
Abstract
This study assesses the frequency of reported paranormal phenomena by palliative care professionals in Portugal and their impact on spirituality, clinical practice, and training. A retrospective study in adult palliative care settings was conducted using the ParaPall survey, created by the authors, between October 2022 and January 2023. Participants answered a demographic questionnaire, ParaPall survey, PANAS score, and Intrinsic Spirituality Scale. A sample of 137 participants was obtained, with 89.4% reporting at least one phenomenon. Terminal lucidity (84.7%) and patients passing shortly after significant visits were the most reported. Professionals who reported more phenomenon tended to adopt a spiritual interpretation (p < .001) and showed a higher investment in patient care, while nonspiritual interpretations were linked to avoidance behaviors. Paranormal phenomena influence spiritual beliefs and professional well-being. Results emphasize the need for open discussions and training to help professionals navigate these experiences, enhancing patient care and provider well-being.
Introduction
The dying process is often accompanied by profound subjective experiences that are deeply influenced by personal history, self-awareness, and interpersonal relationships (Kerr, 2020). Many of these experiences challenge conventional scientific explanations and have been increasingly documented in palliative care settings. They have been referred to in the literature under various terms, including end-of-life experiences (ELEs), deathbed visions, unusual end-of-life phenomena, and nearing death awareness (Brayne et al., 2006; Fenwick & Brayne, 2011; Kerr et al., 2014). These phenomena commonly include visions of deceased loved ones, out-of-body experiences, terminal lucidity, premonitory dreams, and a heightened sense of peace or spiritual presence (Kerr, 2020).
Recent research has shown that ELEs are not uncommon, with their reported frequency ranging from 28% to 87% (Bertão et al., 2025). In studies with healthcare professionals, prevalence ranges from 28% to 95%, depending on whether they have personally witnessed or been informed of such experiences in their clinical practice (Silva et al., 2023). The most frequently reported ELEs include end-of-life dreams and visions, which are often described as deeply meaningful and emotionally impactful (Bertão et al., 2025).
Studies indicate that these experiences are observed across diverse cultures and religious backgrounds. They often occur in the final days or weeks of life (Fenwick et al., 2007, 2010). They tended to be interpreted as inherent to the dying process and considered a spiritual event by patients, relatives and healthcare professionals (Bertão et al., 2025).
From a clinical standpoint, ELEs play a significant role in shaping the quality of the dying process. In most cases, these experiences are described as deeply comforting, offering relief, peace, and a sense of hope to dying individuals and their grieving families (Brayne et al., 2006; Mazzarino-Willet, 2010). However, some experiences can evoke fear or distress, particularly when linked to unresolved emotional conflicts (Kerr et al., 2014; Morita et al., 2016; Nosek et al., 2015).
Contrary to misconceptions that ELEs are mere hallucinations or medication effects, research highlights their distinct psychological and existential significance (Betty, 2006; Ethier, 2005; Fenwick et al., 2007; Grant et al., 2020; Houran & Lange, 1997; Nosek et al., 2015). Nonetheless, patients, relatives, and healthcare professionals often hesitate to discuss them due to fear of skepticism, emphasizing the need for specialized training and guidance to support the clinical management of these experiences in palliative care (Brayne et al., 2006; Devery et al., 2015; Fenwick et al., 2007; Lawrence & Repede, 2013; McDonald et al., 2014).
Despite increasing documentation of ELEs, less attention has been given to the perspectives of palliative care professionals, who often encounter these phenomena in their clinical practice. Healthcare providers play a crucial role in responding to ELEs, yet research on how these experiences influence their spiritual beliefs, clinical decision-making, emotional well-being, and professional training needs remains scarce.
Notably, there is no known research exploring ELEs in palliative care settings in Portugal, leaving a gap in understanding how cultural and professional contexts shape the perception and management of these experiences. This study seeks to address this gap by investigating Portuguese palliative care professionals’ experiences and attitudes toward ELEs. Through the ParaPall survey, we aim to assess the frequency of these experiences, how healthcare professionals interpret them, and their impact on professionals’ spirituality, clinical practice, and training needs. By doing so, this research seeks to contribute to a more comprehensive understanding of ELEs in palliative care, ultimately enhancing the support and care provided at the end of life.
Aims
Paranormal phenomena at the end of life remain unstudied in Portugal. This study pretends: (1) to measure the frequency and type of paranormal phenomena at the end-of-life (EOL) using a new survey called ParaPall; (2) to understand how health professionals interpret paranormal phenomena and their impacts on their spirituality, clinical practice, and training needs; (3) to asses health professionals level of intrinsic spirituality, and emotional affects around paranormal phenomena.
Material and Methods
Study Population and Overview of the Approach
A retrospective study was conducted in the palliative care setting in Portugal. According to the Observatório Português dos Cuida dos Paliativos Relatório 2019 report, there are 103 palliative care teams in hospitals and communities in the country and, on average, 817 healthcare professionals. Initially, the authors suggested visiting the palliative care teams in person. However, the COVID-19 pandemic has limited this proposal. Therefore, the authors chose to find palliative care teams at online meetings.
