
Abstract
Grief is a normal reaction to loss, but some bereaved people require structured support to adjust. This paper reports findings from phase one of a study to develop a statewide model for grief and bereavement support and assess the associated costs and benefits. A desktop review and online survey mapped existing supports and identified gaps in support. Semi-structured interviews provided further insight into areas of unmet need. Results showed existing grief supports for the general population, for targeted community bereavement care, and for specialised professional care, but a lack of integration between supports, challenges in identification and navigation of supports, and a gap in supports for diverse and rural populations. Supports to develop a grief-literate general population, and grief training for professionals were also needed. Identified gaps highlight preliminary key areas to be addressed in the selection or development of a model for statewide grief and bereavement support.
Background
Grief is the subjective experience associated with loss, especially through death, although it can occur after any type of loss or separation (Hopf et al., 2020). It is a normal reaction to that loss and involves individualised emotional, psychological, social and spiritual reactions (Stroebe et al., 2007). Bereavement is a broader term that covers everything that people go through relating to a loss that causes grief (Hopf et al., 2020). In the case of death, bereavement can include the period leading up to the death, the death itself, and the process of adjustment to life afterward (Blackburn & Dwyer, 2017). Bereavement is understood to be a current public health priority on a global level due to higher mortality rates and the public health toll from a host of grief-associated adverse outcomes (Lichtenthal et al., 2024). The literature calls for multi-level national strategies and models to help manage grief and bereavement at a population level (Lichtenthal et al., 2024).
When people grieve, they are coming to terms with, or reorienting themselves to, what has changed in their lives. They are beginning to find new ways of going about their lives to cope with the gaps that the loss has created (Stroebe & Schut, 2010). Adjusting to a life without the person who has died makes heavy demands on each person and the people around them, and human support is a major factor in navigating through grief. This can be support from families and close friends, or the broader community – workplaces, schools, faith-based institutions and every other facet of community (Abel et al., 2023). Although many people cope with their grief with these informal supports, for others, the profound impact of their grief requires more structured support to help rebuild their life (Aoun et al., 2012).
Complicated grief is a condition that emerges when the natural grief process is disturbed or prolonged, that is, when a pervasive and disabling grief response lasts beyond the expected adaptive period (Champion & Kilcullen, 2023). Complicated grief is a major health concern for some bereaved individuals, strongly linked with increased morbidity and mortality (Champion & Kilcullen, 2023). The three-tiered Public Health Model for Bereavement Support highlights three levels of risk for bereaved people, and three associated levels of support they may need. The model predicts that 60% of the population are at low risk of complications of their grief, 30% at moderate risk, and 10% at high risk (Aoun et al., 2012). This model suggests that most people at low risk can manage their grief with the support of family and friends and other informal community supports (Tier 1). Those with moderate risk may need some more targeted additional supports such as attending a bereavement support group (Tier 2). Those at high risk of complex grief issues may need specialist grief support from mental health professionals (Tier 3) (Aoun et al., 2015). There is contention around the benefits of diagnosing complicated grief and evidence that some bereaved population groups are more likely to meet the criteria, with factors such as cause of death and relationship to the deceased playing a major role (Thieleman et al., 2023). This suggests that bereavement support may be better targeted to subgroups to meet unique bereavement needs rather than levels of risk; however, the three-tier model was utilised in this project because it illustrates how different combinations of strategies are needed to meet the needs of all bereaved people and emphasises the use of informal supports located within local communities as the backbone of bereavement care at a population level.
Across Australia, grief and bereavement have been identified as persistent areas of unmet need within the health system (Australian Government Department of Health and Aged Care, 2018, Government of South Australia, 2021). Although the scope of grief within a population is difficult to calculate, some literature has estimated four to ten bereaved people per death (Thompson et al., 2017). Within this, an estimated 5%–10% of bereaved individuals are at risk of developing complicated grief (Thompson et al., 2017). In South Australia, grief has been raised as a concern for many carers and family members in the palliative care system, and causes significant costs, particularly relating to mental health, productivity and community capacity (Government of South Australia, 2019). Despite this, a report from Palliative Care Australia & KPMG (2020) highlighted the scarcity of evidence about the effects of bereavement in Australia, including a lack of quantification of the costs of bereavement, although some international evidence demonstrates significant costs of bereavement related to higher rates of medication use and hospitalisation (Stroebe et al., 2007), and supports the use of regular specialist and counselling intervention to minimise bereaved peoples’ health care service utilisation (Onrust et al., 2008).
Given the limited evidence around the costs of grief and bereavement support in the literature, and the identified importance of such support for the Australian population, a study was conducted to assess the potential costs and benefits of establishing a statewide model for grief and bereavement in South Australia. This paper reports on the findings from the first phase of this larger study. Phase 1 involved mapping the existing grief and bereavement supports in South Australia to identify broad areas of unmet need.
