
Abstract
Cases of terminal lucidity (TL) in children have recently been documented in contemporary literature, yet no studies have examined the impact on caregivers of witnessing TL in children. Using an online survey, this study assessed the impact of witnessing TL in children on seven caregivers who described a total of 11 cases of TL in children. Findings revealed that witnessing TL in children was considered a spiritual experience that influenced caregivers’ belief systems. All caregivers had disclosed what they had witnessed to others, resulting in a mixture of skeptical and accepting reactions. Findings suggest witnessing TL in children may initiate a spiritual transformation that has similar implications for enhancing end-of-life care and creating ‘space’ for TL to be perceived as a natural part of the dying process in terminally ill children.
A spectrum of unusual occurrences has been reported in those who are dying, typically transpiring in the final days, hours, or minutes of a person’s life. One such experience that has come to be known as terminal lucidity (TL), involves an unexpected surge of mental clarity, which can be accompanied by a brief return of cognitive abilities and sometimes physical abilities in patients who otherwise were experiencing a significant degree of cognitive impairment. Because TL occurs in direct proximity to death, it can be considered a medical enigma, given that those who experience TL are often (although not always) presumed to have irreversible physiological declines. TL may also include positive emotions and seemingly transcendental experiences for the dying person. Some of these experiences can include awareness of imminent death, a need to reconcile with loved ones, which can include the dying person saying goodbye, expressing gratitude to caregivers, and reassuring loved ones that they will be okay. TL can co-occur with other end-of-life experiences, such as death-bed visions in which the dying person appears to interact with deceased others (Brayne et al., 2008; Claxton-Oldfield & Dunnett, 2018; Fenwick & Brayne, 2011; Shared Crossing Initiative, 2022).
An estimate of the prevalence of TL is approximately 2%–6% of all dying people, regardless of medical condition immediately before death (Batthyany & Greyson, 2021; Lim et al., 2020; Nahm & Greyson, 2009). Because TL is still not widely acknowledged as a phenomenon that may occur as a natural part of the dying process, information about TL is not routinely collected nor is it frequently reported, making the true prevalence of TL likely higher (Batthyany & Greyson, 2021; Fenwick & Brayne, 2011; Nahm et al., 2012; Nahm & Greyson, 2009). Also contributing to uncertainty regarding prevalence rates is the lack of a commonly agreed scholarly definition of TL, despite active ongoing debates about how it should be defined (Gilmore-Bykovskyi et al., 2021; Nahm, 2022a, 2024; Peterson et al., 2022). Part of the definitional challenge is that episodes of lucidity that are consistent with TL can occur in, for example, people with advanced dementia who may not die immediately following the lucid episode. Terms including paradoxical lucidity, episodes of lucidity and lucid episodes are currently utilized in scholarly literature to describe occurrences of lucidity (e.g., Batthyany & Greyson, 2021; Gilmore-Bykovskyi et al., 2023; Karlawish et al., 2024), particularly as they occur in older aged populations with dementia. Such experiences, while appearing to be similar to TL, are currently differentiated from TL if they do not occur, from a definitional perspective, in proximity to death. Its seeming unpredictability and proximal occurrence to death denies researchers the opportunity to assess the phenomenology of TL from the perspective of the person who experienced it (i.e., the dying person). Consequently, what is known about TL is exclusively drawn from eye-witness testimonies about what the dying person appears to be experiencing.
Impacts of Witnessing Lucidity
Due to the previously mentioned ongoing definitional debates, research investigating eye-witness reactions to TL is, with few exceptions (e.g., Mutis et al., 2024), limited. Instead, the majority of studies have investigated the impact of lucidity episodes in general (which may or may not specifically include TL) on both professional and non-professional (e.g., family members) caregivers involved in dementia care. What such research typically indicates is that analysis of the witnesses’ descriptions of lucidity events provides useful insights into how the experiences are interpreted, as well as their emotional valence for the witness.
For example, initial research suggested that witnessing lucidity episodes can be emotionally complex. Griffin and colleagues found 72% of caregivers reported a positive response to witnessing lucidity, while 17% described it as stressful, and 10% reported a mixture of hope and distress (Griffin et al., 2022). A more recent study has suggested the relationship of the caregiver to the person who has the lucidity episode may have some bearing on how it is interpreted, as well as whether a specific behavior is identified as lucidity or not. For example, caregivers who are the adult children of the patient are more likely to report an episode of lucidity in their parents and are also more likely to appraise the lucidity episode as positive, in comparison to spousal caregivers (Kim et al., 2025).
It is possible the way lucidity episodes are interpreted may influence the emotional reaction caregivers have to them. Peterson and colleagues (2022) found that for caregivers working from the current dominant understandings of dementia as progressive cognitive impairment, lucidity episodes can cause confusion, grief, and distress since such episodes imply that the dying person is suddenly getting better. In contrast, for some caregivers TL was recognized as an indicator of imminent death, but was nevertheless interpreted as a cause for hope (Gilmore-Bykovskyi et al., 2023; Mutis et al., 2024).
Combined, such findings suggest that witnessing lucidity initiates an interesting mix of reactions that may be colored by personal relationships and by pre-existing beliefs about medical conditions and their trajectories. Yet, because most of the research seems to be focused on the witnessing of lucidity episodes in older populations, and particularly in patients with dementia who do not necessarily pass away immediately after their lucidity episode, it is not yet known whether the same impacts might be consistently evidenced in eye-witness cases of TL in adults without dementia, in cases of TL in adults who are not of an older age group, and in cases of TL in children.
