
Abstract
Understanding the meaning of loss for racialized immigrant fathers and addressing their experiences in a culturally competent manner is important in an increasingly ethnoculturally diverse country like Canada. Culture, customs and rituals influence fathers’ grief and culture impacts how individuals discuss death and dying as well as how they perceive the death of a child. This article is part of a qualitative research project, which examined the experiences of racialized immigrant fathers who experienced the death of a child. Guided by Charmaz’s constructivist grounded theory, the methodological aim was to develop a theoretical framework grounded in fathers’ experiences of child death within the hospital setting. Findings suggest that for racialized immigrant fathers their migration experience compounds their losses in unexpected ways and that experiences of objectification or ‘othering’ in hospital and by health care staff were significant.
Introduction
In Canada, western provinces including Alberta have seen an increasing number of immigrants from diverse racial and cultural backgrounds. Statistics Canada (2017) projects that by 2026, 28.4% of the population will be from a racialized (non-white) background. Migration and the challenges of adjusting to life in a new country has implications for mental health and wellbeing, and these are intensified for newcomers who experience a racialized identity when they transition to life in Canada (Gushulak, 2007; Khan et al., 2017; Kirkbride & Hollander, 2015). When a newcomer family experiences child death, parental bereavement can be amplified by the stresses associated with migration and settlement. The death of a child may compound the sense of loss, hopelessness, and disconnection that can accompany adjustment to a new country (Lynch & Hanson, 2002; Pe-Pua et al., 2010; Tripodi-Potocky, 2002). While some research addresses ‘cross-cultural’ bereavement care for parents, scholarship on the experiences of racialized immigrant families is a neglected area of inquiry.
This paper reports on findings from a constructivist grounded theory study which aimed to better understand and address the bereavement support needs of racialized immigrant fathers, and to use their perspectives to inform the development of culturally competent grief support services in healthcare settings. Our analysis suggests that for racialized immigrant fathers their migration experience compounds their losses in unexpected ways and that experiences of objectification or ‘othering’ in hospital and by health care staff were significant. Please note that throughout this article, we use the term racialized to recognize the dynamic and complex processes in which dominant groups produce racial categories that entrench social inequality and marginalization (Ontario Human Rights Commission, 2009).
Background Literature
When a Child Dies: The Impact on Parents
Experiencing the loss of a child is one of the most traumatic events a person can endure (Chambers & Chan, 2000; Hensley, 2006; Li et al., 2003; Woodgate, 2006). For parents, coping with the loss of their child can be a lifelong process (Walsh & McGoldrick, 1991) and mourning can extend far beyond the time the child lived (Miller & Ober, 1999). Bereaved parents experience depression and anxiety, as well as anger, detachment, and a loss of control (Walsh & McGoldrick, 1991), leading to “somatic symptoms, difficulties in social interaction, and a challenge to the meaning of life” (Aho et al., 2011, p. 880). Parental bereavement is complicated by the fact that parents must also continue care for their living children and spouses, with little time or space to grieve. Without appropriate and culturally safe supports, bereaved parents can become seriously physically and emotionally unwell, with long lasting impacts (Li et al., 2003). For example, an association between losing a child and increased probability of early mortality was established in a large-scale study (Murphy et al., 2003), which found that mothers experienced increased mortality risk throughout their lifespan in comparison to mothers who had not experienced the death of a child, and that the mortality rate for fathers was higher in the first year following child death.
The death of a child greatly impacts the well-being of a parent and may also lead to stress on the marital relationship between bereaved parents (Walsh & McGoldrick, 1991), intensifying pre-existing marital problems (Corr et al., 2009). The death of a child is associated with high rates of divorce (Badenhorst et al., 2006; Wing et al., 2001). However, Lang and Gottlieb (1993) suggest that child loss may sometimes improve a marital relationship, leading to increased closeness between a couple (Hagemeister & Rosenblatt, 1997; Lang & Gottlieb, 1993; Wood & Milo, 2001).
Research on parental loss and grief has historically focused on mothers (Badenhorst, et al., 2006; Cacciatore, 2010; Davies et al., 2004; O'Leary & Thorwick, 2006; Rice, 2000), especially the experiences of prenatal and perinatal deaths (Corr et al., 2009), and less is known about fathers’ experiences. Gendered norms and expectations around parental roles in heterosexual couples reinforce assumptions that men are uncomfortable sharing their feelings and are less likely to seek grief support (Staudacher, 1991), and have confined men to the roles of leader, protector, and the emotionally stable “rock” of the family, especially for a traumatic event like child death (Doka, 1996; Doka & Martin, 2002; McCreight, 2004). A father’s protector role may become much more pronounced after he has suffered the death of a child which can have a negative effect on their ability to grieve (Staudacher, 1991). For example, Wood and Milo (2001) showed that bereaved fathers coped with their grief through activities (e.g., playing sports, going to work) and displayed stoicism instead of discussing grief verbally or asking for social support. While there may be gendered patterns to grieving, insisting “men grieve like women,” may create pressure for fathers and miss the opportunity to support and understand the social roles and behaviours associated with men’s grief (Zinner, 2000). Yet extending beyond such broad considerations around the role played by gender norms in shaping parental grief, there is also a need to consider how cultural norms, especially as they intersect with racialization and immigration, shape bereavement for parents.
Culture, Child Death and Parental Bereavement
Williams and Spencer-Rodgers (2010) define culture “as a set of shared meanings and practices that are transmitted, communicated, and reinforced among members of a cultural group, and that, in turn, influence the values, beliefs, emotions, and behaviours of their members” (p. 591). Cultural background and associated processes of socialization influence views on death and dying, including end-of-life processes, rituals, and practices (Saiki-Graighill, 2001; Srivastava, 2007). Culture influences the meaning ascribed to illness, suffering and dying (Kagawa-Singer & Blackhall, 2001), the experience of pain associated with bereavement and mourning, as well as specific beliefs and practices related to the end of life (Pottinger, Perivolaris, & Howe, 2007). Some evidence suggests that bereaved parents from racialized backgrounds do not access mental health support, including grief and bereavement services (Clements et al., 2003; Shapiro, 1996), and that unmet needs in regard to cultural values and practices negatively affects health care for families who have experienced the death of a child (Davies et al., 2011; Hebert, 1998). Yet because of cultural variation, people from the same cultural background may not behave in the same ways following the death of a loved one (Lynch & Hanson, 2002). Cultural norms are not universal when it comes to an experience such as death, as an individual’s response to a death may be impacted by social, ethnic, religious, and philosophical values and beliefs, in addition to cultural values and norms (Rando, 1984).
