
Abstract
This research explored current practices, gaps in services and resources, and identified barriers and facilitators to implementing a bereavement model of care in an Australian health setting. We conducted 34 interviews with staff/volunteers who provide bereavement care to explore their practice and perceptions of care delivery. Five themes were identified through thematic and framework analysis: 1. Conceptualisation of bereavement was setting dependent; 2. Formal versus informal delivery of care; 3. Current bereavement care, referral pathways, and evaluation; 4. Barriers and Facilitators to accessing and providing care; 5. An ideal bereavement model of care. This research highlighted gaps in services and suggests a disconnect between current practice and ideal bereavement care delivery. We present an evidence-based bereaved-centred model of care, that can be tailored to fit specific health context and settings. Identified barriers and facilitators to implementing this model of care should inform strategies that underpin implementation of the model.
Introduction
Bereavement is the emotional, cognitive, physical, spiritual, and behavioral adjustment to the death of a loved one (Bui, 2018). Approximately 40% of Australian bereaved adults have a moderate (35.2%) to high (6.4%) risk of developing Prolonged Grief Disorder (PGD) (Aoun et al., 2015). Prolonged Grief Disorder is a state of chronic mourning where intense grief persists for years, impairing function and increasing risk of poor mental health outcomes (Prigerson et al., 2021). Bereaved people may also experience other symptoms of complicated grief such as clinical anxiety and depression, existential distress or post-traumatic stress (Komischke-Konnerup et al., 2021). Poor psychological wellbeing can also lead to adverse health outcomes (Ennis & Majid, 2021; Li et al., 2003).
Bereavement care supports people to prepare for the death of their loved one and/or navigate their grief afterwards (Agency for Clinical Innovation, 2021; Boven et al., 2022). Bereavement care includes grief education and support, community-based support, spiritual care, and/or psychosocial services (Lichtenthal et al., 2024), and has been found to alleviate immediate distress, improve adjustment to death, mitigate the risk of PGD and complicated grief reactions, and reduce mortality and health service usage (Penny, 2017). The public health approach to bereavement support services in palliative care suggests a stepped care approach to supporting bereaved individuals in their adjustment to the death of their loved one (Aoun et al., 2012). This approach suggests universal bereavement support (e.g., provision of grief education and support) for all caregivers and bereaved individuals and reserving specialist bereavement interventions (e.g., psychological services) for the small percent at high risk of or experiencing prolonged grief (Aoun et al., 2012; Hudson et al., 2018).
In Australia in 2022, there were more than 170,000 deaths (Australian Bureau of Statistics, 2023). Estimates suggest that for every death there are 4–9 individuals impacted by the loss (Thompson et al., 2017). With an aging population the number of bereaved will continue to rise, increasing the need for an appropriate evidence-based model of bereavement care (Australian Institute of Health and Welfare, 2016). Most deaths in Australia occur within the context of the health care system (Australian Bureau of Statistics, 2021) making bereavement care in this setting integral.
A recent systematic review of international bereavement models (Bartley et al., 2025) of care found that most of these models of care are developed and/or implemented in hospital settings, or in a specific services of a hospital (e.g., palliative care/oncology), and predominately in American health settings. The American health system is complex, expensive, and reliant on private insurance, which presents access barriers to a significant number of Americans who are uninsured or underinsured. In comparison, the Australian health system is a mix of universal healthcare with private health insurance for additional benefits. Only five of the 64 studies included in the review were conducted in an Australian health setting. These five studies were set in ICU/palliative/oncology (Blackburn & Dwyer, 2017; Gundry et al., 2023), and emergency/acute (Grant et al., 2021; LeBrocq et al., 2003; Williams et al., 2000) services. The quality and type of bereavement care can vary greatly within a hospital (Goldberg et al., 2021; Grant et al., 2021; Morris et al., 2017) and across health services (Edwards, 2020). Further, bereavement care is under resourced (Hudson et al., 2018), and is not routinely provided or delivered by trained staff (Breen et al., 2014; Grant et al., 2021).
The Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2022), classifies barriers and facilitators to implementation effectiveness in health service research across 5 domains: intervention characteristics, outer setting, inner setting, individuals, and process. A systematic review (Bartley et al., 2025) of the international research on the barriers and facilitators to implementing bereavement models of care highlighted the setting in which a model of care is implemented (inner setting), specifically, work infrastructure, a deliverer-centeredness culture, planning and access to knowledge/information, and adequate resourcing as influencing bereavement care. Also important are the processes used to implement bereavement models into practice, such as engagement, teaming, and reflecting and evaluating (Bartley et al., 2025). Individual characteristics such as staff discomfort with death and dying, or the reluctance of bereaved individuals to return to setting of their loved one’s death, as well as outer setting challenges such as providing care to bereaved individuals across a large geographical area, are barriers to implementing bereavement models (Bartley et al., 2025). However, only four (Grant et al., 2021; Gundry et al., 2023; Lattanzi, 1982; LeBrocq et al., 2003) of the 64 studies reviewed provided minimal information on implementation factors specific to the Australian health context. Understanding barriers and facilitators is important to the development of strategies to support implementation and the design of implementation outcomes (Proctor et al., 2013; Rudd et al., 2020).