Methods
The project scope was limited to grief and bereavement relating to the death of a person.
Phase 1 was an environmental scan, consisting of a desktop review and an online survey. The results of the scan were validated through semi-structured interviews to triangulate data collection and analysis processes. Phase 1 had the following objectives: (1) Summarise what currently exists for grief and bereavement support in South Australia. (2) Identify areas of unmet need. (3) Validate mapping of existing supports and unmet needs with stakeholders. (4) Initiate stakeholder discussion around priorities and ideas to meet unmet needs.
Desktop Review
A desktop search to find current grief supports available to South Australians was conducted broadly using the Google search engine in addition to specific searches of 53 Australian health and bereavement service websites. Each Google search was limited to the region of Australia and verbatim search results, with search customisation turned off. Searches combined the concepts of ‘South Australia’ or ‘Adelaide’, ‘support’, ‘service’, or ‘event’ and ‘grief’ or ‘bereavement’. All pages of results were included until a page was reached with no new relevant results. Every potentially relevant link (assessed by title and description on the search engine results page) was opened and each Web site searched for information about grief and bereavement supports. Links within websites to additional websites were followed and the same process completed until no new results were found. Targeted organisational websites were searched individually using the keywords ‘grief’ or ‘bereavement’. Any grief or bereavement supports found that had not been captured in the Google searches were extracted.
All unique results were recorded in a custom Excel spreadsheet set up with dropdown options and free text capabilities. Data items extracted included: type of support (e.g. event, program, information), service provider (organisation), location (local government area), types of grief/death (e.g. suicide), target population/s, types of support provided (format, delivery methods, group/individual, duration/frequency), support provider (profession), costs to access, URL. Data was extracted per support, i.e., if a single organisation offered multiple types of support or programs, each was counted separately to provide a comprehensive list of types of support available to South Australians. National grief and bereavement supports that were found through this search strategy were also extracted and included as supports accessible to South Australians.
Online Survey
The CEOs of 11 key health and community organisations were contacted via email and invited to participate in the project and share the online survey link with their employees and volunteers. Beyond this initial contact, snowball sampling methods were used to identify further key stakeholders. Survey respondents provided digital consent to participation prior to completing the survey and their data was anonymised prior to analysis. The survey included six qualitative questions around the grief and bereavement supports respondents provided, other community and health system-based supports they were aware of in SA, what supports they thought would help people better navigate their own grief or help someone else through grief, and what supports they felt were missing or needed in the SA community. Any additional supports identified through the survey were searched for on Google and the data added to the desktop review extraction spreadsheet.
Data Analysis and Synthesis
The combined desktop review and online survey data were analysed both quantitatively and qualitatively. Existing types of support and their features (e.g., locations, delivery modes, costs) were analysed by frequency using Excel. Each support was recorded against all relevant categories (i.e., may be counted multiple times). Qualitative data from the surveys were exported to NVivo 14 software for thematic analysis. The results of the environmental scan were synthesised according to the three tiers of the framework of the Public Health Model of Bereavement (Aoun et al., 2015).
Semi-structured Interviews
Participants for interviews were recruited through snowballing methods whereby those who were invited and/or participated in the online survey were also invited to participate in an interview. Some additional invitations were extended to targeted people/groups that were recommended and approved by the funding bodies. Participants were sent a consent form and study information sheet prior to their interview and provided written or verbal consent. A semi-structured interview guide focused on: (i) stakeholders’ goals for a statewide grief and bereavement care model; (ii) stakeholder feedback regarding the environmental scan findings; and (iii) stakeholders’ thoughts on the ways that the existing model could be modified to address identified unmet needs.
Interviews were auto transcribed (with permission) and transcripts were cleaned and edited manually by the interviewer. The cleaned transcripts were sent back to interviewees for member checking. Only those interview transcripts returned by interviewees and validated as accurately representing their perspectives were included in the analysis. All personal and identifiable information was removed, and a pseudonym (numerical ID) was assigned to each participant. Interview transcripts were uploaded to NVIVO 14 for analysis. Any data from the interviews around specific existing grief and bereavement support services or providers in South Australia were added to the environmental scan data for triangulation purposes. Each transcript was first read repeatedly, and data were deductively assigned to a priori codes/organisational categories. Following this, subcategories and overall themes were inductively developed from the data.
Findings
The existing grief and bereavement supports in South Australia as found in the environmental scan are reported below, followed by a thematic summary of the areas of unmet need identified across the desktop review, survey and interviews.
Participants
The online survey was conducted over four weeks in December 2023. There were 28 survey respondents, including nurses (n = 6), management (n = 3), volunteers (n = 3), social workers (n = 2), counsellors (n = 2), allied health (n = 2), spiritual care provider (n = 1), project officer (n = 1), and unspecified other (n = 7). Respondents were predominantly female (80.9%), and most reported Anglo, Australian, or European cultural backgrounds. There were notable gaps in respondent characteristics. Relevant professions such as Psychologists, General Practitioners, and Funeral Consultants were absent, and there were no respondents who identified as Aboriginal or Torres Strait Islander.
