
Abstract
The study aimed to examine the moderator effect of organ transplant waiting time on hopelessness and death anxiety. The study was conducted in a descriptive and correlational design with 378 patients on the transplant waiting list (Agust 2021- March 2022). Multiple linear regression and PROCESS macro-Model 1 were used in the analyses. In this study, the STROBE checklist was followed. According to the results of the regression analysis, waiting for a transplant for 6–10 years reduced death anxiety by 9.38 times and waiting for a transplant for 16–20 years increased death anxiety by 31.3 times. The predictors in the regression analysis explained 33% of the model. The moderator effect constituted 6.4% of the explained part of the model, which was 25.4%; the R2 change was 3.4% and significant. We found that the longer the waiting period for organ transplant recipients, the higher the hopelessness and death anxiety.
Introduction
Organ transplantation is the transplantation of a healthy organ from a cadaver or living donor to the patient to replace an organ that has lost its function for any reason (USRDS Annual Report, 2021). Transplants performed after organ failures, acute diseases, or organ damage resulting from trauma make the patient hold on to life. Thanks to this highly developed and complex treatment, patients have a very high chance of regaining their health. It is known that after successful transplants, the survival rates of patients increase significantly. In a meta-analysis published in 2022, it was reported that the post-transplant mortality rate is 55% less compared to patients waiting transplant (Chaudhry et al., 2022). This indicates the importance of performing organ transplants in a short time.
Various transplant procedures such as heart, lung, liver, pancreas, skin, and cornea are performed in the world; yet, the most transplanted organ is the kidney (NHS Blood & Transplant, 2021a). According to the Newsletter global report, 21.102 of the 34.024 organ transplants in 2017 were kidney transplants (Newsletter Transplant, 2017). Conditions such as stressful life, unhealthy diet, and those brought on by the modern age have led to an increase in kidney diseases. Dialysis is the only treatment for end-stage renal failure (ESRF). The greatest disadvantage of these treatments, whether hemodialysis or peritoneal dialysis, is intravascular complications (USRDS Annual Report, 2021). In addition, in an important meta-analysis published in 2022, it was reported that patients experience complications of dialysis such as decreased quality of life, pain, fatigue, depression, and insufficient sleep (Fletcher et al., 2022). Renal failure and its treatment cause psychosocial problems as well as physical complications. The symptoms caused by the disease, the long-term treatments, and comorbidities cause the patient’s condition to worsen. This progress in prognosis leads to a decrease in the patient’s hope for recovery and may also cause a stronger feeling of death. Previous studies showed that hope is low, hopelessness is high, and death anxiety is serious in kidney patients (Cengiz & Saritas, 2019; Dewina et al., 2018; Ercan & Demir, 2018; Ghiasi et al., 2021; Soylu & Tuna, 2019). A kidney transplant is the only way for patients to recover from life-long renal failure and the dialysis treatment they are dependent on.
Patients without living donor options are recorded on the national organ waiting list for transplantation (Soylu & Tuna, 2019). According to the 2021 report of the United States Renal Data System (USRDS), the number of patients waiting on the kidney transplant list is increasing. The increase, which gained serious momentum, especially between 2018–2019, has reached alarming levels. At the end of 2019, it was reported that 78.690 patients were on the kidney transplant waiting list, but only 24.502 patients were able to receive a kidney transplant (USRDS Annual Report, 2021). The situation is similar in Turkey. The number of patients waiting on the kidney transplant list is 19.049 as of 2022, but the number of transplants performed was 3.375 in 2021 and 2.112 until August 2022. These numbers are quite insufficient (ORGANKDS, 2022). Inadequate numbers are significant factors leading to decreased quality of life in patients. Studies have reported that the quality of life of patients on dialysis is considerably poorer than that of patients with another chronic disease (Kara, 2012).
Difficulty in medical treatments for organ failure, prolonged treatment period, poor prognosis, and the fact that patients constantly face death threats cause mental disorders in patients (Aydemir, 2015). Furthermore, the low number of transplants from cadaver donors causes patients waiting on the list to remain registered on the list for many years and lose hope for transplantation as time passes. As the waiting times of patients on transplant lists get longer, the prognosis worsens, comorbidities develop, and the individual’s physiological processes slow down with age (Kainz et al., 2022). All these situations and long waiting periods lead patients to feel that they are approaching death instead of being able to recover and regain their health. In particular, the number of studies reporting that patients with ESRF receiving dialysis treatment have decreased hope of recovery, see death as salvation, and do not have any expectations that they can have a kidney transplant is increasing (Burns et al., 2017; Dewina et al., 2018; Ghiasi et al., 2021).
Dialysis is the only available treatment for the condition termed end-stage renal failure. While dialysis treatment promises patients a long life, it decreases the quality of life (Fletcher et al., 2022). While the one-year survival rate of these patients is 78% after the initiation of treatment, it has been reported that this rate decreases to 38% within five years (Donmez & Yilmaz, 2012). During this process, many patients sadly abandon the hope of achieving a quality life. It is an undeniable fact that patients refuse treatment due to pain, suffering, loneliness and fear of death and commit a form of passive suicide by not complying with their diets. The fear of death in particular has a significant impact on the quality of life of these patients (Donmez & Yilmaz, 2012).
Death anxiety is an emotion that is present from birth and lasts throughout life, lies at the basis of all fears, has a major role in the development of one’s character, and develops with the realization that one will no longer exist. The dimensions of death anxiety include uncertainty, fear of loneliness, fear of losing relatives, fear of being punished after death, worrying about what one has left behind, fear of pain, fear of losing one’s body and fear of vanishing (Karakus et al., 2012; Turhan, 2021). While uncertainties about incidents cause anxiety in individuals, fear and anxiety about death and what will happen after death leads to great uncertainty. In some opinions and explanations, especially those specific to religions, it is described that 'death is a very painful situation and there are terrible torments after death', which increases the anxiety and fears of people about death (Karakus et al., 2012). However, when religious rules are fulfilled, the explanations and religious coping tools offered by religion about death and life after death play an effective role in reducing the anxiety and fears of individuals (Dogan & Karaca, 2021). In diseases that evoke death such as ESRF in people with this belief, prolonged dialysis and waiting times lead to an increase in the fear of death. Therefore, placing patients who refuse dialysis in separate units may provide time for them to get accustomed to the dialysis unit, which is frightening for patients. In addition, in these units, the reasons for the rejection of treatment can be revealed and a holistic care can be provided to differentiate their perspectives towards dialysis (Donmez & Yilmaz, 2012).
