
Abstract
The suicide or homicide of a close person leaves children dependent on their carer for positive trauma processing. As these situations exist outside everyday parenting skills, this study aimed to better understand carers’ experiences and needs. Ten semi-structured interviews were conducted with carers of children bereaved by suicide or homicide and analysed using reflexive thematic analysis. Four themes concerning the carers’ wishes and support needs relating to their children were generated: A stabilising force, which discusses how the carers themselves need someone “bigger and stronger”, Feeling secure in the knowledge of others, which explores the carers appreciation for someone knowledgeable to guide and enable them, Someone in the same boat, elaborating on the role of self-help; and Easily accessible support, highlighting demands on support offers if they are to be effective. The testimonies of the carers provide important insights for the future development of effective support services for adults and children.
A person dies through suicide every 40 s worldwide (World Health Organization, 2014), and every 5 min, four people die because of homicide (United Nations Office on Drugs and Crime, 2019). As each of these occurrences are estimated to leave at least five close relatives bereaved (Berman, 2011; Rynearson & Salloum, 2021), hundreds of children and adolescents are affected by the violent death of a close person through suicide or homicide every day. As dramatic and highly stressful life events violent deaths complexly influence various areas of the lives of the bereaved (Rynearson, 2006). In particular, children and adolescents affected by suicide and homicide face grave consequences for their health and mental well-being, being at a significantly higher risk than their peers of dying through suicide themselves (Alisic et al., 2015; Guldin et al., 2015; Lysell et al., 2016; Ratnarajah & Schofield, 2007).
Children and adolescents who experience potentially traumatic life events, such as the violent death of someone close to them, depend on their carers 1 to stabilise and orientate them to facilitate positive trauma processing (Finkeldei et al., 2022; Powell et al., 2015). As these occurrences exist outside everyday human experiences and exceed everyday parenting demands, carers find themselves in a situation in which few have a readily available set of skills and behaviours and studies have found carers to feel distinctly helpless after their child had been impacted by violence and trauma (Appleyard & Osofsky, 2003; Cummings, 2018).
It has been suggested that carers’ own insecurity or concerns, as well as the desire to protect the child and themselves are reasons behind a lack of concordance between parent and child on the child’s trauma history, the subjective report of the impact of the traumatic experience, and the presence of post-traumatic stress disorder (PTSD) symptoms in the child (Stover et al., 2010). While PTSD in adults is characterized by distinct clusters of symptoms including re-experiencing the traumatic event through intrusive thoughts, flashbacks, and nightmares; emotional numbing and avoidance of reminders associated with the trauma; and hyperarousal, characterized by heightened anxiety, irritability, and difficulty concentrating (American Psychiatric Association, 2013), it is crucial to recognize that the presentation of symptoms in children can differ significantly from that in adults (Yule, 2001), owing to differences in cognitive and emotional development. Children may struggle to articulate their traumatic experiences verbally, instead expressing their distress through behavioural changes, such as increased irritability, aggression, or withdrawal from social interactions. Younger children might exhibit re-experiencing symptoms through traumatic play, where they repetitively reenact aspects of the trauma in their play activities. Furthermore, children may demonstrate a more generalized fear response, becoming easily startled or developing anxieties related to situations or objects that resemble elements of the trauma. As carers might feel helpless and overwhelmed confronted with the child’s symptoms or a lack of subjective competence to act, they may engage in avoidance behaviour (Scheeringa et al., 2015; Stover et al., 2010), leaving the child without the necessary co-regulation and support.
Furthermore, more often than not the carers will also be affected by the violent death, which adds to their burden and does not only limit their capacities to be finely attuned with their child but also influences their parenting behaviour. Research suggests that 11% of adults exposed to suicide experience PTSD around the event (Cerel et al., 2016) and that 39% of adults exposed to homicide meet criteria for all three symptom clusters of PTSD (Zinzow et al., 2011). If parents themselves suffer from post-situative PTSD, it can be a risk factor for children’s processing of trauma (Kultalahti & Rosner, 2008) because PTSD in parents can result in lower sensitivity towards the child (Meiser-Stedman et al., 2007) and harsher communication (Murphy et al., 2016; Sloover et al., 2023). Adult coping, parenting behaviour, and child processing are also correlated with parental PTSD resulting in maladaptive and hostile parenting styles which negatively influence the child’s ability to process traumatic events (Cobham et al., 2016; Leen-Feldner et al., 2013).
Furthermore, the experience or lack of social support also influence the processing of potentially traumatising events (Bal et al., 2004; Kaufman et al., 2004; Kolaitis, 2017; Trickey et al., 2012). As people grieving losses due to suicide and homicide are known to struggle with stigmatisation and taboos in their direct and wider social circles (Hanschmidt et al., 2016; Hertz et al., 2005; Oexle et al., 2020; Peters et al., 2016; Pitman et al., 2018; Ross et al., 2021), these carers and children likely experience unfavourable social conditions. The carers may not have the necessary support and be cut-off from people they usually rely on for advice and support, while also often having the role of a facilitator in their child’s social life until the child reaches a certain age (Parke & Bhavnagri, 1989).
