
Abstract
This study aimed to estimate the prevalence of prolonged grief (PG) during the COVID-19 pandemic and to analyze associated variables. 142 family members of patients who died during the lockdown at a hospital were surveyed 6 months after the death. Prolonged grief, depression and anxiety, grief rumination, and loss-related variables were captured. Logistic regression analyses were conducted to detect the associated variables of PG symptoms. Prolonged grief was present in 44.4% of the bereaved. 76.2% of the relatives reported feeling distressed due to visitor restrictions, and the majority of them were unable to bid farewell to their family member at the time of death. Pastoral or psychological care was also lacking. Low education (p < 0.001), emotional closeness (p = 0.007), loss of a spouse (p < 0.001), inability to bid farewell after death (p = 0.024), feeling of threat due to the pandemic (p < 0.001), depression (p = 0.014), and anxiety (p = 0.028) were significantly associated with prolonged grief.
Introduction
Since 2020, the world has been facing various lockdown phases due to the COVID-19 pandemic (Koh, 2020). To contain the pandemic, physical contact has been limited, which can cause psychological distress for many people (Pedrosa et al., 2020). This applies particularly to hospitalized individuals and their family members who have to deal with challenges such as communication with medical teams, restricted visitation, and changes to post-mortem rituals (Greenberg et al., 2022; Valley et al., 2020). Qualitative analyses suggest that these challenges, along with patients' isolation and interruptions in relationships, may lead to prolonged grief (Dennis et al., 2022; Kentish-Barnes et al., 2021).
Prolonged grief (PG) refers to severe and persistent grief reactions that occur after the loss of a significant person. PG is currently gaining more attention due to its inclusion in the ICD-11. It is characterized by symptoms such as persistent and pervasive longing for the deceased and intense emotional pain, which have to persist for more than 6 months and cause significant impairment in functioning (World Health Organization, 2018).
PG occurs in approximately one out of 10 bereaved persons (Lundorff et al., 2017), and may have been more prevalent during the pandemic (Bertuccio & Runion, 2020; Eisma et al., 2020; Tang & Xiang, 2021, 2021van Mol et al., 2022). However, some studies have found no difference in grief severity during the pandemic compared to before, but more severe acute grief reactions (Eisma & Tamminga, 2020). The authors suggested, that dealing with loss may be more difficult during this ongoing health crisis. Known predictors of PG include marital closeness, lack of preparation for the death, female gender, psychological problems, unnatural death, and a lack of social support (Lobb et al., 2010; Nielsen et al., 2017). To understand if these factors remain the same during the pandemic, it is crucial to analyze the occurrence of PG in persons who lost their loved ones during lockdowns. Therefore, this study aims to answer the research question: (1) Do bereaved relatives experience more severe prolonged grief symptoms when their loved ones died during COVID-19 lockdown compared to non-lockdown periods? (2) To what extent are specific variables, such as the ability to bid farewell, the relationship with the deceased, or anxiety, associated with PG in bereaved relatives, 6 months after the person's death?
Methods
Procedure
The cohort of patients who passed away during the first and second German lockdowns (March 15th, 2020 to May 31st, 2020, and December 13th, 2020 to February 28th, 2021) at a German university hospital were registered in the pathology department. Six months after the patients' deaths, bereaved relatives were invited to participate in a survey by receiving a letter of invitation and three questionnaires sent to the postal address of the deceased person, along with a return envelope. The bereaved relatives filled out the questionnaires and returned them to the study center. To be included in the study, relatives had to be a family member of the deceased person during the first or second lockdown and have sufficient knowledge of the German language.
Prevalence of Prolonged Grief in the Study Sample and in Comparison Studies Before the Lockdown.
