
Abstract
We studied levels of awareness of impending death in older patients and their family caregivers. Using a mixed methods approach, we interviewed 70 family caregivers in Israel. Of the caregivers, 64% reported having been aware of the impending death, 33% were unaware, and 3% uncertain. Caregivers reported their perception that 36% of patients were aware, 27% unaware, and for 37% they were uncertain about the patient’s awareness. Mechanisms that increased caregivers’ awareness were specific diagnosis, significant deterioration in health, preparation by a health professional, or patient preparations for death. This study clarifies processes which aid awareness, and the relationship between awareness and actual preparation for dying.
Keywords
Introduction
Rates of awareness of impending death vary across studies and may depend on the primary illness and the cognitive level of the dying person. A study of 220 patients (age 60–101) with diverse terminal illnesses, concluded that at least a quarter, but probably more, were aware that they were dying, based on their remarks (Exton-Smith, 1961). Hospital doctors reported that 88% of cancer patients, and 54% of patients with other terminal illnesses were aware of impending death (Seale, 1991). A subsequent study found that of 447 people dying from cancer, 83.9% died with awareness of their impending death, compared with only 51.6% of 93 cardiovascular disease patients, and 71.4% of 28 respiratory disease patients (Seale et al., 1997). Cognitive impairment affected patient awareness in both basic comprehension by the patient and the scope of information caregivers felt they could reveal to a cognitively impaired patient (Andruccioli et al., 2007; Seale, 1991; Seale et al., 1997). Depression was found to be greater among cancer patients who did not acknowledge their prognosis, compared to those acknowledging their impending death, fully or partially (Chochinov et al., 2000). Another study involving patients with incurable advanced cancer found that accurate prognosis awareness was significantly associated with lower level of quality of life for physical symptoms, as compared to patients who were partially aware or unaware (Vlckova et al., 2022).
The importance of awareness of impending death among terminal patients remains a subject of debate. Glaser and Strauss (1965) conceptualized four different awareness contexts of dying in their foundational study. Open awareness of dying, where both the dying patient and the respondent knew that the person was dying, emerged as the most prevalent awareness context. Several papers described the advantages of such awareness including affording patients a sense of control, enabling them to participate in making funeral arrangements, and giving them a chance to take financial actions for their family (Goldsteen et al., 2006), or to consider and plan the dying process, such as the choices of euthanasia and place of death, (e.g., to die at home, or not to die alone) (Seale et al., 1997), helping surrogates make sound medical decisions during the dying process (Rich et al., 2009), such as less aggressive medical care and earlier hospice referral (Wright et al., 2008), and providing patients with an opportunity to feel at peace with dying, to achieve a sense of closure, to reflect favorably on life, and to come to peace with God (Lokker et al., 2012; Steinhauser et al., 2001). In their review of end of life expectations and experiences of patients and their relatives, Fosse et al. (2014) reported that when guidance from health personnel was missing, families experienced uncertainty and distress. This fits with the observation of Rich et al. (2009) that staff were significantly more likely to expect death than family. Health staff’s willingness to disclose impending death to patients also affected the level of awareness (Timmermans, 1994).
In contrast, others opined that informing people of impending death deprives them of hope or damages their sense of wellbeing (Steinhauser et al., 2001), creating uncertainty and ambiguity which may influence expectations among patients and staff concerning appropriate dying (Copp, 1998). For example, a study of terminally ill hospice patients in Italy reported that many families feel that revealing the type and degree of illness progression to a patient, especially to a very old patient, reflects a lack of compassion (Andruccioli et al., 2007).
As distinguished from diagnosis, other background factors were not found to be associated with awareness of death, including age, gender (Lokker et al., 2012; Seale et al., 1997), income, education level, ethnicity, religious affiliation, and religiosity (Steinhauser et al., 2001). Tzuh et al. (2021) found that family caregivers of terminally ill patients were more likely to have accurate cognitive prognostic awareness if they had more contact/communication with the patient and greater subjective caregiving burden. Wen et al. (2022) concluded that caregivers’ cognitive prognostic awareness and emotional preparedness for a patient’s death were associated with caregiving outcomes and with their relative’s end-of-life care.
This study was conducted in Israel, where the Dying Patient Act, enacted in 2005, was designed to strike a balance between a patient’s autonomy in end-of-life decision-making and cultural and religious norms. In 2009, the Ministry of Health issued a policy directive establishing standards for the provision of palliative care. Yet, friction between traditional approaches to end of life and approaches emphasizing greater patient autonomy continues to be manifested among Israeli health care professionals and institutions in the context of limited care options, insufficient funding and lack of professional knowledge and training (Cohen-Mansfield & Brill, 2021).