TL in Children
Although the pool of scholarly information about TL has increased substantially over the past decade, with a primary focus being on quantifiable features, this literature has also mostly focused on TL accounts drawn from aging adult populations (Lim et al., 2020; Nahm et al., 2012; Nahm & Greyson, 2009). Yet, TL has also been witnessed in dying children. To our knowledge, only a handful of cases (e.g., Cantipratanus, 1605; Doka, 2020; Hyslop, 1907; Morse & Perry, 1990) existed in the literature up until recently when we described three new and recent cases of TL in children in a pediatric oncology clinic, and shared other cases that have been provided to us (Roehrs et al., 2024; Tassell-Matamua & Kothe, 2025; Woollacott & Tassell-Matamua, 2025). Additional cases of TL in children are included in a forthcoming publication (Tassell-Matamua et al., 2025).
Although current published accounts of TL in children suggest that quantifiable features of the phenomenon manifest in similar ways to how TL manifests in adults, it should not be assumed that the phenomenology of TL in children and adults is alike. As previously mentioned, published TL reports are exclusively based on the eye-witness testimony of adults, meaning what is currently known about TL in children is through the interpretive lens of adults. The layers of conditioning that adults use to interpret TL may not necessarily correspond to how the child is actually experiencing TL.
Equally pertinent is the impact on caregivers of witnessing TL in children. Again, it cannot be assumed that the impact of witnessing TL in older-aged people or people with dementia will be the same for those who witness TL in children. The proximity to death, the age of the child, and the heightened emotions that often accompany death of a child, might influence the way TL is perceived and the emotional valence it holds for those who witness it. Perceptions and emotional impact of witnessing TL might have implications for end-of-life care, as well as