
Abstract
We developed, implemented, and evaluated a participatory arts-based storytelling initiative called the Reflection Room project. Our aim was to investigate if visiting a Reflection Room, (1) creates opportunities for disclosing emotions and processing thoughts, (2) increases comfort discussing dying and death, and (3) supports advance care planning (ACP), conversations. In the pilot phase of the Reflection Room project, a Reflection Room was installed in 25 sites across Canada from 2016–2017. Data collection included reflection cards (n = 463), and surveys completed by visitors upon exiting a room (n = 271) and 3 months later (n = 50). Analysis involved theoretically driven coding, inductive content analysis, and descriptive statistics. We found reflections contained both emotional disclosures and reflective processing. Survey data indicated visiting a Reflection Room increased comfort in thinking and talking about dying and death as well as the likelihood of engaging in ACP. In the future, we will explore the extent to which the project fosters social connections and well-being.
Introduction
Dying, death, and grief are social experiences that impact not only people who are dying, their family, friends, and caregivers, but also larger networks of supportive relationships between people in the social realm at work, schools, clubs, faith communities, and so on (Abel, & Kellehear, 2022; Kellehear, 2013; McLoughlin et al., 2016). Social factors such as dominant cultural narratives shape this social experience (Krikorian et al., 2020; Lund, 2021; Neimeyer et al., 2014). Life circumstances, culture, and religion influence what is considered to constitute a “good enough death” (Krikorian et al., 2020). Theories of grief describe how the bereaved negotiate the meaning of loss with both family and community (Neimeyer et al., 2014), as well as culturally mediated expectations around mourning (Lund, 2021).
A challenge in Western society is that many people (e.g., healthcare providers, neighbours, caregivers, and the dying) are uncomfortable talking about dying, death, and grief (Carter et al., 2021; Kellehear, 1984). In 1984, sociologist Allan Kellehear argued that at a society level there is no widespread denying of death, but that various institutional forces appear to be leading individuals to avoid talking about death, including the medicalization of death. Arnup (2014) elaborates that the funeral industry and the increased accessibility of hospitals have distanced people from the experience of caring for the dying and dead, meaning fewer people have intimate experiences with dying and death. The same is true of grief. There appears to be a cultural expectation that “normal” grief is short lived and attended to through funeral rituals, while prolonged grief tends to be pathologized and medicalized (Lund, 2021). Given this set of factors, there is social need to develop better responses to dying, death, and grief incorporating policy, language, symbols, ritual, and space (Abel & Kellehear, 2022; Breen et al., 2022).
This paper discusses a participatory arts-based initiative called the Reflection Room project. The aim of the project is to create a space in healthcare and community settings that invites and increases comfort with thinking and talking about dying and death. In this paper we first explore various initiatives that aim to increase peoples’ comfort with dying and death at the societal level. We then describe our Reflection Room project and share our evaluation of the pilot version. We conclude by commenting on what our findings offer the broader societal discussion on attending to dying, death, and grief.
Background
There are many initiatives that aim to increase people’s knowledge, skill, and comfort in talking about the end-of-life (EOL). Examples of initiatives include advance care planning (ACP), the public health palliative care approach, and the death awareness movement. A belief underlying these efforts is that despite the universality of death, people have a hard time talking about it, and that it would benefit society if people were more comfortable discussing the impact of death with others (Incorvaia, 2022; McLoughlin et al., 2016; Malhotra et al., 2022). There is value in being able to discuss dying, death, and grief in medical, social, and community conversations to foster access to information, non-judgemental support, maintain connections, and so on (Abel & Kellehear, 2022; Breen et al., 2022)
ACP is a process to encourage people to confirm a substitute decision-maker and prepare substitute decision-maker(s) for possible future decision-making by discussing values, wishes, and things that are important (Malhotra et al., 2022; Advance Care Planning Ontario (2022)). These discussions can happen with one’s substitute decision maker, clinicians, family, and friends (Malhotra et al., 2022; Advance Care Planning Ontario (2022)). Despite clinicians encouraging ACP, there remains little uptake (Advance Care Planning, 2021). Additionally, there are questions about the effectiveness of ACP in preparing people confronting dying and death to talk in a substantive and meaningful way about their experience (Carter et al., 2022; Morrison et al., 2021).
A public health palliative care approach aims to support communities in caring for each other as people die and grieve (Abel & Kellehear, 2022; Kellehear, 2013). Despite its modern roots in Dame Cicely Saunders’ holistic approach (Graven & Timm, 2021), hospice palliative care in its present form, focuses most on the clinical aspects of dying, and often does not account for the social nature of the EOL (Abel & Kellehear, 2022; Kellehear, 2013; McLoughlin et al., 2016). According to Abel and Kellehear (2022), a public health approach recognizes that well-being for those who are dying, grieving, and caregiving is dependent on social networks engaging in contextualized peer-support including knowledge sharing, reducing social isolation, and cultivating meaning and purpose (Letherby & Davidson, 2015). Accessing hospice palliative care services in their current form necessitates the recognition from clinicians, patients, and caregivers that a palliative approach is needed, and the move to palliative care requires an often missing skill, and willingness to talk about dying and death (Hui et al., 2018).
The global “death positivity” and “death awareness” movements aim to increase dignity, compassion, and social support to all who experience death and loss, with an emphasis on increasing dialogue and acceptance of death and grief (Incorvaia, 2022; McCormick, 2021). Some examples of death awareness initiatives include Death Cafés, The Conversation Project, and Before I Die festivals (Incorvaia, 2022; McCormick, 2021; McLoughlin et al., 2016). Death Cafés are community-driven “pop-up” non-profit events hosted and facilitated by anyone willing to follow the Death Cafés guidelines. The host offers drinks and food, and the facilitator supports people to feel comfortable engaging in unstructured, agenda-free conversations about death (Miles & Corr, 2017). These gatherings are explicitly not grief support groups, yet many who attend are recently bereaved (Miles & Corr, 2017). The reasons why participants attend Death Cafés include processing mortality or the existential experience, sharing experiences of loss, and curiosity (Miles & Corr, 2017).