The authors emailed all the adult palliative care teams of the National Health System of Portugal, inviting them to participate in a voluntary study. The teams that agreed had an online meeting with the authors, who emphasized the significance of the research and clarified the concept of paranormal phenomena. Paranormal (from Greek -para means “beside/beyond,” and from Latin normali, which means “according to the rule”) refers to events or experiences that fall outside the range of what is typically understood by science or conventional logic (Dean et al., 2022). At the end of the author’s presentation, a Google® Forms link was shared so that participants could complete the survey during or after the online meeting, depending on their professional or personal convenience. The Google® Forms link comprises four sections: (1) Demographic questionnaire; (2) ParaPall Survey; (3) PANAS VRP Scale (Galinha et al., 2014); and (4) Intrinsic Spirituality Scale (ISS) (Hodge, 2003). All the sections were in Portuguese, with the last scale (ISS) being translated and validated by the authors beforehand (Dalcolmo et al., 2025). The estimated completion time was approximately 20 minutes.
All participants received a comprehensive and complete explanation of the study and obtained informed consent before participating, with guaranteed confidentiality.
The authors engaged with palliative care teams from the initial invitation through an online meeting held between October 2022 and January 2023. Initially, 21 palliative care teams responded to the invitation, corresponding to a response rate of 20.3%. Among the participants, 140 completed the Google® Forms link, and three duplicate responses were excluded. Considering the composition of the teams that responded to the invitation (N = 333), the authors obtained 137 participants, corresponding to a response rate of 41%.
The participants were provided with an email and telephone contact if they wished to share or elaborate on the paranormal phenomena they experienced beyond the survey.
Eligibility Criteria
The study included nurses, medical doctors, social and mental health professionals, and chaplains working in adult palliative care teams within the Portuguese National Health System across hospital and community settings during the study period. Exclusion criteria applied to palliative care teams working specifically in pediatric care within the National Health System or in adult or pediatric palliative care teams within private settings. Participants who did not agree to participate in the study or did not give their informed consent were excluded.
Ethical Committee Approval
The study was submitted to the Ethics Committee of the Centro Hospitalar Universitário de São João/Faculty of Medicine, University Porto, for ethical approval (CE 306-20) in September 2020.
Demographic Questionnaire
Age, sex, religion, type of religion, practicing religious, profession, number of years of professional activity in general and in palliative care, place of work in a palliative care setting, previous paranormal phenomenon knowledge during the academic or professional path, previous formation in paranormal phenomena and previous spiritual assistance education in palliative care were considered demographic variables.
Paranormal Phenomena in the Palliative Care Health Professionals Survey (ParaPall Survey)
ParaPall is a pioneering survey developed in this study by the authors (two clinical psychologists, one PhD in mathematics and one palliative care doctor), inspired by their clinical experience with EOL patients and influenced by the works of Fenwick et al. (2010), Parra & Amarilla (2017), and Claxton-Oldfield and Dunnett (2016, 2018). This self-report survey measures paranormal phenomena and their impact on spirituality, personal beliefs, and clinical practice among palliative care professionals in Portugal and globally.
The ParaPall survey is structured into two parts. Part 1 (“Para-”) investigates healthcare professionals’ recognition of paranormal phenomena in their clinical practice, including experiences such as out-of-body sensations and feelings of presence. In this segment, professionals select from a list of 20 items (Section A) to indicate which paranormal phenomena they have personally experienced or witnessed (they can choose one or more items). They also choose from another 18 items (Section B) to identify which paranormal phenomena have been reported to them by patients and/or families (they can select one or more items). At the end of Sections A and B, there is also the option for those who have never witnessed or to whom any of the paranormal phenomena above were described. At the end of Sections A and B, the participants can respond to an open-ended question where they can tell their own paranormal experiences.
Part 2 (“-Pall”) aims to assess the impact of these paranormal phenomena across three domains (Section C): personal interpretation of the phenomena (1–10), spirituality (11–16), and clinical practice (17–22), as well as the perceived need for training among palliative care professionals (23–27). Using a list of 27 statements, the participants rated their agreement on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). If professionals answer “no” to every question in Part 1, they can provide hypothetical responses in Part 2.
PANAS VRP Scale
The PANAS (Positive and Negative Affect Schedule) was developed by Watson et al. (1988) to measure individuals’ positive affect (PA) and negative affect (NA), reflecting their emotional experiences. A shortened Portuguese version of the PANAS VRP was developed by Galinha et al. (2014), who granted permission for its use in this study. In this Portuguese version, the five positive affect items included “determined,” “active,” “enthusiastic,” “inspired,” and “interested,” whereas the five negative affect items were “afraid,” “upset,” “scared,” “nervous,” and “guilty.” The internal consistency of the short version of the PANAS VRP in the Portuguese version was 0.86 for PA and 0.89 for NA (Galinha et al., 2014). In this study, the PANAS RSP survey yielded Cronbach’s alpha values of 0.879 for PAs and 0.844 for NAs. This study utilized this scale to validate the ParaPall survey by assessing the positive and negative emotional impact of paranormal phenomena known or experienced by palliative care professionals.