post-death grieving and coping. Indeed, it has been found that caregivers tend to shift their strategies of care after witnessing lucidity episodes (Griffin et al., 2022). Prior work has likewise found a need for open-minded discussions surrounding end-of-life experiences and better support networks for family members and healthcare providers (Morris & Bulman, 2020; Ney et al., 2021).
It is for these reasons that the current study investigated the impact on caregivers of witnessing TL in children. In line with previous research on caregivers of older adults, we wanted to assess how witnessing TL in children is perceived, its emotional valence, whether it influences belief systems of the witnesses, and whether they disclosed the TL experiences to others and what the reactions to disclosure were.
Methods
We adopted a pragmatic approach to research design, data collection and analysis (Ramanadhan et al., 2021), which included utilizing a mixed-method approach of both quantitative and qualitative data. Specifically, we employed an online survey to collect fixed-choice and open-ended responses to a range of questions. As an international team, we employed our unique expertise sets as individuals across the whole research process, and gave specific advice on areas we are especially well-versed in. To comply with funding requirements, data collection began in July 2023 and was completed at the end of May 2025 to enable sufficient time for analysis and publication. The survey was available in both English and Spanish and distributed through our international networks.
Positionality Statement
All authors of the present study are known researchers in the fields of near-death studies, exceptional human experiences, and end-of-life experiences, draw their expertise from a range of different disciplinary perspectives, have differing lengths of professional experience, and all have familiarity with and have published quantitative and qualitative research. This common familiarity with the effect exceptional experiences