
Abstract
Lesbians, gays, bisexuals, and transgender individuals (LGBT) are at high risk for suicide. This study aimed to examine an integrative psychological model of risk factors among LGBT individuals and explore the psychological pathways connecting social stigma, mental pain, and interpersonal characteristics to suicidal ideation and behavior (SIB) in this population. LGBT adults (N = 473) responded to an online questionnaire about stigma, mental pain, interpersonal characteristics, as well as suicidal ideation and behaviors. We found group differences between LGBT respondents in the study variables: Transgender people reported the highest levels of SIB and depression, closely followed by bisexuals. The association between stigma-related variables and SIB was mediated by depression, entrapment, and perceived burdensomeness. These results highlight the role of entrapment and burdensomeness in facilitating suicide risk among LGBT adults, as they may increase the damaging effect of negative societal stigma against LGBTs and thus, elevate the suicide risk in this population.
Introduction
Suicide and suicidal behaviors are major health concerns worldwide, with more than 800,000 individuals dying from suicide annually (World Health Organization, 2019). Suicide rates have increased almost steadily over the last 15 years (Curtin et al., 2016), and suicide is one of the leading causes of death for adolescents and young adults in the U.S. (Heron, 2018). The scientific literature highlights several groups who are at relatively high risk of suicide, such as males (Gvion & Levi-Belz, 2018), those suffering from psychopathology (Zalsman et al., 2016), and immigrants (Lipsicas et al., 2012). One of the significant minority groups found to be at high risk is the lesbian, gay, bisexual, and transgender (LGBT) population (Sidaros, 2017), who are estimated to be two to seven times more likely to attempt suicide in comparison with the general population (Haas et al., 2010). These numbers highlight the importance of understanding the specific risk factors and moderators for suicidal behavior among LGBT individuals in order to implement tailored suicide prevention programs for this population.
Importantly, LGBT is an acronym primarily used as an umbrella term to denote several different sexual orientations and gender identities (American Psychological Association, 2015). Even though these identities are viewed as sharing similar culture, history, and experiences, there is a growing understanding of specific needs and concerns related to each individual identity (Clarke & Peel, 2008). For example, bisexuals face unique social and psychological challenges, as many of them suffer from biphobia, characterized by the stigma and discrimination that bisexual individuals experience from heterosexuals as well as from gays (Zivony & Lobel, 2014). Therefore, it is not surprising that, compared with heterosexuals and gays, bisexuals have shown higher levels of adverse life events, a lack of social support, and more anxiety, depression, and suicide attempts (Shilo & Savaya, 2012).
Studies have tended to include only lesbian, gay, and bisexual respondents, excluding transgender individuals. Moreover, many studies have disregarded distinctions between gay, lesbian, and bisexual respondents, preferring to focus on the disparities between males and females (Haas et al., 2010). Studies focusing on transgender people have revealed that they present higher levels of suicidal ideation and behavior than all other sexual minorities (Bockting et al., 2005; Tebbe & Moradi, 2016) and that up to 43% of transgender individuals reported making one or more lifetime suicide attempts (Clements-Nolle et al., 2006; Grant et al., 2011; Nuttbrock et al., 2010; Whittle et al., 2007).
Moreover, over their lifetime, transgender people who had experienced efforts of sexual orientation change reported a higher prevalence of suicidal ideation and attempts than other sexual minorities (Blosnich et al., 2020). In recent years, whereas more studies have addressed each of the LGBT groups discretely, these studies mainly dealt with risk factors for suicide and not with specific suicide-related variables and their prevalence (Mustanski & Liu, 2013; Skerrett et al., 2014). Thus, studies examining and comparing suicide and distress characteristics of each of the LGBT groups are still needed. In this study, we examined the differences in suicide risk and distress characterizing the various LGBT populations.
Most studies have shown that psychopathology associates with suicidal ideation and behavior of LGBT individuals (Haas et al., 2010; Nepon et al., 2010). These findings could explain the elevated suicide risk by the relatively high prevalence of mental disorders in LGBT populations. However, after adjusting for mental disorders, suicide attempt rates remain significantly higher among LGBT individuals than with the general population (Nepon et al., 2010), suggesting the need for understanding the unique psychological circumstances and factors that may facilitate SIB beyond psychopathology. Extensive research in this field connects LGBT’s SIB to lifetime experiences of prejudice, discrimination, and victimizations (Irwin et al., 2014; Mustanski & Liu, 2013), a contention congruent with the minority stress model.
