
Abstract
Introduction
Perinatal loss is common, affecting approximately 23 million women and families worldwide each year (Quenby et al., 2021). Specifically, 14 to 20% of pregnancies end in miscarriage, and 2.6 million fetal deaths occur annually (Lancet, 2016). There is no consensus in the literature on the definition of perinatal loss, but the most comprehensive definition includes situations involving loss during pregnancy, childbirth, or after childbirth. These situations include spontaneous abortion (loss occurring within the uterus before the 20th week of pregnancy), fetal death or stillbirth (death occurring after the 20th week of pregnancy or during childbirth), neonatal death (loss occurring within the first 28 days of life), and medical and/or voluntary termination of pregnancy (Public Health Agency of Canada, 2000).
Perinatal loss is a potentially traumatic event that affects the mental health of those who experience it, including women, men, and couples. Several studies have demonstrated an association between perinatal loss and depressive symptoms (Herbert et al., 2022). Gold et al. (2016) found depressive symptoms nine months after loss, and Mendes et al. (2023) found high levels of depressive symptoms one month after early pregnancy loss in Portuguese women. In addition to the psychological impact of perinatal loss, women may experience feelings of responsibility or guilt following the event (Bardos et al., 2015).
Guilt is characterized as a painful emotional experience associated with one or more behaviors (Stroebe et al., 2014). According to Hill et al. (2016), experiencing guilt during the grieving process after perinatal loss can lead to a loss of self-esteem due to the perceived failure of women in their maternal role. Additionally, guilt may arise regarding potential causes of loss. Women may feel responsible for actions they took during pregnancy, such as alcohol consumption, excessive exercise, or working too much, or for things they did not do that may have led to the loss (Omar et al., 2019).
Existing literature has identified self-compassion as a protective factor against psychological disturbances, depressive symptoms and guilt (Akin & Akin, 2015; Barnard & Curry, 2011). It is defined as the ability to be kind to oneself in difficult situations, such as failure, and to be open, attentive and sensitive to one’s own suffering (Neff, 2023). It implies an attitude of non-judgement and non-avoidance of these experiences, instead embracing an attitude of understanding and acceptance of one’s limitations, imperfections and difficulties (Neff, 2023). This ability enables one to contextualise adversity as part of the common human experience, recognising that others act and suffer similarly (Castilho & Gouveia, 2011).
Neff (2016) defines self-compassion as a dynamic construct comprising distinct elements that influence each other in order to alleviate suffering. These elements are organised into three domains: emotional response to suffering (kindness versus self-judgement); cognitive understanding of the situation (common humanity versus isolation); and how individuals engage with suffering (mindfulness versus over-identification). A study by Leary et al. (2007) found that higher levels of self-compassion can protect individuals from negative feelings when adverse events occur. Furthermore, Neff (2023) revealed that increasing the capacity for self-compassion leads to a reduction in depression, feelings of shame and inferiority, and submissive behaviour towards others.
Although the literature has investigated the impact of perinatal loss on the mental health of those who experience it, studies on this topic are limited in Portugal. Much of the existing research focuses only on specific types of perinatal loss, such as gestational losses, and excludes losses that occur later in pregnancy or during the neonatal period. Furthermore, virtually no research has been found that assesses the protective role of self-compassion in women who have experienced perinatal loss. In this sense, the usefulness and innovation of the present study are evident. The objective of this study was therefore to assess levels of guilt, depressive symptoms and self-compassion in the sample depending on when the perinatal loss occurred, as well as investigating the relationships between these variables and the mediating effect of self-compassion on guilt and depressive symptoms in women who have experienced perinatal loss.
Methods and Materials
Participants
In the present study, a convenience sample of 501 Portuguese female participants was used from the 545 respondents to the questionnaire. With regard to the sample, adult women who had experienced perinatal loss were eligible to complete the questionnaire if they met the following inclusion criteria: (1) having suffered a perinatal loss, (2) being ≥18 years old, (3) being a woman and (4) being of portuguese nationality. Participants were not eligible if they were (1) of a nationality other than portuguese, (2) male and (3) over 49 years old (decline in fertility) (Kocourková et al., 2015; PORDATA, 2023).
