
Abstract
Drug-related deaths constitute a significant challenge that strongly impacts the lives of the bereaved and the risks of mental and social problems are well-documented. This paper is the first one to explore how bereaved siblings experience informal support after drug-related deaths. Reflexive thematic analysis is used to analyze ten semi-structured interviews with bereaved siblings. Three main themes were identified: (1) valued support elaborates on the range of desired support and content of the support received; (2) barriers to support were connected to complex family relations, different grief reactions, and stigma, shame, and devaluation; (3) ways to promote support focus on openness and mutual closeness. The discussion revolves around the ‘strong’ sibling role, complex family relations, stigma, protective silence, and disenfranchised grief. Interactional aspects involved in social support and the importance of addressing this in clinical practice, to utilize the vital support potential for the bereaved experiencing drug-related death, are discussed.
Introduction
Drug-related deaths (DRDs) have many negative consequences for the close bereaved left behind (Dyregrov & Selseng, 2022; Titlestad & Dyregrov, 2022). Drug-related mortality constitutes a significant public health concern and social challenge in many countries. More than 200,000 people die from illicit drug overdoses every year in Europe and when all DRDs are included, such as overdoses, deaths related to HIV, hepatitis C, and infections, this figure is even higher (EMCDDA, 2019). One can estimate that, in regard to those who were close to the deceased, there may be 10–15 people who are strongly affected by the death, which means that globally, 2–2.5 million people lose someone to a DRD every year. The scarce literature on what happens to the bereaved following a DRD includes some research on family members’ experiences of bereavement (Titlestad et al., 2021), but none concerning how the bereaved siblings cope with such a death. Thus, siblings and their experiences of informal support after DRD are the focus of this article.
Drug-Related Death Bereavement
Although death is, basically, a natural part of life, research has shown that those who experience sudden, unexpected and often premature deaths, especially that of a DRD, struggle more afterwards than when the death is more natural and expected (Dyregrov, 2003a; Li et al., 2003; Rostila & Saarela, 2011; Rostila et al., 2013; Titlestad, Mellingen et al., 2020). Titlestad and colleagues (2020a) documented that parents bereaved by a DRD experienced how silence from helpers, self-stigma and complicated interactions within their social networks contributed to a ‘special grief’.
Being a grieving sibling is a different experience to that of being a grieving parent. Adult siblings have a unique relationship, sharing biological composition, family history, and a long-lasting relationship. Large studies have documented that experiencing sibling loss may be detrimental to the bereaved, as it is often caused by sudden and unexpected deaths (Rostila et al., 2013), such as a suicide, an accident or an overdose. Large scale studies have revealed increased mortality risk following sibling death (Rostila et al., 2017; Yu et al., 2017), that sibling death in childhood is associated with an increased risk of mental disorder (Bolton et al., 2016; Rostila et al., 2019) and poses significant evidence for suicide risk (Bolton et al., 2016; Rostila et al., 2013).
For siblings bereaved by a DRD, we identified one study that investigates consequences for their psychological well-being. In a prevalence study of bereaved family members of a drug-death, 21.8% of the 78 siblings who participated in the study had prolonged grief symptoms above the cut-off score for prolonged grief disorder (Titlestad & Dyregrov, 2022). In a study of sibling suicides, Dyregrov and Dyregrov (2005) termed the remaining siblings as ‘the forgotten bereaved’, as the professional help and social support was only directed at the parents. Additionally, Zampitella (2011) explored adult siblings’ loss and the familial changes post-loss and characterised the bereaved adult siblings as ‘the disenfranchised grievers’.
Drug-Death Related Stigma
According to Link and Phelan (2001), stigma occurs when interrelated components, including labelling, stereotypes, separation (us/them), status loss and discrimination, converge. Thus, stigma is a complex social problem that operates at interpersonal, intrapersonal and structural levels (Hatzenbuehler & Link, 2014; Link & Phelan, 2001). Since individuals with substance use dependence are prone to stigma in most societies, close family members, such as parents and siblings, may be forced to share the discredit that is associated with ‘their’ stigmatised family member and, in this way, can become stigmatised themselves. Sheehan and Corrigan (2020) conceptualise this as associative stigma, describing how family members, friends, health workers or other acquaintances may be tainted by stigma through their connections to the stigmatised individual. Recently, Dyregrov and Selseng (2022) elaborated on how the bereaved following a DRD must deal with the harsh stigma and unkind reactions from their environment on top grieving their loss. Stigma thus adds another burden for the bereaved to deal with post-loss, and this therefore calls for more knowledge about how they are being supported after such deaths.
Informal Support From Social Networks and Peers
Two relevant forms of help stand out for bereaved: ‘formal’ support (professional), or ‘informal’ support (social network support, peer support). We address informal support in this article. Helpful informal support is highly valued by various groups following on from an unnatural death and may be decisive when it comes to dealing with grief processes in a more favourable way (Dyregrov & Dyregrov, 2008; Lakey & Orehek, 2011; Mead et al., 2001; Nurullah, 2012).