often have on those who have them but also those who witness them, as well as familiarity and experience with mixed-methods approaches across different disciplinary perspectives, informed our collective reflections throughout the research process. However, as a multinational team, the authors acknowledge the differing socio-historical-political-cultural perspectives they brought to the research and how this meant that, at times, the authors viewed aspects of the research through different interpretive lenses. When this occurred, the research team engaged in robust discussions, with resolutions being reached by majority consensus. This is implicitly reflected in the analysis and presentation of the data.
Participants
Details of the Caregivers and Their Reported Cases of TL in Children
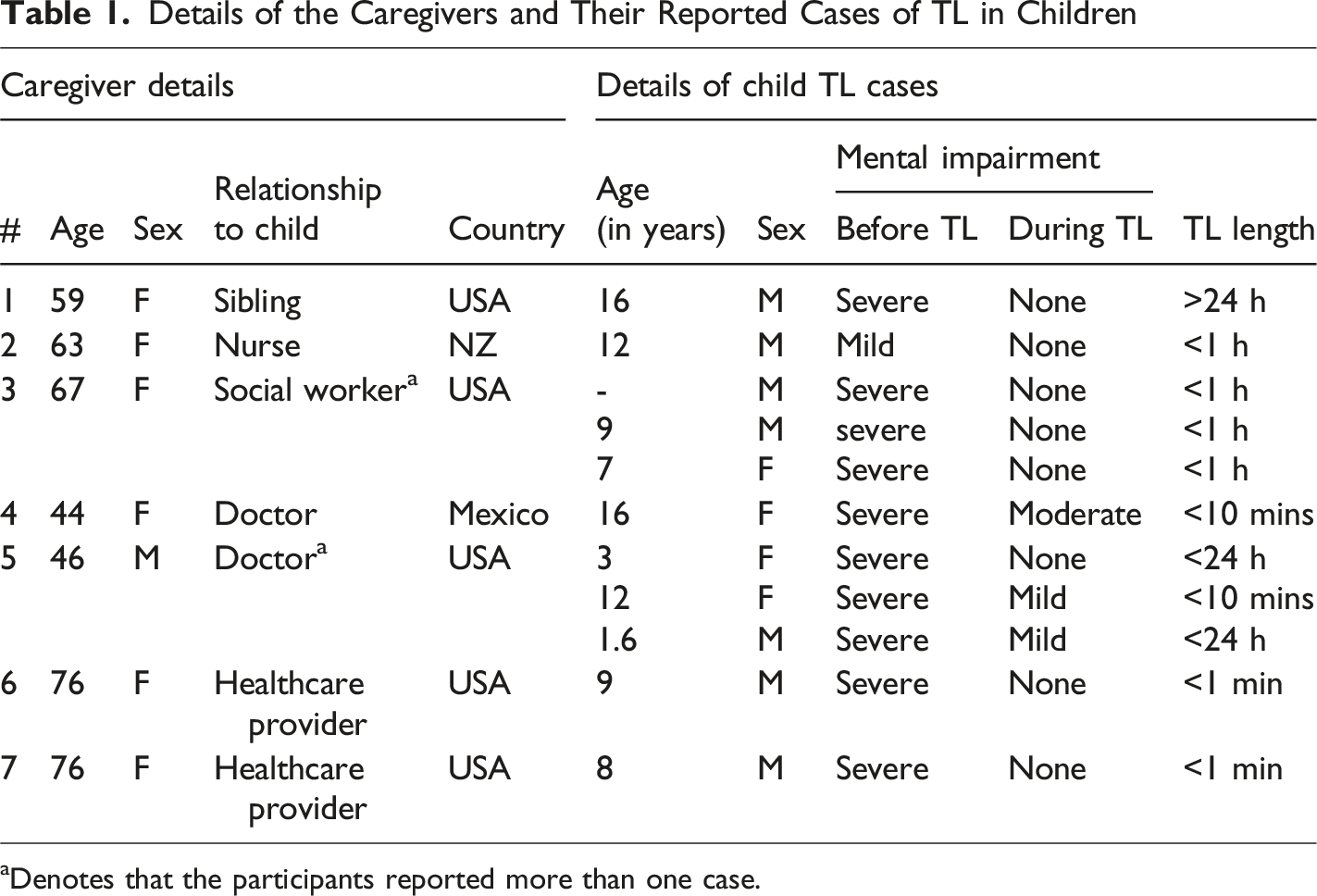
aDenotes that the participants reported more than one case.
Ethics
The Massey University Human Ethics Committee, Aotearoa New Zealand, provided ethical approval for the study (Southern A, Application 22/52). No identifying information about the children whose TL the caregivers witnessed was collected. All participants were given information detailing the study aims and were required to give consent electronically before participating in the survey.
Instrument
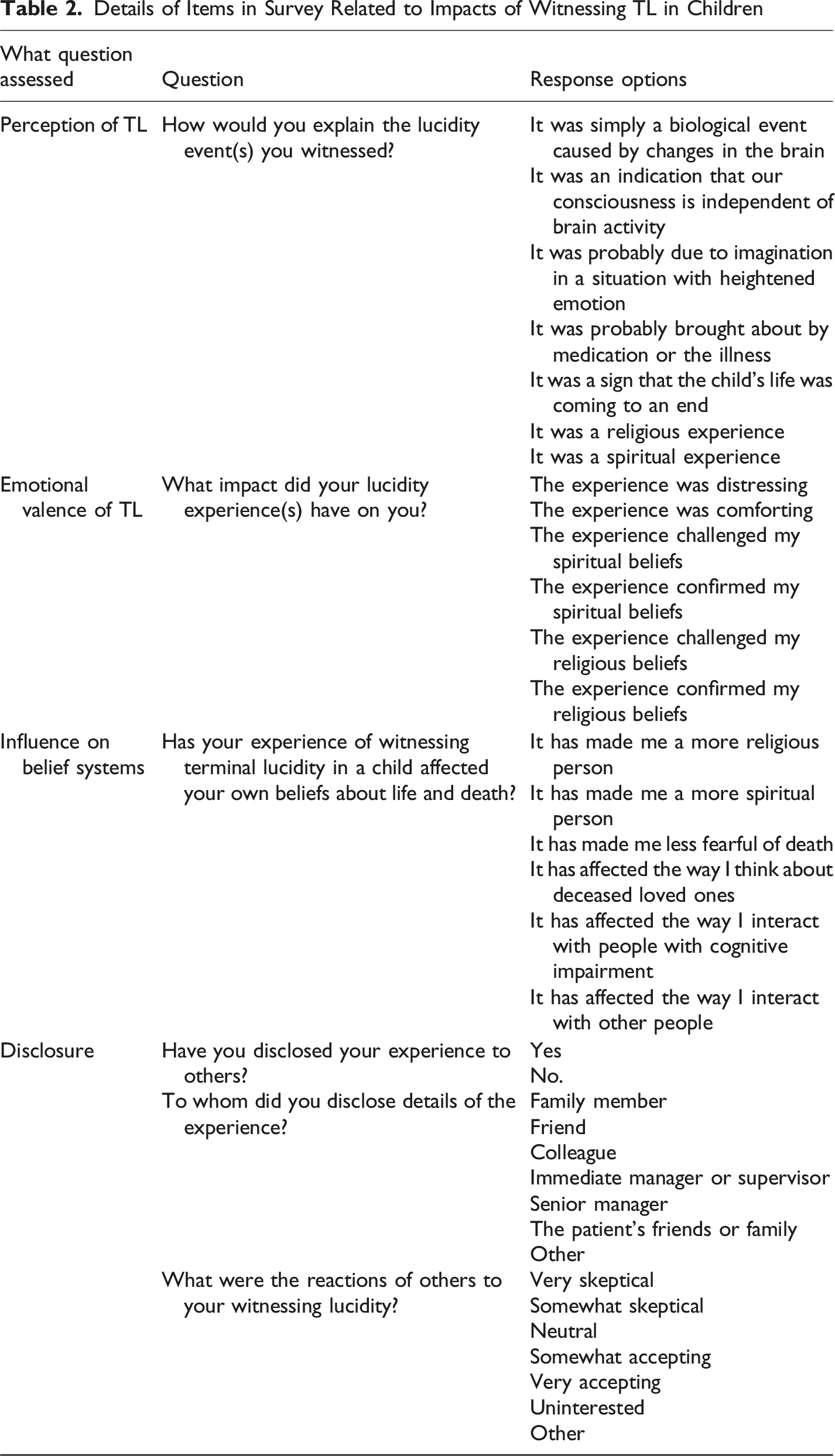
Details of Items in Survey Related to Impacts of Witnessing TL in Children
Findings
Due to the small sample size of seven caregivers reporting 11 cases of TL in children, the findings primarily outline descriptive statistics performed on fixed-response questions, noting that participants completed one survey for every TL they witnessed. Qualitative responses to the open-ended questions have also been provided, where they were given as a response. Because of the limited number of open-ended responses provided, rather than adopting a particular philosophical framework to inform analyses, we instead employed a pragmatic approach to presentation of the qualitative responses. Specifically, we