
Abstract
Identifying patient’s goals and values at end of life is essential to providing patient-centred care. The purpose of this prospective cohort study was to describe the changes in goals of care and the nature of end-of-life care during admission to two intensive care units in South Australia. Under a quarter of patients had their goals of care documented on admission to the intensive care unit and among those who subsequently survived to hospital discharge, only 32% had their goals of care documented on hospital discharge. Most deaths in the intensive care unit occurred after withdrawal of life-sustaining interventions. Data from 154 family meetings were collected and consensus was achieved among all parties in most meetings. In this study, fewer than one in four patients had goals of care documented on admission to intensive care with marginal increases by ICU discharge. This represent an area of care that could be improved.
Background
About half of all deaths in Australia occur in hospital, with nearly 13% of hospital deaths involving admission to an intensive care unit (ICU) (Australian Bureau of Statistics, 2021; Australian Institute of Health and Welfare, 2017). Approximately 9,000 patients die in Australian and New Zealand ICUs each year, this figure is expected to rise with an estimated 6% annual increase in ICU admissions (Australian and New Zealand Intensive Care Society [ANZICS], 2019). In addition to providing life-sustaining or life-prolonging therapies, alleviating suffering and supporting both patient and loved ones during the dying process are key elements of care provided in the ICU. It is imperative that emergency care is provided with appreciation of the patient’s values and wishes, informed by clear communication between clinicians, patients and their substitute decision-makers regarding their needs at end of life (ANZICS, 2014; Cook & Rocker, 2014). Integral to provision of patient-centred care and/or good end-of-life care is identifying a patient’s ‘goals of care’ (Australian Commission on Safety and Quality in Health Care, 2023). The ’goals of care’ (GOC) for the purpose of this study were defined as recording of treatment decisions by healthcare professionals, particularly in relation to life-prolonging therapies, guided by patient’s values, treatment preferences, and/or prognosis. To put it into perspective, this vital information was only documented in 34% of patients with life-limiting illness referred to a single Australian ICU (Orford et al., 2016). It is unclear if this trend is reflective of contemporary practice and/or other ICUs.
Objectives
Given the importance of understanding and documenting a patient’s GOC, our study aimed to examine the patterns of GOC changes and the nature of end-of-life care in the ICU. The objectives of our study were to describe: (1) documentation of GOC, changes and timing of changes made to GOC during ICU admission, (2) documentation of GOC on hospital discharge, (3) care provided during end of life, (4) number and duration of formal family meetings, and (5) whether consensus was achieved during these meetings as part of GOC discussion.
Methods
This was a two-centre prospective observational cohort study conducted over a 90-day period from 13 September 2021 to 12 December 2021. All adult patients aged 18 years or older admitted to the two selected metropolitan ICUs were eligible. The first ICU is a 48-bed mixed medical-surgical ICU, and the second ICU is a 14-bed mixed medical-surgical ICU. The first ICU is also a major referral centre for trauma, neurosurgery, cardiothoracic surgery, haematology and oncology patients. Both sites were selected as they were governed by the same local area health network. A prospective design was chosen to ensure real-time data collection, which minimized recall bias and allowed accurate documentation of decision-making processes as they occurred. This was particularly important for studying GOC discussion and changes, as retrospective data may be incomplete or influenced by documentation variability.
The primary outcomes were the documentation of GOC on ICU admission and modifications of GOC during ICU admission. The secondary outcomes were GOC documentation on hospital discharge, care provided during the end of life and characterisation of formal family meetings (number, duration of meeting and whether consensus was achieved during the meeting) as part of GOC discussion.
