
Abstract
The aim of this retrospective qualitative study was to examine the bereavement experiences and coping of family caregivers, with the Dual Process Model (DPM) as the theoretical framework. A purposive sample of 15 bereaved family caregivers, who had lived with and/or cared for their dying spouse or parent, were recruited from a local hospice. Using the interpretative phenomenological analysis approach, all one-to-one interviews were audio-recorded, transcribed, and entered into NVivo 12 Plus software for analysis. The major themes in this study mirrored well-established components of the DPM, including the concept of overload from the revised model. The cognitive processes of meaning making, an integral component of the DPM, were also discovered and put forth as a fifth theme to illustrate reconstruction of positive meaning. This is posited as an adaptive outcome to successful oscillation between loss-oriented and restoration-oriented grieving processes and, hence, leading to implications for bereavement care and support.
Keywords
Introduction
Bereavement care is a continuation of palliative and end-of-life (EOL) care, given that family caregivers of terminally ill patients will be experiencing the loss of a loved one eventually. While Stroebe et al. (2007) have emphasized that “grief is a normal natural process after bereavement” (p.1969), whereby most bereaved persons can cope adaptively with time and without professional intervention, their review study has also discovered consistent patterns of adverse health outcomes being associated with bereavement. This is unsurprising as bereavement experiences are stressful life events that naturally expose bereaved individuals to increased risks of mortality, physical illnesses, and psychiatric conditions, making it a topic of medical concern (Chen et al., 2020; Ennis & Majid, 2021; Stroebe et al., 2017).
Given that bereavement is a universal experience, and no two persons experience a loss the same way, bereavement studies are often about finding similarities among different losses and differences within similar losses. A common limitation of bereavement studies was that most were on spousal losses, so it remained unproven if those findings could be extrapolated to other loss types (Stroebe et al., 2007; Tseng et al., 2017). The need remains for deeper understanding of the nuanced differences in bereavement experiences, coping, and outcomes across various bereaved groups (Ennis & Majid, 2021). Literature have hypothesized that the type and quality of relationship shared between the deceased and the bereaved person might influence grief processes and affect bereavement health outcomes (Ennis & Majid, 2021; Tseng et al., 2017). For each type of progressive chronic illness, there are also well-established illness trajectories (Murray et al., 2005). Depending on the type of illness, caregiving experiences of bereaved family caregivers can look very different, and this might influence their bereavement experiences. Possibly, relationship and illness types might differentiate bereaved groups, hence justifying more research focus on these study parameters.
When examining the bereavement experiences and coping of bereaved family caregivers, there needs to be certain theoretical and/or conceptual framework(s) to ground the scientific inquiry. A landmark study by Stroebe and Schut (1999) summarized existing theories and models related to bereavement before putting forth the Dual Process Model (DPM) as a framework integrating certain existing ideas. The original DPM provided an overview of the taxonomy of bereavement-specific stressors, labelled loss-oriented (LO) and restoration-oriented (RO), and it was proposed that the oscillation between LO and RO grieving processes is necessary for adaptive bereavement coping (Stroebe & Schut, 1999; 2001a). In a more recent publication, Stroebe and Schut (2016) introduced the concept of overload as a missing link and brought attention to mental and physical health complications when a bereaved person is overloaded by stressors. All in all, the advantage of DPM is its universality in application, coupled with the flexibility for discussion in relation to extant theories and literature.
Beyond understanding bereavement experiences and coping of bereaved family caregivers in Singapore, there is a dire need for evidence-based and theory-driven bereavement interventions that are culturally appropriate. In the recent two decades, there has been more empirical support for DPM as a model that encapsulates bereavement experiences and coping and showing that DPM-guided interventions are more effective than traditional grief therapy that focused solely on LO components (Fiore, 2021), specifically so for Chinese widowed older adults (Chow, 2015; Chow et al., 2019). According to DPM principles, bereaved individuals experiencing physical and mental complications due to bereavement can benefit from interventions targeted at their patterns of oscillation between LO and RO coping processes (Stroebe & Schut, 2010). Theory, research, and practice go together when it comes to delivery of effective bereavement interventions (Chow, 2015; Chow et al., 2019; Lund et al., 2010; Stroebe & Schut, 2010) and this paper aims to be a building block of the Singapore literature in bereavement care and support.
The present article reports on a partial set of data from a qualitative study, which aimed to examine two research questions pertaining to the definition of a good death and dying processes for terminally ill patients, either a dying spouse or parent, as perceived by bereaved family caregivers and the influences of this good death concept on their caregiving experiences and subsequent coping with bereavement. Using the data on the bereavement experiences and coping of bereaved family caregivers, this paper aimed to identify the key processes and mechanisms underlying the studied social phenomenon and compared it against the DPM. Here, the narratives of 15 bereaved family caregivers related to their coping with bereavement are analyzed to answer the research questions: 1. How relevant is the DPM in representing the bereavement experiences and coping of bereaved family caregivers who have lost either a dying spouse or parent? 2. What are the coping mechanisms that support the principles of DPM in adaptive coping with bereavement, if any?