have presented the verbatim responses corresponding to the question asked and have not attempted to code or categorize the verbatim responses thematically in any way. Both quantitative and qualitative findings are organized according to the questions provided in Table 2. Findings were checked through a process of triangulation, whereby all authors engaged in an iterative process of reviewing and revising the findings until there was consensus across the team that the findings are presented in a way that accurately reflects the data.
Perception of TL
To ascertain caregivers’ perceptions of TL, we asked, “How would you explain the lucidity event(s) you witnessed?” As mentioned, when asked to select explanations for the TL they witnessed, caregivers were able to indicate agreement with as many options as they wished. Figure 1 shows all responses that participants chose to select. Most caregivers perceived TL as a spiritual experience and one that signals the child’s physical life is coming to an end. Six participants indicated they perceived TL to be indicative of consciousness operating independently of the brain (i.e., non-locally). One participant perceived TL to be a religious experience. None of the participants indicated that they thought TL was due to medication, was a biological event caused by brain changes, or was due to imagination. Perceptions of TL, as Indicated by Caregivers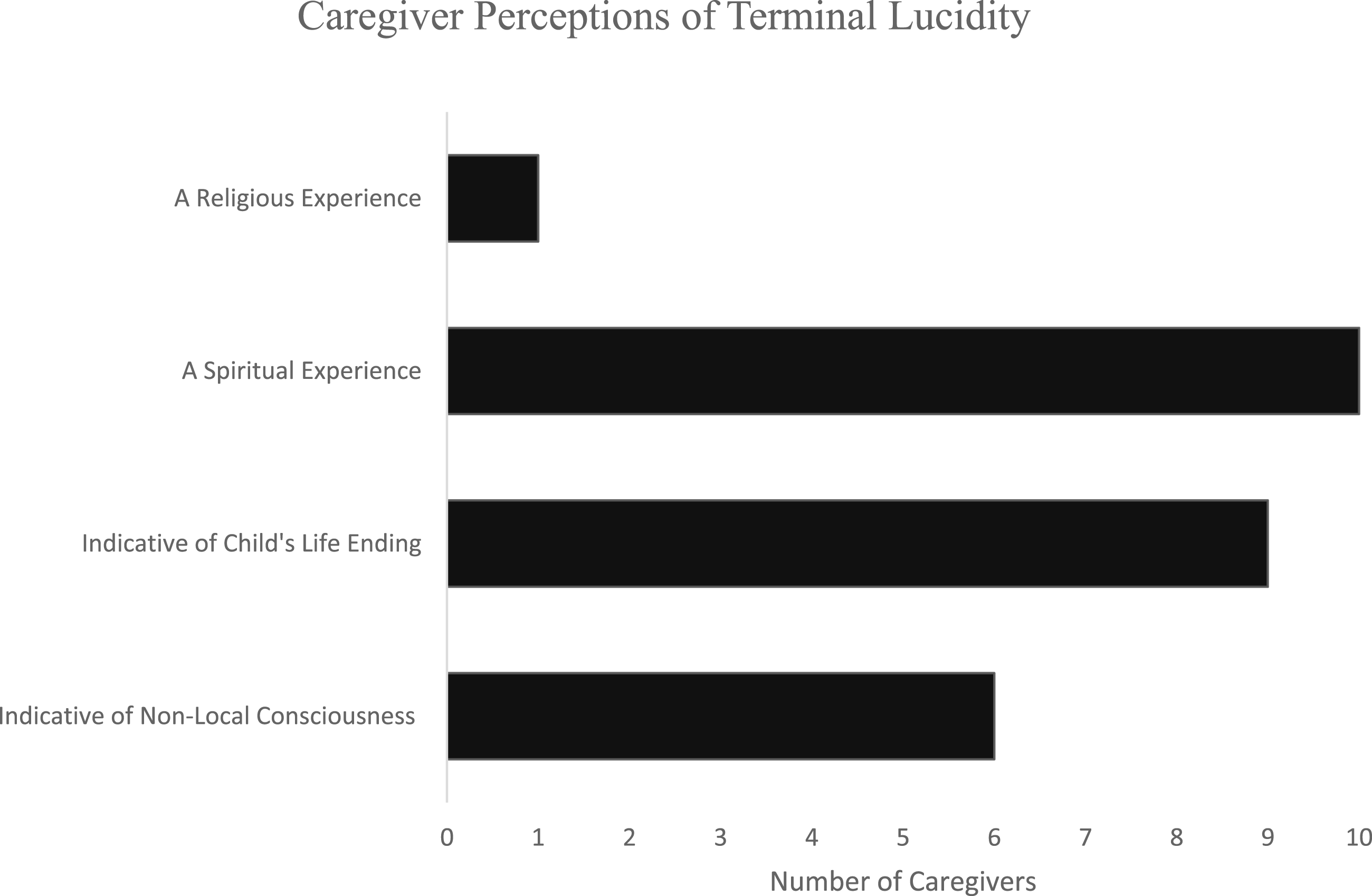
Emotional Valence
Caregivers were asked, “What impact did your lucidity experience(s) have on you?” to determine the emotional valence of the TL. The majority of the responses given by the caregivers indicated that witnessing TL was comforting. A similar number of responses also indicated it confirmed their spiritual beliefs. Notably, the responses to these questions were based on the individual TL experiences that each caregiver reported, rather than being a single response that reflected how caregivers perceived all the TL episodes they had witnessed. As shown in Figure 