The carers’ role and importance in the child’s coping and processing of trauma highlight the responsibility and demands on their parenting skills and behaviours. Although parents seek help and advice concerning parenting behaviour in the context of other potentially traumatic experiences (Alisic et al., 2012; Cummings, 2018), few studies have explored the needs of persons bereaved by suicide or homicide in regards to the care of minor children in the family (Dyregrov, 2002; McMenamy et al., 2008; Provini et al., 2000). Provini et al. (2000) found families with minor children to have significantly more concerns after the suicide of a next-of-kin than those without children, whereas respondents in McMenamy et al.’s (2008) study expressed a strong need for help with supporting minor children after a suicide. Dyregrov (2002) reported that two-thirds of parents wanted more help for their children after the suicide of a sibling.
Attachment theory provides core insights into how children can be supported in their processing of highly stressful life events (Busch & Lieberman, 2007; Cooper et al., 2018; Finkeldei et al., 2022) and a child’s attachment can be a vital determinant of their response to the loss of a close person (Christie & Sandoval, 2024).
Founded by the English child psychiatrist and psychoanalyst John Bowlby in the 1950s (Bowlby, 1959), attachment theory is one of the most important theoretical perspectives in psychology and psychotherapy, integrating results from developmental psychology and psychotherapy research (von Sydow, 2008). Berman and Sperling (1994) define attachment as ‘the stable tendency of an individual to seek and maintain proximity to and contact with one or a few specific individuals who provide the subjective potential for physiological and/or psychological safety and security’ (p. 8). Attachment behaviour is activated by separation from the attachment figure and by external or internal threat, pain, and danger (von Sydow, 2002). The most important function of the attachment figure is to protect the infant or child in situations of perceived threat and to provide emotional and physical security. The attachment figure functions as a secure base from which exploration can take place and is a safe haven where comfort is given in stressful situations (von Sydow, 2002). Therefore, attachment theory postulates the fundamental influence of interaction with attachment figures on the ability of children and adolescents to learn, integrate challenging experiences, and develop. Cooper et al. (2018) state that almost all one needs to know about supporting a (child’s) experience of safety is as follows: ‘always be bigger, stronger, wiser, and kind. Whenever possible, follow the child’s needs. Whenever necessary, take the lead’. Research specific to child bereavement indicates that secure attachment relationships serve as protective factors, helping children navigate the intense emotions and existential questions that arise following violent deaths (Alvis et al., 2023; Bretherton & Munholland, 2008) and how well a child copes with grief, including their anxiety and understanding of death, is deeply affected by their relationship with their carer (Bowlby, 1969; Stroebe & Schut, 2005). Following such tragic events, children’s attachment behaviours are intensely activated precisely when many carers are themselves struggling with shock, grief, and trauma responses.
Although attachment behaviour is most pronounced in young children, it remains significant throughout life, just as the attachment system is most important in early life, but remains active across the lifespan and manifests in thoughts and behaviours related to proximity-seeking in times of need (Shaver & Mikulincer, 2009). Attachment figures in childhood are usually primary carers, and in adulthood, they are likely to be romantic partners or close friends. Shaver and Mikulincer (2009) state the following: ‘Attachment-related interactions are organised around the expectation of receiving protection, comfort, encouragement and support from the attachment figure in times of need, and this protection or support is valued because it allows a person to restore emotional balance and return to effective behavior in the wider social and physical environment’. As carers in the situations under study are likely affected by the traumatic loss themselves and might have lost their adult attachment figure, this leads to unique challenges. When suicide or homicide affects a family, it may result in dual activation of attachment needs with carers having to manage their own attachment-related emotions while simultaneously addressing the intensified attachment needs of bereaved children.
Another reason why attachment is relevant to both sides of the carer–child dyad is that ‘attachment is, in fact, a key to working with people in a crisis’ (Leenaars & Wenckstern, 1998, citing Hoff, p. 367). The carers’ accounts can offer valuable background and information on their wishes and needs, which can guide future policies and support offers.
This study aimed to understand carers’ experiences when faced with the suicide or homicide of a person close to their child and to gain insight into their own coping and ability to meet the needs of the children in this challenging situation, guided by insights of attachment theory. The research question is “What are the support needs and wishes of carers of children bereaved by suicide or homicide, specifically regarding guidance and orientation in their parenting role following the violent death?”