The aim of this research was to explore current practice of bereavement care in an Australian health care setting, to explore gaps in services and resources, and identify whether barriers and facilitators to implementing a bereavement model of care previously identified in international studies are reflected in the context of implementing bereavement care across a public health care district in Australia. Understanding barriers and facilitators to provision of bereavement care will inform a model of care to drive practice change across services in Australia.
Methods
A qualitative approach was used, with semi-structured interviews conducted. Eligible participants were staff/volunteers who deliver bereavement care in a health district in New South Wales, Australia. This health district provides hospital and community-based care to diverse populations reflective of the Australian health context. Purposive sampling method (Palinkas et al., 2015), was used to identify potential participants across the health district, including a diversity of roles (nursing, psychology, psychiatry, medicine, volunteer), services (palliative care, acute care, neonatal, mental health) and settings (hospital, community health centres). Ethics approval was obtained from Nepean Blue Mountains Local Health District (2022/ETH00108) and St John of God Health Care (2005) Human Research Ethics Committees.
An email invitation including the participant information sheet was sent to identified stakeholders. During the interview process participants were asked whether there were any other staff in similar roles who could be contacted for an interview (snowballing). Those interested in participating completed consent and an online survey. The survey collected contact details, demographic characteristics (age, gender), and clinical experience (role, employment status, years in the role, setting, bereavement services provided). The semi-structured interview guide (Supplemental Material 1), developed by the research team based on the literature (Bartley et al., 2025) and their clinical and implementation science expertise, explored the bereavement care provided (including referral pathways and resources); perceptions of quality of current bereavement care as well as challenges and opportunities for improved bereavement care. No changes were made to the interview guide as the research progressed. Researchers contacted interested participants to schedule a telephone/zoom interview. Interviews were conducted by researchers NB and LRG, experienced qualitative interviewers. The average length of interviews was 47 min (range 21–57 min). Recruitment continued until information saturation (no new information emerging after three consecutive interviews) was achieved (Vasileiou et al., 2018).
Analyses
Survey data was subjected to descriptive statistical analysis in SPSS (Corp, 2019). Interviews were audio-recorded, transcribed verbatim, anonymised, and subjected to thematic analysis (Clarke & Braun, 2017) using NVivo 12 (Lumivero, 2020). A preliminary coding structure was developed inductively through an iterative process. Three authors (NB, LRG, JS) individually familiarised themselves with three transcripts, reading the transcripts line-by-line, and applying a code to relevant text. Initial codes were aggregated into categories, which formed the coding structure. This process was repeated once more. The coding structure was then applied to the remaining transcripts by two authors (NB, LRG). Categories were added and revised as required. Themes were developed from the categories alongside characteristic quotes. Differences between researchers were resolved through consensus. Themes identified through thematic analysis were then mapped to a matrix in excel to compare themes across different roles, health services, and settings (Gale et al., 2013).
Qualitative results related to barriers and facilitators to implementation were then mapped against the CFIR domains - intervention characteristics, outer setting, inner setting, individuals, and process (Damschroder et al., 2022).
Results
Demographic Characteristics and Clinical Experience of Interviewees.