Demographic and clinical data were collected from electronic medical records. A document was considered a GOC note when completed by a physician, summarising decisions on medical interventions or life-prolonging therapies guided by patient’s values, preferences and/or prognosis. GOC documentation was screened systematically in each patient’s electronic medical record including patient electronic record headers, resuscitation alert documents, medical admission notes and medical progress notes. Entries in these sections can only be completed by physicians. A resuscitation order had to be completed by a physician for the GOC to appear in the patient electronic record header. The resuscitation alert document was a template for GOC used in all public hospitals in South Australia. GOC documentation was considered complete if recorded in any of the outlined sections. When completed, the GOC were categorised as: (1) full active management (i.e., for all life-sustaining interventions), (2) withholding of at least one pre-specified life-sustaining interventions - namely cardiopulmonary resuscitation, invasive mechanical ventilation, non-invasive ventilation, renal replacement therapy or vasopressor/inotrope infusion, and (3) withdrawal of at least one pre-specified life-sustaining interventions. Withholding of interventions was defined as a decision not to initiate or increase any life-sustaining interventions. Withdrawal of interventions was defined as decision to cease active life-sustaining interventions currently provided. These categories were based on Australia and New Zealand Intensive Care Society Centre for Outcome and Resource Evaluation Adult Patient Database Data Dictionary and Ethicus-2 Study, utilising terminologies accepted in Australasia and internationally (ANZICS, 2022; Sprung et al., 2019). Modifications of GOC during ICU admission were also recorded. In the absence of any documented GOC, it was assumed that the patient was for ‘full active management’. The absence of GOC documentation is a common and major ethical challenge in resuscitation, where “treat first and discuss later” approach in emergency situations, such as cardiopulmonary arrest, tend to be routine clinical practice (Mentzelopoulos et al., 2018).
Data on formal family meetings were collected prospectively by ICU clinicians conducting family meetings. The definition of formal family meeting - hereafter referred as family meeting - was: (1) any family meeting conducted to discuss patient’s GOC, or (2) any meetings conducted in a private meeting room, attended by the patient or at least one substitute decision-maker, and at least one ICU medical representative. Consensus was defined as agreement on decision by specified parties involved in the meeting. Clinicians recorded data using a structured form with predefined fields to ensure completeness and minimize variability. They received training on how to document key aspects of family meetings relevant to our study. This included guidelines on what information to record and how to maintain consistency. The research team conducted periodic checks on collected data, clarifying discrepancies when necessary to maintain data integrity. The ICU clinicians were requested to complete a data collection form available in electronic (REDCap, a secure web-based application) or hardcopy format (Family meeting data collection from available in supplemental material).
Data on aspects of end-of-life care during the dying period were collected. This included specific patient management (administration of analgesia or anxiolytics, endotracheal tube removal), ICU medical team review, palliative care referral and visitations.
Statistical Analysis
Descriptive statistics included frequencies and percentages of patients for categorial data and median, interquartile range (IQR) for continuous variables.
Results
Patient Cohort
Patient Characteristics
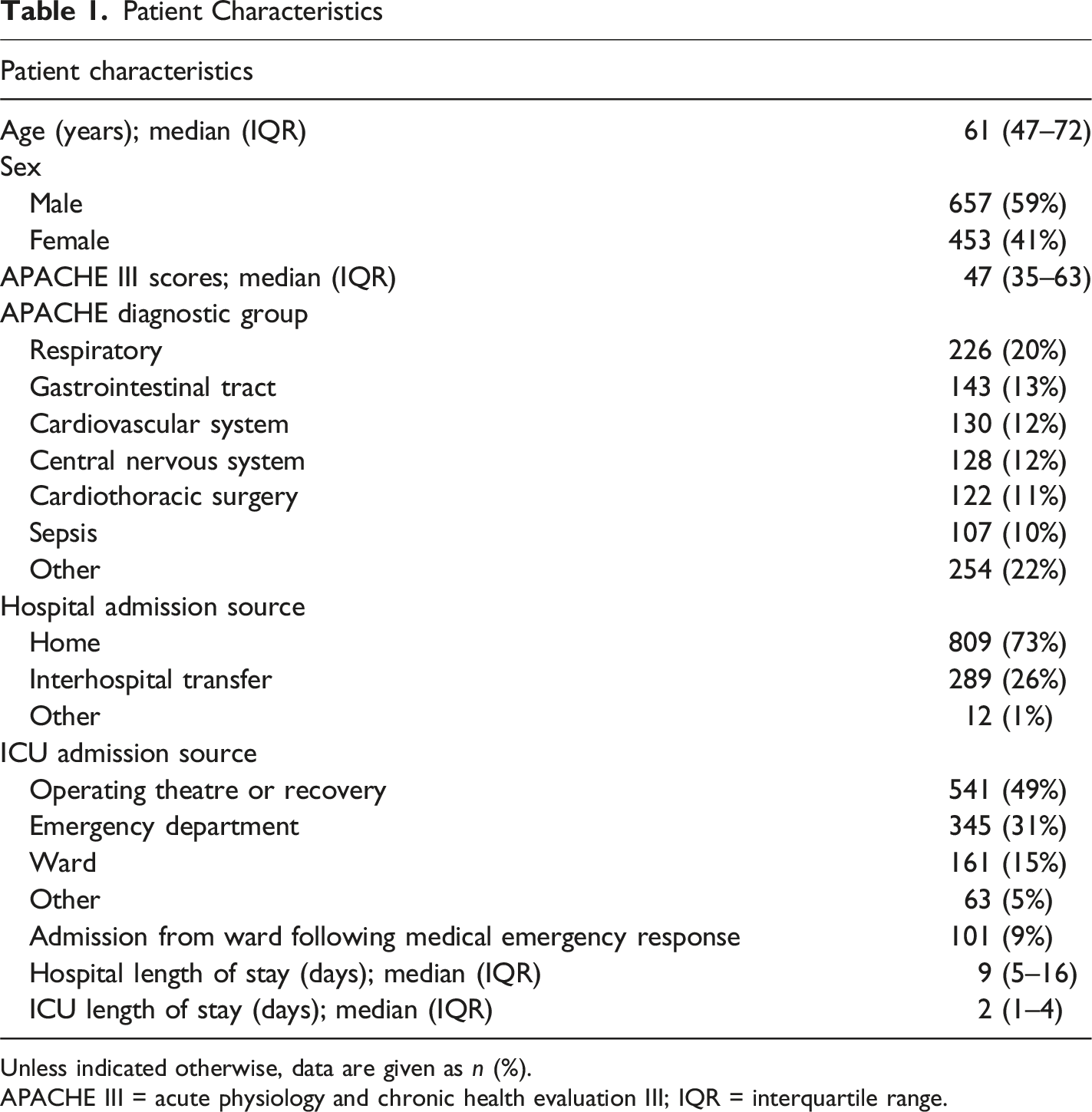
Unless indicated otherwise, data are given as n (%).
APACHE III = acute physiology and chronic health evaluation III; IQR = interquartile range.
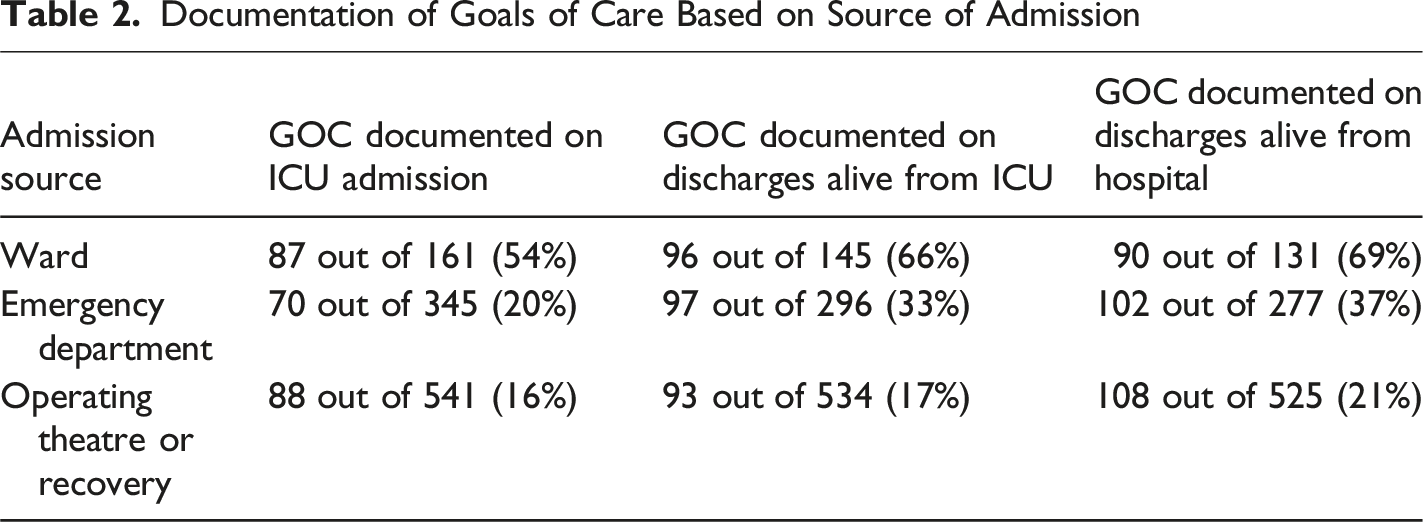
GOC Documentation
Out of the 1110 ICU unique admissions, 246 (22%) patients had their GOC documented on ICU admission. A total of 1,034 patients were discharged alive from the ICU, and 992 were discharged alive from the hospital. The documentation of GOC over the course of ICU admission to hospital discharge is summarized in Figure 1. The frequency of GOC documentation and the corresponding source of admission are presented in Table 2. Documentation of GOC Over the Course of ICU and Hospital Discharge Documentation of Goals of Care Based on Source of Admission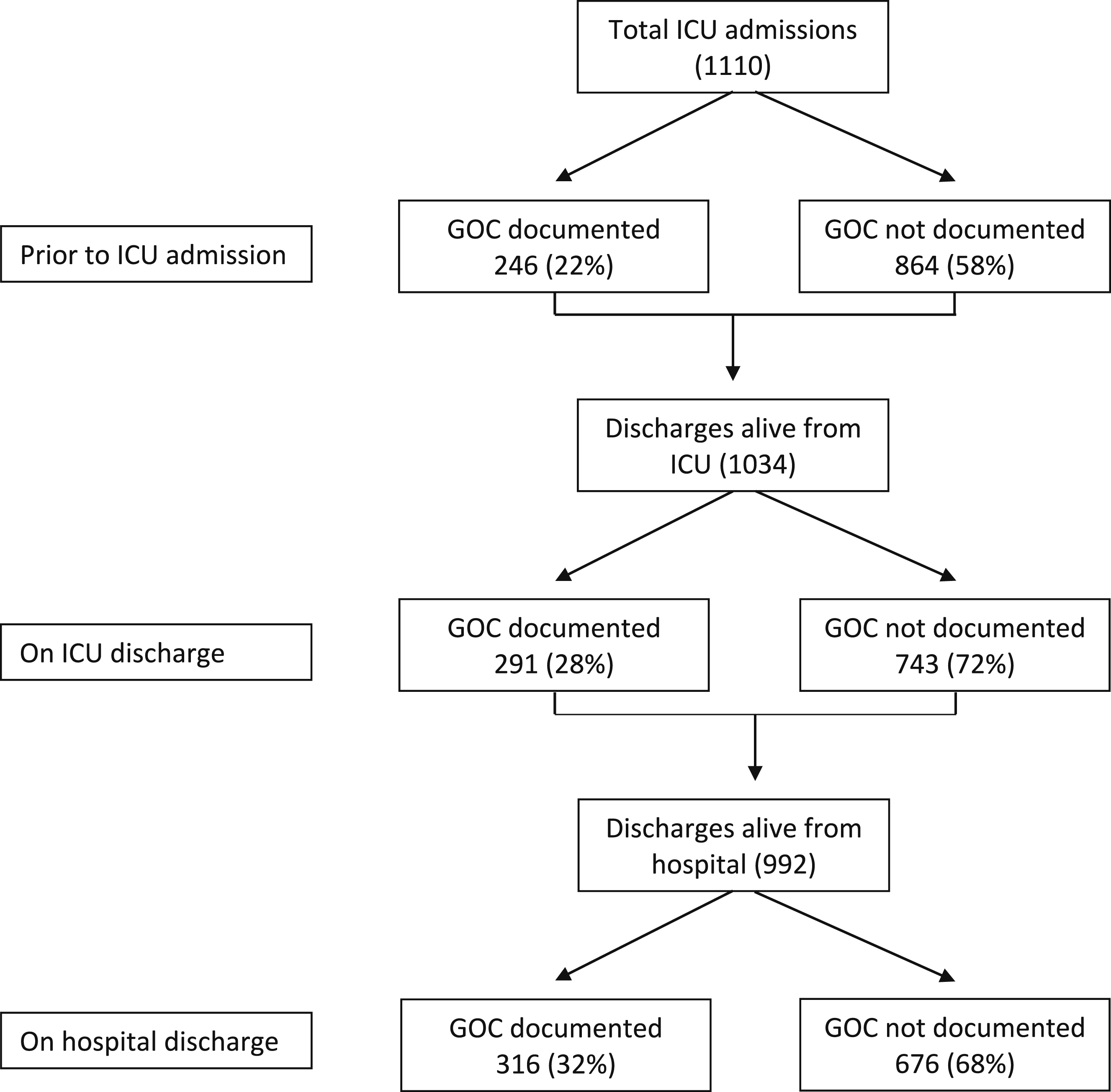
Changes in Intensity of Interventions Consistent With GOC During ICU Admission
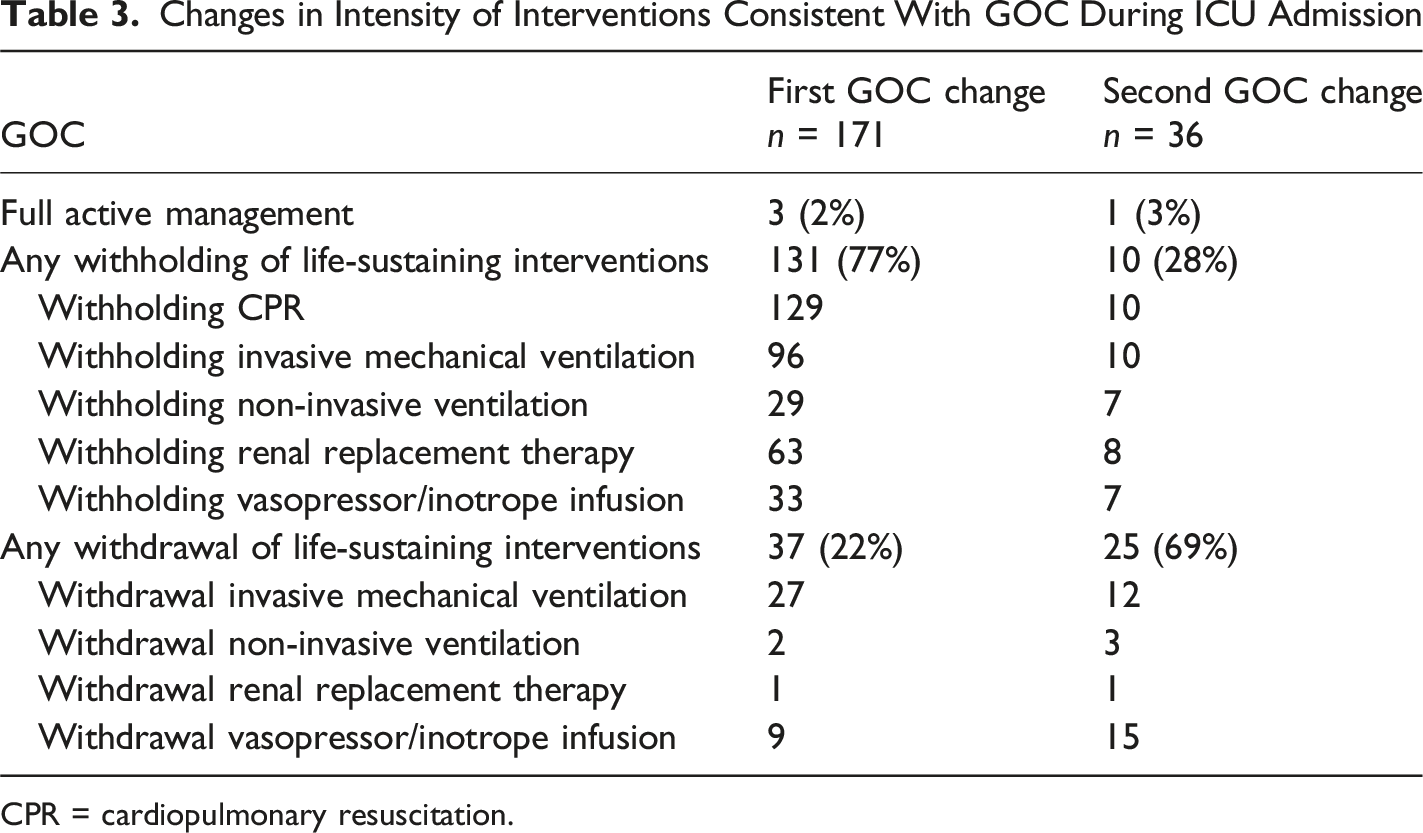
CPR = cardiopulmonary resuscitation.