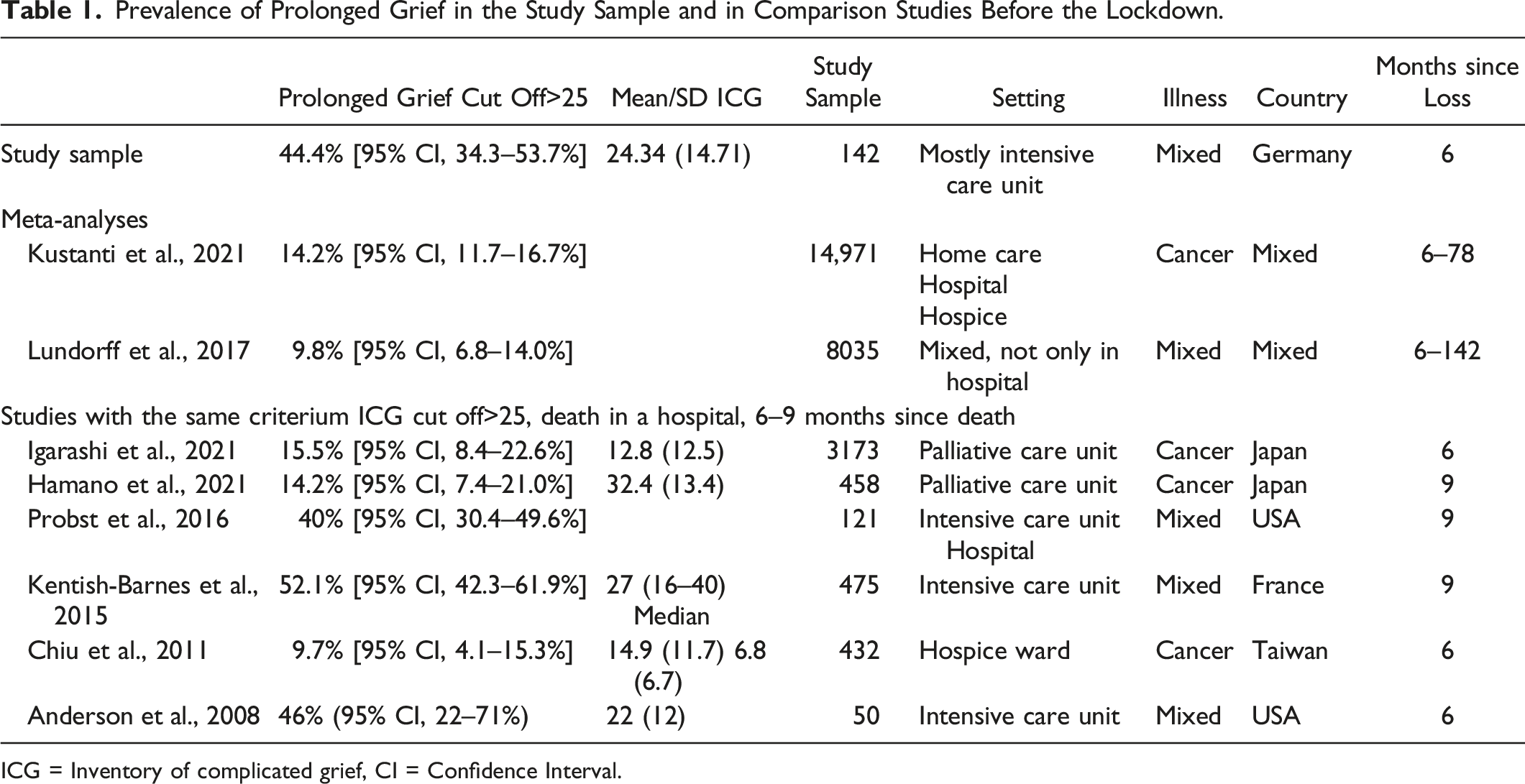
ICG = Inventory of complicated grief, CI = Confidence Interval.
The study was approved by the institutional review board of the department of medicine at the Philipps University of Marburg (178/20) and was preregistered at the German Clinical Trial Register: DRKS00023713. The study was conducted in accordance with the STROBE guidelines for observational studies to ensure transparency and reporting quality.
Measures
Demographic and grief-associated variables
Participants were asked to provide demographic data (age, gender, years of education, working status) and grief-associated information. Grief-associated variables included relationship to the deceased (i.e. partner/spouse, parent, child, sibling), cause of death (i.e. cancer, COVID-19 etc.), possibilities of communications (i.e. telephone, video telephone), emotional closeness (five-point-Likert scale from “1 = not close” to “5 = very close”) and farewell before and after the death (yes/no). Moreover, participants stated if they felt threatened by the COVID-19 pandemic (eleven-point-Likert scale “0 = not distressed” to “10 = very distressed”), if they felt distressed due to the visitors restrictions (five-point-Likert scale from “1 = never” to “5 = always”), if they desired psychosocial support during the lockdown-phase and now (five-point-Likert scale from “1 = never” to “5 = always”) and if they received the offer of psychosocial support (five-point-Likert scale from “1 = never” to “5 = always”).