While serving an important purpose, there are several challenges with ACP, hospice palliative care, Death Cafés, and other structured initiatives. These initiatives tend to attract people who have already contemplated dying or death, demonstrated by their taking action to complete an ACP workbook, request palliative care, or show up to an event. They may not reach people who have not considered the importance of thinking and talking about the EOL. Furthermore, access to many dying, death, and grief initiatives require a facilitator, whether it is someone who guides a patient through ACP, a clinician gatekeeper who controls access to hospice palliative care, or organizers of a death awareness event. Facilitation may make some participants feel constrained in the topics they share or create a sense of being rushed when they desire time for quiet reflection (McLoughlin et al., 2016). Others may be uncomfortable with the lack of anonymity during structured events, which could inhibit the sharing of strong emotions (Hartig & Viola, 2016).
Some community-driven dying, death, and grief initiatives such as festivals and online peer support groups appear to allow for more flexibility in participation, which may alleviate some concerns surrounding over-facilitation. Many online community support groups for grief contain message boards where the grieving can share emotions and thoughts at any time of the day, which offers choice about when and how people participate (Hartig & Viola, 2016). Dying and death festivals such as The Dying.series—an event series that is part of a larger design festival in Toronto, Canada (Sellen et al., 2020; Tracy, 2010)—offer participants from diverse audiences control over the extent of participation by having unfacilitated activities where people choose how much or little to participate. However, it may be that these initiatives also primarily engage people already prepared to talk about the EOL, missing people who have yet to consider their relationship to dying, death and grief.
Recognizing the need for accessible, community spaces with low levels of facilitation that support reflection and the sharing of experiences related to dying and death, we developed, implemented, and evaluated an initiative called the Reflection Room project. What makes the Reflection Room project different from other initiatives like ACP, hospice palliative care, and Death Cafés is that it draws on the benefits of sharing stories of dying and death in a way that is unfacilitated and allows for anonymity and choice regarding level of engagement with the room. We hypothesized that being faced directly with conversations about death might make people uncomfortable and might attract people when they are dying or already bereaved. Drawing on research in spiritual care and unfacilitated storytelling, we imagined how creating a contemplative space for reflection and anonymously sharing stories about dying and death and installing this room in places people already visit such as hospitals, retirement homes, and libraries might reach people who have not yet consider the importance of these conversations.
The Origins of the Reflection Room Project
The project’s origin was at a healthcare conference in 2016 and involved an arts-based representation of emerging findings from a study of institutional best practices to provide spiritual care at the EOL (Holyoke & Stephenson, 2017). This first Reflection Room illustrated four best practices that enable a high-quality approach to spiritual care by care providers (Holyoke & Stephenson, 2017). The first principle is ‘allowing spiritual questions and issues to emerge’, which is about setting aside time and being comfortable to express existential questions and issues that arise with the EOL. The second principle is, ‘allowing for acts of “witnessing”’, which is about perceiving, experiencing, remembering, or reflecting on a person’s life including their needs, questions, struggles, and joys, as well as feeling seen in your own expression of these things. The third principle is, ‘cultivating sacred places’, which is about being attentive to the qualities and aesthetics of a place to make it feel special. The fourth principle is, ‘allocating time dedicated to marking transitions and processing experiences’, which is about prescribed embodied acts that promote transformation (Holyoke & Stephenson, 2017). To avoid an oral presentation of the findings and to animate the mobilization of the knowledge from this study, visitors were invited to reflect on their professional care experiences of their patients’ EOL in the previous year. The reaction to the conference installation was unexpected, with many visitors not reflecting on their experiences as healthcare providers as they were invited to do, but as people who had experienced dying, death, and grief in their personal lives. We decided to investigate the positive initial response with a pilot research project to explore the potential for a transportable installation that could support more widespread thinking and discussions about dying and death in other settings.
Methods
We engaged in a developmental evaluation of the Reflection Room project, which allows us to iteratively design, adapt, and evaluate as the project evolves (Carter et al., 2023). Developmental Evaluation is a method of evaluation that is a non-linear, emergent, and suited to developing dynamic programs and initiatives in complex environments (Gamble, 2008; Patton, 2010). In this section we discuss the design, aims, setting and recruitment, and methods of evaluation of our pilot Reflection Room project.
Design
The pilot Reflection Room project was informed by best practices in EOL spiritual care (Holyoke & Stephenson, 2017) and Candy Chang’s Before I Die and Confessions installations (https://candychang.com/) which are public, unfacilitated, anonymous message boards that invite specific reflections. We also drew on Schenker et al.’s (2015) conceptual model of the benefits of storytelling for bereaved family members in the intensive care unit. This model suggests that a storytelling intervention is supportive of mental health and well-being by helping people disclose emotions, process thoughts, and connect socially (Schenker et al., 2015). The bringing together of these three pieces of work provided a framework informing the design and evaluation of our project.