Methods
This retrospective qualitative study undertook an interpretative stance in examining the recounts of bereaved family caregivers when caring for their dying spouse or parent, and their subsequent coping with bereavement. Ethics approval was obtained from the National University of Singapore Institutional Review Board (NUS-IRB Reference Code: S-19–243) and Agency of Integrated Care Institutional Review Board (AIC-IRB Reference Code: 2019–002) before the start of study recruitment.
Study Recruitment and Participants
Bereaved family members from a local hospice were identified by their medical social workers (MSWs) and counsellors who had prior engagement with them and were able to assess their suitability to participate in the study. They then sought verbal consent for the principal investigator (PI) to contact them for recruitment, which occurred between September 2019 to May 2021. Interviews were conducted either in person or on virtual platform, subjected to the government regulations put in place in response to the COVID-19 pandemic situation, and one-to-one to create a safe space for participants to reflect upon their lived experiences and share in greater details (Smith et al., 2009).
A purposive sample of 16 bereaved family caregivers, who were: (1) aged 21 years and older, (2) bereaved between 6 months to 2 years, and (3) willing to participate in this study, were recruited. The recruitment was also stratified according to illness types (cancer or non-cancer) and relationship types (spousal or parent-child relationship). As a family caregiver, they would have met the criteria of having lived with and/or cared for their dying spouse or parent during EOL and up till the eventual death. All 16 recruited participants were given supermarket vouchers with a value of 20 Singapore dollars as a token of appreciation for their time and participation.
Data of a participant from the non-cancer and parent-child subgroup was excluded because the participant was found during the interview to be experiencing infrequent suicidal ideations with the latest episode happening weeks before the interview. In accordance with the study protocol and with the participant’s best interest in mind, the interview was terminated immediately. Necessary support was rendered to the participant according to the safeguards in place to protect participants’ psychological well-being.
Data Collection
To yield rich data and thick descriptions of participants’ lived experiences, semi-structured interviews were conducted and completed with 15 bereaved family caregivers. An English interview guide, with mandarin translation, devised with open-ended questions and probes was used flexibly to facilitate participants in their sharing. Each participant was interviewed once and interviews were conducted in English and/or Mandarin, which lasted between 45 minutes to nearly 3 hours (103 minutes on average). All interviews were audio-recorded with participants’ permission.
After the interview, participants were contacted within the next five working days and 1-month post-interview to assess if referral to their former MSW/counsellor or other appropriate service providers was necessary because of the interview. For participants who were retired elderly persons (aged 65 years and above), living alone or only living with a domestic helper, the PI made an additional follow-up phone call around 2-months post-interview to ensure that nothing adverse happened after the interview concluded.
Data Analysis
All audio-recorded interviews were transcribed and entered NVivo 12 Plus software for thematic analysis. Data analysis started with a process of familiarizing with the data, including transcription of verbal data, and generating of initial ideas that stayed closely to the data (Braun & Clarke, 2006; Smith et al., 2009). With large amount of data from each transcript, structural coding was performed with reference to the specific research questions (MacQueen, 1998). As the interview guide was structured to answer the research questions, structural coding provided a suitable frame to kickstart the coding process. With an inductive approach, data were coded diversely, without paying specific attention to the themes from previous studies. Initial codes stayed close to the explicit meaning of participants’ words and focused on describing what participants felt, thought, and did, or what they observed of others. Two transcripts from the same subgroup were coded before a code book was developed and refined as more transcripts were coded. During the process, the second author served as a sounding board when the rationale of the codes and themes were challenged.
The subsequent steps involved a recursive process of searching for themes to create an initial thematic map and reviewing of themes to formulate the final thematic map. When reviewing themes, the aim was to ensure coherence of the data within the respective theme and in relation with the study corpus (i.e., accurate representation of all the participants). These processes involved ongoing coding of data that was previously missed out as the themes were reviewed and codes were reorganized or discarded to provide a more coherent reflection of participants’ lived experiences. To bring forth conceptual links between the studied social phenomena, the rich thematic descriptions of participants’ lived experiences were further analyzed to answer the research questions at interpretative levels. Underlying concepts and processes were identified as key findings and further discussed in relation to existing literature, which also functioned as a validity check (Braun & Clarke, 2006; Smith et al., 2009).
Quotes extracted from the narratives of participants’ lived experiences were used to support the findings. To provide some needful context, bereaved family caregivers’ relationship to the deceased (“Spousal” or “Adult Child”), gender (“F” for female or “M” for male), and age (the number after “F” or “M” indicates their age) were included at the end of each excerpt. If the excerpt was translated from Chinese language, “translated” was indicated at the end. When necessary, minor modifications were made to the excerpts for easy understanding, without changing the semantics. Finally, the term “deceased” was used to refer to caregivers’ late spouses or parents both prior and after death.