Prolonged grief
The Inventory of Complicated Grief (ICG) in its German version was used to measure prolonged grief, as it has been shown to be a reliable and valid tool for assessing this construct (Lumbeck et al., 2013; Prigerson et al., 1995) The scale consists of 19 items that assess the immediate thoughts and feelings related to the loss experienced by the participant. The answers are rated on a five-point Likert scale ranging from 0 (never) to 4 (always), and an overall sum score is calculated. A cut-off value of 25 on the ICG was used to identify individuals with prolonged grief, consistent with previous research that suggests this value has good sensitivity and specificity for identifying individuals with prolonged grief disorder (Prigerson et al., 1995). Specifically, studies have shown that individuals with ICG scores above 25 are more likely to experience clinically significant distress and impairment in daily functioning related to grief symptoms. This cut-off value has been used in previous studies and is consistent with the diagnostic criteria for prolonged grief disorder in the International Classification of Diseases, 11th Revision (ICD-11). The internal consistency was good to excellent for both the original (Cronbach’s α = .94) and the German version (Cronbach’s α = .87). In this study, internal consistency was also excellent (Cronbach’s α = .93).
Grief Rumination
To measure grief rumination, the Utrecht Grief Rumination Scale (UGRS) was used, as it has been shown to be a reliable and valid measure of this construct (Doering et al., 2018; Eisma et al., 2014). The UGRS includes five subscales and one overall score, allowing for a more comprehensive assessment of grief-related rumination. Answers are rated on a five-point Likert scale ranging from 1 (never) to 5 (very often), at which the answers indicate the frequency of rumination-related thoughts and behavior in the last month. The internal consistency was excellent for the overall score UGRS (Cronbach’s α = .90) and good to excellent for the subscales (reactions α = .84; injustice: α = .88; counterfactuals: α = .89; meaning: α = .84; relationships α = .74) (Eisma et al., 2014). In this sample, Cronbach’s alpha was also good to excellent (α = .89).
Symptoms of anxiety and depression
Symptoms of anxiety and depression were measured using the Hospital Anxiety and Depression Scale (HADS), which is a well-established measure of these constructs (Herrmann-Lingen et al., 2011; Zigmond & Snaith, 1983). The HADS comprises subscales for anxiety and depression, each ranging from 0 to 21, and an overall sum score, which provides a comprehensive assessment of these symptoms. A score is calculated for each subscale, and the results are classified as indicating minor distress (<15), moderate distress (15–21), or severe distress (>21). The internal consistency of the subscales was found to be good, with Cronbach's α of .80 for anxiety and .81 for depression. Additionally, the current study demonstrated excellent reliability for the depression subscale (α = .90) and very good reliability for the anxiety subscale (α = .86).
Participants
During the first phase of the German lockdown (15.03.2020–31.05.2020), a total of 190 patients passed away in the University Hospital of Marburg. On November 30th, 2020, we sent 189 letters to the addresses of the deceased, which contained a brief description of the study, three questionnaires, and a return envelope. One patient was excluded from the study due to an ongoing criminal investigation. Unfortunately, 24 of the letters (12.7%) were returned unopened due to delivery issues. In the first round, we received 65 completed questionnaires back. During the second phase of the lockdown (13.12.2020–28.02.2021), a total of 220 patients passed away. On July 12th, 2021, we sent the study materials to the corresponding addresses. Unfortunately, 29 letters (13.2%) were returned unopened due to delivery problems. In the second round, we received 78 questionnaires back. One questionnaire from the first round was answered incompletely, resulting in a total sample size of n = 142 participants for analysis.
Data Analysis
The data were analyzed using SPSS version 26. Missing values, which ranged from 1.5% to 2.3%, were imputed using the expectation maximization method. Prolonged grief was determined using a cut-off score above 25, and 95% confidence intervals were calculated for all comparison studies based on the z-contribution.