2, a minority of responses given by the caregivers indicated the TL they witnessed was distressing. The only participant to provide an open-ended response to this question indicated that witnessing TL in a child, “underscored my strong spiritual beliefs - nothing else I had witnessed was to this degree!” [Participant 6]. Emotional Valence of Witnessing TL in a Child, as Indicated by Caregivers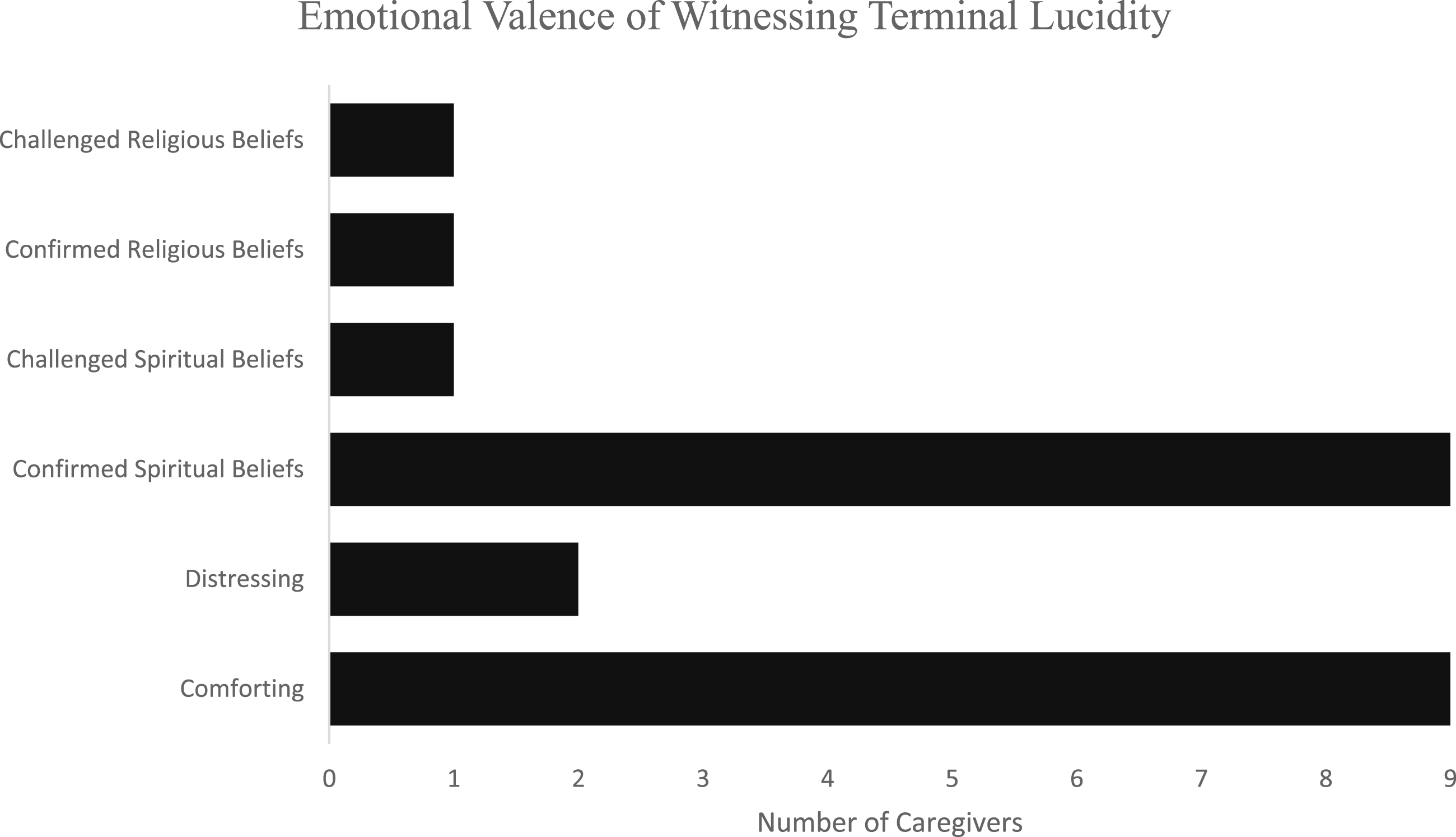
Influence on Belief Systems
To examine the influence on belief systems, we asked the question, “Has your experience of witnessing terminal lucidity in a child affected your own beliefs about life and death?” Figure 3 shows the impact of TL on caregivers’ belief systems. On average, caregivers’ beliefs about life and death were somewhat impacted by witnessing TL in children. The majority of responses given by the caregivers indicated it made them a more spiritual person, which aligns with the findings from Figure 2 above indicating that witnessing TL in a child confirmed their spiritual beliefs. The highlighted sense of spirituality overall is supported by open-ended responses from two participants, who indicated witnessing TL did not influence their beliefs as they already held spiritual ideologies: This did not change my spiritual beliefs, because I was already there with high spirituality, no fear of death, through my work with other children who were dying. [Participant 6] First, I had a near death experience earlier in my life, so I already was a more spiritual person and not afraid of death. [Participant 7] Influence of Witnessing TL in a Child on Caregiver Belief Systems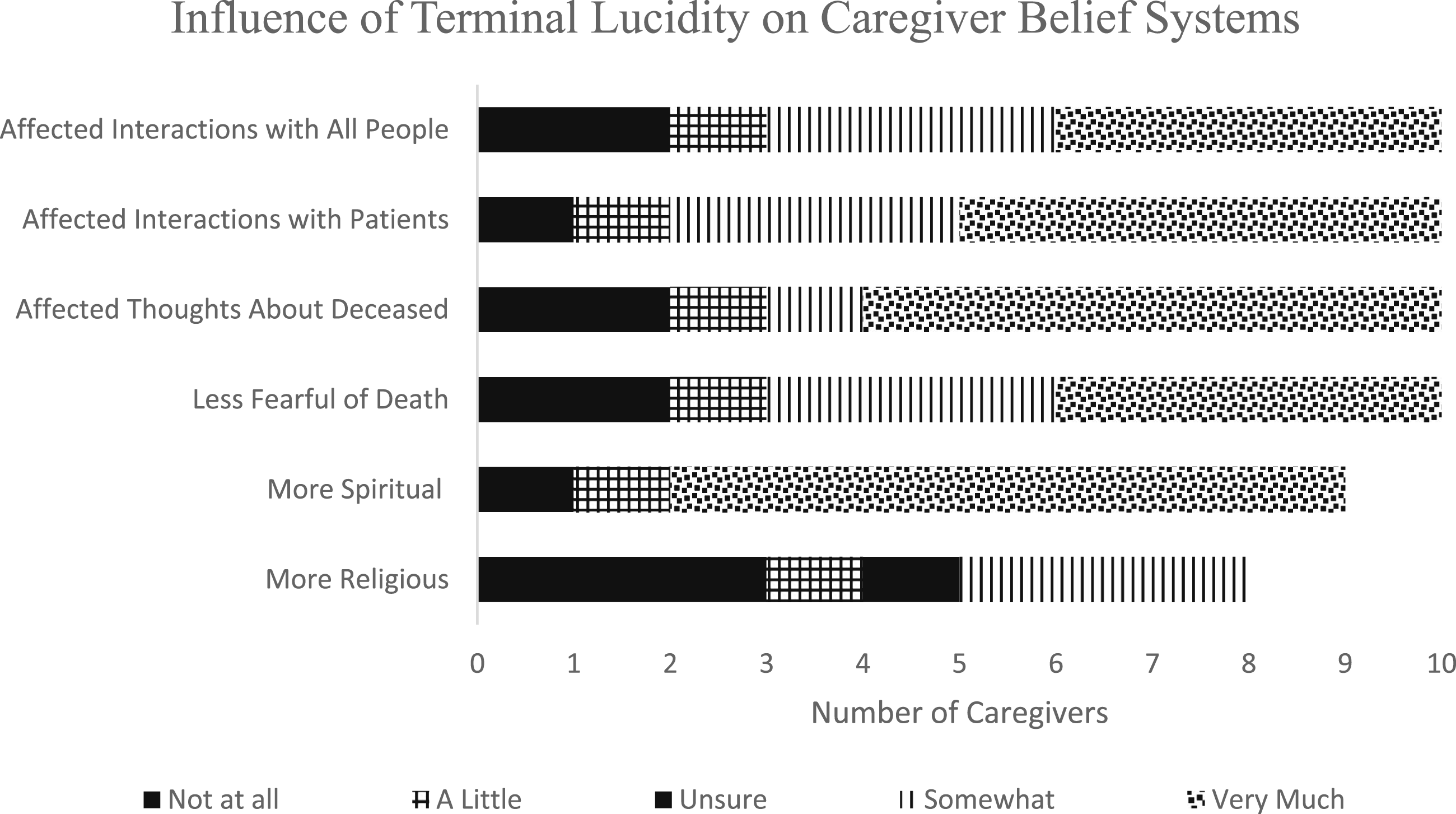
This finding of heightened or confirmed spirituality and/or beliefs contrasts with the finding of only one caregiver indicating that witnessing TL confirmed their religious beliefs. Many caregivers also indicated that witnessing TL affected the way they think about deceased loved ones, as well as the way they interact with patients with cognitive impairment.