Utilizing a dataset which we developed to study end of life, we aim to elucidate the nature and implications of awareness of impending death by addressing three research questions: 1. Are persons at end of life and their family caregivers aware of impending death? 2. Which factors influence awareness and unawareness? 3. How do family caregivers understand their, or the patient’s awareness or lack thereof?
Methods
This research is part of a larger study employing a mixed methods design (Cohen-Mansfield et al., 2018), in which we characterized and described the end of life experience for family caregivers and patients, as perceived by their family caregivers.
Participants
We interviewed 70 family members who served as end-of-life caregivers (17 spouses, 52 children, and 1 cousin) in Israel’s urban center. The interviews were conducted during a time period ranging from a few weeks to a few years after the death of the relative for whom they cared (median = 11 months). Inclusion criteria were: having been the primary informal caregiver during an adult relative’s end of life period and that the informal caregiver was willing and able to respond to our interview questions. Exclusion criteria were lifelong severe psychiatric illness of either the caregiver or the decedent.
Procedure
The study was approved by the Institutional Review Board of Tel Aviv University and the Helsinki committee of Rabin Medical Center. The recruitment process, during which 249 persons were contacted, is described in detail in Cohen-Mansfield et al. (2017). Of the 70 family caregivers recruited, 60 were relatives of patients who died in two geriatric medical centers. The other 10 participants were recruited through other studies. Participants gave informed consent after receiving a description of the study. Interviews, lasting approximately 2–3 hours, were conducted by trained interviewers at locations convenient to participants (e.g., home, coffee shop, university).
Data Collection and Assessment
The interviews included a survey with a combination of open- and closed-ended questions that allowed participants to elaborate on their experiences and their perception of their relative’s experiences during the end of life period. In addition to requesting basic demographic data, we asked family caregivers to rate their relative’s pre-death level of functioning in terms of activities of daily living, including eating, personal grooming, dressing/undressing, walking, getting into/out of bed, and showering (Katz et al., 1970). Possible answers were: (1) requiring no help at all, (2) requiring some help, or (3) requiring full help.
Family caregivers were asked the following questions and then to elaborate on their answers, (1) “Prior to your relative’s death, did you know that your relative is going to die?” (2) “Did your relative know that he/she is going to die?” When family caregivers answered that either they or their relative knew of the impending death, the family caregiver was asked for what period of time prior to death did they or the relative know. In order to study the relationship between the purported advantages of awareness and actual activities undertaken during the dying process, we asked, (1) “Did your relative bid farewell to those dear to him/her prior to dying?” (2) “Did your relative make funeral arrangements prior to dying?” (3) “Did your relative have advance directives concerning treatments he/she might want to forego, or concerning the identity of the person who would make decisions on his/her behalf?” All questions were developed for this study and were administered in Hebrew.
Analytic Approach
Using a mixed methods approach, the analysis consisted of a quantitative component with a descriptive approach to generate percentages, means and standard deviations. We compared subgroups using t-tests and chi-square analyses. In the qualitative analysis, we analyzed the respondents’ comments, which had been transcribed verbatim during the interviews using a thematic approach (Braun & Clarke, 2006). This qualitative component enabled us to gain a deeper understanding of participants’ explanations of awareness of impending death or lack thereof. In the initial coding stage, two research staff members who worked independently separated data into meaningful fragments and ideas for themes. The themes were established inductively, using an iterative process that involved identifying overarching themes until no new themes emerged. The research staff, still working independently, then re-analyzed all transcripts in light of these themes and coded the themes that pertained to each participant. When comparing the findings, the research staff members discussed the meaning of the themes, refined them, and went through an iterative process that included repeated reading, coding, reviewing, and discussion involving other members of the research staff.
Methodological Rigor
The explanatory sequential design of this mixed methods study bolstered the overall analysis and interpretation. In the qualitative component, data saturation was reached when themes emerged repeatedly from the data. Analytical rigor was achieved when consensus was reached after independent analyses were conducted by several members of the research staff. After further discussion, a consensus on categorization was achieved. To assure credibility, quotes derived from participants’ interviews were used to illustrate the themes. Several staff members checked the accuracy of the Hebrew to English translation of the quotes. Quotes are followed by the participant number in the study, sex and age of the family member and of the decedent. Both the validity of the study results and our understanding were enhanced through the use of mixed methods, as each of the methods compensated for the inherent limitations of the other.
Results
Quantitative Findings
Demographic background variables (n = 70) Percentages or Mean (SD).
