
Abstract
Induced After-Death Communication (IADC) therapy, which uses bilateral stimulation derived from EMDR, is an emerging approach to reducing grief symptoms in bereaved individuals. The present study evaluated the IADC protocol, consisting of two 90-min sessions, in 43 bereaved adults with assessments at four time points including a one-month waitlist period to provide control data. Large reductions in grief symptoms were observed from baseline to follow-up (global grief severity d = 1.56; average daily sadness d = 1.33). Two-thirds of participants who exceeded the clinical cutoff score for prolonged grief at baseline scored below this threshold at follow-up. Treatment effects were comparable across delivery methods (in-person vs. online) and were not moderated by time since loss or baseline symptom severity. After-death communications occurred in 79% of participants during therapy and predicted stronger continuing bonds with the deceased. These findings support IADC as an efficient treatment option for bereaved individuals.
Grief is a ubiquitous human experience associated with significant psychological impacts, including depression, anxiety, and loneliness, as well as disturbances in sleep and physical health (Stroebe et al., 2007). However, non-specific grief counselling, when routinely offered to bereaved people, has demonstrated limited efficacy (Neimeyer & Currier, 2009). Additionally, up to 10% of grieving individuals experience prolonged or ‘complicated’ grief with commensurate impairment in functioning and quality of life (Lundorff et al., 2017). The need for more effective approaches to assist grieving individuals is therefore a public health imperative.
Induced After-Death Communication (IADC) therapy is a derivative of eye-movement desensitisation and reprocessing (EMDR), utilizing bilateral stimulation to process the sadness associated with grief and loss. As in EMDR, it is hypothesised that bilateral stimulation (BLS) through eye movements (or tapping) facilitates the emotional processing of grief-related distress. However, IADC differs from EMDR in that it is briefer than standard EMDR protocols (Shapiro, 2018), does not interrupt processing in the case of intense distress, and has clients close their eyes between sets of eye movements. The primary therapeutic mechanism of IADC is in using BLS to reduce the intensity of grief-related sadness, however IADC also recognises that the resulting state of reduced sadness is associated with the experience of after-death communications, although the precise psychological or neurobiological mechanisms remain speculative. The client does not need to have an after-death communication to receive the benefit of the therapy, although it is proposed that these experiences may yield further therapeutic benefits (Botkin, 2000; Valdez et al., 2021).
An after-death communication (ADC) is the experience of perceiving the presence of a deceased person in some way. ADCs are subjective and usually internal sensory experiences such as seeing an image of the deceased in one’s mind’s eye, or perceiving the deceased’s voice, and even tactile sensations such as a sense of being touched or hugged, for example (Botkin, 2000, 2014; Valdez et al., 2021). ADCs are common in the general population, with rates reported between 30% and 85%, with higher rates reported among the recently bereaved (Streit-Horn et al., 2022). ADCs are usually considered by experiencers to be benign or comforting and are associated with enhanced adjustment to bereavement (Penberthy et al., 2023). There are no known reported cases of distressing ADCs in IADC therapy, however spontaneous ADCs can be distressing for a small minority of experiencers (e.g., 4.6% of widowed adults in a Danish survey sample (Kamp et al., 2024)). Some researchers have used the term sensory experiences of the deceased (SED) to describe the phenomenon of ADCs (Kamp et al., 2024). Despite being recognized as a common and non-pathological part of the grieving process, the DSM-5-TR refers to ADCs as “hallucinations” (American Psychiatric Association, 2022). Some researchers have questioned the helpfulness of this language as it implies pathology (Exline, 2021). This is of clinical importance as evidence suggests the acceptance and validation of experiences such as ADCs by mental health professionals is predictive of client adjustment (Beischel, 2019; Makikomsi et al., 2024). The frequency of ADC experiences within IADC therapy is estimated to be approximately 75% (Botkin & Hannah, 2013; Hannah et al., 2013).