Peer support is unique, as the source of the support is that of a peer; i.e., a person who is equal in key areas, as through experienced loss and grief, and is based on an equal relationship. This type of support has several distinct characteristics: fellowship, meaning creation, understanding, hope, advice, and time-out. The positive effect of peer support is especially related to sharing personal experiences, gaining information and knowledge from each other, as well as receiving and providing emotional support (Dyregrov & Dyregrov, 2005, 2008; Kowitt et al., 2019). Lakey et al. (2002) document that people with similar relationships should be more effective in regulating each other’s emotions as their similarities in attitudes, values and life experiences are among the strongest markers of supportiveness (Lakey et al., 2002), and the importance of peer support has been confirmed in relation to both natural and unnatural deaths (Kowitt et al., 2019; Mead et al., 2001).
Social network support derives from family, friends, work colleagues, neighbours and other acquaintances and consists of consolation, social stimulation, information, advice, participation in routines, rituals and practical and economic assistance (Dyregrov & Dyregrov, 2008). What is perceived as a ‘good network support’ often originates from stable and relatively long-lasting social relationships where people are connected to each other on the basis of previous interactions and mutual expectations. Thus, the dynamic and interactional processes that take place during these encounters are highly relevant in understanding the value/helpfulness of such support (Dyregrov et al., 2018; Lakey & Orehek, 2011). The relational regulation theory (RRT) (Lakey & Orehek, 2011) describes how people regulate strong emotions in daily life interactions. Thus, RRT claims that social network support will influence the regulation of one’s feelings and the cognitions and behaviours of bereaved individuals, which will subsequently result in better (or worse) psychological adjustment. Importantly, this regulation is typically reciprocal in that the interaction initiated by a recipient (e.g., a bereaved individual), influences the impact, thoughts and actions of the provider (e.g., a network member), which will, in turn, influence the recipient. Communicating social support that is adapted and appropriate to the individual and the situation might therefore be associated with a myriad of challenges (Lakey & Orehek, 2011).
Attachment Style and Social Support
There is convincing evidence that social support and the importance placed on intimate relationships vary as a function of attachment style (Rapoza et al., 2016). As a result of this, whether the parties have a secure or insecure attachment style seems to be one key element when it comes to understanding the disparate influences that social support can have within dyadic interpersonal relationships. As stated by Florian et al. (1995), the formation of an attachment style is based on the dyadic relationship between caregiver and infant and may explain how the desire for and sense of social support originates. Individuals classified with secure attachment have consistently been found to report more perceived support in the social environment and greater satisfaction with levels of support than insecurely attached individuals.
The level of closeness in a relationship can be identified in features such as trust, intimacy, and mutual support. Rapoza et al. (2016) also reported that dimensions of insecure attachment (i.e., being avoidant and anxious) functioned as risk factors for physical and psychological health, and that insecure attachment was linked to poorer health outcomes. While anxious attachment evidenced a more direct relationship to poorer health, avoidant attachment did so through a more indirect moderated relationship. Social support was moderated by the avoidant attachment dimension, providing little benefit to those high up on the avoidant attachment scale (Rapoza et al., 2016). Thus, both the studies conducted by Lakey and Orehek (2011) and Rapoza et al. (2016) encourage researchers to explore the protective function of social support depending on the extent to which an individual is comforted by the care and concern provided by another.
In interviews with 14 bereaved parents post-DRD, Titlestad et al. (2020b) documented that support from family members and friends was experienced as most important, but only when the support fulfilled their different needs and thus was experienced as helpful. Unhelpful support came from poor communication and ignorant or stigmatic utterances relating to drug use. Moreover, the study also showed that the parents called for peer support from other people who had lost a loved one to a DRD, because they felt that only those who had suffered the loss of a DRD could fully understand them. However, we have no knowledge about siblings’ experiences of informal support after a DRD. Knowing more about bereaved siblings’ experiences of social support and having insight into the factors that act as barriers or promote said social support is pivotal when it comes to facilitating social support within social work. The aim of this article is therefore to convey knowledge about siblings’ experiences with informal support after the loss of a brother or sister in DRD. The article will: 1. Explore DRD bereaved siblings’ experiences with and evaluation of informal support; i.e., support from peers, families, and friends. 2. Explore the factors that inhibits or promote informal support. 3. Explore siblings’ perspectives on how to optimise informal support for those bereaved from a DRD.
Method
Methodological Overview
This article is part of the Drug Death Related Bereavement and Recovery project (END), which is a nationwide, cross-sectional, mixed-methods study conducted in Norway. The main objectives of the END project are to explore how those bereaved by a DRD experience grief and stigma, and how formal and informal helpers support them (ResearchGate, 2022). The END study was approved in February 2018 by the Norwegian Regional Committees for Medical and Health Research Ethics (2017/2486/REK vest). The total sample used for END consists of 255 bereaved who have lost a child, parent, sibling, partner, other family members, or a close friend to a DRD. Among the various groups of bereaved included in the study, siblings who have lost a brother or sister in DRD, will serve as the focus of this article.