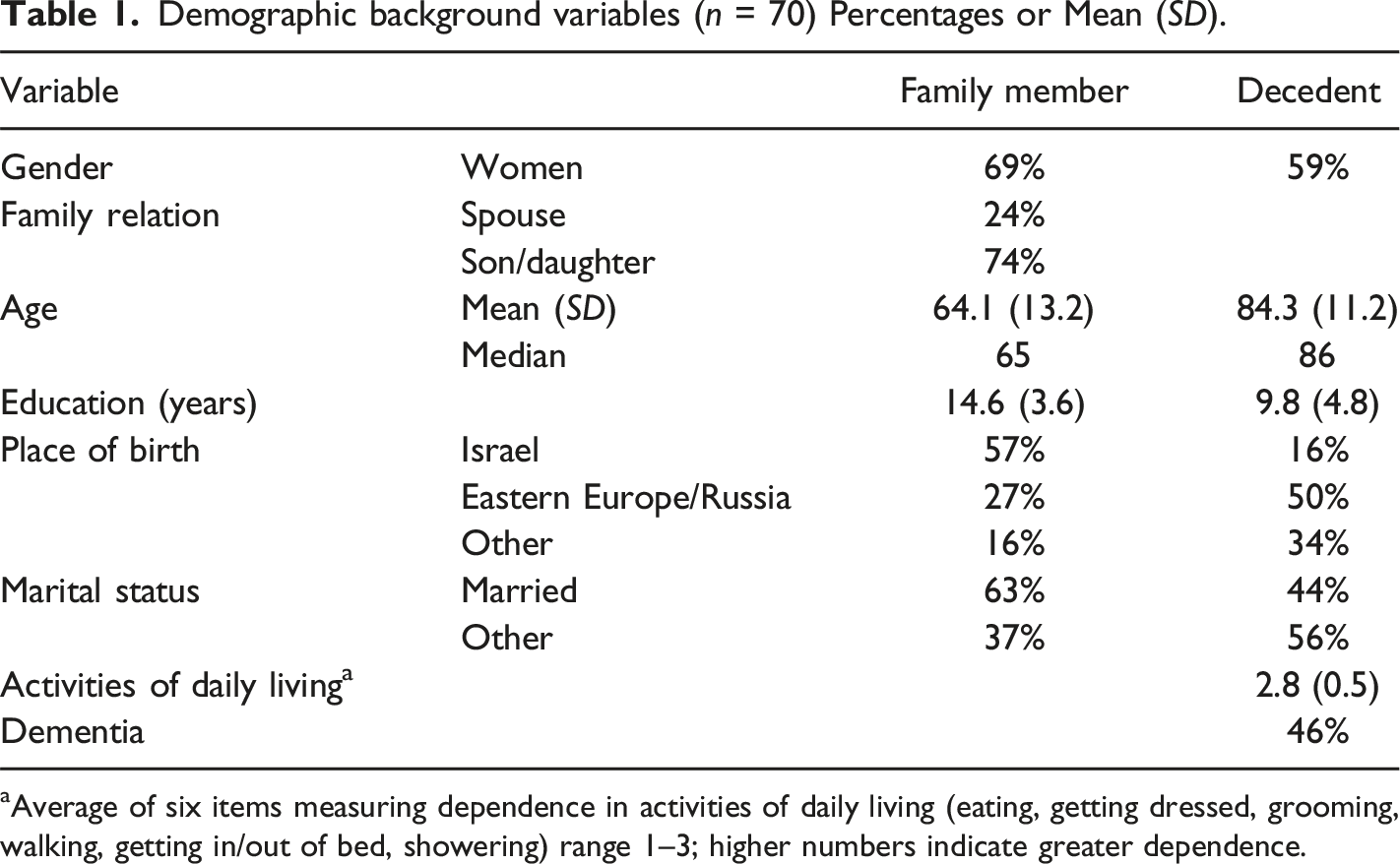
Average of six items measuring dependence in activities of daily living (eating, getting dressed, grooming, walking, getting in/out of bed, showering) range 1–3; higher numbers indicate greater dependence.
Cross tabulation of awareness of impending death: decedent by family member.