Interviews were conducted by one researcher in January 2024. Fourteen interviews were completed. Data from ten stakeholders (P1-P10, 11 interviews) were validated through member-checking and included in the analysis. Participants held various (not mutually exclusive) roles related to grief and bereavement, including employees of grief-related organisations (n = 3), those in caring roles (n = 3), community workers (n = 2), people with lived experience (n = 2), and other grief-related roles (n = 2).
Existing Grief and Bereavement Supports
The environmental scan resulted in a list of supports for grief and bereavement available in South Australia at September 2023. A total of 278 supports for grief and bereavement care were identified (see Supplementary file 1). These supports were provided by 176 organisations, with 134 supports specifically for South Australians (99 organisations). The remainder of supports were available Australia-wide.
All supports were assigned to a tier of the Public Health Model for Bereavement Support (Aoun et al., 2015).
Tier 1 supports (n = 123) were defined as those supports that are situated in the community and universally available to the public. Existing Tier 1 supports included: general information about grief (n = 70); community programs/events focused on discussing experiences of grief/death or developing compassionate communities (n = 19); public events to remember loved ones lost (n = 12); funeral directors/services (n = 7) and end-of-life doulas (n = 5); trainings and workshops for community members (n = 8); and Suicide Prevention Networks (n = 2).
Tier 2 supports (n = 108) are bereavement supports targeted to bereaved people, or equipping people to work with the bereaved, but not at a specialist level. These are often more formal but may be in the community or within a health setting. Existing Tier 2 supports included: programs or events for people working through personal grief (n = 20); South Australian general grief trainings for health professionals (n = 7); Australia-wide grief trainings (n = 8); bereavement services within a broader health service such as a hospital or aged care facility (n = 9); bereavement support groups (South Australia, n = 17; Australia-wide, n = 23); helplines (n = 14); and practical supports (e.g., financial assistance) (n = 10).
Tier 3 supports (n = 47) were classified as those offering specialist professional psychological bereavement services. All supports found at this level were professional counselling services. Eleven national counselling services were identified. South Australian counselling services that mentioned grief support were mostly for the general population (n = 14), but some also specifically targeted children (n = 7), families (not child-focused) (n = 4), Aboriginal and Torres Strait Islander people (n = 4), workplaces (n = 2), LQBTIQ + people (n = 1), Culturally and Linguistically Diverse people (n = 1), tertiary students (n = 1), parents (n = 1), and people with mental health issues and/or their carers (n = 1).
Most supports were available and relevant to people bereaved by any type of death but across all tiers, supports that were specific most commonly related to terminal illness (n = 60) (Figure 1). Number of supports at each level of support targeted to those bereaved by a specific type of death.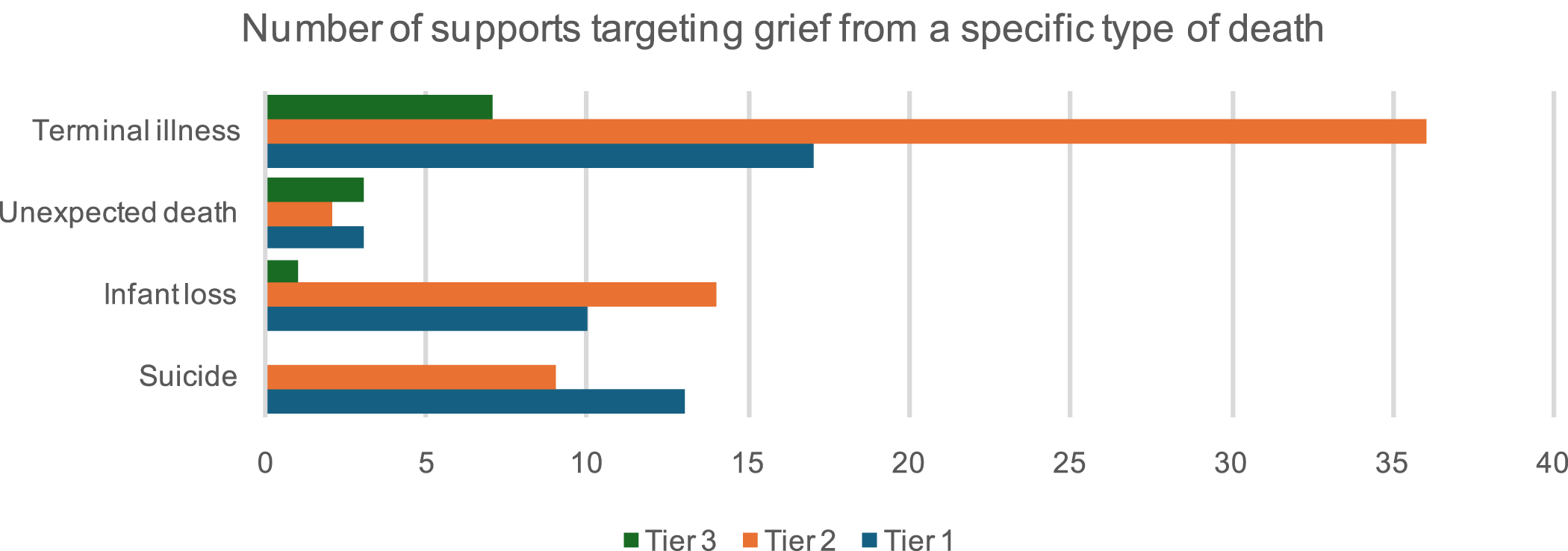
The personnel providing the support was unclear for Tier 1 supports, but Tier 2 and 3 supports were most commonly offered by qualified counsellors (n = 37), volunteers (n = 23), social workers (n = 14), or psychologists (n = 12). In Tiers 1 and 2, the majority of supports were virtual, but face to face delivery was more common for specialist counselling services (Tier 3). Where explicitly stated, the majority of supports in all tiers were provided free for the consumer (n = 98).