Methodology
This was a qualitative study with 14 participants. Semi-structured Problem Centred Interviews (Witzel & Reiter, 2012) were conducted between 17th August and 8th December, 2022. All interviews were conducted in German. Ten of the collected interviews met the inclusion criteria and were included in the data analysis. The four excluded interviews were determined during the interview process to not meet the inclusion criteria (e.g. drug overdose interpreted as suicide, child having just turned 18 at the time of the violent death).
Sample
Participants were recruited via an online survey, which was part of a larger research project on the experiences of cares of children who had experienced the violent death of a close person (doi.org/10.17605/OSF.IO/3P9SW), as well as through the AETAS Children’s Foundation Web site [a non-governmental organisation providing services to children, adolescents, and carers after highly stressful life events (https://www.aetas-kinderstiftung.de/)], various multipliers, and word-of-mouth. Recruitment took place between July and December 2022.
Participants were invited into the study if they were carers to children aged 0–17 years at the time of a violent death (suicide or homicide) of a close person. There were no restrictions as to how long ago the death had occurred.
As the interview guide in problem-centred interviews is ideally a topical guide rather than a list of fixed and rigid questions (Witzel, 2000), the guideline development was informed by key questions relevant to the research project. These were mainly based on the professional experience of the research team, who have been working with families affected by violent deaths for more than 15 years. The interview topic guide comprised questions about the family system, the violent death, interaction and communication between carer and child, help or support, and additional burdens. Open questions were asked at the beginning and at the end of the interview to invite a free account of carers’ experiences.
Ethical Considerations and Informed Consent
Given the sensitive nature of the research (Campbell, 2002; Liamputtong, 2007; Renzetti & Lee, 1993; Robertson, 2000) and the potential of the interview process to be emotionally stressful and triggering for participants, the interviews were conducted exclusively by the first author, who is a qualified trauma counsellor registered with the German-speaking Society for Psychotraumatology (Deutschsprachige Gesellschaft für Psychotraumatologie). All data were collected in person or via Zoom, as it was deemed crucial for the researcher to see all clues relating to the interviewees state (including visual cues regarding body language, facial expressions, and gestures) to gauge potential discomfort or distress.
Participants were asked for their written informed consent, and were told that they could withdraw their participation at any time. All participants chose a pseudonym, which was changed again for added security by the primary researcher. Support from the AETAS Children’s Foundation was available to participants at any time as well as referral to other psychosocial or trauma-specific counselling and care services. Participants were not offered any remuneration for their participation.
This study received ethical approval from the Technical University Munich on the 22th of June 2022 (reference number: 2022-252-S-NP) and the study was registered on the Open Science Framework (doi.org/10.17605/OSF.IO/3P9SW).
Data Analysis
All interviews were transcribed using a transcription service, and the transcripts checked for accuracy by the primary investigator.
Data were analysed using an inductive reflexive thematic analysis (RTA; Braun & Clarke, 2013, 2022) approach. The six steps of RTA were followed in an iterative process with initial familiarisation, coding, and analysis conducted in German and further coding, analysis, and writing of the report in English. This was done by the primary investigator, who had qualitative research and RTA experience.
Data extracts to evidence the analytic claims were chosen from all datasets. Unnecessary details were deleted from the extracts to allow easier access to the meaning (Braun & Clarke, 2022). Data extracts from the transcripts were checked against the audio recordings to ensure the true meaning was captured.
As is the preferable way for presenting results and their discussion in RTA, this paper presents the analysis followed by conclusions (Braun & Clarke, 2024).
Reflexivity
According to Johnson et al. (2020, p. 145) ‘Rigor is best achieved through thoughtful and deliberate planning, diligent and ongoing application of researcher reflexivity, and honest communication between the researcher and the audience regarding the study and its results’. We will briefly elaborate on the aspect of reflexivity, as a vital part of both rigour in qualitative research and RTA (Braun & Clarke, 2022).
It is important to recognise the researchers’ perspective, as it shaped the study design, including the interview guide, and the interpretation of findings. The AETAS Children’s Foundation is firmly grounded in attachment and family systems theories. The primary investigator, who is also first author, is a health scientist experienced in working with marginalised communities and also a certified psycho-trauma counsellor. The second and last authors are therapists at the AETAS Children’s Foundation, the third author is a social epidemiology professor of at the Ludwig Maximilian University Munich. While approaching the research project from a health science standpoint, the researchers’ understanding of psycho-traumatology informed their work. This was beneficial as it provided a trauma-sensitive perspective to the development of the study protocol, interview guide, and the process of dataset generation. Although none of the participants had any prior relationship with the primary investigator beyond her role as a researcher, the trauma-informed approach offered a protective element for participants during the interviews.
Analysis
Participants’ Information.