Differences between participants from the two different waves of data collection were calculated using t-tests and chi-square tests. Logistic regression analyses were performed to examine the association of various variables, including psychological, loss- and lockdown-related, and demographic factors, with prolonged grief symptoms. Prior to conducting the logistic regression analyses, a power analysis was conducted using G*Power 3.1.9.7 software to estimate the required sample size. Based on the power analysis with a desired statistical power of 0.80, and a significance level of 0.05, the sample size required was estimated to be 140. To account for any potential bias or instability in the results, bootstrapping was employed with a resampling size of 1000.
Results
Sample Characteristics
Demographic Characteristics of the Sample and Logistic Regression Analysis.
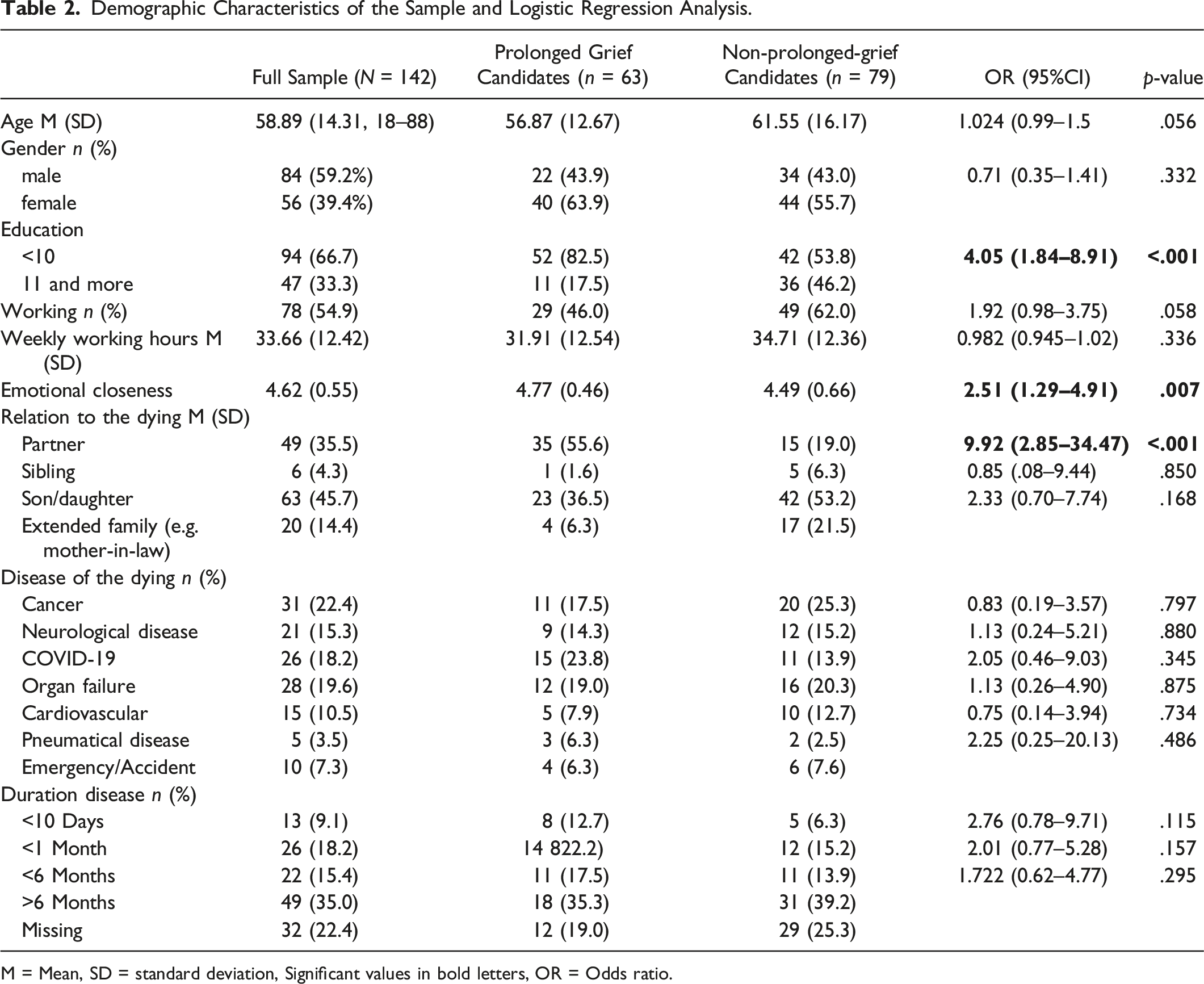
M = Mean, SD = standard deviation, Significant values in bold letters, OR = Odds ratio.
