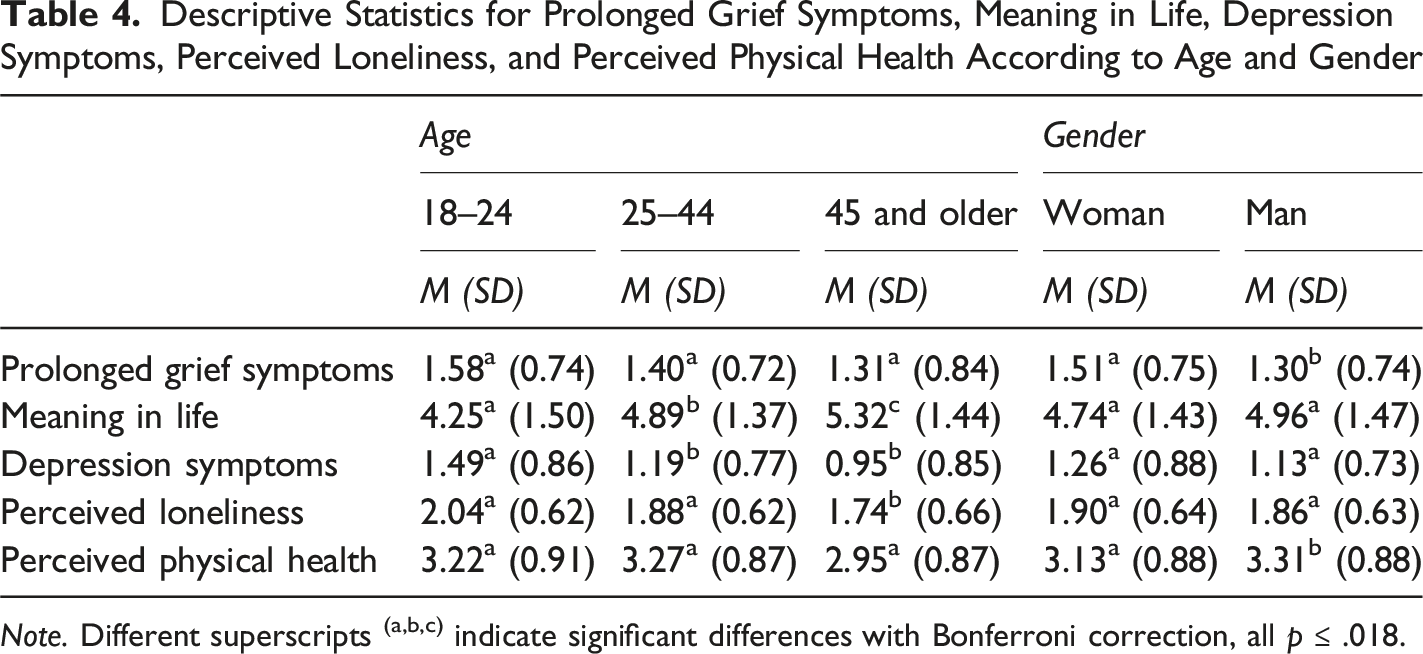
Note. Different superscripts (a,b,c) indicate significant differences with Bonferroni correction, all p ≤ .018.
