
Abstract
The aim of this study was to explore public attitudes toward medically assisted dying, focusing on the role of socio-demographic factors, mental health conditions, and personal experiences. Data were collected via an online panel in Slovenia, which consisted of 567 participants (53.1% men) aged 18 years and older. The majority of respondents supported medically assisted dying for terminally ill individuals (76.4%) and expressed willingness to support a loved one’s decision (72.8%). The analysis indicated that psychosocial factors and personal experiences predict attitudes toward medically assisted dying. In particular, women, individuals with poorer physical and psychological health and individuals in better environmental conditions were more likely to have positive attitudes. In contrast, individuals who had experienced the loss of a loved one were more likely to oppose it. These findings suggest the need for further research to deepen understanding of the factors that predict attitudes toward medically assisted dying.
Introduction
In many European countries, the last decade has been characterized by a growing debate about the acceptance and regulation of end-of-life practices. Growing public sensibility to a ‘right to die’ for terminally ill patients has been one of the main components of these debates. Several countries around the world have passed medically assisted dying laws that allow a physician, or in some cases a nurse practitioner, to legally prescribe or administer life-ending medication to individuals with a serious illness (Emanuel et al., 2016).
Currently (year 2024), medically assisted dying is legal in several European countries (Netherlands, Belgium, Luxembourg, Switzerland, Austria, Spain, Portugal), in ten US states, in Canada, in five states of Australia and in Colombia, while other countries such as France, Italy and Slovenia are currently discussing the possible legalization of medically assisted dying (Bloomer et al., 2024; Güth et al., 2023; Queensland University of Technology, 2024). Most countries where end-of-life practices are legal employ strong regulation and safeguards. These include the patient being of legal age, being mentally capable of making the decision, and suffering from a terminal, incurable illness or unbearable pain. The patient’s request must be voluntary, well-considered and repeated over an extended period of time. Typically, two independent medical professionals must agree to the procedure and before making the decision, the patient must be fully informed about all available treatment options, including palliative care (Emanuel et al., 2016; Vilpert et al., 2020).
Although research points to a broader societal shift towards prioritizing individual autonomy and the right to make decisions about one’s own life and death, trends concerning public opinion on medically assisted dying differs per country (Emanuel et al., 2016). While in many countries acceptance is steadily increasing, some countries report a peak in acceptance followed by a moderate decline between 1999 and 2008, likely due to socio-political and economic changes following the fall of communism that raised concerns about the potential abuse of medically assisted dying (Carlson, 1998; Cohen et al., 2006, 2014).
Attitudes toward medically assisted dying vary from country to country and are shaped by a complex interplay of factors that differ according to population and context. Among the most studied determinants are socio-demographic characteristics such as age, education and religiosity. Studies have consistently found that higher levels of education (Cohen et al., 2006; Rietjens et al., 2005; Stronegger et al., 2013) and sociocultural liberalism (Cohen et al., 2006; Köneke, 2014; Verbakel & Jaspers, 2010) are associated with greater approval of medically assisted dying, while religiosity generally correlates with lower approval (Borovecki et al., 2022; Cohen et al., 2006). This relationship holds at both the individual and societal level, where countries with a strong religious climate show lower support for medically assisted dying. Other socio-demographic factors such as gender, marital status and household size have shown less consistent or no clear associations with attitudes towards end-of-life practices (Stolz et al., 2017).
Evidence suggests that depressive symptoms, psychological suffering, and concerns about future quality of life (Hendry et al., 2013; Smets et al., 2010; Stolz et al., 2017) increase the likelihood of support to these end-of-life practices, particularly in the general population (Buiting et al., 2012), older adults (Sullivan et al., 1998) and severely ill patients (Emanuel, 2002). While many studies of terminally ill patients have consistently emphasized the importance of quality of life for attitudes toward medically assisted dying (Emanuel et al., 2000; Johansen et al., 2005), fewer studies have examined whether this holds true within the general population. These studies suggest that decreased quality of life is a significant factor predicting the perceived justifiability of medically assisted dying. Symptoms associated with a lower quality of life, such as physical and psychological suffering, are strongly correlated with more positive attitudes towards medically assisted dying (Bahník et al., 2021; Hendry et al., 2013). In addition, people are more likely to consider medically assisted dying acceptable for symptoms that negatively impact personal well-being and relationships with others, such as feeling like a burden to others and losing dignity (Bahník et al., 2021).