Findings
Demographic Profile of Caregivers and the Deceased
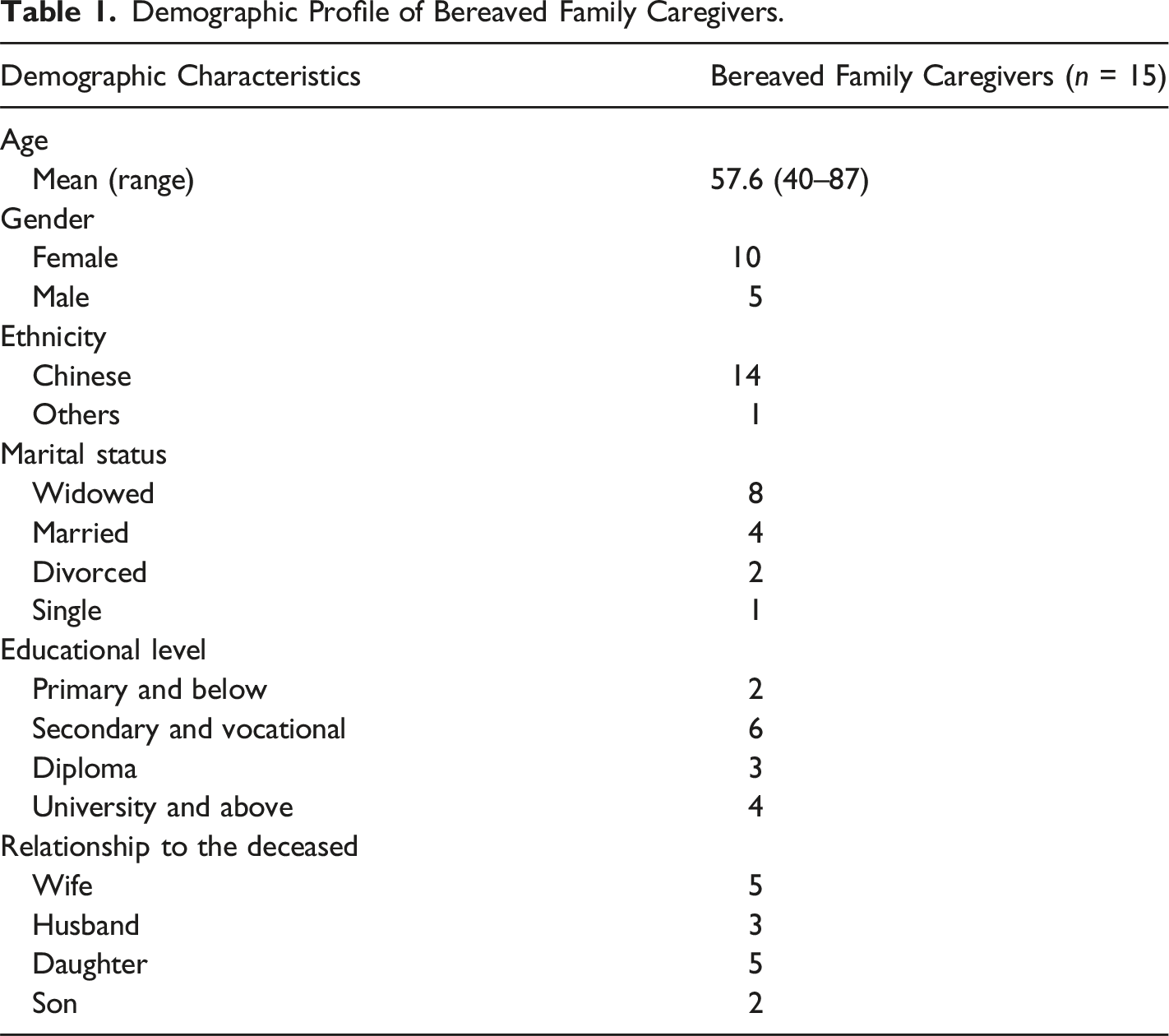
Demographic Profile of Bereaved Family Caregivers.
Demographic Profile of the Deceased.