The mean age of the participants was 34 years (standard deviation = 4.77), ranging from 21 to 47 years. Most participants were married, had an average socioeconomic status and lived in a large city. On average, the sample had experienced 2.31 pregnancies and 1.52 pregnancy losses, with the majority of losses occurring in 2023 (46.3%). Of these, 63.1% were early miscarriages occurring before 12 weeks of pregnancy.
Procedures
This study was previously assessed and authorised by the Ethics Committee of the University of Beira Interior (CE-UBI-Pj-2022-066). The present study was conducted using an online questionnaire distributed between June 2023 and June 2024. The questionnaire, which was created using Microsoft Forms, was made accessible via a link that was disseminated through associations and projects supporting parents who had suffered perinatal loss, via social media, and in person at the Cova da Beira University Hospital Center. The questionnaire began with a brief explanation of the research and its objectives, followed by sociodemographic and clinical questions relating to the period of pregnancy and perinatal loss. Specific assessment scales for the variables under study were also used. Participation was voluntary and anonymous, and all participants provided informed consent.
Instruments
The Self-Compassion Scale (SELFCS; Neff, 2023; portuguese version by Castilho & Pinto-Gouveia, 2015) is a 26-item measure of self-compassion rated on a 5-point Likert scale. In this article, only the positive dimension of self-compassion was used in the present study, comprising self-kindness, common humanity, and mindfulness. This decision was guided by previous research (e.g. Maagh et al., 2023; Shamsababdi & Dehshiri, 2024) indicating that these positive components are particularly relevant for reducing guilt and depressive symptoms, and function as protective psychological resources. Furthermore, using the positive dimension allows for a clearer assessment of the mediating role of adaptive self-compassion, without potential conceptual overlap with the negative components, which are more closely related to self-criticism and rumination. This dimension presented an internal consistency level of α = .92.
To assess recent psychopathological symptoms, participants responded to the portuguese version of the 18-item Barrowman Symptom Inventory (BSI-18). This instrument consists of 18 items and aims to screen for psychological distress across three subscales: depression, anxiety, and somatisation. Participants were asked to rate the intensity (from 0, none, to 4, extreme) with which they had experienced 18 manifestations of psychopathological symptoms in the previous seven days (Canavarro et al., 2017). In the present study, the internal consistency of the inventory was α = .88.
The Personal Attitudes Questionnaire – Shame and Guilt Scale was developed by Harder & Greenwald, 1999, and was translated and adapted into Portuguese by Geada in 2003. Consisting of 22 items, it uses a Likert scale ranging from 0 (Never Feel) to 4 (Feel Always or Almost Always). The total score is obtained by summing the results of the items representing guilt and shame. In the present study, only the guilt scale was used, which had an internal consistency of α = .72.
Analyses
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software (version 29.1). The Mann–Whitney test was used to compare two groups of participants based on how long ago their most recent perinatal loss occurred: those whose loss occurred less than two years ago, and those whose loss occurred more than two years ago. Spearman’s correlation coefficients were used to analyse the relationships between depressive symptoms, feelings of guilt and the positive aspects of self-compassion (self-kindness, common humanity and mindfulness). Additionally, a simple mediation model (Model 4) was employed using the PROCESS macro for SPSS (Hayes, 2013) to evaluate the mediating impact of self-compassion on the relationship between feelings of guilt and depressive symptoms. The significance of the indirect effect was tested using 5000 bootstrap samples and 95% bias-corrected confidence intervals. Normality tests were applied and obtained a p-value <.05, indicating that the study data did not come from a normally distributed population. Missing data were handled using pairwise deletion, allowing all available data to be used in each analysis.
Results
In terms of sociodemographic data, the participants’ ages ranged from 21 to 47 years (mean = 34.00, standard deviation = 4.77; n = 501), and they were all Portuguese nationals. Most were married (49.9%, n = 250) or in a civil partnership (42.1%, n = 211), while 7% were single. 75.4% of participants had attended higher education institutions, 95.6% were in employment, 57.3% had an average socioeconomic status and 41.5% lived in a large city.