Active suicidal ideation and the frequency of such thoughts have been found to predict attitudes towards end-of-life decisions. Although these factors have rarely been studied as determinants. Individuals experiencing such distress may have more positive attitudes toward medically assisted dying and be more willing to hypothetically consider it (Stolz et al., 2017; Suarez-Almazor et al., 2002). Despite the well-established influence of socio-demographic factors and factors such as religiosity, the psychosocial aspects (including social support, mental health status and environmental conditions) that predict attitudes toward medically assisted dying have only been researched to a limited extent. The aim of this study is to examine public attitudes toward medically assisted dying and to also analyse their relationship to various socio-demographic characteristics, mental health conditions and personal experiences.
In this study, the term medically assisted dying refers to the administration—and not the prescription— of a lethal dose of medication by a medical professional to a capable individual who requests it, as defined by the European Association of Palliative Care (Radbruch et al., 2016).
Methods
Procedures
Data were drawn from a longitudinal study, specifically Individual in the Grip of COVID-19: Psychological Consequences of the Epidemic and Protective Measures to Contain the Spread of Infection (Slovenian Research and Innovation Agency, Ljubljana, Slovenia [from 2021–2024]). For the present study, only participants who took part in the last measurement wave (year 2023) were included in the sample.
The data collection was conducted by Valicon, a certified private company with extensive experience in surveys and data collection (Ljubljana, Slovenia). It uses quota sampling so that the allocation of participants within each stratum is a proportional representation of the demographic composition of the total population of Slovenia. Participants were gathered through an online panel. They participated by responding to an email invitation and completing a series of questionnaires. Participation was voluntary and anonymous. Participants received a participation reward in the form of voucher points.
Approval to conduct the study was obtained from the Commission of the University of Primorska for Ethics in Human Subjects Research (KER UP) and the Commission for Research Ethics in the Department of Psychology at the University of Primorska (details are provided in the Section on Ethics). Researchers’ contact details and support resources were provided to inform participants of the support available in the event of an emergency.