Designing the mobile “Room” based on this framework led us to invite visitors to pause, reflect, and write stories about their experiences with dying and death, and read the stories shared by others. While the Room looked different depending on the space, the common essential elements within the Room included several features. Comfortable chairs and a quiet atmosphere were used to encourage reflection. A “ribbon wall” where people could pin up their stories for others to read supported witnessing (see figure 1). Images of nature, a common colour scheme, and quiet classical music encouraged contemplation. To encourage processing experiences, visitors were also invited to write on a reflection card in response to the prompt, “write about your experiences with dying and death”. Example of a reflection room with a ribbon wall.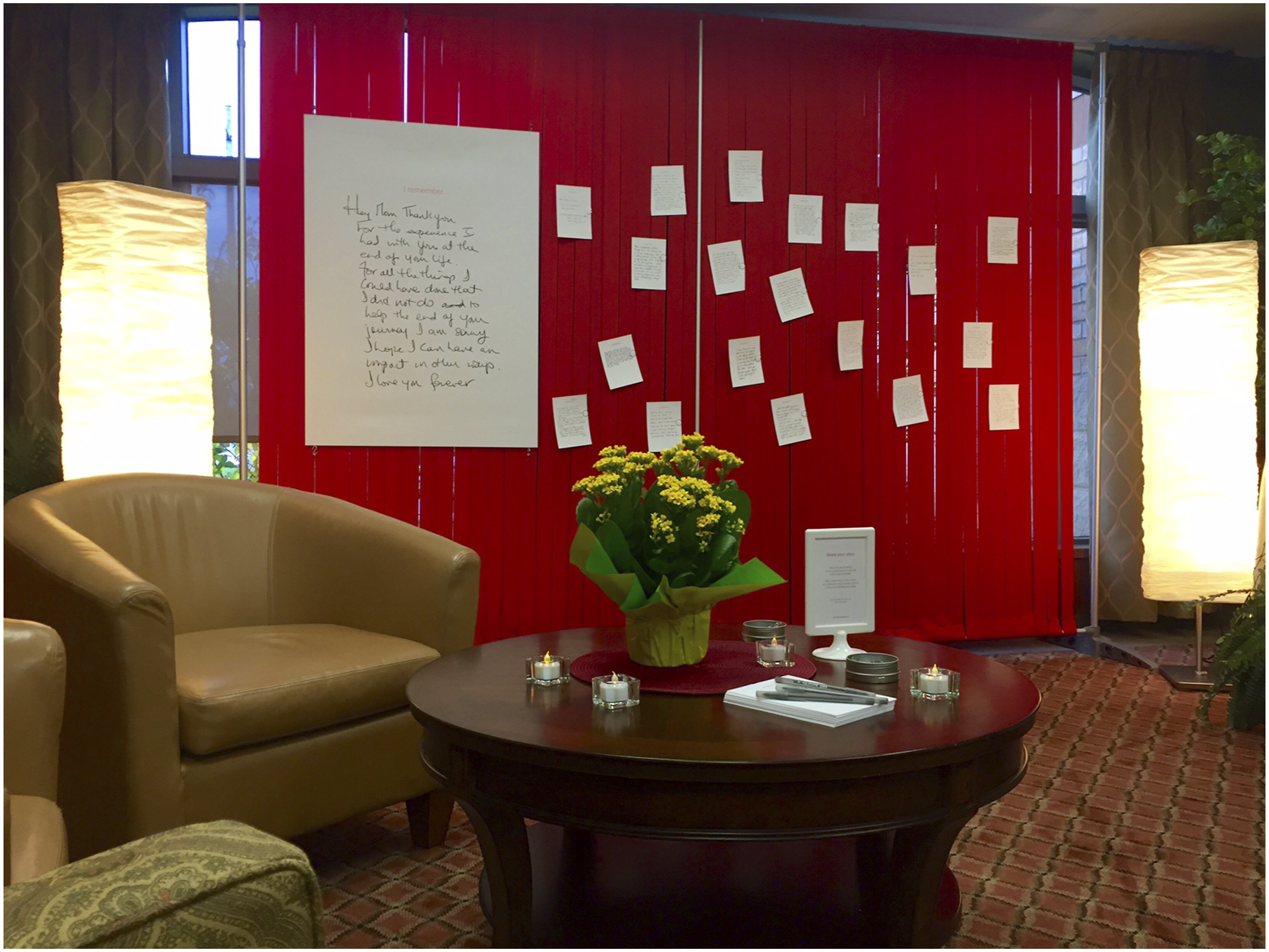
Aims
Our first objective was to design a mobile “Room” with common essential features that could be replicated in various settings in a way that invites quiet reflection; the disclosure of emotions and processing of thoughts; and the opportunity for interpersonal exchanges like online supports but in a way that maintains the benefits of physicality. Our second objective was not specifically focused on well-being but on designing the “Room” to increase peoples’ comfort discussing dying and death. Our third objective was to support people to be better prepared to think through the issues involved in their own death.
Our primary question was, ‘when people take up the invitation to tell their stories about experiences with dying and death, what do they tell’? Our secondary questions were: ‘does an opportunity to engage in storytelling and/or reading stories create the circumstances in which people are motivated to think about dying and death?’; and ‘when people are invited to tell their stories about dying and death and they do not take up the invitation to tell their own, why do they not?’
Ethics approval was granted by the Research Ethics Board at Memorial University (#2016.139). Notices posted within a Reflection Room acted as information and consent. The notice explained how to participate, that participation was voluntary, and that the reflection cards were part of a research project. Participants were advised to avoid including names and other identifiers if they wished to remain anonymous.
Setting and Recruitment
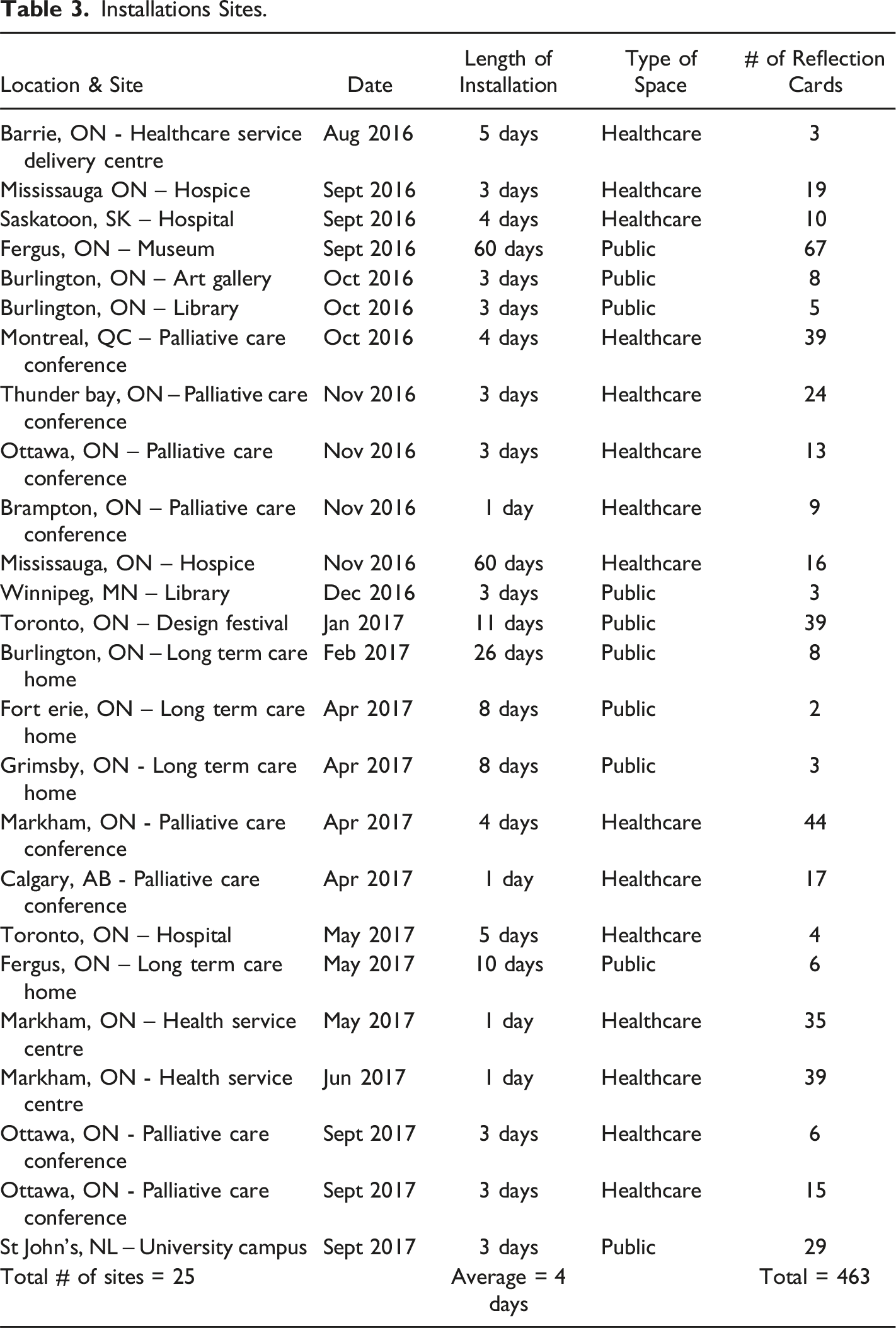
This pilot version of the Reflection Room project ran from 2016–2017, with installations set up in the two types of spaces, public spaces such as art galleries and libraries, and in healthcare-related spaces such as at provider conferences and hospices. Sites were recruited through word of mouth, social media releases, and e-mailing lists. Visitors were invited to engage with the installations via posters, with no research staff directing recruitment. Any individual entering the building where a Reflection Room was installed could participate. No people who volunteered were excluded; cards were regularly reviewed, and those with discriminatory language were removed.