Across all tiers, South Australia-specific supports (n = 134) were mapped against five categories of support: Counselling Service, Event (grief literacy, training, or other), Information provision (grief literacy, links, training, or other), Program/Service, or Support Group (Figure 2), with counselling services being the most common type of support offered. Number of South Australian-specific support by category of support.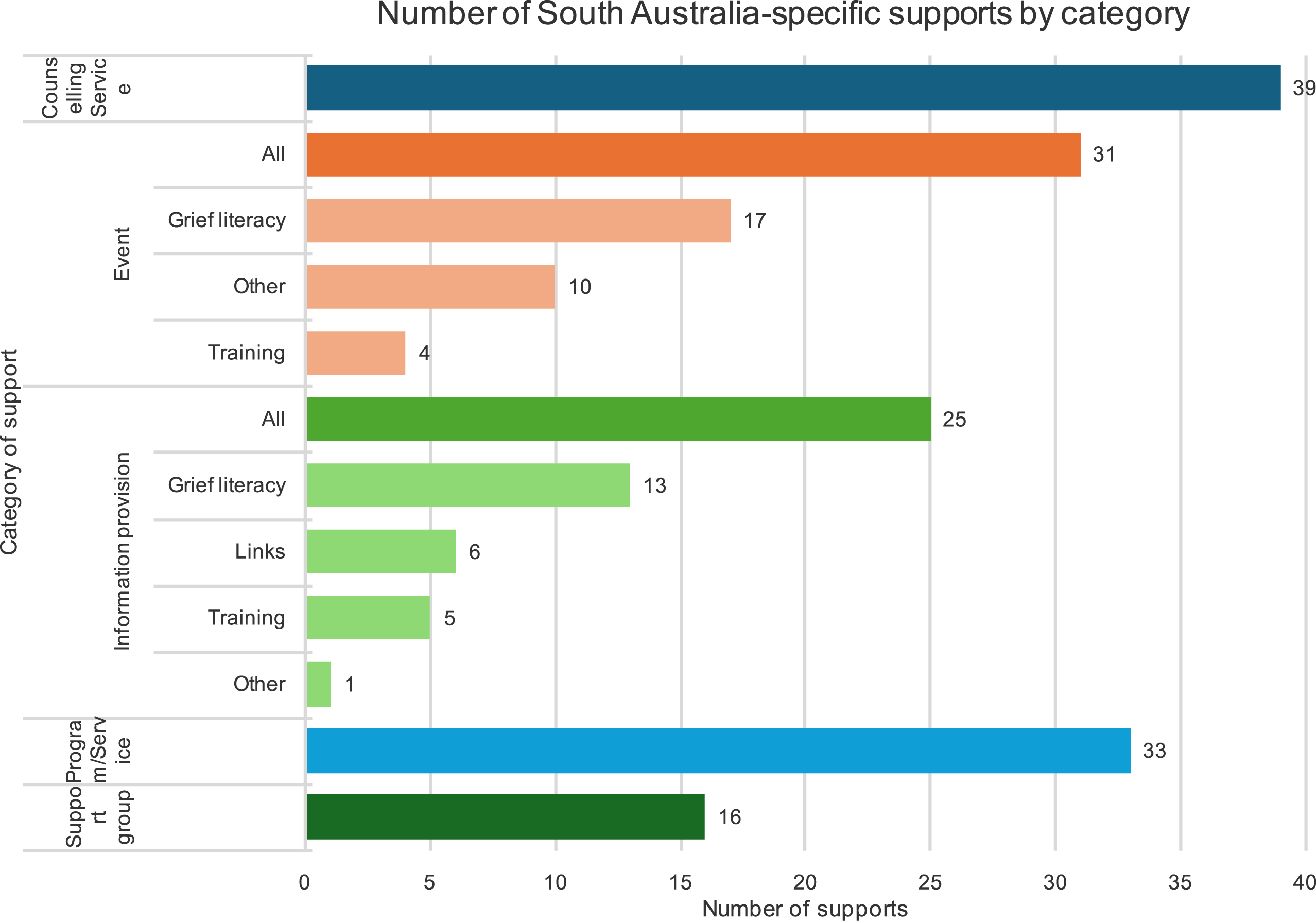
The majority of supports in South Australia with a specific location (i.e. not offered statewide) were located within metropolitan Adelaide (n = 104). Counselling services, support groups and grief and bereavement-related events were particularly lacking in more remote areas, with access in many locations limited to those supports available statewide (e.g. those with virtual counselling/telehealth options).
