
Abstract
There is limited knowledge regarding Colombian patients with advanced cancer preferences regarding their final moments, place of death, and post-death wishes. To better understand these preferences, we conducted 23 in-depth interviews with patients between the ages of 28 and 78 receiving treatment at two academic hospitals and the National Cancer Institute. While many participants desired a peaceful death, few were comfortable discussing the topic of death directly. Some younger participants expressed an interest in euthanasia but had not received any guidance or support. While several participants preferred a home death, some expressed a desire to die in a hospital due to better symptom control. Additionally, when discussing post-death wishes, some participants expressed frustration about being unable to have these conversations with their loved ones and their preferences for funeral arrangements. Socioeconomic and geographical factors significantly impacted the wishes and preferences expressed, with many individuals hesitant to initiate difficult conversations.
Introduction
Cancer is a chronic disease with an increasing incidence worldwide. In Colombia, cancer is one of the leading causes of death, and an estimated 54 987 people died from cancer in 2020 (Ferlay et al., 2010). According to the Cancer Country Profile 2020, cancer was responsible for 36.1% of non-communicable diseases’ premature deaths in Colombia (World Heath Organization, 2020). When the disease progresses to advanced clinical stages, patients progressively develop symptoms such as pain, loss of appetite, fatigue, and breathing difficulties (Hughes et al., 2015; Van Lancker et al., 2014). The presence of such complications and the decline in functionality often leads to the development of patients’ desires and preferences regarding end-of-life-related issues, including wishes regarding the moment of death, such as the place of death, ways of dying, the desire to speak with significant others before dying, and wishes related to the disposition of the corpse (Bergenholtz et al., 2020; Ohnsorge et al., 2019). These wishes differ from person to person, depending on culture and personal circumstances, quality of life, patients’ age, type of cancer, and comorbidities (Brown et al., 2001; Rojas-Solano & Salas-Herrera, 2002).
Palliative Care (PC) is a holistic treatment strategy to accompany and relieve patients’ symptoms (Saunders, 2001). Within PC, decisions involving the end-of-life help patients accept their relatively imminent death and begin to think about their dying process (Llauradó Sanz, 2014). Although many PC and end-of-life preferences may be shared across cultures and countries, differences may exist on specific topics (Barnato et al., 2009).
There is a lack of information regarding patients’ wishes at the end of life in Colombia and how PC in this phase is provided (Reid et al., 2021). Therefore, knowing if the currently offered care aligns with this population’s wishes is impossible. Understanding patients’ end-of-life wishes is essential to palliative care, as it allows patients to receive care that aligns as much as possible with their values, preferences, and goals. Furthermore, knowledge of the desires and real experiences of patients with non-curable cancer play a critical role in palliative care because they guide decision-making about care at the end of life. This knowledge can also enhance patients’ quality of life at the end of life, dignifying the process of dying and the experiences and grieving process for relatives and caregivers (Welsch & Gottschling, 2021).
Therefore, this qualitative study aimed to analyze Colombian cancer patients’ points of view regarding managing their disease and their wishes in the final stages of their life. Here we present the findings regarding the wishes of patients with advanced non-curable cancer involving the time that immediately precedes their moment and place of death and what happens after their death.
Methods
This qualitative study used a critical paradigm with an idealistic ontological position and an abductive epistemological vision (Green & Thorogood, 2018). We used critical realism to understand the experiences and emotions that underlie the participants’ responses and how this information provides additional meaning to their answers. This approach allowed us to explore the patients’ reality in greater detail and give a greater sense and relevance to the interpreted results (Green & Thorogood, 2018).
Selection of Participants
Participants were patients treated at Instituto Nacional de Cancerología, Hospital Universitario San Ignacio in Bogotá, and the Hospital Universitario San José in Popayan, Colombia.