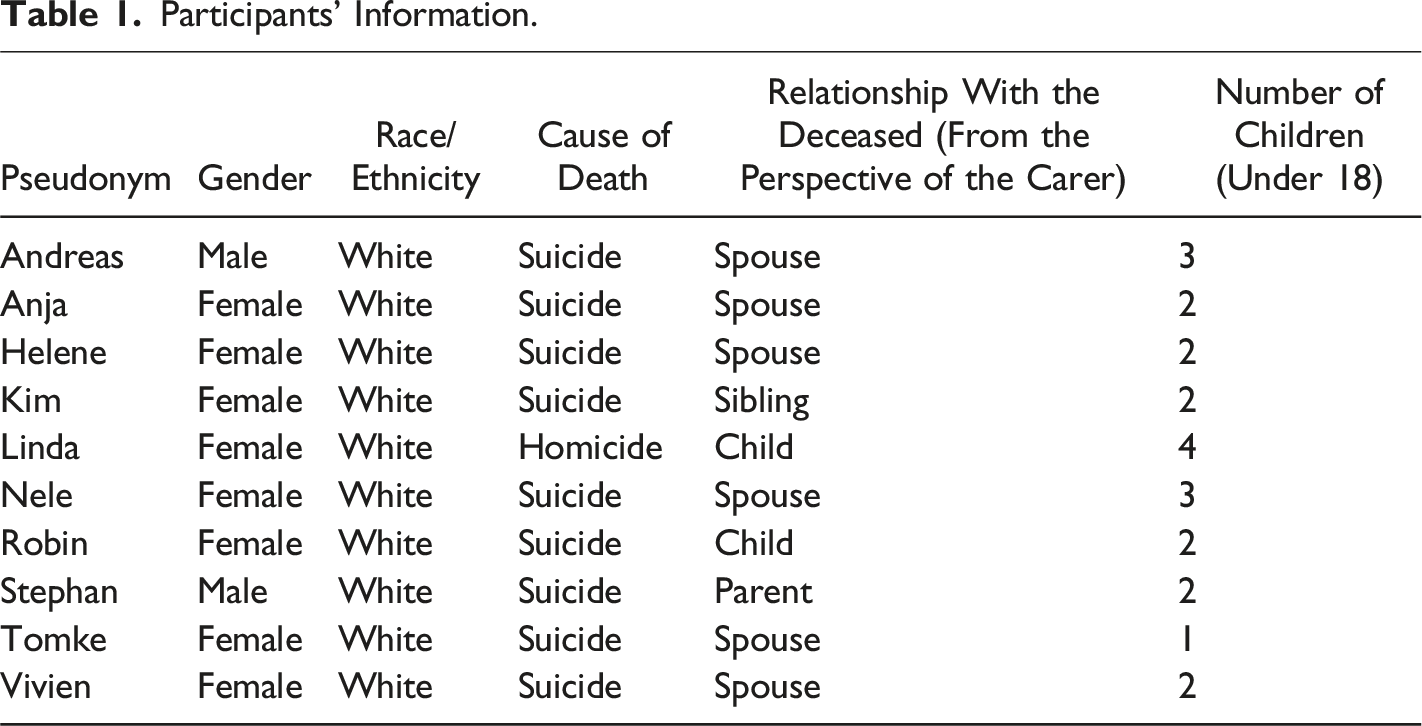
The situations and experiences that the participants described were heterogeneous and complex. The analysis and report within the scope of this paper will focus on the guidance and orientation concerning their children and parenting that the interviewees wished they had had.
The carers’ wish for someone to act as a strong and competent guide for them was evident in essentially all the interviews, as illustrated by Linda’s words: ‘I just need help. I just need someone to tell me what to do now, because this is new territory. I’ve never done anything like this before’. This is key from an attachment theory perspective, as the attachment system of adults becomes activated when they are subjected to conscious or unconscious threats as would be the case after a highly stressful life event, just as for infants and children (Shaver & Mikulincer, 2009). This results in orientation towards and seeking the proximity of an attachment figure or someone ‘temporarily equivalent stronger, wiser, and supportive’ (Shaver & Mikulincer, 2009, S. 26). Some participants claimed that it was only through the guidance and support of others that they were able to have difficult conversations with their children about the violent death, making these stabilising and orienting effects highly relevant or even essential to the enabling of carers (Rinne-Wolf et al., 2024).
Four themes relating to the guidance and support that carers wanted were generated from the data: A stabilising force, Feeling secure in the knowledge of others, Someone in the same boat and Easily accessible support.