Prevalence of Symptoms of Prolonged Grief
Out of the 142 bereaved participants in our study, 63 (44.4%) showed a critical amount of PG symptoms (defined by an ICG-D score >25), whereas 79 (55.6%) did not. In the two current meta-analyses the prevalence were 14.2% and 9.8% (Kustanti et al., 2021; Lundorff et al., 2017). In comparison studies asking bereaved relatives of patients that died in intensive care unit, the prevalence of PG was similar (40–52%) (Anderson et al., 2008; Kentish-Barnes et al., 2015; Probst et al., 2016). In comparison studies analyzing bereaved family members of patients who died in a palliative care unit or hospice ward showed a lower prevalence of 9.7–16% (Chiu et al., 2011; Hamano et al., 2021; Igarashi et al., 2021).
Grief-Associated Variables
Loss- and Lockdown-Related Variables (Logistic regression analysis).
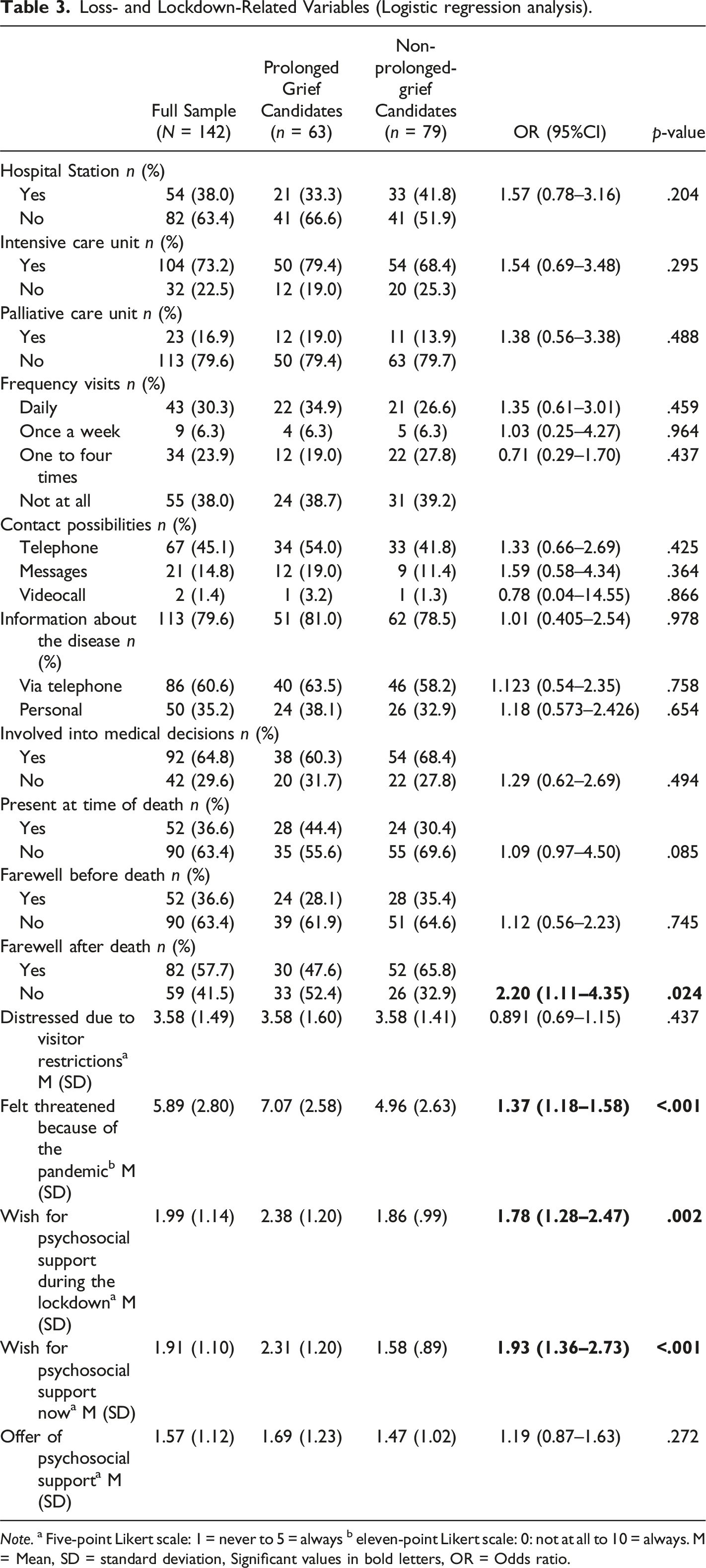
Note. a Five-point Likert scale: 1 = never to 5 = always b eleven-point Likert scale: 0: not at all to 10 = always. M = Mean, SD = standard deviation, Significant values in bold letters, OR = Odds ratio.
