
Abstract
With few investigations of intra-family end-of-life conflict, this study sought to identify its incidence, cause, and impacts. A questionnaire was completed by 102 hospice/palliative nurses, physicians, and other care providers in Alberta, a Canadian province. Participants reported on how often they had observed intra-family conflict when someone in the family was dying, and the impacts of that conflict. 12 survey participants were then interviewed about the intra-family conflict that they had encountered, with interviews focused on why conflict occurred and what the impacts (if any) were. Nearly 80% of families were thought to experience end-of-life conflict, periodically or continuously, among various family members. The interviews confirmed three reasons for intra-family end-of-life conflict and three conflict outcomes that were revealed in a recent literature review. The findings indicate routine assessments for intra-family end-of-life conflict are advisable. Attention should be paid to preventing or mitigating this conflict for the good of all.
In most countries now, the vast majority of people who die each year are older (Rosser et al., 2019). These deaths are not typically sudden and unexpected, but instead usually follow a progressive illness or decline such that death can be anticipated and preferred end-of-life (EOL) care can be planned and hopefully provided (Lee et al., 2020; Mather & Loncar, 2006). Regardless, when anyone is living with an advanced terminal illness or is actively dying, this is usually a stressful and difficult time for the person and their family (Jeon et al., 2018; Teng et al., 2020). It would not be unusual for intra-family conflict to occur, such as disagreements between family members, or between the dying person and one or more family members (Boelk & Kramer, 2012; Lee & Kim, 2022). To date, EOL research has primarily focused on conflict occurring in hospitals and other healthcare facilities between formal caregivers, often physicians or nurses and the dying person or their family members (Mpinga et al., 2006). The shift of death, dying, and EOL care out of hospital and into the home, a shift that has been occurring in many countries, has made it imperative to examine intra-family conflict (Wilson et al., 2017).
According to a Harris/Decima public opinion survey conducted by the Canadian Hospice Palliative Care Association (CHPCA, 2013), 75% of Canadians would choose not to die in a hospital as they would rather die at home with their families present. This preference has also been noted in other countries (Fereidouni et al., 2021). Family EOL caregiving and home-based care circumstances are consequently of increasing importance (Bijnsdrop et al., 2020). A recent research literature review revealed intra-family EOL conflict may be common, although only a few (and often small) studies in the last 15 years have reported an incidence rate, with these ranging from 4.9 to 57% (Wilson et al., 2020). That review identified three common reasons for this conflict (i.e. family disagreements over curative treatment and/or EOL care and care decisions, previous family conflict and other family dynamic matters, and the dying process itself) and three primary conflict outcomes of this conflict (i.e. negative impacts on the dying person, negative impacts on the family or select family members, and negative impacts on other persons or the healthcare system). That review concluded that it is not clearly evident, at this point in time, how often intra-family EOL conflict occurs and why it occurs. Moreover, it is not clearly evident what the impacts or outcomes of intra-family EOL conflict are. A two-part mixed-methods research study was subsequently undertaken over the fall of 2019 and early 2020 to identify the incidence, reasons for or causes of, and impacts or outcomes of intra-family EOL conflict.
Research Design and Methods
With only a few research reports of any type available on the topic of intra-family EOL conflict (Wilson et al., 2020), a mixed-methods study was deemed the most relevant for developing an incidence rate and for gaining insight into the reasons for and outcomes of this conflict. Research ethics committee approval for this study was obtained in advance of data collection (ID# Pro00092598).
To collect quantitative research data relevant to developing an incidence rate, and also identify possible informants for subsequent qualitative interviews, a brief survey tool was developed, pilot tested, and made available in the fall of 2019 in multiple venues to attract participants who would have or are likely to have noticed intra-family EOL conflict (see Appendix A). The targeted informants were hospice and palliative program managers and staff, including volunteers, hospital and community nurses, primary care physicians, and members of organizations designed to address the interests of older adults in the Western Canadian province of Alberta; the home province of the Principal Investigator. Many organizations broadcast an advertisement for volunteers. For instance, the Alberta Hospice Palliative Care Association shared the research advertisement on their Web site, along with the informed consent letter and survey form. In addition, the questionnaire and information letter were provided in paper format at 11 nursing or family caregiver meetings that fall, meetings where attendees who had cared for dying people were present. Study participation was voluntary, and all were assured that no individual or organization (other than the one named above) would be identified in any verbal or written reports of this study.