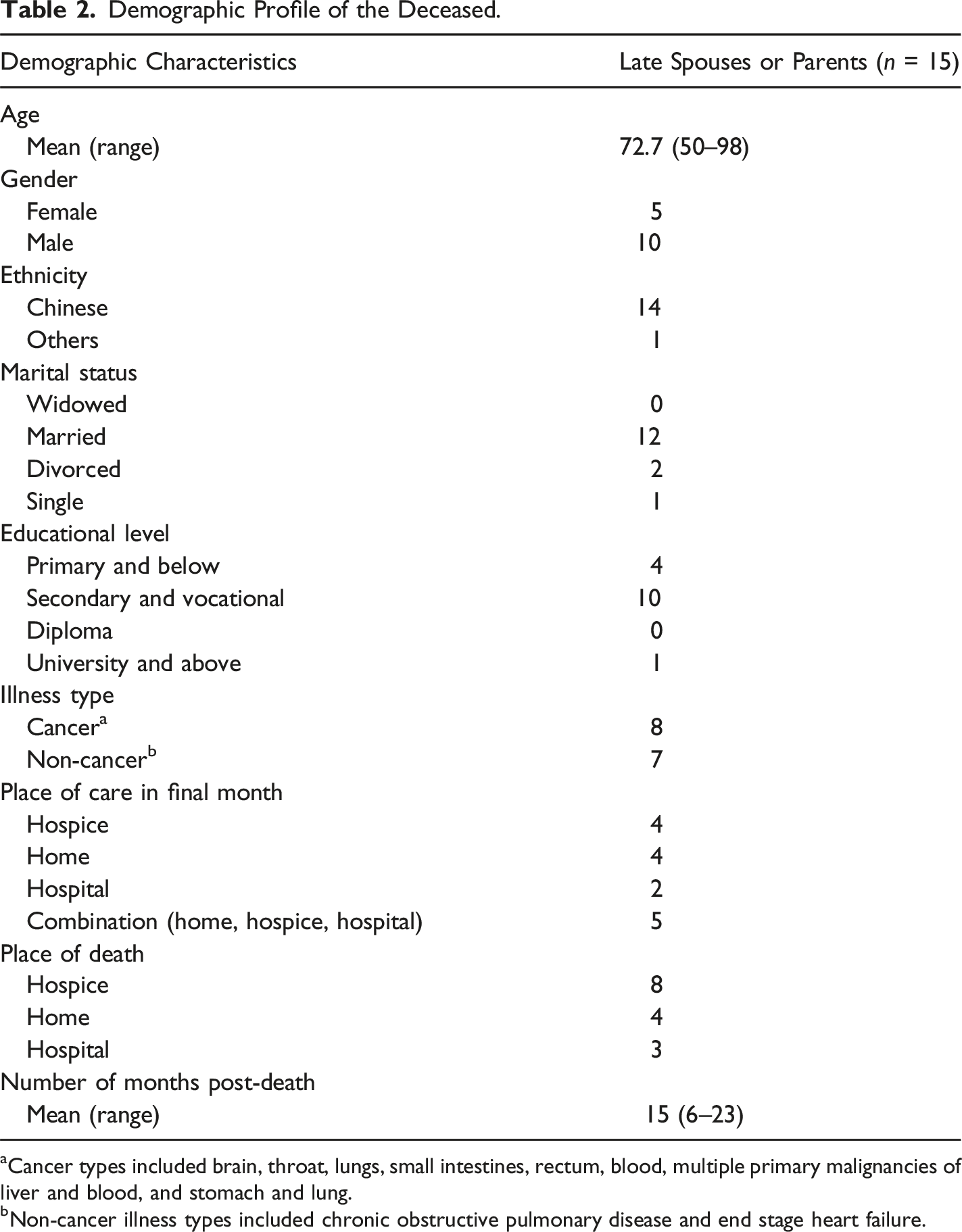
aCancer types included brain, throat, lungs, small intestines, rectum, blood, multiple primary malignancies of liver and blood, and stomach and lung.
bNon-cancer illness types included chronic obstructive pulmonary disease and end stage heart failure.
Major Themes and Subthemes
Bereaved Family Caregivers’ Coping with Bereavement.