Procedure
From March 2018 until the end of December 2018, those bereaved as a result of a drug-death were recruited to the END project. If they consented to participating in such a study, they were then invited to fill in a questionnaire and to participate in interviews. A recruitment flyer that described the project was sent to all Norwegian municipalities’ public email addresses. We also contacted personnel who were engaged in the Norwegian Directorate of Health project to reduce drug overdoses, involving 28 municipalities. Recruitment was also facilitated through non-governmental organisations working with drug use, treatment centres, the Labour and Welfare Administration, and community crisis teams. We also disseminated information about the project via participation at conferences and through various media such as television, radio, and social media, as well as by recruitment through collaborators in other research networks or professionals in clinical settings. Existing participants also recruited new participants, namely via ‘snowball recruitment’, a form of involvement often used in research with hidden and vulnerable populations (see Sadler et al., 2010).
The participants signed a written informed consent form that described the purpose, method, and procedures of the study. Respondents were informed that the data would be published in a non-identifiable manner.
Participants
A sample of 10 siblings was extracted from the total sample of siblings (N = 79) participating in the larger END project (N = 255) (ResearchGate, 2022) and in-depth interviews were then conducted. They were selected according to the fact that they fulfilled an optimum breadth of background variables (i.e., across gender, age, place of residence, education, and age of the deceased). The age of the siblings ranged from 30 to 61 years old (M = 42.7; SD = 9.650), seven of whom were female, and three were male. Five siblings were married, and the rest were single (3), divorced (1), or had a partner (1). The siblings were well-educated, and 80% had achieved higher education (beyond 12 years). They lived in urban and rural areas and represented all regions of the country. They had lost their brother or sister between 1.5–18 years ago (M = 9.5; SD = 5.863). The age of the deceased ranged from 24 to 41 years (M = 34.00; SD = 4.989), and the siblings reported that the deceased had used narcotics for between 0.5 and 2.5 years (M = 1.38; SD = 0.625) before they died. Most siblings described a close relationship to the deceased brother or sister; cf. ‘we were very close… he was my best friend in the whole world’ (ID 22).
In-Depth Interviews
We developed an interview guide for the larger project, which consisted of three main topics that we wanted to explore in-depth: (1) time after death, stigma from surroundings and self-stigma, (2) formal and informal help and support, and (3) self-coping mechanisms and post-traumatic growth. For the second question (help and support), which we report on in this article, we addressed the topic of informal support by asking: ‘Can you describe your experiences with the support from family, friends, work colleagues, and peers?’. Furthermore, depending on the narratives, we explored the answers given in relation to how the support actually functioned, any negative or positive experiences of such support, the most important support they received and barriers to receiving it, and if the bereaved would have wanted a different type of support. The interview method required the researcher to follow up on the thoughts and reflections of the interviewees in order to gain more nuanced information about their experiences of support interactions within their networks. Thus, we also tried to get an impression of the care culture, and if the support had an individual or/and a family focus.
Three researchers interviewed all of the siblings in their homes or another place chosen by the interviewees. The length of the interviews with the siblings varied between one and a half to 3 hours and included required or desired breaks. The interviews were recorded and fully transcribed by a medical secretary. As the interviews were conducted in the participants' native language, the quotes used here were translated by the first author for the purpose of this article. In total, the transcripts consisted of 233 single-spaced pages.
Analyses
The theoretically informed framework for the analyses of the data is grounded in reflexive thematic analysis (Braun & Clarke, 2022b). Reflexive thematic analysis is a method used for identifying, analysing, and reporting patterns (themes) within data. Aware of the fact that analysis will always be shaped by the researchers’ theoretical assumptions, disciplinary knowledge, research training, prior research experiences, and personal and political standpoints, inductive analysis aims to stay as close as possible to what the interviewees intended in the data. The present analyses are rooted in a constructionist paradigm, and themes within the data were identified in an inductive way being firmly grounded in and linked to our sibling data.
Our analyses followed Braun and Clarke’s (2006; 2022a) six-phase process for reflexive thematic analysis: (1) familiarisation with the data; (2) coding; (3) generating initial themes; (4) reviewing themes; (5) defining and naming themes, and (6) writing up the results. The phases were sequential, each building on the previous phase, and the analysis was therefore a recursive process. The main author read and re-read all the written transcribed texts from the interviews to become familiar with their contents. The coded data were set in a matrix, examined, and collated to identify significantly broader patterns of meaning (potential themes). Next, initial themes – defined as patterns of shared meanings underpinned by a central concept or idea – were generated. After moving back and forth between these phases, themes were reviewed and decided upon iteratively and given informative names. A model consisting of the research question, themes, and codes was then produced (Figure 1). Bereaved siblings’ experiences with, and evaluation of, informal support.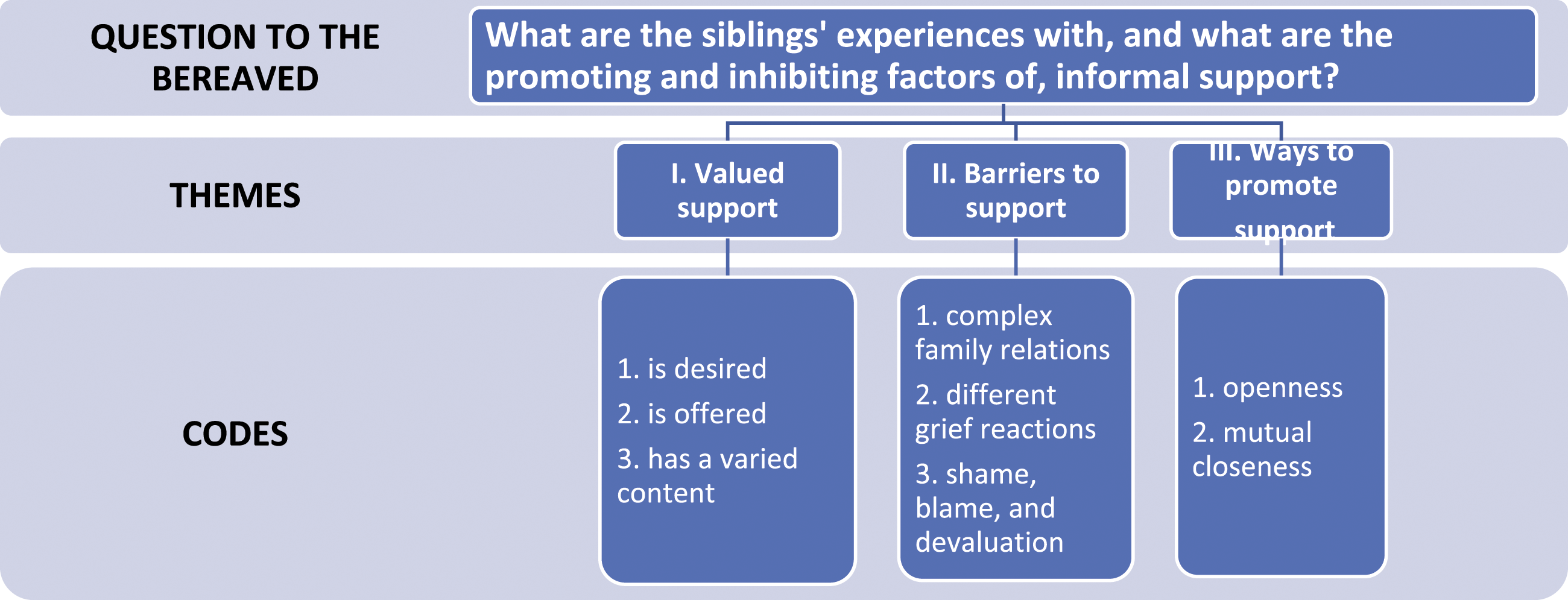
The main analyses were conducted by the first author (PhD in Sociology). Thereafter, the co-authors (PhD in Social Education, PhD in Social Work and Social Policy) studied the data, codes, and themes and decided on their own conclusions regarding the contents for them. Finally, adjustments were made to create a consensus and to agree upon the coding framework, the interpretation of the data and the decisions regarding the codes and themes.
Results
An unambiguous finding in this study was that none of the siblings had experienced peer support from others bereaved by DRD that were unrelated to their own loss. One sibling illuminated how peer support from other people who had lost a sibling to a DRD could have been helpful, i.e., to meet with ‘someone who understands what it is about… someone who has experienced something similar himself… who knows how to talk about this, and who manages to put the right words to it’ (ID 206). Due to the lack of peer support, the findings from the interviews only relate to social network support.
Three main themes emerged from the analyses of the siblings’ experiences with the support from social networks; I) valued support, II) barriers to support, III) ways to promote support (Figure 1). Within each main theme, the various codes (sub-themes) reflect the content of numerous meaning units from all of the interviewed siblings.
Valued Support
Three codes illuminate the perceived support or lack of support that the bereaved described:
The first theme captures that support which was
Several siblings were especially open to contact with the friends of their deceased sibling who used drugs. By listening to them and their stories about their friendships with the deceased it helped the siblings to revise, upgrade and form a less stigmatised view of their sister or brother. The friends’ stories and descriptions of unknown sides of the siblings, or their last days, were highly appreciated. They shared valuable information about the sibling and attended the funeral. This provided very meaningful support that confirmed that their sibling had meant something to someone even amid their sad life; cf. this sister’s description: When I saw all the people and of course many people using drugs… eh, like him, who came to that funeral, I thought that his drug life had been something more, than just what I had seen. And that was good (ID 86).
Some siblings from families with stable and good family relationships were spontaneously
More often however, siblings were disappointed because support was not offered. One sister stated: ‘I had an expectation that people would come and knock on my door… but that was not the case. It became very quiet from two of my best friends’ (ID 25). Other siblings who also had been disappointed by the lack of support, withdrew from these relationships permanently and defined such persons as less influential in their lives. Support from the friends of the bereaved who had previously been defined as less close before the loss and who initiated contact because they themselves had experienced a loss was highly valued. Even though they had not experienced a loss to DRD, having a shared experience of losing a sibling was perceived as significant. A sister described such support as especially moving and powerful: …one friend, with whom I had not had much contact before, she was an old friend for many, many years. But when John died, she stood at the door and it was very special… yes (crying voice). She herself lost her big brother many years ago in illness, so it was like she just knew what it is like to lose a sibling (ID 25).