A Stabilising Force
To have someone perceived as bigger and stronger to lean and rely on appeared to be very valuable for several participants, who described different facets to this. For example, interviewee Tomke described reverting back to a formerly outdated stage in the relationship to their parents, saying, ‘It was really helpful that I had my parents next door because I really regressed to being a child a bit’. This was particularly interesting as it highlighted something akin to a conflict of roles. Being able to leave the role of carer and revert back to that of a child who is taken care of and protected by someone, who, during childhood, had been cast in the role of someone bigger and stronger (Powell et al., 2013), was considered helpful. Although this kind of regression is not unusual (Lokko & Stern, 2015), what is significant is that in this scenario, leaving the role of carer had a direct influence on the carer’s own child currently who was also in need of orientation and guidance. A different aspect of this could also be that the carer could orient and stabilise the child by having their own attachment needs met and experiencing a sense of security themselves. Robin expressed this in their interview: ‘And to be stabilised again and again in such a way that you can also act in a stable manner towards the children—that was the most important thing for me, actually’. Here, the sense of their own vulnerability and need for support became a strength in that it is clear to Robin that ‘a helpless helper is of no help to anyone’. Playing the role of the functioning and strong carer required the carer to be stabilised themselves by someone who, in turn, was strong, knowledgeable, and kind enough to fulfil this role.
Feeling Secure in the Knowledge of Others
Aspects around wanting and needing someone perceived as wiser in this situation were also mentioned frequently as some of the most helpful factors: That was really one of the most important things, to get this support, especially at the beginning. Because I wouldn’t have known how to do it. And just as I was super grateful for the midwives at the birth of the children, I was super grateful that there was someone who also knows how to deal with the end of life, especially in such a dramatic situation, how to say goodbye and how to die and how to do it well—as far as that is possible. (Robin)
Interestingly this analogy of someone like a midwife offering knowledge and support at a time of great and fundamental changes in life was used several times by participants, especially those who had lost children to suicide or homicide. From an attachment perspective, parents regard midwives as persons who fulfil the need for emotional security and reassurance as they step into the role of an attachment figure for a limited but significant time (Brisch, 2007). In Robin’s account, the death of a close person was portrayed as something akin to a birth, in that both are moments of passage that frame life and benefit from a guide who is familiar with these moments that are out of the ordinary. The wish to experience and deal with these life altering situations seems to lead to the need for an expert and guide, someone bigger and wiser. She had so much know-how, knew exactly how I was feeling. (...) And she always anticipated so much from her experience, like which questions the children would ask after [I had given them some] explanations. So, she was always already three steps ahead. Exactly—I am here trying to orientate myself, and she always knew exactly which way to go. (Nele)
Nele emphasised how her helper’s expertise in the area of Psychosocial Systemic Emergency Care (Kern & Finkeldei, 2021) enabled them to know how Nele felt. This implies, that carers show an almost predictable range of emotions after the suicide or homicide of a close person. To be understood and to have someone regard those reactions and emotions after potentially traumatic experiences as ‘normal reactions to abnormal events’ (Juen & Werth, 2004) can be a greatly comforting, orienting, and stabilising.
Nele also pointed out the role of a guide her helper took on for her, who not only saw where Nele was at any one particular time, but was also able to predict the next steps along the way, and who obviously knew the terrain and a path through it. This person appeared almost wondrous to Nele. At another point in the interview, Nele further elaborated on this aspect: And it was really—well—she could always look into the future. So much experience, so much know-how. So, at some point I was able to sit back a little bit because I knew that the plan would work. And I am prepared even for questions that come up later on. So, I really felt all round bolstered about everything concerning the children and delivering the news. (Nele)
By elaborating on the outcome of her feeling so well guided, she draws attention to how it enabled her to face her children’s questions and feel competent as their orienting beacon. Those feelings of safety and security which Nele gained from being equipped for anything the children might ‘throw at her’ is also observed in other carers’ accounts.
A sense of burden which the carers carried regarding the unusual, difficult, and challenging tasks (including evaluating what is right or wrong to say to the child and making parenting decisions at a time when the child’s behaviour may not be how it usually is) was evident in nearly all the interviews. Some of the carers expressed that not having to carry this burden alone and having someone to relieve them of some of the difficult decisions was very valuable and helpful: It really freed me from the burden of having to decide everything on my own and having to know what is appropriate or right or… Yes, simply being supported and simply being given so many practical suggestions and ideas. That helped me the most. (Robin)
For Robin, not being alone in making decisions and being capable of action seemed to be the main points, whereas for others, being offered explanations so that they could explain things to their child took priority: How do I explain to my son that his godfather took his own life? What can I use as an explanation if I haven’t been given any kind of explanation myself? I have no, no letter, no signs, no reasons that make sense to me. (...) That made it particularly difficult for me—that I couldn’t explain to [my son], ‘he had cancer and was terminally ill’ or . . . I think, at some point I would have blocked those conversations if I hadn’t gotten help from [aid organisation]. That was important and helpful for me. (Kim)
Their despair about and burden of not knowing and understanding the reasons behind their brother’s suicide was evident in Kim’s interview. It is known that family members struggle more with questions surrounding meaning making after suicide than those after other causes of death (Jordan, 2001), often leading to complicated grief reactions. The perceived voluntary nature of the death is particularly stressful and has an impact not only on how the survivors view the dead person but also themselves and their whole world (Castelli Dransart, 2013). These unsettling and destabilising factors impinge on the carers’ ability to navigate conversations with the child about the death. Having no models of explanation or understanding of the genesis of suicidality themselves, Kim felt unable to answer their child’s questions. Being supplied with a possible explanation model and the words to convey it was portrayed as the reason behind Kim feeling they did not have to disengage from conversations with their child. A sense of gratitude at not being left alone in these situations and the burden being eased was present in all of the accounts of carers who received help.
