
Abstract
Introduction
Decisions, activities, and processes involving End-of-life (EoL) are laden with complex socio-normative and ethical considerations. These involve difficult decisions, including the willingness to learn the truth about the medical situation, whether and how to pursue medical treatment, balancing curative versus palliative care goals, etc. EoL Care is a challenge for terminally ill patients and the medical teams treating them (Brinkman-Stoppelenburg et al., 2014; Carmel, 2002; Velan et al., 2019; Bodas et al., 2020), but also for their caregivers
EoL conjures a commonsensical linear deterioration of the patient’s health associated with the progression of the disease. The first stage in this process relates to diagnosing the fatal condition. Notably, in Kübler-Ross' “Diagnosis of a Chronic Illness, Divorce, Death, or Grief” (DABDA) model, which starts with the patient’s denial and ends with the acceptance of his condition (Corr, 2020).
After diagnosis, three prototypical models of death trajectories (excluding sudden death from an unexpected cause) are proposed, all marked by the patients' gradual loss of autonomy and agency (Murray et al., 2005): The first is a steady decline from a progressive disease. The second is an advanced illness marked by a slow decline with periodic crises followed by a seemingly unexpected death. The last is a prolonged gradual decline that results in expected death. While different in clinical manifestations, all three pathways share the same basic approach to caregiving: The life-prolonging, and perhaps potentially curative medical care, is gradually replaced by supportive and palliative medical care, which becomes central at the end of the patient’s life.
Palliative care is strongly associated with the quality of dying and, as such, is part of a cultural consensus in medicine. This refers to limiting life-prolonging treatments for terminally ill patients and self-imposed restraint when faced with the abundance of medical interventions available. This is what Livne (2019) calls “economized dying.”
Traditionally, much attention has been given to the role of the two major players in the EoL process, namely terminally ill patients (e.g., Carmel et al., 1999) and the medical teams treating them (e.g., Velan et al., 2019; Bodas et al., 2020). Nevertheless, the understanding that family caregivers supporting dying patients are significant counterparts in EoL interactions leads to increased interest in their role (see below).
The literature regarding this role highlights two significant lines of research. One relates to the family caregivers' vulnerability, perceiving them as ‘the second patient’ (Laryionava et al., 2018). Such studies address the emotional needs of family members (Kisorio & Langley, 2016), examine caregivers' strain (Stajduhar, 2013), assess their needs (Green et al., 2022), and explore the challenges of communication between medical teams and family members (Visser et, al.,2014). Another line of research appreciates the potential benefits that family caregivers provide to the EoL process. Such studies see family caregivers primarily as collaborative partners (Becqué et al., 2021). These studies explore their role as crucial mediators between patients and health authorities (Gerber et al., 2020), as the spokesperson of the patients, representing their needs and wishes (Wallace, 2015), to the point of making them part of the decision-making circle (Quinn er al., 2012). Both approaches have, of course, practical implications. For example, they are making end-of-life discussions comfortable and creating plans that reflect patients' and their caregivers' needs and values (Warner et al., 2021).
Another approach is acknowledging the agency of the medical personnel, the patients, and the caregivers, as equally important since all three have their interpretation of comfort, their initiatives, and create their plans. Agency, mainly when referring to biological human beings, is defined as the people’s capacity to serve as the authors of their actions according to their desires, wishes, and fears (Dowding, 2008). It is rooted in power relations and includes the ability to transpose intentionally personal or professional ideologies and beliefs from any given mental chart into a materialistic reality (Dowding, 2008). Agencies may collide, be absent, complement, support, or replace one another. For this article’s purposes, we attribute agency principally to human agents. However, following Latour (2007) and Dowding (2008), we acknowledge, yet do not elaborate, on the role of nonhuman agents, various social institutions, laws, and cultural norms that frame and sometimes limit the agency of humans.