Psychological Variables (Logistic Regression Analysis).
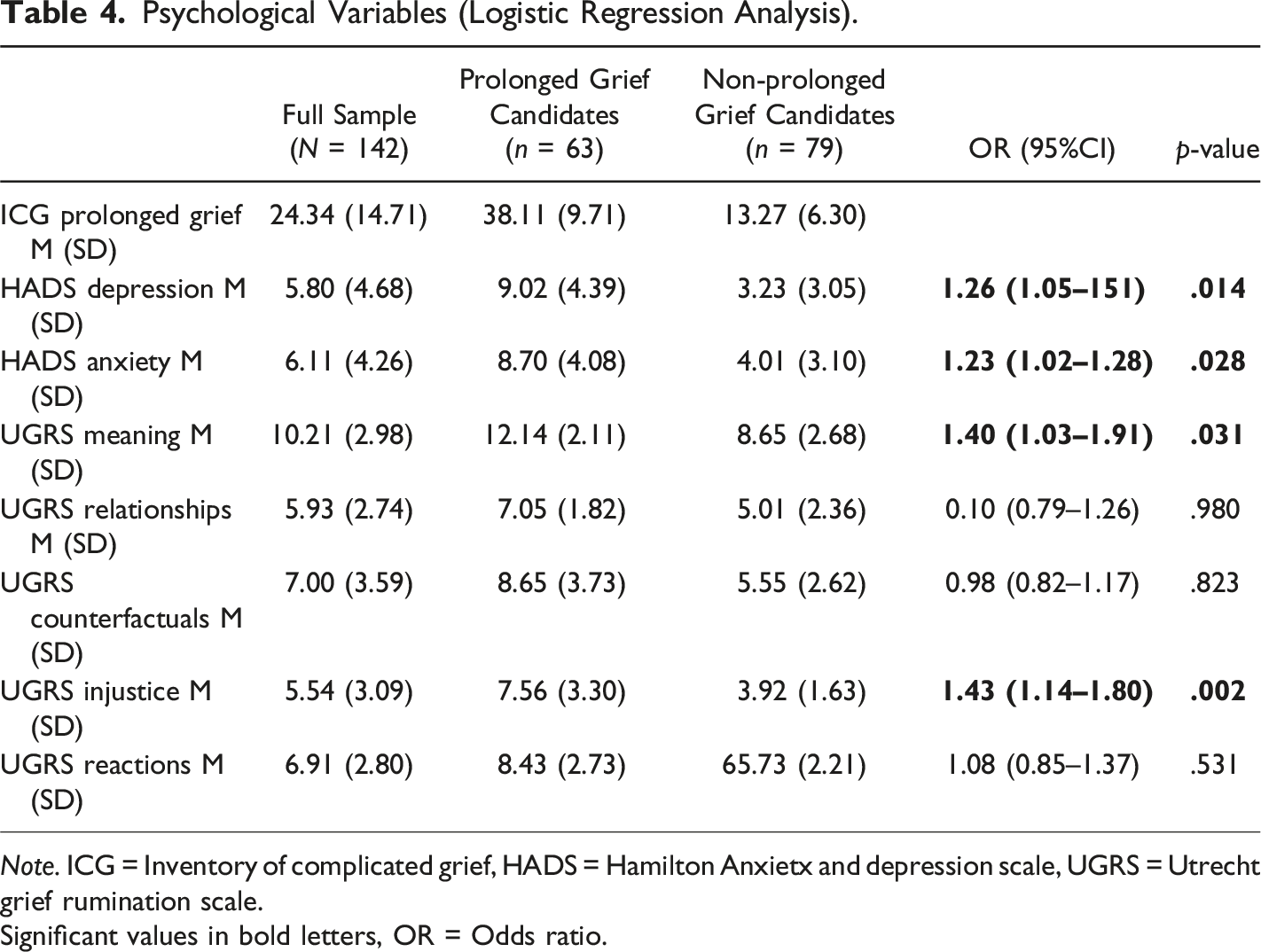
Note. ICG = Inventory of complicated grief, HADS = Hamilton Anxietx and depression scale, UGRS = Utrecht grief rumination scale.