Early evidence suggests IADC therapy may be superior to traditional grief counselling. Holden and colleagues (2019) conducted an experimental pre/post study comparing IADC therapy to traditional grief counseling (TGC) among 41 bereaved adults (Holden et al., 2019). TGC included assisting the client to express their feelings, make meaning from the loss, and address the tasks of coping with grief. Results showed that IADC clients had significantly greater reductions in overall grief symptoms (e.g., I feel a heaviness in my heart; I have difficulty concentrating), compared to TGC clients, with a large effect size as measured by the Hogan Grief Reaction Checklist (Hogan et al., 2001). When examining the six Hogan subscales individually, the IADC group showed significantly greater improvement on one subscale (blame and anger) and nonsignificant improvement on the other five (despair, panic behavior, personal growth, detachment, and disorganization), with effect sizes ranging from medium to small. Importantly, most participants did not meet criteria for prolonged grief disorder, suggesting IADC may be effective for a broad range of bereaved individuals, not just those with severe or complicated grief. These promising initial findings warrant further research into the efficacy, mechanisms, and scope of IADC therapy.
A recent Italian observational cohort study (D’Antoni et al., 2025) similarly reported significant improvements in grief and distress on the Inventory of Complicated Grief (Prigerson et al., 1995) following IADC therapy compared to standard grief interventions. Although encouraging, the study’s observational design, lack of randomisation, and variability in the comparison treatments limit the strength of conclusions that can be drawn. Nevertheless, their findings add preliminary support to IADC’s efficacy and highlight the need for more rigorously controlled research. The studies by Holden and colleagues (Holden et al., 2019) and D’Antoni and colleagues (D’Antoni et al., 2025) are the only two to date that have evaluated IADC therapy in comparison with a control condition.
The present study sought to build on the existing research evaluating the efficacy of IADC therapy for reducing the sadness and grief symptoms following bereavement. We hypothesized that participants’ grief and sadness would be significantly reduced following IADC therapy, and that the experience of an ADC during therapy would be associated with additional benefits. Given the growing popularity of telehealth interventions (Greenwood et al., 2022) and varying experiences of grief severity over time (Pociunaite et al., 2023), we sought to determine whether therapy efficacy varied according to delivery method (in-person vs. online), time since bereavement, or baseline grief severity.
Method
The present study utilised a single-group wait-list control design whereby participants would be assessed over a one-month waiting period prior to the intervention (Time 1 to Time 2). This design would establish a baseline level of grief symptoms, to be compared with data collected at one-month follow-up (Time 4). Some data regarding immediate response to therapy, including acceptability and occurrence of ADCs were assessed immediately posttreatment (Time 3). Ethical approval was granted by Human Research Ethics Committee of the Adelaide University (Approval #H-2023-207). Informed consent was obtained via signed consent forms after all participants had read and understood the approved participant information sheet. All data, including demographics and questionnaires, were collected using Qualtrics survey links and stored on secure university servers, with datasets anonymised prior to analysis with SPSS using one-way repeated measures ANOVAs.
Participants
Participants were 45 English-speaking bereaved adults (41 female) ranging in age from 28 to 73 years (M = 51.51, SD = 10.42) living in Australia, seeking assistance for their grief: to lessen emotional distress, alleviate grief symptoms, and facilitate adjustment to the loss. Recruitment occurred via various online channels including a university research participation website and the social media channels of a major grief services organisation. None of the participants had prior contact with the researchers. Participants predominantly (n = 42, 93.3%) reported losses of a spouse or immediate family member, compared to friend, extended family, or grandparent, with just over half (n = 25, 55.6%) occurring 1-5 years prior to therapy (n = 9, 20% experienced losses less than 12 months prior to therapy and n = 11, 24.4% more than 5 years prior to therapy). Baseline grief severity as reported on the International Prolonged Grief Disorder Scale (Killikelly et al., 2020) ranged widely, indicating both moderate and clinically significant grief. Inclusion criteria were English-speaking adults who were bereaved and seeking assistance for grief. Interested participants then undertook a screening interview with the first author to determine suitability for admission to the study. Participants were then excluded if they were suicidal, if it had been less than six months since the loss, and if they were unwilling or unable to tolerate high levels of emotional distress. The protocol specifies that a minimum of six months since the loss is required to ensure the individual has likely passed through any short-term coping processes (e.g., shock, denial or numbing) and into a more stable grief profile appropriate for a structured intervention (Valdez et al., 2021).
Two participants withdrew from the study following commencement, one due to travelling overseas and the other due to psychoactive medications inhibiting the accessing and processing of sadness. No participants otherwise withdrew their data following commencement. All participants were free to withdraw at any time, and were offered a debrief with the first author at the conclusion of the study.