Descriptive Statistics for Prolonged Grief Symptoms, Meaning in Life, Depression Symptoms, Perceived Loneliness, and Perceived Physical Health According to Education and Perceived Socioeconomic Status
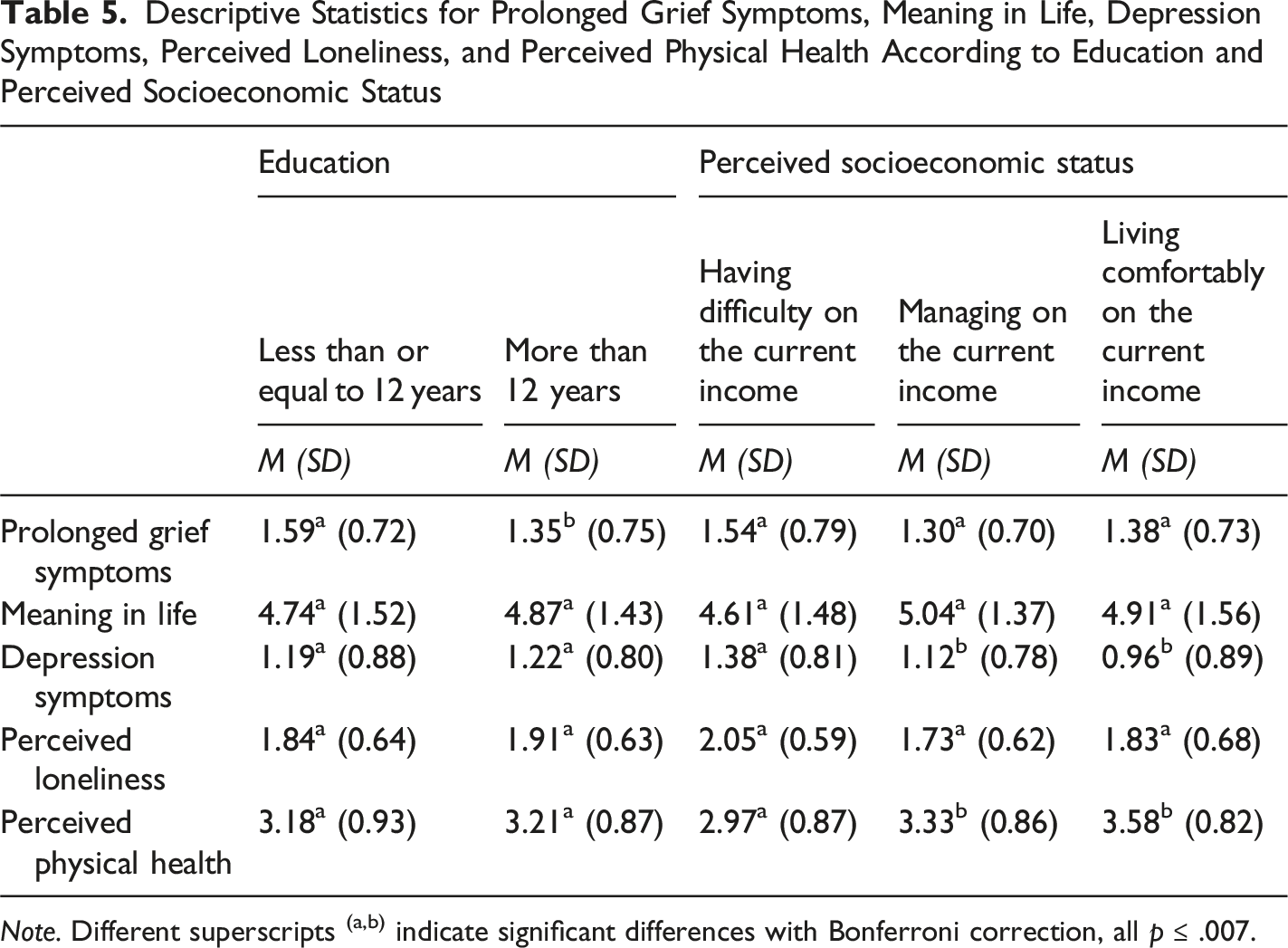
Note. Different superscripts (a,b) indicate significant differences with Bonferroni correction, all p ≤ .007.