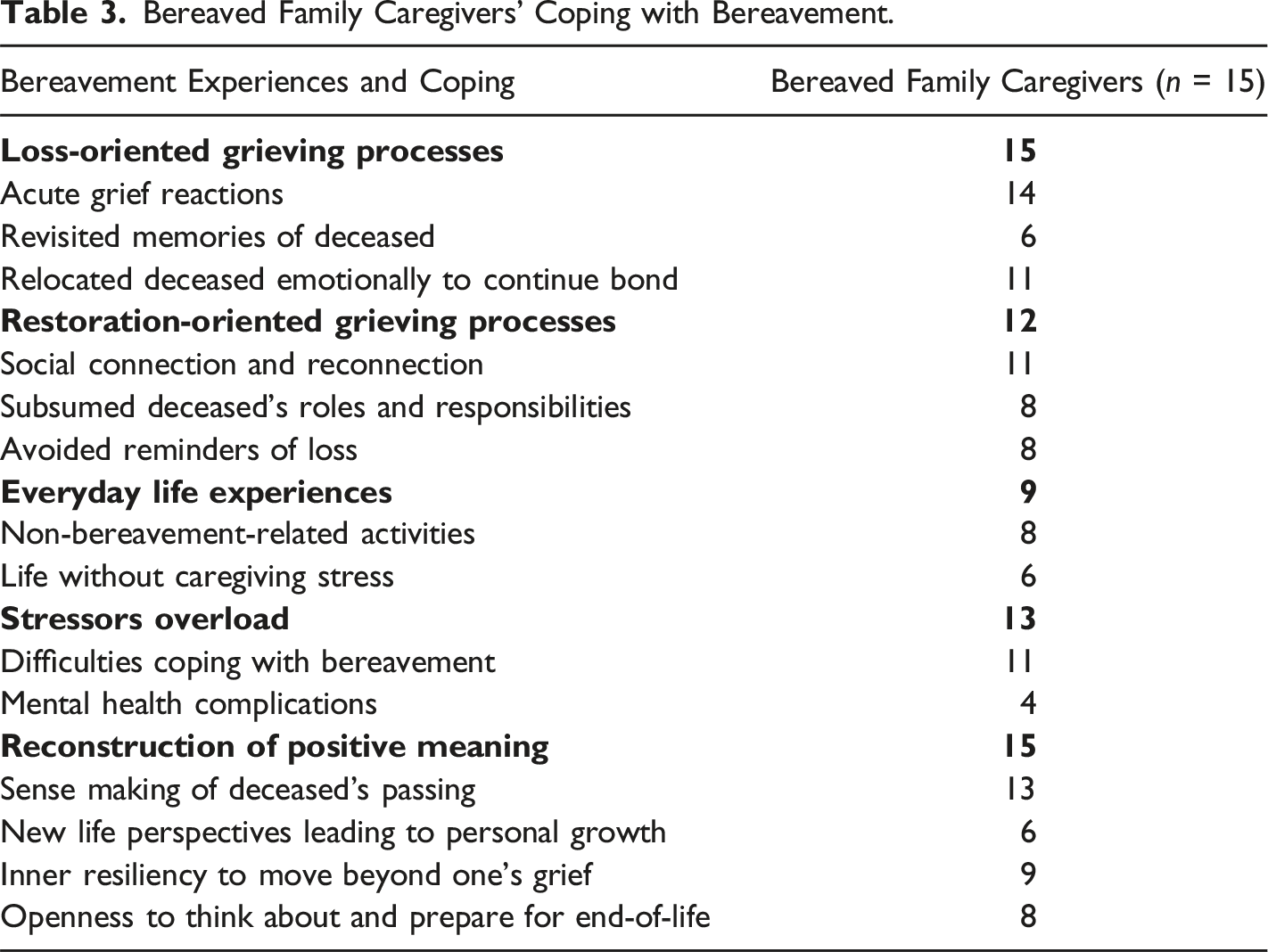
Loss-Oriented Grieving Processes
All bereaved caregivers, in one way or another, coped by centering on their loss experience itself and grieved over the deceased’s demise. In the LO mode, they responded with coping methods that confront their grief to achieve adjustments to their loss. These included acute grief reactions, revisiting memories of the deceased and relocating the deceased emotionally to continue bond.
Acute grief reactions
Like the common belief that a bereaved person experiences immense grief after the death of a loved one, all bereaved caregivers except one bereaved adult child reported experiences of acute grief reaction at some point of their bereavement. Many longed and pined for the deceased to be around. Other painful experiences were the lack of closure to the circumstances surrounding deceased’s death and having to live with regrets because they felt that they did not do enough for the deceased, like for Caregiver G. “The guilt that I wasn’t there (during his last moments). In the last conversation that we had, (I said) ‘I’m very tired, please don’t disturb me.’… Since I was very tired, he decided not to disturb me anymore forever. I really cried… (because) that was a mean thing to say at that moment… I mean I’ve said that many times to him… (but) it was nothing because he didn’t die. But that night, that was the last conversation that we had. In the morning he wasn’t conscious anymore. He was just breathing through the machine.” (Spousal Caregiver G, F58)
Revisited Memories of Deceased
Of the six caregivers who revisited memories of the deceased to cope with their loss, two disparate processes were observed. Bereaved spouses were inclined to ruminate on their loss and wallow in sadness, as presented by Caregiver H. “… I felt more emotional when I return home at night… thinking about things that happened in the past… and the whole process of (her) being sick was part of those memories, constantly appearing in my mind.” (Spousal Caregiver H, M68, translated)
In comparison, adult child caregivers were more likely to reminisce on fond memories of the deceased and remember the deceased together with other family members. Like Caregiver M, coping in these manners brought comfort to her. “So, sometimes after lunch, we would sit around the living room (and) talk about my father, then we share things about him in the past. I think that kind of helped everybody moved on a bit.” (Adult Child Caregiver M, F44)
Relocated Deceased Emotionally to Continue Bond
To cope with their loss, 11 caregivers relocated the deceased emotionally and found different ways to continue bond. This was observed across all subgroups. The most common was to visit the deceased at the columbarium, church, or temple and have conversations. Others placed symbolic objects at home to feel connected and close to the deceased. Even a seemingly simple act of talking to the deceased gave them comfort, like for Caregiver P. “I would say for me, (it was during the) down moments that I would seek her out. But there were also the quiet moments where I just felt like talking to her on a regular basis.” (Adult Child Caregiver P, F54)
Restoration-Oriented Grieving Processes
RO grieving processes focused on secondary consequences to the deceased’s demise. In the RO mode, instead of confronting one’s grief, the bereaved person distracts his/her attention from the loss and rebuilds his/her life without the deceased.