The minority stress model holds that social stigma and prejudice-related life events create unique, chronic socio-psychological stressors that may lead to deleterious health outcomes (Meyer, 2003; Huebner et al., 2004). For example, Reyes and his colleagues (2017) found that the internalization of prejudice against LGBT identity among the LGBT individuals was consistently associated with higher suicide risk (see also Skerrett et al., 2016). Notably, findings regarding the role of outness (i.e., self-disclosure of one’s sexual orientation or gender identity) in SIB of LGBT individuals only partially supports this model: However, some studies found self-disclosure to be a protective factor for SIB, others found it to be a risk factor, especially for adolescents who acknowledge their sexual orientation at a young age (D'Augelli et al., 2005; Michaels et al., 2016; Rivers et al., 2018).
The present study examines SIB among LGBT individuals in Israel. Certain factors in the Israeli context may adversely influence LGBT individuals. Among these factors are dominant and politicized religious systems that promote prejudice against sexual minorities; army-related norms that highlight masculine stereotypes (Kaplan & Ben-Ari, 2000); and the small-town feeling of “everyone knowing everyone else,” making it acutely difficult for individuals to behave anonymously in any sphere, including the sexual domain (Kama, 2005). On the other hand, in the last decade, advanced legislation addressing the rights of sexual minorities in Israel has been viewed as considerably enlightened by Western standards (Kama, 2011). Studies on LGBT youth and young adults in Israel have revealed several mental health risk factors, such as lack of acceptance by self, friends, and family (Shilo & Savaya, 2012) and concerns of being victimized (Shenkman & Shmotkin, 2013), along with protective factors such as high openness to experience (Ifrah et al., 2018).
Several studies have highlighted the internal psychological pathways that may underline the association between social stigma and SIB, including hopelessness and depressive symptoms (Kaniuka et al., 2019), which are associated with LGBT individuals’ higher suicide risk. One of the known facilitators of hopelessness and depressive symptoms is the entrapment experience, defined as individuals’ perception that their adverse circumstances are uncontrollable and inescapable (Gilbert & Gilbert, 2003). Several studies have demonstrated the significant role of entrapment in facilitating suicidality in the general population, in adults as well as adolescents (Johnson et al., 2010; Shelef et al., 2016; Taylor et al., 2011). A recent study found that involuntary subordination, a psychosocial mechanism related to a sense of defeat and entrapment, was strongly associated with suicidal ideation among gay and bisexual men (Li et al., 2016), suggesting that entrapment could be a significant risk factor in this population. However, to our knowledge, no study has yet to examine the contribution of entrapment to suicidal ideation and behavior among the entire LGBT population.
Several interpersonal factors may also play a role in suicide risk among LGBT individuals. These factors are well described in the interpersonal theory of suicide (ITS). The ITS posits two dimensions of the proximal causal interactive risk factors for suicidal desire: perceived burdensomeness and thwarted belongingness (Van Orden et al., 2012). Each of these dimensions represents a specific perception of one’s interpersonal surroundings. Perceived burdensomeness implies that one’s very existence strains family, friends, and society. This view is a source of the notion that “my death will be worth more than my life to family, friends, society, etc.” (Joiner et al., 2009, p. 1). This construct comprises two parts: (1) beliefs that the self is so flawed as to be a liability for others, and 2) cognitions of self-hatred with accompanying feelings such as low self-esteem, self-blame, and shame (Van Orden et al., 2010). Experiencing these disturbing emotions is an antecedent of SIB and distress (Hill & Pettit, 2014). One may assume that when LGBT individuals feel themselves to be a burden or experience self-hated, their depression and attendant suicide risk may be dramatically increased. However, a few studies have documented this association in lesbian, gay, and bisexual populations (Baams et al., 2015; Hill & Pettit, 2012), the mechanism has yet to be examined in a study inclusive to all LGBT identities.