In terms of clinical characteristics, the results showed that the majority of participants (67.1%, n = 336) had experienced only one perinatal loss prior to participating in this study, the majority of which were early miscarriages (63.1%, n = 316). The majority of perinatal losses in the sample occurred in 2023 (46.3%, n = 232), with 29.7% reporting that they did not know the cause of their loss. Additionally, participants reported receiving some form of support, whether psychological or psychiatric (34.5%; n = 173).
Descriptive Statistics: Alphas, Means, Standard Deviations of the BSI-18 – Depression Scale, the QAP – Guilt Scale, and the SELFCS – Positive Dimension and Respective Subscales
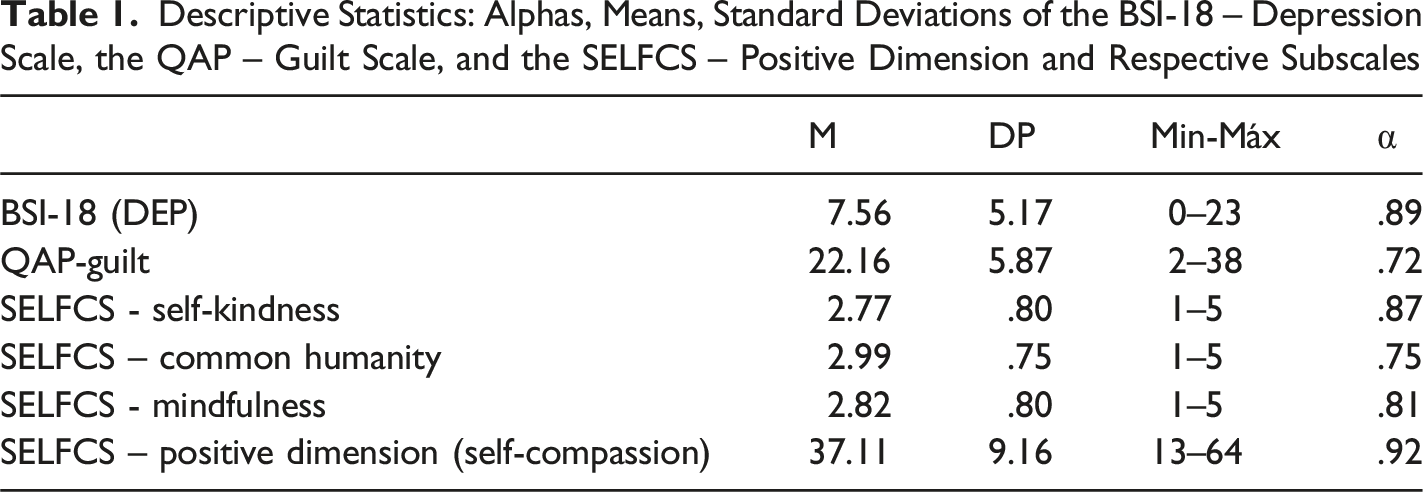
We analysed whether women who had experienced a perinatal loss within the last two years felt more guilt, exhibited more depressive symptoms and had lower self-compassion levels than women whose last perinatal loss occurred more than two years ago. With regard to self-compassion and feelings of guilt, however, there were no statistically significant differences based on the time elapsed since the last perinatal loss (t (499) = −.151, p = .349; U = 21,035.50, p = .219). However, significant differences were found between women who had their last perinatal loss less than two years ago and those who had their last loss more than two years ago in terms of depressive symptoms (U = 19,462.50, p = .018). Therefore, women who had experienced perinatal loss within the last two years reported higher levels of depressive symptoms than women whose last loss occurred more than two years ago.
