
Abstract
Previous reviews on Prolonged Grief Disorder (PGD) treatments were done before it became an official diagnosis, which makes it important to compare the effectiveness of current psychological and pharmacological interventions. In our systematic review and network meta-analysis, multiple databases were searched for randomized controlled trials up to November 2023. The primary outcome was reduction in PGD symptoms, while the secondary outcomes were reduction in symptoms of depression and PTSD. The search strategy resulted in a final sample of 40 eligible studies, which contained data from 4566 participants. This study showed that the most effective treatments for PGD contained an element of exposure, social support, narrative reconstruction, artistic expression, and a cognitive-behavioral aspect. Our study provides a comprehensive synthesis of available evidence on the effectiveness of psychological PGD treatments in adults. However, there was insufficient data for pediatric treatments and pharmacological interventions. This study was registered with PROSPERO (CRD42023477050).
Keywords
Introduction
Grief is a natural reaction to the death of a loved one or a non-death related loss. Usually, the grieving process ends in healing and adjustment to the loss, but in approximately 7–10% of bereaved individuals grief can become dysfunctional and develop into a Prolonged Grief Disorder (PGD) (Kersting et al., 2011; Lundorff et al., 2017). Previously referred to in the literature as complicated grief and persistent complex bereavement disorder (PCBD), PGD was recently included into the 11th edition of the International Classification of Diseases (ICD-11) and the revised fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) (American Psychiatric Association [APA], 2022; Maciejewski et al., 2016; World Health Organization [WHO], 2019). According to ICD-11, PGD is a maladaptive grief reaction accompanied by longing and preoccupation with the deceased, emotional pain or numbness, disruptions in daily functioning, and has lasted for longer than six months (WHO, 2019). DSM-5-TR offers similar diagnostic criteria for PGD, but unlike ICD-11, it indicates that PGD can only be diagnosed after 12 months have elapsed since the loss of a loved one in adults (six months in the case of children and adolescents), and adds symptoms such as identity disruption, avoidance of the reminders of death of the loved one, feeling that life is meaningless, and intense loneliness (APA, 2022).
Psychological Comorbidities
PGD can be particularly harmful to the individual as it is often comorbid with such disorders as depression and post-traumatic stress disorder (PTSD). For example, in their longitudinal study on bereaved individuals, Komischke-Konnerup et al. (2023) found that early severe symptoms of PGD were associated with the development of PTSD and depression. Moreover, with the progression of grief, the relationship between PTSD, depression, and PGD becomes more intertwined (Komischke-Konnerup et al., 2023). Nevertheless, while depressive disorders, PTSD, and PGD share similar symptoms, PGD possesses unique core symptoms (e.g., yearning and preoccupation with the deceased) and is distinguished as its own disorder (Bui et al., 2012; Komischke-Konnerup et al., 2023).
Depressive disorders are one of the most common comorbidities with PGD. According to DSM-5, major depressive disorder (MMD) is characterized by an overall depressed mood, feelings of worthlessness, diminished interest in daily activities, fatigue, and recurrent thoughts of death (APA, 2022). MDD might also occur after bereavement, which is known as bereavement-related depression (APA, 2022). Although bereavement-related depression shares some similarities with PGD, these two conditions have distinct core characteristics. Unlike depressive disorders, PGD can be distinguished by its core symptoms of yearning and preoccupation with thoughts or memories of the deceased person (Komischke-Konnerup et al., 2023). Notably, co-occurrence of depression and PGD might be particularly high in the elderly population (O’Connor et al., 2014).
Following depression, post-traumatic stress disorder (PTSD) is the second most common comorbidity in PGD. PTSD is a psychological condition that frequently develops after a person directly experiences, witnesses, or otherwise experiences some kind of a traumatic event. Its symptoms include re-experiencing, avoidance, negative feelings and thoughts, and hyperarousal (APA, 2022). PTSD and PGD both fall under the category of trauma- and stressor-related disorders and can co-occur, especially in the case of traumatic loss, where the death was either violent, unexpected, or overall traumatizing to the survivor. Similar symptomatology and high co-occurrence rate of PGD and PTSD indicate that the same mechanisms might be at play in these disorders (Eddinger et al., 2021). Nevertheless, while PTSD emerges as a severe fear response to traumatic experiences, PGD results from the major loss of an attachment figure and difficulty processing the loss (Bui et al., 2012).
Treatments for PGD
Some of the examples of existing psychological interventions that have been used to treat PGD include Cognitive Behavioural Therapy (CBT), Eye Movement Desensitization and Reprocessing (EMDR), Narrative Reconstruction (NR), and Interpersonal Therapy (IPT) (Abdul Samad et al., 2023; Duffy & Wild, 2023; Elinger et al., 2023; Yasar et al., 2017). Another therapy for PGD is called Complicated Grief Therapy (CGT). This relatively new therapy combines elements of both IPT and CBT, namely exposure techniques, and focus on the relationships and personal goals. It is tailored specifically to meet the needs of PGD patients and has proved to be effective in past studies (Wetherell, 2012). In terms of pharmacological treatments, such pharmacotherapies as antidepressants, addiction treatments, and psychedelics, might also be effective in reducing symptoms of PGD (Bui et al., 2012; Gang et al., 2021; Low & Earleywine, 2023).
Previous Systematic Reviews
The most recent systematic reviews on the treatments for PGD for adults were performed by Wittouck et al. (2011) and Johannsen et al. (2019). Wittouck et al. (2011) examined the effectiveness of both interventive and preventive treatments for PGD in adults by reviewing 14 randomized controlled trials (RCTs). Nine of the RCTs concerned preventive interventions, while five of the RCTs involved interventive grief treatments. Grief treatments that employed cognitive-behavioural techniques were found to be the most effective in reducing PGD symptoms. Interestingly, it was found that, unlike post-loss treatments, preventive grief interventions were not consistently effective, suggesting that PGD might not be prevented (Wittouck et al., 2011). Overall, this review offers important information on the treatments for PGD, but since this study was performed over 10 years ago and included only five interventive PGD treatments, it can be considered outdated as more treatments have been developed and tested since its publication. Furthermore, this study was performed before PGD became an official diagnosis and did not include pharmacotherapies.