Culture is also not synonymous with racialization but the two are closely linked, as individuals can experience racialization through the imposition of labels and stereotypes associated with skin colour, accent, speech, mannerism, beliefs, attire, practices and habits (University of Guelph Human Rights and Equity Office, 2015). The Ontario Human Rights Commission (2015) describes an individual as a racialized person and a larger collective as a racialized group, to replace out-dated and inaccurate terms such as racial minority, visible minority, person of colour, and non-white. Racialization is a perspective that makes evident the social construction of racism and the corresponding race-based disadvantages embedded in daily interactions, values, policy, and social relations.
To respond to the needs of racialized patients, there is a growing focus on the importance of cultural competency in healthcare and in end-of-life care, but primarily addressed to adult patients (Kagawa-Singer & Blackhall, 2001; Kennedy-Kish Bell, Sinclair, Carniol, & Baines, 2017; Koenig & Davies, 2002). Cultural competency refers to: “An individual’s and program’s ability to honour and respect those beliefs, interpersonal styles, attitudes, and behaviours both of families who are clients and the multicultural staff providing services” (Denboba et al., 1998, p. 47). In practice contexts, cultural competency is not limited to awareness building and sensitivity; it is a concept that includes knowledge creation and skill acquisition. Equally important in cultural competence is the relevance of self-awareness (Field & Berhman, 2003; Srivastava, 2007).
Emergent research on the experiences of bereaved parents from different racialized and cultural backgrounds has been carried out in the United States, Denmark, Japan, Australia, and Finland. Studies conducted in the United States cover the experiences of White Americans and African Americans (Davies et al., 2004) as well as Mexican Americans and Chinese Americans (Davies et al., 2011). In one study Davies et al. (2011) interviewed 10 Chinese Americans and 26 Mexican Americans who had lost a child through death 6 months to 5 years prior to the study. The results suggested that language, healthcare providers’ lack of experience in palliative care, focus on ‘cure,’ and discomforts in discussing dying were barriers to receiving and culturally competent healthcare. Language and cultural barriers, particularly regarding information-sharing by healthcare professionals and spiritual care staff were perceived as challenges in receiving and providing end-of-life care. When there was insufficient information sharing, the parents experienced frustration, resentment, and sorrow long after the death of their child (Davies et al., 2011). In another retrospective grounded theory study, Davies et al. (2004) interviewed eight fathers who were either racially White or African American, who had experienced the death of a child no more than 3 years and no less than 1 year prior to the study. The researchers noted that the fathers referred to their experiences of losing a child as “one living in the dragon’s shadow” (p. 118). According to the fathers interviewed, dragons are perceived as creatures that attack heroes and these fathers felt they had to battle the dragons for their children. These findings illustrated that although the fathers had experience in accessing bereavement services, “interactions between fathers and professionals were not always smooth and pleasant” (p. 131). Indeed, as suggested by Field and Berhman (2003) when healthcare professionals incorporate the family’s cultural, ethnic, and religious beliefs about death and dying into their practice, whatever those beliefs may be, the family is better able to cope with the loss of a child.
Building on this previous work the first authour designed a qualitative doctoral research project to explore the experiences of racialized immigrant fathers who had experienced the death of a child. This study explored how the stress resulting from the death of a child may be compounded for racialized immigrant families due to language barriers, cultural differences, and challenges related to settlement processes, as well as social isolation (Kongnetiman, 2017) Guided by Charmaz’s (2010, 2014) constructivist grounded theory, the overarching methodological aim was to develop a theoretical framework grounded in fathers’ experiences of child death within the hospital setting.
Methodology
Participant Recruitment
This study was part of doctoral research project which was completed in Alberta, Canada by the lead author. Participants were eligible to be included in the study if they were racialized, immigrant fathers whose children had died in the last 5 years (but no less than a year) and who had accessed palliative care and grief support services at a children’s hospital. Fluency in English was a requirement as interpreter services were not available. For this research, racialized immigrant refers to a non-white, ‘visible minority’ person who immigrated to Canada as an adult. Participants were recruited with the help of a coordinator in the palliative care program and other staff at the children’s hospital who sent letters and emails to all families who had accessed services during the 5-year eligibility period. Initial screening for participants who self-contacted the researcher was completed over the phone. This led to four participants and an additional four were recruited through ‘snowball sampling’ (i.e., contacts known to other study participants). Fathers from different racial, ethnic, and cultural backgrounds with different lived experiences were chosen to be part of the study to ensure that diverse experiences were represented.
Data Collection
The interviews were conducted face-to-face by the lead author, with each interview lasting for approximately 90 to 120 minutes. Participants chose an interview location where they were comfortable: some chose to be interviewed in their homes and others at the hospital. An informed consent process was followed, and participants were made aware of their right to privacy and confidentiality, the right to withdraw at any time during the interview, and to receive study findings and follow-up information. All interviews were audio-recorded and subsequently transcribed. An honorarium was not provided as this was a student thesis. Ethical approval was granted by Conjoint Health Research Ethics Board, University of Calgary.
A flexible and exploratory approach to interviewing was employed following an interview guide that included questions about the fathers’ cultural values and beliefs about death and dying, their role within their family when their child died, perceptions of their family’s treatment in the healthcare system, and impacts of bereavement on their health status. This method of gathering data allowed the fathers to be the experts when sharing their experiences with the aim of creating a comfortable environment to freely express their thoughts, beliefs, and experiences (Denzin & Lincoln, 2005). The interview approach aligned with the methodological approach of constructivist grounded theory, which positions interviews as an unfolding story or theoretical narrative created by the researcher and participants (Charmaz & Belgrave, 2012). At the end of the interview, the interviewer reviewed participants’ understanding of the purpose of the research and ascertained their emotional well-being. Participants were given a list of community bereavement support services in case they required support after the interview ended.
To achieve trustworthiness in qualitative research it is necessary to establish credibility, transferability, dependability, and confirmability (Charmaz, 2011; Corbin & Strauss, 2008; Lincoln & Guba, 1985), and these standards for research rigour that are core to the constructivist grounded theory approach were employed. An audit trail was used to track decisions made throughout the study and to document procedural and analytical steps or shifts. As well, a reflexive approach included notetaking and writing journal memos to support identifying any potential bias that could have affected the study in terms of data collection and interpretations (Lincoln & Guba, 1985).