Family Meetings
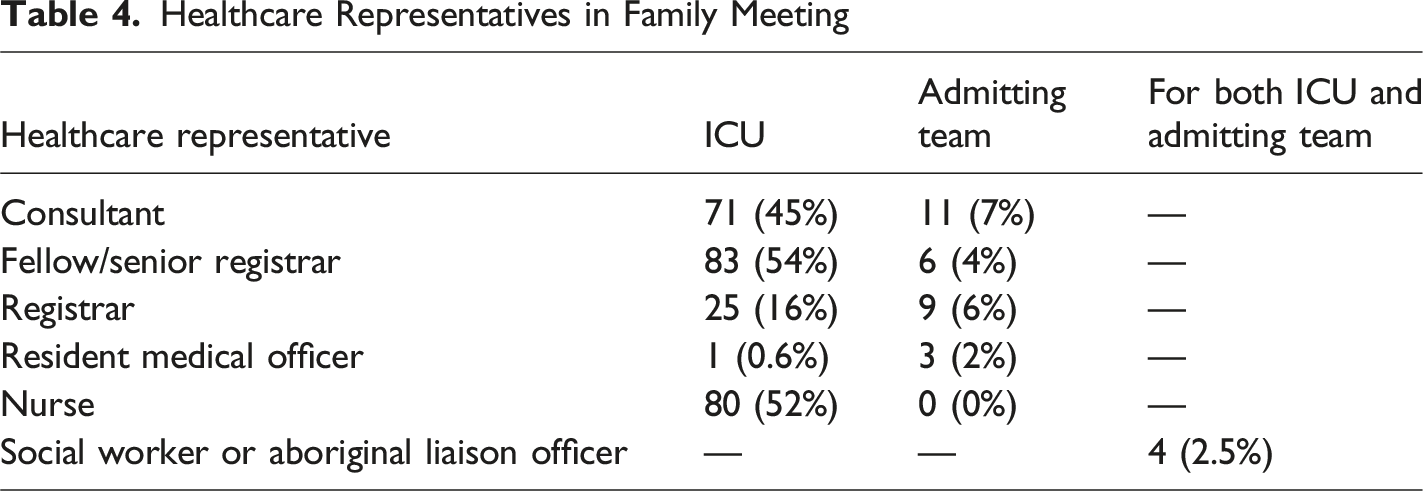
Healthcare Representatives in Family Meeting
Changes to GOC were made after 96 out of 154 (62%) family meetings. Before the family meeting, 92 (60%) patients were for full active management compared to 39 (25%) after the meeting. Overall, the number of interventions withheld and withdrawn increased after the meetings. Consensus was achieved among all parties in 94% (144/154) of family meetings. Family meetings with initial disagreement and eventual resolution were also reported. The initial disagreement occurred: (1) within family (3%), (2) between clinical teams and family (2%), (3) between clinical teams (0.5%). In one (0.5%) family meeting, consensus between clinical teams could not be achieved at the end of the meeting and the patient remained to be for full active management.
End-of-Life Care
During the study period, 76 (7%) deaths occurred in ICU from 1,062 patients admitted. Substitute decision-makers consented to organ donation for eight patients (6 donation after neurological determination of death and 2 after circulatory death). Six patients became organ donors.
Among patients who died in the ICU, the median age was 70 years (IQR 55–77), and median Acute Physiology and Chronic Health Evaluation III score was 95 (81–108). Fifty-eight patients (76.3%) died following withdrawal of life-sustaining interventions, and 17 patients (22.4%) had life-sustaining interventions held when they died. Only 1 (1.3%) patient died on full active management. Among the patients who died in the ICU, 47 of 76 (62%) received invasive mechanical ventilation prior to commencing end-of-life care, and 33 of these 47 (70%) patients had their endotracheal tube removed as part of their end-of-life care. All 76 patients were reviewed by the ICU medical team after decision for end-of-life care and prior to death. Visitor restriction in relation to coronavirus pandemic period were exempted in 75 (99%) patients. The patient who died on maximal therapy was the only exception. Families were present at time of death in 60 (79%) patients. No patient who died in the ICU was referred to a palliative care team.