Spearman Correlation Between Guilt, Depressive Symptoms, and Positive Dimension of the Self-Compassion Scale
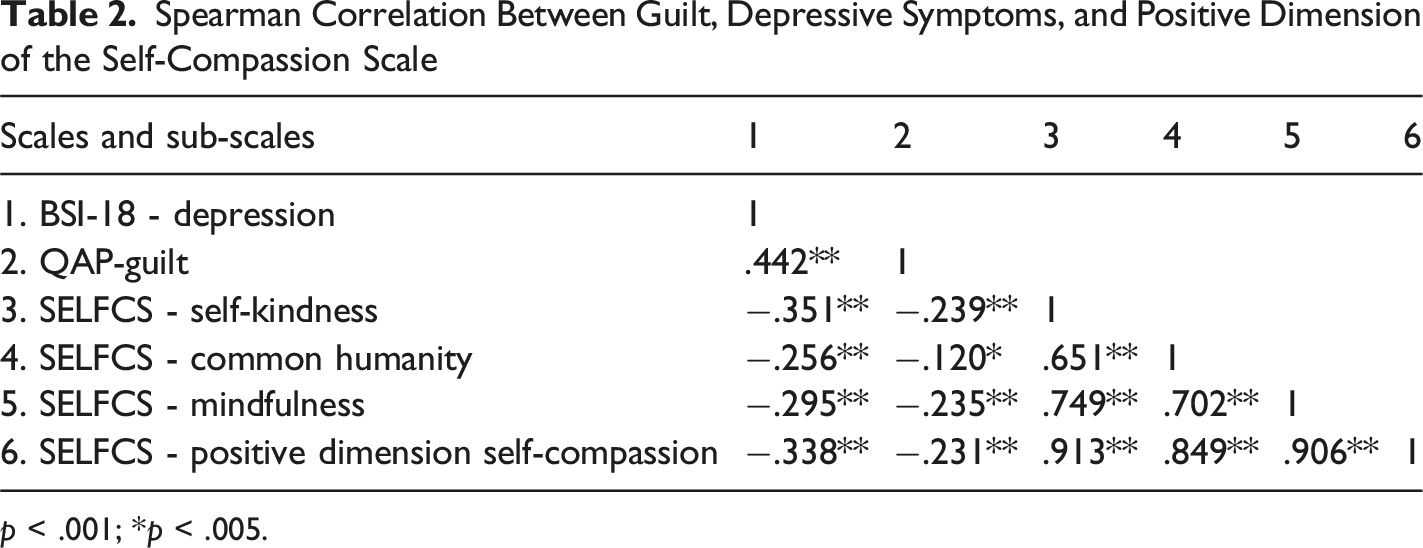
p < .001; *p < .005.
Summary of the Direct, Indirect, and Total Effects of the Simple Mediation Model
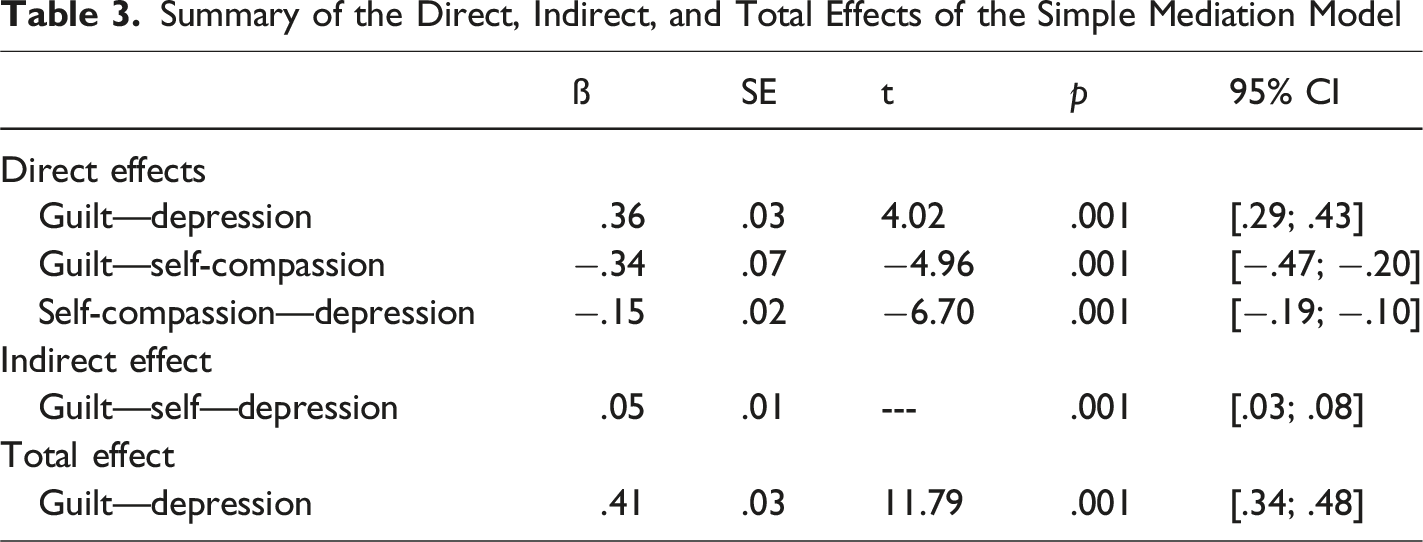
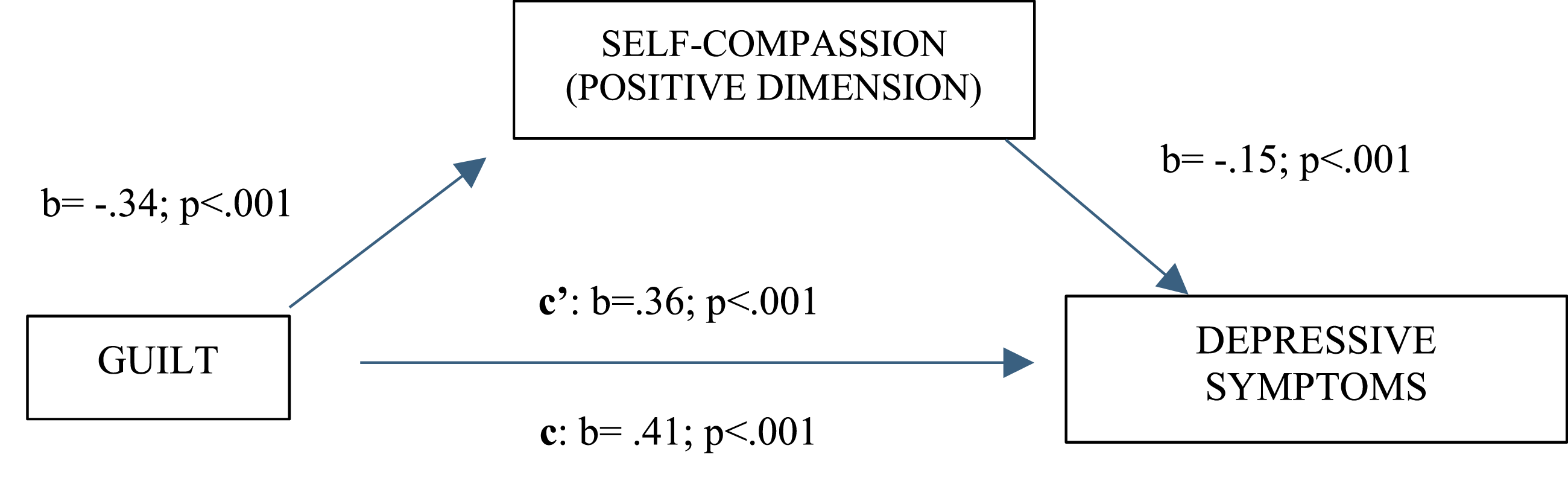
Testing the mediating effect of self-compassion on the relationship between feelings of guilt and depressive symptoms
Discussion
This study aimed to assess levels of guilt, depressive symptoms and self-compassion in portuguese women who had experienced perinatal loss, depending on when the loss occurred. The study also investigated the mediating effect of self-compassion on guilt and depressive symptoms. Of particular note, this study is one of the first to explore the mediating role of self-compassion in the association between guilt and depressive symptoms within a Portuguese population. This provides valuable insights into how cultural context can influence emotional responses to perinatal loss.