Although the immediate support was highly valued, several siblings described that it often vanished too soon, and when they needed it the most, meaning by that point, it was then difficult to ask for more. One sister elaborated on this: People came with food and all sorts of things, and flowers and stuff… and afterwards… as time goes on, and when you come out of that first bubble… when everything is arranged, the funeral is over, and some of the biggest milestones that you just have to go through in the worst period really… then it is very empty… The support apparatus, it disappears in a time when it really might have been most present… For the one who is in the midst of it, it may become more and more straining, because then you start to get a little more to yourself and get to know a little about your emotions… and it is not so easy, at least not for me, to express… that it often lasted too short [a time] (ID 31).
The siblings valued
For some, small signs of support functioned better than deep talks about the loss. This was exemplified by a sister who valued emojis or short messages she received on social media: ‘A good care culture may also lie in a Smartphone… because this may be at the level one is available to receive and for others to communicate’ (ID 206). A sibling that had been living abroad at the time of loss experienced ‘a more superficial’ support through cards of care and texts of condolences as very positive, and not superficial at all. She said: ‘My God how important it was to get those small greetings where they wrote his name and stuff – it was so good, and very different from what we do in our country’ (ID 86).
Barriers to Support
Three main issues seem to inhibit and constitute barriers for social support for the siblings:
Thus, disagreement in the family about how to deal with the deceased siblings and their drug use before death further restrained any family support after the loss. A brother who had very different strategies than his mother when it came to dealing with the drug-using sibling expressed this as: ‘I had my strategies and my mother had her strategies, and … I thought it was just nonsense what she was talking about, and she did not understand my perspective… and that created conflicts’ (ID 1). Another sibling told how disagreement about her brother’s drug addiction broke her relationship to her parents and friends and deprived her of social support because she ‘had to move away to survive’ (ID 86). A sibling who had refused to talk with the sister when she was under the influence of drugs right before the death was then accused of the death. She was ostracised by the family and was not allowed to see her deceased sister nor attend the gathering after the funeral (ID 11).
Due to having had a challenging upbringing and/or a learned silent communication style, siblings described how they had to take care of themselves and how this style resulted in little care from their social networks. Several siblings mentioned that they were positioned, or had positioned themselves, as the ‘strong’ person in the family and within the family network, a position which made it more difficult for them to ask for support. A sibling stated how she tried to keep control and distance herself from her pain to be ‘the support beam of the family’ and thus, it became difficult to share her grief and therefore access support from friends and family members (ID 31). Still, as stated by this sister, some close friends were able to provide support: ‘people become insecure when you are silent and… they do not always know how to deal with me, but… the innermost core of my friends, they are good at reading me…’ (ID 206).
My sister… she will never show how she feels… it’s kind of embarrassing if there are any tears or something like that. I can judge, true, or be furious or… My father, he’s just like… there’s no emotion at all, you do not know if he’s happy or sad or anything. He has just been like that on a regular basis (ID 206).
Another sibling told that her mother was dead, her father needed to repress memories about the dead brother, and she herself was very angry. This complicated situation blocked for support within the family (ID 86).
Being exhausted from grief, some siblings tried to shut their emotions out and not show their grief, neither within the family nor to the outer networks. The grief and loss were there, they thought about it a lot, but could not bear to talk about it, and yet, still they needed support (ID 22). Thus, the very reason for their learning to not need any social support became a barrier to getting it later. New traumas and loss in the family also added to the loss of familial support as the strains became too great (ID 31). Siblings’ strong reactions to the death also prevented communication that could have triggered support from friends. A sibling told that although she had some friends, it could be difficult to use their efforts of support. After having told them about the difficult loss, she sensed that her friends’ reactions seemed to go as follows: ‘wow, this is heavy, and then they become silent’. However, she added: ‘still, I have a few close friends whom I know I can ask about everything, and I know they will help me’ (ID 31).
Finally, both family support and support from close friends could be inhibited due to the siblings shielding family members or friends (or the other way around) from their grief in order to not be a burden to the others. By perceiving their own needs to be less important than others in the family, such as their parents, some siblings decribe how they tried to support others by hiding or underplaying their own needs. Paradoxically, such acts of concern resulted in lacking communication and support within the closest family or friends.
Feelings of being unworthy of others’ care and support because ‘he was just a drug addict’, constituted a barrier to asking others for support. One sibling said: I would have needed someone to come to me and ask if I needed help or to talk… yes. That I should come to someone or seek out someone… in a way I felt it was not really okay, because it is so taboo… he was just a drug addict. For like everyone, yes, then I feel it is harder to make contact than if he had died in an accident. So I think that would have been helpful, at least that someone had contacted me… (ID 206).