The survey tool asked participants to indicate how often they had observed or came to understand that intra-family conflict was occurring when someone in the family was dying. More specifically, each was asked to provide a percentage figure representing what they believed was the proportion of families that experience intra-family EOL conflict. After 102 people had completed and returned the form, with 100 providing a percentage figure, this phase of the study was concluded and the survey form withdrawn from circulation. An average/mean number from the percentages was calculated, and the distribution scores of range and mode were determined using the SPSS (version 21) program.
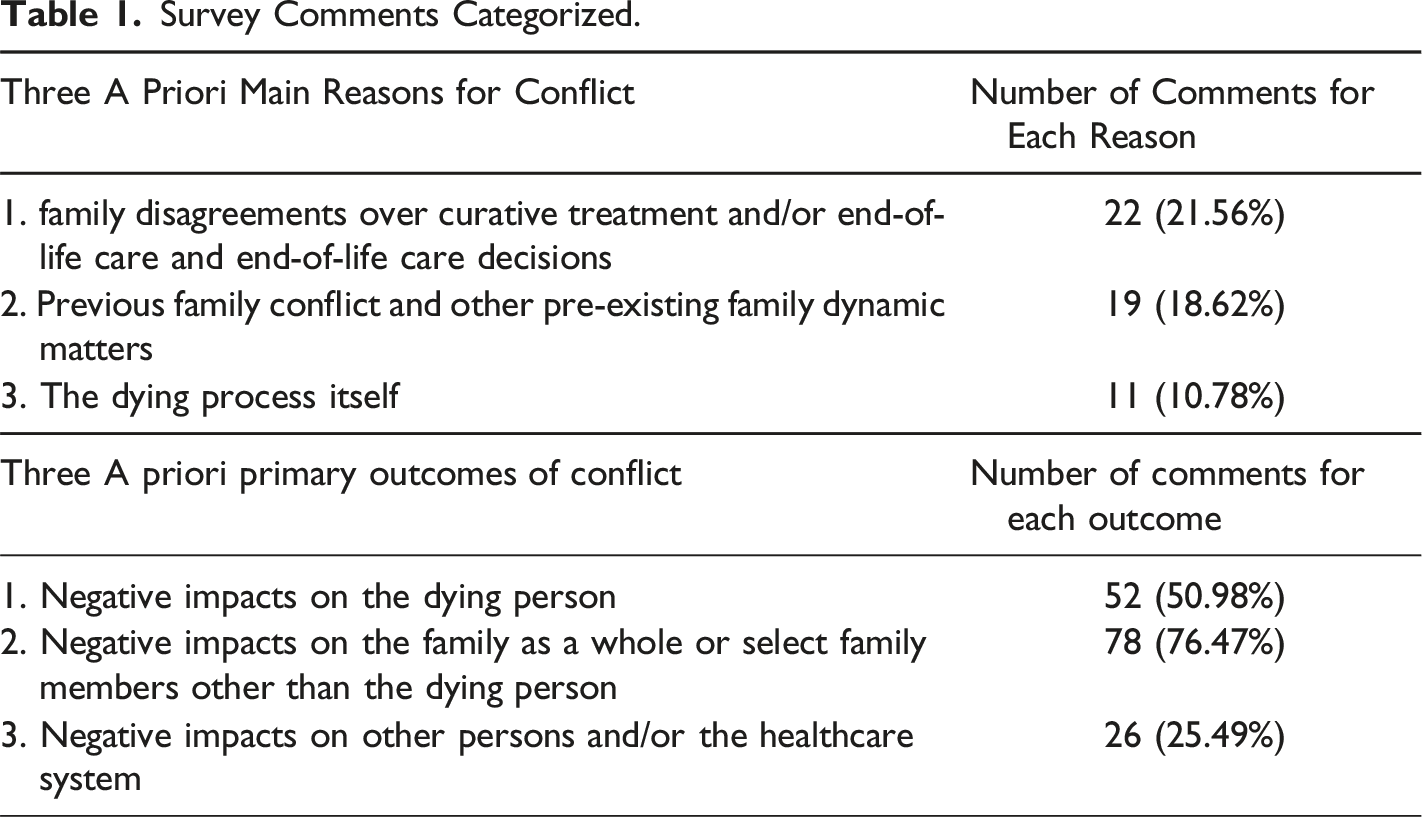
On the survey form, informants were asked to comment on what they saw or believed the impacts or outcomes of this conflict were. Most provided some comments, with some of these comments also revealing factors contributing to or potentiating intra-family EOL conflict. These survey text comments were subjected to content analysis (Hsieh & Shannon, 2005), with this work undertaken to determine if the comments could be grouped into the six EOL family conflict cause and outcome categories that were identified in a recent research literature review (Wilson et al., 2020). As indicated previously, that review revealed three primary outcomes of conflict and three main reasons or factors potentiating conflict. Outliers were to be noted, although none were identified in the survey text comments.