Data Collection
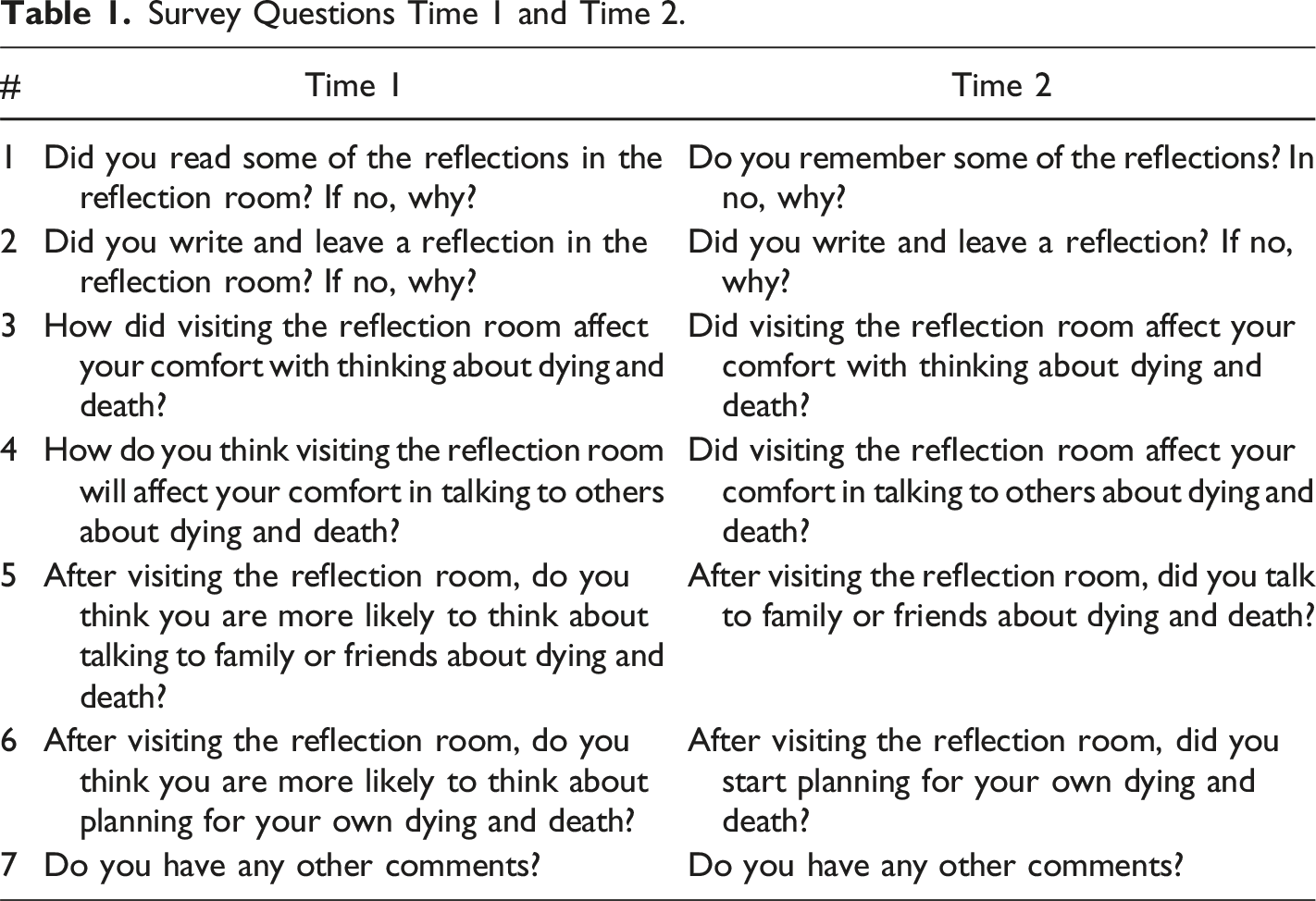
Two sources of data were collected. Reflection Cards were compiled, scanned, and transcribed verbatim, not correcting spelling mistakes or grammatical errors (See figure 2). The second source of data was paper-based surveys voluntarily completed by visitors exiting a Reflection Room (Time 1). Respondents could provide their email address to participate in an electronic follow-up survey 3 months later (Time 2). This interval was chosen to allow the respondents time to experience any change in their thoughts, feelings, or behaviour after visiting a Reflection Room. The two seven-question surveys were designed by the research team. Questions at Time 1 asked about anticipated impacts, and questions at Time 2 asked if any changes had occurred (see Table 1 for survey