As expected, self-compassion was associated with a reduction in depressive symptoms within the sample, thereby mitigating the impact of guilt on the onset or persistence of these symptoms. These results further our understanding of the factors that cause or exacerbate the process of mourning perinatal loss in women. Furthermore, the results emphasise the important role of self-compassion in the grieving process following perinatal loss, thereby enriching the existing literature on the necessity of early specialised intervention based on self-compassion in such situations.
Depressive Symptoms after Perinatal Loss
Perinatal loss is a traumatic and disruptive event that gives rise to painful emotions and symptoms throughout the grieving process. These symptoms can be particularly difficult for some parents to manage. As this study shows, women grieving perinatal loss may experience depressive symptoms (Hutti et al., 2015; Richardson & Schiller, 2021). According to Mergl et al. (2024), the prevalence of depressive symptoms in women who have experienced perinatal loss can range from 22% to 36% following the event. Consistent with our findings, Bennett et al. (2008) found that the levels of symptoms reported by women who had experienced perinatal loss were similar to those observed in a psychiatric sample.
Additionally, our study found that the time elapsed since perinatal loss influences the severity of depressive symptoms. Women whose loss occurred within the last two years reported significantly higher levels of depressive symptoms than those whose loss occurred more than two years ago. This corroborates the findings of Mendes et al. (2023) and deMontigny et al. (2017), who also observed an increase in depressive symptoms during the first two years following loss. However, the study by Bennett et al. (2008) showed that psychopathological symptoms generally decreased over time, except for depression, which remained high in a sample of women who had experienced perinatal loss within the previous five years. However, Cumming et al.’s (2007) study revealed a decrease in depressive symptoms within the first 13 months after the loss, though complete remission of symptoms did not occur.
The presence of depressive symptoms in women experiencing perinatal loss can be explained by the fact that they are grieving. Grief is a normal emotional response to the loss of a significant person and may include feelings of sadness and depression, as well as a longing for the deceased (Badenhorst & Hughes, 2007). In the first few years after their loss, participants have to face the date on which their baby was due to be born, as well as the anniversary of their child’s death for the first time (deMontigny et al., 2020). This can cause greater suffering for the mother, thus increasing the likelihood of depressive symptoms (Mendes et al., 2023).
Furthermore, intrusive and negative thoughts play a central role in the persistence and/or exacerbation of depressive symptoms. Weisenburger et al. (2024) demonstrated that an increase in negative thoughts is associated with subsequent increases in depressive symptoms. Specifically, after the loss of a child due to perinatal loss, it was observed that bereaved parents reported an increase in depressive symptoms and intrusive thoughts over time (Murphy & Cacciatore, 2017). Although this assessment was not carried out in our sample, we believe that women faced with such unpredictable loss, with questions often remaining unanswered — especially regarding the cause of death (Omar et al., 2019) — end up developing negative beliefs about themselves, life and the world. These beliefs impact levels of depressive symptomatology (Boelen et al., 2006).
Guilt After Perinatal Los
Guilt is defined as a negative emotional state involving self-criticism or remorse concerning one’s behaviours, thoughts, or emotions (Stroebe et al., 2014). It is a common emotional response among mothers who have experienced perinatal loss (Pekyiğit et al., 2024). In our study, we found that women who had experienced perinatal loss reported moderate levels of guilt, with no significant change over time. This finding is supported by Gausia et al.'s (2011) study, which indicates that guilt persists regardless of the time elapsed since pregnancy loss. These findings suggest that guilt associated with perinatal loss can be a lasting emotional experience that does not necessarily diminish over time. However, this finding contrasts with that of Maguire et al. (2015), who suggest that the intensity of guilt tends to decrease over time. These contradictory findings may be due to differences in cultural attitudes towards perinatal loss, the measurement instruments used or the support systems available to bereaved mothers. This suggests that experiences of guilt are shaped by multiple contextual influences.