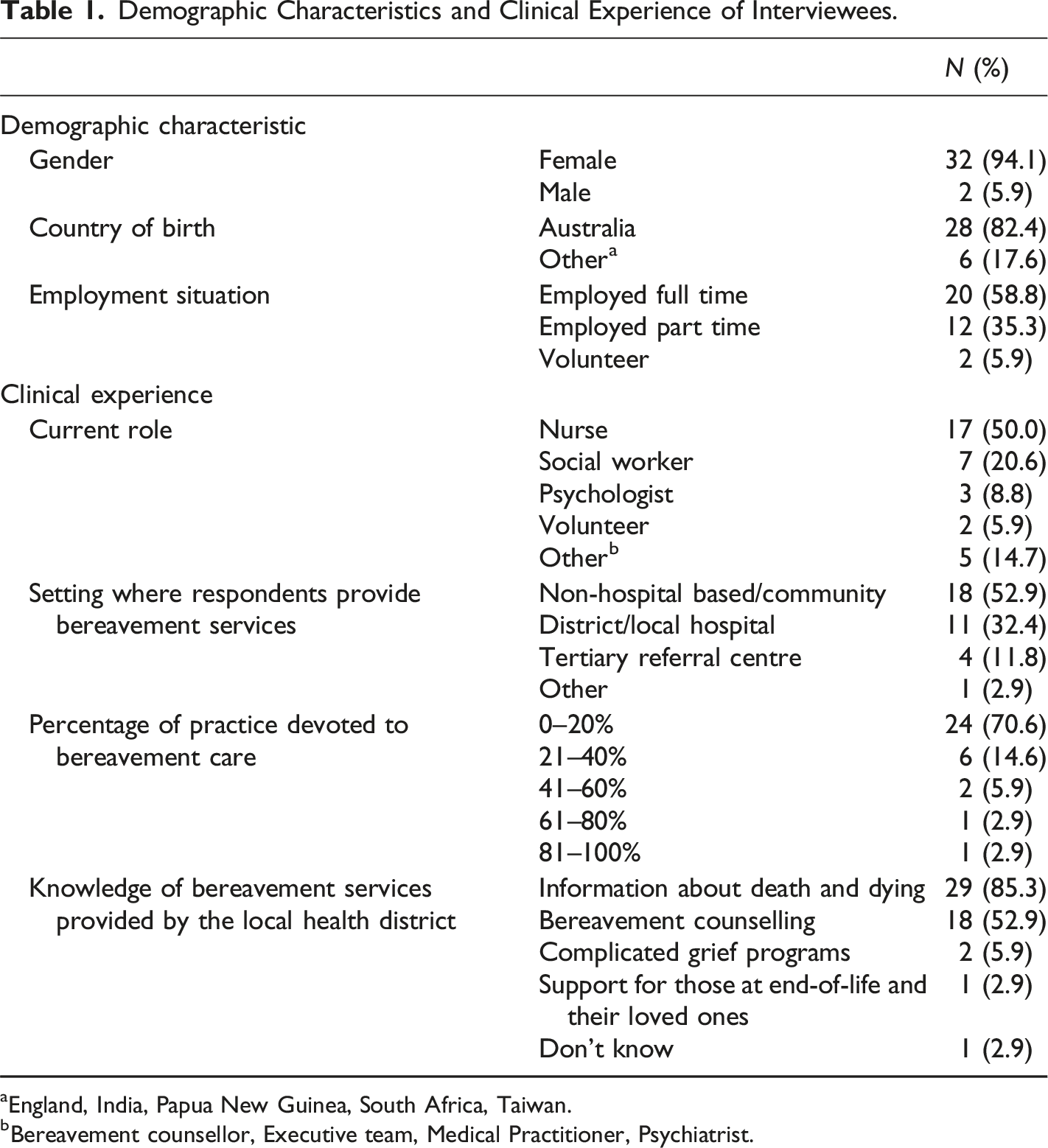
aEngland, India, Papua New Guinea, South Africa, Taiwan.
bBereavement counsellor, Executive team, Medical Practitioner, Psychiatrist.
Thematic analysis identified five themes: 1. Conceptualisation of bereavement was setting dependent; 2. Formal versus informal delivery of care; 3. Current bereavement services, referral pathways, and evaluation; 4. Barriers and Facilitators to accessing and providing care; 5. Ideal bereavement model of care.
Theme 1: Conceptualisation of Bereavement was Setting Dependent
For areas of the health service where death is expected (e.g., palliative care, aged care, chronic/complex care), or when the individual’s role involved caring for patients at end-of-life, bereavement care was perceived as beginning pre-death and included anticipatory grief and loss support, as well as care at and after death. In contrast, in areas where deaths were sudden/unexpected, bereavement care commenced at or after death. ‘We would define bereavement, prior to someone passing but also after… we would do quite a lot of support around grief and loss.’ (PID27) Aged Care ‘I, myself, would say bereavement is after the death.’ (PID24) Neonatal
Theme 2: Formal versus Informal Delivery of Care
Views about formal versus informal delivery of bereavement care focussed on the existence or awareness of protocols, processes, and responsibilities. Neonatal staff indicated that their service had policies, procedures, and protocols for end-of-life care, including bereavement. ‘Yes, for every step really… moving into comfort care, talking to the parents about stopping intensive care… there are policies, procedures, and protocols for everything.’ (PID24) Neonatal
Overall, however there was a sense that bereavement care occurred within an informal structure and most interviewees were unaware of bereavement protocols/policies for the health district. ‘It’s definitely informal. There is nothing structured, there’s nothing formal, there’s nothing that we follow.’ (PID11) Supportive and Palliative Care
Linked to this was the sense that bereavement assessment and care was provided on an ad-hoc basis, depending on perceived roles or responsibilities. Perceived responsibility was often based on previous experience in bereavement care, existing relationships with the patient and/or carer, or capacity. ‘Because I’d already had contact with them, she came back to see me.’ (PID16) Mental Health
Theme 3: Current Bereavement Services, Referral Pathways, and Evaluation
Timing of Bereavement Care
Care provided along the death and dying continuum varied based on role, and service within the health setting. In palliative care, oncology, chronic/complex, and aged care, it was reported that nurses, social workers and volunteers commenced bereavement support for carers/family members prior to the patient’s death by facilitating conversations about death and dying. ‘It’s just providing an opportunity for people to talk and to ask questions.’ (PID25) Supportive and Palliative Care
In settings where deaths were more sudden (neonatal, acute), it was more common for nurses and social workers to report providing support during medical decision-making. ‘Part of the bereavement work that I do, is being in meetings… to make the decision whether we cease intensive care or continue intensive care.’ (PID24) Neonatal
Bereavement Services Provided
Typically, bereavement support across settings included empathetic conversations about the death, support while viewing the body, facilitating a quiet space to grieve, as well as provision of practical and support information. ‘Bereavement pack that we give out to people, we do that pretty close to the death itself… we hand over the pack, which has very general information in it… it’s just a condolence note from us… understanding grief. I find that the Centrelink booklet is very, very useful.’ (PID28) Supportive and Palliative Care
Specific services also arranged memorial services as part of their bereavement support programs and invited bereaved families to attend. ‘I think the memorial day is an important part of [bereavement care]… where people find joy, meaning and connection… gives people a chance to reconnect often with some of the people who took care of their family member.’ (PID25) Supportive and Palliative Care