Someone in the Same Boat
The interviewees also talked about the importance of self-help organisations and peer support that made them feel understood and supported. Helene expressed the following: ‘Well, I think those affected, who have experienced the same thing, are the greatest help themselves because you get the feeling that you are understood’.
The implied notion that those who have not experienced similar events are unable to fully comprehend the situation was mentioned by some of the participants. This seemed to pose an obstacle to what was perceived as helpful. The act of understanding and being understood in itself was portrayed as helpful beyond everything else. An additional aspect for the carers appeared to be that of being accepted with their stories: Because you are affected by something so particular, and just happy when you can talk to someone about something that is so horrible for others that they don’t want to come near it. And that it is actually a matter of course and easy, and I enjoy that in a certain way, that you can just talk about it. (Robin)
As many carers described the taboos surrounding the death and stigmatising behaviour of people in their direct and wider social circles, being able to talk openly about the death and have conversations without fear of judgement was appreciated. This feeling of self-help group members being there for each other and helping during similar experiences, together with a sense of being on the same side, is known from research on self-help and peer-support in other contexts (Hertz et al., 2012; Jordan, 2019). The resulting sense of empathy, sensitivity, and warmth (Hertz et al., 2012), all of which are ideal characteristics of attachment figures (Papoušek & Papoušek, 2002), and regarding self-help groups as secure bases and safe havens (Jordan, 2019), appeared to be the same in the context of peer-support after suicide and homicide.
Orientation through people with similar experiences also seemed to be very helpful to carers, as illustrated by Vivian: ‘To meet people, people who have experienced the same thing, to see—and I still remember this literally—to see: how crazy am I? Is this still normal in this context?’. Gauging whether their own behaviour or that of the children was ‘normal’ against the experiences and narratives of others in the same or similar situations was described in several accounts. Similar mechanisms as described in the previous theme seemed to be at play here. The relief of learning that the normal reaction to an abnormal event was indeed normal, and having others with similar experiences put these experiences into context appeared to be similar. The role of guides in these cases was fulfilled by others in the same situation sharing their experiential knowledge, rather than by external experts. Consequently, the carers expressed no surprise at the knowledge and expertise of the people functioning as guides, as the shared experience automatically made them experts.
Easily Accessible Support
Although the participants appreciated the help, support, and guidance they were afforded by different people and institutions, several of them wished for these stabilising and orienting offers to have been made available to them earlier: And I would have liked it if the lady or the gentleman from the KIT [crisis intervention team] had said: ‘Look, there is a foundation that explicitly cares for children who have either experienced a violent crime or violence, or where a family member has died’. Then perhaps the time between the death and this first contact with the [Psychosocial Systemic Emergency Care professional] would have been shorter, and then maybe I would have felt safer. (Anja)
Like Anja, several participants expressed that the professionals who were involved in delivering the news of death to them (e.g. police, first responders, and psychosocial emergency care professionals) would have been ideally placed to inform them about availability of support for themselves and their children. This need for signposting has also been found in previous research on parents’ needs after a suicide in the family (Wainwright et al., 2020), though not necessarily related to the care of children. Even if carers believed they might not have been capable of taking in information to the full extent at that time, some carers felt that written information to refer back to later would have been helpful. The increased sense of security in dealing with their children from the moment the carers had knowledgeable support by their sides and a sense of regret about not having had this earlier was expressed in Anja’s words and echoed in some of the other participants’ interviews as well: [To know in advance that I could have support] would probably have been helpful for me, because then I might have had some sense of security earlier. However, as acutely affected as I was, I was unable to strategically pursue this. So, that would have been something that would have helped me: to get into touch earlier. (Kim)
An important point that Kim made, which was echoed in other participants’ stories, was that the active search for help and support exceeded what carers felt capable of at the time immediately following the death. It is known that the necessary physical and psychological energy required for seeking help is not available immediately after being affected by suicide (Dyregrov, 2002; Provini et al., 2000). Many of the participants reported that others (siblings, friends etc.) found out about support offers for them, as they did not have the strength and capacity to do so themselves, whereas others remained without help for a significant length of time until they were able to find support themselves. This lack of help caused by depression or inaccessible information has also been described by McMenamy et al. (2008). From a psycho-traumatological perspective, this is highly relevant, as early and specific interventions after potentially traumatic events are regarded as best practice and essential for trauma processing (Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften, 2019). Carers can be assumed to act as gatekeepers to help and support their minor children, leaving both parties without help when the carer is unable to seek help.