questions). Survey response options included yes/no, open-ended, and multiple-choice responses. We did not specifically measure changes in social connections or well-being because it would be challenging to attribute these changes to a Reflection Room alone and because our aim was to increase comfort with the topic of dying and death. Example of a scanned reflection card. Survey Questions Time 1 and Time 2.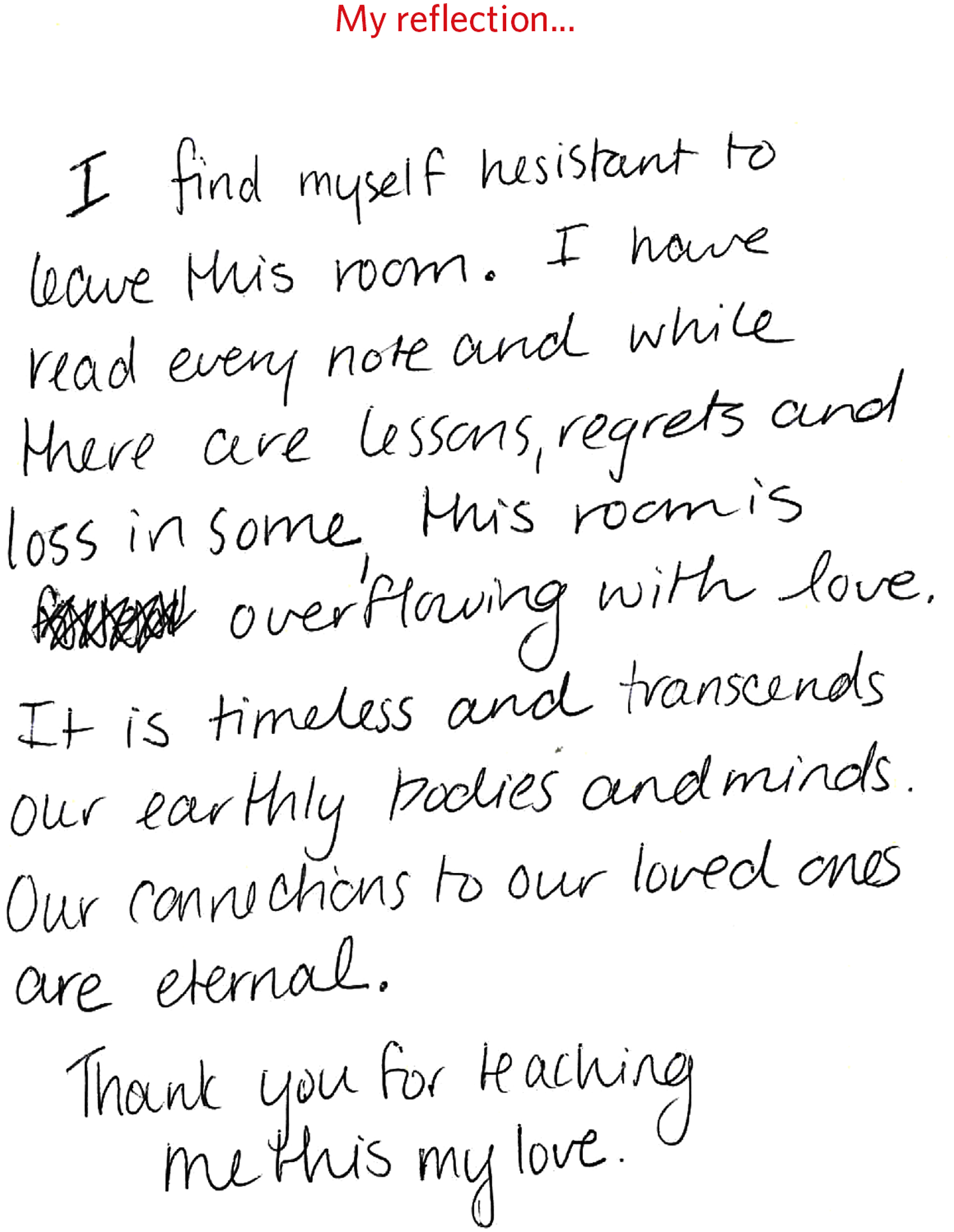
Analysis
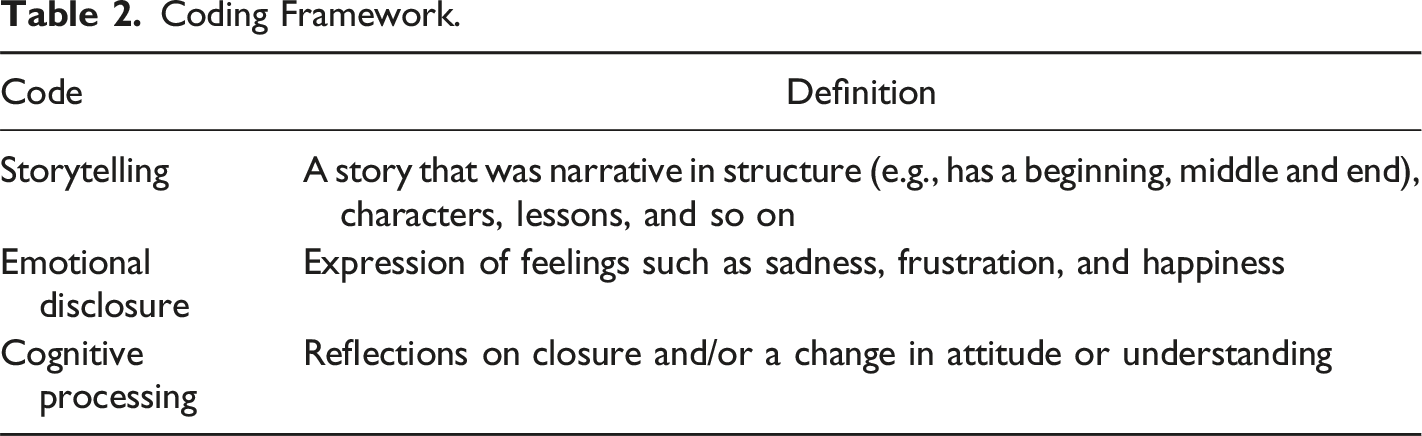
Coding Framework.
Findings
Installations Sites.
The Reflections Shared
Four hundred and sixty three reflection cards were shared and posted across the 25 sites within 13 months in response to the question, “write about your experiences with dying and death”. We examined both the form of reflections and the content of what was written.