The presence of guilt can be explained by the fact that many women believe that they have failed to protect their child adequately (Consonni & Petean, 2013; Testoni et al., 2020), and it is also linked to feelings of helplessness (Evans et al., 2022). Furthermore, the absence of a medical cause of death can exacerbate feelings of guilt in bereaved mothers (Chavez et al., 2019; Jones et al., 2022; Maguire et al., 2015). According to Kersting and Wagner (2012), consistent feelings of guilt can prolong the grieving process, particularly if a woman realises that she may have done something that could have caused her child’s death (e.g. smoking, working too much or exercising excessively). As Gausia et al. (2011) have shown, mothers often feel guilty for not acting more carefully, even when medical information clearly indicates that the loss was not their responsibility.
Guilt and Depressive Symptoms
The significant association between guilt and depressive symptoms is a key finding of this study. Women who experience greater levels of guilt tend to exhibit higher levels of depressive symptoms, which corroborates the findings of previous studies that identified guilt as a risk factor in the development and maintenance of depression (Gausia et al., 2011; Siwik et al., 2021). According to Luck and Luck-Sikorski (2021), approximately 37% of individuals with depression experience guilt. The scientific literature indicates that individuals with depression tend to exhibit greater self-criticism and self-blame than non-depressed individuals (Stroebe et al., 2014), which may explain the results obtained in our study. Furthermore, higher levels of guilt have been shown to predict an increase in symptoms of depression and complicated grief over time (Li et al., 2018).
Although this assessment was not carried out in our sample, we believe that women faced with such unpredictable loss and unanswered questions, particularly regarding the cause of death (Omar et al., 2019), may develop negative self-beliefs that exacerbate depressive symptoms (Canady, 2023). Our study concluded that the cycle of guilt and depression can be complex, with mutual aggravation: guilt increases emotional vulnerability to depressive symptoms, which intensifies feelings of inadequacy and self-criticism associated with guilt.
The Role of Self-Compassion
Self-compassion, which is defined as treating oneself with kindness and understanding that suffering is a common human experience, has been shown to influence the grieving process (Neff, 2023). Our study concluded that self-compassion plays a significant role in women who have experienced perinatal loss.
Our research revealed negative correlations between positive self-compassion and depressive symptoms and guilt. This finding is supported by Shamsababdi and Dehshiri’s (2024) study, which found a negative correlation between self-compassion and symptoms of depression. This suggests that individuals with higher levels of self-compassion experience fewer depressive symptoms (Muris et al., 2024). Furthermore, these authors state that the various components of self-compassion mitigate feelings of guilt, thereby alleviating depressive symptoms (Etemadi Shamsababdi & Dehshiri, 2024). A longitudinal study by Maagh et al. (2023) also found that increased self-compassion in women who have experienced pregnancy loss correlates with reduced psychological distress. Furthermore, studies by Hollis-Walker and Colosimo (2011) and Miller and Strachan (2020) have shown that an increase in self-compassion is associated with a decrease in guilt and self-criticism, thereby promoting well-being.
In our research, we found that self-compassion partially mediates the relationship between feelings of guilt and depressive symptoms. Although self-compassion provides a significant indirect pathway reducing the impact of guilt on depressive symptoms, guilt also continues to exert a direct effect on depression. This highlights that self-compassion can mitigate, but not completely eliminate, the influence of guilt on depressive symptoms. This finding is supported by the research of Etemadi Shamsababdi and Dehshiri (2024), who found that guilt and shame have a mediating effect, indicating that self-compassion can improve emotional well-being indirectly by alleviating these emotions.
Self-compassion appears to enable women to cope with loss more compassionately, rather than judging themselves or succumbing to emotional suffering (Krieger et al., 2015). By fostering greater acceptance of the experience and cultivating a kinder relationship with oneself, self-compassion can mitigate the intensity of guilt and consequently reduce the likelihood of depressive symptoms developing or persisting, thereby enhancing overall well-being (Valdez & Lilly, 2018).