Thwarted belongingness is the experience of feeling alienated from others, emphasizing the painful sense of being outside the family, friends, and other valued groups (Van Orden et al., 2010). Thus, thwarted belongingness appears to capture deep interpersonal experiences and may explain the emergence of suicide risk. Among LGBT individuals, social isolation has been identified as a predictor of psychopathological symptoms (Díaz et al., 2001) and suicidal ideation (Hill & Pettit, 2012). A few studies examined the association of thwarted belongingness with suicidal ideation in LGB populations but yielded inconclusive findings. Some found thwarted belongingness to be a predictive factor to suicidal ideation (Cramer et al., 2014), whereas others did not find this association. Thus, as findings in this field are inconclusive and mostly disregard transgender individuals, further examination of the entire LGBT group is needed.
The Present Study
Our literature review suggests that personal, social, and stigma-related factors all have a role in contributing to suicide risk among LGBT individuals. While some of these factors have been examined, much remains for understanding the underlying mechanisms of suicide risk in this population. Moreover, as suicide risk among LGBT individuals relies upon the interaction of background, stigma-related factors, as well as psychological and social stressors, an integrative perspective is needed to connect the dots and understand how psychological, social, and cultural factors interact and lead to suicide risk.
Hatzenbuehler’s (2009) theoretical framework suggests a knowledge gap regarding the psychological processes mediating the pathway from social stressors to psychopathology in the LGBT population. To further understand these processes, our primary objective in this study was to examine an integrative cultural-social-psychological model of risk factors for SIB in the LGBT population. Thus, the specific aims of the present study were to understand the differences among the LGBT identities concerning suicide risk and the main risk factors of SIB. Furthermore, we aimed to shed light on the psychological processes that mediate the pathways linking social stigma and SIB in the LGBT population. A better understanding of these mediating psychological processes could facilitate tailored psychological treatment options for this population. Also, an enhanced understanding of these processes could help devise adjusted clinical risk evaluations for LGBT individuals in the hope of preventing suicide deaths in this at-risk population. To our knowledge, this is the first study to explore LGBT suicidal ideation and behavior in Israel. Thus, a further objective of this study was to identify unique characteristics of distress and SIB in the Israeli LGBT population, delineating the features of the entire LGBT population while examining the distinctions among gay, lesbian, bisexual, and transgender persons.
Operationally, we examined the relationship between three sets of variables among adults self-identified as LGBT: stigma variables, consisting of stigma-related life events, outness levels, and internalized stigma; mental pain variables, consisting of entrapment, depression, and hopelessness; and interpersonal variables, consisting of thwarted belongingness and perceived burdensomeness. Three main hypotheses were examined: 1. Transgender respondents will report higher levels of mental pain (i.e., depression, hopelessness, entrapment), interpersonal difficulties (i.e., perceived burdensomeness and thwarted belongingness), and SIB levels, compared with other LGBT groups. 2. Higher levels of stigma, mental pain, and interpersonal difficulties will contribute to higher levels of SIB. 3. Exploratory hypothesis: in order to find possible mediators between stigma-related variables and SIB, we will conduct an exploratory analysis with the aim to find the factors which may serves as mediators from the study psychological variables of entrapment, mental pain (i.e., depression and hopelessness), and interpersonal difficulties (i.e., thwarted belongingness and perceived burdensomeness). Our exploratory hypothesis was that stigma-related variables will facilitate higher levels of entrapment, higher levels of both mental pain and interpersonal difficulties which, in turn, will be related to higher SIB levels among LGBTs.
Method
Participants
The study sample comprised 473 participants, aged 18 to 76 (M = 27.59, SD = 8.81). Regarding gender identity, 48% identified as women, 32% as men, and 20% as having a non-binary gender identity. In addition, 15% of the participants identified as asexual.
Identity was measured by asking respondents to select from among various sexual orientations (e.g., homosexual, lesbian, bisexual, transgender), with an option to add additional clarifications in open text form if needed. For this study’s data analysis, the broad spectrum of identities was classified into four categories, including gay (20%, n = 93), lesbian (16%, n = 74), bisexual (23%, n = 111), and transgender (41%, n = 195). These four categories comprised the study groups. Twenty-eight participants (5%) did not choose any identity and thus, exclude from the analyses. Thus, the total sample included 473 participants. Eligibility criteria for this sample required participants to be over 18, identify themselves as part of the LGBT population, and provide consent to participate.