Participants
Bivariate Analyses – Attitudes Towards Medically Assisted Dying by Socio-Demographic Characteristics.
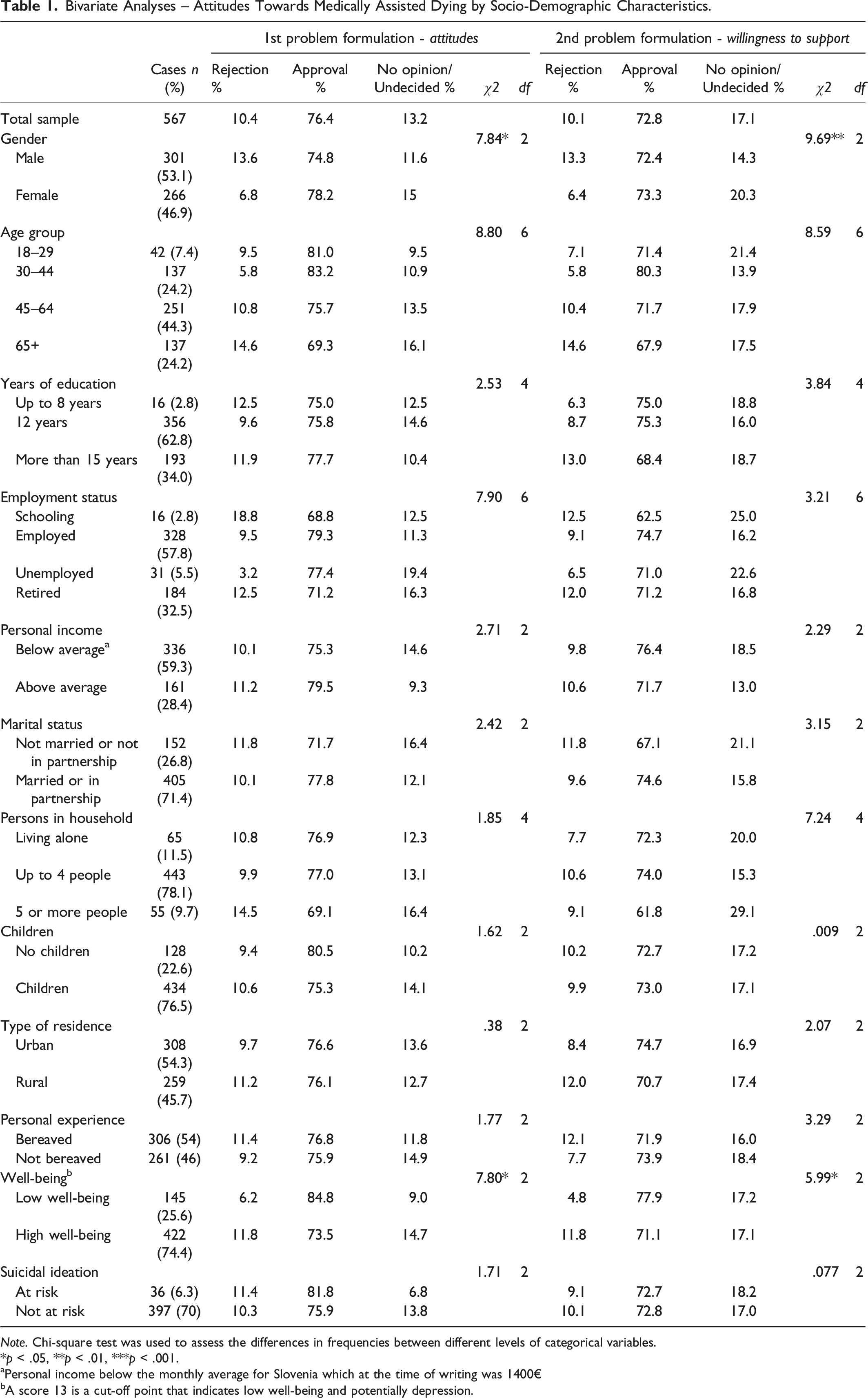
Note. Chi-square test was used to assess the differences in frequencies between different levels of categorical variables.
*p < .05, **p < .01, ***p < .001.
aPersonal income below the monthly average for Slovenia which at the time of writing was 1400€
bA score 13 is a cut-off point that indicates low well-being and potentially depression.
Measures
Data were collected using a comprehensive, self-administered online battery of questionnaires. The analyses in this study were based on the following measures:
Socio-Demographic Characteristics
Participants provided demographic information, including age (in years), gender (male/female), years of education (up to 8 years, 12 years, 15 years or more than 15 years), employment status (schooling, employed, unemployed or retired), personal income (below/above the Slovenian monthly average = 1400.00€) (Statistical Office of the Republic of Slovenia, 2024), marital status (married or in a relationship, not married or in a relationship), household size (living alone, up to 4 people or more than 5 people), whether they have children and type of residence (urban/rural).
Medically assisted dying
To measure attitudes toward medically assisted dying, two different problems were contrasted. Before responding, participants were given a brief definition of medically assisted dying, specifying that it refers exclusively to cases involving terminally ill patients whose death is hastened or induced to relieve pain and suffering. Subsequently, the participants were asked about their attitudes toward medically assisted dying based on the following problem formulation: “Do you think that terminally ill people should have the option to end their lives?”
The second question related to the willingness to support a loved one’s decision to end their life. The following problem formulation was used: “If your loved one was suffering from a terminal illness and wanted the opportunity to end their life, would you support their decision?” The response categories for both variables were “yes”, “no” or “don’t know / don’t want to answer”.
Personal Experience
Participants were asked a dichotomous question about whether they had recently lost someone. The response categories were “yes” or “no”.