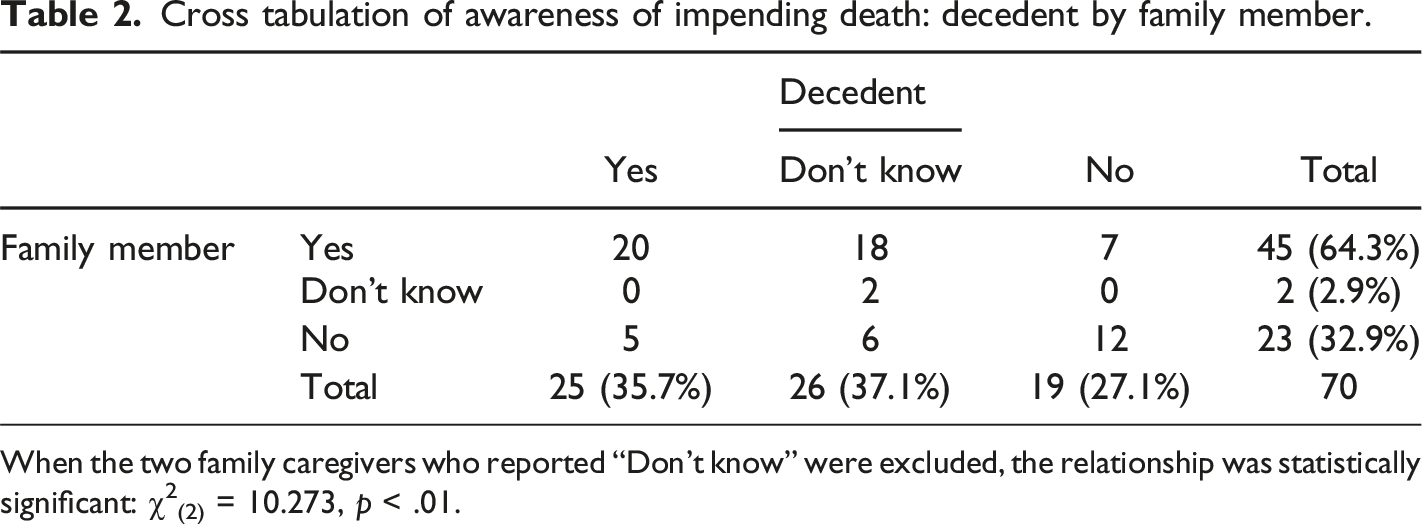
When the two family caregivers who reported “Don’t know” were excluded, the relationship was statistically significant: χ2(2) = 10.273, p < .01.
When asked about the length of time prior to death that the family caregiver or the decedent had been thought to be aware of the impending death, family caregivers reported a very wide range – from one day to years. When family caregivers reported being aware that the patient was going to die, the median time of such knowledge was 45 days prior to death. When a decedent was reported to have been aware of impending death, the median time of such knowledge was reported to be 60 days prior to death. The same median (knowledge of impending death 60 days prior to death) was reported for both family caregivers and their relatives when both were reported to have been aware of the impending death. Only two family caregivers reported having become aware only on the last day of life (and none on the day before last). Only one of the decedents was reported to have become aware of the impending death on the last day of life, and none on the day before. When both the patient and the family caregiver were reported to be aware of the impending death, the reported length of time of awareness prior to death was highly correlated (r = .82, n = 19, p < .001).
When comparing patients who were reported to be aware with those who were not, and when comparing family caregivers who reported being aware versus those reporting not being aware, we found no significant differences in background characteristics of the family caregivers and the patients. When a family caregiver did not know if the decedent had been aware of impending death, the decedent had been somewhat more disabled as measured by activities of daily living (ADL) function (mean = 3.0 vs. 2.7 [for decedents who were reported either to have known or not to have known], p = .04), and such decedents had higher rates of reported dementia – 65% vs. 41% respectively, (p = .056).
Of decedents reported to have had dementia, 28% were reported to have been aware of their impending death as compared to 42% of those not reported to have had dementia, but this difference was not statistically significant (p = .22, two-sided).
In examining the relationship between the decedents reported awareness and involvement in death preparation activities, we found that nine out of 25 (36%) of those reported to have been aware were involved in farewell conversations with relatives, as compared to 9% of those reported to have been unaware (4/45), χ2(1) = 7.81, p < .01. Of decedents reported to have been aware, 48% (12/25) provided pre-death instructions, usually referring to wills or advance directives, as compared to 24% (11/45) of those reported to have been unaware, χ2(1) = 4.04, p < .05. There was no significant difference regarding preparation of funeral arrangements.
Qualitative Findings
Explanations for awareness, lack thereof, or ambiguous and mixed effects.