At the end of life, opioids were used in 54 (71%) patients, most commonly morphine (33/54, 61%), given by continuous infusion (47/54, 87%). Benzodiazepines were administered in 39 (51%) patients, predominantly (97%) in the form of midazolam and administered by continuous infusion in most patients (36/39, 92%). Twenty-one patients (28%) who died in the ICU did not receive opioid nor benzodiazepine agents.
Discussion
The key findings from this study were that GOC were only recorded in under a quarter of patients admitted to the ICU, with modifications in GOC occurring only in a minority (15%). These changes generally reflected a reduction in the intensity of life-sustaining interventions, usually within 48 h of ICU admission, and were reached with consensus between clinicians and surrogate decision-maker.
Our study shows that documentation of GOC was inconsistently completed. The lack of documentation could reflect that the conversations did not occur, or if it did, it was not formally documented. To promote patient-centred care, this step is crucial. Proactive and pre-emptive discussions with patients, or surrogate decision-makers, facilitate delivery of high-quality care aligned with values and preferences upheld by the patients, avoiding urgent after-hours conferences in emergency scenarios (Australian Commission on Safety and Quality in Health Care, 2023; Modes et al., 2019). Timely discussions about GOC would avoid the use of invasive and burdensome interventions that are incongruent with patients’ wishes. Apart from improved end-of-life care, such discussions could also improve family satisfaction, reduce stress, anxiety and depression in bereaved family members (Detering et al., 2010). Clear documentation helps avoid misunderstandings about whether life-sustaining interventions should be continued or withheld. Well-documented GOC discussions may also help maintain consistency in care decisions, especially during shift changes or when patients are transferred between departments.
Our findings are consistent with other studies whereby between 16% and 34% of patients with life-limiting illness who were referred to ICU had GOC documented (Elderkin et al., 2020; Orford et al., 2016). Organisational support to drive improvement in this area is crucial. This empowers clinical units to implement measures to improve performance. Those in leadership positions are key drivers of change, working closely with multidisciplinary team members and consumers. A vital measure to improve GOC documentation is education. This ranges from raising awareness and understanding of the topic to communication training. Electronic health records could be utilised to set reminders if GOC are not documented within a pre-defined timeframe. Performance targets could then be set within each unit and organisation with regular local and external reviews (Mandel et al., 2009).
Modifications to GOC generally involved de-escalation of intensity of life-sustaining interventions, from withholding to withdrawal of life-sustaining interventions, and incorporation of a component of end-of-life care, with only one death on full active management. The stepwise withholding or withdrawal of life-sustaining interventions identified in this study may reflect an evolving clinical picture, indicating failure to respond to therapy and irreversible decline, and ongoing discussions with surrogate decision-makers in redirecting focus of the dying patients’ care from curative to comfort-care (Morgan et al., 2014). Most deaths in ICU occurred following withholding or withdrawal of life-sustaining interventions. This observation was comparable to a retrospective audit conducted in two Australian ICUs where 81% of patients who died in the ICU had life-sustaining interventions withheld or withdrawn (Brieva et al., 2009). This indicates that deaths were anticipated by clinicians and, when a potentially poor outcome was identified, clinicians actively engaged with families. Recognition that a patient is approaching the end of life and discussing this with family is vital to ensure that there is an opportunity to provide appropriate palliative care and for the family to spend time with their loved one (Australian Commission on Safety and Quality in Health Care, 2023). All patients were reviewed by the ICU team after a decision to institute end-of-life care, mitigating concerns that clinical care ends when patients are no longer receiving life-sustaining interventions.
In clinical setting, family meetings are commonly the forum for GOC discussions to occur. GOC discussions go beyond duality of “to resuscitate or not to resuscitate”. It involves a shared decision-making process, where clinical information and patient’s preferences or values are exchanged. This then facilitates development of treatment plan that aligns with the patient’s preferences (Scheunemann et al., 2019). The median duration of meetings in which GOC were discussed was 15 min. Whilst this may be compatible with demands of clinical workload, it is unclear from our data whether this represented an adequate opportunity for families to have their concerns addressed and questions answered. A multicentre study in France described end-of-life family conference duration of between 20 and 30 min (Lautrette et al., 2007).