We employed a parallel pairwise sampling design sample design, where all selected cases are treated as a set, and comparisons are made between them to understand the phenomenon better (Onwuegbuzie & Leech, 2007). We developed a sampling matrix that considered age, the presence of someone who depends emotionally or economically on the patient (for example, young children or elderly parents), and educational level was self-reported by the participant. The type of cancer (including the most prevalent cancers in Colombia and non-solid tumors) was reported by physicians. We ensured to have a representation of at least one participant or case for each cell of the matrix. We employed a homogeneous sampling strategy, as all participants had a common attribute: facing the end of life. Age and type of cancer were provided by the physician; marital status and the presence of a dependent person were assessed during the interview.
Inclusion criteria were: patients ≥18 years of age with an advanced non-curable cancer diagnosis with a life expectancy between 6 and 12 months who understood and accepted their illness and imminent death. Their remaining life expectancy and ability to participate were estimated by the treating oncologists and palliative care physicians who helped identify and invite the patients. Patients who, according to the physician, did not have the mental capacity to understand the purpose of the study or the questions asked or could not transmit coherent information (oral or written) were not invited.
Their treating physicians initially contacted eligible patients, who explained the study’s purpose. The interviewer subsequently contacted those who accepted, described the study’s intention and the method of collecting the information, and asked them to sign informed consent before the interviews were carried out. Two trained interviewers conducted in-depth interviews, one with postgraduate training in psychiatry and the other with postgraduate training in clinical psychology. One single interviewer carried out the data collection at Hospital Universitario San Ignacio and Hospital Universitario San José, and the other at Instituto Nacional de Cancerología. Each participant was offered the opportunity to request additional psychological or spiritual support if they felt the need to do so at the end of the interview.
Setting and Data Collection Methods
The interviews were conducted face to face (interview probes are available in the Supplementary file), in private and comfortable places within the clinics, thus facilitating the subject’s freedom of expression. The interviews were conducted following an unstructured interview script with questions regarding end-of-life wishes in advanced non-curable cancer patients concerning their palliative care and dying process.
Each interview lasted between 30 to 60 minutes. All interviews were audio-recorded with prior authorization from the subjects and transcribed within 90 days. All transcriptions were anonymized.
Data Analysis
Notes were taken within the narratives to indicate the non-verbal language expressed (laughter, crying, sighs). Notes and memos were taken from the transcript and continued throughout the process to assist in the subsequent analysis of the interviews.
A description of the characteristics of the participants was made considering the type of cancer, sex, age, marital status, and the other variables described. The coding and analysis of the interviews were carried out in Nvivo 11 (Windows, 2017).
Two coding cycles were performed. The first coding cycle, conducted by a single investigator, was opened for a more sensitive search of the data, in which the initial codes were identified. Memos about the possible emerging concepts were made based on this first analysis, as well as regarding the relationships between the narratives and traits of each individual and the potential factors that would help explain the origin or motivation behind the identified desires.
The second coding cycle was paired. Both encodings were compared. The possible new categories were discussed through consensus. The categories that raised doubts about their meaning and those grouped in broader themes representing the second level of data abstraction were evaluated (Codebook is available in the Supplementary file). The nodes with the most significant impact and those related to the purpose of the study were chosen.
Methods to Ensure Rigor
The interviewer kept a field diary (Deggs & Hernandez, 2018) where their ideas, thoughts, and emotions were captured during the interviews. MMR made a field diary while transcribing the interviews, which continued during the narratives’ analysis. This field diary was reviewed when starting the synthesis of results as a self-reflection to assess whether there was a relationship between the findings and the author’s thoughts that could have influenced the study’s conclusions.
SM, MMR, and EdV participated in the preparation of the questionnaire (available in Supplementary Materials), as well as in the training of the interviewer. MMR performed the first coding cycle. NAR performed the second coding cycle, organization, and data cleaning. This second round helped confirm some concepts identified in the first coding round, identified some additional subcategories, and reduced the influence of the first coder’s perceptions.
The study protocol was approved by the research ethics committees at Hospital Universitario San Ignacio, Colombia (number FM-CIE-0086-17) and Instituto Nacional de Cancerología, Colombia (number INT-OFI-03,581-2019). The Hospital Universitario San José in Popayan adhered to the decision by the Pontificia Universidad Javeriana.