Primary Measures
International Prolonged Grief Disorder Scale
The International Prolonged Grief Disorder Scale (IPGDS; Killikelly et al., 2020) is a 15-item self-report measure of grief severity and prolonged grief disorder. It has demonstrated strong reliability and validity across different cultural contexts and is often used to operationalize prolonged grief disorder (PGD) in clinical and research settings.
Average Daily Sadness
Participants were asked to rate their average daily sadness on a scale of zero (not at all sad) to ten (as sad as I’ve ever felt), as a means of assessing subjective self-reported sadness, a crucial affective marker of grief.
Secondary Measures
DASS-21
Depression, anxiety, and stress was measured using the 21-item version of the Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995a; Lovibond & Lovibond, 1995b). For each item, participants are asked to rate how much a particular statement applied to them over the past week on a four-point scale from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time). A total subscale score or mean may be derived, where higher scores indicate higher levels of impairment. The DASS-21 has demonstrated strong psychometric properties in a large adult sample (Crawford & Henry, 2003).
Hogan Grief Reaction Checklist
The Hogan Grief Reaction Checklist (HGRC; Hogan et al., 2001). is a 61-item self-report measure designed to assess multiple dimensions of grief, developed from empirical data collected from bereaved individuals. The HGRC includes six factors that represent key aspects of the grief process: Despair, Panic Behavior, Blame and Anger, Detachment, Disorganization, and Personal Growth. It has been shown to have strong reliability and validity, and it is often used in research to capture the emotional and psychological responses to bereavement over time (Hogan et al., 2001).
Ongoing Attachment Inventory – Continuing Presence Subscale
The Ongoing Attachment Inventory (OAI) is a measure designed to assess the extent to which individuals maintain an emotional attachment to a deceased loved one (Hogan et al., 2014). It evaluates the presence of ongoing bonds that persist after the physical loss, reflecting how individuals continue to experience their relationship with the deceased. The Continuing Presence (CP) subscale of the OAI includes ten items specifically to assesses the degree to which individuals feel the ongoing presence of the deceased in their daily lives. It reflects perceptions that the deceased is still emotionally or spiritually close. It was selected for inclusion in the present study as a means of capturing the potential ongoing effects of ADCs on continuing bonds with the deceased. This is distinct from ADCs themselves.
After-Death Communications
The occurrence of ADCs was measured by subjective self-report in response to the following: “During the course of your IADC Therapy (during the sessions or in-between sessions), did you experience or perceive the presence of your deceased loved one in some way OR a distinct emotional experience that you attribute to your deceased loved one?” This item was developed to align closely with descriptions of after-death communication experiences reported in prior empirical and phenomenological research (e.g., Guggenheim & Guggenheim, 1995; Steffen & Coyle, 2011), and reflects the phrasing typically used in IADC therapy protocols to capture both perceptual and affective experiences attributed to the deceased.
Intervention - IADC Therapy
The intervention was delivered by the first and second authors, both experienced clinical psychologists (PhD; MClinPsych) with more than 15 years of experience working with bereaved clients, in private practice settings (in person and via telehealth). The IADC therapy protocol developed by Botkin (2000, 2014) was utilised by both Holden et al. (2019) and D’Antonio et al. (2025) and was applied in the current study. It first involves an assessment of the saddest parts of the client’s current experience of grief. That is, the client and therapist collaboratively identify the strongest ‘pieces of sadness’ – those memories, events, or cognitions that are associated with the strongest intensity of affect. The administration of BLS then occurs by targeting the ‘worst first’: repeated sets of eye movement or bilateral tapping (for example, the therapist tapping the back of the clients hands which rest on their upper legs, or the client self-tapping alternate shoulders with their arms crossed over their chest in a ‘butterfly hug’ position) while the client attends to the saddest aspects of their bereavement. Over repeated sets of BLS, the intensity of affect reduces until the client’s self-reported subjective units of distress (SUDs) are greatly reduced or zero. Over two ninety-minute sessions (usually on consecutive days), the therapeutic protocol directs the therapist to process as much sadness as possible, and to continue BLS if or when the client experiences a complete reduction in sadness and/or experiences positive emotions. By continuing BLS, clients commonly report further increases in positive feelings such as calm or peacefulness. It is expected that some clients during this latter phase will experience an ADC. These ADCs may take the form of subjective visual, auditory, olfactory or tactile sensations associated with the deceased; or a subjective sense of presence usually associated with strong positive emotions. The protocol then directs the therapist to assist the client in making meaning of their experience and invites the client to ask any questions they may have.