Social Connection and Reconnection
To cope with their loss, seven bereaved spouses and four bereaved adult children stayed socially connected. Especially for bereaved spouses, they used to spend their time with their spouse even prior to the illness and subsequently devoted themselves to caring for their dying spouse. Without their spouse, they needed other social activities to occupy their time. They also put in effort to reconnect dormant relationships to restore parts of their life that faded into the background during the caregiving journey. This was illustrated in Caregiver B who was a retired senior and living alone. “That time (when she just passed on) I was also alone, (because) the children were grown up and they had their own families. Sometimes, they came over to see me at night. Otherwise, I went over to see them because we stayed very close and within walking distance. A few months later, all my friends told me to take it easy. Everyone came to persuade me. Friends are very important, especially when you are old, you must have friends… they asked me out to swim and have meals, talked sense to me and then things were alright again.” (Spousal Caregiver B, M69, translated)
Of the bereaved adult children, four also maintained social connectedness. But unlike bereaved spouses, their motivations were about continuing family traditions after the loss of a parent and to keep the family together, as mentioned by Caregiver L. “I’m always the one who didn’t go (for the prayer sessions)… I said (that) next time I would come but I wouldn’t do the worshipping… because my siblings said it was like (a) family gathering… (and we) tried to gather for events… to keep the family together…” (Adult Child Caregiver L, F52)
Subsumed Deceased’s Roles and Responsibilities
In the deceased’s absence, roles and responsibilities previously played by them had to be reallocated to other family members. For six bereaved spouses, the impact was greater as their life with the deceased was closely intertwined within the marriage. Caregiver C was the youngest bereaved spouse in this study and the only one with young school-going children. Unsurprisingly, she faced most difficulties subsuming her husband’s roles and responsibilities. “For example, sometimes for meet-the-parent session, or anything, he would always attend. Sometimes, when our children had any issue and I didn’t know what to do, he was there to help… now if our children have any issues, I am on my own… I am on my own to do everything myself… it is significantly different (without him)…” (Spousal Caregiver C, F47, translated)
Among the bereaved adult children, only two adult child caregivers had to subsume household roles left behind by the deceased because of caregiving duties for their surviving parent, like in Caregiver O’s situation. “I try to take on that role. My helper is still there, I would tell her what to do. She’s a very experienced helper so eventually she knows what to do. And I started doing all the marketing… and get it delivered to my dad’s house.” (Adult Child Caregiver O, F57)
Avoided Reminders of Loss
Another way to cope with one’s grief was to avoid it, particularly at the initial stages of bereavement when grief reactions were immense. This was reported in five bereaved spouses and three bereaved adult children. Like Caregiver G, some engaged in activities that distracted them from thinking about the deceased because remembering was too painful. “Those places that would equate to when he was in his last days were very painful (reminders) for me. That was why when I had the time… (I) quickly got rid of all those things that would remind me of him… I packed all his clothes… (and) given it away. But, of course, I keep his photos there.” (Spousal Caregiver G, F58)
Everyday Life Experiences
Part of bereavement coping was to take respite from grieving and continue with their everyday life, and this was reported by nine caregivers.
Non-Bereavement-Related Activities
Of them, eight engaged in non-bereavement-related activities. This coping strategy was more prevalent among bereaved spouses, where seven bereaved spouses and only one bereaved adult child shared about their daily activities. Some examples were exercising, sourcing for better employment opportunities, and paying attention to one’s health. For Caregiver B, he was steadfast in his exercise regime to stay healthy. “… I usually swim on Mondays, Wednesdays, Thursdays, and Fridays… because (I) want to be healthy… In fact, I’m very healthy. I haven't seen a doctor for decades…” (Spousal Caregiver B, M69, translated)
Life Without Caregiving Stress
Six caregivers felt relieved when without caregiving duties. Especially for those who were full-time caregivers, they felt a greater difference in their daily routines and relief from caregiving demands upon the deceased’s demise. This was more commonly observed in four bereaved spouses as compared to two bereaved adult children, like Caregiver E who was the sole caregiver to her husband for many years. “Right after he passed away, I felt some sort of relief… I didn’t need to think of him every hour and second… (with) no time-limit you know, it went on and on and on, throughout the day and night.” (Spousal Caregiver E, F67)
Stressors Overload
While most caregivers had their fair share of difficulties coping with bereavement, a handful had more detrimental effects on their mental health. These observations paralleled the concept of overload in the revised DPM (Stroebe & Schut, 2016). However, this subtheme did not surface prominently. Due to the selection criteria of study participants, recruited participants were bereaved family caregivers who perceived themselves to be coping well as early as 6 months into bereavement.
