
Abstract
The study aimed to evaluate the effect of participating in bereavement support groups on mental well-being and levels of grief and to gather information about participants´ experiences of participation. The programme consisted of six sessions over six weeks. Data were collected with the Warwick Edinburgh Mental Well-Being Scale (WEMWBS) and the Adult Attitude to Grief scale (AAG) as well as demographic and open-ended questions. 64 bereaved spouses returned at least parts of the study´s questionnaires before participating in the programme while 39 returned the complete WEMWBS and 36 the complete AAG both before and after participation. Most participants were women >60 years old. Participation in the programme resulted in a significant increase in perceived mental well-being and significantly lower levels of vulnerability in grief. Responses to open-ended questions revealed both positive and negative experiences. A lowered WEMWBS score and a relatively high AAG underscore the importance of providing services to the recently bereaved. Routine screening for complicated grief before participating in the bereavement support group sessions is recommended.
Introduction
Grief is a natural reaction when losing a loved one. Most individuals recover within a year after a loss (Szuhany et al., 2021), however, a subset (7–10%) of bereaved individuals experience an extension of the grieving process and may develop a prolonged grief condition (Lundorff et al., 2017; Nakajima, 2018; Shear, 2012).
The purpose of bereavement support groups (BSG) is generally to offer emotional support and to provide information to those who have experienced loss (Schopler & Galinsky, 1993). Research evidence for this kind of support is limited and has been inconclusive due to the many different types of outcomes being evaluated and the different research designs used (Baretone et al., 2018; Grost et al., 2016; Jordan & Neimeyer, 2003). Bereavement support groups also vary in structure and content and thereby the potential they may have to offer effective support (Baretone et al., 2018). Questions have also been raised about whether the right aspects of taking part in BSG are being explored (Dyregrov et al., 2013; Harrop et al., 2020), and whether researchers are measuring outcomes that capture the true experience of participation. Therefore, more research is needed (Dyregrov et al., 2013; Näppä & Björkman-Randström, 2020; Näppe et al., 2016); both qualitative and quantitative.
Qualitative studies in this field have aimed to gain a deeper understanding of different elements of this experience perceived by the bereaved taking part in BSG programms in various settings. A variety of positive impacts have been reported in qualitative studies (Harrop et al., 2020). Some studies, however, have reported negative aspects related to participation. Dyregrov and colleagues (2013; 2014) studied grief group participants´ experiences, benefits, and satisfaction with the group sessions. The authors mentioned various positive experiences from grief group participants including the opportunity to meet with others who have also experienced loss and to share with them their emotions, thoughts, and hope. One of the most critical aspects of negative experiences mentioned by the participants was the distress felt from listening to other participants’ loss narratives.
When grief processes become prolonged and individuals have difficulty accepting the loss of their loved one and adapting to life without them resulting in persistent yearning, they may experience complicated grief (Shear, 2010; Wilson et al., 2020). Dyregrov and colleagues concluded that a lack of screening before taking part in support groups could be a risk for those with complicated grief. Screening could offer early identification of individuals who are likely to experience complications during bereavement. The importance of screening has been emphasized, so that appropriate treatment may be offered to those in need of specific support (Patel et al., 2019).
Findings from a recent study (Näppä & Björkman-Randström, 2020) on significant other´s experiences of participation in BSG offered by a palliative care team, indicated that BSG had the potential to mitigate grief, however not all participants experienced less grief. Harrop et al., (2020) emphasized using results from qualitative studies to identify potential outcomes of interest. This aligns with what Nåppe et al. (2016) reported, emphasizing the importance of more qualitative research to gain a deeper understanding of the benefits experienced. Utz et al. (2013) also concluded that including qualitative reports when evaluating grief support programms was necessary. Additional quantitative research is also needed to determine in more detail the significance and value of this type of support (Harrop et al., 2020).
Based on the findings of a DELPHI study where core outcomes (“Ability to cope with grief” and „Quality of life and mental well-being”) were identified (Harrop et al., 2020) we decided to measure the effects of participation in support groups by following these reported recommendations. Also, to use validated measures to cover these outcomes, we therefore decided to use the well-being-specific tool: Warwick-Edinburgh Mental Well-being Scale (Tennant et al., 2007) and the grief-specific tool: Adult Attitude to Grief Scale (Machin, 2014; Sim et al., 2013).
Due to the findings of a recent systematic review on sleep disturbances in bereaved adults, which reported a gap in the literature related to these problems and how they were dealt with (Chirinos et al., 2019; Godzik, 2020), we also added questions related to sleep disturbances.
The aims of this study were, therefore, to determine if participation in BSG affected bereaved spouses’ perception of mental well-being and levels of grief, as well as gather information about participants´ experience of participating in BSG; that is what participants perceived as helpful or not helpful when participating in the BSG. Accordingly, the research hypotheses and research questions were as follows:
Bereaved spouses who participate in the BSG programme will report significantly higher mental well-being levels at the end of the programme compared to the pre-programme.
Bereaved spouses who take part in the BSG programme will perceive significantly lower levels of vulnerability in grief (reflected in lower levels of vulnerability scores) compared to the pre-programme.
Research Questions
1. What are the positive aspects of participating in the BSG programme experienced by bereaved spouses? 2. Are there negative aspects of participation in the BSG programme experienced by bereaved spouses? 3. Are bereaved spouses in the BSG programme experiencing sleep disturbances and what methods do they, if any, use to improve their sleep?
Methods
Study Design
A quasi-experimental one-group pre-test/post-test design was employed to determine the effect of a group-based intervention for recently bereaved spouses on mental well-being and levels of grief. Furthermore, content analysis was used to analyze responses to open-ended questions about the experience of participating in the BSG programme collected post-test. Power analyses were done before the study using a computer-based power analysis program. Taking a 95% confidence interval and 85% test power into account, as well as an α value of 0.05, the sample size needed for comparison was calculated as 36 individuals (Rosner, 1995). Considering the possibility of the dropout of participants, we aimed to recruit about 90 participants.
Participants and Data Collection
People that had signed up for a 6-week BSG programme for bereaved spouses were approached by the personnel of a non-profit organization that conducted the bereavement support groups and offered participation in the study. The sample was limited to adults (> 18 years old) who could read and write Icelandic. Participation in the study was voluntary. If participation was agreed upon, potential participants received an introduction to the study and the study’s materials/questionnaires, with a return envelope, by mail, before starting the support group course and after the sixth session. They were asked to bring the completed questionnaires in a sealed envelope to the first group session and leave it with the personnel in the reception. Data collection began in the fall of 2020 and ended in the spring of 2022.
Data Collection Tools
Mental Well-being
To determine mental well-being, the Warwick-Edinburgh Mental Well-being Scale (WEMWBS) (Tennant et al., 2007) was used. The WEMWBS was developed to measure mental well-being in general populations and to evaluate the effect of various projects and policies to improve mental well-being. The scale has 14 items, with 5 response categories, summed to provide a single score. The items cover both feeling and functioning aspects of mental well-being. Upon answering, people are asked to look towards mental well-being for the last 2 weeks. Sample items include “I have been feeling optimistic about the future”, and “I have had enough energy to spare”. The scale has been shown to detect deterioration or improvement in clinical settings, schools, and workplaces both among groups and at an individual level. The scores range from 14 to 70 with higher scores indicating increased positive mental well-being (Stewart-Brown et al., 2011). The WEMWBS has been translated and back translated into Icelandic.
Levels of Grief
To evaluate levels of grief, the Adult Attitude to Grief (AAG) Scale (Machin, 2014; Sim et al., 2013) was used. The AAG scale is a validated tool consisting of nine statements that can provide information on reactions and coping responses to loss being experienced at an individual level (Machin et al., 2015). The scale can also identify an additional component which is vulnerability (Sim et al., 2013), and is used in this study to assess levels of grief and changes in vulnerability category scores. It has three subscales (each of three items); Feeling of being overwhelmed; Loss of control; and Resilience. Statements are rated on a five-point Likert scale, with options ranging from “strongly agree “(4) to “strongly disagree “(0). Each subscale score is formed by taking the sum of the three items in the given subscale and an overall Index of Vulnerability (IOV) is formed by adding the overwhelmed, control, and “reversed” resilience scores together. The AAG scale gives an overall index (optimum cut-off scores) of different levels of vulnerability and is calculated by summing the subscale scores (IOV: 0–20 = low vulnerability, 21–23 = high vulnerability, and 24–36 = severe vulnerability). The potential of the AAG scale to be a grief-specific instrument has been recognized by CORE IMS (Clinical Outcomes in Routine Evaluation Information Management Systems) (Machin et al., 2015). The AAG scale has been translated and back translated into Icelandic.
Demographic Questions, Questions About Sleep Disturbances, and Social Support
The respondents also answered background questions about gender, age, length of time leading up to the death of a spouse, and length of time since the loss. Furthermore, based on a literature review the researchers prepared questions about sleep disturbances, (problems falling asleep, shorter sleep duration – awakening early in the morning, frequent awakenings during sleep) and social support. These questions were only asked before starting the BSG programme.
The Intervention – Programme Content
Each BSG participant had the opportunity to meet once a week for six weeks. Every session lasted 90 min and had a predefined theme: (a) introductions/sharing stories (b) expression of thoughts and feelings, (c) responses from family/friends and others, (d) coping with difficult emotions (e) living with the loss (f) looking back and moving forward, “what have we learned.”, based on “Models of adult bereavement support groups” (Sherman, 2012).
The BSG programme was provided by a non-profit organization and the groups were led by two group leaders (with varied occupational backgrounds; theologist, RN) in each group session. The role of the group leaders was mainly to listen and facilitate discussion and to allow everyone to express their feelings and concerns.
Data Analysis
The Statistical Package for Social Sciences (SPSS, v. 23.0) was used for data analysis. Descriptive statistics were used to describe the frequencies and distribution of answers. Chi-square tests were performed to determine differences between participants who only answered the questionnaires before the BSG (Group 1) and those who answered both before and after participation in the BSG (Group 2). Independent t-test calculations were performed to determine differences in well-being (WEMWBS scores) and levels of grief (AAG scores) between participants in Group 1 and Group 2 and between those who experienced time of loss within the last year compared to those who had experienced the loss of a spouse more than one year ago. Also to measure differences in mean scores of well-being and levels of grief of those who experienced sleep problems and compare to those who did not. Paired t-tests were used to measure differences in mean scores between pre-and post-test scores on the study´s main variables WEMWBS and AAG. Only complete (no missing values) questionnaires were used in the t-test calculations. Significance was set at p < .05. Cohen´s d was calculated to estimate effect size (Lakens, 2013). According to Cohen´s criteria, the effect size was considered small if d = 0.20, a moderate effect if d = 0.50, and a large effect if d = 0.80 (Cohen, 1988).
Cronbach´s alpha in this study was 0.93 for WEMWBS and 0.66 for the AAG scale, calculated from completed scales at the start of the study. „Cronbach alpha values are, however, quite sensitive to the number of items in the scale. With short scales (e.g., scales with fewer than ten items) it is common to find quite low Cronbach values (e.g., .5)” (Pallant, 2011, p. 97).
Responses to the open-ended questions were analyzed using a qualitative conventional content analysis (CCA) process (Hsieh & Shannon, 2005), frequently used when analyzing this kind of data. The process begins with identifying text phrases to understand how the individuals describe their experiences. The participants answered a set of questions in writing, and the analysis was performed on these responses in the following steps: At first, all the text responses were read several times by both researchers (ABP, HST), meaning units and codes were developed and codes grouped into categories. The researchers then discussed the categories that emerged when grouping the responses into themes. They also discussed if there were differences in their grouping. An agreement was required of both authors before confirming a theme.
Ethical Considerations
Before conducting the research, ethics committee approval (VSN-20–142) was obtained from the Research Ethics Committee in Iceland. In addition, written consent from the affiliated non-profit organization where the research was conducted was obtained (no number) and permissions for use were obtained from the WEMWBS and AAG Scale owners. The study was conducted by the principles of Helsinki Declarations. All participants were informed about the purpose of the study, and they were also informed of their right to withdraw from the study at any stage.
Results
Demographic Characteristics, Time Leading up to Death, Time since Loss, and Received Support
Age of Participants in Group 1 and Group 2*.
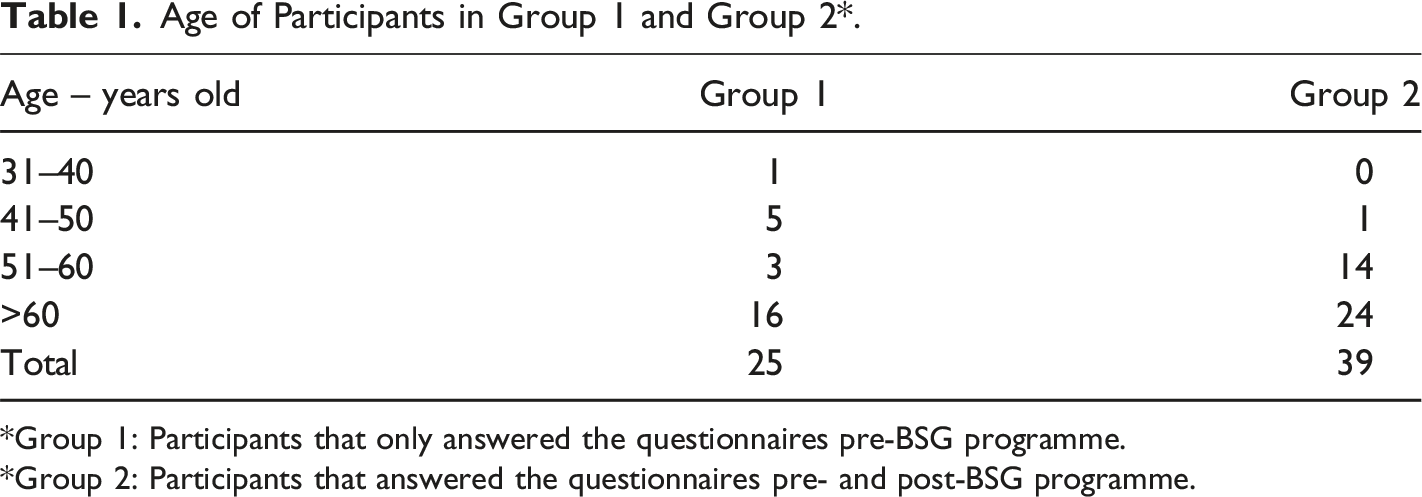
*Group 1: Participants that only answered the questionnaires pre-BSG programme.
*Group 2: Participants that answered the questionnaires pre- and post-BSG programme.
Most of the participants were females (73.4%) over 60 years old (62.5%). The majority (82,5%) of the participants acknowledged that they received support after losing their spouse. Of note, however, is that nine participants (14%) did not respond to this specific question. The support was primarily provided by close friends or family members such as [adult] children.
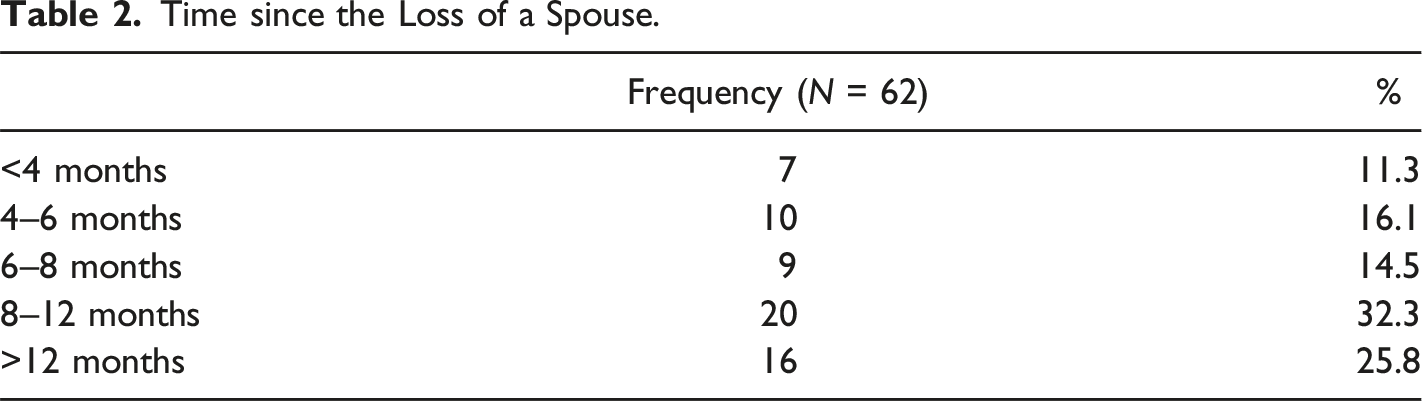
Time since the Loss of a Spouse.
Mental Well-Being
Participants that completed the WEMWBS both before and after the BSG programme were 39. The mean total WEMWBS item score of the participants before starting the programme was M = 46.01 (SD = 10.05), ranging from 24–61. The mean total WEMWBS score after the programme was M = 47.72 (SD = 10.01), ranging from 23–67. The paired sample t-test revealed a significant difference, t (38) = 2.281, p = .028 (two-sided). The effect size as measured by Cohen´s d was d = 0.36 indicating a small effect size. Mean changes in WEMWBS scores were 1.70, with a median of 2, and the most individual change for the better was 13 and 7 for the worse.
Warwick Edinburgh Mental Well-Being Scale Scores.

The hypothesis that bereaved spouses who participate in the BSG programme will report significantly higher mental well-being levels post-intervention compared to pre-intervention is supported.
Levels of Grief
Index of Vulnerability Grouped Into Categories before and after Participation in BSG
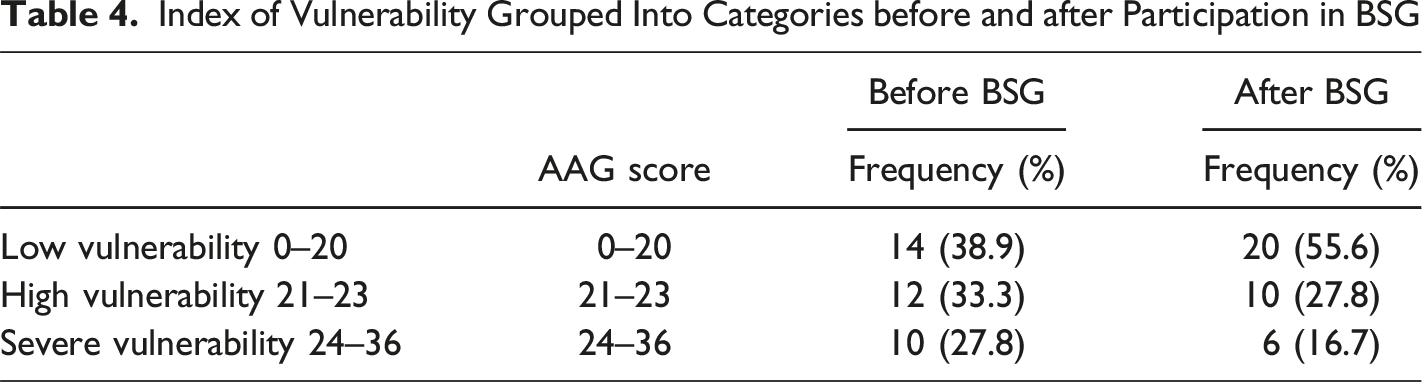
The hypothesis that bereaved spouses who participate in a BSG programme will perceive significantly lower levels of vulnerability in grief post-intervention compared to pre-intervention is supported.
Sleep Disturbances and Resources
Nearly one-third of the general population may experience insomnia (difficulty falling asleep, difficulty maintaining sleep, early-morning awakening) with prevalence rates ranging between 6% to 15% of the population. Complaints of insufficient sleep have a prevalence rate between 20% and 41.7% in the general population (Ohayon, 2011).
Type of Sleep Disturbances Experienced by Participants.
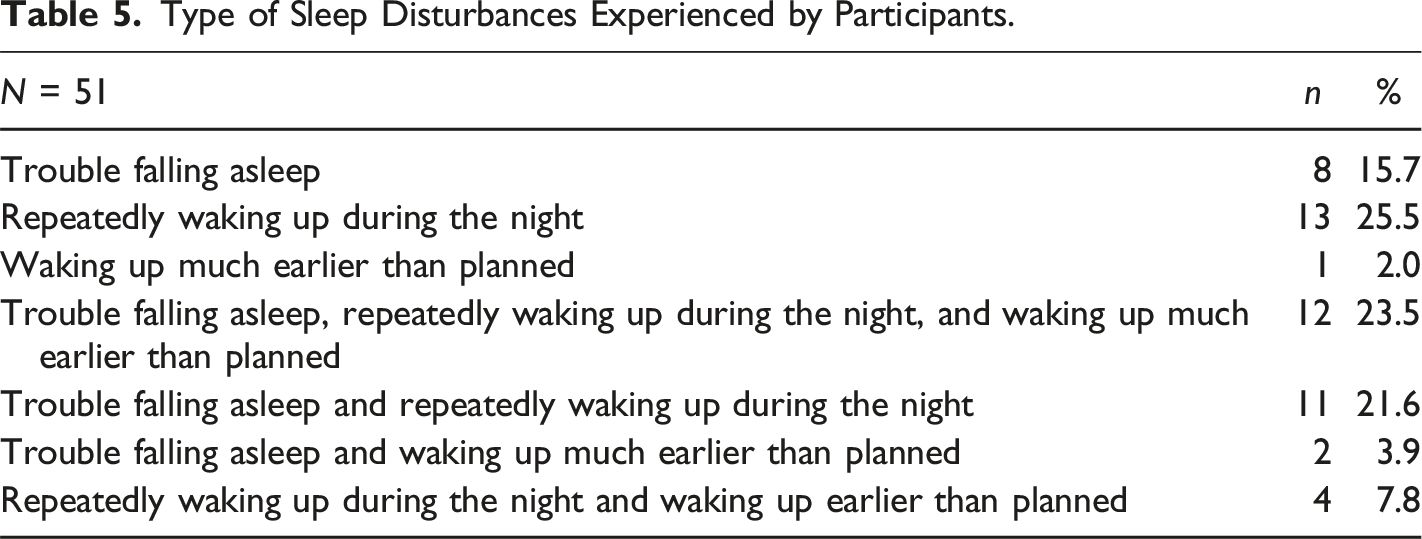
The participants used several different methods to try to improve their sleep, such as reading, exercising, listening to music, relaxation techniques, taking walks, etc. Most used several approaches. About a fifth, 22.2% (n = 14) mention they used sleeping aids/medication; some only occasionally, and then mostly combined with other approaches.
Results from Open-Ended Questions
The data from the open-ended responses was analyzed using a conventional content analysis (Hsieh & Shannon, 2005). After reading the entire narrative data (a) meaning units were developed, (b) codes were developed by using one/two words from the text to name the meaning units, (c) the codes were then grouped based on how they are connected, and categories developed, (d) at last themes were developed by collapsing the categories into smaller groups emphasizing the basic meaning (Hsieh & Shannon, 2005).
Responses to the open-ended questions revealed mostly positive comments regarding participation in the bereavement support groups, however, there were also negative comments reported.
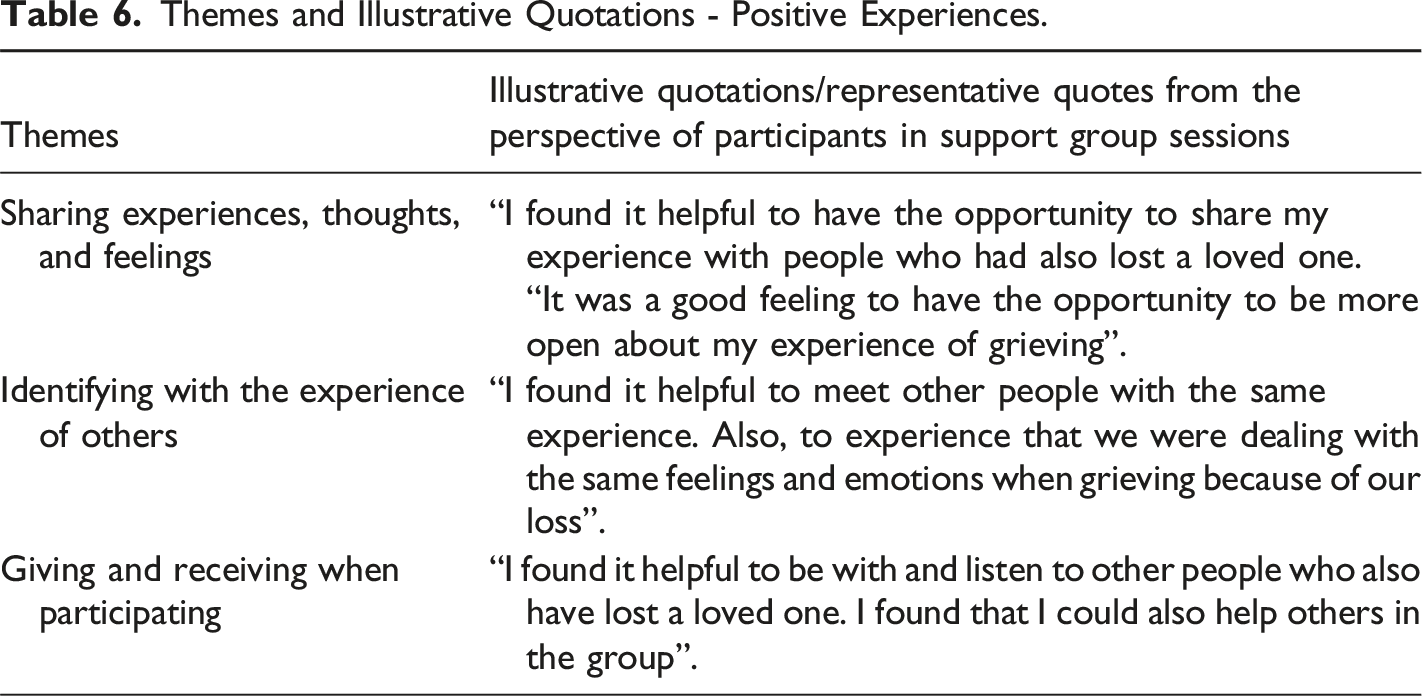
Positive Experiences
Open-ended responses to positive experiences that were identified, were reorganized into three themes: (1) Sharing joint experiences, thoughts, and feelings, (2) Identifying with the experience of others, and (3) Giving and receiving when participating.