Eighteen participants (41.9%) received the therapy in person, while the remaining completers (n = 25, 58.1%) were seen online.
Acceptability
Thirty participants (69%) had previously sought treatment for grief prior to enrolling in the study. Following IADC therapy, participants were asked how likely they would be to recommend the therapy to others on a scale from zero (not likely) to ten (very likely), with a mean result of 9.56 (SD = .881). Forty-two (97.7%) reported that they felt “lighter, less sad, or better able to move forward as a result of IADC therapy”.
Data Analysis
Given the design used, to test the treatment effect, we wished to test whether there was a significant change from baseline to post-treatment. To do so, we ran one-way repeated measures ANOVAs using difference (reverse Helmert) contrasts. These contrasts test whether the mean at each time point is different from the average of all preceding time points. So, this leads to the following two contrasts: (a) T2 (baseline) versus T1 (baseline), and (b) T4 (one-month post-treatment) versus the average of the two baseline measurements. The first contrast tests whether scores are stable over time on the measure during the baseline period. The second contrast, the critical one, compares post-treatment scores against the average scores across the baseline period (which is a better estimate of the baseline score than just taking the Time 2 score). For all our effect size measures, we use a variant of Cohen’s d; where we use the pooled standard deviation of the two baseline measures as our index of the population standard deviation. This measure is uncontaminated by the treatment and also ensures a common denominator in all comparisons for any particular measure.
We also tested moderators of the treatment effect using the same strategy as described above. We repeated the initial analyses (with associated contrasts) to test for the effects of four moderators: (a) delivery method (in-person, via Zoom), (b) time since loss, (c) occurrence of an after-death communication (ADC), and (d) baseline global grief severity. Each moderator was included one at a time, as either a between-subjects factor (delivery method, ADC) or as a covariate (time since loss, baseline global grief severity). For all these analyses, we focussed on the interactions associated with Contrast 2 (average baseline versus one-month post-treatment).
Results
Testing the Treatment Effect
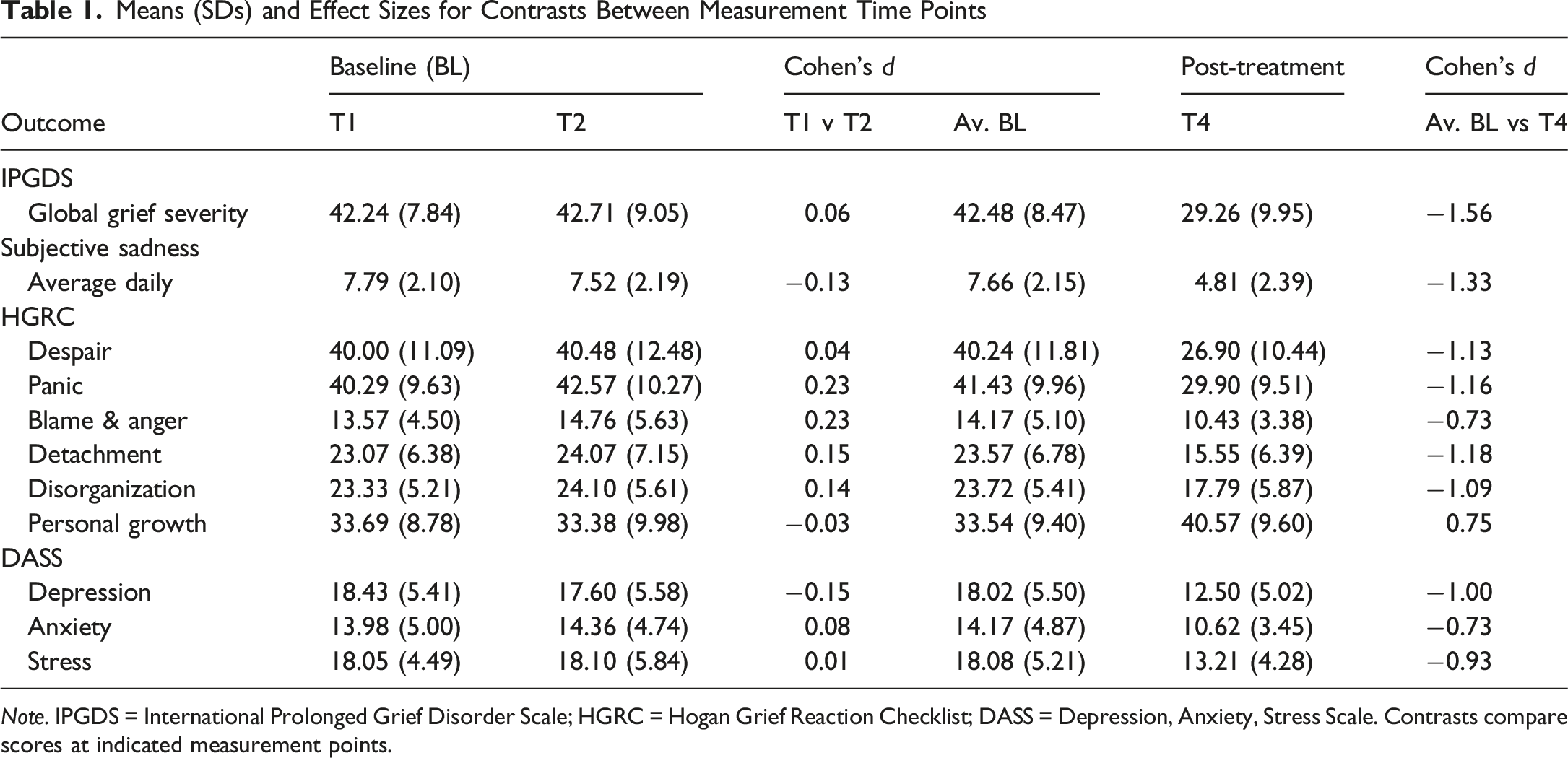
Means (SDs) and Effect Sizes for Contrasts Between Measurement Time Points
Note. IPGDS = International Prolonged Grief Disorder Scale; HGRC = Hogan Grief Reaction Checklist; DASS = Depression, Anxiety, Stress Scale. Contrasts compare scores at indicated measurement points.
ANOVA Results for Planned Contrasts for Change During the Baseline Period and for Change From Baseline to Post-treatment

Note. IPGDS = International Prolonged Grief Disorder Scale; HGRC = Hogan Grief Reaction Checklist; DASS = Depression, Anxiety, Stress Scale. Contrasts compare scores at indicated measurement points.
For all dependent variables, virtually the same pattern of effects was observed in the baseline period. For all but two of our measures, we found no significant difference between scores during the baseline period (i.e., Time 1 and Time 2), Cohen’s d all less than 0.21, reflecting stability during the waitlist control period and confirming that the baseline provided a reliable comparison point for detecting treatment effects at follow up. For the panic and the blame and anger subscales of the HGRC, we found significant results, both with p = .041 but, in each case, we found a very small increase of less than one-quarter of a standard deviation, d = 0.23 in both cases.
In contrast, for our two primary outcome measures, global grief severity and average daily sadness, we found significant decreases between baseline and one-month post-treatment with very large effects for both measures, Cohen’s d were 1.56 (global grief) and 1.33 (average daily sadness).
Similar patterns were observed for all of the HGRC subscales with large improvements observed on all subscales (Cohen’s d values ranged between 0.73 and 1.16). Likewise, on all three subscales of the DASS, large improvements were also observed (Cohen’s d values ranged between 0.73 and 1.00).
Given the similar findings across all our outcome measures we examined a summary of the correlations which showed that in general, for all the variables, there were significant correlations between the outcome measures at all time points in the study. All our secondary outcome measures were significantly correlated with both global grief (r between .35 and .88 at baseline; between .52 and .92 post-treatment) and average daily sadness (r between .25 and .66 at baseline; between .32 and .67 post-treatment).
Clinical Significance of the Treatment Effect
We considered the clinical significance of the treatment effect using the putative caseness (“diagnosis”) score obtained from the IPGDS. Of the 43 patients, 9 (20.9%) had a “diagnosis” pre-treatment (at Time 2). This reduced to only 3 (7.0%) at one-month post-treatment (at Time 4); a reduction of two-thirds in “diagnosed” cases. A McNemar non-parametric test for change in related samples showed that this reduction was significant, χ2 (1) = 4.17, p = .041.
Investigating the Role of Delivery Method, Time Since Loss, and Pre-treatment Global Grief on the Treatment Effect
Considering that the outcomes measures were generally highly correlated, our moderation analyses focussed only on our two primary outcomes. In general, there was no evidence supporting a difference in improvements following treatment between the two delivery methods (in-person or via Zoom). The Contrast 2 by delivery method interaction was not significant for either global grief severity, F (1.40) = 1.28, p = .26, or average daily sadness, F (1.40) = 0.51, p = .48.
The same patterns were observed when we tested whether the treatment effects were moderated by time since loss. For both analyses, the relevant Contrast 2 by time since loss interaction was not significant: for global grief severity, F (1.40) = 2.17, p = .15, and for average daily sadness, F (1.40) = 0.00, p = .99.
Likewise, when looking at the moderating role of average baseline global grief severity, the relevant Contrast 2 by pre-treatment global grief interaction was not significant for global grief severity, F (1.40) = 2.20, p = .12. Taken together with the previous finding, this shows a large decrease in global grief severity following treatment, d = −1.56, irrespective of initial global grief severity. For average daily sadness, the relevant Contrast 2 by pre-treatment global grief interaction did not reach significance, F (1.40) = 2.96, p = .067.
Looking at the estimated means for high baseline global grief severity (i.e., one SD above the mean) and low baseline global grief severity (i.e., one SD below the mean), very large effects were found for both, albeit marginally stronger for high baseline grief severity; at high baseline global grief, est. baseline M = 8.97, est. post-treatment M = 5.68, d = 1.53 versus at low baseline global grief, est. baseline M = 5.97, est. post-treatment M = 3.78, d = 1.02.
Investigating the Role of an Occurrence of an “After Death Communication” (ADC) and Continuing Presence
ADC occurrence was recorded immediately post-treatment via reporting of participants’ subjective experiences. Occurrence of an ADC did not significantly moderate the treatment effect for either primary outcome (global grief severity, F (1.40) = 1.48. p = .23; average daily sadness, F (1.40) = 0.05. p = .81). However, of the 43 participants, 34 (79.0%) had experienced an ADC during therapy. Because there were only nine participants who did not experience an ADC during therapy, the statistical power of the tests was low.
However, despite the low statistical power of the test, we did find that those who had experienced an ADC (M = 44.77. SD = 6.94) had significantly higher scores at Time 4 on the Continuing Presence subscale (of the OAI) than those who had not experienced an ADC (M = 38.75. SD = 9.50), t (41) = 2.07, p = .045, Cohen’s d = 0.81.
Finally, we found that continuing presence was significantly correlated with average daily sadness at baseline (r = .45, p = .002) but not at one-month post-treatment (r = .04, p = .79). On the other hand, continuing presence was not significantly correlated with global grief severity at either baseline (r = .19, p = .23) nor one-month post-treatment (r = −.02, p = .88).
Discussion
The present study achieved its aims of assessing whether grief and sadness were significantly reduced following IADC therapy, whether the occurrence of an ADC was associated with additional benefits, and whether outcomes differed based on mode of delivery (in-person or online). Large reductions in grief symptoms and sadness were observed, and those participants who had an ADC reported a stronger continuing presence of the deceased at one-month follow-up. Therapeutic outcomes were comparable regardless of delivery method.
The observed therapeutic effects provide further support for Holden et al. (2019) and D’Antoni et al.’s (2025) findings and suggest IADC therapy represents a promising therapeutic option for grief which merits consideration alongside established interventions. These findings are of notable clinical significance given two thirds of cases of prolonged grief disorder no longer met clinical cutoff at follow-up. The magnitude of effects also supports the clinical significance of the intervention. The effect size on global grief severity in the present study (d = 1.56) compares favourably to reported effect sizes in reviews of other common psychotherapies e.g., Cognitive Behavioural Therapy for depression (CBT) d = 0.71; Cuijpers et al. 2013, CBT for anxiety disorders (d = 0.84; Norton & Price, 2007), Interpersonal Psychotherapy for depression (d = 0.63; Cuijpers et al., 2011), and EMDR for PTSD (g = 0.66; Chen et al., 2014). Compared to targeted grief interventions, where meta-analyses typically report effect sizes ranging from d = 0.53 immediately post-intervention to d = 1.38 at follow-up (Wittouck et al., 2011), the current findings suggest particularly robust therapeutic effects.