(Mental)health conditions
Quality of life
The Quality of Life Questionnaire (WHOQOL-BREF) (WHO, 2004) consists of 26 items that measure four domains of perceived quality of life: physical health (mobility, daily activities, functional capacity, energy, pain, and sleep), psychological health (self-image, negative thoughts, positive attitudes, self-esteem, mentality), social relationships (personal relationships, social support, and sex life), and environmental health (financial resources, safety, health and social services, living physical environment, opportunities to acquire new skills and knowledge, recreation, general environment, and transportation). Participants rate the responses on a 5-point scale.
Well-being
The World Health Organization Well-Being Index (WHO–5) (WHO, 1998). The scale includes five items regarding an individual’s well-being perceived over the past two weeks. A 6-point Likert scale is used (from 0 “never” to 5 “all the time”). A high score indicates good well-being. A score of 13 is a cut-off point indicating low well-being and possibly depression.
Suicidality
Paykel Suicide Scale (Paykel et al., 1974) contains five items assessing the presence of suicidal thoughts, ideations, and plans in the last two weeks. The first four questions use a six-point scale (from 0 “never” to 5 “always”), where higher scores indicate greater severity of suicidal ideation. The fifth question on previous suicide attempts is answered with one of the following options “yes, in the past two weeks”, “yes, in the past six months”, “yes, but more than 6 months ago”, and “no, never”.
An individual is considered at risk if they respond “yes, in the past two weeks” to the question about previous suicide attempts. Additionally, they are also at risk if they score 4 or 5 on at least two of the first three items regarding suicidal thoughts and intent, or if they score 2 or higher on the fourth item, which asks about having a specific plan.
Statistical Analyses
All data analyses were carried out using IBM SPSS Statistics Version 29. Frequency analyses and descriptive statistics were used to describe the characteristics of the sample. Chi-square and ANOVA were performed to determine the differences between the variables and a post hoc test (Tukey HSD) was conducted to identify exactly which groups differ from each other. Stepwise multinomial logistic regression analysis (backward procedure) was used to identify independent determinants of attitudes towards medically assisted dying. This regression approach begins with a full (saturated) model and at each step gradually eliminates non-relevant variables from the regression model, starting with the least significant variable (Hosmer et al., 2013). At each step, the model is re-evaluated until only variables with significant contributions remain.
Results
The study examined attitudes towards medically assisted dying across various socio-demographic characteristics and psychosocial factors, focusing on attitudes towards medically assisted dying and willingness to support a loved one’s decision to end their life when suffering from a terminal illness. Approximately 75% of participants approved of medically assisted dying, regardless of the problem formulation (Table 1): 76.4% for the first formulation and 72.8% for the second.
The Chi-square test indicated a significant relationship between personal beliefs about medically assisted dying and willingness to support a loved one’s decision (χ2(4) = 477.47, p < .001). Of those in favor of terminally ill patients’ right to end their lives, 89.4% would also support a loved one’s decision to end their life, while only 6.8% of those opposed to medically assisted dying would support a loved one’s decision.
Bivariate Analyses – Attitudes Towards Medically Assisted Dying by Quality of Life Domains.