Measures
Stigma variables: stigma-related life events, outness, and internalized stigma
Internalized stigma
Stigma-related life events
Outness. Outness was assessed using the Outness Inventory (Mohr & Fassinger, 2000), measuring the degree to which the respondent’s sexual and gender identity is known by and openly discussed with various types of individuals (e.g., family, work peers). The scale comprises 11 items rated on a 7-point Likert-type scale, ranging from 1 (person definitely does NOT know about your sexual orientation/gender identity) to 7 (person definitely knows about your sexual orientation/gender identity, and it is OPENLY talked about). The mean scores of the final 11 items were calculated for each participant. Cronbach’s alpha coefficient for the current sample was high (α = .85).
Mental Pain Variables: Depression, Entrapment and Hopelessness
Depression. Depression was assessed using the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001), measuring the severity of depressive symptoms (e.g., “little interest or pleasure in doing things”) by the frequency of experiencing these symptoms. The scale consists of nine items rated on a 4-point Likert-type scale, ranging from 0 (not at all) to 3 (nearly every day). The mean scores of the nine items were calculated for each participant. Cronbach’s alpha coefficient for the current sample was high (α = .90).
Hopelessness. Hopelessness was assessed using the Beck Hopelessness Scale (BHS; Beck et al., 1974). The 20-item scale taps negative attitudes about the future (e.g., “the future seems vague and uncertain to me”) and is rated on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Total mean scores were computed for each participant. Cronbach’s alpha coefficient for the current sample was high (α = .93).
Entrapment. Entrapment was assessed using the 16-item Entrapment Scale (Gilbert & Allan, 1998). It measures the perception of feeling trapped and the desire to escape (e.g., “I am in a situation I feel trapped in”). Items are presented on a 5-point Likert-type scale, ranging from 1 (not at all like me) to 5 (extremely like me). The mean scores of the 16 items were calculated for each participant. Cronbach’s alpha coefficient for the current sample was high (α = .96).
Perceived burdensomeness and thwarted belongingness. Perceived burdensomeness and thwarted belongingness were assessed using the Interpersonal Needs Questionnaire (INQ; Van Orden et al., 2012). The 15-item INQ measures perceived burdensomeness (e.g., “These days, the people in my life would be better off if I were gone”) and thwarted belongingness (e.g., “These days, I feel disconnected from other people”), presented on a 7-point Likert-type scale, ranging from 1 (not at all true for me) to 7 (very true for me). Cronbach’s alpha coefficient for the current sample was high (α = .94 for each subscale).
Suicidal ideation and behavior. Suicidal ideation and behavior were assessed by the Suicidal Behaviors Questionnaire-Revised (SBQ-R; Osman et al., 2001). SBQ-R was used to assess lifetime and current levels of SIB. The SBQ-R presents four questions: (1) lifetime suicidal ideation or previous suicide attempts: “Have you ever thought about or attempted to kill yourself?”; (2) Frequency of suicidal ideation over the past 12 months: “How often have you thought about killing yourself in the past year?”; (3) current threat of making a suicide attempt: “Have you ever told someone that you are going to attempt suicide, or that you might do it?”; and (4) likelihood of suicidal behavior in the future: “How likely is it that you will die by suicide someday?” The four statements were presented on a variable 5- and 6-point Likert-type scale, with participants asked to indicate the frequency they engaged in the indicated suicidal behavior. We used the SBQ-R items in two different ways across the study. In the MANCOVA analysis, we used each item to assess lifetime SIB, the current levels of suicidal ideation, suicide communication, and future risk. In the bivariate analyses and the SEM model, we followed the scoring procedures recommended by Osman et al. (2001) to compute an overall estimate of suicide risk using all four questions, yielding scores ranging from 3–18. The SBQ-R total score yielded adequate psychometric properties and evidence for clinical utility in differentiating between suicidal and non-suicidal sub-groups in both clinical and nonclinical samples (Osman et al., 2001), as well as in military samples (Bryan & Clemans, 2013).