Data Analysis
Coding was carried out using the constant comparative approach from constructivist grounded theory (Charmaz, 2011); this approach meant that the initial codes were constantly compared with new, subsequently gathered data. Data analysis was carried out iteratively over time and in several steps, as new data collected was integrated into the emerging analysis following each interview (Charmaz, 2011). Coding progressed through the focused coding stage (Charmaz, 2006; 2010), with the development of codes that reflected ideas, repeatedly seen within the participants’ narratives, and related to the research question (Charmaz, 2006), as well as the researcher’s subjective interpretations of the data (Charmaz, 2010; Denzin & Lincoln, 2005). Additionally emerging codes and categories were continually discussed and refined between the first authour (doctoral student) and their research supervisor. Throughout this process, coding was done manually by the lead researcher (LK) using word processing software, and analysis software was not used. In terms of research positioning and accounting for its role in data collection and analysis, the lead authour was the primary researcher and is a racialized woman and immigrant to Canada with lived experience of parental bereavement. The second authour is a white, Canadian, non-immigrant woman and mother of racialized children who has not experienced child death or parental bereavement.
Codes were then grouped according to commonalities, forming categories or overarching themes. Through the formation of codes and categories, a theoretical understanding of the participants’ experiences took shape. The final analysis consisted of eighteen codes and six categories: objectification of fathers in the health care system, bicultural grieving; making meaning of the death of their child; multiplicity of roles as a father; and managing their own health following child death. This paper reports on the theme: fathers’ experiences of objectification in the health care context and the findings under three associated codes: mistrust, cultural insensitivity, and procedural experiences. Figure 1 provides a visual representation of the approach to analysis and theoretical development entailed in Charmaz’ constructivist grounded theory that was used in this project. The grounded theory coding process (Charmaz, 2010).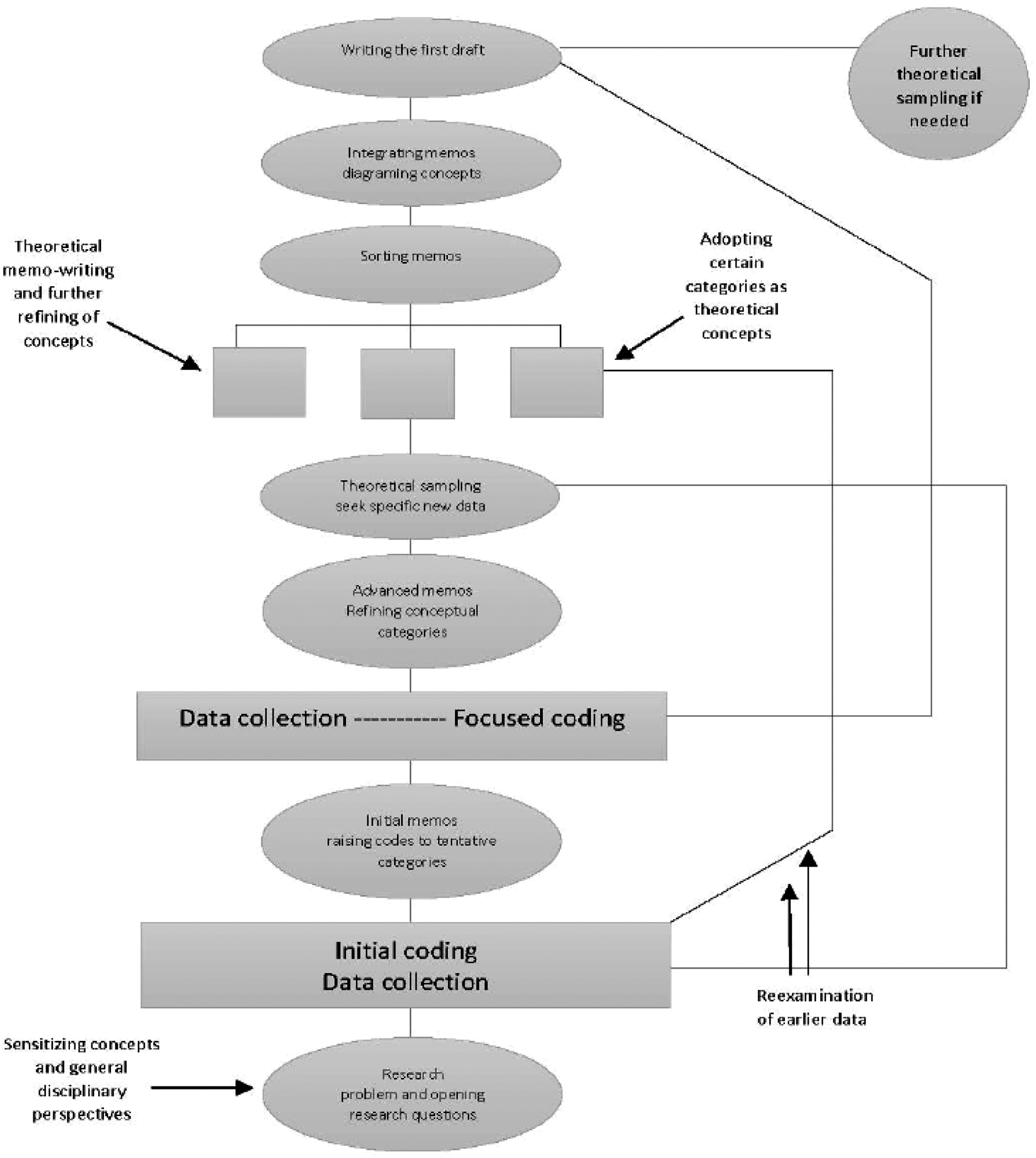
Theory-building: Hollow from the Inside
The overarching theoretical framework grounded in this research can be described as, “hollow from the inside,” (Figure 2, Findings section) a term that encapsulates racialized immigrant fathers’ experiences of grief at their loss, their sense of disconnection, and lack of support. “Hollow from the inside” was a metaphor a participant used to describe how he felt after the death of his child; he perceived himself as a tree, presumably deeply rooted in the ground and appearing to “standing tall,” but feeling an emptiness inside, and a void owing to his loss. This metaphor is connected to the six major categories or roots of the tree. The analysis presented in this paper focuses on one strand or root of the theory tree that was developed, that is objectification within the formal health system, with other analyses planned for future publications. Hollow from the Inside. Note. There are six tree roots that represent the major categories of this research and the codes are embedded below in secondary roots that are supposed to bring nutrients and life to the trunk and the leaves.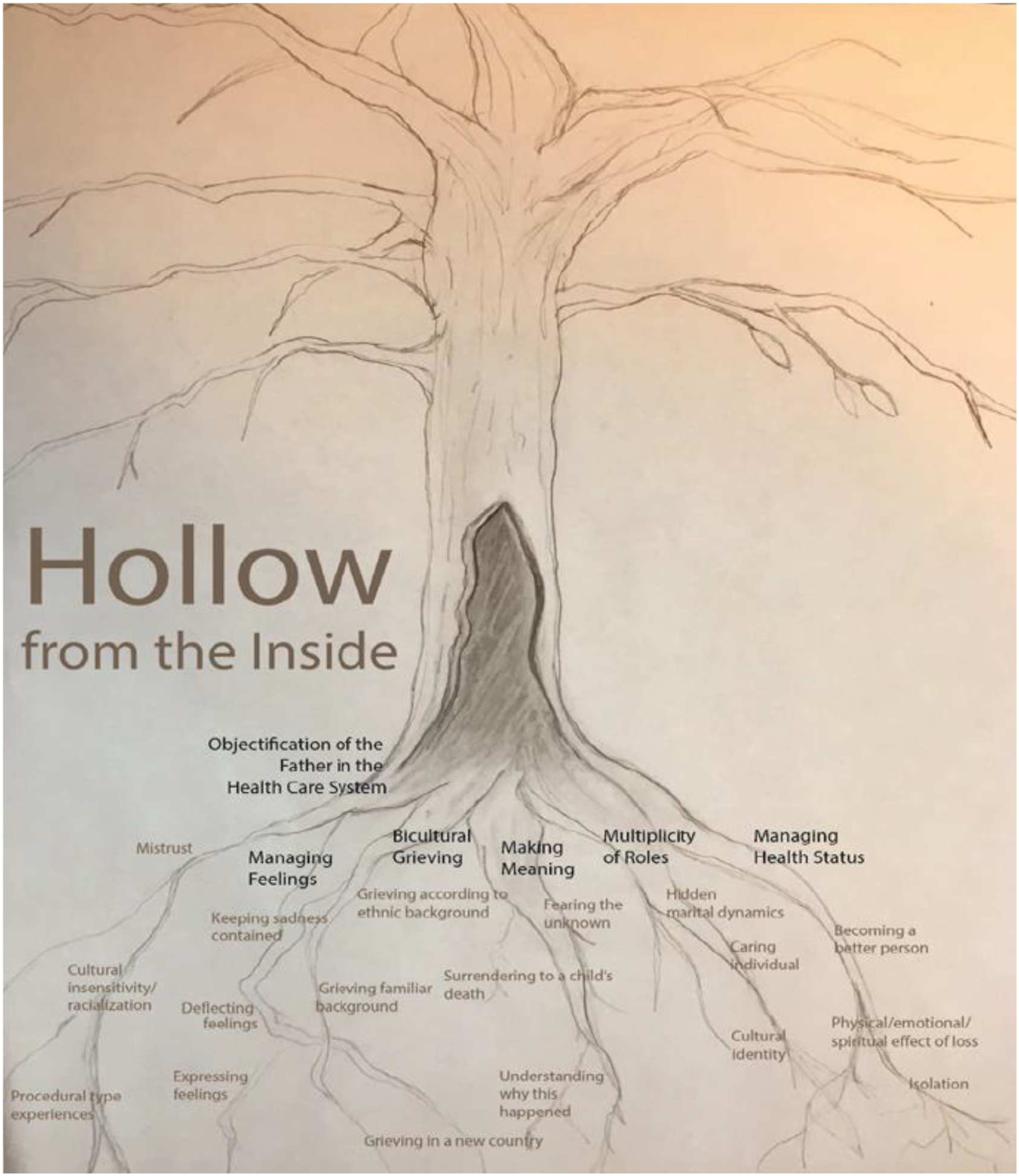
Findings
Participant Demographics.
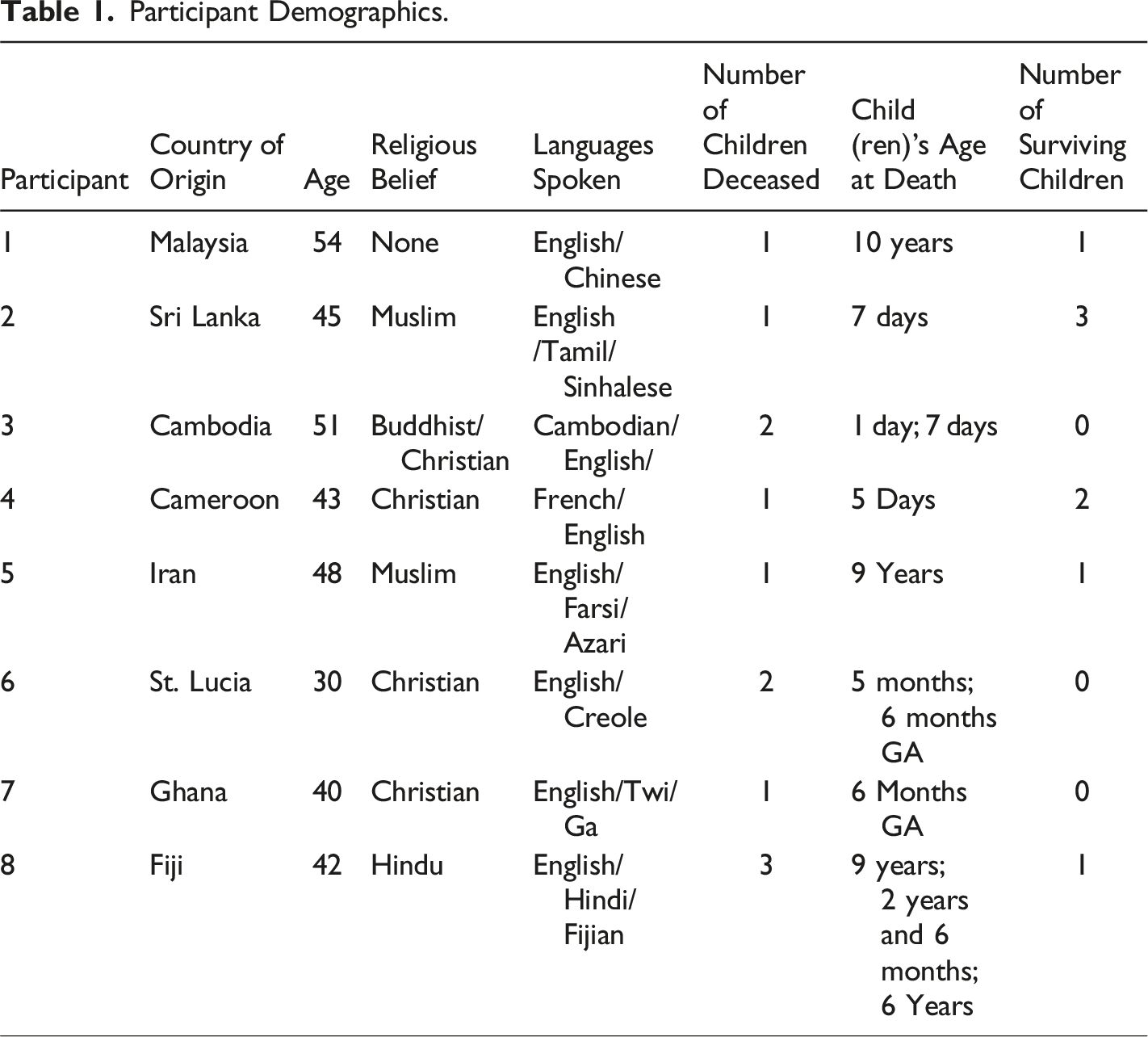
Each father brought multiple layers of experience to the process of bereavement arising from his country of origin, culture, language, immigration history, faith, and everyday life experience in Canada. Fathers’ experiences in the healthcare system were also diverse, with both positive and negative experiences reported. Yet a central theme within the interviews related to how fathers experienced an overall sense of dehumanization or objectification as immigrant, racialized men, and experiences and interactions that led to them feeling unworthy and “less than” human in the context of their interactions around their child’s care. Fathers shared feelings of mistrust and cultural insensitivity they experienced with healthcare providers and the lack of a truly consultative, “family-centered” approach to decision making about end of life care and medical procedures for their child. Fathers also expressed that when accessing services either for themselves or for their children or spouse they often felt powerless, uninvolved, and unheard in the hospital setting. Many shared feelings of anger and self-blame, and the over-arching sentiments were of betrayal and disempowerment, because of their perceived lack of choices and the inability to be meaningfully involved in decision-making about their child’s care.
Mistrust
Mistrust expressed by the participants was related to being treated differently because of cultural beliefs in health and illness and expression of different worldviews. The perception of differential treatment was grounded in the belief that they were being treated differently for expressing cultural views on illness, death and dying that were at odds with those expressed in the healthcare setting or by their child’s medical team. Some of the fathers felt too intimidated to share their “true” thoughts about how they were being treated or how they believed their child should be treated. Because of a perceived lack of cultural understanding, some fathers did not know how sharing certain views could potentially be used against them, as they had witnessed how others were treated when trying to discuss their concerns with healthcare professionals. As a result, many shared that they did not feel heard or understood when trying to explain how their culture influenced their decisions, leading to mistrust.
Misunderstanding of their cultural beliefs and mistrust influenced many aspects of the healthcare experience. This lack of trust and connection was seen through statements such as: “The doctors’ office is like a processing factory” (Participant 4). “Look at your patients as humans” (Participant 2 and Participant 4). For some fathers, this mistrust was compounded by the belief that their child died because of miscommunication or medical error, leaving them to process grief while also mistrusting the people and system caring for their children. As one father shared: “We paid a huge price because of human error” (Participant 4). Some perceived that the system had failed their family, and that there was pressure for their child to be discharged because of lack of beds in the hospital or shortage of other resources. One father described his experiences: I think there was some push to get our child out of the Intensive Care Unit, for some reasons, which I mentioned before, costs and availability of beds and what not? Which caused/expedited the process. Because death, death was coming to him, so they kind of expedited it. (Participant 2)
The sense of being wronged by both miscommunication and a lack of access to resources was not just present in the hospital setting, but in the primary care context, as one father shared how this influenced his wife’s access to prenatal care: I strongly believe that if my wife were in [another province], things would have been different because, first of all, for many months, she couldn’t find a gynecologist. So, we were just, you know, going to the family doctor and there was no proper care, she actually, was sent to go to the lab and do some tests. And then the doctor received the tests, that, the baby kind of not doing well. And we did not get the results of the tests until the very day that she kind of went to see another doctor or something like that, she went for another test and then they said that, you know what, the baby is gone. And then we realized that, you know, the first test has showed that the baby may not survive and they have already sent a report to the family doctor and the family doctor didn’t have the time or somehow missed that information or something like that. So, there’s a whole kind of, difficulties in, the waiting period, to see a specialist and those kinds of things. So, I think that’s also contributed to the loss. (Participant 7)
Some fathers felt physicians did not provide them with the full scope of services and time that their family required. For one of the fathers interviewed, there was a strong sense that their spouse’s care needs were not appropriately addressed: But my wife, saw the doctor but he was busy all the time, you know, only spoke to my wife each time, maybe 3 or 4 minutes, and then he was gone—you know to see another patient. But she was concerned that maybe she doesn’t get the help she needed you know, she didn’t feel like she was being looked after. So, she changed to another family doctor. (Participant 3, lost two daughters)
Fathers’ mistrust of the healthcare system tended to be focused on how health information was shared with them. Some fathers felt like they did not have the full scope of information to make decisions for the well-being of their children. After the deaths of three children, to then hear that it was related to genetics, led one father to be completely dismayed with the healthcare system. This father could not understand the possibility of losing three children in the same hospital and not having known earlier that it was genetically related until he lost his third child: When our third child passed away, then I know, the doctor tells me I got a genetic problem. Then I am worried, why didn’t the doctor tell me before? We don’t have our children anymore. Why we suffer right now, painful, all my life still. Then the medical professionals told my wife and I that it is because the doctor made mistake and doctors make mistakes too. And, right now because of this, like I’m not blaming them but if these doctors know what happened, and that one of the other children would be next, why didn’t they tell me first when my first son died there at the hospital? We would have stopped it, we don’t want to keep suffering. These all my life I am suffering right now. (Participant 8)
Mistrust was also perceived as ‘broken promises’ as another father shared his experiences when his son died and his desire to seek retribution for the death of his child. They pretty much killed the baby. That’s what I would say, you know? The thing is that’s how I feel about it. You’re asking my experience, so that’s how I feel it. And because we don’t know what happened behind the scene. If I was there, they wouldn’t have removed him from oxygen from seven o’clock to until, until when he was moved to another hospital, like twelve o’clock. So, that’s about four to 5 hours, and we know the consequences of removing the oxygen. And, so. I would say not to trust medical professionals on whatever they say. Because you can’t trust them, because they broke the promises in the sense whatever they agreed. This is the problem with the hospital system. You have to sue them to get certain things done. But we didn’t want to go that far we wanted to correct the system, and we had few discussions with the medical team. (Participant 2)
In these instances, fathers who were grieving the loss of a child expressed powerlessness and a lack of trust in physicians and institutions they expected to provide them with care. Compounding this loss, were instances where fathers experienced cultural insensitivity in health care tied to their status as racialized, immigrant families.
Cultural insensitivity
Experiences of cultural insensitivity were seen in how the fathers were treated by healthcare providers or what they witnessed in terms of how others were treated differently because of their cultural or spiritual beliefs, their immigrant status, and because of their racial background. Fathers who encountered racialization in accessing healthcare sometimes articulated these encounters using terms such as ‘insensitivity’ and ‘discrimination,’ without articulating them expressly as ‘racism.’ Although they expressed anger, fear, and helplessness about these experiences, some fathers also felt healthcare providers had little understanding of how their actions were harmful.
Particularly salient in this code were instances where there was a lack of cultural competency demonstrated by healthcare providers, instances where fathers felt racialized in the hospital setting, a lack of understanding of diversity in grieving, and negative experiences associated with receiving bad news about their child’s health status from providers. Additionally, some of the services (e.g., counseling, and palliative care) that were offered were not adequate for addressing their culturally specific needs and/or their religious beliefs. There was little communication between fathers and the healthcare team, and some expressed that they felt pressured to comply with healthcare decisions for their child. In turn, hospital-based services meant to help families with decision-making were not seen as culturally sensitive and therefore were not accessed by families.
For example, fathers shared how the lack of support for decision-making impacted the process of deciding to withdrawal life-sustaining treatment (life support). Some shared that they had felt pressured to make the decision to withdrawal life support and expressed not having had the opportunity to fully discuss and explain the impact this decision had on them culturally and or spiritually. This was a source of anguish and guilt, especially those who held cultural beliefs that withdrawal of life support is culpability for death. One father shared how he felt pressured: And, like I said, we had the neonatal chief talking to us. She is a chief in the sense that she is a main doctor in the department and, quite a few doctors, came and spoke to us and educated us on this issue and that’s when they were talking about, terminating the pregnancy and everything. So, they did their part, and I would say that there was a little bit of pressure to make decision. (Participant 2, lost one son)
Discussions of their child’s limited chance of survival was very difficult for the fathers no matter how it was communicated by the healthcare providers. For some, allowing that conversation to happen was equated with failure as a parent, and a feeling that they were responsible for ‘sentencing’ their child to death. Cultural beliefs about death and dying prevented some fathers from having this conversation with the medical team, and some expressed that they felt caught between their cultural beliefs and western medicine. One father described his interaction with the healthcare team looking after his son: So, Neonatal Intensive Care room over there at the hospital, the doctors are working on it, so then this doctor comes in, and he says, you know, we need to talk. I say, okay, talk. Yeah, I don’t believe your son is going to make it, and I guarantee that he’s not going to be released from here, we can make it easy, you know, give him, some medication, so that he slowly, you know, pass away, you know, he’ll be in peace, and you guys too. And I say, you know what, I don’t, think so, if he lives, he lives. I don’t have a problem with that. But I’m not going to let you euthanize him. (Participant 5)
As well as lacking support for end of life decision-making, in some interviews, accessing formal support such as counseling support for grieving fathers was discussed. Not all the fathers were comfortable with accessing formal support to address their grief experiences. The fathers interviewed felt that their specific cultural needs and perspectives on death and dying may not be well understood in the conventional forms of talk therapy that are offered for bereavement counselling. Others expressed a belief that grief support was best delivered through family members, parents, or elders in their respective communities. To this end, accessing formal grief support outside one’s own community was not seen favourably. Seeking emotional support was seen by some as a sign of weakness and the inability to cope, which challenged cultural beliefs about strength and coping: Because if you look at counselling, in my language, we don’t even have a word for counselling. But we have a word for advice. So, I would have gone to my mother for advice if she was alive. And then she will tell me exactly what to do and provide words of encouragement. Secondly, too, if I were to go see a counsellor, if somebody would have told me that, you know, you need to see a counsellor, whatever, I wouldn’t have gone because I need somebody who understands my culture. And, I, don’t think it will help me to see a counsellor a Canadian counsellor who doesn’t understand anything about my culture, especially when it comes to grieving and those kinds of things. Right, so no, it never occurs to me that I have to see a counsellor or, even I wanted to see a counsellor. No. (Participant 7)
Every father approached the topic of formal support or talk therapy differently. This father shared his experiences with having a social worker provide support to him and his spouse: The same social worker came to do the counseling. I can’t say if we feel better but when she left after a while, we always feel like getting back to our feelings, to that kind of feeling of sadness, depressed—and then, whenever I see my wife cry she would be talking about the baby, about the happy times, you know, while our daughter was still in her womb and everything was happy there. We always try to think about the happy times, but still, you know. They told me, maybe, try to think about, how much happy time you spent with her, she will die, and maybe she is still a part of us. But my wife, she was crying and I was crying too but crying inside, not to let her know. (Participant 3)
As counseling is an individual preference that is culturally shaped, some fathers felt that support should come from their immediate family. One father explained his understanding of accessing formal support: I don’t believe I need counseling. I have some private memories that I want to keep for myself, that I loved my child and that is part of my life, it comes and goes, and so you know, for that reason you know, I can usually get support from my brother, dad, and other people they help me to keep my son close to me for a while, I don’t really get used to the new normal. (Participant 5)
For one father, information-sharing regarding resources might be seen as suitable for some patients, but this was not seen as acceptable for patients from culturally diverse communities. This made him feel as if the healthcare system was discriminatory and privileged other families over immigrant families. This is how this father expressed what he experienced: The first experience that I had in healthcare regarding discrimination was this —we pay our taxes as same as everybody else. We found out that we could have an aide, actually, because my wife was by our son’s side, 24/7 at home without any help. Even our lovely social worker, was saying, there is no discrimination, but there is. Because they are always thinking of us as this immigrant. I feel like they are looking at us like outsider. I couldn’t find a reason where the social worker couldn’t tell us that the government could provide an aide but no one told us, for years until my wife found out from somebody else that she has three aids, 24 hours, and we don’t have any. As a Middle Easterner, as a Muslim we experience discrimination constantly. They are saying no, there is no discrimination but that is totally not true. I never told anybody about my experiences. Who am I going to tell? How are we going to settle? Then we will experience another problem. One of them is going to come out and say, prove it. (Participant 5)
With a lack of culturally sensitive supports, parents expressed feeling ill-at-ease with what the hospital provided to support them in their grief, and this also played out in how they experienced the care and medical procedures their child received prior to their death, and at end of life care.
Procedural Experiences
The coding under procedural experiences explored the different procedures that children underwent and how this affected fathers. Some procedures put the fathers in a very difficult position as they felt pressured to approve invasive and sometimes painful medical procedures and treatments for their children. However, the procedural type of experience was also positive for some. Fathers expressed confidence that the healthcare system had the most up-to-date technology, treatment modalities and state of the art equipment to support their children. Even when the child did not survive, many were comparatively more positive about their child’s experience of a medical procedure, when compared to how they felt about their interactions as a family with the healthcare team. For many of the fathers this showed that the healthcare system was well resourced to take care of their child, especially when they compared these resources to the hospital system in their country of origin. This is how one father described his experiences: Yeah. You know, it was a shocker. You see, what happened was she was just a normal kid. She had bleeding nose, so sometimes she would come in, her pillows all bloodstained. And after that one day, she called in from school, and she had this nosebleed that refused to stop, and we took her to the clinic and the doctor tried to cauterize it, and it did not stop and the doctor freaked out. He said to send her to the hospital. And I said okay when I was growing up as a kid, a nosebleed is nothing, you know? In Chinese culture, we believe that if you are under the sun too long you have what you call, maybe what’s the word in Chinese like your body become too hot and you bleed. So, all you do you just sprinkle some water on the forehead and cool down and you know? It goes away. But it didn’t go away, so they went in they usually do a full check-up and blood check-up and then the doctors came back, and they said, we think she has leukemia. (Participant 1)
Indeed, not every interaction with a negative outcome was equated with an experience of mistrust or insensitivity. Another father commented on this need for personalized care where his family’s health needs would be taken into careful consideration by the health care team, but was reflective about why an important diagnosis may have been overlooked: Take every case, I mean, look at every case as a special case, probably that’s what I’ll say. The healthcare providers have to consider every case as an important case, not to overlook things, look for the detailed information probably that’s what I will say. But I think is whoever made that first mistake it was not an intentional mistake it’s something that probably was unfortunate because that person overlooked some information, and like I said, my wife was told initially that because she has some defect in her womb, you know this is not the time for her to get pregnant, or it’s not a good idea for her to get pregnant. (Participant 7)
Some participants expressed that the practical and medical needs of the child were attended to with great care, but there was little provided in terms of day-to-day emotional support. Despite their assurance in the expertise of healthcare providers, fathers felt there was often a lack compassion and support displayed. This contrasting sentiment was expressed by several participants, as one father shared: Our doctor is an amazing doctor, very bright. But I just couldn’t understand why, I guess he didn’t understand the emotional side. So, we were there for almost a month, and they put a tube in our son’s mouth. Under the respirator, basically, breathing. So, they said, we cannot take it out, if he doesn’t breathe, and we can try one more time but after second time, we’re not going to do it. (Participant 5)
In turn, trusting in the expertise of the healthcare team when it came to end of life care, and relying on them to divorce emotion from medical decision-making was also a source of relief, as one person shared: Ah I feel very sad about it, but I’m glad that it wasn’t me, I’m glad that it’s not my fault that he died, it’s someone else’s fault, right? So, I’m happy in that term, so that’s how I make up my mind. So, I never had to make a decision to remove his CPAP, right? Then I would be suffering with stuff, with guilt the rest of my life, saying, I made that decision to remove his oxygen, or whatever. Sometimes things like that happen, sometimes people have to make difficult decisions. And it wasn’t me. So, that way, I make it up on that point? (Participant 2)
For racialized immigrant fathers, making decisions about end of life care and other procedures was very challenging and, in some cases, the situation demanded that providers make difficult decisions about care that parents felt that they were not capable of making. While parents were fully informed of the circumstances of their child’s care, in some instance it was clear that their inability to make certain choices was tied to their cultural or religious beliefs surrounding death, illness and life. In instances such as withdrawal of life support, terminating a pregnancy for medical reasons, or even making post-mortem arrangements for handling a child’s death (i.e., gathering mementos including lock of hair, handprints and footprints, taking pictures of the deceased child), some fathers expressed relief and gratitude that the healthcare team led these choices for them. This demonstrates that complex relations between families and healthcare providers in times of critical decision-making, end-of-life, and grief. While there were many instances of objectification and mistrust described, at the same time fathers experienced the presence of expert care and support.
Discussion
Summary of Significance
The fathers who participated in this project openly identified experiences of unjust and discriminatory treatment, and the interviews suggested the complex ways that their experiences within the healthcare system were linked to immigrant status, cultural beliefs and racialization. The findings of this study contribute to the literature on the impact of immigration on health and the barriers that many patients experience in accessing health services (Asanin & Wilson, 2008; Gagnon, 2002; McKeary & Newbold, 2010; Srivastava, 2007). Even as there is now a growing emphasis on systemic racism in medicine (Berman & Paradies, 2010) research has long identified the need to focus on racism, racialization and discrimination and its impact on interactions and in healthcare settings (Pollock et al., 2012).
It is always difficult for patients and families to show how they were discriminated against (McGibbon & Etowa, 2009), and sharing experiences of discrimination, racism and racialization can be challenging. In many instances discrimination occurs through subtle behaviors, processes in communications and in experiences that may be perceived as receiving inadequate services that contribute to making them feel like they are less (Beiser et al., 2001; Magoon, 2005; Pollock et al., 2012). In the present study, many of the fathers shared that they experienced mistreatment in the healthcare system connected to culture, religion, or their immigrant status, but did not name it as racism, using terms such as discrimination instead. Some revealed that this was the first time they had an opportunity to express what they went through emotionally when their child or children died and speaking about these incidents and identifying how they had been affected appeared to be painful and difficult for many of the participants. Based on lived experiences as a racialized woman who suffered the loss of two children, the study lead was able to extend compassion and show understanding. Despite apparent differences in gender and culture, this aspect of shared positioning between researcher and participants likely played a role in creating the perception of a safe space for the fathers to share their own lived experiences.
Study Limitations
A noted limitation of this study is that the approach was focused on the experiences of being an immigrant and racialized father in the general sense, and country or culturally specific data (or faith and culture-based data) was not collected or analyzed. We recognize that this study cannot possibly represent the experiences of all racialized immigrant fathers, and there were key categories of fathers that were not included in data collection. In particular, the study did not include people who were refuges or people who did not speak English, factors that may have contributed to additional marginalization or discrimination within the health care system. Additionally, as the lead researcher also identifies as an immigrant woman from a racialized background, this “insider/outsider status” can present challenges – but also strengths – for data collection and analysis. As mentioned previously, strategies for thinking through potential biases in data interpretations included reflexive journaling and debriefing with a research supervisor.
Lastly, the flexibility of constructivist grounded theory allowed leeway for the researcher to employ the method in the ways that will work best in their situational context. No two grounded theory studies follow precisely the same methods because strategies for application of the methods are an outcome of each researcher’s skills, discipline, cultural background, and pre-existing knowledge of the studied phenomenon. In this study, constructivist grounded theory methodology provided specific tools and methods, but the researcher still is responsible for the intellectual and interpretive work that describes and synthesizes the means within participants’ stories. The constructivist approach to data analysis accounts for how share experiences shape meanings and can enhance credibility and authenticity. Indeed, had this study been carried out by a White, Canadian-born, male, who had not lost a child through death resulting theoretical interpretations would have been much different.
Implications for Service Delivery and Practice
There are implications of this project for how end of life healthcare is delivered. It is necessary to address cultural sensitivity and cultural competency in healthcare (McGibbon & Etowa, 2009), particularly for child death. As Peng et al. (2012) stated “understanding culture and its role in care is important for professionals providing end-of-life care since cultural perspectives influence attitude towards sickness, dying, death and grief” (p. 321). Past studies also suggest that even without the experiences of racialization fathers often do not feel supported by healthcare professionals and the lack of communication in these matters exaggerates the negative experience of losing a child (Davies et al., 2004; Peng et al., 2012). Fathers, and all family members, would greatly benefit from a relationship with healthcare professionals that is characterized by caring, meaningful connections and supportive bonds with the medical staff (Davies et al., 2013). In the context of guidelines for pediatric palliative care developed in the United States, Schuelke et al. (2021) describe the need for providers to practice “cultural conscientiousness” and “cultural humility” when working with bereaved families, an approach that requires “lifelong commitment by the practitioner to be learners and allow the child or family to be the expert of their own culture.” (p. 14). Recent analysis from Gerlach and Varcoe (2021) points to the critical need for a structural lens to addressing inequities in child and family-centered models of care, which have typically treated “family” as a unitary concept, and have excluded considerations of the context for health equity in Canada, a “white-dominated society” with historical and ingoing racism and colonialism towards Indigenous peoples and towards racialized families who come to Canada as immigrants or refugees (p. 458).
From a health care equity lens, the experiences of racism, racialization and discrimination that the participants in this study described, are important to consider, especially from a capabilities perspective that recognizes the inherent worth and dignity of each person (Nussbaum, 2000).
In carrying out this study, the intent was for the voices of bereaved fathers to provide evidence that could shift practices in healthcare, by bringing awareness to providers about how interactions can perpetuate racism and mistrust, adding ‘insult to injury’ in the already traumatic context of child death and family grief. To respond to these lived experiences healthcare providers must take seriously how immigrant racialized fathers experience objectification and how their needs can be addressed with compassion, cultural competency, and the absence of bias and discrimination. To this end, the current action in Canada’s health care system towards anti-racism and anti-bias training for medical professionals and increased attention to policies that foster equity, diversity and inclusion are encouraging but only the beginning steps in creating culturally safe services (Rosenkranz et al., 2021; Smile & Williams, 2021). At the same time, we should recognize that despite the best intentions of health care providers and training programs, individual awareness, competencies and “skills building” approaches have limited scope, because racism in health care is a complex, systemic problem that requires structural and policy change. While the findings of this study are situated in relation to models of professional cultural competency, we also echo calls for a stronger emphasis on anti-oppressive and social justice frameworks as tools to more explicitly address racism. As Lei and Guo (2022) and write, “…racialized communities today demand not only recognition of their heritage culture, or more conversations about diversity, but also a heightened awareness and better social mobilization capability to demand immediate action and change for equity and social justice.” (2022; pg.13)
Implications for Future Research
Ethnographic research from Canada highlights the need to move away from paternalistic approaches to working with families whose children are hospitalized and severely ill or dying through a family-centered model of care (Macdonald et al., 2012). Insights gained from our research suggest that beyond a generic approach to the “divergence between professional and family culture” in pediatric hospital settings (Macdonald et al., 2012, p. 246), there is more research needed to specifically address the intersecting oppressions tied to racism/racialization, gender, and immigrant status and how the death of a child impacts the health of fathers. All the father’s interviews identified that losing their child impacted them on a physical, spiritual and or emotional level, and that they felt objectified within the healthcare setting. It would be of value to explore if access to culturally appropriate and safe grief support for the fathers would have had a positive impact on their experiences and on their health outcomes. Culturally safe bereavement services with a focus on addressing racialization may ensure that fathers from racialized backgrounds have access to services where they are less objectified and more included. This could include developing services outside of healthcare, with community and faith-based partners able to offer culturally specific and peer-based supports. Overall, this paper underscores the importance of developing grief programs that are targeted specifically to the needs of bereaved parents (Aho et al., 2011), in colalboration with the parents and families directly affected. It is essential that healthcare providers, especially those who work in palliative and end-of-life care settings, understand racialized fathers’ lived experiences of bereavement and the effects on their health status when their children die.
Footnotes
Acknowledgements
We would like to acknowledge the participants who agreed to be interviewed for this research project.
Ethical approval
Ethical approval was granted by Conjoint Faculties Research Ethics Board at the University of Calgary.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.