Difficulties Coping with Bereavement
Six bereaved spouses and five bereaved adult children reported struggling with bereavement coping. For three bereaved adult children and the youngest bereaved spouse, they had no time to grieve because they were too occupied with their daily lives. As shown in Caregiver Q, spending time on grieving was a luxury that she could not afford after her father’s demise. “Maybe because I’m busy worrying about my mother… there wasn’t much time for me to grieve… Somebody had to hold the family together. Somebody had to do all the things that we still need to do to get our lives moving, to survive Monday, Tuesday, the week, the months, (and) the years, so… I never had the opportunity to really grieve.” (Adult Child Caregiver Q, F49)
Mental Health Complications
Among caregivers who faced difficulties coping with their loss, three bereaved spouses and one adult child caregiver experienced some form of psychological distress. For Caregiver M, it was traumatizing that her father was in a lot of physical suffering during his final days, and she could not make sense of it. Even up till the day of the interview, which was 19 months after his demise, she could only remember the desperate sound of his voice during those last moments. “… Until right now, I can still hear that voice in my head. That’s the only voice I can hear if I think about him now. I couldn’t hear any other things that he said, except that Thursday night when… he kept calling my name in that very desperate sound…” (Adult Child Caregiver M, F44)
Reconstruction of Positive Meaning
Another dimension of bereavement coping was thought processes and behaviours that were geared towards reconstruction of positive meaning, which included positive reappraisals of caregiving experiences, review of life goals, and moving beyond grief to embark onto a new chapter in life. This theme speaks of hope and optimism, is prospective in nature, and it concretizes into actions that build a better future for the bereaved family caregivers.
Sense Making of Deceased’s Passing
Upon the deceased’s demise, caregivers embarked on a journey to make meaning of their loss and, hopefully, come to accept it. While the acts of caregiving were done and dusted, the way caregivers thought and felt about those experiences could change according to the meanings attached to their lived experiences. Many positively reframed negative caregiving experiences to become meaningful and acceptable, which naturally led to more positive emotional reactions towards their loss. For Caregiver L, the sense of having done her best in caring for her father helped her to move on with no regrets and cope better with her grief. “Because when I perceived that he had… a good death, at least I could tell myself that I did my best, I made his life on earth comfortable, and I did my duty as a daughter. I think that (this) was enough for me to cope with the grief for the rest of my life!” (Adult Child Caregiver L, F52)
New Life Perspectives Leading To Personal Growth
Six bereaved family caregivers gained new life perspectives through journeying with the deceased, which led to personal growth and changes to life goals. Interestingly, five of them were bereaved adult children. Some learned lessons through the deceased’s life story and aspired to live a different life to avoid making similar mistakes; others realized that time is limited. They came to appreciate the importance of living life meaningfully, treasuring the time with their loved ones, and living in the present. For Caregiver N, his new life perspectives made him relook at his life priorities. “I realized that life is quite short… because my father passed away at 73 (years old), so that time I was already 38 (years old)… I did the averages and I realized that I was hitting almost half-way mark or slightly more… I realized that life actually is pretty short, and we got to ask ourselves what is important… (and) how much money is enough… For me, it was then relooking at it.” (Adult Child Caregiver N, M40)
Inner Resiliency To Move Beyond Grief
Instead of being stuck in grief, nine caregivers (six bereaved spouses and three bereaved adult children) displayed an inner resiliency to move on with their lives. This is explained by Caregiver Q. “I think the personality and character of that person (matter)… If you’re not mentally strong… it’ll take a much longer time… You need to tell yourself to snap out of it and move on with life… and I think at the end of the day… your mind would determine what you do with your life. How you’re going to move on (and) how you’re going to move out of it.” (Adult Child Caregiver Q, F49)
Some drew strength from their faith to live on, while others simply felt the need to move beyond their grief. This was observed in Caregiver A. “I still feel sad (about my husband’s passing), it's impossible to not feel sad...but life still goes on and I can't be trapped in my grief. I know one thing (for sure) is that I’m stuck in this sadness, and I must get out of it.” (Spousal Caregiver A, F50, translated)
Openness to Think About And Prepare For End-Of-Life
After journeying with the deceased during EOL, eight caregivers displayed more readiness to consider and prepare for EOL matters. Interestingly, this was more commonly observed in those whose loved one died of non-cancer condition, five as compared to three. Many shared that it was inevitable to envision their own death and dying, and often with reference to the deceased’s EOL experiences. For Caregiver F, after witnessing his wife’s passing, he wished for a death without illness to not burden his family. “… I feel that if you are going to die, just pass on and that's good enough. I don’t like being sick so frequently like my wife. When I am about to die, I want to die naturally and… don’t (want to) make it too difficult for (my) children and grandchildren to take care (of me)…” (Spousal Caregiver F, M87, translated)