Bereavement care provided on an ad-hoc basis included facilitating cultural and religious death rituals, and follow-up care (e.g., home visits, phone calls). These were more likely to be provided if the staff/volunteer had formed a bond with the bereaved while caring for the patient. ‘We might call them just to follow up in a couple of days to see how they are… do a follow-up two and six weeks after.’ (PID8) Supportive and Palliative Care
Bereaved individuals were referred for more intensive bereavement care by staff/volunteers involved in the care of the patient pre-death and at death. ‘For complex grief, that’s when we get (social worker) involved… prior to their death… and I’ve got to say when we have the intervention with (social worker), it’s fantastic.’ (PID18) Supportive and Palliative Care
Bereavement counselling provided by social workers occurred in crisis situations, but there was also a sense that referrals to social work occurred when staff/volunteers were not confident or comfortable with providing. ‘So after-hours roster is sort of short, sharp interventions… And that’s often immediately before someone passes or immediately after they’ve passed… we then can refer to longer-term support if needed.’ (PID27) Aged Care ‘Sometimes we probably get the referrals because staff are panicking, and they don’t know what to do and they don’t feel comfortable, so they look for someone they can refer to.’ (PID10) Acute Care
The Aboriginal Health Unit and Aboriginal Health Liaison Officers were seen as integral in connecting bereaved Aboriginal and Torres Strait Islander peoples to appropriate cultural, community, and health services. ‘[Aboriginal Health Liaison Officer] helped to facilitate a smoking ceremony to help the person’s spirit to be able to leave ICU, so he was very much involved with the social worker, working together, to try to enable that to happen from a cultural perspective.’ (PID10) Acute Care
Referral to community services, such as community-based counsellors, not-for-profit organisations providing bereavement counselling, websites and information on grief and bereavement, bereavement support groups, and telephone support services (Griefline, Lifeline), were more commonly mentioned for specific populations (e.g., neonatal, cancer). Additionally, interviewees discussed referring individuals to their General Practitioner (GP) when unsure of other referral pathways, or to discuss and facilitate access to specialist grief intervention. Some interviewees, particularly palliative care, oncology, and chronic/complex staff/volunteers stated that referring to community-based services was not ideal as they felt like they were abandoning the bereaved. ‘The only place I can refer someone on to is GriefLine, Beyond Blue, their GP, somewhere like that which feels awful, I really hate doing that.’ (PID14) Supportive and Palliative Care
Bereavement Risk Stratification Practices
Where social workers felt that bereaved were at risk of PGD, they referred to specialist psychology and psychiatry services. ‘If we did think it was complicated grief, we’d often refer, probably, to the psychiatry team here at [the hospital].’ (PID27) Aged Care
However, within the district there was no formal bereavement risk screening process. Clinical judgement, familiarity with the family, own discomfort with death and dying, and knowledge of referral pathways were reportedly used to determine who and when to refer for further bereavement care. Formal bereavement assessment was done only as part of specialist intervention. Interviewees felt that relying on staff/volunteer judgement for referrals meant that those with less visible grief sometimes fell through the gaps. ‘Families that look like they’re managing, they might not get referred, because the nurses think, “oh, well, they’re okay”, and so we might get a referral or might not, whereas if there’s a lot of distress, we will often get that referral.’ (PID10) Acute Care
Interviewees noted a lack of services to refer onto, for example peer support groups, bereavement counsellors, and community resources, as well as a lack of cultural/language appropriate resources available. Interviewees did acknowledge that their own lack of awareness of the services available was also a gap. ‘We actually don’t have a lot of other bereavement resources in our area... We don’t have any group support to refer people to.’ (PID 13) Supportive and Palliative Care
Theme 4: Barriers and Facilitators to Accessing and Providing Bereavement Care
Participants highlighted both patient, health professional and system level factors that influenced access to and provision of bereavement services.