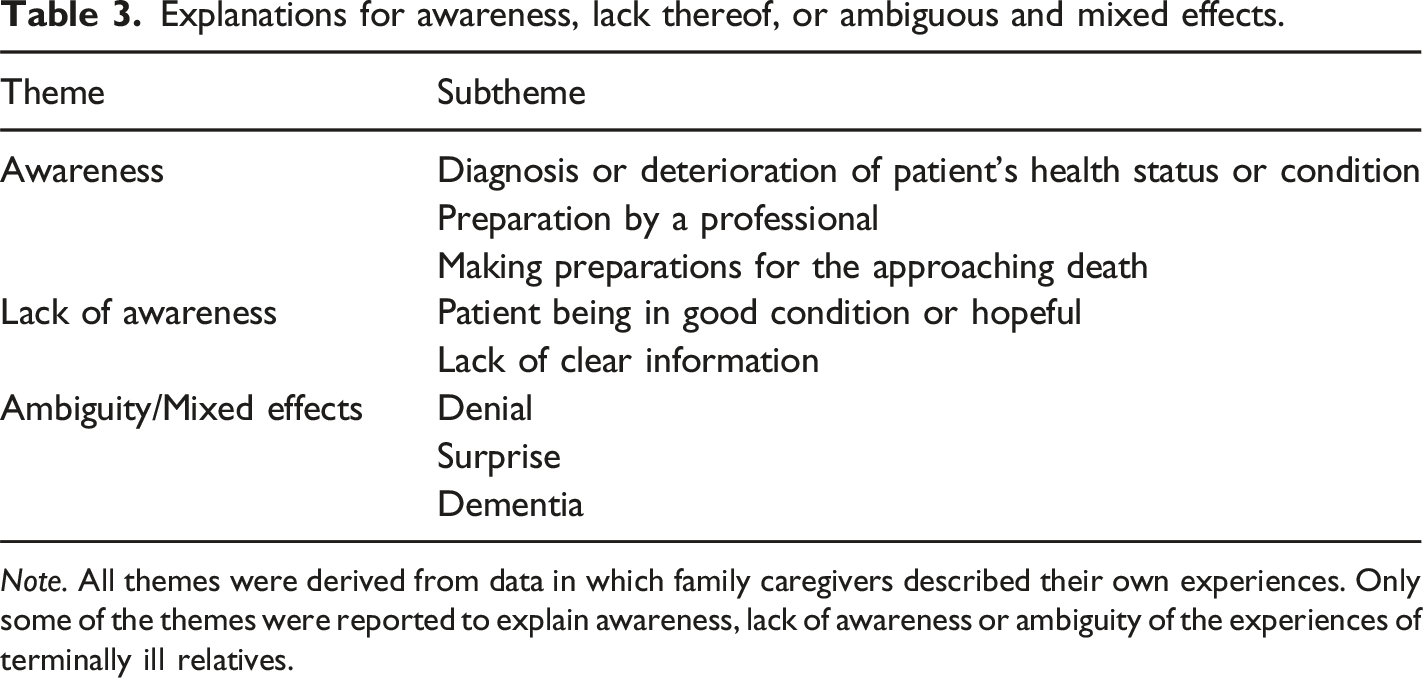
Note. All themes were derived from data in which family caregivers described their own experiences. Only some of the themes were reported to explain awareness, lack of awareness or ambiguity of the experiences of terminally ill relatives.
Awareness
Diagnosis or Deterioration of Patients’ Health Status or Condition
Family Caregivers’ Awareness
For some family caregivers, the diagnosis gave a clear indication of the patient’s approaching death: “Prior to the diagnosis of cancer, I did not know anything. […] After the diagnosis of the cancer, I realized that she had around a year left, that she, in her general condition, could not survive any longer (#63, other family member: 68-years-old Male [68yo-M]; decedent: 74yo-F).
Others noted a deterioration in the patient’s health as an indicator: My mother said 2 months before he [my father] passed away that he was deteriorating, I had thought he could live longer and longer. And my mother prepared herself mentally, and began to talk about what they would do and if people would come. During his last week, my mom felt there was another day or two. Everyone came to say goodbye to him, also my brother who had had cardiac arrest and is [therefore] very sensitive. And my father shed tears. It was a difficult farewell. (#60, daughter: 60yo-F; decedent: 92yo-M)
In some cases, family caregivers observed signs of dying or deteriorating health despite a contrary diagnosis by staff: “I knew she was going to die; I saw that foam was already coming out of her mouth, I saw her fluttering, and I asked the nurse who told me it was okay, that she was only coughing” (#27, daughter: 60yo-F; decedent: 86yo-F).