Following this analysis of written survey text data, survey participants who had indicated that they were available and willing to be interviewed (N = 32), and who had supplied an email address and telephone number, were contacted to arrange a telephone interview. The telephone interviews followed an email to each potential interviewee to ensure that they understood the study purpose and its procedures, which included a verbal consent to be interviewed by phone on a day and time of their choosing. Moreover, a set of questions was shared with them in advance of the interview to facilitate each semi-structured interview (see Appendix B). All were told through this email and at the beginning of a pre-arranged telephone call that these voluntary interviews were being done to gain insight into the reasons for intra-family EOL conflict and the outcomes or impacts of this conflict. After 12 informants had been interviewed, each through 45–95 minute telephone calls, data saturation was reached and this (second) phase of the study was ended.
Notably, all data were collected before the COVID-19 pandemic began to greatly impact Canada and other countries in March of 2020. The Principal Investigator conducted all of the interviews because she has completed many qualitative studies, and is comfortable with qualitative interviewing and data analysis. No participants dropped out after arrangements had been made to conduct their interview on a day and time of their choosing. None wanted to review the transcript of their interview. No participant names or other identifying information were kept on the interview transcripts or field notes, so only the interviewer could identify or determine who had been interviewed.
Each semi-structured interview was taped and transcribed the same day for rapid constant-comparative data analysis. The manual analysis of transcript data, conducted first by the Principal Investigator, focused initially on validating the interview questions and process, and then on identifying and verifying the findings through ongoing coding and categorization of the data. Each transcript was also reviewed to determine if new or unclear data and information gaps existed, particularly in relation to any outliers identified through the survey text analysis, and then to determine when data saturation was present. Following this initial data analysis, the research team reviewed and after discussion and revisions ultimately approved the findings. The team then assisted in developing this report of findings. In this way, the trustworthiness of the qualitative data gathering, management, analysis, and reporting process was enhanced.
Results
Survey Findings
As indicated above, 100 people provided a percentage estimate of how often they had observed or came to understand that intra-family conflict was occurring when someone in the family was dying. The average/mean was 79.86%, with scores ranging from 20% to 100%. The distribution of scores was skewed and bimodal, with 14 participants reporting 95% and another 14 reporting 100%.
As indicated, most (98%) of the 102 survey informants commented (briefly) on what they saw or believed were the outcomes or impacts of EOL intra-family conflict. Many comments revealed more than one outcome, and some also revealed factors causing or potentiating intra-family EOL conflict. Roughly half of the written comments were focused on the last case of conflict or perhaps the worst case that they could recall, while the remaining half were more general in nature. For instance, one informant wrote “I recall one case, where the family members stopped talking to each other and some stopped visiting the patient; one became the decision maker then and that person was angry and upset, and our (hospice) staff had to deal with that anger.” Another wrote “the dying person and their family are often impacted, as it fractures family relationships; this creates stress on dying people and creates confusion among the caregivers.”
Survey Comments Categorized.
Qualitative Interview Findings
The interviews also confirmed the three a priori conflict factors and three conflict outcome categories. No additional categories were identified through the 12 interviews. The following is an overview of the interview findings for each category, with selective quotes provided to illustrate the diversity within but also relevance of each category.
1. Conflict Causes
1.1 Family Disagreements Over Curative Treatment and/or End-of-Life Care and Care Decisions
All interviewed participants provided insights about family conflict arising over treatment decisions or EOL care and EOL care decisions, if not the decision-making process for these decisions. Three quotes illustrate the diversity of this conflict.
“Most family members have never been involved in such major decisions before. It is really hard on them, and so it is not unexpected that there would be disagreements among them about what to do when confronted with death. How would they know what to do? They are often given the impression that they alone are making these decisions, when the reality is that nature will take its course, one way or another. And, there are often advance directives now, and also EOL care standards and good patterns of care to follow” (P6).
“Once in a while someone in the family is very pro-life, at all costs. This is often someone who jumps in at the end, and they want a say in decision making. Sometimes they present themselves as an expert. That makes it tough on the rest of the family, and even the dying person who may still be trying to direct their own care. The worst was when someone demanded that chemo and the works be done, after three rounds of chemo had not worked, and the patient had said no more. At that point, the patient was clearly dying and unable to speak for himself. What was the rest of the family supposed to do? Most were accepting of the coming death, but were brought into a major conflict by that one family member who was yelling at them and saying we would all be sued as what we were doing was immoral” (P4).
“At the heart of this is love for the person who is dying; with huge losses for those left behind. This is major grief, anticipated, expected, and soon to be a reality; this is not just passing sadness over the death of a friend, but instead a big death. No wonder the family as a whole can disagree about EOL care. This is the end, you don’t get another chance. It is someone irreplaceable” (P12).
1.2 Previous Family Conflict and Other Existing Family Dynamic Matters
All but two of the participants highlighted previous family conflict or existing family dynamic issues as a contributor to conflict. Three quotes illustrate the relevancy of considering previous family conflict or other established family dynamic matters for sparking new or continued conflict.
“It quickly became obvious that the family members were not talking to each other. One told us they had not been a family for years. Each would come to the (hospital) desk and ask about something, often times just wanting some information, or make a demand for us to do this or that. It was repetitious and time consuming for us to deal with all that, and sad that they could not come together to share information and support each other” (P10).
“I think family issues explain a lot. For instance, sometimes we see a less than perfect dying person. There can be a lot of baggage among that person’s children or other family members. Add death and dying on top of that, and you should expect conflict. Conflict can be so severe, sometimes no one comes to visit the deathbed. That is when you know how bad it is, or it must have been in that family. We send the nursing students in then to sit at the bedside until the end. At least that way, they are not alone” (P3).
“We provide home care services and sometimes have had to threaten to call the police, or leave and come back later when certain family members have left the home, as the family is at war. Fighting must make for a pretty poor death for the family, and they still have the funeral to get through” (P8).
1.3 The Dying Process Itself
All informants highlighted the dying process was a contributor to family conflict. Three quotes illustrate how the dying process can lead to conflict.
“Once the main family carer and the others realize that it is very close to the end, this is a time of high anxiety, and it does not take much at this time to spark conflict in the family” (P2).
“Not many family members have ever been at a deathbed, and sometimes the smells and the look of the dying person is just too much for them. Anger is common and questions come out such as why is she/he smelling or looking like that? Basically, they are saying - what are you doing wrong or not doing right - so a pretty death takes place. There are not many pretty deaths, I’m afraid to say” (P5).
“Sometimes it is hard to control pain or restlessness at the end. It can take some time to get the doctor to come and assess the patient and order terminal sedation or a pain killer that we (the hospital nurses) think would work. Then it takes time to get the med up and for it to work. Every minute that passes is tough for the family sitting there. Each one has expectations and each manages stress a little differently – so conflict among them is likely to be common then” (P7).
2. Conflict Outcomes
2.1 Negative Impacts on the Dying Person
All interviewees commented on direct and indirect negative impacts on the dying person with intra-family EOL conflict. Three quotes illustrate these negative impacts.
“Can you imagine being on your deathbed, and being aware of your family fighting around you? I can’t think of a worse death; how stressful that must be, and how tiring and upsetting. We had a patient who would cry after his visitors left, after he tried to make peace between them. We could not get him comfortable and out of pain; he was so preoccupied with making peace” (P11).
“As a palliative nurse practitioner, I have had to set up rules as to when each family member can visit, and what each one is supposed to do when visiting, and also what they cannot do. I remember one person trying to force food and water into someone who would have choked on it. She was not ready or accepting of the death. But I feel really bad about one case where an older woman died alone at home, when one family member had left and another had not arrived. She had been so afraid of dying alone; she had end-stage lung disease and would gasp for breath” (P9).
“Our father was at home with me near the end, and it started to become obvious that no one would visit him in my house. He asked to move back to his house, but I could not be there 24/7. None of my sisters or brothers knew how to care for him, and I don’t think they wanted to, they just were mad at me; so he did not get much help as he got weaker and weaker. I will never forgive them for that” (P1).