One brother gave an example of how self-stigma and shame may prevent the initiation of social support, such as when his mother ‘was very preoccupied with the thought that the priest should avoid mentioning the cause of death at the funeral’ (ID 10). Still, the priest did mention that the cause of death was an overdose, to facilitate support from networks and make it easier for the bereaved to relate to what had happened.
Ways to Promote Support
The bereaved siblings pointed out that
One sibling expressed how important it had been that so many people in their network showed up for the funeral, where the priest had talked about her brother. The priests’ speech gave her another perspective on him and demonstrated that the brother had many positive qualities and meant something to other people. The speech had created openness about the loss and facilitated social support afterwards. Furthermore, through open and direct communication it would be possible to divide between those within their networks who were insecure about how to provide support compared to those who had stigmatising attitudes. One sibling commented on this, explaing that: ‘By daring to talk about it, then one will also win the trust of the other’ (ID 86). One sister who had managed to talk about the loss of her brother and had ‘taken control in dialogue with others’ demonstrated how support is interactional and relational. She explained the difficulties she had in talking about her brother, but how she perceveied it to be her responsibility to do so in order for friends to be able to come forward and provide that support.
So as not to reinforce the taboos surrounding the DRD, one sister summarised her reflections and experiences about losing her sibling: If I were to do these things again, there is
Mutual Closeness
As aforementioned, many siblings pointed out that they had experienced distrust and disappointments in their close relationships throughout their lives. One sibling in particular pointed out that mutual closeness and trust in a relationship are unconditional prerequisites for a helpful support network. She stated that for the bereaved to be available to receive and accept support that can be comforting, their trust, confidence and the time it takes for them to respond were all vital. Without these components, one is not able to share sensitive information and the strong emotional reactions they were experiencing following a DRD – meaning, whether they could ‘be open’. The sister elaborated on this But how much I tell, and what I tell to whom, it all depends on the situation, and how much time we have. So I have colleagues with whom I have told the whole story in much the same way as I have told you, and I have other colleagues who do not know anything. And I think that is, it’s a bit like that it must be probable… one has to look at both the situation and the person before one can necessarily tell everything… If I take it up with a person, then there is… also a declaration of trust in it… And then I must also give that person the opportunity to give a response to it (ID 54).
Consequently, it was also pointed out that someone who was grieving needed to have a level of tolerance for their network’s different ways of showing support, as some of it may be provided in a clumsy manner. As reflected on by the same sister, members of her network did not want to signalise that they held certain prejudices: I think people will make sure they do not disclose their prejudices by generalising about drug addicts and stuff. So… I think it’s important to people when I tell them about this (the death), I think people want to be able to say to me, ‘but it’s ok, or that it’s not, that it’s nice that I have shared it’, maybe. That is, because it is taboo, and it is not anyone who shares in the same way as if she died in an accident or something like that (ID 54).
Discussion
Three themes were identified in exploring the participants’ experiences of informal support following their sibling’s DRD. The theme valued support elaborates on the varied wishes for support as well as varied levels and content of the support received. Barriers to support describes the main issues that inhibit and constitute barriers for the sibling to receive social support. Ways to promote support highlights the importance of openness and mutual closeness. The last two themes build on the first theme; many of the siblings who were bereaved as a result of a DRD called for informal support from others outside the family and some siblings described valuable support from friends who had also suffered bereavments, both from their own friends as well as friends of the deceased. As documented in peer support studies post-loss (Kowitt et al., 2019), a few siblings felt that it might have been helpful to meet with peers and listen to their stories and experiences after a difficult DRD loss. Thus, the following discussion revolves around the informal support provided by social networks of family and friends.
Scarce Social Support
The siblings had been very close to their deceased brothers or sisters, were therefore afflicted by the death and expressed a need for support. However, many siblings had experienced minimal support from social networks of family and their own friends. In line with other groups of people suffering from a loss, they appreciated varied support they wanted and that was offered to them so that they did not have to seek it out themselves (Dyregrov & Dyregrov, 2008; Dyregrov et al., 2018). As with parents bereaved as a result of a DRD (Titlestad et al., 2020), the network support included signs of empathy immediately after the death, conversations or time-off with friends, and some had valuable support within the family. Reporting that they were positively surprised, the siblings pointed out the contact with and support from their brothers or sisters’ bereaved friends was especially valuable. The support from these bereaved friends was also described by parents after DRD as unexpected and highly valued (Titlestad et al., 2020b). This is in line with other studies of bereaved populations, such as those after suicide or deaths resulting from terrorism (Dyregrov et al., 2018), thus showing that friends may support the process of continuing those bonds of friendship and enable meaning-making that helps the siblings cope with the loss (Neimeyer et al., 2006). Distractions and ‘time-outs’ from grief, provided by doing fun things together with friends, were highly appreciated. Although this is not the main coping strategy, this kind of support may be very valuable and help the oscillation between loss-oriented (LO) and restoration-oriented (RO) tasks in the Dual Process Model of coping with bereavement (DPM), by helping to avoid the harsh reality for some time (Stroebe & Schut, 2010). In the LO coping, the siblings would try to confront the loss and grief and accept what happened, and to remember and seek closeness to the deceased, whereas the RO tasks are about handling the practical challenges of the loss and arranging for a further life without their deceased sibling. Stroebe and Schut (2010) claim that oscillating appropriately between the two forms of coping in DPM is considered crucial for a good grieving process.