Johannsen et al. (2019) performed another systematic review of PGD treatments in adults, which included 32 RCTs. Their main finding was that individually delivered interventions were more effective in reducing PGD symptoms than group interventions. Moreover, psychological interventions led to significant reduction in depressive, PTSD, and distress symptoms. This study also provides important information about treatments for PGD. Yet it has been performed before the inclusion of PGD into DSM-5-TR and only followed diagnostic criteria outlined in ICD-11. As was mentioned earlier, in ICD-11, PGD can be diagnosed six months post-loss, while DSM-5-TR states that in adults, PGD can be diagnosed only after 12 months since the death of a loved one. Therefore, if PGD treatments are reviewed from the DSM-5-TR perspective, interventions that were initiated before 12 months post-loss can be considered preventive interventions that might be treating normal grief. Furthermore, this study also did not include pharmacological treatments for PGD.
In summary, although some systematic reviews and meta-analyses have been performed to test the effectiveness of treatments for prolonged grief, they did not follow the new DSM-5-TR diagnostic criteria for PGD, did not include pediatric populations, and did not include pharmacological treatments. In addition, those reviews did not conduct a network meta-analysis (NMA), which, unlike traditional meta-analysis, allows comparison of various treatment arms across trials simultaneously. Thus, it is important to explore areas not covered in previous systematic reviews, including treatments for PGD in children and adolescents and pharmacological treatments. In addition, there is a need to compare studies that have followed the diagnostic criteria listed in both ICD-11 and DSM-5-TR in order to reduce confusion regarding the concept of PGD and its core symptoms.
Current Study
Considering the aforementioned limitations of the previous reviews, the main goal of our study was to collect and meta-analyze information on the psychological and pharmacological treatments for PGD. Our systematic review aimed to investigate the effectiveness of existing interventions while considering the new criteria for PGD diagnosis. By conducting a thorough analysis of the literature, we strived to provide an accurate understanding of the current psychological treatments and expand our current knowledge of the effective treatments by discussing pharmacological treatments.
Our study attempted to answer the following questions: (1) What psychological treatments are available for PGD? (2) What pharmacological treatments are available for PGD? and (3) What are the most effective treatments for PGD? Our main hypothesis was that psychological interventions designed specifically to address prolonged grief would be more effective in treating PGD than general treatments. We also hypothesized that pharmacological interventions previously successful in treating PGD’s comorbidities (i.e., depression, PTSD) would be effective in reducing prolonged grief symptoms. Our primary outcome was pooled effectiveness of those treatments (i.e., reduction in PGD symptoms). Our secondary outcomes were reduction in symptoms of depression and PTSD.
Methods
This systematic review and network meta-analysis (NMA) was conducted according to a prespecified protocol registered in PROSPERO (CRD42023477050). This review is also available on the Open Science Framework (OSF) website: doi.org/10.17605/osf.io/tbrv6. This review was reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Hutton et al., 2015; Moher et al., 2015; Page et al., 2021). See eTable 1 in the appendix for more details.
Data Sources and Searches
PsycINFO, MEDLINE, Embase, ERIC, Cochrane Library, and CINAHL were searched up to November 2023, without restricting location, language, publication date, or participant age. Clinical trial registries were also searched, including clinicaltrials.gov, clinicaltrialsregister.eu, and anzctr.org.au. Additionally, a grey literature search was conducted. Relevant studies, which were not discovered by online database searches, were manually investigated from the reference lists of already included research papers. See eTable 2 in the appendix for the full list of search terms and Boolean operators.
Study Selection
Four reviewers (AP, CO, JT, AB) independently examined titles and abstracts using the online Covidence systematic review program, once duplicates had been removed (Covidence, nd). The same reviewers evaluated full-text articles to decide which articles met the selection criteria and were retrieved for detailed review. In case of disagreement, reviewers negotiated to reach a consensus. Studies were considered suitable for inclusion in this systematic review if they satisfied all of the following requirements: (1) included participants that met the ICD-11 or DSM-5-TR criteria for diagnosis of PGD or were identified as having prolonged grief based on previously used criteria (i.e., before 2019); (2) were treatment-based studies that used random assignment and had a control group; (3) included a quantitative measure of PGD symptoms; and (4) reported pre- and post-therapy symptoms. We defined psychological treatments as treatments administered by psychologists, therapists, medical doctors, or other health professionals, which involve cognitive-behavioural, emotional-supportive, or psychoeducational content. Pharmacological treatments were defined as treatments administered by health professionals, which use a psychoactive medication intended to treat PGD symptoms.
The following exclusion standards were used: (1) study designs that did not meet the research design criteria above (e.g., case reports, review papers, opinion pieces, conference abstracts, and editorials devoid of original data); (2) studies using non-psychological and non-pharmacological treatments (e.g., massage, acupuncture, alternative medicine); (3) studies including types of loss other than live-born person loss (e.g., pet loss, job loss, prenatal loss, stillbirth); (4) studies initiated prior to the loss (e.g., palliative care) or employing preventive treatments; and (5) interventions aimed at healthcare professionals working with grief (e.g., medical practitioners, nurses).
Non-psychological and non-pharmacological treatments were excluded because the focus of this review was on evidence-based therapies that incorporate an active psychological component or a psychoactive medication. The reason for excluding studies with therapies designed to prevent development of PGD was due to participants in those studies not meeting the PGD criteria outlined in ICD-11 and DSM-5-TR, as the loss occurred less than six months ago. Moreover, we focused on interventive treatments only, because previous research found that preventive treatments for prolonged grief tend to be ineffective (Wittouck et al., 2011). Studies on perinatal loss were excluded for the purpose of obtaining a homogeneous sample, due to the fact that those studies often included both prenatal and postnatal losses, so it would be difficult to separate participant scores for the analysis. However, we recognize that by excluding perinatal loss, we inadvertently neglected a cohort of bereaved parents, whose grief is often disenfranchised. Therefore, it would be important to include perinatal loss in future systematic reviews on PGD treatments. If a study did not contain sufficient information to judge eligibility, the corresponding authors were contacted. If they did not respond, then the study was excluded.
Data Extraction and Risk-of-Bias Assessment
Five investigators (AP, CO, JT, MF, AB) reviewed all data extractions for completeness and accuracy and also independently assessed the quality of the studies included in the meta-analysis. Disagreements were resolved by consensus. All data were extracted in duplicate and included: (1) study characteristics (author, publication year, country, study design, sample size); (2) participant details (relationship to the deceased, time elapsed since loss, cause of death, mean ± SD age, percent of female participants); and (3) treatment characteristics (type of intervention, control, treatment duration, and treatment outcome). The subsequent clinical outcome data were duplicated and extracted for NMA: (1) mean ± SD PGD, depression, and PTSD symptom scores at baseline, post-treatment, and follow-ups; and (2) sample size per treatment group. If there was a secondary analysis or a follow-up study that was published separately, it was merged with the primary study and treated as a single study. If an article only provided confidence intervals or standard error, then standard deviations (SDs) were obtained using the methods described in the Cochrane Handbook (Higgins et al., 2023). Additional data were collected by contacting corresponding authors, accessing clinicaltrials.gov, and obtaining follow-up articles.