Descriptive Statistics for Prolonged Grief Symptoms, Meaning in Life, Depression Symptoms, Perceived Loneliness, and Perceived Physical Health According to Relationship With the Deceased
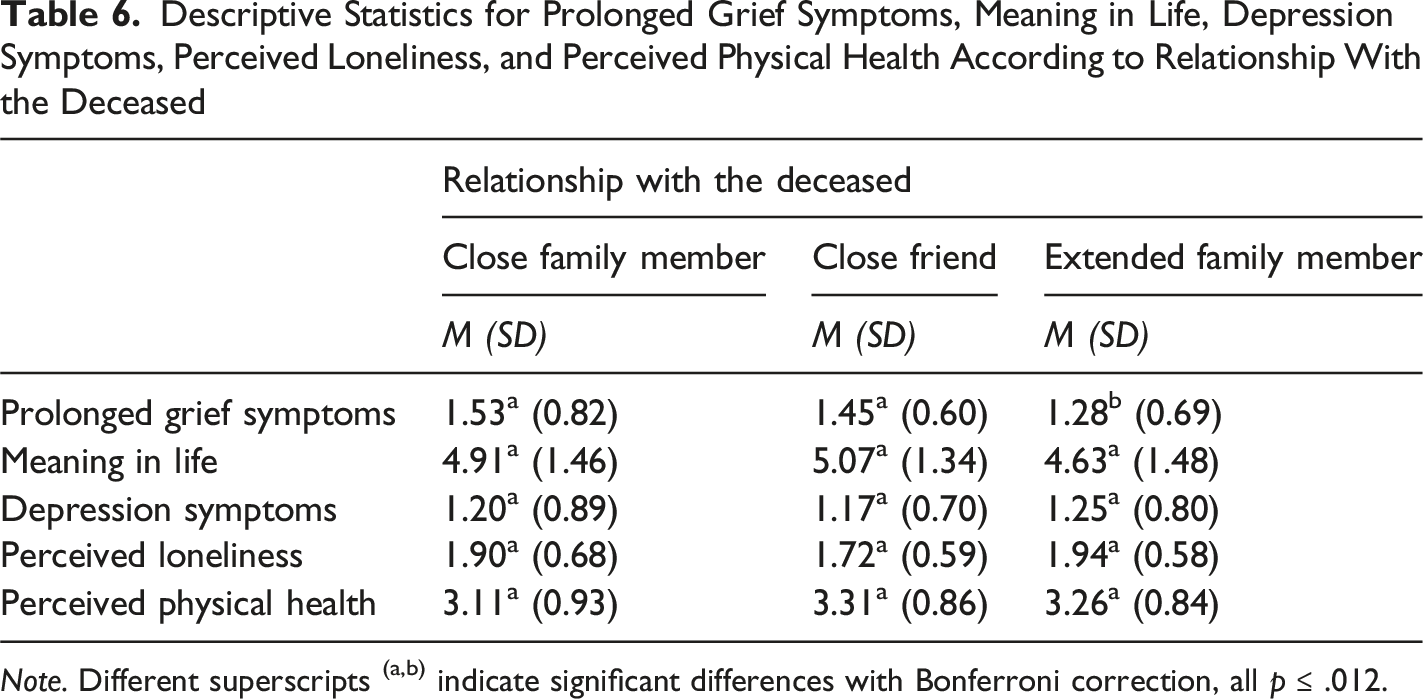
Note. Different superscripts (a,b) indicate significant differences with Bonferroni correction, all p ≤ .012.
Despite the differences reported above, the results of the mediation models remained significant even after controlling for the risk factors.
Discussion
Past research has shown that higher levels of prolonged grief symptoms contribute to mental and physical health impairments (Carlsson et al., 2023; Maccallum & Bryant, 2020). Alongside worsened health outcomes, prolonged grief symptoms also include feelings of meaninglessness (Prigerson et al., 2009, 2021). Understanding the changes in perceptions toward life is particularly important, as meaning in life was found to explain associations between psychological variables (e.g., anxiety, hopelessness) and perceived mental and physical health (e.g., depression, perceived physical impairments; Jim & Andersen, 2007; Sun et al., 2022; Szcześniak et al., 2022). However, these studies were conducted among different types of cohorts (e.g., cancer survivors; Jim & Andersen, 2007). By including meaning in life in our hypothesized model, our findings offered novel insights into an underlying mechanism also observable among bereaved samples. As expected, we found that higher levels of prolonged grief symptoms were associated with more depression symptoms (H1a), higher perceived loneliness (H1b), and lower perceived physical health (H1c). Our findings are aligned with recent research (Eisma & Buyukcan-Tetik, 2025; Peinado et al., 2024) and show that experiencing prolonged grief symptoms is significantly related to poorer mental health outcomes, including more depression and anxiety symptoms, and higher perceived loneliness. Extending past research (Grauerholz et al., 2021; Lenger et al., 2020; Nielsen et al., 2020), our results highlight that prolonged grief is also negatively associated with physical health. Hence, we advance the literature by suggesting the potential physical implications of prolonged grief and opened the door for future research efforts. Based on our current findings, future research could explore additional physical health outcomes, such as increased risk of cardiovascular disease and coronary heart disease (Hart et al., 2007; Pini et al., 2015), or metabolic disorders (Cunningham et al., 2025). Future studies could additionally investigate whether meaning in life also helps explain associations with these physical health outcomes, or even explore alternative or complementary psychological mechanisms (e.g., emotion regulation).