Writing Form of the Reflection Cards
Three forms of reflections were shared: stories that met our definition of story in Table 1, and two other unexpected forms, utterances, and letters. Two hundred reflection cards (43%) were categorized as stories because they had a narrative structure with a beginning, middle, and end with characters and a moral or lesson. For example, one reflection contained this story: As an RN working at the hospital I was asked to head to the ICU department to bring a patient back to our palliative floor as the family had made the decision to take an EOL approach. I went with a college to bring our patient back, as we did the majority of the family opted to go home/shower/rest as they had been up for the better part of 2 days with their father. Our patient’s wife did not leave but came with us and helped with the transfer. When we got our patient settled, we the nurses asked his wife what we could do for her. All she wanted was to be with her husband. So at this point we were all ready to make this happen. He was a big/tall man that took up most of the bed but we were able to erect just enough room to help his wife climb into bed and lay with him. This is where she stayed for the next hour and was able to be with him as he took his last breath.
One hundred and thirty seven reflection cards were categorized as utterances (30%). Utterances were often shared in the form of quotes, advice, ideas and wishes. Two examples of reflections that were utterances include: The Creator knows our path in life long before we are born. We just need to embrace that and recognize that there is a greater plan for us I just wish I knew. I just wish I knew then what I know now when my grandmother was dying 20 years ago
One hundred and twenty sixtwenty six reflection cards were categorized as letters (27%). Letters were written explicitly to someone. While they were posted publicly, they did not seem to be written for the public but as a way of communicating thanks or regret to someone important to the writer. Letters were often addressed to a deceased person, but some were addressed to health care staff or other individuals. Here is an example of a reflection that was written as a letter: Wish I could go back in time. Too [sic] spend more time with you. Get you more flowers, hold your hand. All the things you liked to do, I would do it. I was absolutely heart broken when you left us so suddenly. No chance to say good bye. Just gone. No one to be my champion to pick me up when I was sad. You made me who I am. You were my idol. A piece of me went with you. I miss you so much. Until we meet again All my love. XO
Content of the Reflection Cards
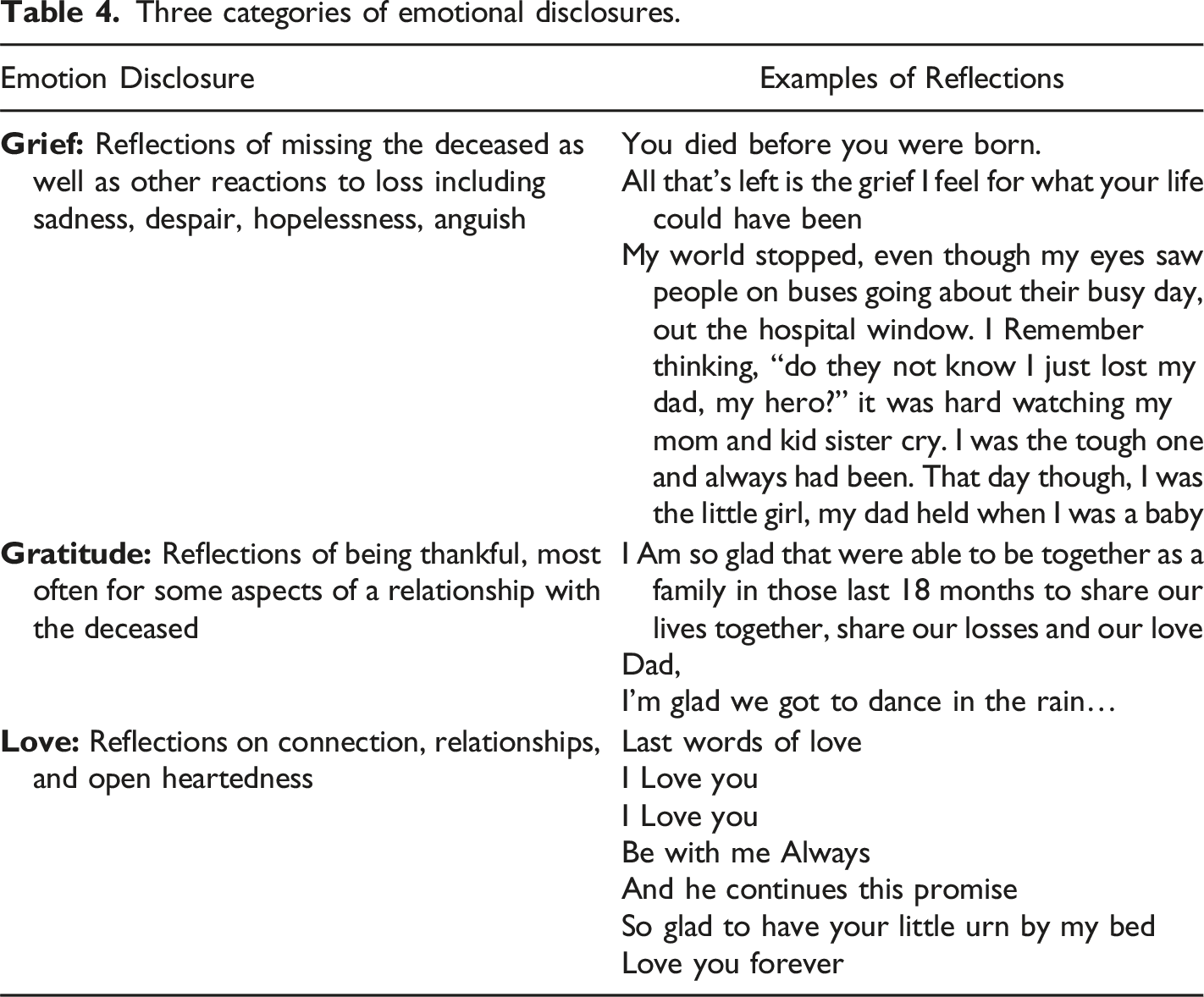
Three categories of emotional disclosures.