There was also greater openness to think, prepare, and talk about EOL matters for self and others. For bereaved spouses, two had prepared for their funeral arrangements and purchased a niche to be with their late spouse, while three had put in place their last will, advance care planning, and/or lasting power of attorney. Preemptively, two bereaved adult children also started EOL conversations with their surviving parent. Caregiver D, like many bereaved spouses, felt the need to manage her EOL matters in advance. “In some ways, I am afraid that one day I would pass away suddenly, and then I would’ve a lot of things unsettled. For my husband, I could help him settle. As for me, I tried my best to slowly settle those that I could settle first, threw away things that I didn’t want, and gave away things that I wanted to give away. I wrote my LPA, appointed (the executer) for my will, and settled all that I could settle… because I don't know which day would be my turn to go, so I want to be mentally prepared first.” (Spousal Caregiver D, F71, translated)
Discussion
Four of the major themes identified in this study closely mirrored the key components of the revised DPM (Stroebe & Schut, 2016), making it an applicable theoretical framework to explain the bereavement experiences and coping of family caregivers in Singapore. Consistent with the well-established DPM (Stroebe & Schut, 1999; 2001a; 2016), all bereaved family caregivers deployed a repertoire of LO and RO coping strategies to deal with their loss and the adaptive oscillation between LO and RO grieving processes was prominent. They needed the time and space to experience the pain and sadness of losing the deceased, but also restore and rebuild their lives without the deceased. An often-neglected component of bereavement coping is the importance of taking time off from dealing with one’s grief and engaging in non-bereavement related matters, which is prevalent in the narratives presented in this study. Moreover, bereaved family caregivers who faced difficulties in coping with bereavement-specific stressors were more prone to experiencing stressor overload, which led to mental health complications.
Beyond the commonly known components of DPM, this study identified another integral part to the DPM – reconstruction of positive meaning. The processes of meaning making in bereavement is compatible with the principles of DPM, whereby the conceptual understanding of oscillating between LO and RO grieving processes fits with the oscillation between positive and negative reconstruction of meaning during meaning making (Stroebe & Schut, 2001b). Based on the studied narratives, bereaved family caregivers who achieved positive reconstruction of meaning saw beyond their loss and grieved adaptively. They progressed beyond the oscillation of LO and RO grieving processes into an adaptive state of bereavement. Their focus was no longer on the death event and the deceased, but how they wanted to live their own life differently and constructively because of their loss experience. This prospective element may be important both as an assessment and intervention tool to bereavement work, where positive reconstruction of meaning can be assessed as an outcome of adaptive coping and second-order change interventions can be geared towards achieving these adaptive states of bereavement.
With these study findings, this paper postulates that the DPM is an applicable theoretical framework for the bereavement experiences and coping of bereaved family caregivers who have lost either a dying parent or spouse within the Singapore context. It also gives indication that meaning making in bereavement is an integral component to the DPM and positive reconstruction of meaning might be a measure of positive bereavement outcomes. These findings support the need for more intervention studies to examine the effectiveness of bereavement interventions using DPM principles on bereaved groups. However, in line with existing literature (Chow et al., 2019; Stroebe & Schut, 2010; Stroebe et al., 2007), bereavement interventions should be targeted at a smaller group of bereaved individuals who are experiencing extreme and persistent mental and physical health complications because most bereaved individuals do possess the natural resiliency to cope with their losses. This inner resiliency to move beyond one’s grief was also observed among bereaved family caregivers in this study, especially for bereaved spouses who were more affected by their loss but still managed to adjust adaptively at their own pace.
This study has several limitations pertaining to its sampling criteria – age and race. There are emerging themes that suggested younger spousal caregivers had different caregiving and bereavement experiences as compared to their older counterparts. Given that they are more likely to have younger school-going child (ren), their parenting capacity for their child (ren), caregiving capacity for their dying spouse, and the time and space for them to grieve become competing needs. With a primarily older profile of bereaved spouses, the findings could not be extrapolated to younger bereaved spouses. Secondly, the recruited participants for this study were primarily Chinese (93.3%). As such, the findings might only be generalized Chinese bereaved caregivers.
Conclusion
The study supports the DPM as a suitable theoretical framework to guide assessment and intervention in bereavement work. More importantly, the discovery of positive reconstruction of meaning within the narratives of bereaved family caregivers suggests a promising outcome measurement to adaptive bereavement coping. Practitioners can then assess for successful oscillation between LO and RO grieving processes by identifying these adaptive states of bereavement.
Footnotes
Acknowledgments
We are grateful for the immeasurable support received from the colleagues at Assisi Hospice in the recruitment of study participants and the bereaved family caregivers who shared their life experiences. We also wish to thank Margaret Stroebe for her insightful comments on an earlier draft of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lien Centre for Palliative Care (LCPC-EX19-0003).