
Abstract
People living with cancer may experience death anxiety and depression which may impact their experience of posttraumatic growth (PTG). Social support is a psychosocial resource that protects against negative psychological outcome. Although a direct association among these variables exist, little is known about their interactive effect. Dwelling on the buffering hypothesis, this study examined the role of social support in the association of death anxiety and PTG. We further investigated whether depression-PTG relationship would be moderated by social support. Cancer patients (N = 412) were randomly selected from two healthcare institutions. Participants completed relevant self report measures, and data were analyzed using Hayes PROCESS macro for SPSS. Results showed that social support buffered the effect of death anxiety on PTG. The relationship between depression and PTG was also moderated by social support. Interventions to facilitate PTG should target social support network of patients due to its potentials in buffering the effect of death-related anxiety and depression on patients’ PTG.
Introduction
The diagnoses and treatment of cancer is one stressful life experience that is known to potentially result in the development of mental health problems including posttraumatic stress disorders symptoms (PTSD) (Mitchell et al., 2023), and suicide ideation (Chen et al., 2024). However, cancer may also positively impact the lives of majority of patients through a process called Posttraumatic growth (PTG). PTG represents a “positive psychological change that occurs as a result of the struggle with highly challenging life circumstances”, and these changes are known to occur in many areas of the individuals’ life such as the patient’s ability to identify new possibilities, relate to others very well, show more appreciation of life, increased personal strength, and spiritual change (Leong Abdullah et al., 2015; Ma et al., 2022). Previous research has established the existence of PTG among cancer patients (Aliche, 2022; Feng et al., 2024; Leong Abdullah et al., 2015; Ma et al., 2022; Ning et al., 2023). There is the need to identify specific risk and protective factors for the development of PTG among cancer patients. Identifying these factors helps researchers to develop empirically informed interventions for the promotion of health and wellbeing of patients. Therefore, the present study aimed to examine the combined roles of death anxiety, depression and social support in PTG among cancer patients.
Many people who are diagnosed with cancer often undergo certain existential crisis arising from death anxiety (Hong et al., 2022). Death anxiety is referred to as a chronic or persistent fear and worry about one’s own death (Aliche et al., 2023; Tomás-Sábado et al., 2005). Death anxiety is a natural part of the human experience, but this anxiety can be heightened in those with a chronic health condition (Natalie, 2019). According to Tomás-Sábado et al. (2005), death anxiety may occur in various forms such as externally generated death anxiety, death acceptance, death finality, and thoughts about death. Research has shown that among people with chronic illness, death anxiety was linked to poor health-related quality of life (Aliche et al., 2023), but for the association between death-related anxiety and PTG, findings have been quite inconsistent. Some studies have found a positive relationship (Alkan et al., 2020; Leong Abdullah et al., 2015; Natalie, 2019), others reported a negative relationship (Park & Im, 2021), and also a non significant relationship has been observed (Xiao et al., 2022). More research is needed to understand the reason for the inconsistent results particularly among cancer patients. There is the possibility that the effect of death anxiety on PTG may be moderated by some other factors (Aliche et al., 2023; Long et al., 2021), and social support has been proposed to be a potential candidate in that regard (Kagan, 2021). In view of this, we believe that examining the role of social support as a moderator of the relationship between death anxiety and PTG would help to identify subsets of patient whose PTG might not be severely affected by the experience of death anxiety.
Research has also established that depression is a very common psychological consequence prevalent among cancer patients (Javan Biparva et al., 2023; Long et al., 2021). Higher depressive symptoms in cancer patients have been associated with over 25% higher mortality rate, a lower recovery rate, and the development and maintenance of other psychological problems including increased pain sensation, symptoms of posttraumatic stress disorder, and poor quality of life (Ardebil et al., 2023; Unseld et al., 2021). Meanwhile, findings on the association between depression and PTG have been contradictory (Kleim et al., 2009). There is evidence of a negation association between depression and PTG (Long et al., 2021; Palmer et al., 2016), a non significant association (Milam et al., 2004; Vaughn et al., 2009), and a curvilinear relationship (Kleim et al., 2009; Xu et al., 2018). Thus, Wang et al. (2014) has proposed that social support may be an important factor that could potentially moderate the relationship.
Social support refers to the provision or a persons’ perception of certainty of accesses to important non-remunerative material and emotional assistance from others or group (Ning et al., 2023). This kind of support can come from family members such as parents or siblings, friends, or others including healthcare providers who play significant role in the health and recovery of the patients (Bibi & Khalid, 2020). Social support plays a critical role in improving quality of life and PTG among cancer patients (Ma et al., 2022; Ning et al., 2023).