Risk of bias was evaluated using the Cochrane Collaboration’s tool (i.e., RoB 2) for assessing risk of bias (Higgins et al., 2023). Quality assessment did not influence the decision to include studies in the network meta-analyses. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to evaluate the quality of evidence associated with the results in the NMA (Puhan et al., 2014). The strength of evidence was graded as high, moderate, low, or very low in five domains: risk of bias, imprecision, inconsistency, indirectness, and publication bias. Two reviewers (DD, AB) assessed each domain for each outcome and determined an overall grade. Differences were resolved by consensus.
Data Synthesis and Analysis
To account for potential variations among studies, we conducted a series of DerSimonian and Laird random-effects meta-analyses on eligible studies (DerSimonian & Laird, 2015). The primary focus was on overall effectiveness of the treatments on PGD symptoms, and the key statistic used for the meta-analysis was the pooled effectiveness. Due to the differences in PGD symptom scales and the principal summary measures used across the majority of meta-analyses, effect sizes were calculated as Hedges g. Hedges g were reported as the standardized mean difference (SMD) of PGD, depression, and post-traumatic stress disorder (PTSD) symptom scores at post-treatment and available follow-ups. Thus, the likelihood of a reduction in PGD, depression, and PTSD symptoms in participants who received a similar intervention was compared to a control.
Treatment effects between individual intervention arms were evaluated using a random-effects multivariate NMA assuming consistency and a common heterogeneity across all comparisons in the network model (Caldwell et al., 2005). Baseline characteristics (e.g., age, type of loss) that might modify the treatment effect were restricted using an a priori inclusion criteria to prevent inconsistencies from being introduced into the model. Publication bias was assessed through a network comparison-adjusted funnel plot (Chaimani et al., 2013). Statistical heterogeneity was assessed using the I 2 statistic (Higgins & Thompson, 2002). Interrater reliability for title and abstract screening was calculated using the kappa statistic. All effect sizes with a p < .05 were considered significant, while SMD of 0.2 represented a small effect, 0.5 a medium effect, and 0.8 a large effect (Cohen, 1988). All analyses were conducted using R code, and graphical representations displaying the effectiveness of treatments (treatment vs. control condition) were generated (Harrer et al., 2022; R Core Team, 2021; RStudio Team, 2020).
Role of the Funding Source
There was no funding source for this study.
Results