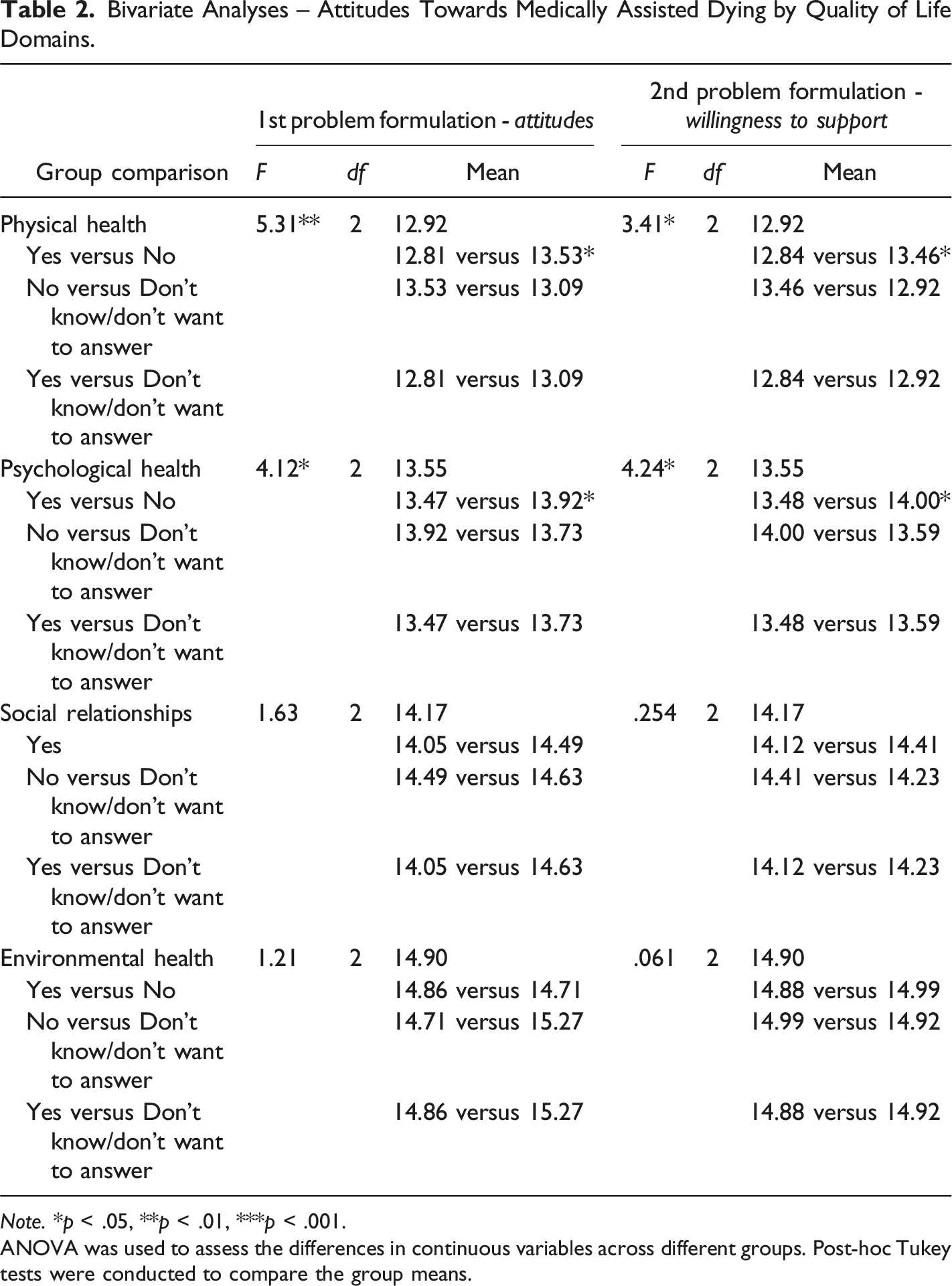
Note. *p < .05, **p < .01, ***p < .001.
ANOVA was used to assess the differences in continuous variables across different groups. Post-hoc Tukey tests were conducted to compare the group means.
Participants experiencing a low level of well-being indicated a higher level of approval (84.8%). In terms of quality of life domains, physical and psychological health were significantly related to attitudes toward medically assisted dying and willingness to support a loved one’s decision. The use of Tukey’s post hoc test showed which pairs of values significantly differed. Analysis of the test indicated that there was a significant difference between the “Yes” and “No” groups in attitudes and willingness to support, with the “Yes” group showing significantly lower physical and psychological health levels compared to the “No” group.
Multivariate Analysis
Multinomial Logistic Regression Analyses (Stepwise Backward) Results for Attitudes Toward Medically Assisted Dying (N = 567).