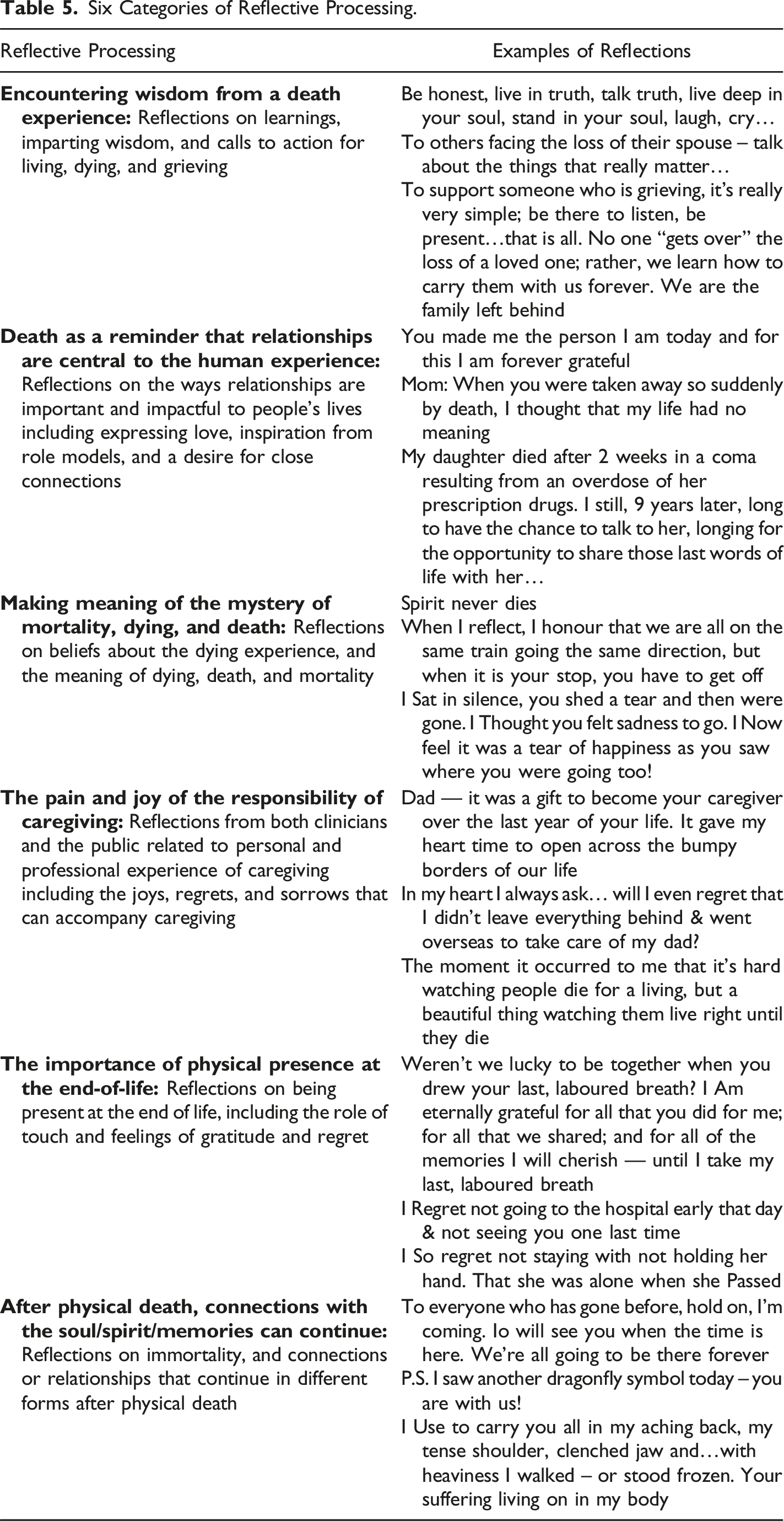
Six Categories of Reflective Processing.
Increasing Comfort with Dying and Death
Two hundred and seventy one Time 1 surveys were returned, and 50 Time 2 surveys were returned 3 months later. At Time 1 68% (n = 179) of respondents selected the responses “a bit more comfortable” or “a lot more comfortable”’ when asked how visiting a Reflection Room affected their comfort with thinking about dying and death. Seventy eight percent (n = 204) of respondents selected the response options ‘a bit more likely’ or ‘a lot more likely’ when asked how visiting a Reflection Room will affect their comfort in talking to others about dying and death. When asked if they were more likely to think about planning for their own dying and death, 44% (n = 109) selected the response ‘definitely, yes’, with another 33% (n = 83) selecting the response ‘maybe’.
At Time 2 69% of respondents (n = 34) felt “a bit more comfortable” or “a lot more comfortable” thinking about dying and death, and 74% (n = 37) were ‘a bit more likely’ or ‘a lot more likely’ to talk to others about dying and death. We also found visiting a Reflection Room led some respondents to take actions aligned with death awareness. Seventy eight percent (n = 39) answered yes when asked if they had talked to family or friends about dying and death, and 32% (n = 16) answered yes when asked if they had started planning for their own dying and death.
Based on open ended comments within the Time 1 and Time 2 surveys, some responses (n = 29 at Time 1 and n = 15 at Time 2) indicated the Reflection Room project did not increase comfort with, or likelihood of talking about dying and death because the respondent was “already very comfortable” and “already talks a lot about it”. However, other open-ended comments within the two surveys provide context into why the intervention did increase most respondents’ comfort talking and thinking about dying and death. Respondents said a Reflection Room offered a place to express emotions (e.g., “Very moving experience! The room really is powerful reflecting on my personal experience and provides an environment of open, true expression!”) and contemplate (e.g., “This was a lovely secret space to reflect deeply, quietly on loss for me”). Respondents said the experience was cathartic and peaceful (e.g., “What I think this does is normalize the experience and helps you to express personally what someone who died meant to you. It also allows to write down regrets hopes and wishes. That is cathartic” And “Very inspiring, a real comfort in grieving, so peaceful.”). Some also shared the experience supported social connections (e.g., “It was comforting/validating to read the thoughts of others” and “Great community building!”).
The Need for More Reflective Time
Reasons for not leaving a reflection.

The ‘other’ reasons respondents did not leave reflections were shared in short answer comments. These included: (1) they had no experience with loss (n = 8) (e.g., “Don’t have an experience to share”); (2) it would elicit too much emotion (n = 10) (e.g., “I might not stop crying if I do so here now”); (3) they needed more time to write something meaningful (n = 15) (e.g., “Still thinking about it”); and (4) reflections are private (n = 6) (e.g., “I chose not to share my personal thoughts”).
Discussion
Many research-based storytelling interventions supporting death-related fears, grief, and/or comfort with EOL, are facilitated therapeutic interventions for specific populations (Neimeyer, 2016; Otto et al., 2016). The Reflection Room project is one of the first research-informed storytelling initiatives that is unfacilitated, designed for a broad audience, and shown to be helpful in increasing comfort thinking and talking about dying and death as well as influencing people to contemplate as well as start planning for their own death. While a storytelling framework guided this work, when people were invited to share their experiences, they shared it in three forms: utterances, letters, and stories. Future work could examine how these different writing forms could support death awareness initiatives.