2.2 Negative Impacts on Their Family or Select Family Members
All interviewees commented on negative impacts on family members or the family as a whole as a result of EOL intra-family conflict. Three quotes illustrate the range and intensity of these impacts.
“I will never forgive them (for making my father move back to his home from mine and then not helping him there as he was dying). We got through the funeral, and I have not seen or talked to any of them since. I don’t ever want to see or talk to them again” (P1).
“We have had to step in and establish who will speak for the patient, as we have seen the wife and other main caregivers bullied by a family member. They know exactly what the dying person wants, they have talked about it together, even if there is no written directive, but then are made to feel bad and doubtful by the bully. Imagine that legacy, something they will always think about and regret into the future, long after the death” (P10).
“We often see family members in again after the death for bereavement care. Usually, these are the ones where it was not a good death for them. Often this is because of unresolved anger or upset with the dying person or because of family feuds. We do everything to have the best death possible in our hospice, but we can’t do away with years of family fighting” (P12).
2.3 Negative Impacts on Other Persons or the Healthcare System
Most but not all interviewees commented on direct and indirect negative impacts on other people or organization, and/or the healthcare system as a result of EOL intra-family conflict. Three quotes illustrate this diversity and seriousness.
“Her family was furious at me (for setting up visiting hours to separate family members, and then the woman died alone), as if I could predict when she was going to die. What was I supposed to do? They could not be in the same room at the same time or they would fight. They complained about me to my boss and their MLA (provincial politician), and I had a lot of explaining to do” (P9).
“We have people coming to our hospice because of family conflict. A home death, even if that is what the dying person wants, is not possible. Their conflict carries on, into our hospice” (P4).
“I recall a sad case where the family members were not talking to each other. We could have sent the patient home to die, and we needed the bed as the hospital was full, but with that much conflict in the family, no one was willing to take him home” (P10).
Discussion and Implications
The evidence identified through this mixed-methods study, although not generalizable across or outside of Canada, nor likely representative of all intra-family EOL conflict situations, should be useful for raising awareness of intra-family conflict as an EOL consideration. This awareness may generate changes in hospice/palliative programs and other EOL services or service approaches to ensure routine assessments for potential or actual conflict and perhaps also systematic efforts to prevent or address existing intra-family EOL conflict. It would appear that this work is imperative as intra-family conflict was found to be both common and consequential. This conflict also appears to be easily initiated by many different factors or circumstances, although these could be categorized into the EOL care decisions and EOL care itself, the dying process, and previous family conflict.
Considering this, and the fact that family conflict is a factor that will most certainly interfere with the provision of high quality EOL care (Kramer & Yonker, 2011; Oetzel et al., 2015), the Family Health System model may be a useful approach as it “offers an integrated way to examine family dynamics, family strengths, and family concerns in health and illness across the life span” (Anderson, 2000, p. 104). Care staff training to expect and manage intra-family EOL conflict is another option (Krakowiak, 2020; Trankle et al., 2020). To that end, a Decisional Conflict Scale is available for use in assessing conflict (Fairlie, 2018). Moreover, reviewing the conflict resolution strategies that have been used by others could be helpful (Hopeck & Harrison, 2017). This work is important as families often feel a major imperative to enhance the dying person’s quality of life until a dignified death occurs, but with this goal a major stressor for them (Phillips & Reed, 2010).
The current study and its findings will also hopefully encourage future research on intra-family EOL conflict. More research is needed as this study report is only one additional report added to 18 research reports on intra-family EOL conflict published in a recent 15-year (2004–2019) timeframe (Wilson et al., 2020). That 15-year timeline was employed because Mpinga et al. (2006) reviewed end-of-life family conflict reports published before 2004. Mpinga et al.’s (2006) review was confined to causative factors and outcomes of conflict, however. Of particular importance now is for research in other Canadian provinces and countries to be done to validate or correct this study’s identified high incidence (nearly 80%) of intra-family EOL conflict, and validate or add to the identified six a priori categories of conflict causes and outcomes. Evidence-informed learning about and insights into intra-family EOL conflict are very much needed.
Some research considerations and limitations arising with the design of this mixed-methods study are necessary to outline. The first is that select Albertans were asked to complete a newly-drafted simple and short survey tool (attached); this tool may require further development. Moreover, the number of survey respondents was small (N = 102), with larger studies advised, particularly population-based or population-representative ones.