Disclosure
We asked three questions relating to disclosure. In response to the question, “Have you disclosed your experience to others?” all caregivers indicated they had disclosed their experiences to others. We then asked, “To whom did you disclose details of the experience?” Responses indicated that caregivers had told family members, friends, and colleagues. Our final question asked, “What were the reactions of others to your witnessing lucidity?” Caregivers described others’ reactions ranging from very skeptical to very accepting. Some noted they were careful about whom they disclosed their experiences to. For example, one participant elaborated on the reactions of others in an open-ended response, stating that: I only share with those I feel comfortable with that I trust. I know there will be some who are skeptical and I would not want to dishonor the child’s precious experience. I am discerning in who I share these things with. [Participant 2]
Several caregivers noted that some colleagues tended to be skeptical. For instance: Other medical professionals tended to be more skeptical and/or uninterested, with some even challenging whether the events actually occurred. [Participant 5]
One participant who reported three cases, indicated that nurses were quite open to the phenomena, stating: Nurses began to share their practices with dying patients in non-responsive states. Nurses caring for these kids became connected. We could sense when a child died and many of us called the hospital asking about a very sick kid only to learn that they had passed a few moments ago. We could feel the children passing. [Participant 3]
Discussion
The purpose of this study was to examine the impact that witnessing TL in children had on caregivers by investigating how TL is perceived, its emotional valence, and its influence on belief systems. An additional area we explored was disclosure experiences: if caregivers disclosed the TL to anyone and what the reactions to those disclosures were.
Most caregivers in this sample perceived TL in a dying child to be a spiritual experience. Although we did not seek to examine the underlying mechanics of this perception (i.e., what caregivers thought made TL a spiritual experience), previous research suggests experiences often classified as spiritual are subjectively meaningful occurrences that involve a sense of transcendence of the self (Yaden & Newberg, 2022). The observable features of TL may appear to involve transcendence of the child beyond himself or herself and/or may involve a felt sense of transcendence in the witness. It is plausible these are the same features that caregivers in our sample considered when classifying TL as a spiritual experience. Regardless, that TL was perceived as spiritual might have important implications for caregivers of terminally ill children, as might the finding that most caregivers endorsed the TL experience as both comforting and confirming of their spiritual beliefs.
The synergy between the caregiver’s sense of spirituality and the patient’s spiritual experiences at the end-of-life has been identified as an important aspect of end-of-life care, seeing a common spiritual connection between caregiver and patient as a relational practice and shared journey (Batstone et al., 2020). Prior research (e.g., Holland & Neimeyer, 2005) has also shown increased salience of spirituality while caring for the terminally ill is a protective factor against burnout. Miller (2021) similarly discovered that those who more regularly and profoundly experience spiritual perception of life also have greater resilience to the diseases of despair (i.e., depression, anxiety, addiction and suicidality), and thus, better mental health, an innate sense of meaning in life even through suffering and challenges, and physiologically, a heathier brain with thicker cortices.
The caregivers in this sample are plausibly more resilient to burn out because they interpreted TL as a spiritual and comforting experience, rather than a pathological medical condition. From this perspective, remaining neutral about spirituality as a caregiver does not serve the spiritual needs of the dying child, and at the same time, may also lead to more stress and burnout for the caregiver. Since death impacts all humans, having a way to connect through this universal predicament is vital for caregivers of the terminally ill. Miller’s (2021) theory could help explain why caregiving for the terminally ill may actually deepen the capacity to perceive life through a spiritual lens and subsequently become more resilient to the challenges of caring for those with terminal illnesses.
A further compelling finding of this study is the influence of witnessing TL on a caregiver’s belief systems. One caregiver identified that they were religious and likewise found that witnessing TL in a child confirmed their religious beliefs. In this case, the caregiver witnessed the child interacting with “A light and the presence of Christ” during TL. Perhaps because the caregiver had a Christian background, they more readily felt comforted and were able to use their existing religious beliefs as a reference point for making sense of the TL in this child. Having knowledge of religious and spiritual figures that may become relevant to the dying child during TL as one of several ways to explain or understand TL, may deepen the meaning of the experience and reduce distress in the caregiver. Notably however, the majority of caregivers indicated they were comforted by the TL and had a decreased fear of death after witnessing TL in a child.
Similar findings from a rich body of literature on near-death experiences (NDE) have found that both those who have had an NDE as well as those who learn about NDEs report many positive changes, including a reduced fear of death (Greyson, 2006; Long & Woollacott, 2024; Tassell-Matamua et al., 2017). These overlapping findings suggest the fear of death may be inversely related to a capacity for spiritual perception, because when one either directly experiences coming close to dying (an NDE), learns about others who almost died, or witnesses TL in a dying person, their own fear of death decreases while their sense of spirituality increases. Witnessing TL, like learning about NDEs, can increase a sense of the interconnected nature of beings, where being a second-hand witness to the experience has similar effects to those of the experiencer themselves, and also illuminates the way death serves to awaken a sense of spiritual perception that, according to Miller’s (2021) work, is an innate capacity in all humans.