Intrinsic Spirituality Scale
The ISS was developed by Hodge (2003) based on Allport & Ross (1967) Allport and Ross’s intrinsic religious motivation scale (1967) and was modified into a six-item scale. This six-item ISS assesses the degree to which spirituality functions as an individual’s master motive, within and outside religious frameworks, for both theistic and nontheistic populations. Each item has two phrases linked to a continuous scale ranging from 0-10. The average score across the six items indicates the intrinsic spirituality level. A score of zero represents an individual for whom spirituality does not act as a motivating factor. Conversely, a score of ten indicates a person who is highly motivated by their spirituality. The ISS demonstrated an overall Cronbach’s alpha of 0.96 in the original study. The researchers translated and validated the scale previously into European Portuguese, awaiting publication, and obtained an internal consistency of 0.966. The ISS had a Cronbach’s alpha of 0.945 in the current study.
Contribution to Validate the ParaPall Survey
A pilot test was first conducted in April 2022 with 30 students enrolled in the Master’s and Doctorate programs in Palliative Care at the Faculty of Medicine of the University of Porto. This test was administered in person to the participants. For validation purposes, only Portuguese students were included. After analyzing the responses, the authors modified section C of the ParaPall Survey, reducing the initial 30 questions to 27.
Based on correlation rates, eight items were consolidated into four: (1) “The occurrence of paranormal phenomena makes me believe in the existence of a soul” was revised to “The occurrence of paranormal phenomena makes me believe in the existence of a higher being/power” (item C11); (2) “The occurrence of paranormal phenomena makes the dying process less frightening for me” was revised to “The occurrence of paranormal phenomena reduces fear of my death” (item C15); (3) “The occurrence of paranormal phenomena makes me feel more invested in caring for and accompanying my EOL patients” was combined with “caring for the families of my patients” (item C17); and (4) “Experiencing these phenomena makes me avoid my patients” was linked with “their families” (item C18).
Three additional items were excluded because they were redundant with the PANAS VRP scale. Two items were refined for clarity and simplicity: (1) “Paranormal phenomena are spiritual and transcendent experiences” was revised to “paranormal phenomena are spiritual phenomena” (item C5); (2) “Paranormal phenomena are part of the dying process” elicited significant disagreement, as it did not align with other interpretations of the phenomenon. To avoid appearing deterministic and overly general, it was modified to “Paranormal phenomena are expected events in the EOL process” (item C6). Finally, four new items were added based on Fenwick’s questionnaire (2010) and a systematic review on the topic previously elaborated by the authors and awaiting publication: (1) “Paranormal phenomena are fabrications of the imagination” (item C4); (2) “Paranormal phenomena are prognostic indicators, more frequent in the last hours to days of life” (item C7); (3) “Paranormal phenomena positively contribute to the grieving process of family members” (item C10); and (4) “I feel that the medical community stigmatizes the reporting of paranormal experiences at the end of life” (item C24).
Retest ParaPall Survey
A test-retest reliability analysis was conducted to evaluate the consistency of the responses across the two time points, with a temporal difference of approximately 2 months. To assess the test-retest reliability of the questionnaire items, we calculated Cohen’s kappa (κ) for the nominal items in Sections A and B and the weighted Cohen’s kappa for the ordinal items in Section C (Cohen, 1960), following the recommendation of the Guidelines for Reporting Reliability and Agreement Studies (GRRAS) (Kottner et al., 2011). Cohen’s kappa accounts for the agreement occurring by chance and can range from −1 to +1. We adopted the interpretation of the κ value proposed by Landis and Koch (1977). According to their guidelines, a κ value of up to 0.20 indicates slight reliability, values from 0.21 to 0.40 indicate fair reliability, values from 0.41 to 0.60 indicate moderate reliability, values from 0.61 to 0.80 indicate substantial reliability, and values from 0.81 to 1.00 indicate almost perfect reliability (Landis & Koch, 1977). Agreement between responses at different times was also assessed (for each question) through the proportions of agreement (PAs), with 95% confidence intervals. This measure provides a straightforward indication of the percentage of times the test and retest agreed without adjusting for chance agreement. The agreement was considered poor if the lower limit of the 95% confidence intervals for Proportions of Agreement was lower than 0.50 (Cohen, 1960).
Using these methods, we aimed to provide a comprehensive evaluation of the test-retest reliability of the questionnaire items, ensuring that the reliability measures were robust despite the small sample size. Unweighted and weighted Cohen’s κ with respective confidence intervals were computed via the package “psych” (Revelle, 2020) from R software, v 4.3.0 (R Core Team, 2020). The reliability and agreement between the two applications of the instrument, accessed with the kappa statistics and the proportions of the overall agreement, for all the questions (dichotomic) in sections A and B, respectively. (Supplemental Material Table 1 and Table 2) There is poor agreement between the test and retest results for 5/21 of the answers in section A (A8, A11, A14, A17, and A19). Concerning section B, the agreement is poorer: only 5/19 of the answers comprising section B did not exhibit poor agreement between the test and retest (B2, B5, B6, B9, and B19. The reliability and agreement between the two applications of the instrument, assessed with weighted kappa statistics and the proportions of overall agreement for all the questions (5-point Likert scale) in section C are shown in Supplemental Material Table 3. There is poor agreement between the test and retest results for all the items of section C except for C.16.