Siblings had some support from their close families that they appreciated, but the impression was that this form of support was more sparse, as seen in a study of bereaved parents following their child’s DRD (c.f. Titlestad et al., 2020b). Some of this may be explained by the sibling role (c.f. Dyregrov & Dyregrov, 2005), and the stigma connected to DRDs (c.f. Dyregrov & Selseng, 2022).
Fragile Basis for Interactional Social Support
Considering social support as an interactional phenomenon, the barriers pointed out in this study constitute a fragile basis for the support processes (Dyregrov et al., 2018; Lakey & Orehek, 2011; Nurullah, 2012). They seem to block open communication and disclosure of genuine feelings of grief that could result in a reciprocal understanding and respect for each other’s grief orientations and needs (Lakey & Orehek, 2011). Thus, if siblings choose to avoid sharing their grief experiences and remain silent about this experience, the networks are then left to their own subjective judgment to interpret that silence, which means that it is also open to misinterpretations, misunderstandings, or their own silence. The same happens when network members under-communicate their questions and dilemmas. Consequently, the fragile basis for this support is discussed from a relational and interactional perspective to explain the minimal social support provided to those who have lost their sibling to a DRD.
‘Strong’ Siblings in Complex Relationships
The siblings themselves pointed out possible conditions that may explain the scarce social support. Several of those who participated in the interviews were very close to their deceased siblings and took on, or were appointed to, a ‘strong’ sibling role both within the family system and to their friends. For several reasons, they seemed to distance themselves from full acknowledging the loss inwardly, and forced themselves to let go of strong emotions.
As discussed in the literature, unhealthy and difficult family relationships may block healthy and open communication among family members, as well as influence the interactions with other social relations (Adams, 2019; Dyregrov & Dyregrov, 2008; Goldsmith, 2004). The findings demonstrated how harmful upbringings (sexual abuse, violence, neglect) or conflicts connected to the deceased prior to their death seemed to have resulted in a lack of trust in others, teaching them to be strong and rely on themselves. The siblings revealed that arguing against accusations and reproaches for the death was not possible in a family system that had a weak communication climate. They seemed to avoid emotional connections with others and appeared independent in dealing with their grief.
Attachment style may be a beneficial framework to use in helping to understand the relationship between social support and health. Overall, there is convincing evidence that social support and the importance placed on intimate relationships vary depending on one’s type of attachment style (Rapoza et al., 2016). Attachment theories state that people with an avoidant-dismissive insecure attachment style tend to find it difficult to tolerate emotional intimacy and connection with others as they do not rely on others (Rapoza et al., 2016). When families in our study had practiced closed communication, due to a lack of trust in the family, it was clear that the siblings had learned this communication style, which also became their tool to use after the loss. The siblings described themselves as independent, content to care for themselves and preferred fleeting, casual relationships with networks that kept their distance emotionally. The mechanism by which insecure attachment relates to poorer social support may be complex and multifaceted. Still, Anders and Tucker (2000) pointed out that insecure attachment was related to deficits in interpersonal communication competence that mediated the relationship between attachment and poorer support networks (Anders & Tucker, 2000).
Furthermore, as most friends were given few signals regarding the intensity of the siblings’ grief, they were not in the position to provide optimal support. In line with other research, the solution was to communicate on unproblematic matters in a more superficial manner. Such communication of support was short, simple, and with distance to the bereaved through tools for communication known to most people (social media). An example of this was when siblings appreciated and related better to emojis and SMS than to any deep conversations, as the latter requires positive experience and competence in open communication.
Protective Silence and Disenfranchised Grief
Paradoxically, siblings with a more secure attachment also ended up with little familial support. Not wanting their parents to suffer any more, some siblings tried to be the ‘strong’ one in the family unit, and protect the parents from their own pain. Thus, it seemed that they defined themselves as lower down in the grief hierarchy. Studies regarding bereavement following suicide, terror-killings and accidents have shown that if a family member is overly preoccupied with their own grief situation, loses interest in the family or becomes increasingly angry and irritable, other family members can either pull away from this person, or alternatively become overly protective of them (Dyregrov & Dyregrov, 2008). In her study of communication between parents and siblings after the suicide of a sibling, Adams (2019) described this as ‘the paradox of protective silence’. As also explained by Stroebe and Schut (2015), a paradoxical effect may emerge involving attempts by parents and siblings to protect each other from further pain by camouflaging their grief and refraining from sharing it only to increase their own level of distress. Due to the same processes, we saw siblings going through a DRD bereavement describing disenfranchised grief (Doka, 2016), meaning that their grief was unacknowledged or invalidated. In other words, the silence that is intended to shield grieving people from further distress may result in more distressing feelings of rejection, anger and alienation, leaving the bereaved person to process their grief alone, in silence.