Areas of Unmet Need in South Australia
The findings from the desktop review, online survey and interviews were combined, with each subsequent data collection activity validating and building further understanding of the identified gaps in support. Six key areas of unmet need were identified and are described below, with quotes from participants where relevant.
Equitable and Timely Access to Support
Participants placed considerable emphasis on providing equitable access to support services. Concerns were verbalised around accessibility barriers, particularly in regional and remote areas, and the environmental scan confirmed a particular lack of face-to-face supports and supports for children and young people in non-metropolitan locations. “There’s a lack of in-person support in regional and remote areas, and everything’s online and it’s not okay.” (P9)
Participants also presented an urgent need to advocate for low-cost and timely support to ensure equitable access for all individuals. “Keeping that in mind, the overarching goal should be that it's accessible, probably equitable, low cost, and timely.” (P8) “It's very expensive for some specialised counselling...” (P7) “…people can't go on wait lists like they need to be addressed here and now and have things happen quickly.” (P2)
Centralised Place and Processes for Information and Support Navigation
All participants placed emphasis on coordination and integration of services to ensure holistic support for bereaved individuals. They highlighted the need to advocate for partnerships with existing support networks and community organisations to enhance navigation and service delivery. Navigation support was wanted to guide people in finding and accessing the right grief and bereavement supports for them. This also included the need for a first point of contact and triage system. “…people going through grieving... they need to be able to navigate the different areas. The overall program should have the idea of coordination in it, making sure that people have access to the right sort of services.” (P3) “I think that navigator role would be to tap into the support that is already there…needs to be some sort of first point of contact and triage, and we need to find out quickly and sensitively what people's needs are.” (P9)
Some participants suggested an information hub or directory to make it easy for health providers and the general public to find what grief and bereavement services exist across the state. “… the fact that you can't even access services, or you could go to the GP and get mental health things, but a lot of people don't know that that's available. I don't know how well publicised that is to people, but they don't know it's there.” (P7) “I like the idea of this information directory or repository, someplace whether that's a physical location or somewhere online that people could drop into… information hub might have a decision tree of sorts for people to, to sort through and identify, to find and access those supports that might be best suited for their journey.” (P1)
Part of successful navigation is having effective care and referral pathways to bereavement services for the general community. In particular, participants reported that pathways were needed for GP referrals and other allied health, as these professionals were the most likely first point of contact for many bereaved people. “…the only contact they really have that would refer them to any kind of service would be the medical and allied health staff.” (P2) “There’s a range of ways, but certainly the hospitals are good starting points and I mean I know a lot of social workers pick up the bereavement issues with people who die in hospitals, but you know it is very limited, they're not for example able to visit people…” (P3)
Continuity of Care
Participants emphasised the need for continuity of care throughout the grief and bereavement journey, which at times begins well before an actual death occurs. Supports need to enable continuity of care across services and tiers of support (e.g., in the transitions from health-related services to community grief support services), as well as continuity of care across time (e.g., pre-death grief to post-death grief in palliative care), and across interactions (i.e., not having to retell their story every time a new person is involved in their grief support journey). “…how we provide continuity of care…from death into grief and bereavement support…” (P1) “As the disease progresses and moving toward the end, working with the informal carers and then we are seeing where counselling is needed… but we do sort of definitely do that and contact family at 6–12 months sometimes after a loved one passed away…. That’s so important because the trust in the relationship would already be there…” (P9) “The way that I would see that operating is when they encounter the service that could be any member of staff who is assigned to get people triage time appropriately, but once they are in their appropriate care pathway, there is a system in place that allows for that touch base continuity over time.” (P5)
Cultural Sensitivity and Diversity and Underserved Populations
Participants described a need for care to be culturally sensitive, and some raised concerns about the lack of cultural sensitivity and understanding in existing support services. “Recognition of the need for culturally sensitive care and support tailored to the unique needs of diverse populations.” (P1) ‘…specific cultural element that needs to be considered, for example, First Nations’. (P5)