Our data indicate that nearly all family meetings achieved consensus between parties. Indeed, of 154 meetings, each with up to three parties (family, ICU and representative of the admitting team), in only one instance was consensus not eventually reached between all parties. This is an important and reassuring finding for clinicians. Physicians were consistently present in these family meetings, with ICU nurses present in just over half of these meetings, social workers infrequently present (<5%) and nursing staff from admitting teams never present, suggesting there may be under-representation in multidisciplinary team approach when compared to international data (Lautrette et al., 2007). Interprofessional family meetings are important facilitators of patient- and family-centred care. These meetings, as described by Kentish-Barnes and colleagues, involve families, physicians, nurses and other ICU clinicians (Kentish-Barnes, Jensen, & Curtis, 2022). It has been shown that nursing support during the dying process has reduced grief in the relatives of dying patients although the benefits of nursing attendance in family meetings remain unknown (Kentish-Barnes, Chevret et al., 2022).
The strengths of our study include the prospective design, consecutive enrolment and inclusion of two separate hospitals. This is also the first study to describe the trend and changes in GOC for patients admitted to Australian ICUs. Data on family meetings was collected prospectively, and these data, particularly data on consensus, would be difficult to collect by retrospective medical record review. A limitation of this study is the inclusion of only two ICUs from the same state in Australia. Although the inclusion of both a tertiary and secondary institution with significantly different case mix adds external validity to our findings. A greater number of ICUs may provide better understanding of an Australia-wide practice. It is possible that not all family meetings were documented in the patient medical records and therefore not captured during this study period (Uyeda et al., 2023). But it is unlikely that any meetings that were not recorded included senior medical staff from the ICU. Another limitation of our study is that we did not assess if the documented GOC aligned with the care that the patients received.
We identified and recorded agreed GOC and reaching of consensus from the clinicians’ perspective. Whilst this is crucial, since it is the clinical record that directs ongoing management, future studies should seek to explore the perspective of the family and patient, to evaluate whether their assessment of the content of the meeting and achievement of consensus matches that of the clinician (Modes et al., 2019). Future studies may also wish to evaluate whether programs to assist clinicians with communication may increase the quantity and quality of GOC and/or end of life care discussions (Orford et al., 2019).
Conclusion
Only a minority of patients have GOC documented on admission to ICU. This warrants attention and improvement to ensure delivery of patient-centred care. Most meetings held in the ICU to discuss GOC occurred early in the admission period and were associated with a consensus agreement to change GOC. Most of the deaths that occurred in ICU followed the withholding or withdrawal of life-sustaining intervention.
Supplemental Material
Supplemental Material - Establishing Goals of Care and End-of-Life Care in the Intensive Care Unit. A Period Prevalence Study
Supplemental Material for Establishing Goals of Care and End-of-Life Care in the Intensive Care Unit. A Period Prevalence Study by Nikki Y. Yeo, Adam M. Deane, Nancy Kentish-Barnes, Hao Z. Wong, Krishnaswamy Sundararajan, Benjamin A. J. Reddi in OMEGA - Journal of Death and Dying
Footnotes
Acknowledgements
The authors would like to acknowledge the dedicated staff at The Queen Elizabeth Hospital and the Royal Adelaide Hospital Intensive Care Units who were involved in this study.
Ethical Considerations
This study received ethical approval from Central Adelaide Local Health Network Human Research Ethics Committee (reference number 14959) on 5 August 2021. Waiver of consent was granted to screen and recruit participants due to low-risk nature of the study. Patient data will not be shared with third parties.
Author Contributions
Nikki Y. Yeo: Conceptualization, Methodology, Investigation, Writing-Original draft preparation, Review and Editing, Visualization. Adam M. Deane: Conceptualization, Methodology, Investigation, Writing-Original draft preparation, Review and Editing, Supervision. Nancy Kentish-Barnes: Methodology, Writing-Original draft preparation, Reviewing and Editing. Hao Z. Wong: Investigation, Writing-Review and Editing. Krishnaswamy Sundararajan: Methodology, Writing-Original draft preparation, Review and Editing. Benjamin A. J. Reddi: Conceptualization, Methodology, Investigation, Writing-Original draft preparation, Review and Editing, Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, NY, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.