Highlighting the caregiver’s proactive agency is not self-evident. The primary agents in EoL are designated as the patients and the medical teams. The formers derive their power from accepted ethical norms related to the patient’s autonomy and sovereignty over the diseased body (Sullivan, 2017). The latter relies on professional authority and the basic obligations toward the patients and their well-being (Jonsen et al., 2006). In contrast, the agentic proactivity of supporting family members remains fluid, as it lacks a theoretical basis and is not grounded in norms, praxis, and legislation (apart from that related to formal custody)
These gaps led us to focus on the role of caregiving family members in the EoL process. We base our research on the accounts of 12 individuals who practically supported their loved ones during the final stages of their life. We use the caregivers' narratives to delineate the longitudinal process leading to EoL. This allows us to portray the agency dynamics related to the three major players.
Methodology
This study is based on the qualitative analysis of interviews with 12 individuals who closely supported a close relative to their death from a terminal illness. This allowed them to provide their perspective on the action of the other two principal counterparts: the dying patients and the medical team. More importantly, this allowed them to describe their interactions with these two counterparts, thus describing a tri-partite interaction (Patient/caregiver/medical team) rather than a bi-partite one (Patient/Doctor) at the EoL.
Participants were recruited as a convenience sample to represent the diverse Israeli society regarding gender, age, religion, religiosity, and cultural-political orientation. Interviews took place from September to December 2021, ranged in length from 40 to 90 minutes, and were conducted in Hebrew via the Zoom platform (Zoom Video Communications, Inc., San Jose, California). Interviews stopped when an acceptable variation in the EoL stories was reached.
A semi-structured questionnaire was used for all interviewees. The tool comprised a set of open questions covering several categories: questions related to the interviewee’s and patient’s social profile, questions pertaining to medical circumstances at the EoL, questions related to the comportment of the patient (behavior and beliefs), questions related to the role of the family (involvement and dynamics), and questions related to the medical personnel (attitudes, practices, and interactions with patient and family). Interviews were initiated with open questions designed to elicit the interviewee’s narrative, followed by complementary questions when needed. The interviews were recorded, and the transcripts were used to extract relevant motives.
The principal motives in the transcribed interviews were identified using content analysis based on the principles of the interpretative phenomenological approach (Giorgi, 1997), as interpreted by Shkedi (2011). This yielded about 20 EoL-related statements per transcript.
The various motives were then grouped using two criteria. The first was the temporal association between the manifested agencies and the ongoing medical process, e.g., motives related to coping with fatal diseases versus motives associated with the dying process. The second grouping criterion was the attribution of the manifested agency to the various players in the EoL process, namely, the patient, family members, and medical team. All this yielded six different groups described in the Result section. Selected citations were translated into English and incorporated into the text.
Results
Characteristics of the death synopses described by interviewees.
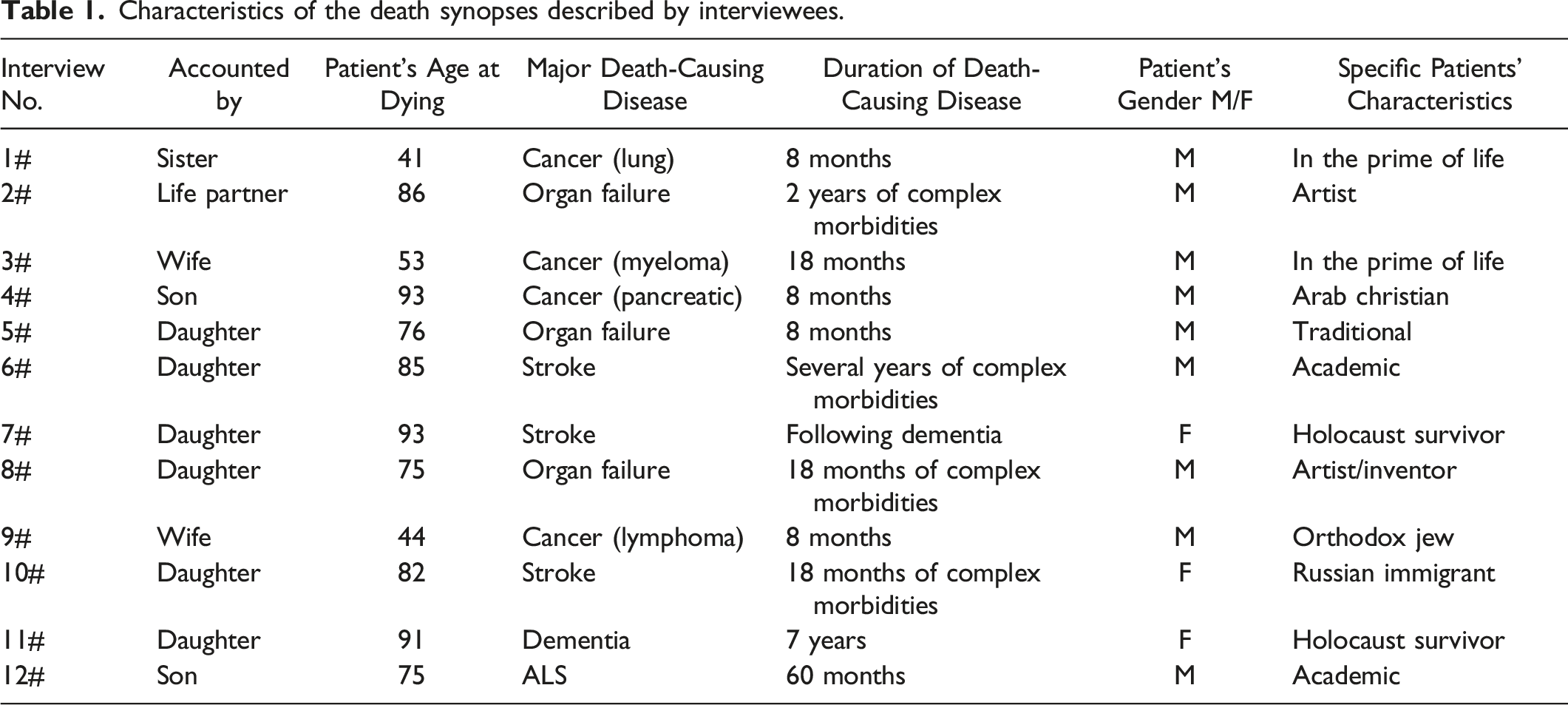
All information collected in this study was provided from the viewpoint of the narrator supporting the dying patient. Nevertheless, by carefully analyzing interview transcripts, one can dissect the specific actions and attitudes of all major stakeholders: the patients, the supporting families, and the medical teams.
The agency-related themes extracted from the transcripts are presented in two dimensions. The first relates to the behavior of the triad of players in the EoL process (the dying patient, the caregiving family members, and the attending medical personnel). The second relates to the two consecutive challenges during the EoL process: coping with the fatal disease along the disease management stage and coping with upcoming death during the active dying stage.
Agency Manifested by Patients in the Course of Fatal Diseases
Patients approaching death display a set of agencies witnessed and reported by their family members, who offered critical insights into various actions associated with dealing with a fatal disease.
Generally, patients diagnosed with a life-threatening illness can adopt two divergent attitudes: Distancing themselves from the disease or facing the harsh reality. It should be noted that in both cases, the collaboration of others is required. Distancing often involves cooperation with family caregivers, while coping with the disease depends very much on the instrumentalityof medical teams.
In an attempt to evade the harsh reality, some patients can ignore the situation. One of the interviewees described the attitude of his elderly father, who had pancreatic cancer: “He kept his life going as usual. He never really dealt with his disease” (#4). In this case, the outdated attitude of ‘don’t ask, don’t tell’ towards cancer was embraced by family members by cooperating with the patient through avoidance and effectively minimizing the event’s medicalization. A different manifestation of avoidance is observed among patients with deteriorating cognition. The daughter of one patient described the behavior of her cognitively impaired mother: “Whenever we came to visit her, she tried to cheer us up by singing the old popular song ‘Que Sera Sera’ (whatever will be will be) with a big smile on her face. (#7)”. However, it should be noted that in cases of this sort, one cannot always distinguish between conscious evasion versus non-conscious evasion.