A number of specific populations were identified as underserved in regard to grief and bereavement care by the study participants or through the environmental scan of existing supports. These included older persons and the aged care setting, Culturally and Linguistically Diverse Populations, LGBTIQ + people, workplaces and schools, pastoral care workers and bereaved carers. There was also emphasis on the need to consider different types of support or adapt supports to meet the needs of different groups, such as Aboriginal and Torres Strait Islander populations, military and emergency services personnel, those with disabilities, and bereaved children and adolescents. “Then for emergency services there is actually nothing that is specific and because we are very aware of the fact that military and emergency services and their families actually do form a unique cultural group…. So when we are looking at supports for those specific groups there needs to be a specific cultural lens applied. Because they will often feel as though civilian resources are not going to target the needs that are specific to their cultural group.” (P5) “…people with mental health issues need to be acknowledged.” (P2) ‘…they need to be vastly effective up to an adolescent, yeah young adults and developmental needs, …like people with disability, First Nations people, LGBTIQ + people.” (P4) ““And the other thing is when we have people with particular needs, older persons people have been associated with suicide homicidal trauma of some sort, or neurodivergent, disabled, First Nations people need to have a double lens as well…” (P10)
It was felt important to consider the benefits of tapping into the services that already work with and target those populations, rather than creating completely new services to fill the gaps. “Tap into all those things that are already set up in underrepresented populations because people are already accessing them…” (P9)
Evidence-Informed General Community Supports
The environmental scan identified a gap in supports that equip the general population with the confidence and knowledge to provide helpful informal support to the bereaved people in their personal social networks. “People need just a little bit of a kickstart to know how to help somebody who's grieving.” (P3)
Participants highlighted the need for community supports to include emotional support, information, practical support, and skill-building. This also included advocacy for community education and awareness programs to enhance understanding and empathy and normalise grief as a natural part of loss and life. “If we as a community are talking more about death and dying and planning for it then I think part of that conversation needs to involve grief and bereavement… continuing to get that message out, continuing to advocate for this, creating a compassionate community…” (P2) “Information about how it can present, what does it look like in reality because it is a unique experience for every single person.” (P6) “There needs to be broad community education by way of TV advertisements getting grief and bereavement onto TV soaps.” (P3)
When envisioning a statewide model for the future, participants also perceived person-centred governance approaches as important. This was linked to building community capacity and consumer involvement in decision-making processes. “We need appropriate representation from different stakeholders in governance…” (P1) “... it really needs a person-focused management.” (P3) “I think clear accountability and clear responsibility you know some kind of regular network that brings providers together… getting the right combination of people in governance…” (P9)
Professional Development in Grief Support
A lack of training, certification, and accreditation for specialisation in grief and bereavement care for health professionals such as psychologists and counsellors were identified, with some participants perceiving a consequent absence of grief counsellors in South Australia. “I think the current model... doesn't have the specialist… We found about two [counsellors] actually offer grief counselling.” (P3) A lack of grief training for other health and non-health sectors (e.g., emergency services) who come in regular contact with bereaved people was also highlighted. ‘…training and modules around grief and bereavement and specialist areas…first responders…how can we ensure that those that are first on the scene…” (P1) “…they might not even need anything else you know, they can triage and that reassurance might be all they need…” (P2)
Some participants noted a shift in university education from a ‘grief informed’ model to a ‘trauma informed’ model suggesting that universities should reintegrate explicit grief-related information into their courses. Others commented on the value of a general grief-informed approach. “Universities are a good place to go to get the ball rolling, to actually have loss and grief information given to students.” (P3) “…having a more grief-informed perspective...is probably more relevant than having trauma-informed care all the time…the last two or three years has been a lot more trauma informed training.” (P2) …” they certainly ceased the loss and grief courses that we were offering to undergraduates and I (sic) so I don't know that the graduate certificate exists any longer.” (P3)
Discussion
While the environmental scan showed existing services in South Australia at all three tiers of the Public Health Model for Bereavement Support (Aoun et al., 2012), six key areas of unmet need were identified. These included: (a) equitable and timely access to support, (b) centralised place and processes for information and support navigation, (c) continuity of care, (d) cultural sensitivity and diversity and underserved populations, (e) evidence-informed general community supports, and (f) professional development in grief support. These areas encapsulated key priorities, challenges, and recommendations from participants in relation to the concept of implementation of a statewide grief and bereavement care model but are also reflected in the broader literature.