As expected, we also found that experiencing higher levels of prolonged grief symptoms was linked to perceiving less meaning in life (H2). These results complement other findings (Hilberdink et al., 2023; Ivers et al., 2024; Kersting & Kroker, 2010; Prigerson et al., 2009, 2021) and show that prolonged grief may be related to changes in how bereaved individuals perceive their lives (e.g., feelings of meaninglessness), and how they cope with the identity disruption caused by the death of an emotionally intimate person (e.g., feeling that a part of themselves has died). Given that less meaning in life has been associated with impairments in psychological (e.g., depression symptoms; Kleftaras & Psarra, 2012) and social functioning (e.g., feelings of loneliness; Macià et al., 2021), our findings offer empirical evidence that can be used by researchers and mental health professionals to develop not only training programs for bereaved individuals, but also awareness campaigns to the general public addressing the role of meaning in life during bereavement.
Also as expected, experiencing less meaning in life significantly explained why higher levels of prolonged grief symptoms were related to poorer mental (H3a and H3b) and physical health outcomes (H3c). Our results are aligned with recent research (Sun et al., 2022; Szcześniak et al., 2022), showing that lacking meaning in life can help explain different psychological impairments (e.g., higher anxiety, hopelessness) and depression symptoms among different cohorts (e.g., individuals diagnosed with depression). To the best of our knowledge, our study also innovated by showing that meaning in life is among the psychological mechanisms that explain why prolonged grief symptoms are linked to poorer mental and physical health outcomes among bereaved individuals. Our findings can serve as an empirical basis in more applied domains (e.g., for mental health professionals working with bereaved adults) to help improve mental and physical health while addressing the changes in the way bereaved individuals perceive their lives.
We also observed a priori differences on several risk factors. Indeed, older participants reported significantly more meaning in life, fewer depression symptoms, and lower perceived loneliness. These results are aligned with past research showing that individuals at later (vs. earlier) life stages are more likely to report more meaning in life (Steger et al., 2009), and also fewer depression symptoms (Nolen-Hoeksema & Aldao, 2011) and lower loneliness (Barreto et al., 2021). Regarding gender differences, our results complement previous research (Johnsen et al., 2012) and indicate that bereaved women (vs. men) may be at a higher risk of developing prolonged grief symptoms. Differences observed according to education are also aligned with recent findings (Mason et al., 2020), showing that bereaved individuals with fewer years of education are more likely to report higher levels of prolonged grief symptoms. Similar to past research, our results also showed that participants who reported lower socioeconomic status reported more depression symptoms (Jespersen et al., 2025) and lower perceived physical health (Kivimäki et al., 2020; Wang & Geng, 2019). These findings highlight the potential effect of certain sociodemographic characteristics (e.g., being young and a woman, having fewer years of education, perceiving lower socioeconomic status) on experiencing prolonged grief and reporting poorer mental and physical health outcomes. Moreover, we found that participants who lost close family members and close friends reported higher levels of prolonged grief symptoms compared to those who lost extended family members. Past research has shown that having a closer relationship with the deceased is also a risk factor for developing prolonged grief and experiencing general health impairments later on (Hibberd et al., 2010; Jann et al., 2024; Quadlander-Goff & Meyer, 2024; Thomas et al., 2014). Unexpectedly, no differences emerged depending on the type of death (i.e., higher levels of prolonged grief symptoms due to COVID-19-related or unnatural/sudden death; but see Boelen, 2015; Buur et al., 2024; Hardison et al., 2005). Arguably, the nonsignificant differences observed according to different types of death might be influenced by our participants’ grief experiences (i.e., our sample mostly represented grief experiences following natural causes of death, such as chronic diseases and sudden health failures). Despite the differences across multiple risk factors, our main results remained unchanged, thus attesting the robustness of our findings and the crucial role of meaning in life on grief experiences.