Statistical Analysis
Categorical variables were described by absolute and relative frequencies (n, %), whereas for quantitative nonnormally distributed and ordinal variables, medians and interquartile intervals [Q1; Q3] were used. The data were analyzed via SPSS Statistics (v.28.0; SPSS® Inc., Chicago, IL, USA). Correlations between ordinal and/or quantitative variables (most were not normally distributed) were assessed via Spearman’s correlation coefficient. Comparisons of quantitative/ordinal variables between independent groups were performed via the Mann‒Whitney test. In all the statistical tests, p values <0.05 were considered significant.
Results
Demographic Analysis
Characterization of the Health Care Professionals in Palliative Care Participating in the Study (N = 137).
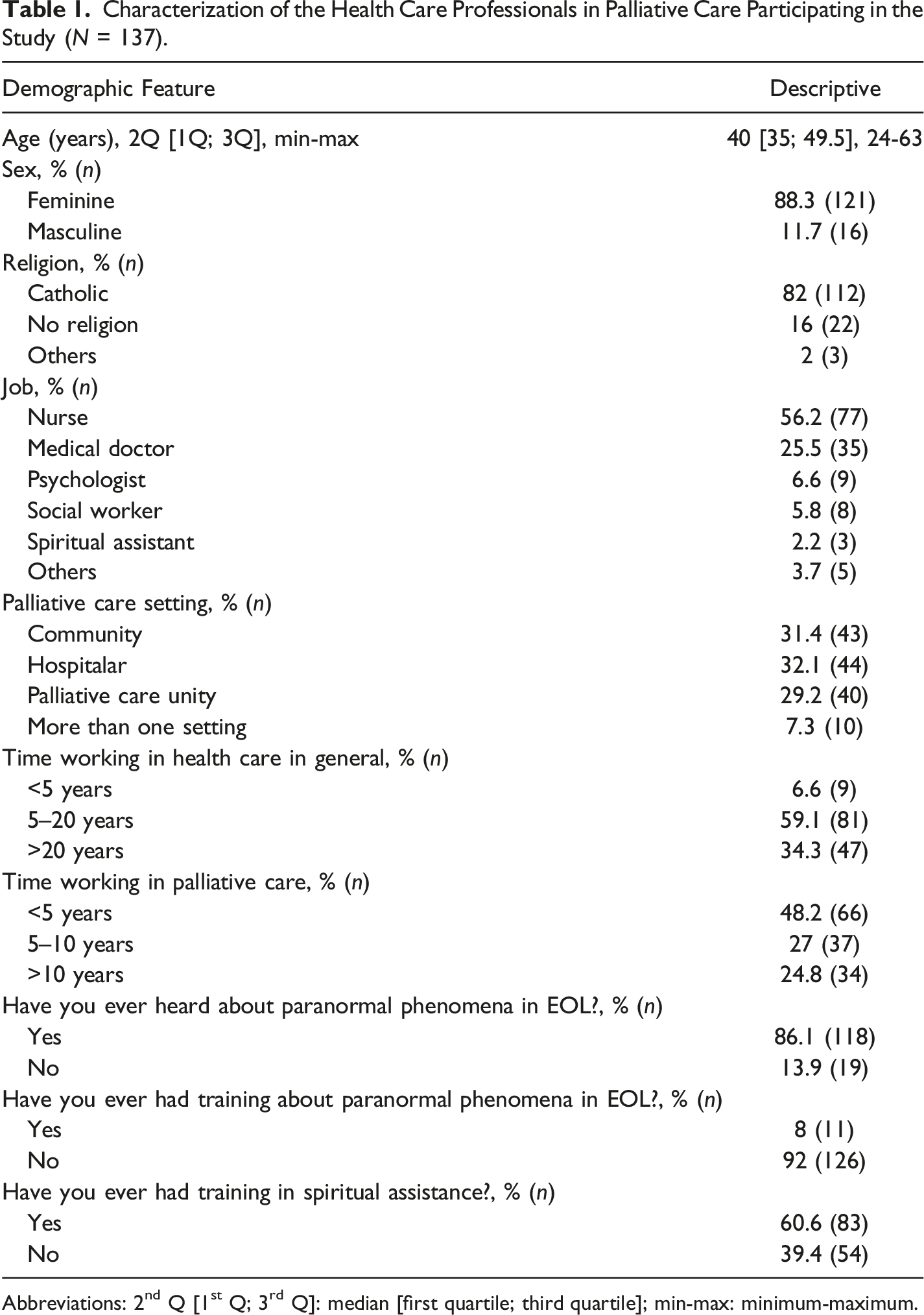
Abbreviations: 2nd Q [1st Q; 3rd Q]: median [first quartile; third quartile]; min-max: minimum-maximum.