The prolongation of the transplant waiting time leads to the inability to fully provide patient treatment, increases health expenditures, and negative affects health care (USRDS Annual Report, 2021). Nurses take patients’ future expectations into account and encourage patients to participate in their care while providing their treatment with a holistic care approach. One of the important factors affecting the patient’s participation in care is the hope that he/she will recover. It is known that care and treatment are more difficult in patients who feel the opposite. This situation negatively affects the health workforce and care costs as well as the patient prognosis. Our clinical observations have shown that patients less participate in care and lose hope for the future as the transplant waiting time gets longer. At the same time, patients think of death as the absolute end rather than the treatment of the disease as time passes by. In our country, studies on death anxiety have been conducted in dialysis patients, COPD patients, palliative care, elderly, and coronavirus patient populations (Inci & Oz, 2012; Kandemir, 2020; Karakus et al., 2012; Turhan, 2021). In light of these observations and the current literature, there is a need to investigate how transplant waiting time affects the levels of hope and death anxiety in patients waiting for transplantation (Figure 1). Accordingly, the two main hypotheses of the study are as follows: Conceptual framework (Depiction of analysis using Hayes’ (2017) PROCESS model 1).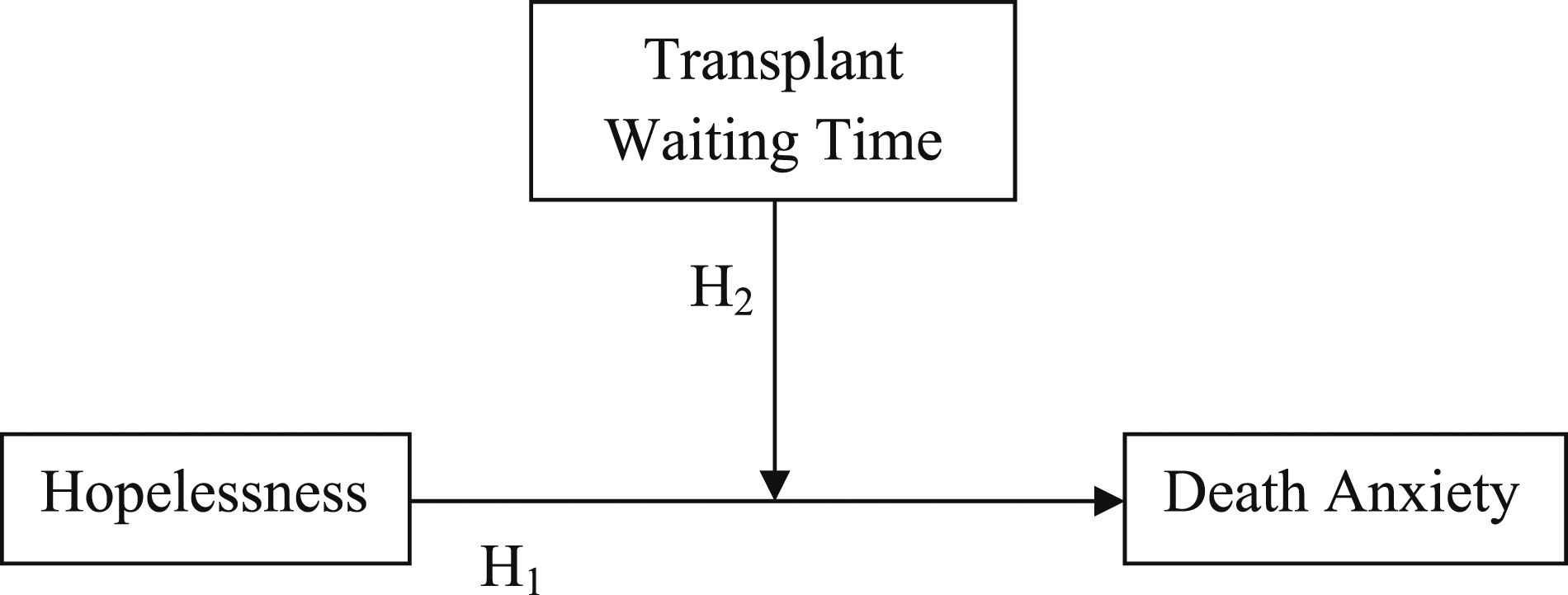
Hypotheses
Hopelessness is positively correlated with death anxiety.
Transplant waiting time has a moderator effect between hopelessness and death anxiety.
Conceptual Framework
Hopelessness is one of the most important factors that affect patient care negatively. Unfortunately, successful clinical treatment cannot be performed for patients who do not have hope for the future, survival, and recovery. Death, on the other hand, is the end everyone expects. However, diseases cause death to be remembered more often. There may be positive reactions to death as one gets used to the disease whereas patients may also have an uncontrollable fear that death is approaching as the time spent with the disease increases. Waiting for a transplant requires more than one’s best for the treatment. This process proceeds beyond the patient’s control. As time progresses, the hope that a suitable organ will be found may decrease and one may think that death is approaching. For this reason, the aim was to predict the study, especially in this concept. The lack of such studies in the literature and the gradual prolongation of organ waiting lists necessitated the assessment of patients in this direction. The second aim of this study was to contribute to the acceleration of organ transplants by drawing the attention of health policymakers to these issues.
Methods
Study Population and Data Sources
This descriptive and correlational study was conducted with patients registered on the national kidney transplant waiting list in a transplant center in Turkey. In Turkey, patients diagnosed with ESRF are added to the organ transplant list of the transplant center in their province and wait until a suitable organ is found (Soylu & Tuna, 2019). Patients are scored according to the National Coordination System based on certain conditions and are ranked in the list according to the score they get. Dead patients are automatically excluded from the list by the system.
In the center where the study was conducted, 564 individuals were registered on the kidney transplant list. 525 patients who met the inclusion criteria were included in the sample. 65 of these patients could not be reached through their phone numbers and 82 patients did not volunteer to participate in the study. Thus, the study was completed with 378 voluntary patients.
In Turkey, there are 19.049 individuals on the organ transplant waiting list in 2022. This number constituted the population of the study. Sample sufficiency was calculated according to a margin of error of 5% and a confidence level of 95% and the inclusion of 378 individuals in the study was found to be sufficient.
Inclusion criteria of the study: Patients aged over 18, with no diagnosed psychiatric disorder, no recent experience of grieving, and available contact information.
Exclusion criteria of the study: Patients aged under 18, who did not agree to participate in the study, and who could not be reached via the contact numbers on the transplant waiting list of the center.
The study data were collected by the researchers over the phone between 08/15/2021 and 03/15/2022. One of the researchers, Dr. Soylu is the organ transplant coordinator nurse in the unit where the research was conducted and his/her constant communication with the patients provided a reliable data collection process. At the time of the study, the measures for the COVID-19 pandemic were still ongoing; therefore, interviews were held over the phone, which was for the benefit of the patient to prevent any contamination that may occur in the patients. The patients were informed about the study at the first call and interviews were held with those who gave consent. For those who were busy, an appropriate date was determined to meet for the phone interview and they were interviewed again. Phone calls lasted approximately 30–45 minutes for each patient.
Data Collection Tools
Personal Information Form
The form was prepared by the researchers by reviewing the relevant literature (Cengiz & Saritas, 2019; Dewina et al., 2018; Ercan & Demir, 2018; Ghiasi et al., 2021; Inal et al., 2018), includes 15 questions regarding the introductory and disease-related characteristics of the patients.
Beck Hopelessness Scale (BHS)
The scale was developed by Beck Aron and Beanmesderfer (1974) in order to measure the negative expectations of individuals about the future. The scale consists of 20 items, which are ranked as true or false, and is scored between 0–20. Higher scores indicate higher levels of hopelessness. The level of hopelessness is classified as 0–3 none or minimal, 4-8 low, 9-14 medium, and 15-20 high (Beck Aron & Beamesderfer, 1974). The scale was adapted to Turkish by Durak and Palabiyikoglu (1994). The Cronbach alpha reliability coefficient of the scale was .85 (Durak & Palabiyikoglu, 1994). In our study, it was calculated as .88.
The Arabic Scale of Death Anxiety (ASDA)
The scale was developed by Abdel-Khalek (2004) to measure the anxiety of individuals towards death. The scale has a five-point Likert-type rating and consists of 20 questions in total. The score obtainable from the scale ranges between 20–80. The death anxiety of individuals increases as the scale score increases (Abdel-Khalek, 2004). The scale was adapted to Turkish by Saricicek Aydogan et al. (2015). The Cronbach alpha reliability coefficient of the scale was .86 (Saricicek Aydogan et al., 2015). In our study, it was calculated as .97.
Ethical Considerations
Ethical rules and principles of the Declaration of Helsinki were followed at every stage of the study. Prior to the study, permission was taken from the Clinical Research Ethics Committee of Kırşehir Ahi Evran University (Protocol Number: 2021-13/146, Dated: 03/08/2021). Patients were included in the study on a voluntary basis.
Data Analysis
The data were analyzed in SPSS 25 (IBM Corp., Armonk, New York, USA). Descriptive statistics were given as number, percentage, mean (sd), median (min-max). A multiple linear regression (
The moderator effect of the transplant waiting time in determining the effect of hopelessness on death anxiety was investigated. This analysis was performed with PROCESS version 4.1, Model 1 (Hayes, 2017). The influence of moderator was tested by probing the moderation at low, average and high values of moderator variable, determined by -1SD, Mean, +1SD and Johnson-Neyman output according to Hayes (2017). This model provided the opportunity to examine the effects of hopelessness alone, transplant waiting time alone, and hopelessness*transport waiting time (interaction) together on death anxiety and also prevented the variables from being affected by each other. All models tested met the assumptions of normality, independent errors, and absence of multicollinearity. Results are presented as linear regression coefficients (unstandardized and standardized β), reporting 95% confidence intervals (95% CI), t, p-values (p), correlations (zero, part, partial), and variance inflation factor (VIF). Statistical significance threshold was set at p = .05.
Results
Findings Regarding Descriptive Characteristics and Mean Scale Scores of Patients
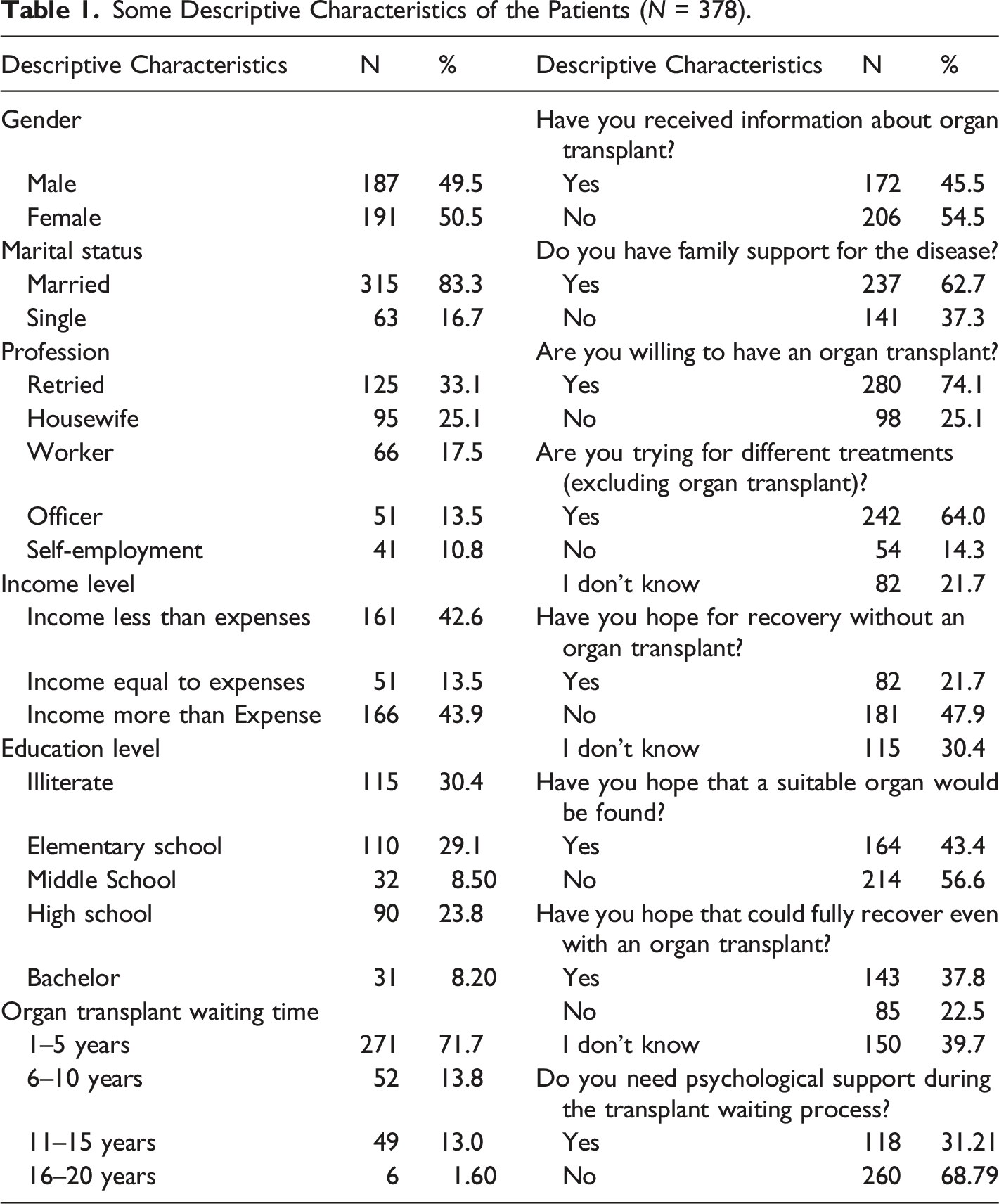
Some Descriptive Characteristics of the Patients (N = 378).
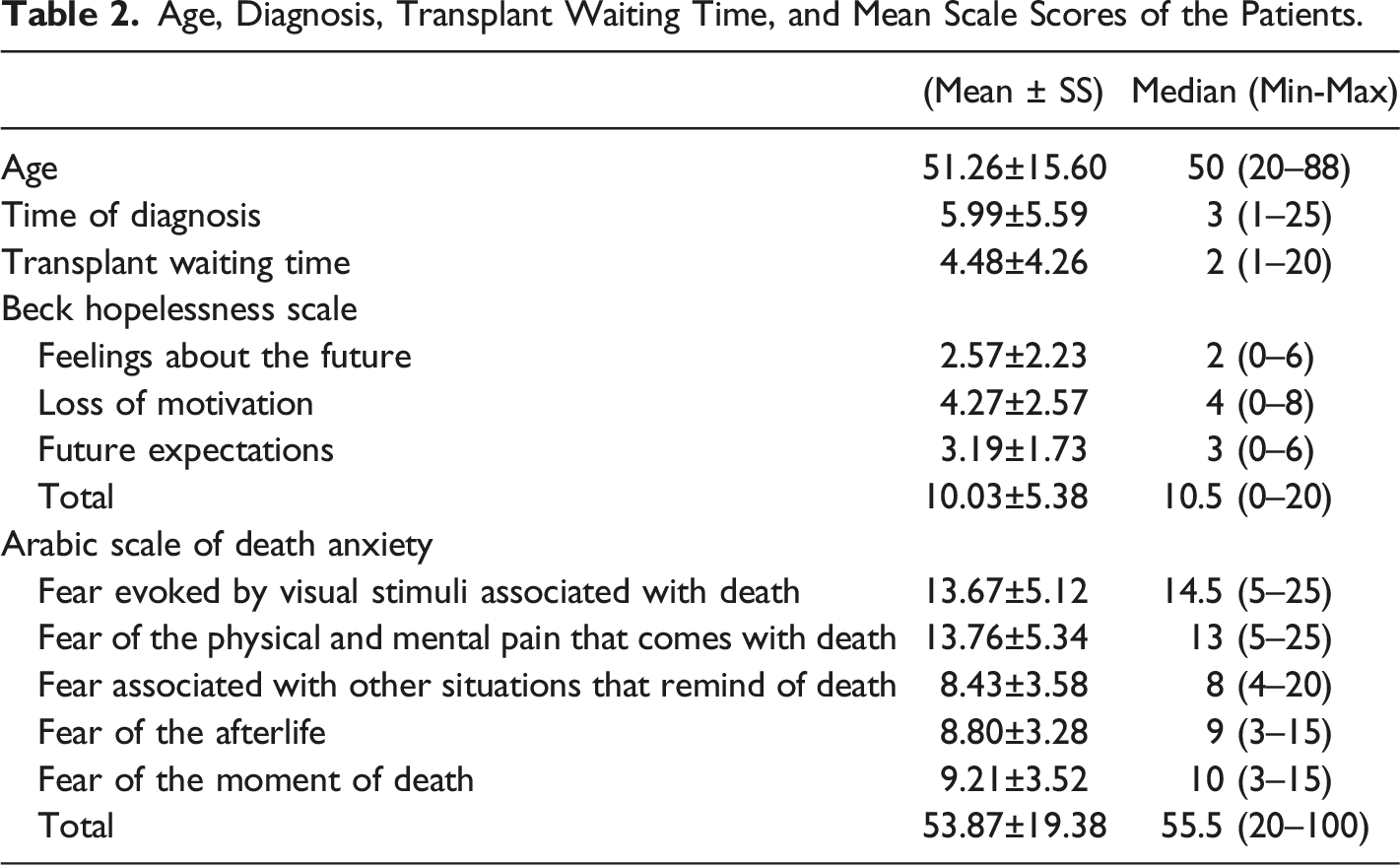
Age, Diagnosis, Transplant Waiting Time, and Mean Scale Scores of the Patients.
Regression Analysis Findings of Patients
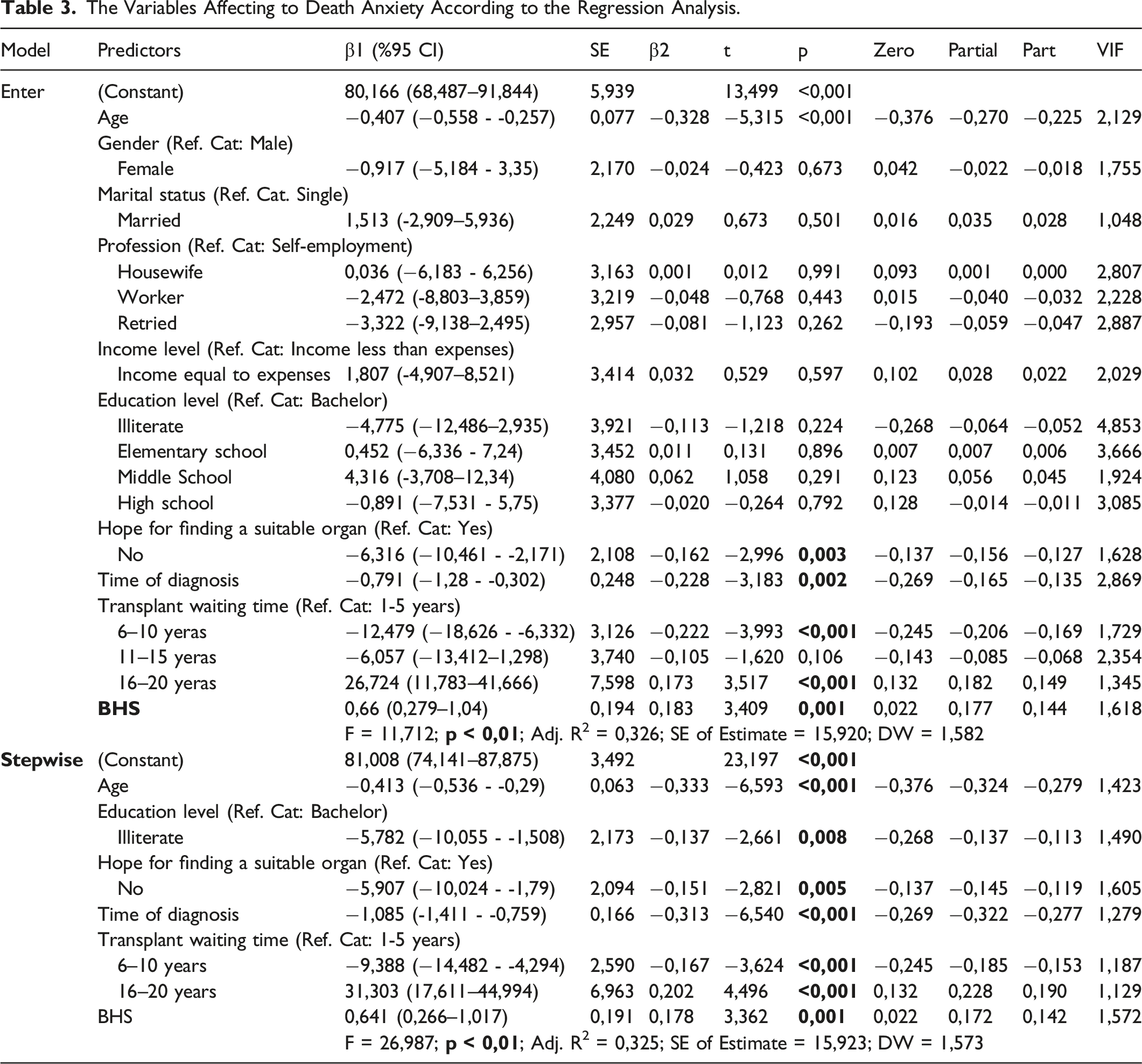
A multiple linear regression model was established to estimate the ASDA level based on age, gender, marital status, profession, income level, education level, hope for finding a suitable organ, time of diagnosis, transplant waiting time, and BHS level. The regression model, which was first examined with the Enter method, was statistically significant (F = 11.712; p < .001) and Adj. R2 was .326. The VIF values of the independent variables were examined and all of the values were found to be within the appropriate limits of less than 5. According to the Durbin-Watson (DW: 1.582) coefficient, there was no multicollinearity problem. A stepwise model was used in multiple linear regression to eliminate variables that did not have a significant effect on ASDA. This model was statistically significant (F = 26.987; p < .001) and Adj. R2 was found to be .325. VIF values were less than 5 and within appropriate limits and DW was 1.57. These variables explained 33% of ASDA. Age (p < .001), education level (p = .008), hope for finding a suitable organ (p = .005), time of diagnosis (p < .001), transplant waiting time (p < .001), and BHS (p < .001) had a significant effect on ASDA. In line with these variables, a unit increase in age decreased death anxiety by .41 times, illiteracy by 5.78 times, being hopeless about finding a suitable organ by 5.9 times, time of diagnosis by 1.08 times, and transplant waiting time between 6-10 years by 9.38 times. However, remarkably, death anxiety increased 31.3 times in those waiting for a transplant for 16–20 years.
The Variables Affecting to Death Anxiety According to the Regression Analysis.
Results of Moderator Effect Analysis
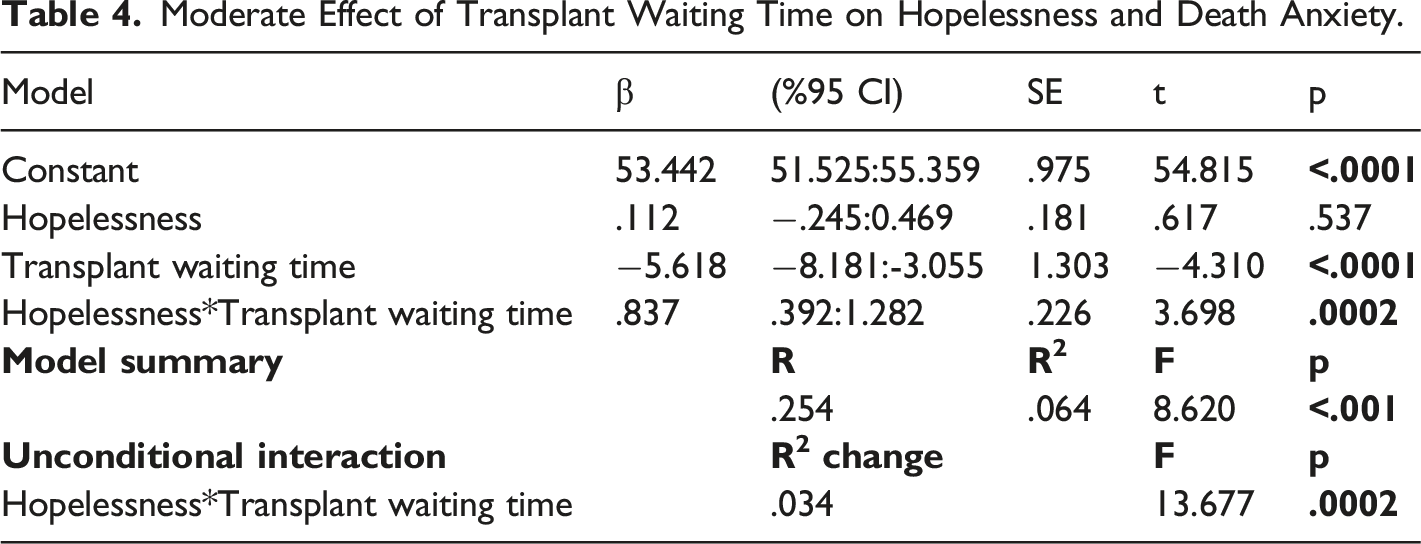
Moderate Effect of Transplant Waiting Time on Hopelessness and Death Anxiety.
Simple Slopes for Organ Transplant Waiting Time to Predict Points at Each Level of Attendance.

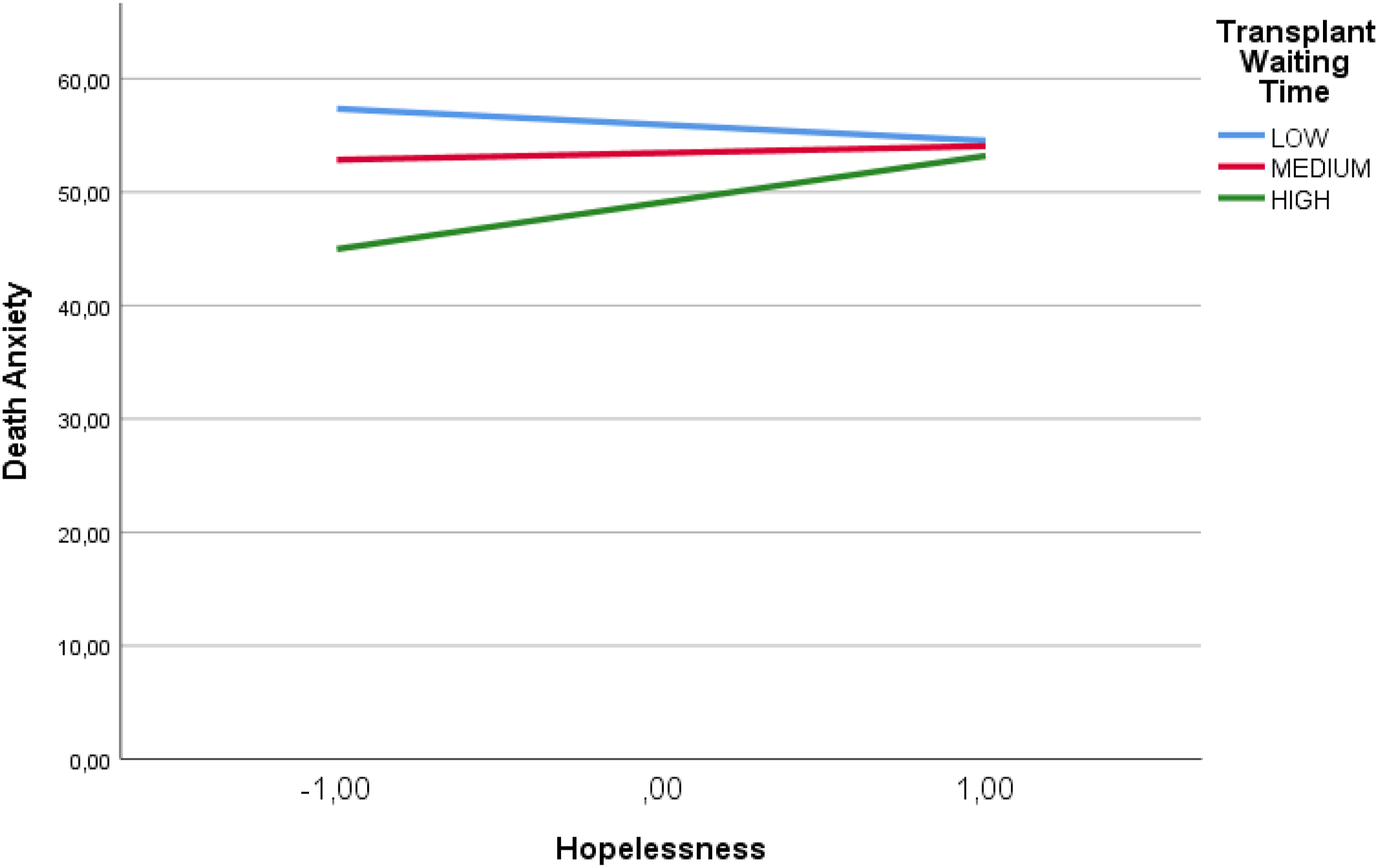
The change of the effect of hopelessness on death anxiety according to organ transplant waiting time.
The results of moderator value defining the Johnson-Neyman region of significance were examined in order to evaluate at which level the transplant waiting time started to affect death anxiety significantly. Patients participating in the study had been waiting for transplantation for between 1-20 years. The lowest significant effect was observed at 1 year, the least waiting time (t = 1.96, p = .05, β = .37), whereas the strongest effect was observed at 20 years, the longest transplant waiting time (t = 3.78, p = .0002, β = 2.25). These results also support the moderator effect analysis and demonstrated that the effect of predictors on death anxiety increases as the transplant waiting time increases.
Discussion
In this study, in which the moderator effect of the transplant waiting time on the relationship of hopelessness and death anxiety in patients waiting for an organ transplant was investigated, the median age of the patients was 50 (20–88). In a meta-analysis in which a total of 793,731 patients receiving dialysis treatment who were on the organ transplant waiting list were examined, it was reported that the mean age of the patients was 51.3 (37–73) (Chaudhry et al., 2022). Considering the distribution of the patients in our study based on gender, it was seen that the ratio of women was higher. It is known that women are at higher risk for kidney diseases than men. In their meta-analysis, Hill et al. (2016) reported that women suffer from kidney diseases more than men (Hill et al., 2016). Likewise, in a comprehensive epidemiological study conducted with 10,749 individuals in 23 provinces in Turkey, the prevalence of chronic kidney disease was reported to be 18.4% in women and 12.8% in men (Suleymanlar et al., 2020). Our study group consisted of individuals from the largest city in the Southeastern Anatolia region, which is one of the 7 geographical regions of Turkey. This region ranks second in terms of the regional distribution of chronic kidney diseases (Suleymanlar et al., 2020). In line with these results, it can be suggested that the characteristics of the patients included in the study (Table 1) can be discussed with literature results.
The patients in our study had been waiting for an organ transplant for 4.48 years on average (Table 2). In the USRDS 2021 report, the waiting time was 4.3 years (51.6 months). In the study conducted by Kainz et al., patients waited five years until the first transplantation (Kainz et al., 2022). In the study of Piskin et al., it was reported that patients waited 6 years (74 months) for organ transplantation (Piskin et al., 2022). In our study, it was observed that the waiting time was lower than in the literature, leastwise. However, this is thought to be related to the characteristics of the sample. Because studies often emphasized that organ transplantation is insufficient in Turkey. According to the latest data, kidney transplants performed in Turkey have reached approximately 19%. Approximately 81% of patients are still living with dialysis treatment (Suleymanlar et al., 2020). This situation is far behind in western countries. According to Eurotransplant International Foundation statistics, kidney transplants (deceased donors) were listed as 31.0 in Belgium, 29.6 in Austria, 29.5 in Croatia, and 26.6 in Netherlands (per million population) (Eurotransplant, 2021). In the report published by the National Health Service in England, it was stated that 7846 patients registered on the kidney transplant waiting list in 2021 represented 52.6 patients per million in the population (NHS Blood and Transplant, 2021b). According to the USRDS 2021 data, the number of transplants performed was higher than the number of patients receiving dialysis treatment in the last five years and it was stated that this was pleasing but still insufficient due to the increase in the number of dialysis patients (USRDS Annual Report, 2021). In the USA, according to the data for 2021, the number of patients waiting for a kidney transplant was 43,617 whereas the number of transplants performed was 25,490, of which 19,519 were made from cadavers (OPTN, 2022). In this comparison, it is obvious that Turkey is quite insufficient in terms of transplantation. In Turkey, organ transplants are generally made from living donors. In 2020, 1335 transplants were performed from living donors and organs were taken from cadavers in only 5 transplants (Suleymanlar et al., 2020). In a study reported in 2012, organ donation was allowed in only 242 of the 1470 brain deaths in Turkey. These numbers are an indication of the insufficiency of organ transplantation from cadavers. It was emphasized that this arises from some religious thoughts and financial, social, and cultural approaches (Burns et al., 2015). In a country with a population of approximately 85 million, the number of organ transplants must be immediately increased and national action plans must be implemented. It is obvious that serious developments and reinforcements are required in terms of individual and social aspects and policy-makers. It is thought that the number of donations should be increased immediately, with a system such as the Belgian model, in which those who do not want to be a donor apply to the state and other citizens are legally considered as donors.
Waiting for organ transplantation is a particular concern to the patient’s hope for the future and recovery. Uncertainty in health status and thinking that it will get worse are important factors that psychologically affect patients. The level of hopelessness of the patients in our study was moderate (10.03 points). In particular, the highest sub-dimension scores were taken from loss of motivation and expectations about the future (Table 2). This clearly shows the unwillingness of patients to be treated and participate in care activities and the lack of hope for transplantation in the future. Moreover, more than half of the patients (56.6%) thought that a suitable organ could not be found and a large portion of them (47.9%) thought that they would not be able to recover without transplantation (Table 1). These thoughts showed that the expectations of the patients for finding a suitable organ were negative. In their study, İnal et al. conspicuously showed the emotions of the patients with some patient expressions: ‘…I said I will die anyway; they cannot find a kidney from a cadaver waiting list…’, ‘…I get more hopeless day by day. Many (patients) do not think that they will find an organ and they even make me think of getting off the list with what they say…’, ‘The list is getting longer day by day, it is very difficult for us to find one’ (Inal et al., 2018). In the study, it was reported that the most important reason for patients to have these feelings is the length of the transplant waiting time. Similarly, Burns et al. (2015) emphasized the importance of the sense of uncertainty in the waiting process of patients: ‘…if you’re not on the transplant list you feel, oh my god! You think about your rest of life; feel bad like this until you…’ (Andrade et al., 2015). On the other hand, some patients see dialysis treatment as an important option for recovery. Such patients wait for the day they will have an organ transplant with hope and think that they will get effective results from the treatment (Andrade et al., 2015; Inal et al., 2018). However, many studies focused on the feeling of hopelessness rather than hope in patients. Many studies in the literature reported that patients with ESRF and receiving dialysis are hopeless about recovery and the future (Cengiz & Saritas, 2019; Ercan et al., 2018; Mollaoglu et al., 2016; Oz, 2010). The most important problem that hopelessness will cause in the patient is psychological problems such as depression. In the autobiography of Öz, hopelessness was predicted as being on the verge of suicide (Oz, 2010). Andrade et al. (2015) reported that hemodialysis patients have high levels of hopelessness, suicidal ideation, and depression (Andrade et al., 2015). Similarly, in our study, a substantial portion of the patients (31.21%) stated that they needed psychological support during the transplant waiting period (Table 1). It is expected that patients with this thought will have difficulties participating in their treatment and care in the future. The provision of nursing services is closely associated with care activities. For this reason, every patient should be properly assessed and hopeful care should be provided for a healthy life that awaits in the future. Instilling and increasing hope in patient care, which is one of the basic roles of nurses, should be an indispensable approach for patients in this process (Mutlu & Duyan, 2012). However, the extended waiting lists and the time spent by patients cause them to lose their hope for recovery and remember death more often.
The death anxiety of the patients included in our study was evaluated and it was found that they had above-average death anxiety (53.87 points). In particular, the highest score among the sub-dimensions of the scale was taken from the fear of physical and mental pain accompanying death (Table 2). Although death is expected for every person, diseases remind death more often. In particular, receiving dialysis treatment two or three times a week keeps the patient’s treatment obligation and lifelong commitment to this treatment in mind. In their study, Dewina et al. (2018) revealed that death anxiety significantly increased in patients receiving dialysis treatment more than once a week (Dewina et al., 2018). Moreover, the negativities brought by the treatment and the worsening of the prognosis can also increase the negative feelings of the patient. In their study, Mutlu and Duyan reported that 80.4% of dialysis patients thought about death (Mutlu & Duyan, 2012). In another study, patients expressed their fear of death while waiting for a suitable organ with the following statements: ‘I felt that my life had passed to another dimension… the world came crashing around my ears… I never thought I would die if an organ was not found’, ‘If no organ is found on the waiting list, I always think of bad things (death) since I have no living donor’ (Inal et al., 2018). Ghiasi et al. (2021) reported that receiving dialysis more than once a week decreased the quality of life of patients and significantly increased death anxiety (Ghiasi et al., 2021).