An additional implication of this finding of a reduced fear of death may relate to the care given to dying children. In westernized societies, death is often conceptualized as negative or something to be fought at all costs, which limits the expression of the positive aspects of dying and degrades the possibility of dying a “good death” (see Cottrell & Duggleby, 2016). One of the caregivers in the present study described that TL tended to occur in the dying child only after the decision to halt life-saving procedures and shift to palliative care. The caregiver noted it is a more common practice in treating terminally ill children to delay the shift to palliative care as long as possible, which sometimes results in the child dying suddenly in the ICU. Palliative care focuses on comfort rather than life-saving procedures, creating a gentler transition from life to death, and possibly increasing the likelihood of TL occurring; however, more research is needed to verify this claim. Future research should continue to explore how the fear of death, especially in caregivers of terminally ill children, may impact end-of-life decision-making and interfere with a child’s ability to have a “good death.”
Most caregivers perceived TL as signaling that the child was close to dying, while also indicating that consciousness is independent of brain activity. Both perceptions of TL contradict dominant reductionist models that view consciousness as a biproduct of brain activity. Yet, caregivers who witness TL feel otherwise, as they experience a person’s normal or even expanded state of consciousness unexpectedly arising after a period of severe cognitive impairment. These findings build a case for improved death literacy that considers alternative metaphysics of the nature of consciousness that are more aligned with the actual experience of witnessing TL.
It should be noted that while the emotional valence of witnessing TL was mostly considered to be comforting, in two cases of TL the caregivers reported that it was also a distressing experience. These findings are similar to prior research that found a small percentage of lucidity episodes witnessed were stressful or induced a mixture of hope and confusion (Griffin et al., 2022). The authors attributed this finding to caregivers not knowing what lucidity episodes are, confusing momentary lucidity as a sign that the person was getting better, and/or knowing that lucidity often signals death is near and thus experiencing grief for the dying person. The current study did not ask caregivers why they felt TL was distressing, and so no definitive conclusions can be drawn from our findings. However, it is worth noting that witnessing TL is a complex emotional experience that may affect caregivers differently depending on their own pre-existing beliefs, relationship to the dying person, and degree of death literacy. For example, TL may be distressing to witness if it challenges prevailing beliefs and scientific discourses that imply consciousness arises exclusively from brain activity. Thus, we reassert our position that caregivers of the terminally ill be educated in multiple theoretical orientations to equip them for end-of-life experiences that are not adequately explained or understood when only using a reductionist model of consciousness (Perera et al., 2025). Additionally, a general understanding and open-mindedness towards multi-cultural and multi-faith perspectives on spiritual and religious beliefs of the patient may help caregivers recognize TL, and consequently, feel less distressed or confused by what they witnessed.
Finally, caregivers were asked if they shared their TL with others and what kind of reaction they received to their disclosure. It is important to acknowledge stigma exists around disclosure of death-related experiences and this may prevent such experiences from being studied and recognized more broadly in the healthcare community (Holden et al., 2014). In the case of the current sample, all caregivers reported they had shared the TL experience with others, both personal connections and colleagues, and received a mixture of accepting and skeptical responses. Healthcare providers were noted to be the most skeptical of TL, except in one case, where those who had worked closely with the dying child came to feel a connection with the child. Prior work has found that the fear of not being perceived as credible or competent is a common reason for healthcare providers not to share the experience of witnessing TL with colleagues (Brayne et al., 2008). While in many cases this may still be true, this study found other colleagues were comforted and inspired to learn of the TL their colleague had witnessed. The results of this study shed light on the need for greater education around end-of-life experiences for healthcare providers, which could reduce the stigma of disclosing TL to colleagues, and in turn, provide much needed peace and comfort to the caregivers of terminally ill patients.
Limitations
While our findings provide some useful insights into the ways witnessing TL in children impacts caregivers, they are not without limitations. Notably, our recruitment approach utilized acquaintanceship networks, which may have led to selection bias. All authors of the present study are known researchers in the fields of near-death studies, exceptional human experiences, and end-of-life experiences. It is likely participants who were also collegial acquaintances were aware of what TL is, and possibly more inclined to endorse spiritual perspectives. They may have been more eager to complete the survey as their experience was largely a positive one that confirmed their beliefs. The findings may look different in a randomized sample of caregivers, and particularly those with no prior understanding of TL.
Conclusion
Research into TL is still in its infancy. Yet, what is known about TL to date is that it appears to be a profoundly moving experience for the dying, and a potentially transformative experience for those who witness it. Although much of what is known about TL comes from studies of adults, examining TL in children more thoroughly is a necessary part of understanding the full manifestation of this phenomenon across the lifespan. The findings of the present study suggest witnessing TL in children may initiate a spiritual transformation that has similar implications to posttraumatic growth or the changes often found in those who have had an NDE or who have been educated about NDEs. While the underlying mechanics of such change remain to be determined, the implications for enhancing end-of-life care and creating ‘space’ for TL to be perceived as a natural part of the dying process in terminally ill children, remain enormous. We therefore encourage more systematic investigations into the impacts of witnessing TL in children.
Footnotes
Acknowledgements
We wish to thank Professor Allan Kellehear and Dr Alex Gomez-Marin for their contributions to our research team over the past several years.
Ethical Considerations
The Massey University Human Ethics Committee, Aotearoa New Zealand, provided ethical approval for the study (Southern A, Application 22/52).
Consent to Participate
All participants were given information detailing the study aims and were required to give consent electronically before participating in the survey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Bial Foundation (Application ID: 129/2022).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the data, it is not openly available online. However, it is available by making a request to the corresponding author.