Global Prevalence of Paranormal Phenomena
Overall, 89.4% (n = 123) of the healthcare professionals in this study reported encountering at least one paranormal phenomenon, either first-hand or second-hand. Fourteen (10.6%) participants reported never having a first-hand or second-hand paranormal experience.
First- and Second-Hand Paranormal Phenomena
Paranormal experiences have been widely reported. The main participants reported first-hand experiences of terminal lucidity and patients passing soon after visits from significant individuals (84.7%). Other frequently reported phenomena included (1) sensing a presence (25.5%); (2) witnessing patients speaking with deceased relatives (38%); (3) intuitively knowing about a patient’s death or worsening condition (30.7%); and (4) terminal lucidity in previously unconscious or confused patients (50.4%). In second-hand reports (from patients or families), the most common phenomena were (1) visions of deceased relatives (48.9%); (2) terminal lucidity (65%); and (3) death shortly after farewells (67.9%).
Description of the Open-Ended Questions
Many participants described some of the paranormal phenomena they witnessed in more detail. There were four main types of paranormal phenomena: (1)
Paranormal Phenomena Interpretations
Sociodemographic Features
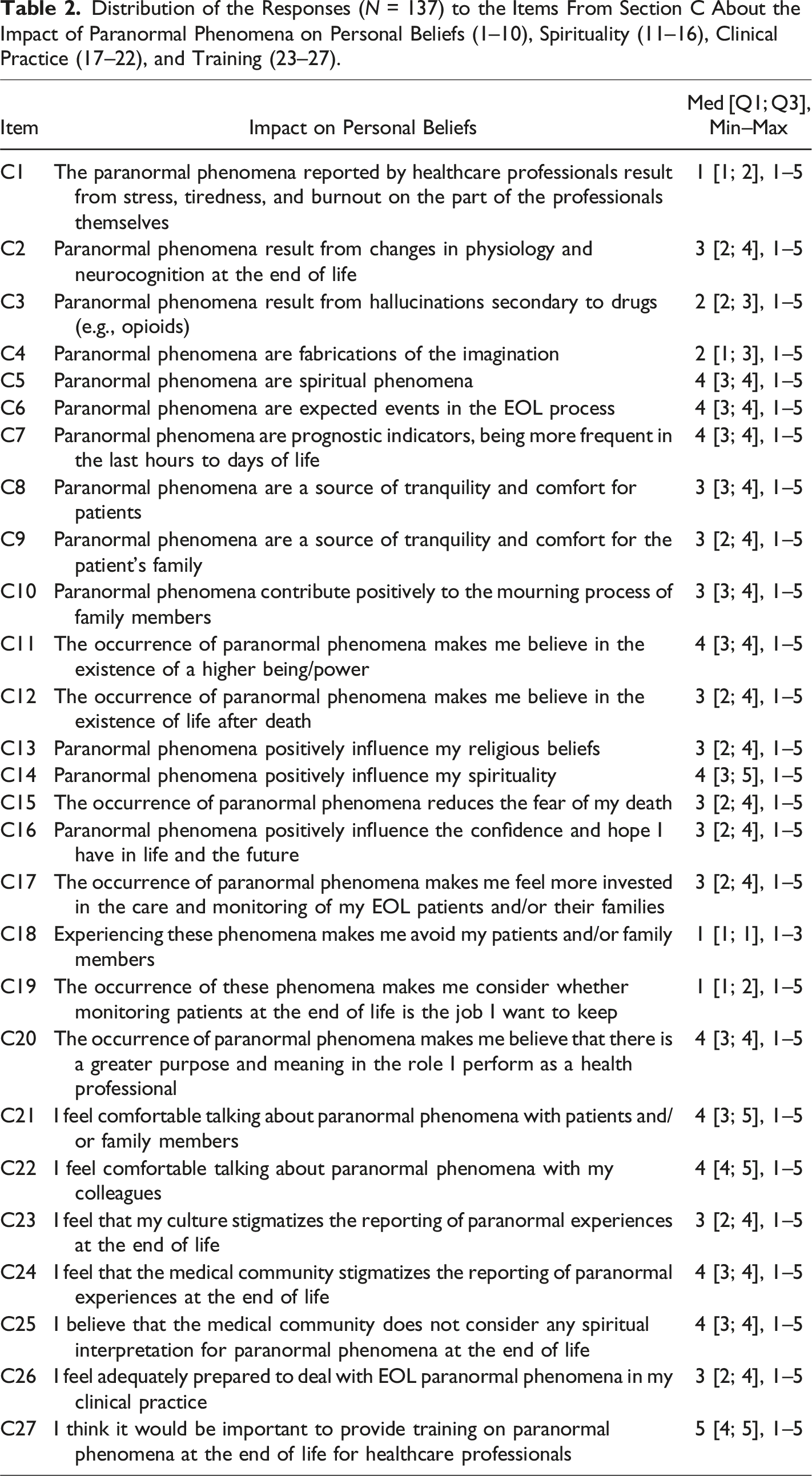
Distribution of the Responses (N = 137) to the Items From Section C About the Impact of Paranormal Phenomena on Personal Beliefs (1–10), Spirituality (11–16), Clinical Practice (17–22), and Training (23–27).