Results
Twenty-seven patients were interviewed. However, we had to exclude one interview because the participant had severe dyspnea, which made their answers monosyllabic (yes/no), and they could not provide more in-depth information. The participants who were finally included were aged between 28 and 78 (median age 53 years, IQR 42.5–67.5). Twenty of the participants were women. The interviewees had different educational levels from elementary to graduate school, most of them with primary or, at most, secondary education.
The most frequent types of cancer among the participants were: breast cancer, cervical cancer, colon cancer (four participants each), and stomach cancer (three participants).
Twelve of them were living with their partner during the study time. The other 14 had no partner for different reasons (single, divorced, or widowed). Fifteen participants had children who depended on them. Two also had dependent parents.
The analysis considered the characteristics of each participant. The themes reported in this document reached a sufficient depth among the participants regardless of the type of hospital, cancer, sex, or vital moment (Francis et al., 2010). Several participants expressed that the interviews allowed them to discuss issues they had not discussed with their families or doctors and were grateful for this opportunity.
Throughout the results, some textual citations that justify the affirmations are presented. To give context to the reader, each quote is referenced with the participant’s sex, age, and type of cancer.
Figure 1 shows the themes and categories structure. The codebook is included in Supplementary Materials. Themes and categories.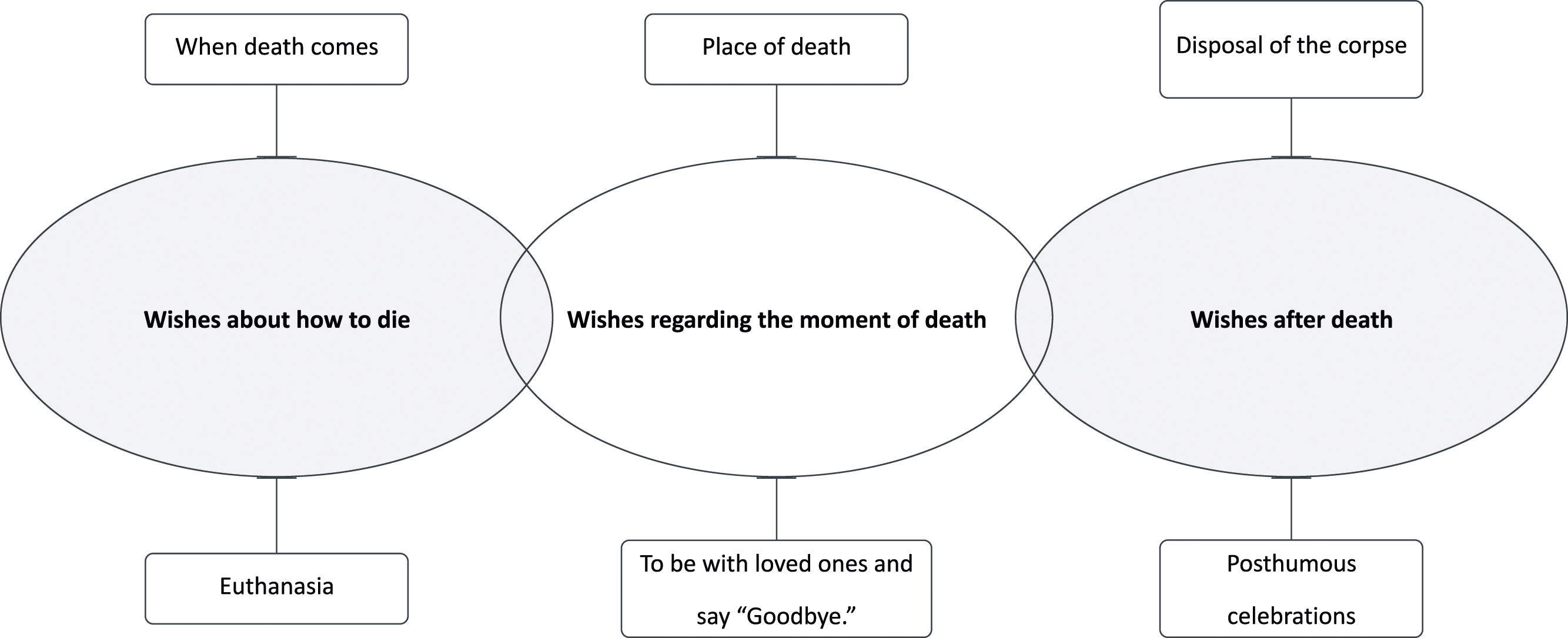
Wishes About how to Die
The participants generally expressed the desire to die calmly and peacefully. Such tranquility seems to be related to intensive symptom control – most interpreted dying calmly as being without pain at the time of death or, more specifically, without being aware of the moment death arrives. Three of the interviewees stated this in different ways: “Let me take a deep sleep, and that’s it.” (Woman, 29 years old, cervix cancer), “fall asleep and no longer wake up.” (Woman, 28 years old, colon cancer), “That one does not feel death.” (Woman, 56 years old, breast cancer).