Schenker et al.’s (2015) model indicates that through storytelling, people experiencing loss form social connections, disclose emotions, and process thoughts, and these together support mental health and emotional well-being. Other research indicates storytelling related to dying, loss, and grief can have affirming, healing effects on both the storyteller and those who hear or receive the stories (Pangborn, 2019; Rolbiecki et al., 2021). With about half of our Time 1 survey respondents indicating they read but did not write a reflection, more work is needed to understand the impact of not just writing but also receiving stories and how this shapes comfort with dying and death. Returning to the spiritual care principles, it may be that cognitive processing is supported by visiting a Reflection Room that is experienced as special and allows questions to emerge. It is also possible that without writing a reflection visitors feel “witnessed” in readings other’s stories that resonate with their own experience and that the embodied processing occurs by being in the room.
While this study did not evaluate how visiting a Reflection Room impacted social connection or mental well-being, from open text comments in our survey responses, there is some indication that feelings of connection developed with others by reading stories by visitors who engaged with a Reflection Room. Some respondents also felt a sense of catharsis. It appears there is potential for future research to explore an expanded version of Schenker et al.’s (2015) model that incorporates how various reflective writing and the reading of stories supports the therapeutic aspects of storytelling initiatives related to the EOL.
The content of the reflection cards primarily expressed the feelings of love, grief, and gratitude; the centrality of relationships; and how experiences with death generate wisdom. This aligns with other research explaining that attachment between people is vital for survival, cooperation, and culture, and grief is a normal part of experiencing a disruption in these life-affirming attachments (Lund et al., 2021). Simply put, “grief is a by-product of love” (Lund et al., 2021, p. 4) and so it follows reflections on relationships, love, and grief, would emerge together.
A body of literature exists on death experiences being a generative time for learning and growth (Hogan et al., 2001). While most wounds of loss never go away, there can be meaning that arises from death experiences such as new understandings about life and wisdom about how to carry on (Genest et al., 2021; Hogan et al., 2001). Spiritual practices such as using reflection to connect with oneself and processing through writing or other arts-related practices, support learning and personal growth after bereavement (Hidalgo et al., 2022). Spiritual practices that foster feelings of connection, a sense of peace, and making meaning can also result in a sense of gratitude for what was (Holland & Neimeyer, 2005). This research helps to elucidate why visiting a Reflection Room elicited peoples’ expressions of wisdom and gratitude.
We suggest the key elements of the mobile Reflection Room that increases peoples’ comfort with dying and death includes: (1) providing an opportunity to share and receive stories; and (2) spiritual care elements that encourage quiet calm spaces and dedicated time to process. Reflective time appears to be important based on the responses that many people did not write a reflection because they wanted more time to contemplate and articulate something meaningful. Others who wish to support death awareness could consider how they invite ample opportunity for quiet reflection. The results also suggest the immersive and unfacilitated nature of the mobile Reflection Room are important features. This design allows different people to engage with the topic of death regardless of being pre-contemplative or curious but not ready to share one’s own story.
Visiting a Reflection Room led most respondents to feel ‘a bit’ or ‘a lot’ more comfortable thinking about dying and death, talking about it, and planning for their own death. When asked 3 months later, most respondents had talked to a family or friend about dying and death, and about a third had started planning for their own death. More comfort talking about dying and death is thought to be beneficial as it may make it more possible for peer-support within a public health palliative care approach to thrive (Abel, & Kellehear, 2022; Breen et al., 2022) and perhaps support access to palliative care, increasing patient, family, and clinician well-being (Malhotra et al., 2022).
Our findings indicate that the Reflection Room project supports death awareness and may also encourage engagement with ACP. Talking about and/or planning for ones’ dying and death is typically avoided, with about 77% of Canadians thinking it is important to discuss ACP with clinicians, yet only 7% stating they have done so (Advance Care Planning, 2021). Our findings did not explicate why some people might be more likely to engage in ACP after visiting the Reflection Room, however, it may be related to increasing comfort thinking about the EOL. Sharing stories about dying and death has been shown to reduce people’s reservations about ACP (Mroz et al., 2022). With ACP being beneficial for supporting communication between the patient-caregiver-clinician triad (Morrison et al., 2021; Malhotra et al., 2022), future research could explore how quiet reflection and storytelling supports people to engage in this practice.
As we continue to engage in Development Evaluation of the Reflection Room project we will be adapting, designing, and evaluating based on our learnings of this pilot specifically investigating how the design and setting of a site impacted engagement. In subsequent versions of the Reflection Room project, we will explore how to invite more reflective time and how the length of installation periods affect outcomes including how visiting a Reflection Room might provide social connections and support well-being.
Limitations
Due to the design of our study and the goal to be as non-invasive as possible we did not gather participant data and therefore cannot describe our participants beyond location of the installations. Additionally, the design of the study also made it impossible to link reflection cards and survey responses in our analysis. Our findings might also not be reflective of the general population due to many installations being hosted in palliative care settings with people visiting who might already be somewhat comfortable talking about dying and death. We also note three limitations regarding accessibility and inclusion. The first is that the focus on writing a reflection as opposed to drawing for example, limits who can participate. The second is that the placement of a Reflection Room in specific public places may limit inclusion of diverse experiences. The third is that the Reflection Room was only available in English. In the future we would want to support linguistic diversity.
Conclusions
To foster supportive experience of dying, death, and grief at the societal level, there is a need to address peoples’ discomfort in thinking and talking about dying and death; at the societal level, we also need to create more opportunities to reflect on dying and death. Our findings point to how visiting a Reflection Room offers an immersive arts-based storytelling space accessible to a wide variety of people, which provides the opportunity to share and receive stories and have quiet time to process thoughts and emotions. Our results are promising as most respondents had increased comfort thinking and talking about dying and death as well as an increased likelihood of engaging in ACP. This increased comfort may strengthen communication between patients-caregivers-clinicians at the EOL, lead people to be more likely to access timely EOL care, and increase peer support for the dying, grieving, and caregiving, however, this is yet to be determined.
Footnotes
Acknowledgments
We’d like to acknowledge the SE Research Centre members who have been involved in the study over the past 5 years, the Saint Elizabeth Foundation, the many organizations that have hosted a Reflection Room, and all those who have visited a Reflection Room and shared a reflection or read the reflections of others.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies