
Abstract
To explore the grief experiences of men from culturally and linguistically diverse (CALD) backgrounds following perinatal death in Australia. Qualitative analysis of interview data using thematic analysis. Participants were health service providers (n = 6), and CALD community members (n = 10) who were either community leaders with experience working with CALD men following perinatal death in Australia (n = 6), or were CALD men who had lived experience of perinatal death (n = 4). Thematic analysis identified four themes related to CALD men’s grief. These included the role of religion and rituals, grief as stoic, the partner- and family-centred nature of men’s grief, and finally grief as ensuring and changeable over time. This research points to the strong need for CALD men’s specific needs to be included in the development of policy and practice surrounding perinatal death.
Keywords
Introduction
Perinatal death is a not uncommon, but potentially a highly traumatic event faced by parents worldwide. In Australia during 2019, there were at least 2843 perinatal deaths, equating to seven stillbirths and 2.2 neonatal deaths per 1000 births (Australian Institute of Health and Welfare [AIHW], 2020). Perinatal deaths are typically distressing, leading to grief, relationship stress, and poor mental health outcomes (Burden et al., 2016). However, previous research in this area has focused on women’s grief experiences, with only a small body of research that relates to men (Obst et al., 2020). Moreover, the experience of sub-groups of men, including those who are culturally and linguistically diverse (CALD), remain under-explored. This is a significant gap, since CALD families experience disproportionately high rates of perinatal death (Belihu et al., 2016; Davies-Tuck et al., 2017; Flenady et al., 2020) signifying a need for comprehensive research addressing CALD men’s experiences of perinatal death, including grief outcomes.
Definitions
In the Australian context, CALD status has been broadly defined as “people born in non-English speaking countries, and/or who do not speak English at home” (Pham et al., 2021, pp. 1). This definition encompasses over 300 ethnic backgrounds and languages spoken in Australia (Australian Bureau of Statistics, 2017; Pham et al., 2021). This paper also uses the term ‘perinatal death’ to refer to both stillbirth (defined as a death in-utero after 20 weeks’ gestation or over 400 g in eight) and neonatal death (defined as the death of a live-born baby with 28 days of birth; Stanton et al., 2006).
Background and Previous Literature
In general, men’s grief following perinatal death has been found to be consistent with instrumental grief, characterised by an outwardly reduced emotional expression (Burden et al., 2016; Obst et al., 2020). Men may also have a greater tendency to somaticise their psychological pain (Janssen, 2016). Consequently, and since an absence of affect may be interpreted as an absence of attachment, men’s grief may go unacknowledged and unsupported (Doka & Martin, 2011). Men are therefore often considered to experience disenfranchised grief following perinatal death (Attig, 2004). Additionally, heterosexual men have been found to adopt a ‘supporter’ role within the relationship with their (female) partners following perinatal death (Bonnette & Broom, 2012; O’Leary & Thorwick, 2006); a role which may lessen the impact of grief (Franz et al., 2021) or, alternatively, prevent men from processing their own grief (Obst & Due, 2019).
Whilst there have been various models and approaches to conceptualising grief in the literature over time, recent understandings of grief have emphasised recognition of the various biological, social, psychological and cultural factors that can shape individual grief experiences (Bronfenbrenner & Morris, 1998; Hua et al., 2020 Stroebe & Schut, 1998; 2010). Expanding on this theoretical viewpoint, Obst et al. (2020) proposed a Socioecological Model of Men’s Grief to capture the relationships between individual, interpersonal, community, and public policy factors that can shape men’s grief following perinatal death. This model facilitates examination of the interaction between individual characteristics or social norms for men (e.g., the expectation ‘to be strong’) and the social, cultural and public policy factors affecting men’s grief. For example, the woman-centred nature of many maternity care models may influence men’s presentation of stoic, or partner-focused, grief (McCreight, 2004). A socioecological approach was therefore chosen for this study in order to facilitate exploration of the multiple factors that may impact CALD men’s experiences of perinatal death across different levels, and outline how these factors may interact to affect grief for this cohort.
In line with this approach, there are a range of predictors which may shape CALD men’s experiences of perinatal death and grief, including, at a cultural level, norms about fatherhood and grief expression (Eisenbruch, 1984). For example, the presence or absence of stigma towards expressions of grief and psychological distress is likely to affect grief outcomes for CALD men following perinatal death (Lin & Tsang, 2020). Grief may also be worsened by the absence of religious, cultural or social norms surrounding how to grieve following the loss of a baby in the perinatal period (Blignault et al., 2009; Knifton, 2012). On the other hand, CALD men may experience protective factors associated with cultural and/or religious background, where these offer ways to cope with grief (Khawaja et al., 2021). For example, previous research has shown that religious beliefs may offer support to bereaved parents and mediate psychological distress following perinatal death in CALD populations (Wright, 2020). Indeed, religion has been shown to shape expressions of grief and mental health among bereaved CALD populations following death more generally (Khawaja & Khawaja, 2019; Snider & McPhedran, 2014). However, the precise impact religion and culture have on grief following perinatal death remains under-explored, especially in the Australian context, and for CALD men more specifically. This study therefore aimed to explored CALD men’s experiences of grief following perinatal death in Australia. Specifically, the study aimed to contribute to better understanding of the potential impacts of various cultural and/or religious factors on perinatal grief for CALD men within a socioecological framework. This aim was explored through the perspectives of CALD men with lived experience of perinatal death, as experts in their own lives and grief experiences. To triangulate responses and to consider how grief may be conceptualised at a cultural and social level, the views of community leaders and health service providers who support CALD men following perinatal death were also sought.
Methods
This study utilised a contextualist epistemological approach, simultaneously acknowledging the validity of subjective participant accounts, and contributing research recommendations within the healthcare context (Madill et al., 2000).
Participants
Participant Characteristics.
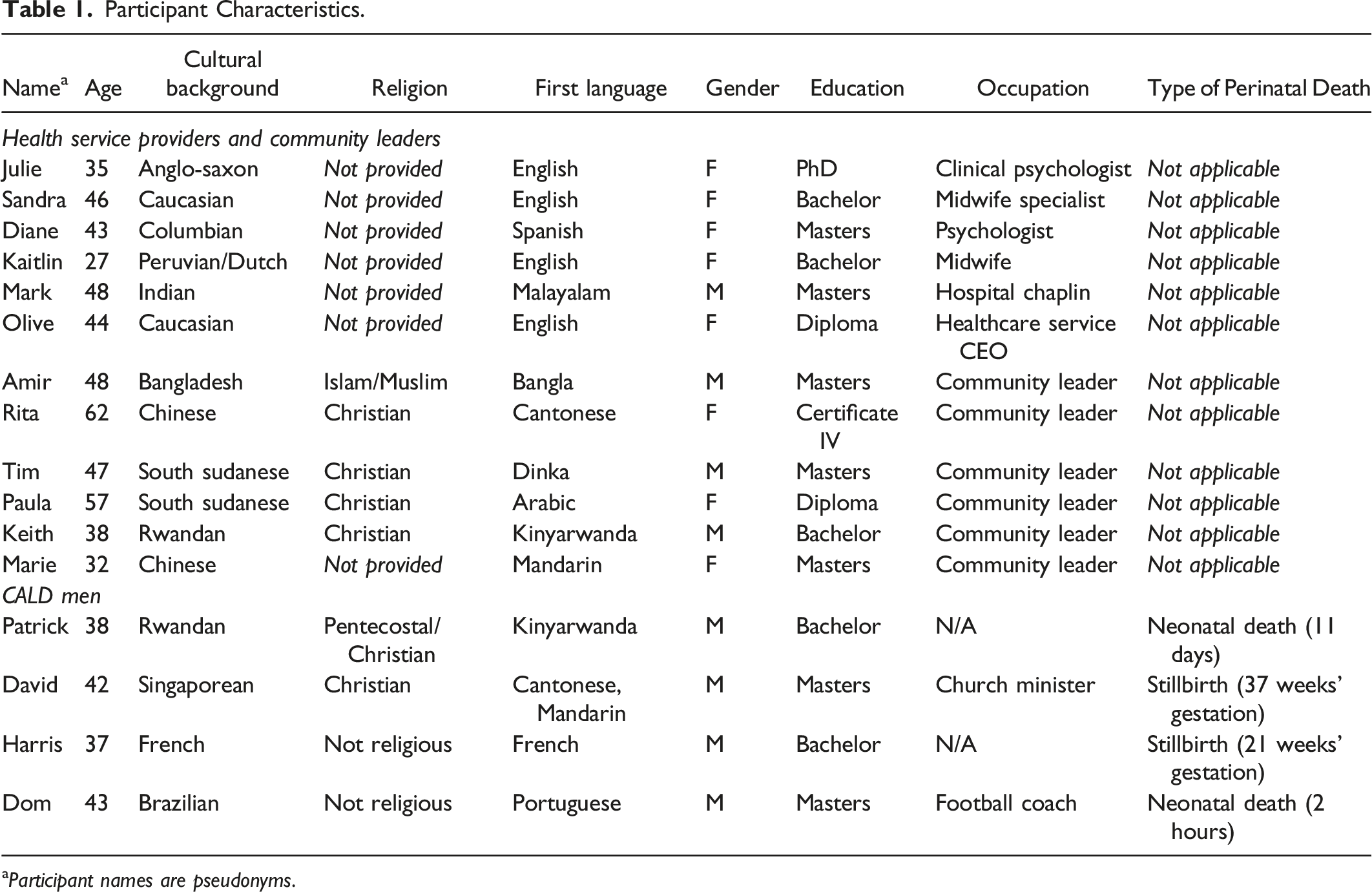
aParticipant names are pseudonyms.
Procedure
Participants in Group One were required to have experience working with CALD men after a perinatal death in Australia. Participants in Group Two were required to self-identify as CALD (e.g., English was not their first language or they self-identified as culturally diverse) and were either community leaders with experience working with CALD men following perinatal death or had experienced a perinatal death themselves during the previous 12 years in Australia. CALD participants who had experienced perinatal death within the previous 6 months were not included, to minimise potential distress. Notably, given the significant lack of research in this area as outlined previously, the definition of CALD was deliberately kept broad, and with a focus on the self-identification of participants into this category.
This study received full ethics approval from The University of Adelaide Human Research Ethics Committee on 31 March 2021, approval number H-2021-048. Information about the study was disseminated to a broad range of health service clinics, individual healthcare professionals, community support organisations, CALD community groups, and perinatal research organisations based in Australia. Snowball sampling was also used.
Most interviews were conducted via videoconference (n = 14), however two CALD men with personal experience of perinatal death elected to be interviewed via phone and in-person. Notably, research suggests that videoconferencing is a suitable way of interviewing CALD populations in qualitative studies, and thus these multiple interviewing methods were considered appropriate (Gray et al., 2020; Ahangari et al., 2021). Informed consent was gained from all participants. While there are various approaches to sampling in interview-based studies (e.g., Braun & Clarke, 2019), this research used data saturation to determine sample size. In relation to the research question concerning cultural and social elements impacting grief for CALD men, data saturation was achieved by the 15th overall interview.
Interviews were conducted in English by the first author. In line with the exploratory aims of the research, questions were open-ended and semi-structured, including demographic questions (age, gender) and questions about grief experiences, including cultural elements. Example questions for CALD participants included: ‘Could you tell us a bit about how perinatal death is viewed in your community?’, ‘Could you tell us about men’s experiences of perinatal death for people from your cultural background’, and ‘Are there any specific grief considerations for men from your community/cultural background’. Example questions for healthcare providers included: ‘Can you tell us a bit about your work with CALD men following perinatal death’, ‘How do you think culture might impact grief for men following perinatal death’, and ‘Could you tell us how cultural impacts on grief have looked for any men from culturally diverse backgrounds that you have worked with, including any examples you can provide?’. Notably, as interviews were semi-structured, they followed the lead of participants and questions were used as prompts only.
Seven interviews were conducted with community leaders and health professionals before the first interview with a CALD man who had experienced perinatal death; this interview resulted in the addition of questions in future interviews regarding perceived social pressure and burial arrangements for the baby who died.
Interviews lasted an average of 61 minutes (49 minutes for Group One; 69 minutes for Group Two). Men from CALD backgrounds and community leaders received a $50 voucher for their participation. All interviews were conducted between April and August 2021 and audio-recorded with participant consent. Each interview was transcribed verbatim by the first author, according to the orthographic method (Braun & Clarke, 2006). All personally-identifying information was removed from the transcriptions and names replaced with pseudonyms (which participants themselves chose). Member checking led to 12 participants (75%) reviewing their transcript; none requested changes. An audit trail was kept by the first author in line with Tracy’s (2010) criteria for enhancing methodological rigour in qualitative research. This consisted of reflections on the interview process, initial codes and themes, copies of communication with participants, and meeting notes. The audit trail provided direction for the analytical strategy and interpretation of themes.
The six steps of thematic analysis as outlined by Braun and Clarke (2006) were followed. Specifically, codes were identified first at a semantic level, with initial data familiarisation and domain summary coding to identify inductive, bottom-up codes within the data sets. Subsequently, codes were examined in approximation to the Socio-ecological Model of Men’s Grief (Obst et al., 2020), with this context informing the development of themes. Next, codes were developed into fully-realised themes. Triangulation between participant groups occurred throughout the analysis.
Results
Thematic analysis identified four themes that mapped onto the research aims concerning CALD men’s experiences of grief. Specifically, these were that: 1) Religion and rituals help shape expressions of grief, 2) Culturally and linguistically diverse men’s grief if often stoic, 3) Partner- and family-centred grief, and 4) Grief is an enduring and changeable process. Extracts below include pseudonyms and note whether participants were health service providers (HSP), community leaders (CL) or men with lived experience of perinatal death.
Religion and Rituals Help Shape Expressions of Grief
In terms of the role of culture on CALD men’s experiences of grief following perinatal death, a key theme identified in data analysis was that of the role of religion and ritual. In particular, both groups of participants indicated that rituals helped shape expression of grief for CALD men. For example, Mark, an ecumenical hospital chaplain, explained: “When [CALD men] are very much connected with their religion and their culture, about the loss of the baby, their grief is much, much lower. But if a person cannot connect with their religion or culture, I think they don’t know what to do. There’s no conclusion.”
Similarly, even where not considering themselves religious, CALD men participants reported that ritual was important for expressing their grief following perinatal death. For example, Dominic (Brazilian) described creating his own personalised “healing” ritual after stillbirth: “And then we did a ritual with close friends and we put his ashes on the river, not far from where I am right now actually. In a place called [redacted] beach, was beautiful. It’s very beautiful ceremony. Very important. It’s very healing, very soothing, very sad. But it brought us together.”
Importantly, participants highlighted that there were sometimes culturally held perceptions of differences in terms of the appropriate rituals to complete depending on whether a baby was stillborn or died in the neonatal period, particularly in terms of religious burial practices. Solomon (South Sudanese) explained: “[For a stillborn baby] they pray together a little, they don’t do 40 days like a born one. A born one they do… after the death, three days, and then a day of burials. And then the 40 days after that... But the [stillbirth]… then they just pray once.”
Similarly, Pauline (South Sudanese CL) explained how men’s grief in her community was shaped by cultural understandings of stillbirth as compared to neonatal death: “That one [stillbirth] we can say ‘ah it is not good, no one saw’. Maybe the baby was like, three months, four months. Doesn't matter. But the baby you saw [neonatal death], it’s like a human being. And then you think, the year comes, I saw my baby, it was supposed to be this year. I was supposed to be doing this. So, we think different.”
As such, CALD participants highlighted culturally-perceived differences between stillbirth and neonatal death, both in terms of appropriate rituals and associated perceptions at a community level, which they felt were important in shaping their grief responses. However, notably David highlighted that, in his lived experience, these culturally-held views actually made his grief more difficult following the stillbirth of his baby. Specifically, David said that the absence of culturally prescribed rituals and burial practices for stillborn babies made his grief particularly acute: “for a stillborn baby... What photo do you have? And what memories? So actually some people say that is the hardest part when you have nothing to celebrate.”
Finally, participants pointed to culturally held views about the role of men following a perinatal death. In terms of religion and rituals and their role in expressions of grief, a key point raised by both groups of participants was men’s role in facilitating burials and other rituals and practices, with this often seen as the man’s responsibility. In line with other themes below, where men were not able to fulfill this role this had a negative impact on their grief, typically making it worse. For example, participants discussed being required to modify their cultural and religious practices in relation to child burial due to issues such as funeral expense, and disconnection from family. For example, many participants reported the religious significance of burial, however this was reported to be prohibitively expensive in Australia. To illustrate this, Mark (Hospital Chaplain) recounted a story about men he had worked with from India who had experienced perinatal death, and their responsibility to ensure their children were given an appropriate funeral, saying: “So men might immediately start calling their family in India. And they said, ‘this is the situation... and it is very expensive here and what should we do?’ So they usually compromise their religion...and they go for cremation. That is the man’s job. And, and that is the way [in those cultures]. So the men, they don't do much talking or all these things… But that is the way they grieve.”
Here, Mark described how ensuring their children who had died in the perinatal period were given an appropriate funeral was a key way in which men from culturally diverse backgrounds – in this case from India – expressed their grief.
In summary, it was apparent that participants indicated that religious and other rituals for mourning their baby were important in their grieving processes and expressions of grief. Some participants pointed to culturally held views about differences in appropriate rituals and burial practices for babies depending on whether they died in the neonatal period or were stillborn; but notably one CALD man whose baby was stillborn specifically highlighted that such understandings had made their grief more challenging. Finally, in terms of men’s roles specifically, participants pointed to the role men often held in relation to organising practical components and the way that enacting this role may be an expression of grief in and of itself for men in particular.
Culturally and Linguistically Diverse Men’s Grief is Often Stoic
Both groups of participants indicated that CALD men generally restricted outward displays of emotion during their grief following perinatal death. Participants typically framed this stoicism as resulting from normative, gendered expectations of grief following perinatal death, despite underlying affect such as sadness or hopelessness. For example, Julie (HSP, Clinical Psychologist) noted that in many cultures: “…it’s more appropriate for women to be expressive in emotions and for men to be kind of stoic holders of stability. And there might be shame about falling apart. But real, real sadness, real, real depression and real sadness of the loss.”
CALD participants similarly discussed gendered norms of men’s grief as aligning with cultural values related to stoicism for men. For example, Rita (Chinese, CL) described “…in Chinese culture there’s a poem saying that men can lose their blood, but not lose their tear”. Pauline, a South Sudanese elder, similarly said: “Our men, they don’t cry, but they cry inside.”
Whilst being framed as culturally-normative, both participant groups reported that appearing stoic could be difficult for CALD men and was associated with hidden emotional strain. David (Singaporean) reflected on his lived experience: “I’ve cried. I’ve never cried so much in my life... I really cry to, I think until three am or so. And what happened was the doctor said, “his heartbeat stopped.” Around that time... So I don’t, I just can sense it. So that, even though I’m not proud to say I cried so much. But that was my grieving process.”
Similarly, Patrick (Rwandan), whose baby died at 11 days old, shared his personal grief response: “Yeah, to be honest it was quite bewildering and very difficult, but obviously I knew I had to be strong, you know for my wife as well, because if I broke down, I don't think she could have handled it herself. So, I had to be strong for the whole family. But it was very difficult.”
In summary, CALD men’s grief following perinatal death was described as stoic in nature, informed by culturally-normative expectations of appropriate grief expressions. In part, this stoicism was described as necessary since often CALD men “had to be strong” for their wives or partners and broader family members, leading to the next theme.
Partner-and Family-Centred Grief
Both groups of participants noted that CALD men’s stoic grief was associated with culturally-normative responsibilitGiven that all the interviews were conductedies to care for their wives and partners following perinatal death. For example, David (Singaporean), explained that a period of reduced emotions permitted him to support his family following the stillbirth of his baby: “You’re able to not feel the pain for a short period of time to fix it. I feel, emotionally to going through the grief where, yeah, I did have my grief and cry, then in the process of facing death, and having to deal with funeral and things like that, there was that numbness of grief to be able to still function, to care for others, to do for my wife and even for the grandparents.”
HSPs had a shared perspective that CALD men’s focus was often on their wives and partners following perinatal death. Olive, a health service CEO, noting: “they do put themselves at the back of what their wife’s needs are”. HSP participants also reported that CALD men often only engaged in mental health support to support their partners, as Diane (Psychologist) indicated: “They come [to therapy] mostly to support their partners. And so I do always make the point of asking them both about how they are doing and they [men] tend to reflect the question back to their partners. So, it’s kind of, I need to be okay, in order to support her because she was the one who gave birth to the baby we lost.”
Importantly, this focus on wives and partners sometimes led to expectations and behaviours which contradicted gendered expectations for men. Amir, an Islamic leader from Bangladesh, noted: “…when [perinatal death] happens, he has to help. He helps around the house. Traditionally in our culture the boys are the bread-earner. In Muslim culture, people generally expect men try to work outside the house…”
Importantly, there were tensions in the data in relation to whether or not partner-centered grief only negatively impacted CALD men’s ability to process their own grief. Specifically, some CALD men themselves reported indirectly benefiting from adopting supporter roles. For example, Harrison (French) said that his partner-centred focus helped his immediate grief following the death of his child after her birth: “I decided following the delivery that for my recovery and mental health…not to see the child. I tried not to look, instead focusing on my wife. [Baby] was not fully-formed, I didn’t want the picture of the un-formed child, who was blue, to haunt me. [Instead] I was focusing on my wife, and she was hungry. So, I went and got food.”
This account demonstrates that a focus on partners and corresponding instrumental grief responses are not straightforward in their impact on grief for CALD men.
Overall, participants indicated that sociocultural expectations of CALD men’s gendered responsibilities shaped both stoic and partner-centred grief responses. Partner-centred grief, while often presented as a potential barrier to CALD men’s grief, was also sometimes posited as adaptive.
Grief is an Enduring and Changeable Process
Consistent with the conceptualisation of grief as a process, participants indicated that grief was often something was lasted significant amounts of time, but that the expression of that grief changed over time. In particular, CALD men reported that their grief endured over years, including after subsequent pregnancies and the birth of other children. For example, Patrick (Rwandan), whose baby died in the neonatal period a decade prior, explained: “When we lost her, we had only one child. She was going to be the second and so, at that point, I thought, maybe if we have another child, that’s going to be closure. We will stop worrying because we have had almost compensation, if you can call it that, for the lack of a better word, with another child. But yeah, even after having other children, it’s just a void that can’t be filled. Because she was unique in her own way.”
Participants also noted that grief was enduring, although reduced over time. For example, Dominic (Brazilian) recounted how his intense experiences of grief following stillbirth were replaced with different emotions: “We held him, I looked at him and… When I think of [my stillborn baby] I have this warm feeling. Like it’s a good feeling. I don’t feel guilty. Yes there’s the sadness. There always is if you ever lost somebody in the family, you know that, there’s this sadness. It’s always there. But then again, I don’t…. I don’t feel… I feel this warmth…”
Overall, participants noted that grief following perinatal death was enduring, even after subsequent pregnancies. However, for some participants, over time the memory of their babies was not associated with grief but rather replaced with a sense of warmth.
Discussion
This study begins to address a significant gap in the literature surrounding CALD men’s experiences of grief following perinatal death, with a focus on the role culture may play in relation to those experiences. Whilst several findings overlap with previous literature on men’s experiences of grief after perinatal death more broadly, specific cultural and religious factors also appeared to impact upon, and play a role in, CALD men’s grief.
The first theme of the study relates to the role of religion and ritual in shaping men’s grief expressions. This was particularly the case in terms of the ability to perform particular rituals that are consistent with religion, which was seen as beneficial for grief. These findings support previous research about the role of religion more generally in easing any distress associated with grief (Wright, 2020; Khawaja et al., 2019). The findings also extend previous literature, to highlight the importance of ritual more broadly for CALD men, even when not specifically associated with religion.
Additionally, two separate but interrelating themes identified were CALD men’s grief expression as stoic and partner-and family-centred, both characteristic of instrumental grief patterns (Doka & Martin, 2011). Stoic and partner-centred grief patterns also reflect research with other (western) groups of bereaved fathers (e.g., Obst et al., 2020; Obst & Due, 2019; McCreight, 2004; Pollock et al., 2020) and thus normative expectations of men to ‘be strong’ (as one participant described it) and support their families thus seems to be a common theme across cultural groups. Similarly, and also in line with prior research with men more generally, this study found that the roles and responsibilities that CALD men may be assigned or may adopt for themselves (e.g., organising funerals) often made it difficult to grieve perinatal death (Obst & Due, 2019; Avelin et al., 2013). Taken together, these findings are consistent with the concept of an ‘affective bias’, where CALD men may experience disenfranchised grief if instrumental grief processes (such as those related to organisation of burials and religious practices) go unrecognised. This may lead to a misperception that men, including CALD men, experience lower levels of grief when compared to women following perinatal death (Avelin et al., 2013). The findings of the current study are not sufficient here to fully support this bias, nor whether or not CALD men specifically experience disenfranchised grief, and thus this is an important topic for future research.
Importantly, participants frame the focus on partners and other family members as purposeful within the culturally-informed roles and responsibilities CALD men enacted in support of their families. Additionally, HSP participants in particular discussed the dilemmatic nature of CALD men acting as ‘supporters’ for their partners and families, where this may be both harmful and protective in relation to grief following perinatal death (Obst et al., 2020; O’Leary & Thorwick, 2006; Franz et al., 2021). Here, then, instrumental grief (in the form of supporting family) was represented as adaptive, enabling CALD men to fulfill these culturally informed support roles, and process their own grief. This is consistent with previous research highlighting the importance of men’s partner-support roles in enhancing recovery and responding to pregnancy related trauma (Franz et al., 2021).
In this study, there was a distinction drawn by some participants between neonatal death and stillbirth; in particular community leaders, who had often worked with numerous families, highlighted the perception that stillbirth was considered less significant than neonatal death. Previous research has demonstrated stigma following stillbirth for mothers in countries such as the UK (Brierley-Jones et al., 2014), Tanzania (Haws et al., 2010), and Uganda (Kiguli et al., 2015), with neonatal death attracting less stigma and more understanding. Additionally, this is consistent with religious and cultural beliefs where foetuses are sometimes considered ‘pre-human’ (Khorfan & Padela, 2010; Pollock et al., 2020) and therefore attracted less personal and public grief.
However, within this study, HSPs and one CALD man who experienced stillbirth specified that the ambiguity and hidden nature of stillbirth complicated grief, potentially leading to worse grief outcomes over time. These findings are consistent with previous literature indicating that stillbirths are also highly significant to bereaved parents, leading to disenfranchised grief when the baby is not publicly recognised (Obst et al., 2020). Research into complicated and prolonged grief shows that bereaved parents may rely on dysfunctional coping patterns, and experience relationship distress and unacknowledged pain (Mehran et al., 2013). Prolonged grief has also been shown to be associated with stigma, whereby individuals’ enduring grief is not recognised by the broader society (Eisma, 2018). Further, previous research has shown that perinatal death is strongly associated with complicated grief (Kersting & Wagner, 2012). The stigma, disenfranchised grief, guilt, and enduring grief reported in this study suggest that some CALD men may be at increased risk of complicated grief following perinatal death and particularly stillbirth (Heslehurst et al., 2018).
While this study is one of the first to consider CALD men’s grief following perinatal death, it is limited by the small sample of CALD men who had lived experience of perinatal death, and their restricted demographic profiles. In particular, they were largely religious and well-educated. Given that all the interviews were conducted in English, participation in the study also required a certain level of English-language fluency, which may have excluded potential participants including some from culturally-specific new and emerging communities in Australia where levels of English language competency may be lower. While overall having a sample of community leaders and healthcare providers led to data saturation, future research with a more diverse sample of CALD men, including by specific population sub-groups, is required to provide a more in-depth understanding of how grief is shaped or influenced by specific cultural and religious nuances.
Conclusion and Recommendations
Overall, this study contributes important recommendations, including working with men as they support their partners, ensuring that healthcare providers understand cultural norms around grief following perinatal death (including stillbirth and neonatal death distinctly), and having continuing support for men over time. In particular, the study points to the clear need to consider intersections of culture and gender norms for CALD men, who may experience isolation and disenfranchised grief following perinatal death.
Footnotes
Acknowledgments
The authors would like to acknowledge all the fathers who contributed to this study by sharing their stories.
Author Contributions
The study and methodologies were planned by all authors. TP conducted interviews and led analysis. CD and KO reviewed analysis and thematic structure. All authors contributed to writing and preparing the final manuscript.
Ethics
Informed consent was obtained from all participants in this study. The study was approved by The University of Adelaide Human Research Ethics Committee on 31 March 2021, approval number H-2021-048. The study was performed in accordance with the Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.