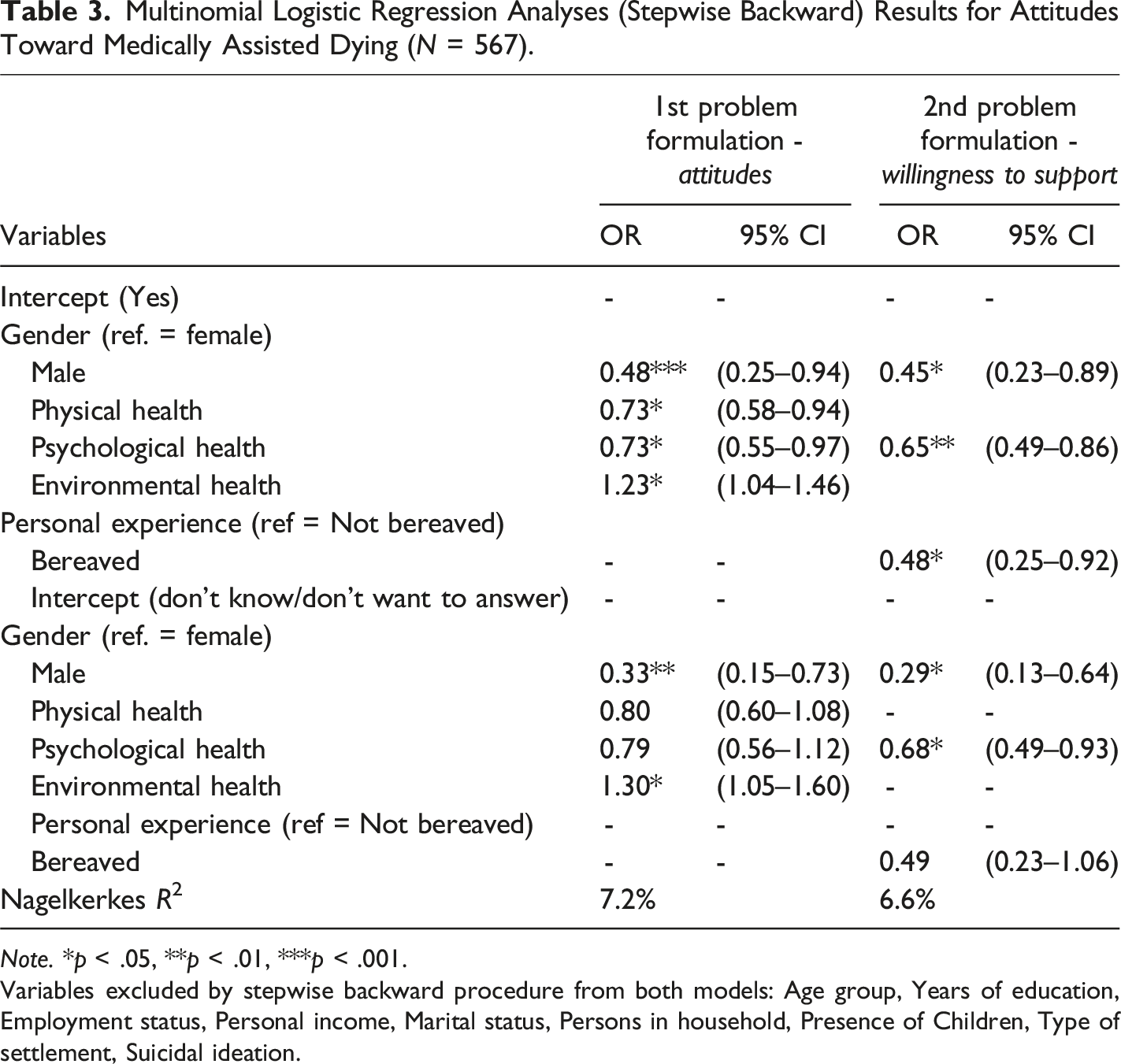
Note. *p < .05, **p < .01, ***p < .001.
Variables excluded by stepwise backward procedure from both models: Age group, Years of education, Employment status, Personal income, Marital status, Persons in household, Presence of Children, Type of settlement, Suicidal ideation.
Similar to the bivariate analysis, there were no strong associations in the sociodemographic variables except for gender. Men were less likely than women to approve medically assisted dying and to support a loved one’s decision, and they were also less likely than women to be undecided.
Better physical health was associated with lower approval of medically assisted dying. Better psychological health was associated with lower approval and lower support for a loved one’s decision. Higher environmental health scores were associated with greater support for medically assisted dying. Those who had recently experienced a death were less likely to support a loved one’s decision. The Nagelkerke R2 values for the models were 7.2% for attitudes and 6.6% for willingness to support, indicating modest explanatory power.