As opposed to the manifestation of passive avoidance, one of the patients opted for active avoidance, namely deliberate self-neglect, which, in its inverted proactivity, countered the caregiver’s and the medical personnel’s instrumentality: “This was a long-term self-neglect that eventually led to stroke and death, … She refused to take her medications and go for check-ups. (#10).”
A milder manifestation of distancing oneself from a fatal disease is searching for distractions. Some patients did not deny their grave condition yet concentrated on maintaining their routine life: “He spoke about his plans and about buying a new car... He cared about the children, grandchildren, and his wife, whom he loved dearly. (#6)”; “He fought to continue his life routine; we even had a summer family vacation in a hotel. (#9)”. Again, the family played a significant role in fulfilling the patient’s will.
An interesting variation on this was the tendency of some patients to concentrate on activities that were meaningful to them throughout their life, thus replacing the routine with the significant. For instance, the artist focused on creation and education: “He kept creating until the last moment. He continued teaching children to work with clay. He was still creating artwork” (#2). The Rabbi tried to continue with what he defined as ‘things that he had to do’: “He went to the Yeshiva until the very last days, even when he could barely walk. He continued managing a charity organization for orphans as long as he could” (#9). Likewise, the scientist (#12) tried to remain professionally relevant till the end.
In some instances, fighting the disease was accompanied by a need for maintaining control and exerting self-sufficiency as well as dignity, for example: “He didn’t exhibit any (signs of) pain or suffering… He remained in control until the very last day. (#3)”; “He used to tell me that he wants painkillers at a dosage that will allow him to keep studying and talk to people. Not to be paralyzed by pain, yet not to be fully medicated. (#9)” In all these cases, the caregivers and the medical staff were present to assist the patient to execute their performance, whether referring to routine acts or singling out significant aspects of their lives.
In summary, patients facing a fatal disease develop a range of attitudes towards the situation. These attitudes are translated to various forms of agency, including evasion, seeking distractions, prioritization, coping, fighting, and maintaining dignity.
Agency Manifested by Patients in Relation to Death
Some of the patients described by our interviewees addressed the option of death at various stages in life. Some were ready to deal with it before the onset of the fatal disease, some upon the diagnosis of the disease, and some upon the progression of the disease.
Four patients were actively involved in making preliminary legal preparations for eventual death when they were still healthy. They express, at early stages, their explicit intentions related to dying and proclaim autonomy over their bodies in advance. This was described in interviews #2, #7, #8, and #10. For example, “Ten years earlier, he signed a DNI/DNR (do not incubate, do not resuscitate) document… When we got to the ER, I asked him if he wanted to implement it, and he replied: ‘When I signed it, I knew what I was doing. (#8)”
Upon diagnosis of the fatal disease, some patients were reluctant to accept that death was impending (see above). Nevertheless, once the cure was ineffective, the death option was present: “My husband and I knew that death was a possibility, but became aware of this only when treatment was not providing answers. (#9)” As the disease progressed, some patients indicated to their relatives that they were ready to go: “He told me that he had been in all the places he wanted to be in, that he met interesting people, that he had thousands of good experiences, and that he had fulfilled everything, and that is enough. (#8)”. In such a situation, the family member becomes the closest confidant of the patient and shares the immense burden of decision-making.
When the situation deteriorated, some patients realized that the point of no return had arrived and appeared to accept this: “One day, he said, ‘don’t bother to come tomorrow, I won’t be here. (#1)”, and indeed he died during the night. “When his organs began to fail, he closed his eyes. I gave him medications, and at some point, he said: ‘just stop,’ and I did so. (#2)”.
The ultimate case of accepting death was provided in interview #12, a patient incapacitated by ALS: “When he was no longer able to speak, he asked to call his doctor and wrote on a note ‘terminate me.’ The doctor replied that he could not do that and wrote back: Put me to sleep.” It should be noted that this was an exceptional case; in most cases, the patients just drifted gradually toward their death.
All these cases reflect various patient agencies related to death. However, it should be noted that the agency present is not only the patient’s. The family is engaged in active listening: They pay attention, show understanding, respond and act with the legitimacy given by the patient.
Medical Team’s Agency Related to Terminally ill Patients
The duties of medical teams caring for patients with fatal diseases are well-defined by medical traditions, medical norms, and the law. The most basic responsibility of the medical professional is to exhibit professionalism. Some interviewees referred to this:“They all were OK: I have no bad things to say about them. (#7)”; “They all cared for him, starting with the professors, through nurses and ending with the people behind the scene.” (#5)” Nevertheless, sometimes these praises hide expectations for more: “They were professionals, he got what he expected to get, they did not go beyond this” (“5).
The expected ‘extra mile’ may relate mainly to accessibility, compassion, empathy, and respect. Some interviewees were appreciative when they experienced this: “His doctor was there for us 24/7: instructions, video conferences, paperwork, connecting with other professionals. (5#)”; “When I was at his bedside in the hospital, the nurse would tell me: go relax in the shopping mall, I shall keep an eye on him and call you if needed (9#).”; “My husband needed a rectal examination; his female doctor summoned a male doctor to perform the procedure (#9).”
The most demanding decision for doctors who treat patients with a fatal disease is to identify when curative treatment should be gradually replaced by palliative treatment. Here, gaining the cooperation and understanding of the supporting family is crucial. This was best exemplified by the experience of one of the interviewees: “The head of the department told me that from now on, (my) father will not receive life-prolonging treatments, and we shall not perform any procedure that may cause suffering. Whenever there is a doubt, we shall seek your agreement. (#8)”
As expected, medical teams rely on given medical doctrines as strictly medical decisions have to be made. Doctors can, however, express their individual power in their interactions with the patients and their supporting family members. Here, they can exercise compassion, respect, truthfulness, and consideration. Indeed, doctors and nurses were lauded for expressing compassion towards family members. Therein too, lies the family’s instrumentality; By expressing satisfaction with the medical team’s actions, caregivers promote such cooperation and most likely contribute to its reenactment with other families.
The Medical Team’s Agency Expressed at the Imminence of Death
Moving from treating disease to preparing for death during the active dying stage is a major turning point for medical teams. The most important adaptation is related to the purely medical realm and involves shifting from corrective procedures to palliative ones. At the same time, medical teams have to deal with the complex socio-psychological aspects of interacting with the various stakeholders.
One of the duties of physicians relates to truthful disclosure to patients. This obligation becomes extremely tasking when the truth consists of disclosing forthcoming death. The accounts of our interviewees suggest that in some cases, information about the approaching death was communicated in a direct yet sensitive way: “The nurse made death present to us. She ensured I understood the situation and knew it would end this way. She did not wait for me to ask the difficult questions (#9).”
In parallel, the medical team has to reexamine the EoL choices or wishes of the dying individual. They are expected to comply with patients' pre-ordered directives. One interviewee described the treating physician’s compassionate and thoughtful approach: “Dad signed a DNI/DNR document, and they respected it. The head of the department told me: look, in Israel, it is complicated to disconnect a patient from life support once we put them on such support, so we will honor his request and avoid that.'… (#8)”
However, this was not the experience reported by all interviewees. For instance, one interviewee noted: “We had a durable power of attorney. I thought it would help at the end of life, but it was effectively meaningless – nobody cared about it. (#10)”
The medical team’s most tasking action is navigating through the very last procedures before death. These difficulties are best exemplified in the case of cancer patients suffering excruciating pain. A common practice, in this case, is palliative sedation, which entails immense ethical burdens. One interviewee was very grateful to the medical team for dealing with the palliative sedation very compassionately: “The head of the department took me aside and told me one of the most important sentences I think any family should hear at the end of the life of a loved one: ‘it’s not your decision. It’s mine. It’s a medical decision.'… Most of the time, this isn’t being said. Instead, the medical teams tell the family, ‘it’s up to you; make the call.’ (#3).”