When Death Comes
Despite their illness and awareness of their condition, some participants refused to think about their death, limiting conversations concerning these issues. Men, more than women, tended to respond by redirecting their attention to how the diagnosis was made or to statements concerning their religiosity that ignored the possibility of their death. This refusal to talk about death and everything related to it by many participants is a finding in itself. Most participants who showed a more pronounced refusal to talk about death had a technical or higher educational level.
Given the difficulty of talking about these issues, a greater instigation of the interviewer was required to obtain answers.
Euthanasia
Four participants, all young, expressed a desire to accelerate the dying process. Three of them expressed their interest in obtaining help to fulfill this purpose, such as euthanasia. These patients emphasized wanting more information about euthanasia and the difficulties those interested in accessing these services may face. They expressed wanting to seek these options when the disease significantly compromised their quality of life, “I agree with euthanasia. I’d say that if one deteriorates, has become ‘nothing’ and there is nothing to do, why to be connected to a machine, […] it seems silly to hold on then.” (Woman, 40 years old, brain cancer). “But for me, seeing that the pain is so delicate, so severe... I would like to be, I would like to be euthanized. That they would do that to me.” (Woman, 61 years old, colon cancer).
Not all participants knew that euthanasia is allowed in Colombia – some who were unaware of this possibility expressed desires to hasten death by other methods such as suicide. The following two quotations expose these feelings:
Wishes Regarding the Moment of Death
In the end-of-life process, there are decisions around the moment of death, such as how and where to die and who will be present at the time of death. Most of these wishes are influenced by other people and the patients themselves, and hopes and wishes regarding how and where to die sometimes vary over time within the same patient.
Place of Death
Although most of the participants preferred to die at home, the motivations behind this preference varied from wanting to be in the company of their loved ones to wanting to avoid difficulties for their families, such as moving the corpse back to their village in case of hospital death and the degree of morbidity and care needs expecting before dying.
Patients who anticipated a more significant deterioration of their health more frequently expressed a wish to die in the hospital “If God allows me to die at home, it is better […] if I must die here (in hospital) if it is more serious there […] more distressing for the family to take my body home.” (Man, 68 years old, stomach cancer). One of the women said, “I think that I would like to die at home where things are calmer, but I also think that I do not know what impact (dying at home) it will have on my family and the people who live there.” (Woman, 42 years old, ovarian cancer). Another one expressed, “I have told my family, wherever I am, that if I am very ill, to take me home, not to leave me in a hospital.” (Woman, 53 years, breast cancer).
Furthermore, one of the oldest participants communicated the ease of dying at the hospital: “I want to die where they are treating me. It’s ok in the hospital... because they are going to have consideration for my son... they are going to let him in. I don’t want to die at home alone... no doctor! I want to die in the hospital... where they are treating me”. (Woman, 77 years old, stomach cancer)
To be With Loved Ones and say “Goodbye”
Most participants wish to be accompanied on their deathbed, usually by their family or loved ones. Along with being accompanied, some participants explicitly mentioned a desire to say goodbye, some emphasizing the urge to apologize to loved ones, especially the family. A patient with colon cancer stated, “I still need to talk to... People. Like my mom. With significant people to whom at some point, I may have been rude […] also people that I would like to speak to and ask for forgiveness.” (Woman, 28 years old). Other one commented, “At home... With my family, I see myself in a bed (laughs) […] I would like my family to be there supporting me at that time.” (Woman, 53 years old, breast cancer). The interviewer asked one of the patients if she would like to talk to someone or ask someone for forgiveness, and the woman answered, “Just my mother, nothing more.” (Woman, 29 years old, cervix cancer).