Discussion
Research on attitudes toward medically assisted dying often focuses on various socio-demographic factors. In our study, we expanded this framework by also considering psychosocial factors that may provide a deeper understanding of the motivations behind individuals’ attitudes toward medically assisted dying. Previous studies have examined health-related factors, but usually at a broader, national level — focusing on aspects such as healthcare systems, infant mortality and life expectancy (Inglehart et al., 2021). However, there is a need to emphasize the role of health-related experiences at the individual level. It is also important to note that this study was conducted on a Slovenian sample, as attitudes toward medically assisted dying in post-communist countries remain under-researched. Given the known cross-cultural differences in these attitudes, further research is needed in this context, especially as many of the existing studies are also outdated.
In recent decades, empirical research has consistently shown a trend toward increasing acceptance of medically assisted dying (Attell, 2020; Emanuel et al., 2016; Inglehart et al., 2021). In our study, we found that a significant majority of participants were not only in favor of the availability of medically assisted dying for terminally ill persons but were also willing to support a loved one’s decision to pursue it. This is consistent with previous research showing that Slovenia has a relatively high level of acceptance of medically assisted dying among Central and Eastern European countries (Cohen et al., 2013, 2014; Inglehart et al., 2021). It is also consistent with broader trends observed in high-income countries, including Slovenia, where in contrast to many post-communist countries that have experienced a religious revival, religiosity remains low in Slovenia, as in Estonia and the Czech Republic (Cohen et al., 2013). This secular trend correlates with a higher acceptance of medically assisted dying. In addition, the degree of personal permissiveness, which reflects society’s tolerance of personal life choices such as divorce, abortion and homosexuality, also plays a decisive role. In Slovenia, this tolerance is closely linked to a higher acceptance of medically assisted dying, similar to that observed in Western Europe (Cohen et al., 2006; Inglehart et al., 2021).
Contrary to much of the existing literature, we found that socio-demographic factors, with the exception of gender, did not significantly predict attitudes toward medically assisted dying. These results could be due to the characteristics of the sample itself. In terms of gender, we found that men were slightly more likely to oppose medically assisted dying than women, while women were less determined but had higher overall approval rates. Our findings differ from numerous studies (Bachmetjev et al., 2024; Ryynänen et al., 2002; Saadeh et al., 2023; Yun et al., 2011), conducted in varied cultural contexts, which reported that men were more likely to approve of medically assisted dying than women. However, not all studies were consistent with these findings, with some studies finding no difference between genders (Evenblij, Pasman, van der Heide, Hoekstra, & Onwuteaka-Philipsen, 2019; Rietjens et al., 2005; Stronegger et al., 2013). In contrast, other studies have found that older women have more positive attitudes toward medically assisted dying (Lifshitz et al., 2024) and are more likely to be involved in conversations about death in a palliative health care center (Skulason et al., 2014).
With regard to physical health, our findings are consistent with previous studies indicating that poor physical health, loss of meaningful activities, and functional decline are common motivators for supporting or considering medically assisted dying (Butt et al., 2003; Pearlman et al., 2005). In addition, factors such as fear of disease progression, inability to enjoy life, prolonged physical suffering, and inability to perform activities of daily living have been associated with public support for the legality of medically assisted dying (Evenblij, Pasman, van der Heide, van Delden, & Onwuteaka-Philipsen, 2019; Ganzini et al., 2008; Hendry et al., 2013; Monforte-Royo et al., 2012). This reflects our observation that those with poorer physical health are more likely to support medically assisted dying.