The last task of the medical team is to create conditions for a respectable farewell which concurs with the “good death” ideology: “They watched us from outside through their monitors, and did not disturb us. Altogether, this was a graceful and respectable experience (#6).”
At the end of the EoL, the caregivers and the medical personnel are overpowered by death as a natural force. The power of the medical personnel is relegated to communicating impending death, practicing economized dying and self-limiting actions for themselves and the caregivers, and even helping to find solace in tragedy.
Family/Caregivers' Agency Related to Terminally ill Patients
The transcript of the interviews suggests that patients' family members face many inherently proactive tasks during the earlier phases of the EoL process. The duties involved in attending to a seriously ill patient are both medical and non-medical: Interaction with the outside world, dividing responsibilities among family members, serving as a surrogate medical agent to the patient, and sometimes even managing the actual healthcare the patient was receiving.
The burdens of interaction with the outside world were best described by an interviewee who was the only child of her dying mother: “I had to deal with all the bureaucracy, insurance, authorities, as well as to take her to examinations and medical visits. (#10)” Being part of a bigger family can ease the burden but requires division of responsibilities among family members: “My mom was the primary caregiver to my father; my sister and I would help when asked. (#12)”; “Family members always surrounded him. Each one would do something – one was a doctor and gave advice, one just sat with him for coffee, others helped with administrative matters\ (#4)”.
Another important task of family members during the stages of the illness was to create good experiences, for example: “The only way to communicate with her was with songs in Yiddish. We mostly sang rather than talked. She always had a smile on her face (#11).”
Nevertheless, the central role of family caregivers is to attend to the health needs of the patients: “When he was in excruciating pain, I knew to increase the dosage of painkillers he was receiving. (#9)” More importantly, they tried to be part of the decision-making process surrounding the patients. Two examples illustrate the complexity of such situations, given that family members have no legal or formal role in the medical shared decision-making process: “Whenever I wasn't there, I asked the doctor if it was OK for my mom to record the discussions with him so that I could listen to them and see if anything major required my attention. (#5)” “When we just arrived at the hospital for the first time, I wanted to ask something. The doctor stopped me with a hand gesture and said to my husband: ‘I'll finish explaining things to you and then will take care of your wife. (#3)”
In both cases, the family members understood the ethics of patient-doctor interactions, yet explicitly requested to be part of the picture.
Family/Caregivers' Agency Manifested When Death was Imminent
Perhaps, the family caregivers' agency was most vividly apparent when the terminally ill patient was approaching his death. The agencies expressed by family members and caregivers during this stage were diverse.
One mode of action unveiled in the interviews is deciding to shield the patient from the truth. For example, such an approach was adopted by the family of an elderly cancer patient: “We told him he was sick and needed medication, but we never told him it was cancer (#4).”
The opposite approach was to face the truth and act upon it. The burdens of making decisions on behalf of a dying family member may cause tension related to intra-family interactions. Thus, in addition to coping with the harsh situation, one of the major tasks at this time is establishing a consensus among all family members concerning the right thing to do: “We were together. The family was cohesive. Yet, my mom made the calls. (#6)” The life partner of one patient related to the complexity of such situations: “A day before he died, his daughter told me it had to stop, that he would want to live like that. I told her I agreed but didn’t want to say anything before his children spoke. (#2)”
The ultimate involvement of the family in EoL may occur at the very end when the patient is devoid of any form of capacity to make decisions, and family members are asked to interact with the medical teams regarding the final decisions: “When he lost consciousness. The nurse called me and said, ‘we will take orders only from you (his wife). (#3)”; “My mother told the doctors that when my father was still conscious, his instructions were not to be connected to any [life-prolonging] machines. (#7)”
Taken together, the caregivers' testimonies suggest that family members are significant operators in managing the ‘case’ of a seriously ill individual. With the loss of the patient’s autonomy, at the final stages of the EoL process, family members move from having a supportive role to agents that make the calls, sometimes for the first time in their lives. Though they often complement the medical personnel’s agency, it is important to note that when they do so, such agentic proactivity is not always backed by the necessary experience, knowledge, or emotional resilience.
Discussion
During the EoL process, all humans involved act with agentic proactivity. However, an inherent agentic paradox lies at the heart of EoL decisions within the patient/medical personnel/family caregiver’s triad. Specifically, we underline the discrepancy between the scripted roles of the parties involved and their actual role in the EoL process. Contrary to the well-defined roles of patients and of the medical team, the family caregivers' scripted role remains secondary and somewhat passive. We argue that in practice, the family caregivers' role carries many proactive aspects and is crucial. Therefore, the improvement of the quality of the EoL process for all parties involved, especially nearing death, is closely tied to the clarification and empowerment of the otherwise vague caregivers' role and the subsequent enlistment of all of the agency that emanates from it.
The first contradiction concerns the patients. By virtue of being entitled to autonomy, which in medicine primarily denotes self-reliance, decision-making, and action (both mental and physical) (Sullivan, 2017), the patients should author their own lives, EoL included. This right is acknowledged by the law, the patient-centered culture of most Western societies, and is validated by the patients' knowledge of themselves (Cohen-Almagor, 2016; Wallis, 2018; Hagens et al., 2021). Furthermore, since the EoL is a natural continuation of life, it is also strongly related to the pre-illness stage. This supports the notion mentioned by Woods (2006) that there ought to be some consistency between a person’s life and that person’s EoL.
As the disease progresses, and especially in the transition from early to late stages, the patient’s sense of control over their fate gradually dissolves and is now marked by powerlessness. At this stage, the nearly only impactful course of action is to proactively hasten death, thereby altering the timeframe of an event that would otherwise occur later. During the late stages of EoL, incapacitated patients could communicate their wish to die through various clues to a family member or medical personnel. Still, they must rely on the willingness of others to materialize such agentic measures. Similar notions were described in previous studies highlighting elderly patients concerns of becoming a burden and avoiding futile life-sustaining treatment (Gardner & Kramer, 2010)
The second contradiction concerns the medical personnel. Like patients, the medical staff is allegedly an influential actor in the EoL. They constitute authoritative leadership through their command of medical knowledge and their professional experience (Warner et al., 2021). From the patient’s and the caregivers' perspective, this may imply some sense of power over the disease in modifying its course. This overestimation, especially when coupled with the universal human penchant for denying death (Becker, 1973; Mayer, 1998; Solomon et al., 2015), does manifest in the form of some disappointment on the patients' and family members' part when faced with truth-telling throughout the various stages of EoL (Deschepper et al., 2008). As human agents, the medical personnel redress the imbalance caused by the illusion of mastery of life over death and, in varying degrees of proactivity, introduce death in the life of the patients and their caregivers, either through truth-telling or through palliative care.
As the disease progresses, the medical personnel’s agency is crucial, though palliative care differs from disease-modifying or curation, with which medicine is usually associated. Both parties, the patients and the medical personnel, turn into observers of death’s inevitability. That is not to say that medical agency is absent, of course. It manifests itself in the tremendous help the medical personnel offer to patients and caregivers, both in technical competence and as compassionate human beings familiar with the territory into which the patients and their caregivers step.
The third contradiction concerns the family caregivers, but in contrast to their triadic counterparts - medical teams and patients, whose agency is often less robust than expected, the paradox here is inverted. The caregivers may appear as the triad’s weakest agent, both insofar as the law is concerned and in their relations vis-a-vis the patient and the medical personnel. Their roles are scripted as witnesses, providing comfort, support and some information and entitled to comfort, support and information, yet subjugated to the patients' ultimate will and the medical personnel’s authority. Nevertheless, family caregiver nowadays comprise the majority of caregivers to patients in their end of life, and as such they face a multitude of challenges and difficulties (Kehl et al., 2009; Ornstein e tal., 2017; Oechsle, 2019).
As active agents, during the lengthy and exhausting early stages, the families try to cope with the patient’s condition, provide comfort and care, and serve as administrators of the case. Similar notions were previously reported by others, suggesting that family caregivers experienced substantial burden and loss in their care of their loved ones, has limited understanding of the terminal disease progressions, and faced difficulties in setting goals for their loved one’s EoL processes (Gessert et al., 2001; Oechsle, 2019).
As more passive agents, the consequences of family members bearing witness to the active dying stage deserve special attention. This stage, as well as death itself, is not a mere degradation in the disease management stage but, for most, a completely unfamiliar territory, which is nevertheless familiar to the medical personnel (the patients are absent). Even if known to some extent to the caregivers, it cannot be compared to the medical personnel’s experience and requires preparation (Rabow et al., 2004). This insight is of particular importance since it is corroborated by the findings and analysis relating to the medical personnel’s agency.
However, the caregivers often reveal themselves as highly valuable to EoL processes: They are, for most of the process' duration, present, healthy, possess a sound of mind, are relatively level-headed, and most often well-acquainted with the patient’s wishes, needs, and strengths - or lack thereof (in contrast to the medical staff). This status enables their agentic power and the subsequent collaborative opportunities with the patients' and the medical personnel’s agency: The caregivers may acquire relevant medical knowledge and contribute accordingly, partake in medical decisions, carry out personal decisions, communicate information to the patients, and decode information when this is particularly difficult (Gardner & Kramer, 2010). They may serve as extensions of the patients' selves as they try to hold on to life, for instance, as family representatives and leaders and even as extensions of some medical ordinances for the patients in more private settings.
Most importantly, and as shown in the findings, the caregivers never stop displaying agentic proactivity. There is a growing number of publications focusing on caregivers’ experience and needs (Quigley & McCleskey, 2021), and our findings are added to this body of literature. Nevertheless, it is important to note some unique features of the Israeli society for a more context situated discussion. In particular, it is noteworthy that familisim (i.e., the centrality of the family) is Israel remain an identifying mark of the Israeli society (Fogiel-Bijaoui & Rutlinger-Reiner, 2013). Other societies demonstrate varying degrees of familism that may affect the perception of the caregivers’ role at EoL (Mucchi-Faina et al., 2010; León & Pavolini, 2014).
Enhancing the agency of family caregivers requires, first of all, the definition of clear structures for carrying out the caregiver’s duties and addressing rights and responsibilities. In addition, enhancing caregivers' instrumentalityrequires providing appropriate ‘death education’ and fostering a culture of advance care planning (Gessert et al., 2001). This should be targeted specifically to practicing caregivers, but also to the lay general public, since everyone is in a way a potential caregiver.
Limitations
This study is based on the accounts of family members caring for terminally ill patients and represents their perspective on the subject. This, by definition, generates a representation bias, thus underling the role of family members in the EoL process. One should remember that not all EoL events are supported by loving family members, suggesting that in many cases, the agency interplay is not tripartite (Patient/Family/Doctor). It should be noted that in Israeli culture, the family does benefit from a privileged position that translates into a relatively high degree of involvement in medical settings, despite their lack of legal standing in EoL decision-making. This may be different in other socio-cultural settings.
Conclusions
The family caregivers, without ever losing their agency, gradually move from the role of a mere helper to the position of a true mediator and a valuable partner in decision-making. We call to continue exploring, through the term agency, the various ways the caregivers' role may be clarified and expanded for the benefit of all parties involved during all stages of the EoL process. In addition, the general public, specifically potential caregivers, should be offered “death education” to prepare them better for their crucial role at the EoL.
Footnotes
Acknowledgments
The authors thank the interviewees who participated in this study and shared their struggle narratives with us. We thank the Gertner Institute for providing scientific support to facilitate the research. We thank The Israel National Institute for Health Policy Research for supporting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Israel National Institute for Health Policy Research [grant numbers A-6-2020, 2020].
Ethical Approval
This study was approved by the ethical committee of the Sheba Medical Center (approval number SMC-7384-20). All participants provided written informed consent prior to enrollment in the study.