Patients’ Awareness
When the patient seemed to be aware of the approaching death, family caregivers often realized it: I knew it was the end when she was still at home and did not want to eat and get out of bed. She was so determined. I tried to convince her, but it was clear that this was the beginning of the end. (#28, daughter: 73yo-F; decedent: 93yo-F)
In other cases, in retrospect, it seemed clear that patients were aware due to their deterioration and suffering from their condition: “In the last week I think she already knew, she also asked to die. She said she could not continue like this; she lay in bed like a mummy, did not care about anything” (#31, daughter: 60yo-F; decedent: 88yo-F) or “From the moment she realized she was in [the geriatric institution] she knew she was going” (#9, daughter: 58yo-F; decedent: 84yo-F).
Preparation by a Professional. Family caregivers’ awareness
Clear communication by doctors or nurses about the impending death contributed to family caregivers’ awareness: “We knew she was going to die. … The nursing home manager told us it was a matter of hours” (#8, daughter: 56yo-F; decedent: 76yo-F) or: The hospital explained to us that the seizures were the turning point at which Dad was moved to the long-term geriatric hospital, and there was a nurse there with whom we became very close, and she said it will not take more than two months. She told me the steps – he may have seizures and it will be near the end. So when the seizures came, I would say goodbye to him every day. … I was already mentally ready every time I would finish a shift with him; In the last two weeks, I would say goodbye to him. I highly recommend going through this conversation of what the next steps are. In the hospital they talked to us a lot and in the long-term geriatric hospital we also understood what the direction was. Mother, with the power of faith, said you will see that father will stand up, but this is mother. I really appreciated that they spoke to me honestly. (#18, daughter: 55yo-F; decedent: 80yo-M)
Making Preparations for the Approaching Death
Family Caregivers’ Awareness
Awareness was expressed by making plans for the period of dying or after death: “I realized that this was his last road, so I did everything to provide him with a good quality of life and longevity, including morphine that the doctors prescribed for him, and I made sure that he would get it (#32, wife: 81yo-F; decedent: 86yo-M).
Patients’ Awareness
Similarly, preparation for death was an indicator of patients’ awareness of their approaching death: I did not feel or think it would continue like this. Had it continued, I would not want him to suffer and deteriorate further. Every day when I would leave, during the last month, he would constantly ask me if I had bought the plot for the burial. He would remind me every day and tell me not to forget. My sister was by his side at the time he passed away and she did not feel he was dead. I felt bad that day. That day he also did not feel so well and my sister was there and fed him. Suddenly the nurse called and told me he was dead. I was shocked, like crazy. First, I called for the grave. He gave me a list, he wanted everything according to the list. I had to sort out all the things…based on the lists and things that he asked for and the plans that he made. It means, he was ready to die. Otherwise…he would not make all these plans. (#5, wife: 83yo-F; decedent: 88yo-M) or:
We got to the hospital, and he said to me, “Let’s travel to Switzerland, so they will inject me.” So I told him, “Let’s see what happens to you first.” He told me he wanted me to kill him, and I told him I was born to give life and not to take it. (#32, wife: 81yo-F; decedent: 87yo-M)
Lack of Awareness
Family Caregivers’ Lack of Awareness: Patient Being in Good Condition or Hopeful or Stable
Some family caregivers stated that staff told them that their relative would recover, giving them hope: “At the hospital they said he would go to a geriatric institution and there he would probably recover. I kept hoping he would get up and recover and I would talk to him” (#12, daughter: 65yo-F; decedent: 92yo-M) or: When the parent is not well – requiring skilled care, one understands, but is always repressing [this understanding] and finding [psychological] mechanisms [to cope] – that it will not happen tomorrow, etc. [interviewer: meaning not thinking about it in a realistic way]. So when it came, we were surprised. (#62, son: 64yo-M; decedent: 96yo-F)
Patients’ lack of awareness: The Pretension of Optimistic Prognosis
According to family caregivers’ reports, lack of awareness by patients occurred when the patient was considered to be medically stable or hopeful of recovery: “On the contrary [she did not anticipate death], I would always say ‘wait patiently,’ in a few more days you will leave this place” (#40, husband: 92yo-M; decedent: 86yo-F). In this case, the family caregiver encouraged the optimistic outlook which resulted in the patient’s lack of awareness.