Although people may wish to end their life due to various medical conditions, society or legal frameworks do not consider all these cases to be equally justified for medically assisted dying. In terms of psychological health, we found that those with poorer psychological health were more likely to accept medically assisted dying and support a loved one’s decision. This is consistent with previous studies that have identified depressive symptoms, along with loss of meaning, purpose, control and self-worth, as critical psychological mechanisms mediating the relationship between quality of life and the desire for hastened death (Butt et al., 2003; Evenblij, Pasman, van der Heide, Hoekstra, & Onwuteaka-Philipsen, 2019; Pearlman et al., 2005; Robinson et al., 2017). From a legislative standpoint and prevailing public opinion, medically assisted dying is generally framed around cases of severe physical illness, often with terminal or irreversible physical suffering (Bahník et al., 2021; Emanuel et al., 2016). When it comes to psychological suffering, legislative frameworks tend to be far more restrictive and nuanced, largely due to complex ethical, philosophical and medical dilemmas.
As for the environment, we found limited empirical evidence to support our findings that a better environment is associated with more positive attitudes toward medically assisted dying. Previous studies such as those by Jorgenson and Neubecker (1981), Cohen et al. (2006) and Stolz et al. (2017) suggest that individuals living in urban settings are generally more supportive of medically assisted dying, while those living in rural areas are more opposed to it. In our analysis, the type of settlement was not statistically significant. This could be due to the sample itself. Furthermore, as this was a self-assessment, it is possible that some participants may have identified their settlement as urban, even if it does not technically fall into this category, which could influence the results. Therefore, the environmental health variable could provide a more comprehensive indicator of settlement type by capturing factors such as transportation, services and opportunities in the surrounding area, with those living in somewhat more favorable environmental conditions showing a greater likelihood of supporting medically assisted dying.
Personal experiences with death and end-of-life suffering of a loved one may predict their views on topics such as medically assisted dying, palliative care, and other end-of-life decisions (Fadem et al., 2003; Hendry et al., 2013; Mak & Elwyn, 2005; Pearlman et al., 2005; Verbakel & Jaspers, 2010). Participants in the previous studies describe powerful, emotional accounts of witnessing unbearable pain, loss of dignity, and prolonged suffering that reinforced their belief in the importance of having control over their own death through medically assisted dying or other end-of-life practices. One might expect that the recent loss of a loved one would be associated with higher approval of medically assisted dying. However, our results suggest that this is not the case. One possible explanation for this could be that the emotional impact of the death of a loved one leads to a greater awareness of the complexities and ethical concerns surrounding medically assisted dying, causing some individuals to reconsider their views. Diversity in personal coping mechanisms and cultural or religious beliefs may also play a role in shaping different responses, even after similar loss experiences (Cohen et al., 2006; Fadem et al., 2003; Hendry et al., 2013; Inglehart et al., 2021; Mak & Elwyn, 2005; Pearlman et al., 2005; Sabriseilabi & Williams, 2022).
Our study found that poor physical and psychological health were significant predictors of support for medically assisted dying, which is consistent with previous research. This suggest that addressing and improving individuals’ physical and mental well-being might play a crucial role in changing attitudes toward medically assisted dying. However, environmental health showed limited empirical support, emphasizing the need for further research to better understand how factors such as urbanization, access to resources, and living conditions predict attitudes toward medically assisted dying. In addition, personal experiences such as the loss of a loved one highlight the complex interplay of factors that predict attitudes toward medically assisted dying.
Limitations
Despite the key findings, there were several limitations in this study that may have impacted results. Quota sampling, which focused on gender, age, and region, may fail to account for other important variables such as education, income, and marital status, which could potentially affect the research outcomes. This limitation could result in relevant demographic or contextual factors being underrepresented. Although the sample may be representative within each age group, generalizability to the broader population is limited. Furthermore, the panel-based design of this study poses an additional limitation to generalizability, as only panel members were eligible to participate, which may lead to potential sample bias.
The relatively modest Nagelkerke R2 values (7.2% for attitudes and 6.6% for willingness to support) suggest that while these factors are significant, they explain only a small portion of the variability in attitudes, indicating that other unmeasured factors may also play a crucial role. One such variable could be religiosity, which has been identified as an important predictor in attitudes toward medically assisted dying.
Future research directions need to focus on qualitative studies to gain a deeper understanding of the underlying factors, motivations and personal experiences that shape individuals’ attitudes and decision-making processes in relation to medically assisted dying.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Slovenian Research and Innovation Agency, under grant number J5-3113.
Ethical Statement
Author Biographies