Recognition of Paranormal Phenomena
Professionals who reported more paranormal experiences were significantly more likely to adopt a nonmaterialist/spiritual interpretation of these phenomena and associated them with spiritual events (item C5, r = 0.471, p < .001), prognostic indicators (item C7, r = 0.278, p < .001), comfort for patients (item C8, r = 0.212, p = .010) and families (item C9, r = 0.245, p = .004) and contributed to the grieving process (item C10, r = 0.262, p = .002).
On the other hand, professionals who did not report any paranormal experiences tended to associate them with changes in physiology (item C2, r = 0.312, p = .004), drug-induced hallucinations (item C3, r = 0.295, p = .006), and fabrications of the imagination (item C4, r = 0.346, p = .002), resulting in a materialist interpretation of these events.
Impact on Personal Beliefs
Paranormal phenomena are largely considered spiritual events, are expected during EOL care, and are viewed as prognostic indicators. (Table 2) Stress or burnout as the cause was rated low, as were hallucinations due to medication. (Table 2) However, some phenomena are attributed to physiological changes in dying patients. (Table 2)
Impact on Spirituality
The impact of the occurrence of paranormal phenomena on spirituality tends to be positive. (Table 2) A higher median score supports the positive influence of paranormal phenomena on spirituality and belief in a greater being/power. (Table 2) Those who tend to understand these phenomena as spiritual events (item C5; Table 2) are associated with a belief in greater power (item C11: r = 0.530, p < .001), a belief in life after death (item C12: r = 0.340, p < .001), and a positive impact on spirituality (item C14: r = 0.412, p < .001) (Supplemental Material Table 6).
Interestingly, the participants who have personal beliefs associated with a more materialistic interpretation (items C2, C3, and C4; Table 2), as described above, are associated with lower belief in greater power (item C1: r = −0.311, p < .001; item C2: r = −0.295, p < .001; item C3: r = −0.232, p = .006; item C4: r = −0.371, p < .001), lower spirituality (item C1: r = −0.373, p < .001; item C2: r = −0.255, p = .003; item C3: r = −0.173, p = .043; item C4: r = −0.296, p < .001), fear of death (item C1: r = −0.246, p = .004; item C2: r = −0.199, p = .020) and lower hope (item C2: r = −0.219, p = .010; item C4: r = −0.306, p < .001) (Supplemental Material Table 6).
Impact on Clinical Practice
In general, the participants do not recognize that experiencing paranormal phenomena leads them to avoid patients and/or family members, nor leads to doubts about their job in palliative care. (Table 2) In contrast, paranormal phenomena make them believe that there is a greater purpose and meaning in their role as healthcare professionals. (Table 2) The participants also reported feeling comfortable discussing paranormal phenomena with patients/families and colleagues. (Table 2)
Spiritual interpretations (item C5; Table 2) were associated with greater investment in patient care (item C17: r = 0.260, p = .002), a stronger sense of purpose in their work (item C20: r = 0.369, p < .001), and more comfortable discussions with patients and families (item C21: r = 0.247, p = .004) (Supplemental Material Table 6).
Materialist interpretations of paranormal phenomena (items C1, C2, C3, and C4; Table 2) are consistently linked with negative outcomes in clinical practice and professional well-being. Healthcare professionals who hold these views demonstrate lower levels of engagement in patient care (item C1: r = 0.235, p = .006; item C3: r = 0.198, p = .021), greater avoidance behaviors (item C1: r = 0.311, p < .001; item C3: r = 0.287, p < .001; item C4: r = 0.246, p = .004), greater career dissatisfaction (item C4: r = −0.303, p < .001; item C1: r = −0.296, p < .001), and discomfort when discussing these experiences with patients and/or family (item C1: r = −0.321, p < .001; item C3: r = −0.240, p = .005; item C4: r = −0.270, p = .001) and colleagues (item C1: r = −0.194, p = .023; item C4: r = −0.259, p = .002) (Supplemental Material Table 6).
Impact on Training and Stigma
The participants perceived that medical culture stigmatizes the discussion of paranormal phenomena, with similar views about broader societal stigmatization. (Table 2) Specifically, medical doctors reported greater stigma around discussing paranormal phenomena within the medical community (item C24, p = 0.007). There is a strong belief that spiritual training for healthcare professionals is needed to better handle these experiences in EOL care. (Table 2)
Intrinsic Spirituality and Emotional Response
The median score for each item of the ISS was between 7 and 8, and the median total ISS score was 7.5. The PANAS median positive affect score was 18, and the median negative affect score was 8.