Crucially, we proposed that greater perception of social support may buffer the effect of death anxiety and depression on PTG among cancer patients. According to the buffering hypothesis, social support can help individuals overcome stressful or negative life experiences (Alloway & Bebbington, 1987). This model posits that social support buffers or protects people from the possible negative outcomes after experiencing some kind of negative or stressful life events. Certain negative experience such as death anxiety and depression could impact negatively on the patients’ ability to function optimally and cope effectively with their illness. However, having adequate social support following cancer diagnosis may help prevent patients from experiencing heightened death anxiety and symptoms of depression. In other words, the buffering effect of social support also suggests that, unlike low social support, a strong social support from different sources such as the family, friends and significant others can help alleviate the negative psychological impact of death anxiety and depression on PTG among cancer patients (Alloway & Bebbington, 1987). Although this postulation is yet to be examined in the literature, previous studies revealed that higher perceived social support has consistently play a key role in alleviating death related anxiety (Bibi & Khalid, 2020; Huang et al., 2022; Khodarahimi et al., 2021), and reduced symptoms of depression in cancer patients (Onyekachi et al., 2023; Wondimagegnehu et al., 2019; Zamanian et al., 2021). This suggests that higher social support can improve a successful psychological adjustment to cancer diagnosis and treatment. Individuals with higher social support usually report higher PTG (Aliche et al., 2019; Feng et al., 2024; Ma et al., 2022), and studies have identified social support as a robust moderator of the association between adverse psychosocial antecedence and mental health outcomes. For instance, Kagan (2021) found that higher social support moderated the relationship between death anxiety and psychological distress among Israeli nurses. Among adult survivors of Wenchuan earthquake, Xu and Wei (2023) found social support as a moderator of the relationship between anxiety and depression. Further evidence has revealed the moderating role of social support in the association between depressive symptoms and quality of life outcomes of breast cancer survivors (Huang & Hsu, 2013), and the relationship of depression and anxiety for gastric cancer patients and their family caregivers (Jeong & An, 2017), and also the association between depression and stress (Shi, 2021). Social support moderated the association between negative life events and depression in adolescence (Miloseva et al., 2017), the relation between childhood trauma and prenatal depressive symptoms in adolescent mothers (Nowak et al., 2022), and the relationship between loneliness and depression (Son et al., 2022). Lastly, Rubio et al. (2020) found social support and substance use as moderators of the relationship between depressive symptoms and suicidal ideation in Adolescents. Considering the psychological impact of cancer on the patients’ wellbeing, and the well established positive effect of social support in PTG of cancer patients, it has become very imperative that researchers examine whether cancer patients’ perceived social support would moderate the association between death anxiety, depression and PTG.
The Current Study
Research has reported contradictory finding on the association of death anxiety and PTG, as well as the association of depression and PTG. Social support in an important environment factor that may offer a better understanding of these findings. Having been identified as a protective factor especially during life crisis, social support may buffer the impact of death anxiety and depressive symptoms on PTG among cancer patients. As far as it is known in literature, there is no current research exploring the moderating role of social support in the relationship between death anxiety, depressive symptoms and PTG among cancer patients. The exploration of this moderation effect would not only help to understand patients’ personal experiences in coping with cancerous disease, but also would help inform adequate psychological interventions targeted towards promoting PTG among cancer patient. Therefore, the goal of this research is to examine whether social support would moderate the association between PTG and (1) death anxiety, and (2) depression. Based on previous studies, we hypothesized that among cancer patients, social support would moderate the relationship between PTG and (1) death anxiety and (2) depression (see Figure 1). Conceptual model of social support moderating the association of death anxiety, depression and PTG.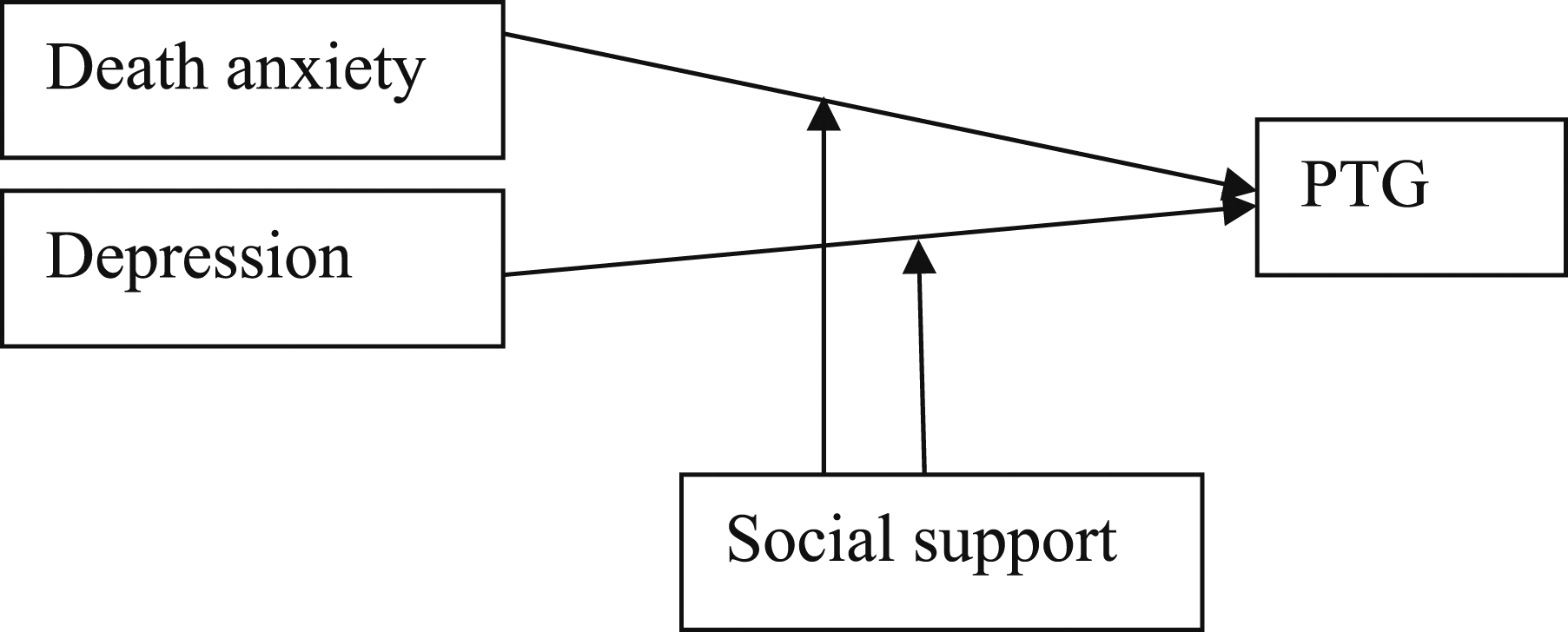
Materials and Methods
Participants
Participants included a random sample of 412 cancer patients drawn from the oncology outpatient unit of two tertiary healthcare institutions. Eligibility criteria for participation included (1) adults (>18 years), (2) diagnosed with cancer for at least 1 years ago before the present study, (3) able to read and understand English language at least at the high school level (4) must have completed active medical treatment (e.g., radiotherapy or surgery) and is currently visiting the hospital for routine medical check-up as an outpatient. (5) must not be taken any antipsychotic medication as at the time of this study (6) not diagnosed of any neurological disorders, major co-morbidities, psychiatric conditions, or any other condition that could affect the quality of their responses.
Results showed that the mean age of the participants was 40.35 years (SD = 11.50, ranging from 23 to 67 years). Majority of the participants (70.9%) were females, married (92.2%), and had secondary education (58.7%). In terms of their religious affiliation, most (97.1%) were Christian and unemployed (74.1%). Regarding the type of cancer diagnosed, (38.8%) had breast cancer, (67%) had colorectal cancer, (81.6%) had lung cancer, (13.6%) had cervical cancer, whereas (4.9%) had other kinds of cancer.
Procedure
After obtaining ethical clearance from the institutional research ethics committee of the facility where the study was conducted, the last author recruited and trained 4 research assistants for the study. They approached the participants at the oncology outpatient unit of the hospitals while participants were waiting to consult with their doctor. They explained the purpose of the study to the participants, and verbally obtained informed consent. Those who were available, willing and verbally consented to engaging in the study were selected. The questionnaires were administered to those who met the inclusion criteria for participation. The data collection lasted for a period of five months (August, 2023-December, 2023).
Measures
Death anxiety was assessed using the 17-item Death Anxiety Inventory–Revised (DAI-R; Tomás-Sábado et al., 2005). The DAI-R has four dimensions which included: death acceptance, externally generated death anxiety, death finality, and thoughts about death. The items (e.g., ‘I think I am more afraid of death than most people”) are rated on a 5-point scale ranging from 1 = (strongly disagree), to 5 = (strongly agree) with higher score representing greater death anxiety. The inventory has good reliability and validity estimates, with an internal consistency reliability coefficient value of 0.92 (Tomás-Sábado et al., 2005). There is evidence of good psychometric properties of the scale among Nigerian population with chronic illness (Aliche et al., 2023). In this study, the DAI-R was used as a unidimensional scale with the internal consistency Cronbach’s alpha of 0.81 obtained.
Depression was measured using the 11 item Iowa form (Kohout et al., 1993), a shorter version of the Centre for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977). The items (e.g. “In the past week, I felt depressed,”, “In the past week, I enjoyed life” (reverse coded) were rated on a 3-point scale ranging from 1 = rarely or almost none of the time, to 3 = most or all of the time), with total score ranging from 11 to 33. The scale has demonstrated good validity and internal consistency (a = 0.85) among Nigerian population (Onyekachi et al., 2023). In the present study, an internal consistency reliability coefficient value of 0.81 was obtained.
Social support was measured using the 12-item Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) that assesses perceived support from different sources such as the family, friends, and significant others. The items (“I get the emotional help and support I need from my family”) are scored on a 5-point Likert-type structure ranging from 1 = strongly disagree; to 5 = strongly agree. The internal consistency of MSPSS (Cronbach’s alpha) was .89 (Zimet et al., 1988). The MSPSS has recorded good psychometric properties among Nigerian sample of trauma survivors (Aliche et al., 2019). In the present study, the internal consistency reliability coefficient Cronbach’s alpha of 0.82 was observed.
Posttraumatic Growth was measured using the original 21 items posttraumatic growth inventory (PTGI; Tedeschi & Calhoun, 1996) that assesses the positive psychological changes that may occur following stressful life event. The PTGI has 5 subscales for example, relating to others, new possibilities, appreciation of life, personal growth, and spiritual change. The items are scored on a 6-point Likert-type scale ranging from zero = not at all, to 5 = very high degree, with higher score suggesting higher levels of PTG. The PTGI has excellent psychometric properties (Tedeschi & Calhoun, 1996), and has also demonstrated same among Nigerian sample of cancer patients (Aliche, 2022). In the present study, a Cronbach’s alpha coefficient value of 0.80 was obtained.
Statistics Analysis
We carried out a preliminary analysis using descriptive statistics. Pearson’s correlation was employed to examine the association between the demographic variables (e.g., age, gender, education and marital status) and the main study variables. The Hayes PROCESS macro for SPSS Model 1 was used in testing the moderation hypothesis (Hayes, 2018). All the data analysis was carried out using the Statistical Packages for Social Sciences (SPSS), version 23.
Results
Correlations Among the Study Variables.
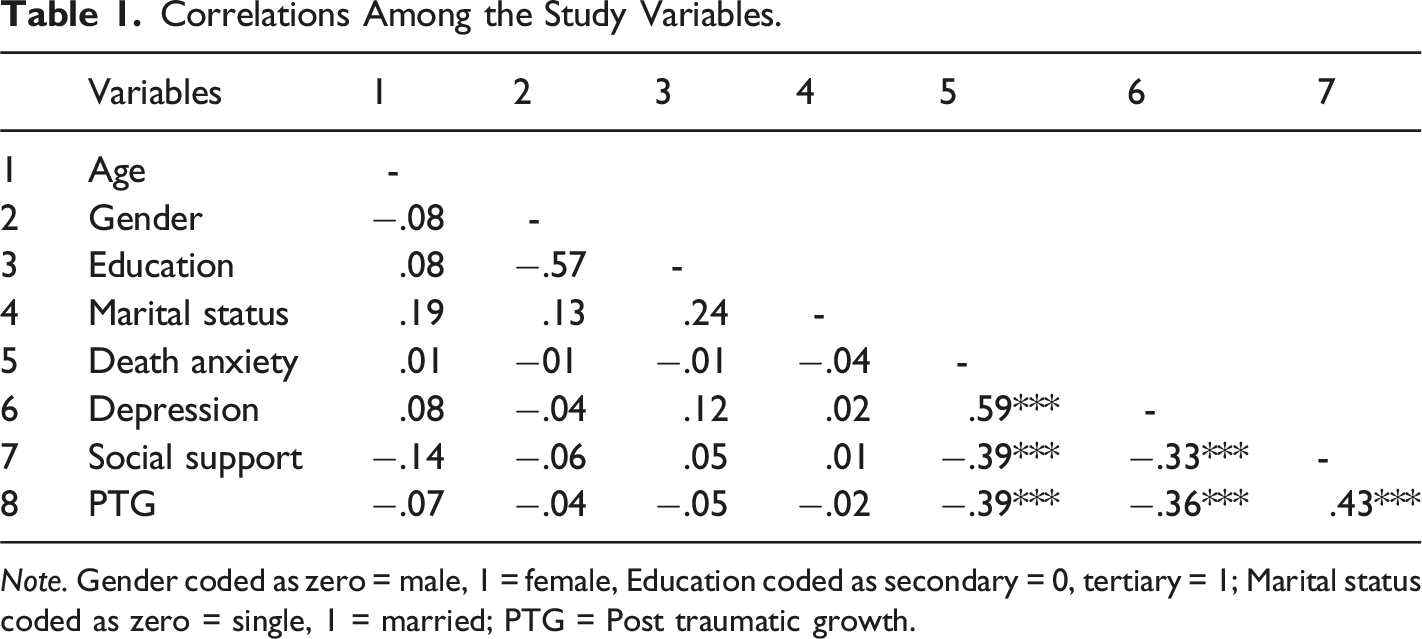
Note. Gender coded as zero = male, 1 = female, Education coded as secondary = 0, tertiary = 1; Marital status coded as zero = single, 1 = married; PTG = Post traumatic growth.
Moderation Analysis
Hayes PROCESS Regression results on the Moderating Effect of social Support Between death Anxiety, depression and PTG.
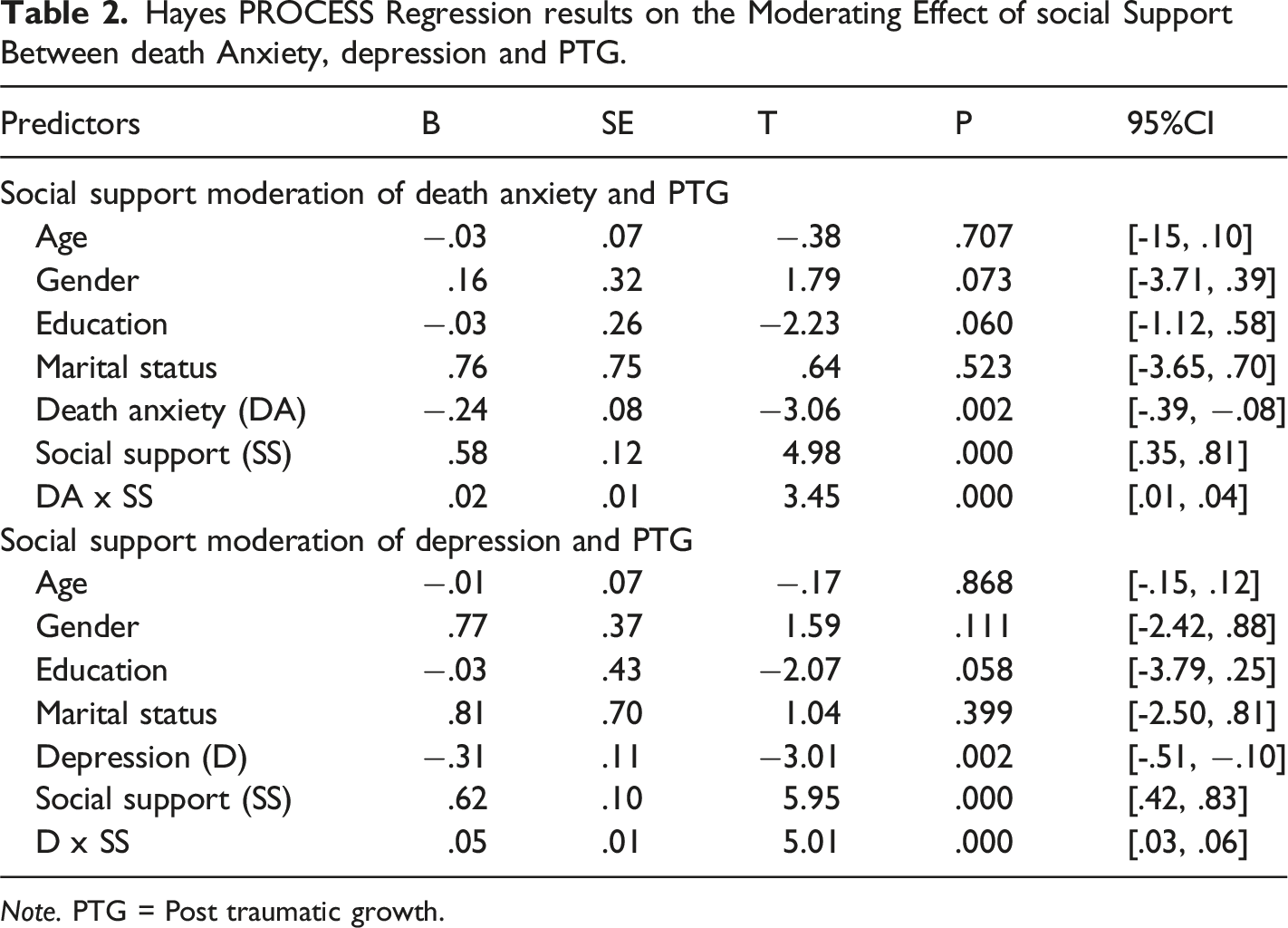
Note. PTG = Post traumatic growth.
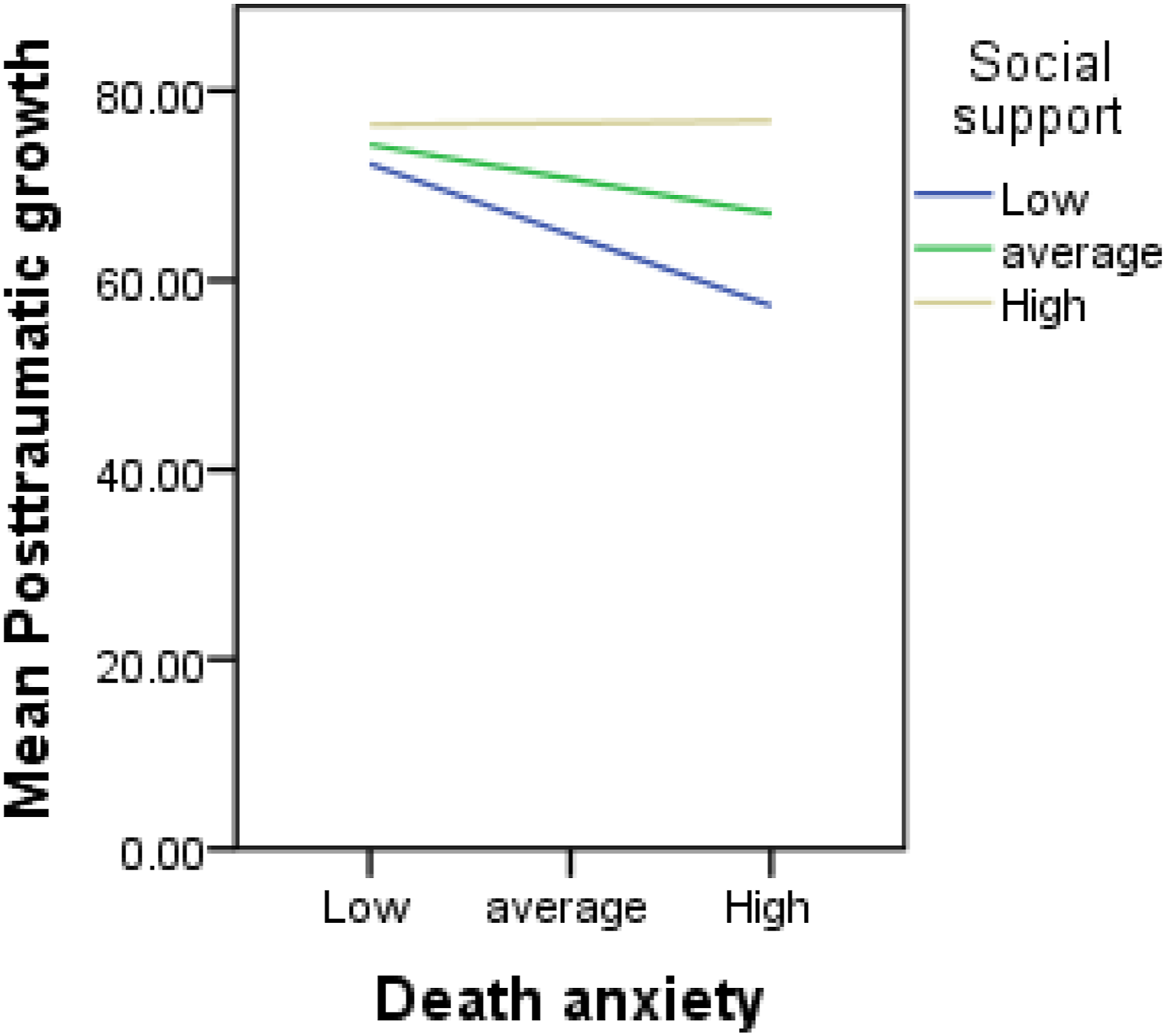
Showing the moderating role of social support between death anxiety and post traumatic growth.
When we examined the moderating role of social support in the association between depression and PTG, results revealed that PTG was not significantly associated with age (B = −.01, p > .05), gender (B = .77, p > .05), education (B = .03, p > .05) and marital status (B = 81, p > .05). However, results showed that depression was negatively associated with PTG (B = −.31, p < .01). Social support was positively associated with PTG (B = .62, p < .001), and moderated the association between depression and PTG (B = .05, p < .001). The slope of the interaction (Figure 3) indicated that depression was associated with lower levels of PTG only at low and average, but not at high levels of social support. Showing the moderating role of social support between depression and post traumatic growth.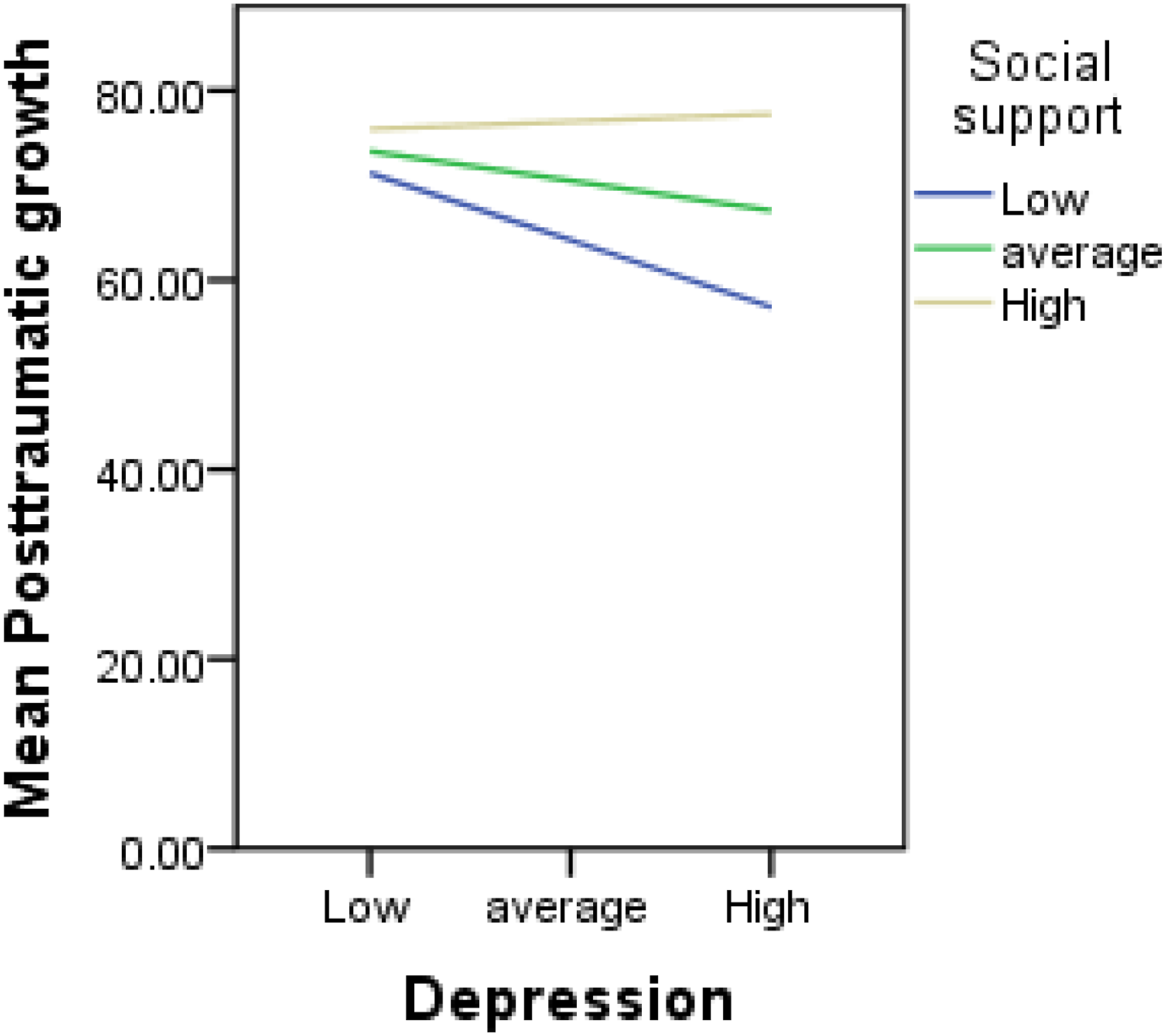
Discussion
The current study investigated the role of social support as a moderator of the relationship between death anxiety and PTG. We further examined whether social support could moderate the association of depression and PTG in a sample of cancer patients. Being the first research, to our knowledge, to examine the association among these variables, results showed that social support moderated the association between death anxiety and PTG, such that death anxiety was associated with lower levels of PTG only among cancer patients with low and average levels of social support, but not among those with high levels of social support. This suggests that higher social support buffered the effect of death anxiety on PTG among cancer patients, consistent with the affirmation theory of this research: the buffering hypothesis (Alloway & Bebbington, 1987). Among individuals diagnosed with cancer, death anxiety may involve an overwhelming mortality-related thoughts, worries and feelings which are quite disturbing and distressing to the individual due to their health condition (e.g., “I frequently think of my own death”; “It annoys me to hear about death”). As a result, patients with higher score on death anxiety may wish to avoid objects, places or situations that reminds them of their death (e.g., I get upset when I am in a cemetery). Such individual patients may experience poor quality of life (Aliche et al., 2023) and lower levels of PTG (Park & Im, 2021). Although the diagnosis of cancer and the awareness of a protracted period of its management is potentially one existential crisis that is capable of provoking unpleasant feelings of helplessness, hopelessness and a sense of mortality, our findings have shown that cancer patients who have greater perception of social support from different sources are able to navigate through these existential problems and cope adequately with their illness in the form of PTG (Kagan, 2021).
A strong social support is the most important protective factor during stressful life challenges and cancer patients with higher perceived social support are aware that they are not alone in their battle for survival from cancer (Feng et al., 2024). Adequate social support from a family member and friends, particularly in a collectivist society, provides a sense of security and safety among people who survived a traumatic event (Aliche et al., 2019). When confronted with a chronic illness, support from these sources can provide the opportunity for patients to express their emotional feelings, worries, and concerns which will in turn benefit from the advice and encouragement from others. Rather than engaging in death-related thoughts, such encouragement can enable patients to easily engage in positive reappraisal of their health condition which helps to increase their optimism and hope for survival, and for a better future (Feng et al., 2024). In addition, offering of assurance and the provision of sincere and accurate information to patients by healthcare professionals such as doctors, nurses, and clinical psychologists who constitute the significant others dimension of social support could be an important source of social support capable of protecting cancer patients from increased thoughts about death and dying (Huang et al., 2022; Khodarahimi et al., 2021). With this kind of support, cancer patients may be more willing to learn about their illness through asking questions during their retinue medical check-up and seeking further knowledge on the most appropriate lifestyle henceforth in order to facilitate treatment, recovery and PTG (Feng et al., 2024; Ma et al., 2022). What is more? There is nothing more than to posit that the findings of this study is in agreement with those of previous studies (Kagan, 2021; Nowak et al., 2022; Son et al., 2022) more generally on the role of social support in moderating the relationship between adverse psychosocial factors and mental health outcome. Therefore, patients with high death anxiety may leverage on support from the family, friends and significant others as a coping strategy to remain in an optimal level of activation which is very critical for the development of PTG.
Another interesting finding of the current study was that social support moderated the relationship between depression and PTG such that depression was associated with lower levels of PTG only among cancer patients with low and average levels of social support, but not among those with high levels of social support. This finding is consistent with previous related studies on the beneficial effect of social support in decreasing the effect of depression on mental health outcome (Huang & Hsu, 2013; Jeong & An, 2017; Rubio et al., 2020; Shi, 2021). The diagnosis and treatment of cancer is a negative life experience that is prominently very distressing enough to trigger unpleasant emotions including sadness, emptiness and hopelessness (Jeong & An, 2017). However, the finding of this study has revealed that those with higher perceived social support adjusted very well with these negative emotions and experienced growth in many areas of their lives.
The buffering effect of social support found in the present study suggests that adequate social support may act as inter- and intrapersonal resources to adapt and cope with stressful life conditions (Huang & Hsu, 2013). In other words, this finding indicates that not every cancer patient with depressive symptoms may necessarily experience low levels of PTG but rather, there is diversity of PTG experiences depending on levels of perceived social supports. Adequate social support may operate in such a way that helps influence stress appraisal in stressful situations, and can potentially alleviate the negative emotions caused by a chronic illness. Previous studies demonstrated the potency of high social support in promoting the health of cancer patients by buffering the effect of depressive symptoms (Huang & Hsu, 2013), facilitating the development of PTG (Aliche et al., 2019), and helping people to rebuild their sense of wellness (Huang & Hsu, 2013). Therefore, the finding that social support moderated the depression-PTG relationship has provided preliminary evidence that social support from the family, friends, and significant others could protect cancer patients from the negative impact of depression on PTG.
There are notable limitations of this study that deserve to be mentioned. The adoption of a cross sectional research design and self report measures which may inherently precluded the assessment of causal inferences. The use of experimental or longitudinal design may produce result with higher internal vitality. The participants in this study were drawn from a developing country with a collectivist culture. This may have some implications for the role of social support in moderating the effect of death anxiety, and depression on PTG. We are yet to confirm whether research from individualistic culture would find similar results. However, a major strength of this study is the utilisation of moderately large sample size and random sampling method which helps to increase the reliability of the findings.
Conclusion
The present study remains the first research to examine the role of social support as a moderator of the relationship between death anxiety, depression, and PTG among cancer patients. The findings have contributed to the broader literature in oncology by revealing the protective role of social support in buffering the effect of death anxiety on PTG among cancer patients. Additionally, this research also added new knowledge by revealing that social support can decrease the effects of depression on PTG among cancer patients. Based on these findings, the researchers are proposing for a holistic treatment and care for cancer patients. Any psychological interventions aimed at improving PTG of cancer patients should begin with a comprehensive assessment and monitoring of patients’ level of social support particularly among those with high score on death anxiety and depression. In this sense, clinical effort should then consider promoting social support network of patients, as this would help decrease the negative impact of death anxiety and depression on wellbeing and PTG.
Footnotes
Acknowledgements
We are grateful to all the participants who volunteered to take part in this study. It would not have been possible to conduct this study without their co-operation. We also thank all our research assistants for their assistance and cooperation all through the period of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.