Another point illustrated by the participants was that several support and help offers were not low-threshold as they could not be accessed without major hurdles or requirements (Konter, 2019). These thresholds existed on various dimensions ranging from spatial (e.g. accessibility, location), monetary (costs and fees), life situation-oriented (e.g. single parenthood), and psychological (e.g. fear, shame, excessive demands) thresholds, from the perspective of the person affected or seeking help (Konter, 2019). The hurdles described by the participants sometimes lay in spatial aspects (difficult accessibility owing to their place of residence), but were far more often founded in life situation-oriented and psychological thresholds. The wish to be informed by the professionals present at the reception of the news of death can be understood as the wish for low-threshold access to services. From the carers’ highly burdened situation, it was clear that any offer needed to be easily accessible and oriented towards their individual life situations, as outlined as ‘early and outreach assistance’ by Dyregrov (2011).
Limitations
Although this study offers valuable insight into a hitherto understudied population, several limitations need to be acknowledged. One of the most significant limitations is that all participants identified as white cisgender individuals, which leaves other sections of society not represented. Most participants had sought advice or counselling following their loss, suggesting they may possess greater emotional literacy than the broader population of caregivers dealing with similar issues.
Another limitation is that nearly all participants were recruited through an online survey which was part of a wider research project, which lead to a certain selection bias pertaining to the online ‘survey. Research indicates that individuals with higher educational qualifications are often overrepresented in online surveys (Blasius & Brandt, 2009), and this trend was reflected in our participant sample: over half (69.4%) of the participants had a university degree, while individuals without a degree or with only a lower secondary school certificate were absent from this group. This overrepresentation of highly educated individuals was also apparent in the interview sample, which needs to be acknowledged when considering implications from the carers’ accounts.
Additionally, six out of ten were recruited through direct outreach by the AETAS Children’s Foundation, meaning they either received support from the organisation (four cases) or were at least offered assistance (two cases), even if they refused it. This connection may have influenced their responses, as some participants might have felt compelled to express gratitude or highlight the benefits of the foundation’s support. Nevertheless, the remaining four participants were sourced through multipliers and had no prior contact with AETAS Children’s Foundation.
Lastly, it is important to recognise that experiences during and after potentially traumatic events could impact recall accuracy, leading to possible recall bias (Van Der Kolk et al., 1997).
Implications
The qualitative study of carers supporting children bereaved by suicide or homicide reveals the profound challenges faced by these families and the complex support needs that arise. The findings underscore that effective intervention must address both carers’ and children’s needs simultaneously, recognizing their interdependence and the relational nature of trauma processing. The attachment framework also illuminates why the violent death of a close person creates such profound disruption. When the deceased person was an attachment figure for the child, the loss represents not just grief but the destruction of a central security structure. Similarly, if the deceased was an attachment figure for the carer (such as a spouse), the carer must manage their own attachment disruption while simultaneously providing enhanced attachment security for the child—a tremendously challenging task. The principle that attachment figures should be bigger, stronger, wiser, and kind (Cooper et al., 2018) offers a foundational framework for supporting both carers and children. This principle suggests that effective support requires both compassion and competence—helpers must demonstrate both emotional attunement and practical expertise. When carers receive the stability, knowledge, connection, and accessible support they need, they become better equipped to serve as secure bases and safe haven for affected children. This creates a foundation from which children can process their grief and trauma while maintaining developmental progress.
Based on the findings and broader research, there is a clear need for trauma-informed support systems specifically designed for carers of children bereaved by suicide or homicide. These systems should integrate three critical components: psychological support for the carer’s own trauma and grief, education about children’s trauma responses and needs, and practical guidance for navigating specific challenges. Interventions should be designed with attachment principles at their core, recognizing that carers need both emotional containment and practical direction. Importantly, these support systems must be proactively offered rather than requiring carers to seek them out.
The findings regarding carers’ knowledge gaps suggest a critical need for accessible, evidence-based educational resources about supporting children through bereavement by violent deaths including psycho-educational as well as practical information relating to parenting and concerns around children. These resources should address common questions about age-appropriate communication, normal trauma reactions, and effective support strategies. Key topics to address include: how to talk with children about suicide and homicide in age-appropriate ways; recognizing trauma symptoms versus normal grief responses; managing practical challenges like school reentry; and helping children maintain healthy connections to the deceased person while processing the traumatic nature of the death. These educational resources should also be readily available at key points of contact, including hospitals, schools, funeral homes, and victim services. An example for these kinds of educational and supportive resources are the “Kurswechsel” materials provided by the AETAS Children’s Foundation (https://www.aetas-kinderstiftung.de/kurswechsel-projekt/).