There was a significant positive correlation between higher ISS scores and the number of paranormal phenomena experienced (r = 0.236, p = .005 for first-hand experience, and r = 0.278, p < .001 for second-hand experience). (Supplemental Material Table 7) Healthcare professionals with higher spirituality scores on the ISS were more likely to experience a positive impact on clinical practice and personal spirituality after encountering paranormal phenomena, including finding greater purpose and meaning to their role as healthcare professionals (0.452, p < .001), feeling more invested in patient care (r = 0.355, p < .001), having a stronger belief in greater power (r = 0.520, p < .001), having a belief in life after death (r = 0.417, p < .001), and having a positive influence on religious beliefs (r = 0.377, p < .001). This correlation also extended to reducing fear of death (r = 0.365, p < .001) and fostering greater hope and confidence in life and the future (r = 0.455, p < .001) (Supplemental Material Table 8).
For the PANAS, participants with greater positive affect were more likely to interpret paranormal phenomena as spiritual events (r = 0.423, p < .001), whereas those with greater negative affect were more likely to attribute such phenomena to stress and burnout (r = 0.172, p < .044). Negative impacts were observed among professionals who reported higher levels of negative affect, as they were more likely to avoid patients (r = 0.340, p < .001) and to question their career choices in EOL care (r = 0.223, p = .009). (Supplemental Material Table 9) Additionally, a negative affect was associated with discomfort in discussing paranormal phenomena with patients and families (r = -0.215, p = .012) and colleagues (r = -0.176, p = .040) (Supplemental Material Table 9).
Discussion
This study confirms that paranormal experiences at the end of life are widely recognized by Portuguese palliative care professionals, with 88.3% of participants reporting at least one such occurrence. These results align with previous research, which found similar prevalence rates, such as 62%–84% in the UK (Fenwick et al., 2010), 94.4% in Brazil (Santos et al., 2017), and 98% in the U.S. (Lawrence & Repede, 2013). These findings reinforce that ELEs are commonly observed worldwide in palliative care settings.
Our study revealed some key typologies of paranormal phenomena recognized by healthcare professionals that resonate with those reported in the literature. Terminal lucidity was observed by 84.7% of participants, with 50.4% reporting cases where cognitively impaired patients experienced sudden clarity before death. This finding resonates with Batthyány and Greyson’s (2021) report, which indicates that 87% of dementia patients exhibited paradoxical lucidity, enabling meaningful communication with loved ones.
Additionally, 84.7% of participants noted that patients appeared to delay death until a significant event or the arrival of a particular person, consistent with Fenwick et al. (2010) and Schreiber and Bennett (2014), who described such phenomena as psychological and spiritual processes of preparing for death.
Visions of deceased loved ones were reported by 48.9% of professionals, either through second-hand accounts or direct observations of patients speaking with or reaching out to the deceased (38%). While this prevalence aligns with the 48%–62% range reported in Fenwick et al. (2010), it is considerably lower than the 88.2% found in Santos et al. (2017) and 95% in Lawrence and Repede (2013). The variation in reported frequencies across studies may stem from differences in research methodologies and cultural influences. Despite these discrepancies, the widespread acknowledgment of deathbed visions as meaningful and often comforting experiences is consistent across studies.
The differentiation between ELEs and hallucinations has been a subject of considerable debate, with concerns that misclassification could limit their clinical and research significance (Brayne et al., 2006; Grant et al., 2020; Kerr et al., 2014; Nosek et al., 2015; Nyblom et al., 2021). The moderate agreement in our study regarding physiological and neurocognitive factors as causes of paranormal phenomena aligns with the literature on the high prevalence of delirium in end-of-life care (Hosker & Bennett, 2016). However, drug-induced hallucinations were less commonly endorsed as explanations, reinforcing findings that ELEs are perceived as distinct experiences (Brayne et al., 2006; Grant et al., 2020; Kerr et al., 2014; Nyblom et al., 2021). Unlike hallucinations, which are often disorganized, distressing, and responsive to medication adjustments, ELEs are typically coherent, emotionally meaningful, and usually framed within the patient’s life story (Brayne et al., 2006). Recognizing these distinctions is crucial for ensuring appropriate clinical responses and avoiding unnecessary medicalization (Fenwick et al., 2010; Brayne et al., 2006).
Paranormal experiences were predominantly interpreted as spiritual events, aligning with several studies in the literature (Claxton-Oldfield et al., 2018; Claxton-Oldfield & Richard, 2022; Fenwick et al., 2010; Santos et al., 2017). However, personal exposure to ELEs played a significant role in shaping these interpretations.
Our findings indicate that professionals who reported more firsthand experiences with ELEs were more likely to adopt a spiritual perspective, while those without direct exposure remained more skeptical, associating ELEs with hallucinations or fabrications of the imagination. This pattern has been observed in previous research, supporting the idea that a lack of exposure often correlates with scientific explanations, possibly due to professional education and cultural norms (Claxton-Oldfield & Dunnett, 2016; Fenwick et al., 2010; Kellehear, 2017; Santos et al., 2017).
The way ELEs are interpreted also impacts clinical practice and professional well-being. Those who viewed these experiences as spiritual events reported a greater investment in patient care, a stronger sense of purpose in their work, increased comfort discussing these experiences, and an overall positive affect. These findings align with research showing that spiritual perspectives can improve communication, enhance professional fulfillment, and help people cope with emotional demands (Claxton-Oldfield & Dunnett, 2016; McDonald et al., 2014; Nosek et al., 2015; Santos et al., 2017).