Wishes After Death
Just as there are wishes involving the moment of death, there are also wishes that people hope will be fulfilled after their death, related to the disposition of the body or place of rest and posthumous celebrations. Conversations regarding these preferences are challenging but can represent peace to the patient and their family. In one of the interviews, a woman with brain cancer talked about if a relative did not listen to her: “No… and my children neither… they do not pay attention to me. They are like, ‘Calm down, all will be fine, nothing will happen to you.’ I do not even mention it to my friends because they’ll all be like, ‘take it easy, you should not get depressed.’” (Woman, 40 years old, brain cancer)
Disposal of the Corpse
Most participants expressed a desire to be buried at a cemetery close to their family, usually their hometown. The next conversation reflects that. Interviewee: Yes (Woman, 28 years old, colon cancer)
Only one participant described her desire for a different disposition of the corpse, contemplating ideas beyond traditional Colombian burial or cremation concepts. “I told them I would like to be cremated because I do not want them to bury me. I do not like being buried. I think that extends the pain for those who remain. It forces them to go visit bones, land […]. I would like my ashes to be left near a tree or something like that”. (Woman, 42 years old, ovarian cancer)
Posthumous Celebrations
Some patients expressed additional wishes about what they would like to happen after they die, going beyond the place of death and cemetery. Some of these wishes are associated with what they would like to happen at their funeral. “
One participant who was not religious expressed difficulties in communicating not want a religious ceremony: “I do not want religious rituals of any kind […] culturally, there are many deep-rooted things, and people cannot separate death from the religious part, so no matter how much one goes to find out, they always offer you the plan that your Mass and your things, so that is a bit shocking for me…”. (Woman, 42 years old, ovarian cancer)
Discussion
This study revealed advanced cancer patients’ wishes without a curative option regarding the last moments of their lives. There are some similarities with the wishes described in the literature regarding the desire to die at home or be able to say goodbye to loved ones (Miccinesi et al., 2012; Nilsson et al., 2017), but some results differed from literature from other places, such as the reasons behind a wish for a home or hospital death.
Colombian and Latin-American-wide studies concluded that many home deaths in Latin America, in rural and remote areas, probably indicate the absence of good healthcare services rather than what is considered a “good” death (Seitz et al., 2022). Over-treatment is still common, and referral to PC services is difficult and limited – partly because of feelings of failure among oncologists at the moment of referring to PC services (Castillo et al., 2022; Luna-Meza et al., 2021), partly probably influenced by financial incentives for oncologists to try third, fourth, or even fifth lines of chemotherapy for cancer patients.
Death has different ways of being perceived. The patient’s vision often differs from that of the family or the treating physician. Several studies have highlighted the importance of talking with the patients, knowing their perspectives, inquiring about their wishes at the end of life, and evaluating how they interact with their beliefs, education, and the social environment becomes essential to improve health care and decision-making (Rodríguez-Prat et al., 2017; Shih et al., 2015), yet these are often lacking in inpatient attention in Colombia (Calvache et al., 2021; Castillo et al., 2022; Luna-Meza et al., 2021), as was evident in some patients’ narratives.
Understanding the desires and choices of dying patients is crucial, but it is also essential to acknowledge that physicians may occasionally misinterpret these preferences (Wenger et al., 2000) or provide care that does not align with patients’ expectations (Modes et al., 2020). Identifying and understanding wishes is, therefore, an important first step but not sufficient to improve end-of-life care. Addressing and fulfilling patients’ wishes poses a continuous challenge for healthcare providers and requires consensus among stakeholders regarding what is suitable and pertinent for the patient and their family (McCaffrey & Eckermann, 2018).