A number of other Australian studies point to gaps in bereavement support coordination, integration between grief services, and provision of a centralised place for accessing grief and bereavement information (Aoun et al., 2021a; 2021b; Bindley et al., 2023; Blackburn & Bulsara, 2018; Breen & O'Connor, 2013; Bull et al., 2002). Limited coordination of bereavement services has also been highlighted as a gap in palliative care services in the United Kingdom (Breen et al., 2014). Although bereavement support standards state that bereavement programs in palliative care services should provide coordination (Hudson, Hall, Boughey, & Roulston, 2018), and care coordination is a common feature of palliative care services internationally (Birtwistle et al., 2022; Gorin et al., 2017; NSW Ministry of Health., 2018; Reeves et al., 2020), this coordination does not necessarily extend to bereavement care or beyond the death (Aoun et al., 2021a; Bindley et al., 2021; deCinque et al., 2006). The absence of care coordination bridging pre- and post-death grief, points to continuity of care as a particular issue for the palliative care sector (Lichtenthal et al., 2024), as well as in acute and critical care (Boven et al., 2022; O’Sullivan et al., 2021; Pattison et al., 2021) and residential aged care (Banerjee & Rewegan, 2017; O’Connor & Wilson, 2021). Bereaved families are often discharged at the time of the patient or resident’s death, shifting the responsibility for bereavement care away from those services, or limiting the time-frame in which bereavement care is offered (Sealey et al., 2015). The resulting separation from known and trusted professional supports following a death is reported to create a sense of abandonment for many families (Aoun et al., 2021c; Back et al., 2009; deCinque et al., 2006; Lichtenthal et al., 2024; She & Prigerson, 2018). An international review of hospital-based bereavement care services after the death of a child recommended guidance in the lead up to, and consistent bereavement follow-up that ensures continuity of relationships between staff and families after, the death as best practice (Donovan et al., 2014). This is further mirrored in primary care settings, where patients perceive bereavement support as more helpful when the provider is known, and deeper involvement between clients and clinicians is reported to increase proactive responses to bereavement and allow tailoring of supports to meet individual needs (Pearce et al., 2021).
In addition to this, as reflected in our study, continuity of care is also needed in relation to the connections between formal service providers, and between clinical and community settings (Pattison et al., 2021). Having a single place or person to contact for information and assistance about grief and the available supports may also promote continuity of care over time, and minimise distress by negating the need for bereaved people to contact multiple people/services and retell their story repeatedly (Bindley et al., 2021). Although navigation support was confirmed as a gap in our study at the time of data collection, a bereavement navigation service is currently being piloted in South Australia, designed to connect people with bereavement and grief information and supports (Adelaide, 2024). The participants in our study more strongly focused on the aspects of information access, navigation, and coordination, than on the need for more actual supports, which suggests that unmet needs in South Australia may be better addressed through an overarching model for grief and bereavement support which articulates the processes for integrated, interconnected statewide support rather than simply the establishment of new grief services. This pilot bereavement navigation service may be foundational in achieving this. As articulated by Abel et al. (2023), effective and sustainable bereavement care relies on collaboration between community networks and professional services. Referral pathways for grief and bereavement care, therefore, should also be part of the process designed to support such interconnected care (Sealey et al., 2015).
One area of service provision itself that was perceived as lacking by our study participants was the number of available grief counsellors. However, the results of the environmental scan showed that, at least in metropolitan areas of South Australia, there is an abundance of general counselling options. One of the key factors making these options insufficient for addressing grief and bereavement needs is a lack of professional specialisation in grief. South Australia lacks any current formal education programs for specialisation in grief and bereavement care, making it difficult for counsellors and psychologists to offer the specialised grief-specific support that forms Tier 3 of the Public Health Model for Bereavement Support (Aoun et al., 2015). In South Australia, this lack reflects a shift from previously available stand-alone grief and bereavement qualifications to a trauma-informed care focus. Although grief-informed care and trauma-informed care overlap, they are not the same, so may not be suitable for substitution (Schuurman & Mitchell, 2020). The international literature frequently highlights concerns about professionals working with bereaved individuals lacking specialised knowledge and training in grief (Breen, 2010; Doughty Horn et al., 2013; Guldin et al., 2015; Hall & Henning, 2022; Ober et al., 2012). This lack of training often results in counsellors feeling unprepared to discuss grief and loss, leading to increased anxiety when dealing with death-related issues (Doughty Horn et al., 2013; Ober et al., 2012). Although there is some evidence that grief-specific training improves the self-perceived competence of counsellors (Ober et al., 2012), there appears to be an absence of research measuring the impact that specialist grief training has on client outcomes. Whilst the Public Health Model suggests that only 10% of bereaved people are at high risk and require this level of support, its value cannot be underestimated (Aoun et al., 2012). However, the majority of bereaved people’s needs should be met by community supports, whether these are Tier 1 universally available community supports and personal networks, or Tier 2 targeted community supports. This highlights the need for broader professional development and evidence-informed general community supports as well.