Thus, it can be concluded that self-compassion’s emotional support can help this population manage feelings of hopelessness and guilt, which are common in the grieving process following loss, in a more adaptive way (Felder et al., 2016; Maagh et al., 2023). Furthermore, it fosters greater resilience in the face of adversity, contributing to a reduction in depressive symptoms over time (Neff, 2023).
Practical and Clinical Implications
This study emphasises the importance of recognising perinatal loss as a profoundly impactful experience. The fact that depressive symptoms can persist for long periods highlights the importance of early screening for perinatal mental health issues, as well as the implementation of psychological and emotional support measures.
As self-compassion has been identified as a factor that can alleviate depressive symptoms and guilt, therapeutic interventions that promote this trait, such as self-compassion-focused therapy and acceptance and commitment therapy, could be beneficial in managing perinatal grief. Specific techniques may include guided meditations on self-compassion, exercises in writing compassionate letters, and journaling to acknowledge and reduce self-critical thoughts. Professionals intervening in perinatal grief should validate parents’ suffering and provide guidance and coping strategies to help them accept and reduce it (Cassaday, 2018; Testoni et al., 2020). Healthcare providers can support bereaved women by normalising feelings of guilt and sadness, actively listening without judgement and offering resources such as support groups, psychoeducational sessions and referrals to qualified therapists (Roberts et al., 2024). Furthermore, recognising the influence of guilt on depressive symptoms can inform the development of more effective therapeutic strategies for bereaved women (Li et al., 2018; Wagner et al., 2018).
Our findings provide valuable insight into the importance of self-compassion and the need to reduce feelings of guilt related to perinatal loss. This information is essential for healthcare professionals who communicate the news of loss to these women, as well as for their partners, family members and friends, who play a key role in the grieving process.
Ideally, the discourse surrounding perinatal loss should change. This study shows that, above all, these women have lost a child, along with all the plans, expectations and dreams that they had built either before conception or throughout pregnancy. We believe that recognising and appreciating perinatal loss will enable a gentler and more welcoming approach to this group, thus facilitating the grieving process.
Limitations and Future Research
This study has some limitations that should be considered. Although we obtained a representative and geographically diverse sample, data collection was conducted via an online questionnaire. This method may have resulted in a higher dropout rate, particularly among women who did not wish to revisit their experience of perinatal loss. Additionally, inaccurate responses are possible, such as women who have never experienced perinatal loss participating. Another limitation relates to the study design when testing mediation relationships. According to Frazier et al. (2004), longitudinal studies are recommended to ensure the correct temporal order of variables and allow them to be measured at different times. Furthermore, a longitudinal study could yield different results with regard not only to depressive symptoms and levels of guilt, but also to self-compassion. Although self-compassion was found to explain the variation in depressive symptoms experienced by women who had suffered perinatal loss, this capacity may also be crucial in a more general context. Intervention programmes focused on self-compassion could provide women with strategies and resources to help them cope with grief in a more adaptive and less painful way. Despite its limitations, this study is an important first step in highlighting the relevance of self-compassion in the context of perinatal loss. It provides initial evidence that may inform more robust, longitudinal studies with multiple data collections, or more in-depth interventions in the future. Finally, qualitative studies of the grieving process following perinatal loss could provide valuable insights. A more detailed analysis of the emotions involved, the difficulties experienced and the coping strategies adopted could contribute to a deeper understanding of this type of loss.
Footnotes
Acknowledgments
A special acknowledgment goes to all the women who participated in this study, as their contributions were essential in achieving these important results. We would like to express our appreciation to the “Associação Pais Coragem”, “Associação Uma Vida Mais Fértil”, the “Amor Para Além da Lua” group, the “Amor com Asas” website, the “Sofia’s Wish” project and the Cova da Beira University Hospital Center. We also extend our thanks to the doctors, nurses, and psychologists who played a vital role in the dissemination of this research.
Ethical Considerations
This study was previously assessed and authorized by the Ethics Committee of the University of Beira Interior (CE-UBI-Pj-2022-066).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, M. R., upon reasonable request. The data are not publicly available due to restrictions (privacy concerns or the inclusion of information that could compromise the confidentiality of research participants).