Significant values in bold letters, OR = Odds ratio.
There were no differences between the different diagnoses, different hospital units nor between the frequency of visits or involvement into medical decisions. Moreover, a missing possibility to bid farewell after the death is associated with more PG (OR = 2.20, 95% CI: 1.11–4.35). Participants, who felt more threaten due to the pandemic showed more symptoms of PG (OR = 1.37, 95% CI: 1.18–1.58). The wish for psychosocial support during the lockdown (OR = 1.78, 95% CI: 1.28–2.47) and now (OR = 1.93, 95% CI: 1.36–2.73) was higher in participants with PG symptoms. Nevertheless, there was no difference in the offer of psychosocial support in participants with and without PG.
Out of the psychological variables, depression (OR = 1.26, 95% CI: 1.05–1.51) and anxiety (OR = 1.23, 95% CI: 1.02–1.28) are associated with PG. Additional, meaning (OR = 1.40, 95% CI: 1.03–1.91) and injustice (OR = 1.43, 95% CI: 1.14–1.80) are associated with PG, but none of the other rumination types.
Additional Analyses
Participants with higher scores on the Inventory of Complicated Grief (ICG-D) reported a stronger desire for psychosocial support both during the lockdown period and later during the bereavement process. The correlation was significant for the wish for psychosocial support during the lockdown (r = .329, p < .001) and after the bereavement (r = .306, p < .001). Additionally, participants who felt threatened by the pandemic expressed a greater need for psychosocial support (r = .210, p = .014).The majority of relatives (74.6%) did not receive an offer for psychological or pastoral support, while only 8.5% reported receiving support infrequently and 16.9% reported having regular access to psychosocial or pastoral support. These findings highlight a significant gap in the availability of support services for bereaved individuals during the pandemic.
Discussion
Due to the COVID-19 pandemic, hospitals worldwide implemented visitor restrictions during lockdown-phases. The study aimed to descriptively evaluate whether bereaved family members experienced higher levels of prolonged grief (PG) during the pandemic compared to non-lockdown times. The prevalence of PG may be higher during the pandemic compared to the general population of bereaved persons, but not compared to bereaved who lost their relatives in intensive care units before the pandemic. Variables such as depression, anxiety, education, relationship, emotional relation to the dying and the possibility not to bid farewell after the death were found to be associated with increased levels of PG.
The prevalence of PG candidates in our study, at 44%, was comparable to other research examining PG prevalence during COVID-19 pandemic, which ranges from 37.8% to 48.4% (Tang & Xiang, 2021; Bovero et al., 2021). Our results indicate that family members of patients who died during the first or second lockdown-phase had a higher prevalence of PG compared to the general population of bereaved persons before the pandemic. This indirectly suggests a connection between prolonged grief and the contact restrictions implemented for infection protection during the pandemic. The PG symptoms observed in our cohort are in the same range as those from bereaved relatives of patients who died in an ICU before the pandemic. It is worth noting that certain parallels can be drawn between the contact restrictions in the pandemic and the visiting restrictions that often exist in ICUs regardless of the pandemic. In many cases, patients in ICUs pass away after a serious illness or accident without the presence of close family members. However, our study demonstrates that high prevalence of PG is not limited to bereaved individuals from ICUs but is equally observed across various care structures in the hospital. This can be attributed to the visiting restrictions implemented during the pandemic.