The factors that caused the highest fear of death in patients in our study were analyzed with a multiple linear regression model (Table 3). According to the regression analysis, predictors included in the model explained 33% of death anxiety. A human being is a bio-psycho-social, multi-dimensional entity that can be affected by many factors. Such an effect, which will enable us to predict the death anxiety of humans, is a very pleasing result in terms of planning the appropriate care that can be provided to patients. When the effects of predictors were examined alone, it was found that age slightly reduced death anxiety. According to Registry 2020 data, the age range with the highest rates of organ transplants was reported as 20-44 by 45.6% and 45-64 by 41.7% (Suleymanlar et al., 2020). The median age of the patients in our study was also in these ranges. The fact that most transplants in Turkey are performed in these age ranges shows that the patients in our study may have thought that they were at the right time for transplantation. Thus, the thought of regaining health before the disease further progresses may have reduced the death anxiety of the patients. According to the USRDS data, the most successful results in transplantations were achieved in the age group of 45–64. This result supports our finding (USRDS Annual Report, 2021). In the literature, various studies reported that the fear of death increases with increasing age (Bowling et al., 2010). This is thought to be related to the sample characteristics. The reasons for the reducing effect in our study, besides the ones mentioned above, may include the fact that the mean age of the patients was similar to those reported in the literature (Chaudhry et al., 2022), that 71.7% of the time of dialysis was between 1-5 years, and that society in the geographical region where the study was conducted adopted a more fatalistic approach in terms of its social nature. It is also thought that this was associated with the education level of the patients in our sample. In the model, it was revealed that illiterate people experienced 5.78 times less death anxiety than those with a graduate degree. This result may be due to the fact that individuals are unconscious about researching and questioning their diseases, learning different treatment options, or preparing themselves for what awaits them in the future. One of the important points in the model was that death anxiety decreased 9.38 times in those with a waiting time of 6–10 years but increased 31.3 times in those waiting for 16–20 years. This remarkable finding is actually not surprising. Patients experience fear and panic during the first years of the disease which include events such as being diagnosed for the first time and encountering new treatment options; however, they may think that they can adapt to the disease in time and get treatment. The data of USRDS also support our opinion. According to the report, 20.4% of patients have a kidney transplant 5 years after dialysis. Considering the distribution of transplants by age, the highest number of transplants was performed between the ages of 0–17 (84.6%) whereas the least number of transplants was performed at the age of 75 and above (1.5%) (USRDS Annual Report, 2021). These data show that patients have a higher chance of having transplantation after approximately 5 years of treatment and at younger ages. For this reason, it was not surprising to see that death anxiety decreased in those who waited for 6–10 years since they thought about the possibility of having transplantation.
Conclusion
ESRF is a progressive disease with a gradually worsening prognosis. Patients may lose hope for recovery and the thought of recovery may be replaced by death as they receive dialysis treatment every week and more than once a week. In the study of Yanar (2015), it was reported that hopelessness and uncertainty about what awaits in the future increase the level of intolerance as the organ transplant waiting time increases (Yanar, 2015). Similarly, Burns et al. (2015) found that the motivation of patients to cope decreases as time progresses during the waiting period for transplantation (Burns et al., 2015). Although our study findings are similar to those reported in the literature, the patients who experience death anxiety the most are those who have been waiting for transplantation for 16–20 years. Hopelessness included in the regression model showed a strikingly lower positive effect. This result indicates the necessity to investigate the moderator effect of the transplant waiting time on the effect of hopelessness on death anxiety.
According to the Process Macro Model 1 analysis, there was no direct significant correlation between hopelessness and death anxiety; however, it is an important finding that the transplant waiting time affected death anxiety negatively. This finding suggested that the patients got used to the disease and its treatment over time and believed in the possibility of transplantation. However, when the model was established with the interaction, it was found that hopelessness actually increased death anxiety along with the transplant waiting time. Thus, in our study, we showed that the evaluations made alone in patients are insufficient and that the most accurate patient result can be reached thanks to advanced analyses. In this version, the model explained 25.4% of death anxiety, of which the transplant waiting time constituted 6.4%. This rate is significant and high. The transplant waiting time revealed a 3.4% R2 change with the moderator effect. The result of the simple slopes analysis also proved that the highest effect on the patient occurs as the transplant waiting period progresses. As seen in Figure 2, high waiting times directly increase hopelessness and death anxiety. Johnson-Neyman analysis results revealed the time when patients experienced the strongest death anxiety according to the minimum and maximum years and the strongest effect was seen in 20 years. All of our findings support each other and provide new and important results to the literature.
In increasing cadaveric organ donation, education for Muslim patients, family involvement, and collaboration with religious leaders may constitute a profitable strategy for providing culturally sensitive nursing care (Muliira & Muliira, 2014). Abbasi et al. (2018) reported that most of the participants required religious support to be able to donate organs (Abbasi et al., 2018). In Uzuntarla’s (2016) study in which he provided training on organ transplantation and donation, the rate of those who believed that there was no religious objection increased from 24.8% prior to the training to 80.5% post training (Uzuntarla, 2016).
In a study by Yngman-Uhlin et al. (2016), it was reported that during the waiting process, patients were concerned about what would happen to them and what preparations would be carried out for transplantation, their time was getting tighter and tighter, their health concerns increased accordingly, they needed support from others and constant information from hospital staff, and they were in need of relaxation and hope for the future (Yngman-Uhlin et al., 2016). Since the waiting experience is stressful, social support is necessary for patients in need of kidney transplantation. One of the most effective ways to provide social support is through family and friends. Since the dynamics of relationships with family and friends are impacted by the experience of waiting for a kidney transplant. The family should be included in the process through trainings to be conducted to the families and they should have foresight about the steps that are ahead of them. In addition, the need for moral support as well as physical support should be underlined to the family members. Considering the impact of the social environment, opportunities should be provided to develop new relationships within the medical team and the community of dialysis patients (Burns et al., 2015).
Footnotes
Acknowledgements
The authors thank all the study participants.
Author Contributions
Ceyhan and Soylu made substantial contributions to conception and desgn, or acquistin of data, or analysis and interpretation of data; Soylu carried out the implementation phase of the study; Ceyhan and Soylu involved in drafting of the manuscript or revising it critically for important intellectual content; and authors gave final approval of the version to be published. Each author should have participated sufficiently in the work to take public respoonsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.