Associated and Internalised Stigma
An important barrier that seemed to reduce social support from the general community was an internalised associative stigma (c.f. Sheehan & Corrigan, 2020). This phenomenon describes how the siblings were affected by stigma through their familial connections to the stigmatised individual, specifically in this case, that of the drug-using deceased (Nieweglowski et al., 2018). As also seen from the results, some siblings experienced parents’ negative self-evaluations or self-blame for the cause of death (their internalised stigma), which prevented the possibility of social support for siblings. As documented by Dyregrov and Selseng (2022), the person bereaved as a result of a DRD experienced disgraceful and harsh direct and indirect stigmatising communication from social networks (i.e., both close and distant family members and friends), consisting of dehumanising labeling, unspoken and implicit stigma, and blaming.
Advice to Improve Social Support in a Relational Perspective
Analysis of the interview data identified two categories of advice that could help promote and improve social support, openness and mutual closeness, both of which are relational concepts. We also suggest that mutual closeness is the prerequisite for, and can lead the way to, openness. As pointed out in the grief literature (Adams, 2019; Dyregrov & Dyregrov, 2008; Stroebe & Schut, 2015), it is crucial that bereaved persons can trust the network and are certain that any private and personal information will remain so, in order for any emotional support to be beneficial. After a stigmatised death, it may be even more important that everything expressed in confidence is not leaked to outside parties. Thus, helpful support will presuppose trust and solidarity between the bereaved and their networks. Goldsmith (2004) showed in her research that solidarity and a direct form of communication were experienced by people in difficult situations as being the most helpful (Goldsmith, 2004).
The siblings who participated in this study advocated ‘openness’ as the most important component in facilitating social support. This is in line with parents who have lost their child as a result of a DRD (Titlestad et al., 2020b) and with other groups of bereaved after unnatural deaths, such as terrorism (Dyregrov et al., 2018), suicide, SIDS, and accidents (Dyregrov, 2003b). In the Support and Care project, 81% of the people bereaved following a suicide, SIDS and accidents suggested that ‘openness’ represented what they felt was the most important strategy for coping with the difficult situation after the death. For them, openness implied sincerity, honesty, and direct speech, meaning that to a large extent, it was a matter of their giving clear signals to their surroundings. Such signals were important to inform others of what had happened, how they were feeling, the type of support needs they had, and how others could best support them (Dyregrov, 2003b).
In a parallel interview study of 111 friends and family members who had supported the same parents, the network members expressed that they sometimes had been so overwhelmed by the strong grief and the special situation the bereaved were dealing with, that they withdrew because of a feeling of helplessness in relation to what to say or do (Dyregrov, 2006; Dyregrov & Dyregrov, 2008). Finally, both the bereaved and the networks claimed that openness was their best empowering strategy when faced with ineptitude as well. Thus, both parties engaging in social support (the bereaved and their social networks) asked for open and frank communication in order to optimise social support after an unnatural death. However, as the siblings in this study stressed, mutual closeness and trust are prerequisites for openness. Health and social workers should include this perspective in their interactions with those bereaved following a DRD.
Strengths and Limitations
To facilitate readers’ ability to judge the validity (i.e., the trustworthiness and transparency) of the findings, the data gathering process has been described, and the analytical process was made explicit both in the description of the methods used and in the findings. The article presents numerous quotations from the interviews with the siblings to allow the reader to assess the credibility of the themes. We consider the analytical trustworthiness to be good as the main author analysed the data, and thereafter all three authors discussed the codes and themes to yield the most ‘credible’ conceptual interpretation of data (credibility). Furthermore, the analyses are based on the authors’ thorough knowledge as interviewers in the larger END project and from their extensive previous work with people who have drug use challenges and who have experienced unnatural losses. Moreover, transparency is brought forth by referring to IDs for typical citations of the bereaved that exemplify the themes.
The degree to which the findings can apply and be transferred beyond the present sample (transferability) is uncertain but may be adaptable to siblings bereaved following a drug-death with similar demographics. Finally, we consider the data analysis and theory generation to be reliable as it has been completed by three senior researchers representing the fields of both bereavement and substance use problems (c.f. Lincoln & Guba, 1985).
Conclusion
The solution to the lack of tools the participants had to master the situation after losing their sibling to a DRD, was for them to stay strong, avoid and repress their outward displays of grief and the stigma and blame from others. Thus, they accessed little support for themselves beyond a small trusted group. The ‘strong sibling role’ counteracted others seeing their grief and hardships, and that they needed support. The findings expand on the understanding of the challenges and interactional factors involved in social support and the importance of addressing this in social work and clinical programmes aimed at supporting the bereaved experiencing loss after a DRD. Although challenging due to possible trauma histories, the findings point to the necessity of mutual trust and open communication as a way of fostering better social support for bereaved siblings. Finally, the complete absence of support from other bereaved (peer support) should be addressed in order to utilise this important support potential for helping grieving populations after DRDs.
Footnotes
Acknowledgments
A special thanks to the bereaved siblings for taking the time and effort to respond to the END project survey and for participating in the interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Council of Norway [grant number 300732].