Another limitation is that the survey respondents for the current study may not have been the best informed on the subject of intra-family EOL conflict, and so the identified incidence of 79.86% may be artificially high or low. Indeed, if assessed against the findings of other published studies, which ranged from 4.9 to 57% (Wilson et al., 2020), it would appear that the gained Alberta incidence is high. However, the survey informants who provided a percentage estimate were people who through their healthcare work or involvement in hospice/palliative and seniors organizations should be able to report on this matter. As such, the incidence rate may be correct, and even if too high, an incident rate nearing 80% should warn hospice/palliative and EOL providers of the need to anticipate and address intra-family EOL conflict (Hamano et al., 2018).
Another limitation is that this study did not establish the timing of conflict. Some other research has done that, however, such as Rhodes et al.’s (2017) study that revealed intra-family conflict occurred at periodic intervals over the course of a terminal illness. Another investigation revealed 57% of 116 family members noticed some EOL conflict occurring over the course of a terminal illness, but family conflict became uncommon after a hospice admission had taken place (Kramer & Boelk, 2015). A different investigation found conflict occurred when an immediate death became obvious (Kramer et al., 2010). Other timing or geospatial considerations may be important, as Muni et al.’s (2011) study of the nursing notes written for 3,138 patients who died in an intensive care unit revealed 4.9% of white families and 7.9% of non-white families were observed as having intra-family conflict while their family member was receiving care there. As such, it is possible that intra-family conflict is periodic, but it is also conceivable that it is ongoing or permanent once initiated.
Another consideration for future research is in relation to qualitative research studies often using reflexivity and other measures to ensure that no preconceived or predetermined understandings of the data or the subject area exist among the researchers in advance of or during the data collection and data analysis. This mixed-methods study instead used six a priori categories of findings gained through a literature review of 2004-19 research publications on contributing or causative factors and also conflict outcomes or impacts. Those categories were used as a basic framework to analyse the survey text and interview data. As identified earlier, the survey comments and interview transcripts confirmed all six a priori conflict factors and outcomes, with no additional categories identified.
As such, it was apparent through this study that there are harmful effects from intra-family EOL conflict for the dying person, the family as a whole or individual family members, and also negative impacts on other persons and organizations. It is of great concern then, with intra-family EOL conflict, that the care needs of the dying person may not be met as planned and as desired in advance (Arnold et al., 2007). Moreover, the dying person will likely have more stress or distress and less support from the family (Boelk & Kramer, 2012; Broom & Kirby, 2013; Elliott et al., 2007; Morasso et al., 2008). It is also of great concern that EOL conflict can impact individual family members or the entire family. Other studies have illustrated more stress and distress for families where there is EOL family conflict (Boelk & Kramer, 2012). The primary family caregiver is often the most at risk in these conflict situations (Benson et al., 2019; Chung et al., 2018; Morasso et al., 2008). Severed family ties now and into the future is another concerning outcome, as indicated in this study and other studies (Boelk & Kramer, 2012; Morasso et al., 2008). In addition, more severe and also prolonged family member post-death grief is another impact established in a previous EOL family conflict study (Kramer et al., 2011).
The current study found intra-family EOL conflict was often also impactful on other people and healthcare organizations. Previous studies have found nurses experience more stress and distress when they provided EOL care in a hospice or other care setting while intra-family conflict was occurring (Boelk & Kramer, 2012). This outcome is important to consider as intra-family EOL conflict may create harsh working environments for nurses and other formal care providers, which can lead to emotional burden or burnout. Furthermore, hospice and hospital admissions are necessary when home deaths became impossible because of family conflict (Broom & Kirby, 2013; Kouyoumdjian et al., 2019). This location change is problematic for many reasons, including increased health system utilization and higher EOL healthcare costs.
Conclusion
This two-part mixed-methods research study identified an incidence of 79.86% for intra-family EOL conflict, and confirmed (previously-identified) three primary causes and three main impacts or outcomes of intra-family end-of-life conflict. Using a priori categories to analyze qualitative text and transcribed interview data was a useful way of making sense of highly diverse survey and interview data. The findings suggest routine assessments for potential intra-family EOL conflict or already existing conflict are advisable. Much can be done to prevent and alleviate this conflict, with good communication perhaps the most important measure given the stress and anxiety of all involved (Hebert et al., 2009). Clearly, attention needs to be paid to prevent or mitigate this conflict for the good of all (Borgstrom, 2020).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.