Periyakoil et al. propose a model of mourning preparation known as the Preparatory Grief Dual Process Model (Periyakoil et al., 2005), which suggests that when facing death, patients experience various emotions. These emotions can be categorized into loss-oriented emotions, such as separation, shock, sadness, and anger, and restoration-oriented emotions, including hope, meaning, and relationships. The process of navigating and coping with these emotions contributes to anticipatory grief. In examining the narratives of the participants in our study, the occurrence of these types of emotions both before, during, and after death is evident. Religiosity and religious practices are particularly evident in these emotions. For some participants in our study, their religious beliefs offered them hope and reassurance (restoration-oriented emotions). In contrast, the constant offer of spiritual (religious) support, typical in Colombian hospital institutions, or the idea of religious posthumous celebrations were cause for loss-oriented emotions, e.g., anger and frustration, for those who were not religious.
The importance of family and loved ones in the Colombian culture is obvious in the answers regarding the importance of continuing bonds and the well-being of the bereaved family members after the moment of death, considering which options would be least distressing or financially burdensome for the family regarding the place of death and burial, but also desires to say goodbye and want to reduce the pain and grief for those who stay behind. This importance of considering the wishes and preferences of the family influences patients’ preferences: for most, their decision is, at least to a certain extent, influenced by the preference of their family members. Participants who mentioned that their own wishes were not aligned with those of their loved ones, asked for conversational support in communicating their wishes and considerations.
To our knowledge, existing frameworks for mourning do not incorporate euthanasia nor funeral wishes. Both issues were of importance to important groups or our participants. The way our participants managed and talked about death varied greatly. Some seemed to have loss-oriented emotions, especially sadness and shock related to their imminent death (Periyakoil et al., 2005). Even though some expressed detachment, trying to escape the topic in their responses, others stated that they feared suffering and therefore considered the possibility of accelerating their moment of death.
Most types of wishes regarding end of life were present among participants of distinct age groups, except for consideration of euthanasia or other ways to accelerate the end of life, which, in our study, was only expressed by the younger participants. Although our methodology and sampling method does not allow us to infer anything from this distribution, it seems plausible that younger generations are more open to less traditional viewpoint regarding death and dying.
Although our participants were primarily women, it is relevant to highlight that the proportion of male participants was similar to that of men who consult health services in our country. The data indicate that only 32% of health consultations in Colombia are made by men (Rodriguez et al., 2009). This disproportion in healthcare-seeking behavior between men and women is associated with virility-related reasons, such as not seeking preventive services or not requiring health services to solve their problems (Organización Panamericana de la Salud, 2019). In addition, there is evidence that men’s coping strategies in the face of illness promote emotional distancing and the absence of expression of emotions and feelings (Organización Panamericana de la Salud, 2019). Despite this context, we found no differences between the wishes of men and women about death and dying.
In Colombia, specialized services in oncology and PC are still scarce. Specialized hospitals and home-based care are primarily available in the main cities. Over-treatment at the end of life is common, and hospice care is virtually non-existent (Gempeler et al., 2021). This represents a barrier to cancer patients – many of them need to migrate to a city for medical attention (NCDs | Global Atlas of Palliative Care at the End of Life, 2015; Soto-Perez-de-Celis et al., 2017), including strong financial barriers (de Vries et al., 2021) Therefore, the specific reasons for preferences for home or hospital-based deaths could be linked to the health system context.
Several patients expressed a fear of being abandoned by the system once they would receive only palliative care, and many were worried about being a burden to family members – they expressed this as one of the reasons to want to be attended to in the hospital as the disease progresses. Other reasons mentioned to prefer to die at the hospital, although the patient would like to be at home, are caused by worries about practicalities regarding the displacement of the corpse, highlighting the great potential for improvement and the importance of local specific circumstances in these wishes. Another study has shown that many Colombian caregivers face substantial economic sacrifices for caring for an ill family member (de Vries et al., 2021).