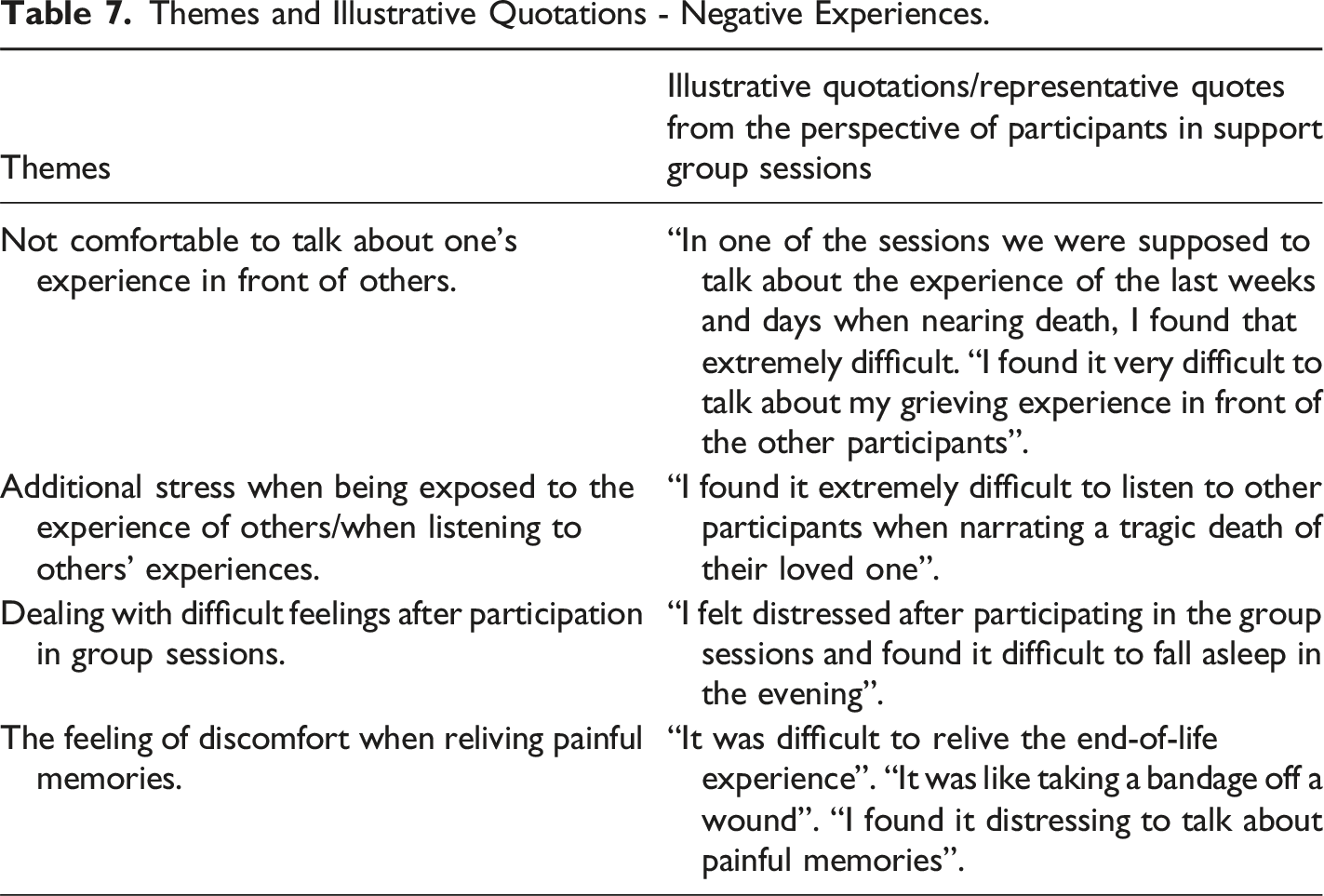
Negative Experiences
Themes and Illustrative Quotations - Positive Experiences.
Themes and Illustrative Quotations - Negative Experiences.
Validity and Integrity of the Procedure
The researchers identified the themes through the conventional content analysis approach and provided information about the study processes to ensure transparency (Cook et al., 2016). The integrity of the data analysis was partially confirmed by the agreement of both researchers regarding the findings through continuous discussions on the answers of the participants (Ingham-Bromfield, 2014). The integrity of the data analysis was further assured by obtaining a consensus among the two researchers when finalizing the themes. To enhance the external validity, direct quotations from participants were included (shown in Tables 6 and 7).