The search strategy generated a total of 3190 records. After removal of duplicates, the total number of records was 1882 unique citations, from which 1796 citations were excluded after reviewing title and abstract. Interrater reliability between the four independent reviewers in the abstract and full-text screenings was moderate (κ = .44). A total of 86 articles were retrieved for full-text review. Of these, 40 primary studies and five follow-up studies were eligible for inclusion. Additional data for one study was acquired from the author (Acierno et al., 2021). Three other studies were excluded from the meta-analysis due to no response from the contacted authors (Harrsen et al., 2022; Piper et al., 2007; Shear et al., 2016). This yielded the final sample of 37 studies included in the NMA. The grey literature search did not result in any additional studies.
Reasons for exclusion were study protocols (n = 11), wrong outcomes (n = 10), wrong study design (n = 9), absence of full text (n = 6), wrong intervention (n = 4), wrong patient population (n = 4), incomplete study (n = 1), and a review paper (n = 1). Fifteen of the studies that were included in the previous systematic review by Johannsen et al. (2019) were not included in our study due to them not meeting our inclusion criteria (i.e., participants in those studies did not meet the criteria for PGD and the treatment was initiated prior to the loss or before a minimum of six months had elapsed since the death of a loved one). The study selection process is shown in Figure 1. Prisma flow diagram of systematic search and included studies.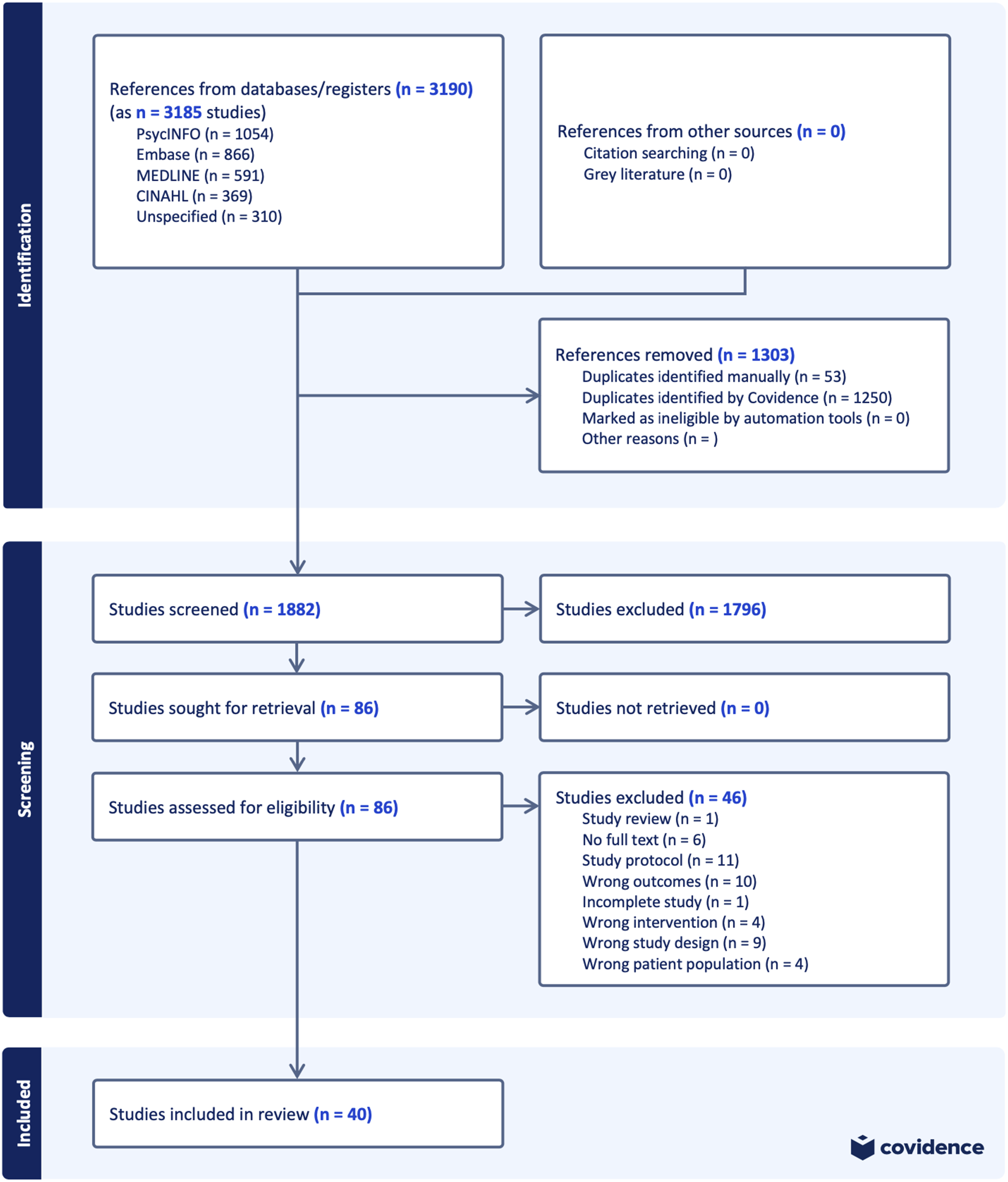
Study and Participant Characteristics
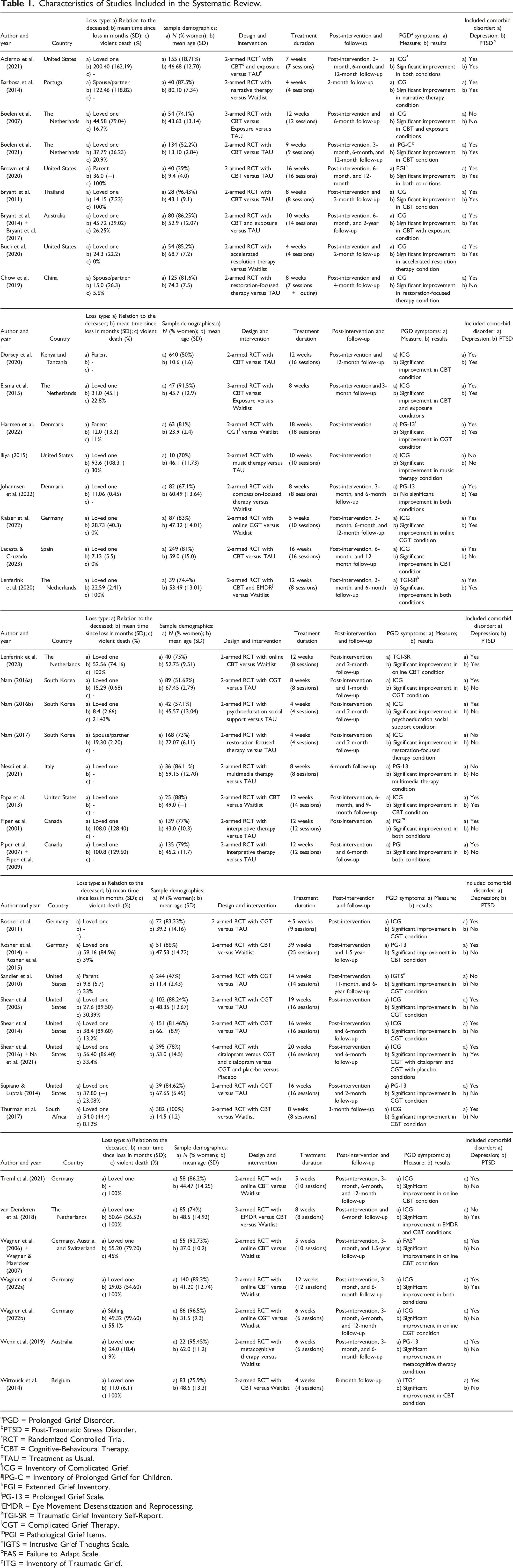
Characteristics of Studies Included in the Systematic Review.
aPGD = Prolonged Grief Disorder.
bPTSD = Post-Traumatic Stress Disorder.
cRCT = Randomized Controlled Trial.
dCBT = Cognitive-Behavioural Therapy.
eTAU = Treatment as Usual.
fICG = Inventory of Complicated Grief.
gIPG-C = Inventory of Prolonged Grief for Children.
hEGI = Extended Grief Inventory.
iPG-13 = Prolonged Grief Scale.
jEMDR = Eye Movement Desensitization and Reprocessing.
kTGI-SR = Traumatic Grief Inventory Self-Report.
lCGT = Complicated Grief Therapy.
mPGI = Pathological Grief Items.
nIGTS = Intrusive Grief Thoughts Scale.
oFAS = Failure to Adapt Scale.
pITG = Inventory of Traumatic Grief.
Among the included 40 RCTs, 36 were 2-armed studies, three were 3-armed studies, and one was a 4-armed study. The mean treatment duration was 10.54 weeks. In total, there were 16 unique interventions, which included Cognitive-Behavioural Therapy (CBT), Complicated Grief Therapy (CGT), Online CBT, Exposure Therapy, Eye Movement Desensitization and Reprocessing (EMDR), Restoration-Focused Therapy, Online CGT, Interpretive Therapy, Narrative Therapy, Compassion-Focused Therapy, Accelerated Resolution Therapy (ART), Metacognitive Grief Therapy, Music Therapy, Psychoeducation with Social Support (PSS), Multimedia Therapy, and Citalopram. Moreover, in several studies, interventions were combined: CBT with Exposure, CBT with EMDR, Citalopram with CGT, and CGT with Placebo. There were three types of control conditions: Waitlist Control, Treatment as Usual (TAU), and Placebo. In terms of comorbid disorders, 34 studies examined depressive symptoms, and 18 studies examined PTSD symptoms.
Primary Analysis
The most common comparisons were CBT versus Control (n = 11), Online CBT versus Control (n = 7), and CGT versus Control (n = 7) (Figure 2). In all network plots, nodes are weighted according to the number of studies, including the respective interventions. The numbers in each line show the exact number of studies that were included in the corresponding comparison. Several treatments indicated high effectiveness (SMD >.80). For the studies that examined PGD treatments for children and adolescents, only five studies were available for analysis and only two types of treatments were included, which were CBT and CGT. Thus, there was not sufficient data for the network meta-analysis. See eFigures 8–13 in the appendix for the network and forest plots for PGD, comorbid depression, and comorbid PTSD treatments in children. Network plots for adult PGD treatments. (a) Adult PGD treatments at post-treatment; (b) adult PGD treatments at short-term follow-up; (c) adult PGD treatments at six-month follow-up; (d) adult PGD treatments at long-term follow-up. CG – Complicated Grief; CBT – Cognitive-Behavioural Therapy; EMDR – Eye Movement Desensitization and Reprocessing.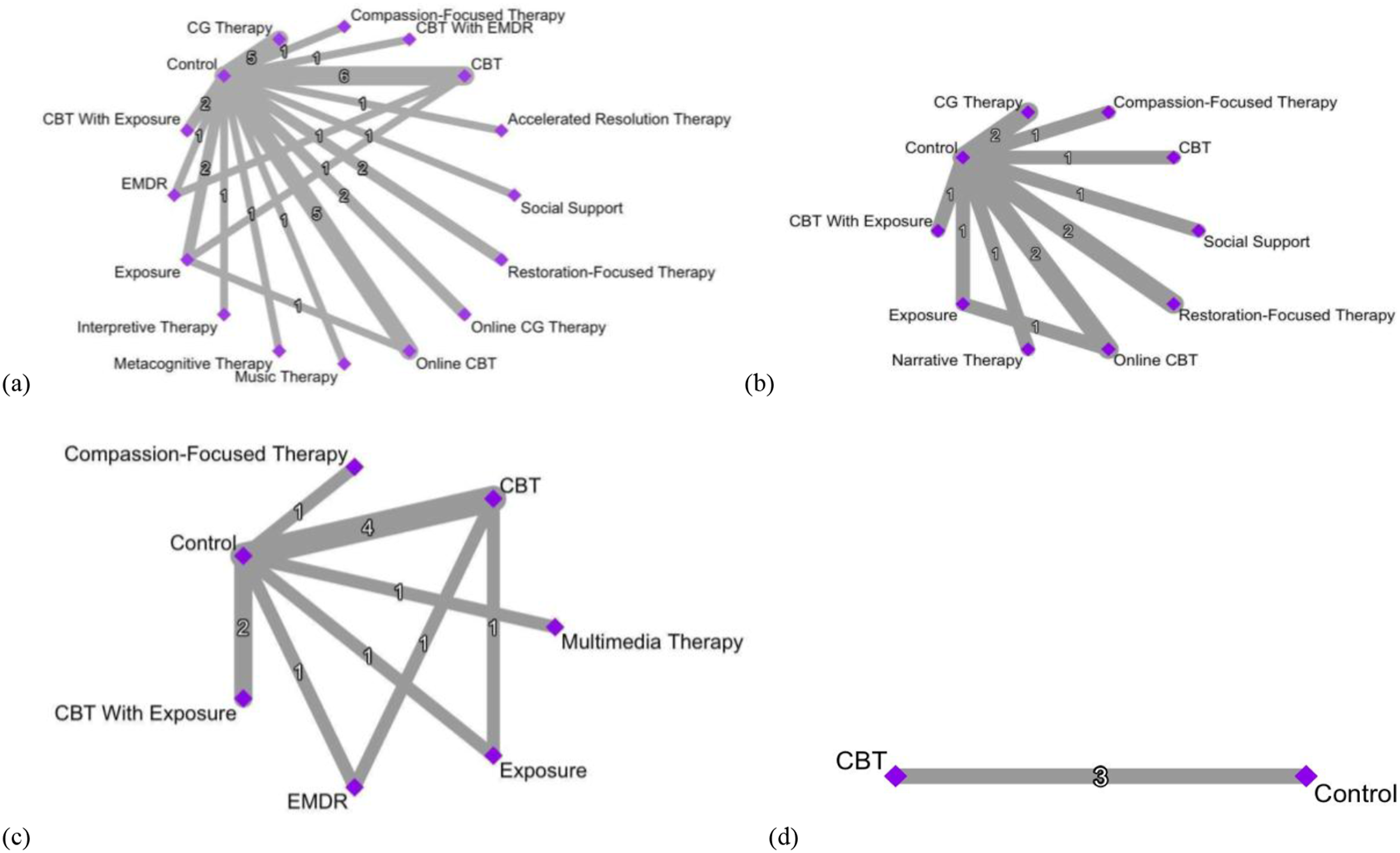
For adult PGD interventions, Accelerated Resolution Therapy (SMD = −1.86, 95% CI [−3.09, −0.63], p = .003), Psychoeducation with Social Support (SMD = −1.86, 95% CI [−3.11, −0.61], p = .004), Metacognitive Therapy (SMD = −1.65, 95% CI [−3.05, −0.25], p = .02), Music Therapy (SMD = −0.89, 95% CI [−2.54, 0.76], p = .29), Exposure Therapy (SMD = −0.89, 95% CI [−1.66, −0.11], p = .03), and CBT (SMD = −0.84, 95% CI [−1.33, −0.35], p = .001) were associated with the highest effect sizes in the post-treatment (Figure 3(a)). Heterogeneity was considerable (I
2
= 81%; p < .0001), which indicated that the studies were significantly different from each other (e.g., population type, type of loss). See eFigure 1(a) in the appendix for a heat plot of inconsistency within the network. Forest plots for adult PGD treatments. (a) Adult PGD treatments at post-treatment; (b) adult PGD treatments at short-term follow-up; (c) adult PGD treatments at six-month follow-up; (d) adult PGD treatments at long-term follow-up. CBT – Cognitive-Behavioural Therapy; CG – Complicated Grief; EMDR – Eye Movement Desensitization and Reprocessing.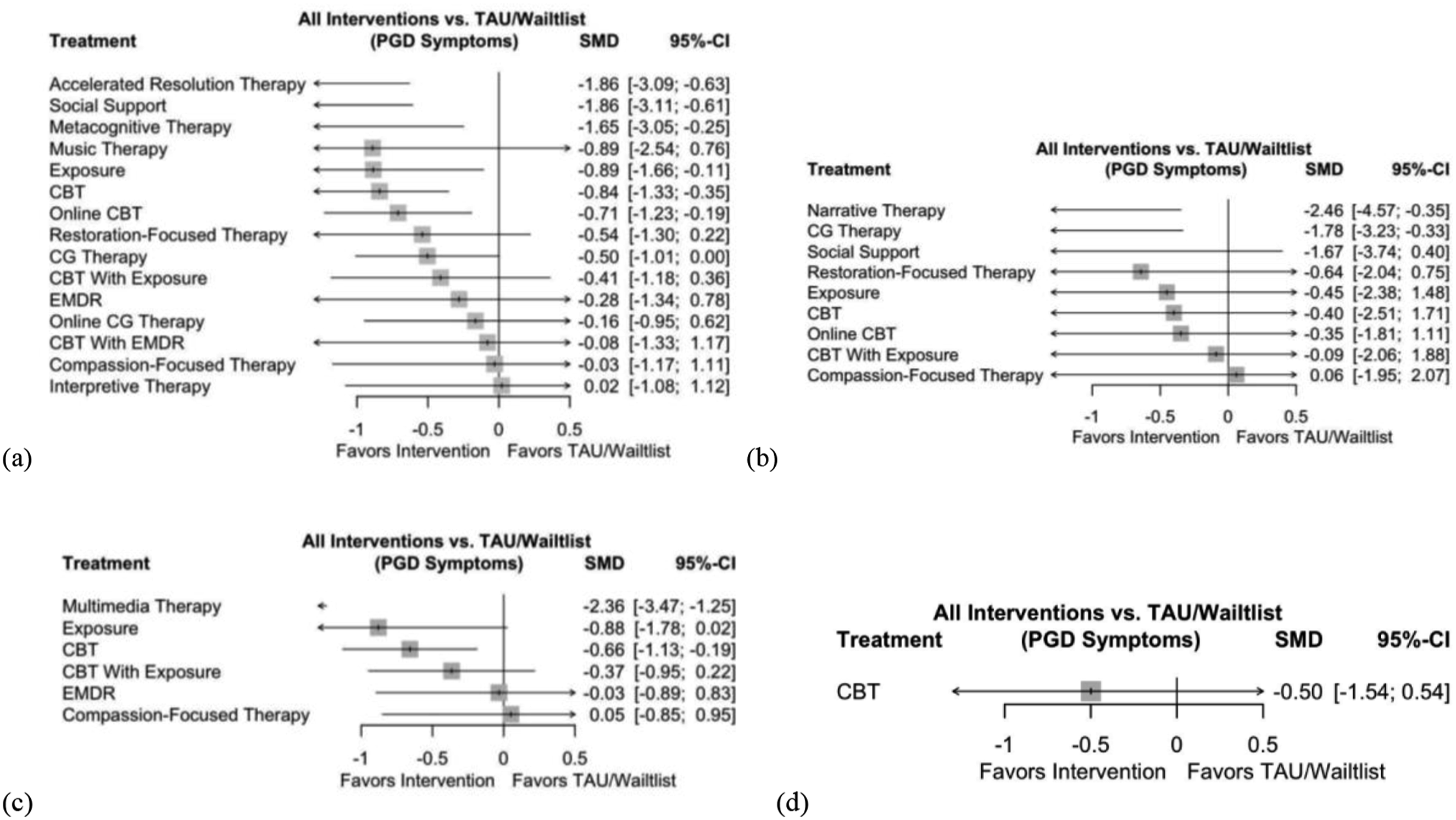
Narrative Therapy (SMD = −2.46, 95% CI [−4.57, −0.35], p = .02), CGT (SMD = −1.78, 95% CI [−3.23, −0.33], p = .02) and Psychoeducation with Social Support (SMD = −1.67, 95% CI [−3.74, 0.40], p = .11) were the most effective treatments in the short-term follow-up (Figure 3(b)). Heterogeneity was considerable (I 2 = 94%; p < .0001). Multimedia Therapy (SMD = −2.36, 95% CI [−3.47, −1.25], p < .0001) and Exposure Therapy (SMD = −0.88, 95% CI [-1.78, 0.02], p = .06) were the most effective treatments in the six-months follow-up (Figure 3(c)). Heterogeneity was substantial (I 2 = 67.9%; p = .01). Long-term follow-up only had three studies that compared CBT to Control. There were no large effect sizes. Heterogeneity was considerable (I 2 = 92.4%; p < .0001).
Secondary Analysis
For the treatments of comorbid depression and comorbid PTSD, there was a similar trend as in the PGD treatments, with CBT versus Control (n = 10 and n = 7), Online CBT versus Control (n = 7 and n = 4), and CGT versus Control (n = 7 and n = 0) being the most common comparisons. However, more treatments indicated low effectiveness (SMD < .20) as can be seen in eFigures 3, 5, 11, and 13 in the appendix. See eResults in the appendix for results on the inconsistency within the networks.
Network plots for adult comorbid depression interventions are depicted in eFigure 2 in appendix. Metacognitive Therapy (SMD = −1.50, 95% CI [−2.95, −0.05], p = .04), Accelerated Resolution Therapy (SMD = −1.24, 95% CI [−2.51, 0.03], p = .06), and CBT (SMD = −0.83, 95% CI [−1.47, −0.20], p = .01) were associated with the highest effect sizes in the post-treatment (eFigure 3(a)). Heterogeneity was considerable (I 2 = 83.3%; p < .0001). Narrative Therapy (SMD = −1.61, 95% CI [−4.47, 1.25], p = .27) and Complicated Grief Therapy (SMD = −0.96, 95% CI [−2.96, 1.04], p = .35) were the most effective in the short-term follow-up (eFigure 3(b)), and heterogeneity was considerable (I 2 = 94.8%; p < .0001). There were no large effect sizes in the six-month (eFigure 3(c)) and long-term follow-ups (eFigure 3(d)). Heterogeneity was substantial (I 2 = 56.4%; p = .10) in the six-months follow-up and considerable (I 2 = 72.1%; p = .03) in the long-term follow-up.
Network plots for adult comorbid PTSD interventions are depicted in eFigure 4 in appendix. Accelerated Resolution Therapy (SMD = −1.71, 95% CI [−2.93, −0.49], p = .01) and Exposure (SMD = −1.21, 95% CI [−2.38, −0.03], p = .04) were associated with the highest effect sizes in the post-treatment (eFigure 5(a)). Heterogeneity was substantial (I 2 = 66.4%; p = .82). See eFigure 1(b) for the heat plot. Narrative Therapy (SMD = −3.66, 95% CI [−4.75, −2.57], p < .0001) was the most effective in the short-term follow-up (eFigure 5(b)). Heterogeneity was low (I 2 = 22.7%). There were no large effect sizes in the six-month (eFigure 5(c)) and long-term follow-ups (eFigure 5(d)). Heterogeneity was low in the six-months follow-up (I 2 = 38.5%) and unavailable for the long-term follow-up.
Risk-Of-Bias Assessment
The risk of publication bias was low, which is confirmed by the non-significant Egger scores of p = .38, p = .67, and p = .37 respectively (eFigure 6). Furthermore, as the treatments were organized in chronological order (i.e., from oldest to newest), there is no indication of any publication bias based on the time of publication of the studies. Quality assessment of RCTs is reported in Figure 4. Also see eFigure 7 in the appendix for the risk-of-bias summaries. Overall, risk-of-bias analysis indicates that almost half of the included studies had low risk of bias (n = 17), about a quarter of the studies had some concerns (n = 14), and the remaining studies had high risk of bias (n = 9). Almost all RCTs had a low risk of bias for Domain 1 (n = 37). RCTs had a higher risk of bias for Domain 3 (n = 6). There were more RCTs with some concerns of bias for Domain 2 (n = 9), Domain 4 (n = 10), and Domain 5 (n = 19). See eTable 3 in the appendix for GRADE risk-of-bias assessment. Risk-of-bias graph for RCTs. Review authors’ judgments about each risk of bias item presented as percentages across all included studies.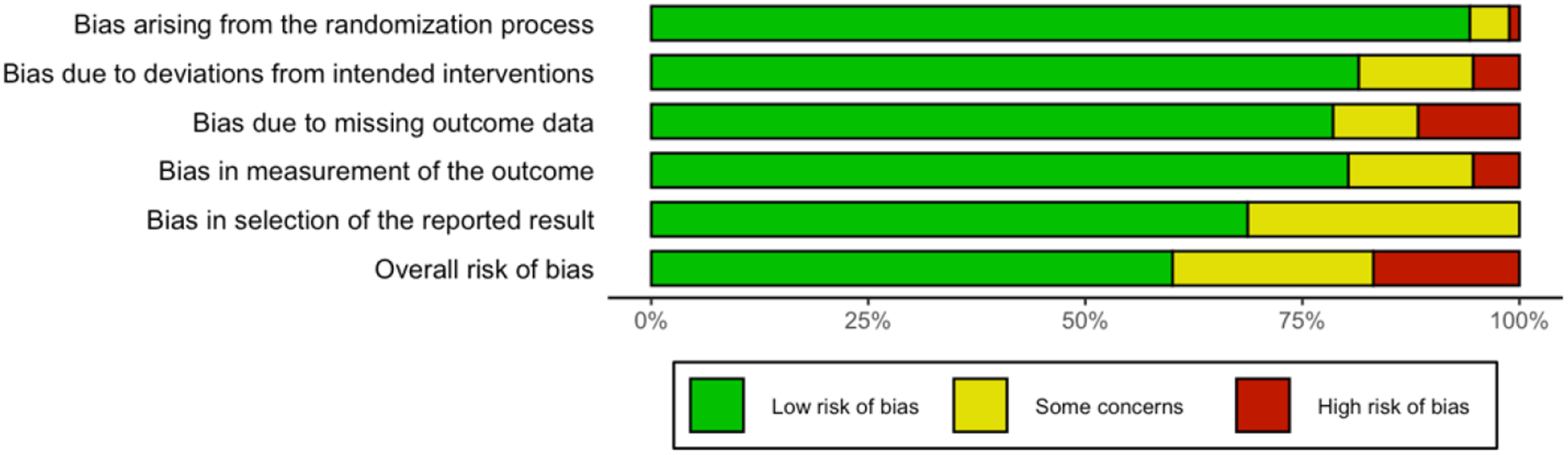
Discussion
The results of the primary analysis show that for the adult PGD interventions, ART, Psychoeducation with Social Support (PSS), Metacognitive Therapy, Music Therapy, Exposure Therapy, and CBT were associated with the highest effect sizes in post-treatment. The most effective treatments in the short-term follow-up were Narrative Therapy, CGT, and PSS. Multimedia Therapy and Exposure Therapy were the most effective in the six-month follow-up. However, there were no large effect sizes in the long-term follow-up. In terms of the secondary analysis, for adult comorbid depression interventions, Metacognitive Therapy, ART, and CBT were associated with the highest effect sizes in post-treatment. Narrative Therapy and CGT were the most effective treatments in the short-term follow-up. There were no large effect sizes in the six-month and long-term follow-ups. As for the adult comorbid PTSD, ART and Exposure Therapy were associated with the highest effect sizes in post-treatment. Narrative Therapy was the most effective treatment in the short-term follow-up. There were no large effect sizes in the six-month and long-term follow-ups.
Our first hypothesis, which stated that psychological interventions designed specifically to address prolonged grief would be more effective in treating PGD than general treatments, was partially supported, as the majority of the treatments with the highest effect sizes were tailored to address prolonged grief. However, contrary to that hypothesis, CGT did not show consistent effectiveness. The second hypothesis stated that pharmacotherapies previously successful in treating PGD comorbidities would be more effective in reducing prolonged grief symptoms. We were unable to reject or support this hypothesis as we could not obtain data for the RCT with citalopram (Shear et al., 2016) or find additional RCTs that used pharmacological treatments.
One of the most effective treatments was Psychoeducation with Social Support (PSS), whose main active component was educating patients about the nature of prolonged grief and utilizing participants’ natural social support network. It might have been successful because social support is a crucial protective factor against the development of PGD (Nam, 2016a; Nielsen et al., 2017). In addition to PSS, treatments with exposure and narrative reconstruction elements, such as ART and Exposure Therapy, were also effective. During the course of ART, participants learned to recall traumatic experiences associated with the death of the loved one without attaching emotional distress to them (Buck et al., 2020). In Exposure Therapy, participants were encouraged to engage in gradual exposure to the most painful memories of the loss or reduce excessive behaviours associated with preoccupation with the deceased person (Eisma et al., 2015). Elements of exposure might be effective because avoidance and sense of isolation are the major risk factors in the development of PGD (Maercker et al., 2017; Mason et al., 2020).
Cognitive Narrative Therapy also showed promising results. In their study, Barbosa et al. (2014) used a combination of cognitive elements and narrative reconstruction, where participants were asked to recall and process memories associated with the loss, which allows the patient to tell the story of their loss by focusing on the most challenging memories and reduces avoidance through exposure. Other types of effective treatments with elements of exposure and narrative reconstruction were Music Therapy and Multimedia Therapy. The main focus of the Music Therapy was to facilitate imaginary conversation between the patient and deceased through instrumental improvisations and singing (Iliya et al., 2015). Multimedia Therapy used such methods as discussing photographs and videos featuring the deceased and selecting and listening to songs associated with the deceased (Nesci et al., 2021). These treatments might have been effective due to the element of exposure and re-examination of the relationship to the deceased.
Finally, therapies with cognitive-behavioural components such as Cognitive-Behavioural Therapy (CBT), Metacognitive Therapy (MCT) and Complicated Grief Therapy (CGT) also showed high effect sizes, which was in accordance with the results of the previous meta-analysis on PGD treatments conducted by Wittouck et al. (2011). However, our results have indicated that while CBT showed a high effect size, it was not as high as such therapies as ART, PSS, MCT, Music Therapy, and Exposure. This might signal that treatment of PGD requires a modified version of CBT or some kind of a hybrid therapy that incorporates elements of CBT. For example, a study by Bryant et al. (2014) showed that CBT combined with exposure led to significantly better results than CBT alone.
With regard to cultural differences related to treatment efficacy, there needs to be additional analysis done on region-specific outcomes, as it was beyond the scope of our study. Moreover, considering the small number of included studies and the fact that certain treatments were only tested in specific parts of the world, it is hard to generalize the current findings to PGD patients from all cultures. For example, Accelerated Resolution Therapy for PGD, which showed one of the highest effect sizes in post-treatment, was only tested in the United States. Similarly, the effectiveness of Psychoeducation with Social Support was only examined in South Korea. Nevertheless, treatments with elements of CBT were present in all five regions (North America, Europe, Asia, Africa, Australia) and showed consistently positive treatment outcomes. This suggests that some aspects of PGD treatments may be universally beneficial.
Strengths and Limitations
Our study has several strengths, which make it quite useful to the clinical field. Firstly, it was a network meta-analysis that compared interventions that have not been compared before through the use of indirect evidence, thus expanding on the findings from the previous systematic reviews on treatments for PGD. Secondly, we examined treatments from all over the world without restricting age or language. Thirdly, we conducted a secondary analysis on the effectiveness of PGD treatments for the two most common comorbidities of PGD, namely, depression and PTSD. Finally, our inclusion criteria were very strict as we only included RCTs and excluded preventative treatments or treatments initiated before six months had elapsed after the loss, thus avoiding accidental inclusion of treatments for the normative grief.
Despite the strengths of our study, there also exist several limitations. Firstly, the data for the long-term follow-ups and treatments for children and adolescents was insufficient to conduct proper NMA. Secondly, the study that used a pharmacological intervention for PGD (i.e., Shear et al., 2016) had to be excluded from meta-analysis. Therefore, we were unable to meet our goal of collecting and analyzing information on pharmacological treatments for PGD. Thirdly, some studies only reported scores at post-treatment and did not have a follow-up, while other studies reported scores for the follow-up, but not for the post-treatment. In addition, depressive and PTSD scores were not always examined in the studies. This made it difficult to compare the effectiveness of all treatments in the same time frame and for both comorbidities. As a result, it is hard to determine whether some treatments (e.g., PSS) would be effective as a long-term intervention or not and if treatments that were tested for only PGD (e.g., Music Therapy) will also be effective for its comorbidities.
Fourthly, most of the treatments with the highest effect sizes had wide confidence intervals, which shows high variability of the scores and indicates that further analysis is required. Fifthly, the way data was organized might have prevented CGT from showing the highest effectiveness and resulted in the overall low to moderate effect sizes, because treatments referred to as regular bereavement therapy were grouped together. Sixthly, while including studies from different parts of the world provides a broader picture of existing PGD treatments, it can also be considered a potential limitation due to the fact that region-specific cultural beliefs related to death and grieving might have influenced the effectiveness of particular treatments. Therefore, it is important to consider the possibility that certain treatments shown to be effective in more individualistic regions such as North America, Europe, and Australia, might not be as effective in collectivist cultures of Asia and Africa.
The final and most serious limitation was that the highest effect sizes often came from a single study with a novel treatment that was not yet replicated. This makes interpretation difficult and raises a concern regarding the applicability of those results to clinical work. Nevertheless, those novel treatments might share certain elements with more traditional and well-studied therapies. Some of those treatments, such as Accelerated Resolution Therapy (ART), have also previously shown promise in treating PGD comorbidities, yet only recently started to be tested for treating PGD (Kip et al., 2013).
Conclusion
Overall, the results of our study show that the most effective treatments for PGD contained an element of exposure, social support, narrative reconstruction, and artistic expression, along with a cognitive-behavioral aspect. These results contribute to the existing literature and research on PGD and provide more information on the causes, course, and treatment outcomes of PGD. The findings of our study also provide valuable information to therapists working with prolonged grief and can potentially lead to the development of better treatments. In terms of the directions for future research, further research is needed to compare group interventions to individual interventions to replicate the findings of the meta-analysis by Johannsen et al. (2019). It is also important to examine PGD treatments specific for perinatal loss, as this type of loss was not included in this review. Moreover, primary analysis could benefit from examining studies that used designs other than randomized controlled trials, while the secondary analysis can be expanded by including anxiety as another comorbidity of PGD. Finally, because in our study different subtypes of CGT were grouped together, it is important to account for this limitation and ungroup complicated grief treatments from the regular grief treatments in future research.
Supplemental Material
Supplemental Material - Treatments for Prolonged Grief Disorder: A Systematic Review and Network Meta-Analysis
Supplemental Material for Treatments for Prolonged Grief Disorder: A Systematic Review and Network Meta-Analysis by Anna Pleshka, Shawn Crawford, Michele Wellsby, Anees Bahji, Caitlyn O’Connor, Julia Trieu, Aleithia Beck, Marwa Faqiri, and Daniel Devoe in OMEGA - Journal of Death and Dying
Footnotes
Author Contributions
Pleshka had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Conceptualization: Pleshka, Crawford, Devoe. Data curation: Pleshka, Bahji. Formal analysis: Pleshka, O’Connor, Trieu, Beck, Faqiri. Investigation: Pleshka. Methodology: Pleshka, Devoe. Project administration: Pleshka, Crawford, Devoe. Resources: Pleshka, Crawford, Devoe, Bahji. Supervision: Crawford, Devoe. Validation: Pleshka. Visualization: Pleshka. Original draft: Pleshka. Review and editing: Crawford, Wellsby, Devoe.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
See Data Sharing Statement in the appendix.
Supplemental Material
Supplemental material for this article is available online
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.