Patients’ Lack of Awareness: Not Being Told of the Prognosis
Encouraging the patient’s optimistic outlook, the patient’s son reported that he did not have the heart to tell his mother that she had terminal cancer. Being a doctor himself, he tried to raise her hope by explaining that her condition might be due to other causes: I hospitalized her and they found metastases and I realized it was already the end. I knew it would be a difficult end, but I did not think it would be this bad. It is hard to see a terminal patient, but when it is your mom, and you understand that it’s the end and you cannot tell it to mom until the end ... I tried to lie to her, to tell her it’s a result of surgery or osteoporosis, I told her it was because she sat a lot. It did not rob her of hope. She understood what she had but she hoped it might not be cancer. I told her it might be pain from her inactivity, ... I tried to lie to her. But in the end her level of thought declined, and it was easier to lie to her. (#48, son: 51yo-M; decedent: 85yo-F)
Family Caregivers’ Lack of Awareness: Lack of Clear Information
Other family caregivers said they were unaware because doctors did not inform them about their relative’s situation. Thus, the possibility of imminent death did not occur to them: “I did not think about it. The doctor may have known by the tests, but I did not” (#4, wife: 88yo-F; decedent: 84yo-M).
Ambiguity and Mixed Reports
Denial and Family Caregivers’ Ambiguity
Some family caregivers were clearly informed by staff, but still hoped that the patient would recover: “I knew because the doctor told me, but I did not think it would happen. I was still hoping he could be taken home” (#33, wife: 80yo-F; decedent: 83yo-M) or:
The doctor asked me if I was ready for it, I did not think about it, maybe I did not want to, yes, I did not want to. They prepared me but I did not want to think about it. I did not internalize that he was going to die. (#24, daughter: 65yo-F; decedent: 91yo-M)
Ambiguity was also manifested when death took longer than anticipated: I did not know when this would happen; I was amazed that she held on for so long. She looked awful; It was already any minute, but actually, it took 8 months. She did not want to go because she wanted to resolve some things that she had left unresolved – this is my guess. (#16, daughter: 65yo-F; decedent: 90-F)
Patients’ Ambiguity
Family caregivers also suggested that the patient may have been aware, but acted as if unaware: “Maybe in the heart [he knew], but he never said anything like that; He just talked about wanting to go home and that everything would be fine” (#19, wife: 79yo-F; decedent: 83yo-M).
Surprise and Family Caregivers’ Ambiguity
In many instances, family caregivers were aware of their relative’s approaching death, but did not know when it would happen and were often caught by surprise when it occurred: We knew but did not know when – like a candle about to go out. It’s not as sudden as a car accident. But we did not think when we took her to [the geriatric institution] that it was close to the end. (#26, husband: 62yo-M; decedent: 52yo-F) or: Every day it was a miracle that she was still alive for 3 months, but even when she was home, we did not think she could go on like this much longer and yet, it still happened in a second [that she died]. (#29, daughter: 66yo-F; decedent: 92yo-F)
Despite knowing that their relative was approaching the end of life, some family caregivers were unable to bid farewell because death came sooner than expected: I knew I was taking him home on Sunday morning, I knew he would die of cancer - but that on that night it would happen? The last words I said to him [were] – “On Sunday we go home. Not even a farewell. (#45, wife: 74yo-F; decedent: 85yo-M)
Inconsistent Reports
When we considered awareness of impending death of those reported to have dementia, both awareness and lack thereof were reported for the patient and for the family caregiver without a consistent pattern. Family caregivers explained assumed lack of awareness by the patient: “When she deteriorated, she already had dementia. Every time she was in the hospital, she wanted to run away” (#29, daughter: 72yo-F; decedent: 93yo-F). Others reported that the patient was aware, often simply stating that they thought the person was aware, and at other times offering an explanation such as, “For the past 2 years she has suffered in a way that she knew one could not endure for long” (#59, son: 63yo-M; decedent: 95yo-F).
As to family caregivers of persons with dementia, some reported being aware, providing various explanations enumerated above, such as being told by medical staff or realizing the health decline. Similar to the patients without dementia, some family caregivers emphasized their own lack of awareness: We did not understand. I expected that she, in her current condition, she would not last – it is impossible, both the age and the diseases. But I did not anticipate… that this would happen [death]. Even if it is in front of our eyes, we do not see. Even when she went in for the surgery from which she did not emerge, I have not yet seen the death. (#59, son: 63yo-M; decedent: 95yo-F)
In summary, we did not find a relationship between the reported presence of dementia in patients and reports of awareness of impending death by patients or family caregivers.
Discussion
Reported rates of awareness of impending death were 64% for family caregivers, and 36% for patients. The rates we found were within the wide range of previously reported data. The high percentage of family caregivers unable to report whether or not their relative was aware of impending death may be understood by the fact that the reported deaths occurred in hospitals which provided long-term geriatric care. In addition, some patients who were not reported to have had dementia may nevertheless have had some degree of cognitive impairment, given the setting and our study’s reliance on family caregivers’ reports concerning the presence of dementia.