The findings regarding the complementary values of professional guidance and peer support suggest an opportunity for integrated models that combine these approaches. Rather than viewing professional and peer support as separate pathways, services could be designed to deliberately integrate both elements. Models might include professionally facilitated peer support groups, where clinicians with trauma expertise provide structure and education while encouraging peer connection and validation. The AETAS Children’s Foundation represents one organization implementing elements of this approach. Expanding and replicating such models, with careful evaluation of outcomes, could help address the complex needs identified in the research.
The findings regarding accessibility barriers highlight the need for comprehensive service redesign focused on eliminating obstacles to support. The timeliness of offers of help and support is of particular relevance, as many participants described not having been aware of offers in the time immediately after the death. This can lead to a vital period of time during which interventions for both carers and children pass without help, and carers lack security and orientation. Carers voiced their wish for professionals, such as emergency response professionals or the police, to inform them about available support after such highly stressful experiences. The implementation of automatic referral systems through first responders, schools, or victim services could help overcome the barrier of having to seek help during a period of overwhelming distress. Therefore, coordination between systems that interact with bereaved families is essential. Schools, healthcare providers, law enforcement, and mental health services should have established protocols for communication and referral to ensure families receive comprehensive support without having to navigate complex systems independently. The necessity for services to see the whole family system, rather than only individuals, is highlighted by the findings of this study.
Services for carers of children bereaved by suicide or homicide should incorporate principles of trauma-informed care, including transparency, trustworthiness, and choice. Furthermore, the research suggests support is needed both immediately after the death (crisis response) and over the long term (ongoing guidance). Service systems should be designed to accommodate both acute and long term needs, with smooth transitions between levels of care. Additionally, information material in the form of leaflets or flyers for later reference could be supplied.
Finally, the challenges faced by carers of children bereaved by suicide or homicide extend beyond individual family units to broader societal and policy contexts. The stigma surrounding violent death, particularly suicide, creates barriers to support that cannot be addressed through clinical interventions alone. Public education campaigns aimed at reducing stigma and promoting understanding for families affected by violent deaths could create more supportive communities for these families.
The recommendations outlined here seek to translate these insights into practical approaches that address current gaps in service provision. By developing trauma-informed support systems, comprehensive educational resources, integrated professional-peer networks, and accessible service models, we can better respond to the needs of these vulnerable families. Ultimately, supporting carers of children bereaved by suicide or homicide requires a coordinated, compassionate response that recognizes both the universal aspects of traumatic grief and the unique challenges posed by violent deaths. Through such approaches, we can help transform devastating loss into a painful but manageable life experience that does not define a child’s future.
This study appears to be one of the first to focus on the support needs of people bereaved by suicide or homicide in their role as carers to minors. It offers valuable insights into the help and support offer requirements and structures that need to be implemented to reach this highly vulnerable population. Further research is required to extend the limited knowledge in this field. Longitudinal studies tracking outcomes for children bereaved by suicide or homicide would provide valuable insights into the long-term impacts and effectiveness of various support approaches. These studies should measure not only symptom reduction but also positive indicators of resilience and post-traumatic growth. Furthermore, implementation science approaches are needed to understand how to effectively translate research findings into accessible services across diverse contexts. This includes studying barriers to service utilization and strategies for increasing engagement among hard-to-reach populations. To complement insights into these highly relevant topics and to add to them from a child rights’ perspective it would also be highly desirable to hear the children’s own voices on these issues.
Footnotes
Acknowledgments
The authors wish to convey their heartfelt appreciation and respect to the carers who took part in this study. Their experiences, courage, and resilience have profoundly inspired and moved us. It is our sincere hope that this publication honours their contributions and helps individuals facing similar circumstances in the future.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted within the framework of the project “Kurswechsel” of the AETAS Children’s Foundation. While the Bavarian State Ministry for Family, Labour and Social Affairs funded project “Kurswechsel” it did not influence the research, analysis or findings.
Ethical Statement
Data Availability Statement
The datasets generated during and analysed during the current study are not publicly available due to the sensitive nature of the qualitative data and restricted consent from participants.
Note
Author Biographies
![]() ) was established in Munich to secure the programme’s continuity, with Ms Kern serving as Clinical Director. As a lecturer, she teaches and publishes on her specialist subjects of emergency psychology, trauma therapy, and the consequences of complex trauma in childhood and adolescence.
) was established in Munich to secure the programme’s continuity, with Ms Kern serving as Clinical Director. As a lecturer, she teaches and publishes on her specialist subjects of emergency psychology, trauma therapy, and the consequences of complex trauma in childhood and adolescence.