Accessibility to Bereavement Services
Interviewees perceived that accessibility (telehealth, publicly available information) and affordability (financial comfort, free services) facilitated bereaved individuals accessing care. Further, bereavement staff to help navigate the bereaved through the health system, as well as follow-up care provided by staff known to the bereaved facilitated greater engagement with bereavement care. ‘It depends on what the relationships were and how long it’s been before they died with the carers. If it’s been like, six months or more, you’ve got a relationship and they’re quite open to you coming back for a visit just to see how they are. But if it’s been very quick… They’re just not open to that… they don’t know you, so they don’t have that relationship with you.’(PID35) Supportive and Palliative Care
Participants reported that cost of community-based services, costs associated with accessing care in person (travel) and via telehealth (internet, data) impacted families from accessing bereavement care in their community. Similarly, low health literacy, a lack of culturally appropriate resources and unappealing information resources that fail to draw people’s attention to available information and support were identified as barriers for families engaging with written resources. “it’s all printed out skewed, it’s not straight, it’s not coloured, it’s not pretty, it didn’t draw my attention to it, …it’s something that someone’s photocopied from a photocopy of a photocopy… Kind of an afterthought is how it feels.” (PID39) Clinical Management
Some families were also reluctant to return to the health service where their loved one died to receive bereavement care. Additionally, those with pre-existing mental illness, who are potentially at greater risk of developing complicated grief, are also potentially less likely to engage with bereavement services due to negative experiences with mental health services previously and/or less likely to be offered specialist bereavement support. ‘It can be quite traumatic to come back… they have memories of the patient, the patient has gone through treatment and things like that… the treatment centre itself can be a barrier.’ (PID32) Cancer Care “having mental illness means that they're less likely to access services that they need. Or they might be referred back to their usual mental health services instead of getting sort of dedicated professional bereavement support, which is a slightly different thing.” (PID13) Supportive and Palliative Care
Staff Factors
Staff/volunteer characteristics, skills or experiences facilitated provision of bereavement care. Staff with a clinical interest in grief, loss, and bereavement and/or comfort with death and dying were more likely to provide bereavement care. Similarly, previous clinical experience and personal bereavement experience as well as bereavement training were identified by participants as facilitators to bereavement care. ‘I went to my first memorial service for my husband… and it was just so important for me to see the team that allowed us to do what we achieved. Now… I get very involved in the memorial service. I go on the committee and just make sure I’m a presence there…’ (PID9) Supportive and Palliative Care
Staff/volunteers not having an opportunity to build rapport with bereaved, was identified as a barrier to providing care. Interviewees also felt that visibly distressed individuals or families who had established a relationship with the patients’ health professionals during care would be more likely identified by healthcare teams as needing bereavement care. ‘We may only know them for a day or two. So, it’s a bit weird. If I haven’t got a relationship with them, I don’t give a card. I give my condolences.’ (PID18) Supportive and Palliative Care
System Level Factors
Appropriate resourcing, such as dedicated staff (bereavement counsellor) and spaces (family rooms), and established referral pathways and community connections were identified as supports for staff in delivering bereavement care. Bereavement training and support for staff/volunteers were also noted as important facilitators to care delivery. ‘We do support and training in grief and anticipatory grief… and the different sorts of grief.’ (PID20) Supportive and Palliative Care
One interviewee noted that collecting data related to bereavement care provision was motivating for staff as they could see that providing this care did not impact their workload and it was well received by bereaved individuals. ‘The bereavement phone calls, we are tracking time, they’re taking anywhere from 20 min to about 45 min… we keep track of whether they were agreeable for the follow-up, who we referred to and any comments that the family made… so it looks like we’ve gone through some grief resources, we’ve arranged for some calls with medical teams.’ (PID10) Acute Care
As the bereaved are not considered clients of the health service, a key barrier was the lack of a funding model to support bereavement care. Further, system barriers identified included a lack of training, workforce capacity, and a lack of time. ‘But it’s a huge local health district, and they’re just spread way too thinly.’ (PID20) Supportive and Palliative Care
Theme 5: Ideal Bereavement Model of Care
Interviewees felt that an ideal bereavement model of care included continuity of care. This involved bereavement care being provided by staff known to the family or coordinated care across the district via a dedicated bereavement coordinator or counsellor. ‘In an ideal world, they will have the consistent clinicians coming through the door and that’s their supporting group throughout the process.’ (PID31) Community Health ‘If there was a bereavement counsellor who we got involved with families before the death of their loved one who could then continue the care afterwards that would be great.’ (PID34) Supportive and Palliative Care
Quality care, resources, and established referral pathways were also identified as key to ideal bereavement care. ‘It would be good to have resources that we could actually give out to people… in different formats as well, and obviously different languages and things.’ (PID26) Supportive and Palliative Care ‘It will just be good to have a reliable supportive and palliative care bereavement service that we know is sufficiently resourced to support our patients and caregivers.’(PID36) Supportive and Palliative Care
The model also included structured and formal bereavement processes; ‘A service where there’s sort of a systematic assessment of everybody who comes through our service that might need care, rather than this kind of ad-hoc refer if you’re worried kind of service.’ (PID13)
Supportive and Palliative Care an inclusive service, considering cultural and religious customs; ‘Asking them “are there any special cultural or religious considerations we need to hear from you, so we can support you in this time.”’(PID19)
Supportive and Palliative Care and staff education and support. ‘Training the staff… the staff being able to pick up the differences… and being able to provide the basic psychoeducation and provide those basic referrals.’ (PID41) Mental Health
The bereaved-centred bereavement model of care in Figure 1. Illustrates the relationships between themes and subthemes and the CIFIR domains captured in these themes and subthemes (e.g., inner setting, implementation processes). Bereaved-centred bereavement model of care.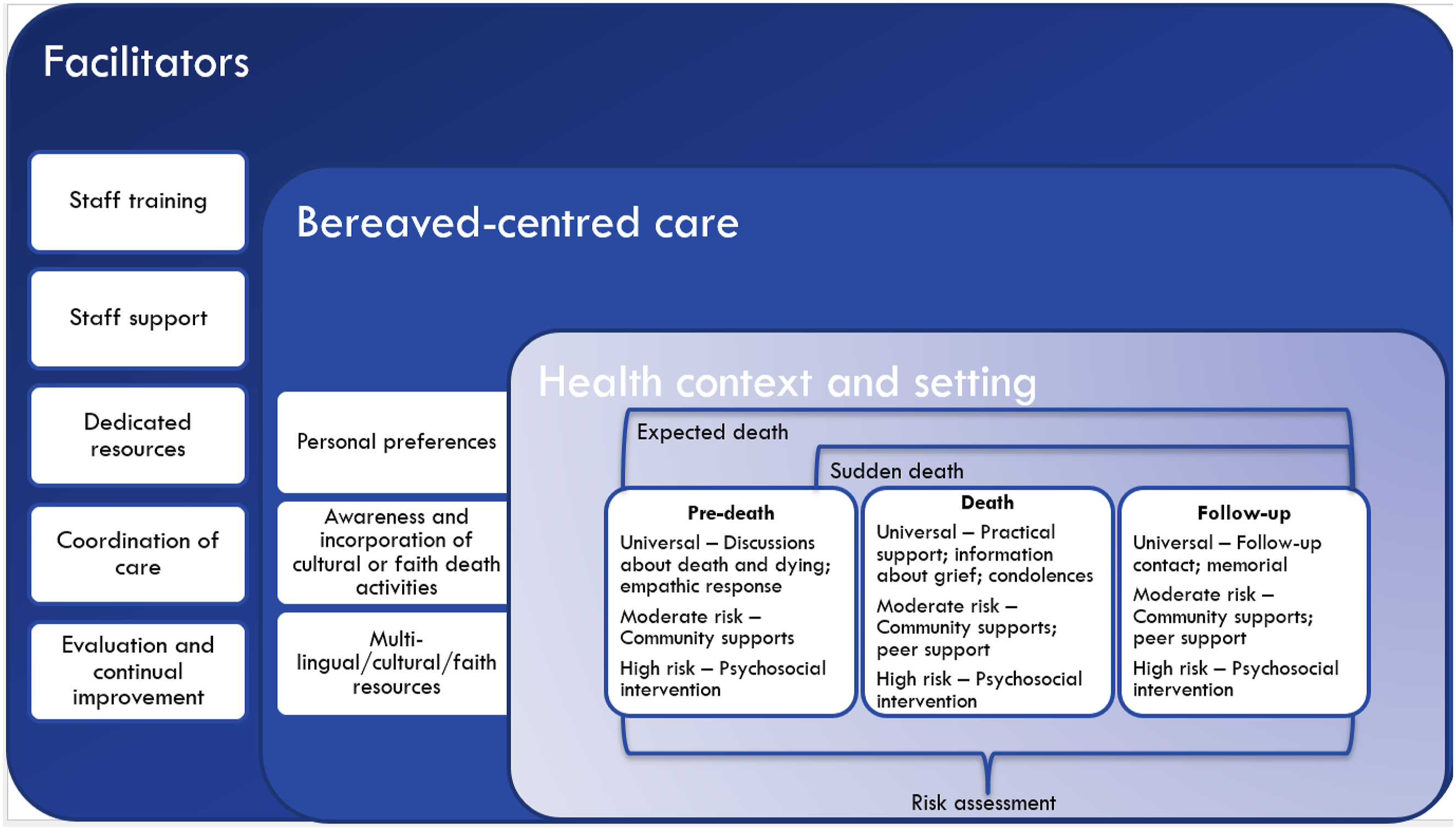
Discussion
There is a disconnect between current bereavement practice in Australia and what is considered best practice in the literature, and by staff/volunteers delivering care. Services are siloed, and the level of care provided is not consistent. Previous research has focused on bereavement models developed for specific services, such as palliative care, with little consideration of the model’s utility across departments/services (Bartley et al., 2025). This approach reinforces the siloed approach to health care delivery and does not consider the value of co-ordination of care and resources across the wider health service.
Our research found that the health context and setting influences bereavement care and timing. Similar to previous research we found that care is ideally initiated at end-of-life (expected deaths) (Blackburn & Dwyer, 2017; Cole et al., 2020; Edwards, 2020; Goldberg et al., 2021; Grant et al., 2021) or as the patient dies (sudden deaths) (Cooper et al., 2020; Edwards, 2020; Goldberg et al., 2021; Grant et al., 2021; LeBrocq et al., 2003; Williams et al., 2000), and continues through post-death follow-up. Our findings also support the public health stepped approach (Aoun et al., 2012; Mc Loughlin, 2018; National Institute for Clinical Excellence, 2004) to bereavement care provision, with universal care for all bereaved, through to specialist services for those at risk of PGD and/or other adverse health outcomes such as development of anxiety, depression, post-traumatic stress reactions that contribute to complicated grief. The appropriate care, resources, and referral pathways at each step should be tailored to when along the death and dying continuum it is delivered. For example, universal care typically takes the form of conversations about death and dying pre-death, bereavement packs at death, or memorial services in follow-up (Bartley et al., 2025).
Consistent with previous research in ICU, palliative care, oncology and hospital wide settings, (Morris & Block, 2015; Morris et al., 2017), we found that patients and subsequent bereaved populations influence care, resources and referral pathways. For example, bereavement care provided in the context of neonatal deaths focusses on parents and includes memento/memory making activities, and referral to support groups (Bartley et al., 2025). Whereas bereavement care in oncology or palliative services may involve carers/family members more broadly, and could include bereavement packs, condolences cards, memorial services, and/or psychoeducation (Bartley et al., 2025).
Further, we know that that individuals and families experience bereavement differently (Downar et al., 2020; Stewart-Lord et al., 2022). Therefore it is important for those delivering bereavement care to understand death rituals, practices and customs for the communities that they serve (Blackburn & Dwyer, 2017; Goldberg et al., 2021; Grant et al., 2021; LeBrocq et al., 2003; Levick et al., 2017). Where possible, understanding patient and family preferences and any cultural beliefs and customs should occur early in their interactions with the health service. In Australia, this could be incorporated into the Advanced Care Planning process. An inclusive bereavement model of care is particularly important in the context of Australia’s First Nations and Culturally and Linguistically Diverse Communities and highlights a need for resources that are not only readable, understandable, and actionable at a general population level, but also relevant to and inclusive of multi-lingual, multi-cultural, and multi-faith communities (Chaplin, 2003; Cole et al., 2020; Mayland et al., 2021; Rodriguez Grieve et al., 2024). This suggests that bereavement models of care should allow for flexibility to tailor care for specific populations and align care to personal and cultural belief preferences.
Our research found that bereavement risk assessment was occurring informally, however there was a desire for a more structured and formalized risk screening process to enable identification of risk of adverse psychological outcomes and guide the level of care. These results are supported by a recent systematic review of 64 studies (Bartley et al., 2025) which found that that most bereavement models of care internationally across a variety of health settings and populations do not include formal assessment for bereavement risk.
As grief evolves and changes over time (Prigerson et al., 2021), repeated screening should be conducted as bereaved individuals move through the death and dying continuum (Blackburn & Dwyer, 2017; Grant et al., 2021). The best approach to risk assessment - use of routine screening tools (Blackburn & Dwyer, 2017; Snaman et al., 2017), versus clinician judgement (Grant et al., 2021) - is however debated in the literature. Routine formalized screening and risk assessment has been shown to be effective in assisting health care providers to identify psychological distress in primary care (Salinas et al., 2023), and in cancer patients (Mitchell, 2013), and is recommended as standard of care (Butow et al., 2015; Salinas et al., 2023). An essential element of screening for risk, however, is to ensure that referral pathways are in place to manage those identified at risk of adverse outcomes.
This research adds valuable insights into factors that influence implementation of bereavement models of care. Consistent with a systematic review of international bereavement models of care and implementation barriers and facilitators including studies across a range of health services (Bartley et al., 2025), we found that staff training and support, infrastructure and available resources, and continual improvement were seen as important facilitators to health professionals and volunteers in our study. These facilitators also align with inner setting domain and implementation process domain constructs of the CFIR (Damschroder et al., 2022).
Studies reporting on implementation of bereavement models of care across a broad range of services suggests that staff/volunteers who provide bereavement care need training on grief, loss, and bereavement, and the specific model of care (Bartley et al., 2025). Access to knowledge and information can also be through guidance documents such as formal protocols, process, responsibilities, and documented health service and community referral pathways (Cole et al., 2020; Cooper et al., 2020; Edwards, 2020; Goldberg et al., 2021; Morris et al., 2017; Silloway et al., 2018; Snaman et al., 2017; Steen, 2019). Similarly, the CFIR inner setting domain construct deliverer-centeredness culture, which ensures that staff/volunteers, especially those exposed to multiple patient deaths, are provided with informal (e.g., debriefing), or formal (e.g., bereavement rounds) support is important is in reducing their own risk of distress (Bartley et al., 2025).
The evidence also highlights that infrastructure and available resources (inner setting domain) are required for successful implementation of the bereavement model of care. Specifically, bereavement staff (e.g., bereavement coordinator or counsellor) (Grant et al., 2021; Morris et al., 2017), formalized roles and responsibilities within existing staff roles (e.g., nurses, social workers) (Cole et al., 2020; Silloway et al., 2018; Snaman et al., 2017; Steen, 2019), dedicated spaces (e.g., family rooms) (Williams et al., 2003), and/or publicly accessible bereavement information and webpages.
Finally, reflecting best practice in implementation (CFIR implementation process domain), assessing implementation, service, and patient outcomes ensures continual improvement in the care delivered (Proctor et al., 2011).
This research used an implementation framework, the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2022) to understand the contextual factors that influence provision of bereavement care across health settings, proposing a model of care (Figure 1) that will be feasible and acceptable to deliver across health services in Australia. A similar model, the Transitional Model, has recently been recommended for bereavement in the context of palliative care (Lichtenthal et al., 2024). This model highlights the need to bridge the gap between health-care systems and community-based bereavement support available to the bereaved. The model highlights the importance of bereavement care being initiated within palliative care prior to the patient’s death and a coordinated risk stratified transition from hospital- to community-based care after death. However, the model proposed by our group extends beyond this model to include bereavement care recommendations for those families for whom death is sudden and unexpected and uses the CFIR (Damschroder et al., 2022) as a conceptual framework to understand the facilitators to provision of bereavement care across health settings. This bereavement model of care seeks to provide a framework for bereavement care provision that can be tailored to provide specific services and resources depending on the health context and setting, and personal and cultural and/or faith practices. Future research to evaluate the feasibility and acceptability of implementing the model in a range of health care settings is required. Implementing the model into different settings will help determine the level of tailoring of the model and will assist in development of implementation strategies, such as staff training, to facilitate implementation (Damschroder et al., 2009). With debate in the literature around the best approach for screening and risk assessment, future research should investigate the most appropriate, and acceptable method for screening for risk of poor outcomes in bereaved individuals. For example, a qualitative study (n = 38) exploring acceptability of a new bereavement risk screening measure in the context of advanced cancer reported that while people experiencing bereavement were generally supportive of screening, the timing and process of screening varied across participants (Roberts et al., 2020).
Although this research included staff and volunteers who deliver bereavement care within a single health district in NSW, Australia, the findings are relevant to Australian health settings more broadly as this health district includes broad health service delivery, encompasses hospital and community-based services and a large diverse patient population. The findings may inform but may not be generalizable to international health services with different service delivery models. We also did not include bereaved individuals in this stage of the research, so the views of care recipients are not captured in this research.
This research contributes further evidence on delivering bereavement care in the Australian health system. The model developed provides a framework for bereavement care delivery and recommends tailoring the model to the specific health context and setting, as these factors will influence service delivery.
Supplemental Material
Supplemental Material - Developing a Bereavement Model of Care for an Australian Health Context
Supplemental Material for Developing a Bereavement Model of Care for an Australian Health Context by Nicci Bartley, Luna Rodriguez Grieve, Laura Kirsten, Cindy Wilson, Betsy Sajish and Joanne Shaw in OMEGA - Journal of Death and Dying
Footnotes
Acknowledgments
Thank you to the health professionals and volunteers for taking the time and effort to participate in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Nepean Blue Mountains Local Health District through the NSW Health Enhanced Bereavement Funding Scheme.
Ethical Statement
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.