The findings show that awareness of impending death most often occurs a relatively long time prior to the date of death, with a median of 1.5-2 months prior to dying in this population of long-term care patients. For those who are aware of impending death, this time frame would seem to provide a reasonable time period both for saying goodbye and making preparations for death and funeral. We found significantly higher rates of death-preparation for saying farewell and providing pre-death instructions among those reported to be aware, but no differences as to making funeral arrangements. These findings partially support the advantages claimed for awareness, as mentioned in the literature. However, the implications need to be examined in light of other potential factors, such as past communication patterns and ability to communicate at the end of life, or gender, educational level, and socio-economic status, which have been previously found to have an impact on whether older adults have financial and health end-of-life plans in place (Su, 2008).
As to factors affecting awareness, we found that when a patient became aware of impending death, the family caregiver was likely to be aware, but that was not the case conversely. Presumably, when the patient is aware, ensuing discussions increase family caregivers’ awareness. Such exchanges may not be as common when the family caregiver, but not the patient, is aware of impending death. Other factors that impact awareness according to family caregivers’ comments are a diagnosis known to be terminal, a precipitous deterioration in health or apparent symptoms of dying, and being told by a professional that death is approaching. Future research should examine the methods by which family and other caregivers draw conclusions concerning whether or not patients are aware of impending death, including whether discussions have taken place about the topic, and who was informed of the diagnosis, expected medical course and time trajectory.
Consistent with other research, we found the reported lack of awareness to be partially explained by dementia or low functional status (Andruccioli et al., 2007; Seale, 1991; Seale et al., 1997). Further research is needed to clarify the impact of dementia on awareness. It would likely depend on the stage of dementia, since in later stages, communication difficulties impede understanding the point of view of the person with dementia. Even in the early stages of dementia, lack of awareness may be influenced by formal and informal caregivers’ reluctance to discuss the topic, or by the patient’s short-term memory loss that can render patient awareness of the prognosis disclosure transient. On the other hand, memory in the early stages is affected by the significance of the information, in which case the disclosure may be better retained. Further research is warranted, although such research will be subject to difficulties such as the sensitivity of the topic and the frailty and compromised communication level of persons with dementia. Consistent with prior research, we did not find a relationship between background demographic variables and awareness (Lokker et al., 2012; Seale et al., 1997).
Another recurring theme was the ambiguity of the sensation of awareness, as family caregivers may understand that death is close without a sense of the exact timing, and may be caught by surprise when death occurs. Thus, it seems possible for people to be aware and unaware concurrently. This conclusion finds expression in Timmermans (1994)’s research about the complex nature of open awareness, which can range from acceptance of dying and preparing for it, to choosing to ignore or disbelieve the information communicated by medical staff. This further highlights the importance of emotions, as in our study, unawareness was also associated with sentiments of denial or persistent hope, exemplifying the emotional difficulty of accepting impending death (McGrath, 2002). While acceptance and hope are competing emotions, they can be held simultaneously, further exemplifying the complexity of these emotions when it comes to end of life and dying (McGrath, 2002).
This study’s main limitation is having been undertaken in a population mostly residing in long-term care facilities in Israel. However, prior research demonstrated that rates of awareness depend on terminal disease category (Exton-Smith, 1961; Seale, 1991; Seale et al., 1997), and the current study concerning Israelis receiving residential care at the end of life complements prior findings. In addition, recall bias, in which grief reactions may color the memory of awareness, is acknowledged. Another limitation is that we were unable to interview the decedents’ family caregivers about this issue prior to their relatives’ death. Pre-death interviews are subject to both practical and ethical challenges.
The study is innovative in examining family caregivers’ perceptions of awareness for patients’ impending deaths, probing the relationship between perceived patient's and family caregiver awareness, and considering the duration of awareness and potential consequences of awareness. “Acceptance of death” may be a sign of awareness, which can occur for the family caregiver or terminally ill person. Seale (1991) found that, of people who were aware that they were likely to die, 61% were definitely accepting; 25% fairly accepting; and 11% not at all accepting. The question of acceptance was not directly queried in our study, and only emerged in family caregivers’ comments. However, the reasons for acceptance, its nature and prevalence warrant further exploration. For example, according to Exton-Smith (1961), some terminally ill patients who are aware of impending death lose the desire to live, refuse to eat and drink, and express a wish to die, all of which may be signs of acceptance or resignation concerning their approaching death.
Future research needs to examine the relationship between awareness of impending death and the utilization of additional potential benefits of such awareness, including expressing final thoughts, conveying love, attending to financial and funeral planning, and achieving closure. Future research should also examine longitudinally the effects of such awareness on family caregivers’ experience of various symptoms of grief.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Minerva Foundation, grant number 3158329500.