Not only is IADC therapy clinically efficacious, as a two-session intervention it is also very efficient. This contrasts with other grief interventions which typically require many more sessions (e.g., complicated grief treatment which is 16 sessions; Shear et al., 2016). It also appears to be versatile. Large reductions in grief and sadness were observed regardless of the baseline severity, suggesting IADC therapy may be suitable for both severe and moderate grief. Furthermore, effects were comparable for both in-person or Zoom delivery. Time since loss also did not moderate the outcome. The occurrence of ADCs was not associated with greater improvements on the primary outcome measures; however, this analysis was underpowered and therefore should be interpreted with caution.
Consistent with the purported therapeutic mechanisms of IADC, reductions in sadness were not dependent on the occurrence of an ADC. As in EMDR, the bilateral stimulation reliably reduces emotional distress. However, having an ADC resulted in a stronger sense of the continuing presence of the deceased, which represents a secondary and additional therapeutic effect. This is consistent with research indicating that maintaining an ongoing internalised bond with the deceased can foster comfort, continuity, and meaning reconstruction in bereavement (Klass et al., 1996; Neimeyer et al., 2006).
Prior to treatment, a sense of the deceased’s continuing presence was associated with feeling sad whereas after treatment it was not, which is consistent with the intent and reported phenomenology of IADC therapy (Botkin, 2000; Holden et al., 2019). Neimeyer and colleagues (Neimeyer et al., 2006) emphasised the shift in grief therapy from accepting the loss of the deceased to maintaining ongoing bonds. They suggested that ongoing bonds with the deceased assists in meaning making following a loss and can be associated with improved adjustment throughout the bereavement process. By inducing ADCs in grief therapy, IADC can assist in enhancing a sense of continuing presence, whereby the bereaved’s ongoing attachment to the deceased is no longer associated with sadness. Rather, the continuing presence of the deceased is consistently reported to be associated with feelings of love, gratitude, peace and acceptance (Botkin, 2014; Valdez et al., 2021).
Given the prevalence and associated burden of prolonged grief worldwide (Comtesse et al., 2024; Hilberdink et al., 2023; Rosner et al., 2021), the wider dissemination of IADC therapy represents a significant public health opportunity.
Limitations and Recommendations for Future Research
A limitation of the present study included the lack of an active control condition, which means we cannot rule out that non-specific factors (such as therapeutic alliance and expectancy effects) may have contributed to the observed improvements. Research in psychotherapy more broadly indicates that these common factors account for a substantial proportion of outcome variance across modalities (Flückiger et al., 2018; Sparks & Duncan, 2016). While the wait-list control design allowed us to control for the effects of time and spontaneous recovery, future research would benefit from comparing IADC therapy to established grief interventions such as Complicated Grief Therapy or EMDR to determine relative efficacy. Such comparisons would also help isolate the specific therapeutic mechanisms underlying IADC’s effectiveness. Due to the small number of participants meeting diagnostic criteria at baseline (n = 9), interpretation of clinical significance should be viewed cautiously, although large effect sizes were robust across the sample.
A strength of this study is that it represents the third controlled evaluation of IADC therapy and the first to test both in-person and telehealth delivery.
Future research into IADC therapy should utilize larger samples with more male participants and randomization to active control conditions. This would enable a more granular analysis of predictors of response to therapy, would clarify whether ADCs are associated with greater improvements, and help refine clinical guidelines.
One of the identified priorities for grief research is the prevention of complicated/prolonged grief (Hay et al., 2021). Given the significant psychological, social, and physical health consequences of prolonged grief, including elevated risks of depression, suicidality, and functional impairment (Prigerson et al., 2021; Rosner et al., 2021), the efficiency and efficacy of IADC therapy make it a promising candidate for such a study.
Conclusion
These findings collectively suggest that IADC therapy is an efficacious and efficient intervention for reducing grief symptoms, daily sadness, and depressive symptoms in individuals experiencing prolonged grief, with high acceptability. The large effect sizes observed, coupled with improvements across various dimensions of grief and a substantial reduction in PGD caseness, underscore the clinical significance of these results. Further research with larger sample sizes is recommended.
Footnotes
Ethical Consideration
Ethical approval for the trial was granted by the Human Research Ethics Committee of the Adelaide University (Approval #H-2023-207) and registered with the ISRCTN Registry (#ISRCTN10485391).
Consent to Participate
All participants provided informed consent.
Funding
TThe authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
TN and JD receive fees for conducting IADC therapy as part of their respective clinical practices, however no fees were received for work relating to this study.