Participants with increased symptoms of prolonged grief reported feeling more threatened by the pandemic and were more likely to be unable to bid farewell after the death of their loved one. This finding is consistent with qualitative research that suggests many relatives were unable to attend ceremonies or view and mourn the deceased's body during the COVID-19 pandemic (Kentish-Barnes et al., 2021). Relatives reported the feeling of “stolen moments” in the contact possibilities before and after the death. In our study, 38% of the participants have not visited their loved one in the hospital at all, and more than half of the participants were not present at the time of the death, preventing them from not bidding farewell before the death occurred. Furthermore, communication with family members was a critical challenge during the pandemic (Greenberg et al., 2022).
Unsurprisingly, participants who felt emotionally closer showed higher levels of grief, as has been observed in previous research (Bovero et al., 2021; Kustanti et al., 2021; Lobb et al., 2010; Tang & Xiang, 2021). In addition, social support should be provided, particularly to those participants who are at higher risk. It has been shown that participants with higher levels of prolonged grief often express a desire for psychosocial support during and after the bereavement period, highlighting the importance of easily accessible support services. Morris and colleagues suggested multiple steps for hospitals and intensive care units to care for bereaved family members during the COVID-19 pandemic, both before and after the death of a patient (Morris et al., 2020; Wallace et al., 2020). Their suggestions included assigning a clinician or other team member to check in with the family, recommending support groups, and sending a team sympathy card, among other recommendations. While many relatives have expressedsatisfaction with the efforts of the medical staff during the pandemic (Greenberg et al., 2022), it is important to acknowledge that medical staff members have reported being overburdened at various times (Luo et al., 2020). Balancing the demands of providing care to patients while also attending to the emotional needs of bereaved family members can be challenging, highlighting the importance of adequate support for healthcare providers as well.
There were no differences in grief reactions detected between the death due to COVID-19 and deaths from other causes. However, this finding contradicts the results of Eisma and colleagues, who found higher rates of PG in relatives who- lost loved ones to COVID-19 compared to those who experienced natural deaths (Eisma et al., 2021). This association was explained by the unexpectedness of the loss. People who experienced COVID-19-related bereavement more often perceived the loss as unexpected compared to those who experienced natural deaths.
This study results confirm a strong association between bereavement and psychological outcomes such as depression and anxiety (Boelen & Lenferink, 2020; Wang et al., 2021). Specially participants with dysfunctional cognitions were found to be at higher risk for prolonged grief (Boelen & Lenferink, 2020; Doering et al., 2018). Feelings of injustice regarding the loss and thoughts about the personal meaning and consequences of the death were particularly associated with a higher amount of grief symptoms. Furthermore, specific risk assessment tools already exist and are in preparation for German-language use (Müller et al., 2020) and there are promising psychological interventions available for PG (Johannsen et al., 2019; Rosner et al., 2018). In order to enhance nationwide bereavement care services, a stepped care model for professionalized bereavement support is currently being adapted to the German context (Müller et al., 2021). This model will include the provision of psychological treatments at an outpatient level in addition to interventions in the hospital setting.
Limitations
Some important limitations have to be considered on this study. Firstly, we only received 35% of the questionnaires back, which may result in a self-selection bias. It is possible that the current sample may have showed higher rates of PG symptoms as only bereaved relatives with persistent grief felt addressed by the questionnaire. Furthermore, it was not controlled which of the grieving family members completed the questionnaire. Finally, the results are limited by the fact that the study used self-reported measures to determine the prevalence rates instead of objective measures.
Conclusion
In conclusion, it can be assumed that the pandemic has increased the risk of prolonged grief among vulnerable bereaved compared to before the pandemic. However, the level of risk may be similar to that experienced by bereaved individuals whose loved ones died in an intensive care unit. Thus, pandemic restrictions as the missing possibility to bid farewell after death can be a risk factor. Looking for known risk factors in bereaved participants like being the partner, feeling emotionally closer, having a lower education, and having the thoughts about injustice and meaning would be worthwhile also during the pandemic. Therefore, professionals who work with seriously ill and dying patients, should take these changes in grief processing into account in their daily work and offer appropriate support to the bereaved.
Footnotes
Acknowledgments
The research did not receive any specific grant from funding agencies in the public, commercial, or non-profit-sectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Note
The study was approved by the institutional review board of the department of medicine at the Philipps University of Marburg (178/20) and was preregistered at the German Clinical Trial Register: DRKS00023713.