In contrast, interpreting ELEs as the result of stress, hallucinations, or fabrications was correlated with lower levels of engagement in patient care, greater avoidance behaviors, greater career dissatisfaction, and discomfort in discussing these experiences. Additionally, a significant association was found: participants who believed these experiences were a result of fatigue or burnout of professionals themselves reported higher levels of fear, anxiety, guilt, and distress when encountering ELEs. These results highlight the importance of fostering open discussions about ELEs in palliative care, as increased awareness and education could mitigate distress and improve professional well-being (Nosek et al., 2015; Santos et al., 2017).
Our findings suggest a bidirectional relationship between spirituality and ELEs. Professionals who reported more encounters with ELEs also scored higher on the ISS, suggesting that these experiences may deepen spiritual beliefs or, conversely, that individuals with stronger spirituality may be more receptive to them. Research indicates that greater exposure to death is linked to higher spirituality/religiosity scores among healthcare professionals (de Camargos et al., 2015), supporting the idea that palliative care settings may cultivate existential reflection and spiritual growth. Additionally, 71.6% of professionals reported that ELEs positively impacted their spirituality, reinforcing their belief in a higher power and an afterlife and reducing their fear of death. This suggests that ELEs are not merely observed phenomena but may be transformative experiences that shape and strengthen professionals’ spiritual worldviews, consistent with prior research (McDonald et al., 2014).
Interestingly, despite the spiritual significance of these experiences, religious affiliation did not significantly influence the type or frequency of ELEs reported. This challenges the assumptions that ELEs are inherently linked to religious belief systems. Similar findings have been reported in other studies, suggesting that ELEs may be a universal human experience rather than a product of religious conditioning (Claxton-Oldfield et al., 2018; Fenwick et al., 2010; Santos et al., 2017).
Finally, participants noted that ELEs remain a stigmatized topic in the medical community, preventing professionals from addressing patients’ spiritual needs effectively (Brayne et al., 2006; McDonald et al., 2014). Our study also identified a strong demand for training, a need echoed in several other studies (Brayne et al., 2006; Claxton-Oldfield & Dunnett, 2016; Claxton-Oldfield & Richard, 2022; Fenwick et al., 2010; Lawrence & Repede, 2013). Research shows spiritual care training enhances clinical confidence, reduces stress, and improves patient-provider communication (Wasner et al., 2005). Implementing training programs that integrate spirituality workshops, reflection practices, and ELEs documentation could provide healthcare professionals with the tools to navigate these experiences more effectively, benefiting both patient care and professional well-being (Fenwick et al., 2010; Grant et al., 2020; Lawrence & Repede, 2013; McDonald et al., 2014).
Limitations and Future Research
This study has several limitations. The COVID-19 pandemic necessitated shifts to an online format, which may have affected participation rates. The absence of a longitudinal design made it impossible to assume some causal associations. The retest phase had lower-than-expected participation, with only nine participants completing the questionnaire at both time points, limiting full validation of the ParaPall survey. Additionally, while we examined religiosity correlations in ELEs’ perceptions, this was based solely on demographic self-reports rather than a validated religiosity scale, limiting the depth of analysis.
Furthermore, cultural stigma surrounding “paranormal phenomena” in Portugal may have influenced participation, with some professionals hesitant to engage due to fears of associating the topic with pseudoscience. Future research should explore patients’ experiences of ELEs in Portugal, enabling comparisons with international findings and a deeper understanding of cultural influences.
Despite these limitations, this study represents the first systematic investigation of ELEs among Portuguese palliative care teams, marking an important step in integrating these experiences into scientific and clinical discussions.
Conclusion
This study confirms the high prevalence of ELEs among Portuguese palliative care professionals, aligning with international findings. Professionals who reported more ELEs also had higher intrinsic spirituality scores. ELEs were widely interpreted as spiritual events, with those embracing this perspective reporting greater professional fulfillment, engagement in patient care, and positive impacts on their spirituality. Conversely, those attributing ELEs to stress, hallucinations, or fabrications experienced higher avoidance behavior and career dissatisfaction. Personal exposure to ELEs played a significant role in shaping these interpretations. These experiences remain stigmatized in medical settings. The strong demand for training found in this study suggests that structured education on ELEs could better equip professionals to navigate these experiences, improving both patient care and their well-being.
Supplemental Material
Supplemental Material - Study of End-of-Life Paranormal Phenomena Recognized by Palliative Care Health Professionals in Portugal
Supplemental Material for Study of End-of-Life Paranormal Phenomena Recognized by Palliative Care Health Professionals in Portugal by Úrsula Dalcolmo, Manuela Bertão, Luísa Castro, and Francisca Rego in Journal of Death and Dying.
Footnotes
Acknowledgment
We sincerely thank all healthcare professionals who participated in this research and the BIAL Foundation for their funding and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação Bial (358/20).
Ethical Statement
Data Availability Statement
All data generated or analyzed during this study are included in this published article (and its supplemental information files).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.