Limitations and Future Research
Our study has some limitations that must be discussed. First, the use of correlational data prevents us from inferring causality between our variables. We hypothesized that prolonged grief was associated with less meaning in life (see also Hilberdink et al., 2023; Ivers et al., 2024; Prigerson et al., 2021), but it might also be that individuals who perceive less meaning in life are more likely to experience higher levels of prolonged grief symptoms. Future studies could consider conducting longitudinal research to collect data from bereaved individuals using larger and more diverse samples to examine whether higher levels of prolonged grief symptoms are associated with long-term changes in the perceptions of meaning in life and experiences of mental and physical health outcomes, and whether our theoretical model is generalized to different types of grief experiences (as our findings seem to suggest). Second, we measured perceived physical health with a single item which limits the scope of our inferences. Hence, researchers could consider using different measures (e.g., eating behavior, sleep, cardiovascular health) to determine more specific changes in perceived (or actual) physical health. In addition to meaning in life, certain cognitive determinants and regulatory strategies may explain how grief experiences are related to health and well-being. For example, loss-related coping self-efficacy and emotion regulation were found to predict perceived mental and physical health (e.g., emotional distress, physical health perceptions), and explain improvements in prolonged grief symptoms (Benight et al., 2001; Brodbeck et al., 2022).
Third, we conducted a secondary data analysis using data from a larger project. This approach has several advantages particularly when working with difficult to reach populations (e.g., bereaved adults who lost an emotionally intimate person), but limits the inclusion of additional variables that could help gain a deeper knowledge of the process (e.g., self-efficacy, emotion regulation) to meet time restrictions (e.g., careful consideration of which variables are included to prevent participation burden). Future studies could address the role of cognitive processes to further understand whether these factors may buffer the negative effects of prolonged grief on less meaning in life, and poorer mental and physical health. Additionally, future research could consider assessing prolonged grief by using a cut-off score in order to compare bereaved individuals’ mental and physical health outcomes who report higher versus lower levels of prolonged grief symptoms.
Implications and Conclusion
Our findings highlight the clinical importance of assessing perceptions toward life during bereavement, alongside other risk factors for prolonged grief symptoms. Our results suggest that meaning in life should be considered when developing and testing the efficacy of therapeutic approaches to better understand how prolonged grief translates into health and well-being. These findings offer insights that can be used to develop protocols and interventions aimed at helping bereaved individuals regain a sense of coherence in life, and subsequently, experience greater mental and physical health. Furthermore, past research showed that bereaved individuals with higher levels of prolonged grief symptoms may have difficulty receiving social support from close others (Asmat et al., 2024) and experience significant changes in the way they perceive their lives (Steffen, 2019). Hence, our results suggest that fostering meaning in life among bereaved individuals is crucial and, from an applied perspective, this could be worked on in social support group sessions conducted by mental health professionals.
Footnotes
Ethical Considerations
Prior to the data collection, this study was approved by the Ethics Council at Iscte-Instituto Universitário de Lisboa (Ref.: #22/2021).
Author Contributions
Ecem Sarper: Conceptualization, Methodology, Formal Analysis, Validation, Investigation, Writing - Original Draft. Sílvia Luís: Validation, Writing - Review and Editing, Supervision. David L. Rodrigues: Conceptualization, Methodology, Validation, Investigation, Writing - Review and Editing, Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Fundação para a Ciência e a Tecnologia with a grant awarded to Ecem Sarper (Ref.: 2023.05086.BDANA), and funding awarded to Sílvia Luís (Ref: UIDB/05380/2020), and to David L. Rodrigues (Ref.: 2020.00523.CEECIND).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.