Discussion
This study aimed to determine if participation in BSG sessions affected bereaved spouses’ perception of mental well-being, levels of grief (i.e., levels of vulnerability in grief), as well as gather information about participants’ experience of participating in BSG sessions, that is what participants perceived as helpful or not helpful when participating in the BSG. The findings of a significant increase in mental well-being and decrease in levels of grief at the end of the six weeks as compared to the ones at the beginning are quite important. Due to the period between the two-time points, a direct cause-and-effect relationship cannot be affirmed, however, it indicates that the BSG sessions have a clear impact on well-being and levels of grief, although the findings need to be corroborated within a larger sample. The instruments were chosen because of their ability to effectively capture changes (Machin, 2014; Sim et al., 2013; Tennant et al., 2007)
A noteworthy finding from this study is also that although a significant reduction in perceived vulnerability was found, there were still 16.7% of the participants who expressed a severe level of vulnerability after participating in the BSG sessions. A total of 27.8% reported severe vulnerability at baseline. According to a study conducted by Xiu et al. (2020) which aimed to detect changes in levels of prolonged grief severity in adult spouses following participation in the BSG programme, showed that those who reported high levels of baseline grief scores had elevated risks of symptom recurrence.
Most of the participants in this study were more than 65 years old and it has been emphasized that older adults experiencing grief receive limited attention in healthcare regarding their supportive needs (Gerber et al., 2022). They may be facing various physiological and psychological effects when encountering the death of a spouse, among those sleeping disturbances. The findings in the current study also underscore the importance of discussing sleep and related issues, in the BSG sessions, as well as proven ways to deal with sleep problems, as sleep quality is such an important aspect of well-being. A systematic review by Lancel and colleagues (2020) has pointed out the value of screening for sleep problems among bereaved individuals and the importance of future research in this field.
The qualitative findings suggest several benefits that help explain the impact mechanisms of participation, however also adverse effects that need to be taken into consideration. In the study of Näppä & Björkman-Randström (2020) it was reported that in some cases the participants did not experience less grief after participating in bereavement support groups. The authors also emphasized the uncertainty of the long-term benefit of participation. Johnson and colleagues (2011) found that participants who had been identified with prolonged grief reported less satisfaction with grief group participation and fewer positive effects on quality of life.
An interesting finding from the qualitative data was that there was a considerable overlap between what the support group participants experienced as positive and negative. Participants reported a range of mostly positive comments, but as mentioned adverse experiences were also noted. Those participants thought that they were not benefiting from their participation in the group sessions. Given the potential for these adverse effects, this area should be more thoroughly investigated through regular monitoring and evaluation when offering participation in bereavement support groups. The reasons why some of the participants did not perceive the benefit of participation might be that they are experiencing bereavement difficulties that persist instead of diminishing over time (Lundorff et al., 2017) and this needs to be considered.
Limitations and Strengths
The study is limited to where it was conducted and to participation in bereavement support groups for spouses provided by one non-profit organization. Due to the promise of confidentiality and that the BSG sessions were provided by a third party, knowledge about why those participants answered the pre-BSG questionnaire only is not available. The study was also to some extent conducted during the COVID-19 pandemic. The absence of comparison groups, use of convenience samples, and sample size limit the strength of the conclusions that can be drawn from the study. Unfortunately, a question about the number of BSG sessions (out of six) attended was not included in the post-questionnaire. However, the findings were conclusive.
Regarding questions about sleep, it would have been of value to ask questions about sleep disturbances before the loss of a spouse and to ask about changes in sleep patterns after the loss. Also, the questions about social support and relationships would have needed to be more precise. This study adds to the limited evidence reported in the literature regarding the effect and impact of participation in bereavement support groups. There are nonetheless important aspects from the participant’s experiences of participating in the bereavement support groups that surface and critical issues that need to be taken into consideration. Mental well-being and levels of grief were measured at two time points, before and after participation. The study´s qualitative components provide a deeper understanding of the experience of participation in bereavement support groups. Future studies should focus on utilizing a longitudinal design using the same outcome measures to explore further the bereaved experiences over a considerable time to determine whether the participation helped to ease grief reactions and increase well-being over the long term.
Conclusion
This study provided evidence that those who participated in bereavement support group sessions reported perceived increased mental well-being after the intervention compared to before and perceived levels of vulnerability in grief declined at the same time. The main findings emerging from this study are like those found by Dyregrov and colleagues (2013; 2014), that most participants may benefit from participating in bereavement support groups, however, there are some that experience negative effects and that must be taken into serious consideration, to avoid that those with complicated grief do not experience adverse effects with participation in the bereavement support groups. Leaders of bereavement support groups are therefore challenged to implement methods of screening potential group participants and taking measures to provide the specific help that may be needed. Additionally, to assess participation experience of bereavement support group sessions so that evidence can be used to refine the state of bereavement services.
Footnotes
Acknowledgements
The authors are grateful to the participants of the study, for sharing their experiences, and the volunteers of the non-profit organization who facilitated our data collection.
Author Contributions
Both authors contributed to the design and implementation of the study. ABP supervised the project and drafted the first manuscript. HST performed the statistical calculations. Both authors contributed to the interpretation of the results, prepared the manuscript, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.