To meet the identified gaps in support, professional development should not only consider the formal training, and potential certification and accreditation of counsellors and psychologists to specialise in grief and bereavement care, but also training in grief for the whole health sector and non-health sectors. Targeted community supports may be offered by other professionals within the health system, such as social workers in a hospital setting (Gundry et al., 2023; Williams et al., 2000), which suggests that some grief training for other health professionals may also be necessary to meet bereaved people’s needs. Authors of a review of international palliative care policies and bereavement support practices similarly concluded that educational interventions for primary care practitioners and community pharmacists are essential to bridge the gaps in palliative care bereavement support (Breen et al., 2014). In addition to this, non-health professions such as police are often first responders in the event of a death, and their responses to bereaved individuals may significantly impact their bereavement experience (Bellon et al., 2015), pointing to the likely benefits of offering grief training more broadly.
Distinct from the training of professionals, public education is needed to equip the general population with the skills and knowledge to support bereaved people in their own lives if the majority of bereaved peoples’ needs are to be met by universal community supports (Aoun et al., 2012). This community capacity forms the foundation for effective grief and bereavement support at the population level and has the potential to lower the demand for higher level supports, thereby saving individual and health system costs (Comans et al., 2013; Visser, Comans, & Scuffham, 2014), and also minimising the wait lists for specialised counselling services. Although bereavement care has become professionalised, it is clear that the compassion one can extend to others during times of grief does not require professional skill or management, so although professional services have their place and some targeted education may benefit the general public, ultimately formal services need to enable informal community supports to occur naturally (Abel et al., 2023).
Participants also mentioned building the capacity of the community to participate in decision-making and governance of any grief and bereavement model implemented at a statewide level. Effective grief and bereavement care is necessarily person-centred, so person-centric approaches to governance are called for. The Australian Commission on Safety and Quality in Health Care (2018) identify person-centred governance systems as one of seven key attributes of high-performing person-centred healthcare organisations. This involves integration of patients, families and consumers as active partners in governance at multiple levels throughout an organisation (Australian Commission on Safety and Quality in Health Care, 2018). Since grief is a natural and universal human phenomenon (although experienced uniquely by each individual) (Abel et al., 2023), it is an area in which all people have some expertise. Governance structures for the oversight of any programs or model for grief and bereavement support at a population level, therefore, are particularly suited to including broad representation from a wide range of community members as stakeholders.
Limitations
Data in this desktop review were extracted and categorised based only on the available written information on publicly accessible websites (or direct communications) so, where assumptions would have to be made, data were classified as unclear and not counted. Additionally, although the methods searched specifically for South Australian supports, some supports available nationally were found. These supports were also included and reported as supports available to South Australians but do not represent all grief supports available Australia-wide. Similarly, the findings may not represent the existing supports and unmet needs in other states and countries. This study was also limited to the perspectives of people working in the grief and bereavement space, and so may not represent the unmet needs from a consumer perspective. However, the findings were in keeping with the broader literature which includes consumer voices and international evidence.
Conclusion
Many grief and bereavement supports are currently available in South Australia, ranging from online information for the general public to better understand grief, to face-to-face professional counselling services for bereaved people. However, the options for support can be difficult to find and most services appear to function in silos, with very little evident connection between providers. While there is a good foundation for statewide grief and bereavement care in South Australia, with existing supports at all three tiers of the Public Health Model of Bereavement Support, work is needed to integrate existing supports, enable easy identification and navigation of suitable supports, and ensure that supports meet the needs of the diverse and geographically dispersed population. Finally, to ensure the future capacity of grief and bereavement service providers, it may be necessary to reform training and education. This would involve expanding professional development opportunities, providing evidence-based community support, and offering specialised education on grief and bereavement. These findings further our understanding of unmet needs in grief and bereavement care, providing a basis for the selection or development of a model that could meet the needs of bereaved people at a population level.
Supplemental Material
Supplemental Material - Identifying Gaps in Grief and Bereavement Support: Insights from a Multi Methods Study
Supplemental Material for Identifying Gaps in Grief and Bereavement Support: Insights from a Multi Methods Study by Deborah Forsythe, Kate Davis, Greg Sharplin, Kate Swetenham, and Marion Eckert in OMEGA - Journal of Death and Dying
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the South Australian Department for Health and Wellbeing RFQ reference number: A4771790 and The Hospital Research Foundation Group RFQ reference number: A4771790.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, KD, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Greg leads the development, implementation and evaluation of the RBRC five-year Strategic Plan; fostering national and international links and strategic collaborative relationships with relevant research institutions, universities and community bodies; day-to-day management of the RBRC; and leading research activities associated with the RBRC’s research program.
Her achievements include a Churchill Fellowship, the 2024 Sigma Theta Tau International Hall of Fame Nurse Researcher award, and co-leading the first Australasian Nursing and Midwifery Clinical Trials Network. With 35 years in healthcare strategy and implementation science, she partners globally, including with Commonwealth Centre for Digital Health, and is pursuing a Bachelor of Law (Honours).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.