A strength of this study is the relatively high number of participating patients, which allowed obtaining enough width and depth of the spectrum of patients dying from cancer regarding the type of cancer, time of life, and support network composition (Francis et al., 2010). The participants had different socioeconomic and cultural characteristics, which enriched our results, allowing us to generate emerging categories in what we know about patients’ end-of-life wishes with non-curable cancer. Our study included participants from different realities of Colombia (public and private institutions and patients from the cities but also from rural areas who had to travel to these cities for attention). However, we recognize our country’s great geographical and cultural diversity and lack of representation of other regions and cultures that could exemplify cultural or social differences in terms of the conception of death or other aspects. Even though we faced a taboo concerning talking about death (Luna-Meza et al., 2021), we were able to explore the meaning of death and dying with our participants, who expressed relief and gratitude for this opportunity. It is crucial to gradually break this taboo, as this hampers the achievement of patients’ desires and impedes optimal decision-making processes, leading to suboptimal communication and potentially suboptimal care and symptom management (Onyeka et al., 2013; Shen & Wellman, 2019).
Evaluating saturation in qualitative studies is a complex task because it involves a stage where enough knowledge of each concept is achieved within the situation of interest and enough data to exemplify and support the findings (Saunders et al., 2018). In this study, we did not pretend to reach a saturation point; however, we believe we have obtained enough depth in the responses. In the results, we highlighted what was mentioned by most participants as it represents the same thought in people with different conditions, those experiences mentioned by a minority were also analyzed to know the variability of their response. The ones different from those described in the literature were mentioned here. One of the wishes of most significant interest was those related to reducing treatments or wishes for euthanasia or considering suicide, primarily expressed mainly by young patients of higher educational level and some prior knowledge about the subject. It is possible that the older or less educated participants did not mention or consider euthanasia due to historical and religious influences, lack of knowledge, or taboo. This could be explored in future studies.
Conclusions and Recommendations
It is important to know patient preferences regarding the place of death and the disposition of their body to try and align care with those preferences. Many patients need help initiating conversations with their loved ones regarding their wishes and fears, an essential issue in accepting the disease. Even so, communication skills are part of medical training; healthcare personnel should strengthen these skills to inquire about the end-of-life wishes of patients with cancer. Likewise, the participation of families in decision-making is fundamental from the perspective of our patients. Patients explicitly asked for the mediation of the health/social care team to encourage and facilitate the expression of patients’ end-of-life wishes, and teaming up with families is indispensable for the care and attention of this type of patient in our context. This help could consist either of support to caregivers, help in initiating conversations with loved ones to communicate the individual wishes of the patients, or even resolving strongly differing preferences for future treatments. Efforts should be directed to fulfill the patient’s wishes, providing some peace in their dying process. It is vital to encourage the generation of advance directives to give them autonomy even at the end of their lives, such as therapeutic limitation (no resuscitation maneuvers, no intubation, no ICU) or palliative sedation as options to dignify the moment of death.
Our findings could inform the debate on end-of-life care with Colombian patients’ wishes, the possible relationships with our culture, and shortcomings in our health system that potentially affect the quality of life and death of patients with non-curable cancer. We must begin to see patients with non-curable cancer more comprehensively, go beyond treatment, and improve the support we are giving to this population and their families and caregivers.
Supplemental Material
Supplemental Material - End of Life in Patients With Advanced Non-curable Cancer: Patient Considerations Around the Moment of Death
Supplemental Material for End of Life in Patients With Advanced Non-curable Cancer: Patient Considerations Around the Moment of Death by Socorro Moreno, Mauricio Medina-Rico, Katalina Osorio Clavijo, Nicole A. Rodríguez, Víctor M. Vicuña Jiménez, Jose A. Calvache and Esther de Vries in Journal of Death and Dying.
Footnotes
Acknowledgments
Thanks to patients for sharing their fears, hopes, and points of view with us. We would also like to thank healthcare professionals in Hospital San José de Popayan and Instituto Nacional de Cancerología for their support. Finally, our gratitude to María Jose Sarmiento for conducting the interviews and to Ligia Elena Del Toro Osorio for facilitating the interview process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Minciencias, in the framework of the “777-2017 Convocatoria para proyectos de ciencia, tecnología e innovación en Salud 2017”, Decisiones médicas al final de la vida en pacientes oncológicos en Colombia (Project CT-826-2018)”. Minciencias (Colombian government research funding body). The funder had no influence in the design of the study, the collection, analysis, and or interpretation of the data nor in writing the manuscript.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.