
Abstract
The (in)ability to accept and find meaning in the loss of a loved one can lead to the development of prolonged grief disorder (PGD), a return to normal level of functioning, or posttraumatic growth (PTG). This study aims to examine the factors that can predict PGD and PTG, in order to understand the differences between these two paths of adjustment. 269 bereaved adults participated in completing a questionnaire on PGD, PTG, presence and search for meaning, spirituality, relationship quality, depression, and anxiety. Results show that there are common factors that positively predict both intense grief and posttraumatic growth, such as the impact of the event, spirituality, and a relationship of proximity. The final model explained 68% and 32% of the variance of symptoms of PGD and PTG, respectively. This study highlights the importance of examining PGD and PTG together to understand better what distinguishes an adaptive from a maladaptive adjustment to grief.
Introduction
The loss of a loved one, such as a friend, spouse, parent, or family member, is a painful and common experience of human existence. Despite this, grief is also a singular and subjective process that varies in its duration and intensity (Bonanno & Kaltman, 2001), according to several personal (e.g., individual characteristics, relationship with the deceased) and external factors (e.g., circumstances of the death, sociocultural factors) (Burke et al., 2015; Burke & Neimeyer, 2013; Mason et al., 2020). Approximately 90% of the bereaved manage to react and adapt to the loss in a healthy manner. However, a significant percentage of people (between 6 to 15%) struggle to move past their grief, persistently engaging in maladaptive strategies (e.g., denial, avoidance), which increases the risk of physical illness and mental health disorders, such as prolonged grief disorder (PGD) (Lundorff et al., 2017).
PGD is characterized by persistent and intense symptoms of grief that disrupt and compromise the individual’s ability to function in daily life. These symptoms include difficulties accepting the death, marked yearning for the deceased, intense emotional pain, anger or apathy, loss of meaning in life, loneliness, and isolation (American Psychiatric Association (APA), 2013; Lobb et al., 2010). According to the ICD-11, PGD can only be diagnosed 6 months after the loss (World Health Organization, 2018). However, the DSM-V considers that only 12 months after the loss (APA, 2013; Prigerson et al., 2009), can the presence and intensity of the symptoms cease to be considered as a normal reaction to grief (Shear et al., 2011). There is, therefore, a significant time frame that allows for preventive interventions in an early and acute stage of grief.
The death of a loved one can be an impactful event that has the potential to disrupt an individual’s life profoundly, often leading to a search for meaning. The meaning reconstruction theory suggests that one of the key components of grief is precisely the search for a meaning in the death (Gillies & Neimeyer, 2006). And so, after the death of a loved one, people need to find a meaning that will allow them to make sense of the loss, which is an essential first step to accept, integrate, and adjust to the experience (Neimeyer, 2015). On the other hand, as research has shown, difficulty in finding meaning is a strong predictor of intense and prolonged grief (Burke & Neimeyer, 2013; Milman et al., 2017). This is explained in the theory of meaning reconstruction, which also indicates that risk factors (e.g., violent death, spousal loss) can block the meaning-making process, increasing the likelihood of the development of PGD (Neimeyer, 2016). The results of several studies have supported this theory, focused on the role of meaning in bereavement (Currier et al., 2006; Holland et al., 2010; Milman et al., 2019b; Thimm & Holland, 2017).
The ability to make sense of the loss can not only lead to an integration of the event in one’s narrative but also contribute to personal growth. Posttraumatic growth (PTG) is the perception of positive psychological changes and the experience of personal growth that resulted from a traumatic or highly challenging event (Tedeschi & Calhoun, 1996; Tedeschi et al., 2018). According to the model of PTG, these positive changes are experienced in five domains: new way of relating to others, perception of new possibilities, personal strength, appreciation of life, and spiritual and existential change (Tedeschi et al., 2018). The death of a loved one can potentially challenge an individual’s core beliefs about oneself, others, and the world, provoking emotional distress and giving space for intrusive rumination. The inability to successfully face and cope with the experience can lead to PGD, as mentioned before. However, those who can adaptively cope, transforming intrusive rumination into more deliberate and constructive thinking, as well as making sense of the loss, are more likely to perceive growth (Bellet et al., 2018). Studies have supported this theory, finding that the reconstruction of identity and the construction of a new worldview are essential for the development of PTG in bereaved individuals (Bellet et al., 2018; Captari et al., 2021). This is particularly true in the case where the death is perceived as more traumatic, unexpected, or violent (Currier et al., 2006).
Most studies on bereavement focus on PGD and PTG separately, analyzing their prevalence, risk, and protective factors or the outcomes of these conditions. Thus, few studies examine what the common and differentiating factors are between these two paths of adjustment. Which still leaves the question of what mechanisms can be targeted in order for a better adjustment to the loss to occur (Milman et al., 2019a). The aim of this study is therefore to analyze the contribution of different factors that have been shown to positively and negatively impact the severity of grief symptoms and the process of PTG, as well as the relationship between PGD and PTG. Considering that the majority of the research focuses on the effect of intrapersonal factors (e.g., age, gender, previous losses, attachment style) and factors related to the death (e.g., kinship, circumstances of death), our focus will be on the impact of the level of stress regarding the death perceived in the moment and in the present, the presence and search for meaning, spirituality, symptoms of anxiety and depression and the quality of the relationship.
Methods
Participants
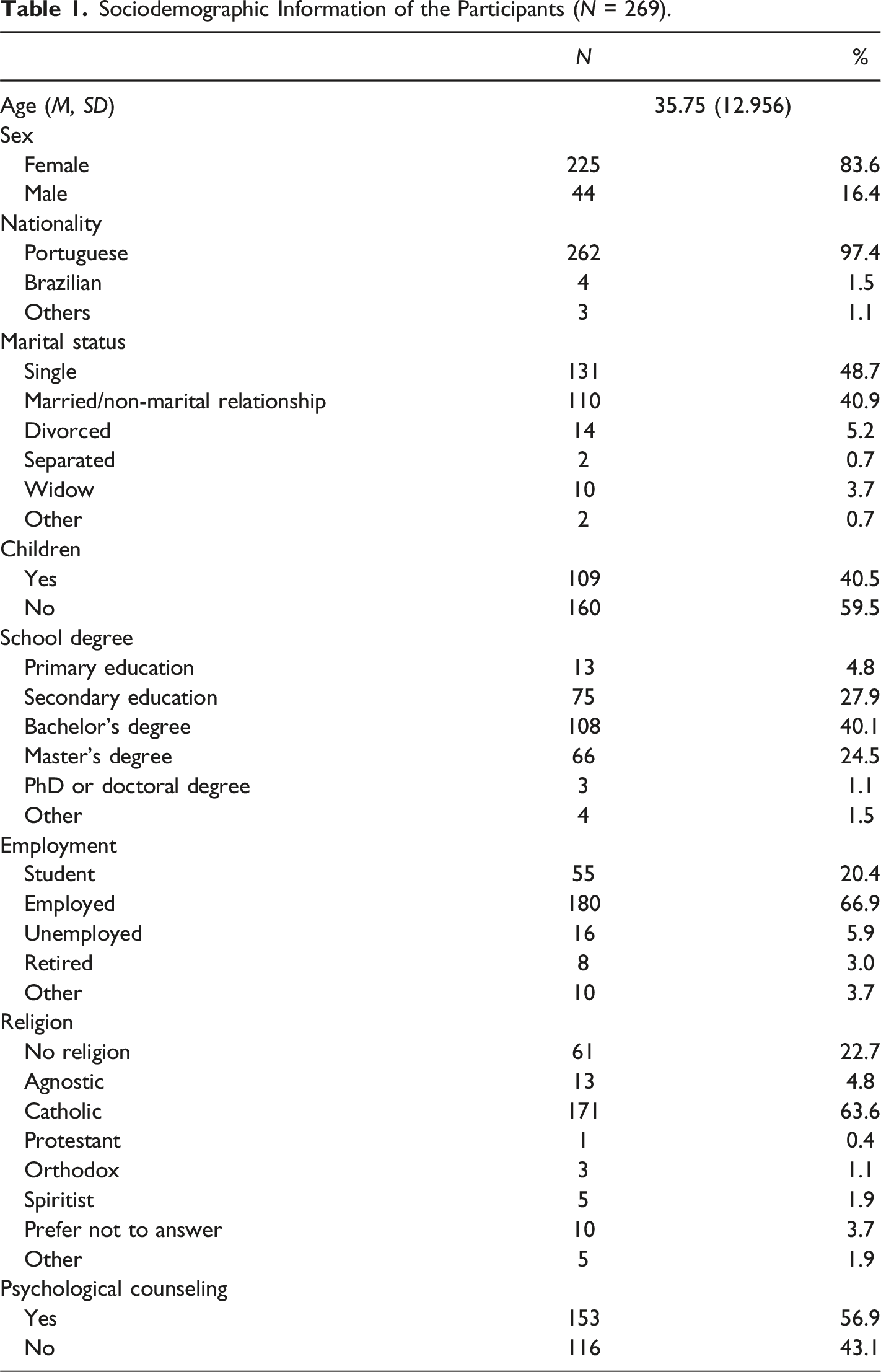
The sample consisted of 269 bereaved adults who had gone through the loss of a loved one in the last five years. There were 467 responses to the questionnaire, from which 198 (42.4%) were incomplete or did not meet the inclusion criteria. The inclusion criteria included: (a) being an adult (age equal to or greater than 18 years); (b) having experienced the loss of a loved one in the past five years; (c) being able to understand and read Portuguese. The sample is not representative of the Portuguese population as it was recruited by convenience sampling.
Sociodemographic Information of the Participants (N = 269).
Material
A sociodemographic questionnaire was applied to gather information regarding the participants characteristics (age, sex, nationality, marital status, employment, school degree, children, residency, religion and psychological counselling), the information regarding the death of the loved one (time since death, cause and place of death) and the information of how and who delivered the news of death.
Stressfulness of the Event
To assess the level of stress perceived from the death of the loved one, two independent questions were constructed based on the study of (Lindstrom et al. 2013). Participants were asked about the levels of stress perceived when learning about the death (“What was the level of stress that you felt when learning about the death of your loved one”) and at the present moment (“What is the level of stress that you feel in this moment regarding the death of your loved one?”). Answers were given in a 7-point Likert scale (from 0 = “Not stressful at all”, to 6 = “Extremely stressful”).
Symptoms of Prolonged Grief
The Prolonged Grief Disorder Revised (PG-13-R) was developed and revised by Prigerson et al.(2021), which was adapted to the Portuguese population (Delalibera et al., 2011), was used to assess the symptoms of prolonged grief disorder (PGD). This questionnaire consists of 13 items that assess a variety of symptoms, including separation anxiety, cognitive, emotional, and behavioral symptoms associated with PGD. A 5-point Likert scale (from 1 = Not at all to 5 = Overwhelmingly) is used for 10 of the 13 items. Only 10 items were used in the data analysis, as the remaining three items are considered for diagnostic purposes.
Presence and Search for Meaning
The Meaning in Life Questionnaire (MILQ) was developed to assess the presence and search for meaning in life (Steger et al., 2006). This questionnaire consists of 10 items, divided into two subscales – Presence of Meaning and Search for Meaning – assessed using a 7-point Likert scale (ranging from 1 = Absolutely Untrue to 7 = Absolutely True). The questionnaire has been translated and adapted for the Portuguese population (Portugal, 2017), showing good internal consistency. Higher scores on the Presence of Meaning and Search for Meaning subscales indicated a greater sense of meaning and a higher search for meaning in life, respectively.
Spirituality
To assess spiritual well-being, the Functional Assessment of Chronic Illness Therapy - Spiritual Well-Being – Non-Illness Version (FACIT-Sp-12-NI) was applied. The original version was developed by Peterman et al. for patients with chronic illness (2002). It is validated for the Portuguese population (Pereira & Santos, 2011). The scale used in this study is an adapted version that can be applied to other individuals who have experienced adversities unrelated to illness. There are 12 items, divided into two dimensions: Meaning/Peace and Faith, which are answered using a 5-point Likert scale (0 = Not at all to 4 = Very much). Higher scores indicate a higher sense of spirituality and spiritual well-being.
Posttraumatic Growth
The Expanded Version of the Posttraumatic Growth Inventory (Tedeschi et al., 2017) (PTGI-X), is a revised version of the Posttraumatic Growth Inventory (PTGI) developed by Tedeschi and Calhoun (1996) to appraise the perception of positive psychological changes in an individual after experiencing a traumatic event, such as the loss of a loved one. This is a self-report scale with 25 items, organized in five dimensions: Relating to Others, New Possibilities, Personal Strength, Spiritual and Existential Change, and Appreciation of Life. The participants were asked to identify the degree to which they experienced a particular change, using a 5-point scale (0 = I did not experience this change as a result of my loss, to 5 = I experienced this change to a very great degree as a result of my loss). The original scale has been validated for the Portuguese population (Ramos et al., 2016), and the revised version is currently undergoing validation.
Relationship Quality
The Relationship Quality between Caregiver and Patient Scale was used to assess the quality of the relationship between the bereaved individual and the deceased loved one. There is a total of 12 items that assess two types of relationships: Proximity and Conflict. Participants’ answers were based on a Likert scale of 5 points (1 = Not at all to 5 = Very much), with the additional option “0 = Do not know or Prefer not to Answer). This scale has been validated; however, the article is currently under submission for publication.
Anxiety and Depression
The Portuguese version of the Hospital Anxiety and Depression Scale (HADS) (Pais-Ribeiro et al., 2007) was used to assess the symptoms of anxiety and depression. This scale comprises two seven-item subscales, each measured on a 4-point Likert Scale (ranging from 0 to 3). In the Anxiety subscale, higher scores represented more intense symptoms of anxiety. While in the Depression subscale, higher scores represented lower levels of depression.
Means, Standard Deviations, and Cronbach’s Alpha of Variables (N = 269).
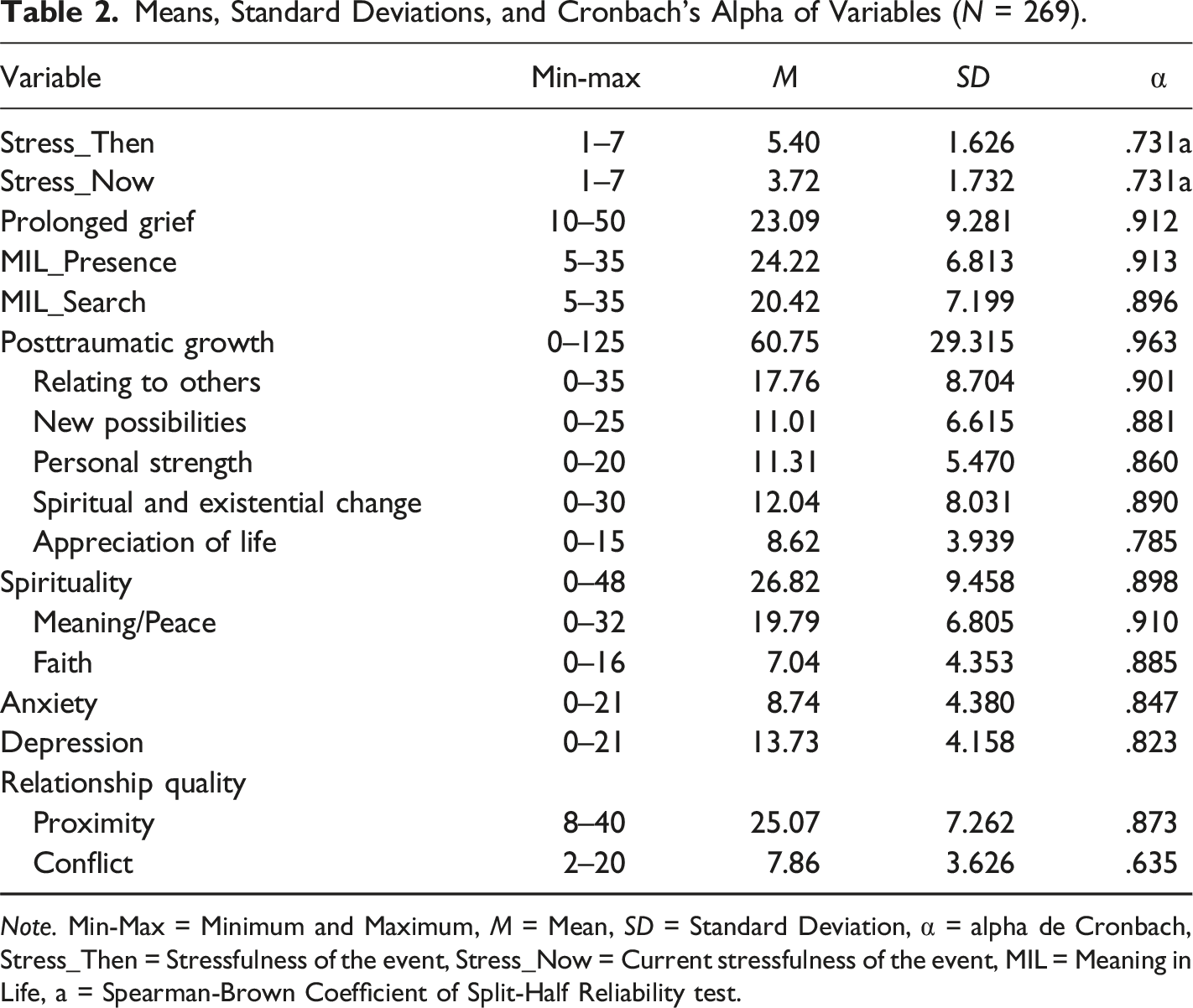
Note. Min-Max = Minimum and Maximum, M = Mean, SD = Standard Deviation, α = alpha de Cronbach, Stress_Then = Stressfulness of the event, Stress_Now = Current stressfulness of the event, MIL = Meaning in Life, a = Spearman-Brown Coefficient of Split-Half Reliability test.
Procedure
This observational, descriptive, cross-sectional, quantitative study is part of a larger research project entitled “Finding Meaning in Loss: Meaning-Making and Posttraumatic Growth in Adjustment to Grief”, which was approved by Ispa – University Institute Ethics Committee. This study was conducted in accordance with the Declaration of Helsinki.
Participants were recruited from social media platforms (WhatsApp, Facebook, Instagram, LinkedIn) from December 2023 to March 2024. Participants were asked to read an informed consent form, which informed them of the study’s objectives and procedures, ensuring that all data were anonymous. Participants were then asked to answer an online questionnaire available at Qualtrics. At the end of the questionnaire, an informational flyer was made available to participants regarding the symptoms of Prolonged Grief Disorder and the contact information for national support lines.
Data analysis was conducted using the IBM Statistical Package for the Social Sciences (SPSS) and AMOS, version 29. All statistical analyses were conducted at a significance level of 0.05 (α ≤ 0.05). To assess the internal consistency of the instruments, a reliability test was performed using Cronbach’s alpha. Pearson’s correlation coefficient was used to assess the correlation between variables.
To determine the relationship between the secondary variables (search and presence of meaning in life, spirituality, relationship quality, stressfulness of the event, anxiety and depression) and the main variables (prolonged grief and posttraumatic growth), it was conducted a Structural Equation Modeling with observed variables in AMOS, with PGD and PTG as dependent variables. Firstly, the assumptions of the test were confirmed by: (a) assuring the absence of missing data; (b) verifying the possible existence of outliers, through the Mahalanobis distance (D2); (c) examining the normal distribution of the variables, with the values of skew (|Sk|<3) and kurtose (|Ku|<10) (Marôco, 2010). The model tested included all of the independent variables in the first analysis. The non-statistically significant variables were then removed from the final model. Model fit was assessed using indices such as: (a) qui-square test (p > .05); (b) chi-square divided by degrees of freedom (χ2/df < 5); (c) RMSEA (<.05); (d) CFI (>.90); (e) NFI (>.90); (f) TLI (>.90) (Marôco, 2010).
Results
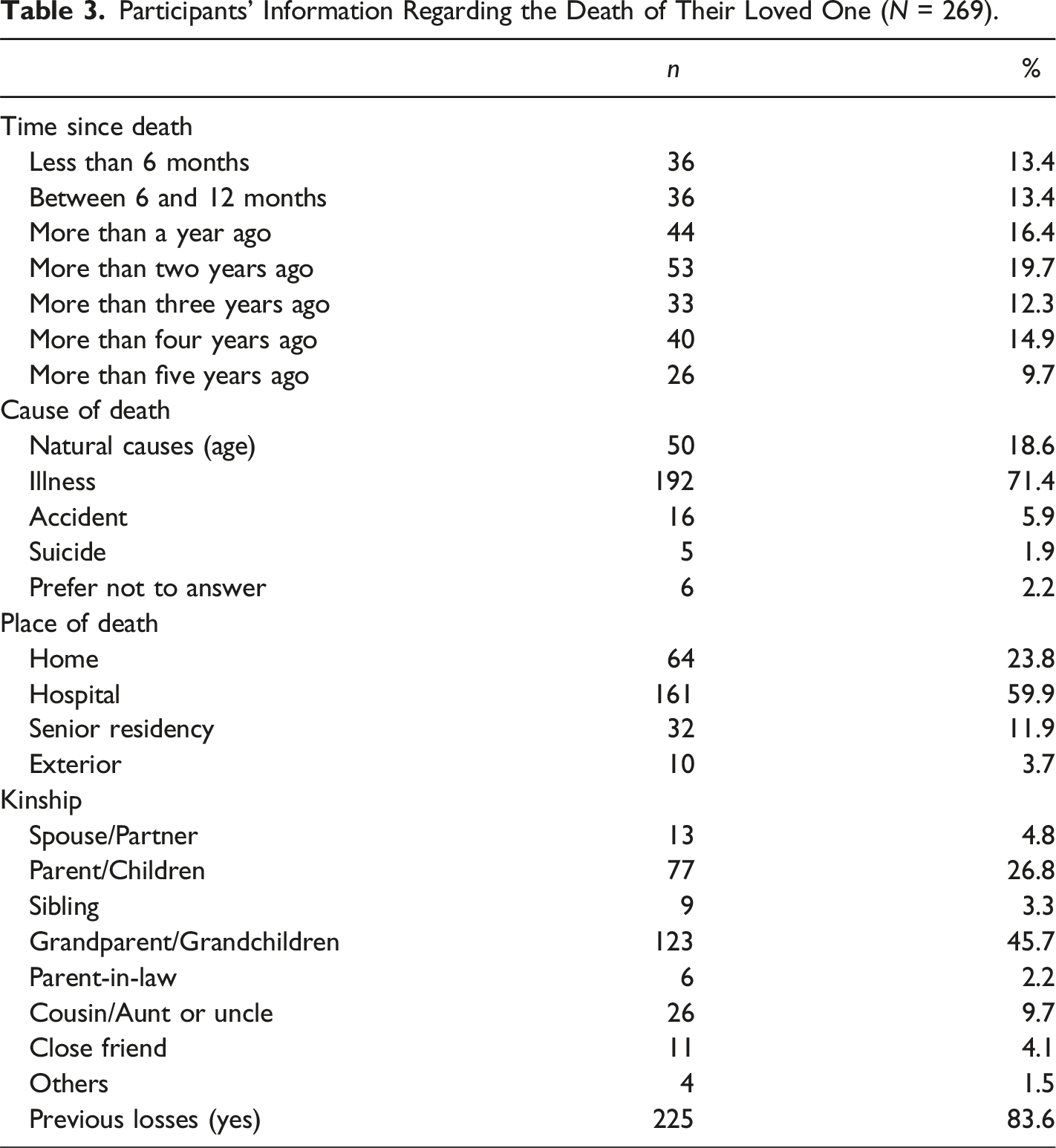
Participants’ Information Regarding the Death of Their Loved One (N = 269).
Bivariate Pearson Correlations Between Variables (N = 269).
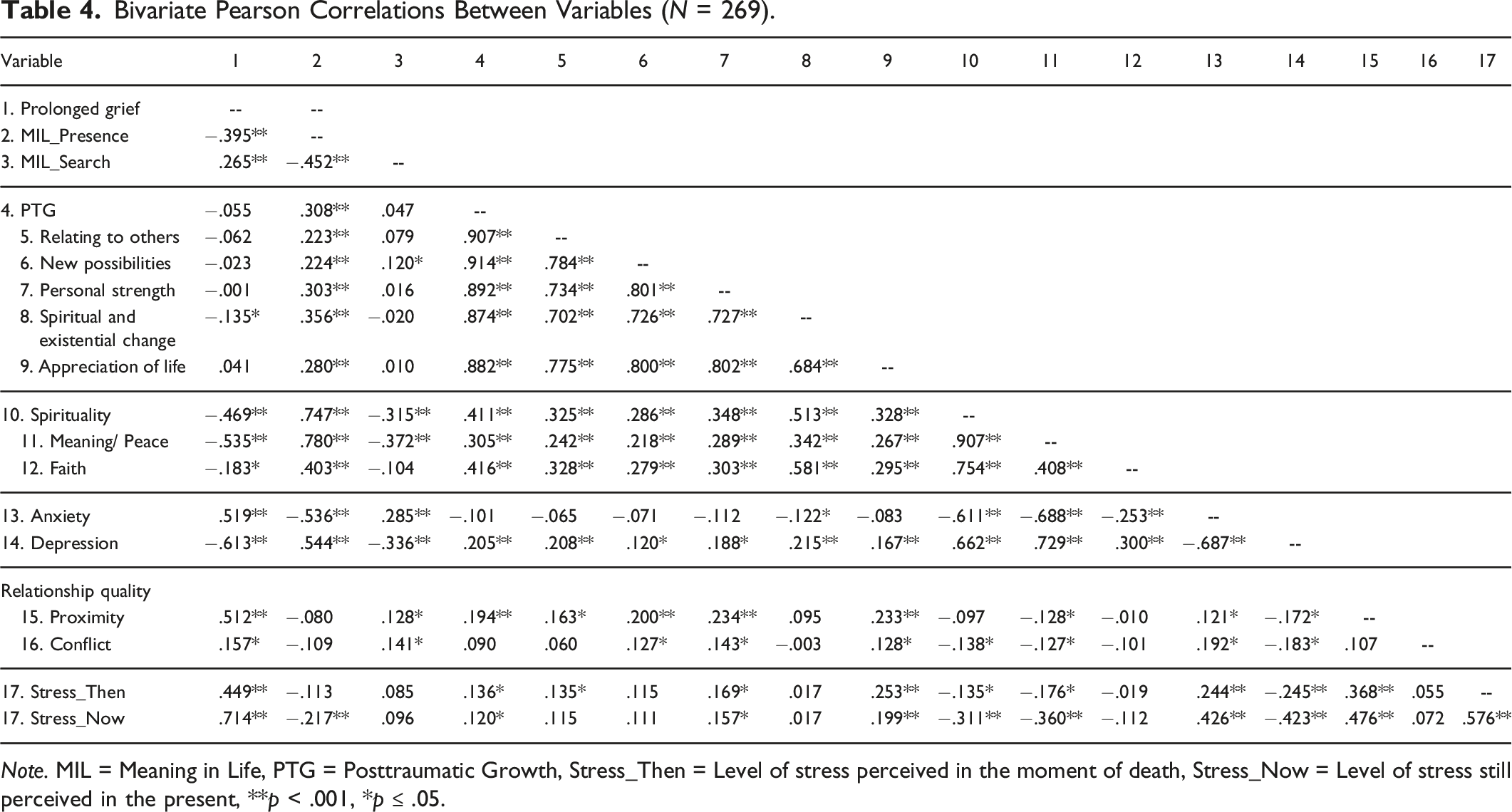
Note. MIL = Meaning in Life, PTG = Posttraumatic Growth, Stress_Then = Level of stress perceived in the moment of death, Stress_Now = Level of stress still perceived in the present, **p < .001, *p ≤ .05.
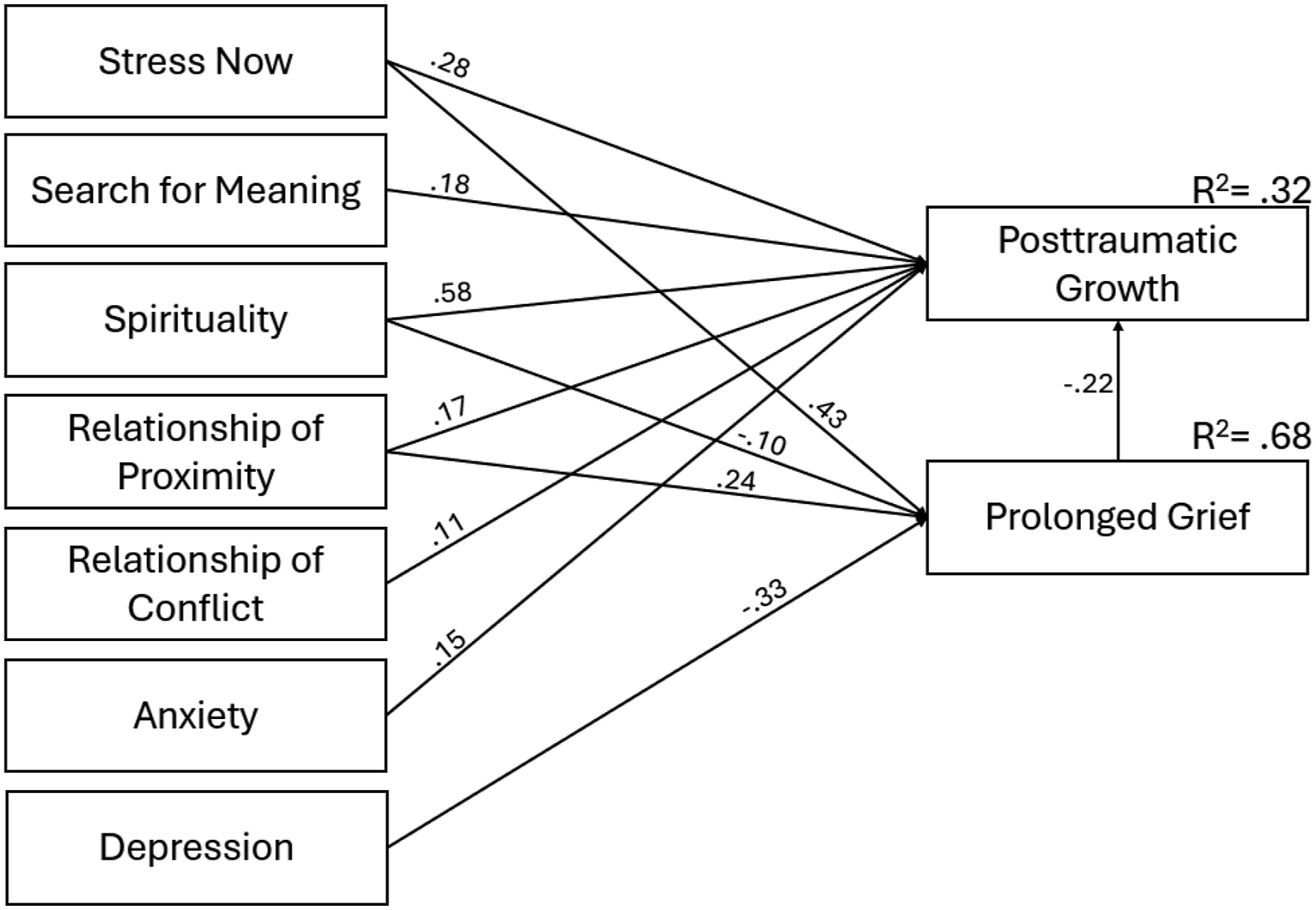
A structured equation model analysis was conducted to examine the relationship between presence and search for meaning in life, anxiety, depression, the quality of the relationship, and spirituality and the current stressfulness of the event with PGD and PTG, accounting for the relationship between PGD and PTG, as can be seen in Figure 1. No outliers were found, and the variables exhibited a normal distribution. The non-significant variables and paths were removed from the initial model. The final model revealed that the current stressfulness of the event (β = .431, p < .001), depression (β = −.326, p < .001), a relationship of proximity (β = .241, p < .001), and spirituality (β = −.096, p = .039) significantly predict symptoms of PGD. Suggesting that the current stressfulness of the event, depression, and a relationship of proximity are related to a higher prevalence of symptoms of prolonged grief. Moreover, spirituality is related to lower symptoms of prolonged grief. The results also indicated that spirituality (β = .575, p < .001), current stressfulness of the event (β = .281, p < .001), search for meaning (β = .178, p = .001), anxiety (β = .152, p = .028), a relationship of conflict (β = .110, p = .033), and a relationship of proximity (β = .174, p = .005) significantly predict PTG. This suggests that spirituality, the current stressfulness of the event, the search for meaning, a relationship of proximity, and a relationship of conflict are related to a higher perception of PTG. Additionally, a relationship was found between PGD and PTG (β = −0.218, p = .009), with more symptoms of PGD predicting a lower perception of PTG. The final model, presented in Figure 2, indicated a good fit to the data (χ2 (4) = 4.477, χ2/df = 1.119, p = .345, NFI = .995, TLI = .995, CFI = .999, RMSEA = .021). This model explains 67.6% of the variance in symptoms of PGD and 32.4 % of the variance in PTG. Hypothetical structured equation model. Final Structural Equation Model for PGD and PTG. Note. Only significant pathways are represented in the model. Values above the arrows represent the standardized beta values.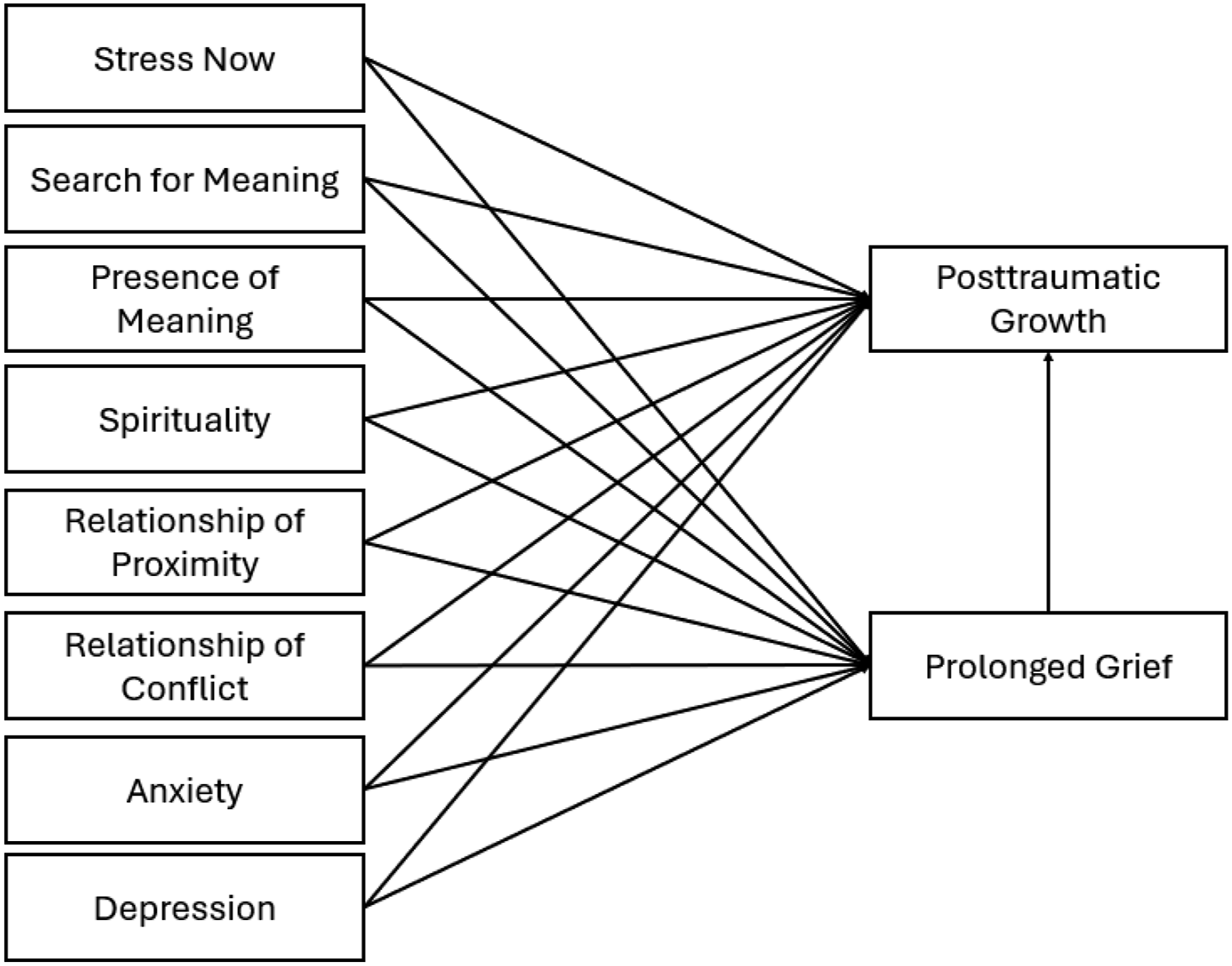
Discussion
The path to adjustment to the loss of a loved one is a difficult one. The goal of this study was to analyze the contributions of several factors to symptoms of PGD and PTG. The results obtained suggest that common factors contribute to both adaptive (personal growth) and maladaptive adjustments (prolonged grief). The current stressfulness of death, spirituality, depression, and a relationship of proximity with the deceased significantly predicted symptoms of PGD, explaining 68% of its variance. The results also showed that current stressfulness of the event, search for meaning, spirituality, PGD, anxiety, a relationship of proximity, and a relationship of conflict with the deceased significantly predicted PTG, explaining 32% of its variance.
Regarding the current stressfulness perceived from the death of the loved one, the results show it to have a significant impact on prolonged grief and PTG. More precisely, higher levels of stress were related to more intense symptoms of PGD but also a higher perception of PTG. One possible explanation for these results is that the level of stress perceived by the participants can be seen as an indicator of the impact and importance of the death of the loved one. In this case, considering that the impact of the event (i.e., death) is one of the key factors for the development of both PGD and PTG, it would be expected that the stressfulness of the event would predict both PGD and PTG. The impact of the loss of a loved one is directly linked to a variety of factors, from the kinship with the deceased to the circumstances of the death. Several studies have shown that factors related to the death (e.g., violent death, place of death) (Milman et al., 2017) and the kinship between the bereaved and the deceased have a significant impact on the development of PGD (Burke & Neimeyer, 2013; Lobb et al., 2010; Mason et al., 2020). On the other hand, even though it is necessary to experience a stressful or traumatic experience for PTG to occur, research on the impact of the event in predicting PTG in bereavement is unclear. While some studies suggest that the centrality of the event significantly predicts PTG (Brooks et al., 2017; Ryan & Ripley, 2023), there does not seem to be a consensus regarding the impact of the circumstances of death (Cofini et al., 2014; Polatinsky & Esprey, 2000) or kinship (Ogińska-Bulik & Kobylarczyk, 2017).
Interestingly, Ogińska-Bulik and Kobylarczyk (2017) study showed that people who lost their parents or siblings had a higher perception of growth than those who lost a child or a close friend. Whereas Murphy et al.(2003) study on bereaved parents revealed that most had trouble finding meaning in the death of their child over time. These studies might suggest that in some cases, the impact of the death can be too overwhelming for PTG to occur, which would explain why the levels of stress are a better predictor for PGD than for PTG. As the meaning reconstruction (Gillies & Neimeyer, 2006) theory explains that the ability to find meaning in the experience or to reconstruct an individual’s core beliefs is crucial to the process of adjustment and even growth after the loss of a loved one. And like it was mentioned before, there are some factors, including the kinship with the deceased, that can block this process and lead to the development of PGD (Neimeyer, 2016).
After the death of a loved one, there is often a need to find meaning in the loss and, in some cases, even the meaning of life in the absence of that person (Neimeyer, 2016). The process of searching for meaning is then considered a natural part of the grief process. And while some can quickly make sense of their loss and return to their emotional baseline within a few months, others struggle with this process (Bonanno, 2009). This struggle to find meaning can be considered as part of the process of reconstruction of core beliefs, which could ultimately result in a personal change or PTG (Gillies & Neimeyer, 2006; Neimeyer, 2019). This could explain why, in this study, the search for meaning was a significant predictor of PTG.
It is, however, important to note that a search for meaning does not imply a lack of meaning in one’s life, which is why the presence of MIL did not significantly relate to PGD or PTG. Nonetheless, there was a significant and negative correlation between the presence of MIL and PGD, suggesting that the absence of MIL is associated with higher symptoms of PGD. There was also a significant and positive correlation between the presence of MIL and PTG, indicating that the presence of meaning is associated with the perception of PTG. These results indicate a connection between MIL, PGD, and PTG, although none of them significantly predicts the others.
Another component often related to life’s meaning and the process of searching for meaning is spirituality. Religious and spiritual beliefs can be a source of meaning, a way to make sense of the world (Pargament, 1999; Park, 2013). In bereavement, studies have shown that experiencing the loss of a loved one can shatter our core beliefs, particularly those that are built on religious beliefs, leading to a disruption in the relationship with God (Burke & Neimeyer, 2014). However, spirituality can also be a source of comfort and peace after death, promoting the integration of loss, psychological well-being, and even personal growth (Neimeyer & Burke, 2015). This could explain why spirituality had a negative relationship with prolonged grief symptoms, indicating that higher levels of spirituality are related to fewer symptoms. Additionally, the correlations showed that the component of spirituality with the strongest association to PGD was the meaning and peace subscale, rather than faith.
The scale used to measure spirituality in this study assessed not only religious and spiritual beliefs, but also a sense of peace and meaning. The results revealed spirituality to be one of the strongest predictors of PTG. This goes in line with previous literature, indicating that spirituality plays an important role in the process of PTG (Currier et al., 2013; Ryan & Ripley, 2023; Testoni et al., 2022). More recently, there was even an expansion of the PTGI precisely to add items related to the spiritual and existential change, as it is one of the five components of PTG (Tedeschi et al., 2017).
Regarding depression and anxiety, it is curious to see how they relate differently to symptoms of PGD and PTG. While depression was related to greater symptoms of PGD, anxiety seemed to relate to higher levels of PTG. When it comes to PGD, it could be easy to mislead PGD for depression, seeing as they share some of the same symptoms, such as anhedonia, lack of meaning, or social isolation. There are, however, differences between these two disorders, particularly the intense yearning for the deceased (Shear et al., 2011) and the preoccupying anxiety over separation felt in PGD (Maercker et al., 2017). Studies have shown that there is not only a high prevalence of comorbidity of PGD and depression (Kokou-Kpolou et al., 2021; Maercker et al., 2017), but that preexisting and immediate depression can be a risk factor for the development of PGD (Mason et al., 2020). On the other hand, when it comes to PTG, the relationship between anxiety and depression is more unclear. A meta-analysis revealed the existence of mixed results on the matter, with some studies indicating that more symptoms of anxiety are related to higher PTG, particularly in non-cancer populations. However, the results from the effect of anxiety in PTG were barely significant (Long et al., 2021). These results might suggest that the relationship between these two variables is more complex. More recent studies have analyzed the possibility that the relationship between anxiety and PTG is curvilinear, showing that moderate levels of anxiety are related to higher PTG than high or low levels of anxiety (Eisma et al., 2019; Weber & Schulenberg, 2022). This denotes that for PTG to develop, a person must perceive a certain level of distress, but not enough to disrupt and block the process of growth (Eisma et al., 2019; Li et al., 2021).
Regarding relationship quality, a relationship of proximity predicted both PGD and PTG, while a relationship of conflict only significantly predicted PTG. The results show, therefore, that a close relationship with the deceased predicted higher symptoms of PGD as well as PTG. There are, however, some considerations that must be taken into account regarding the instrument used to measure the quality of the relationship before interpreting the results. The items concerning the relationship of proximity not only assessed proximity and level of caring but also addressed the existence of a specific, practical, and emotional dependency of the bereaved on the deceased. Regarding the results obtained from the subscale of relationship conflict, these may not be the most reliable, given that it showed low internal consistency for this sample.
A pre-loss proximity between the bereaved and the deceased is one of the predicting factors of higher symptoms of PGD (Burke & Neimeyer, 2013; LeRoy et al., 2020). This is particularly true when there was a preoccupied attachment, and therefore a more dependent relationship with the deceased (Smigelsky et al., 2020). A relationship of closeness can, in this case, cause a greater difficulty in accepting the death and adjusting to it, leading to more intense symptoms of grief. This occurs because the proximity to the deceased relates to the impact of the death. As mentioned earlier, the impact of death is a key component in the adjustment process. The greater the impact, the higher the chance that the individual will experience intense symptoms of grief, potentially blocking the process of integration of the loss and allowing for PGD to develop. On the other hand, when a person goes through a potentially traumatic experience, there is also a certain probability that event will elicit a process of change, possibly leading to PTG. The results support this theory, as a relationship between proximity and PTG was also found. There are, however, few studies regarding the quality of the relationship and PTG in bereavement (Ludwikowska-Świeboda & Sekowski, 2024). Interestingly, the presence of conflict in the relationship also predicted PTG. Furthermore, while there is insufficient literature to explain these results, one must consider the fact that the presence of conflict in a relationship still implies a proximity and closeness that will inevitably cause the death to be a significant event. Additionally, the presence of conflict and possibly unresolved issues can also serve as a source of reflection, prompting one to reconsider the priority of present relationships and their relationship to others.
Our study reveals common factors that relate to and predict both symptoms of PGD and the development of PTG. As Bellet et al.(2018) demonstrated, PGD and PTG can co-occur, reinforcing and weakening each other. Thus, explaining why they not only seem to have a negative relationship, but also why they share some of the same predictors. This still leaves the question of what factors can make the difference between a path of prolonged grief and a path of growth after the loss of a loved one. Being able to understand what mechanisms are behind the change from intense bereavement to growth could further facilitate the impact and effectiveness of psychological interventions in this population. Future studies would benefit from using a mixed or qualitative design, allowing for a deeper understanding of the role and impact of these common factors in predicting PTG rather than PGD. Additionally, considering that the process of grief is not a linear one, longitudinal studies would enable us to understand the entirety of the adjustment process better.
Our study had some limitations regarding the sample, as most deaths were due to illness and therefore were more likely to be expected deaths. The sample was also not representative of the Portuguese population, as most participants were female with an average age of 36 years. The kinship with the deceased was not analyzed due to a misinterpretation of the question by a significant part of the participants. Lastly, the recruitment of a larger sample would have allowed us to examine in more detail the impact of other sociodemographic and clinical variables. Nonetheless, the results of this study shed light on the coexistence of prolonged grief and personal growth. This underscores the need to investigate the relationship between these two processes further and what distinguishes them.
Footnotes
Author Contributions
M.F.A. and I.L. conceptualized the study. M.F.A., J.C., C.M., M.L.A., A.C. participated in data collection and analysis. M.F.A. and C.R. analyzed the data and wrote the main manuscript. All authors reviewed and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author, Margarida Ferreira de Almeida, work is funded by a PhD scholarship awarded by FCT – Fundação para a Ciência e Tecnologia, with the reference number 2023.00702.BD. This work is funded with national funds from FCT – Fundação para a Ciência e Tecnologia, I.P., in the context of the project UID/04810, DOI: 10.54499/UIDB/04810/2020 and ![]() .
.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Author Biographies