Demographic data. Demographics, tapping age, sexual orientation, education level, income, marital status, religiosity, and use of psychiatric medication were recorded.
Procedure
Data collection took place between January 2018 and April 2018 (duration of four months), following approval of the study by the [anonymized] Academic Center Ethics Committee. LGBT participants were recruited through multiple Facebook groups and pages addressing the LGBT community, as well as general Facebook groups, such as LGBT groups based in Israeli cities and neighborhoods and university student LGBT groups. Participants were also approached through anonymous LGBT forums in the Tapuz and GoGay web platforms. Participants were also recruited through LGBT organizations that distributed the survey, including Ma’avarim for the transgender community and the Israeli National LGBT Task Force.
All potential participants were informed of the risks and compensation procedures prior to participating. They were promised at the outset that questionnaire data would be completely anonymous, with no personal identifying information collected, with the option of withdrawing from the study at any time. All participants were sent a recruitment letter outlining the purpose, method, and procedure and were provided with the researchers’ contact details. Consenting participants were requested to sign an informed consent form, after which they completed the questionnaire online (using Qualtrics online survey software). After completing the survey, participants were provided contact information for mental health hotlines and several LGBT organizations if they were to experience distress from the survey questions. Following the completion of the survey, participants received a voucher for coffee and pastry (approximate value of US $5).
Data analysis
In the first step of the analysis, four multivariate analyses of covariance (MANCOVA) were carried out (with age, education level, and income as covariates) to examine differences between the LGBT identity groups in the study variables––suicide risk, mental pain, interpersonal, and stigma variables. These MANCOVA analyses were performed to reveal possible differences between the LGBT groups on the combination of aspects of each of these variables, as has been done in previous studies on sexual minorities (Shenkman et al., 2021; Warne, 2014). Scheffé’s post-hoc analysis was conducted to determine the source of differences, followed by a series of Pearson correlation tests between the study variables. To examine the mediational role of mental pain and interpersonal characteristics in the relationship between stigma and SIB, structural equation modeling (SEM) with observed variables (path analyses) was performed. To obtain a full representation of the model, a combined rule for model fitness was defined with the following accepted values: a non-significant chi-square test (χ2), the normed fit index (NFI) > 0.95, the comparative fit index (CFI) > 0.95, and root mean square error of approximation (RMSEA) < 0.06. Missing data were handled with a maximum likelihood (ML) module in AMOS software. Compared with conventional methods, such as arithmetic mean, listwise or pairwise deletion, the ML method has been recommended as optimal for computing missing data to avoid bias (e.g., Schafer & Graham, 2002). However, this method has limitations, such as non-robustness to non-normality and the assumption that all observed variables are continuous. The Statistical Package for the Social Sciences (SPSS, version 20.0 for Windows) and the AMOS software (version 20.0 for Windows) were used for all analyses. The level of statistical significance was set at p = .05.
Results
Socio-demographic characteristics
Participants’ education level varied between elementary school education (1.2%, n = 6), high school education (37%, n = 185), bachelor’s degree studies (26.3%, n = 132), bachelor’s degree (16.8%, n = 84), master’s degree (16%, n = 80), and doctoral degree (2.8%, n = 14). Participants’ self-reported income levels varied from very low income (61.5%, n = 308), low income (24.8%, n = 124), average income (8.2%, n = 41), high income (3%, n = 15), and very high income (2.6%, n = 13). Additionally, 26% of the participants reported being treated with psychiatric medications.
A MANOVA analysis was carried out to compare the demographics within different LGBT identities. We found significant group differences in age, F(4, 496) = 6.06, p < .001; income, F(4, 496) = 14.33, p < .001; and education, F(4, 496) = 7.65, p < .001. Regarding age, gay respondents were the oldest, followed by lesbian, transgender, and finally bisexuals. Gay respondents also reported the highest levels of income and education, followed by lesbians, bisexuals, with transgender people reporting the lowest education and income levels. These variables were used as covariates in the multivariate analysis of covariance. No other significant differences were found between the study groups in the other demographic characteristics.
Mental Pain and SIB Characteristics
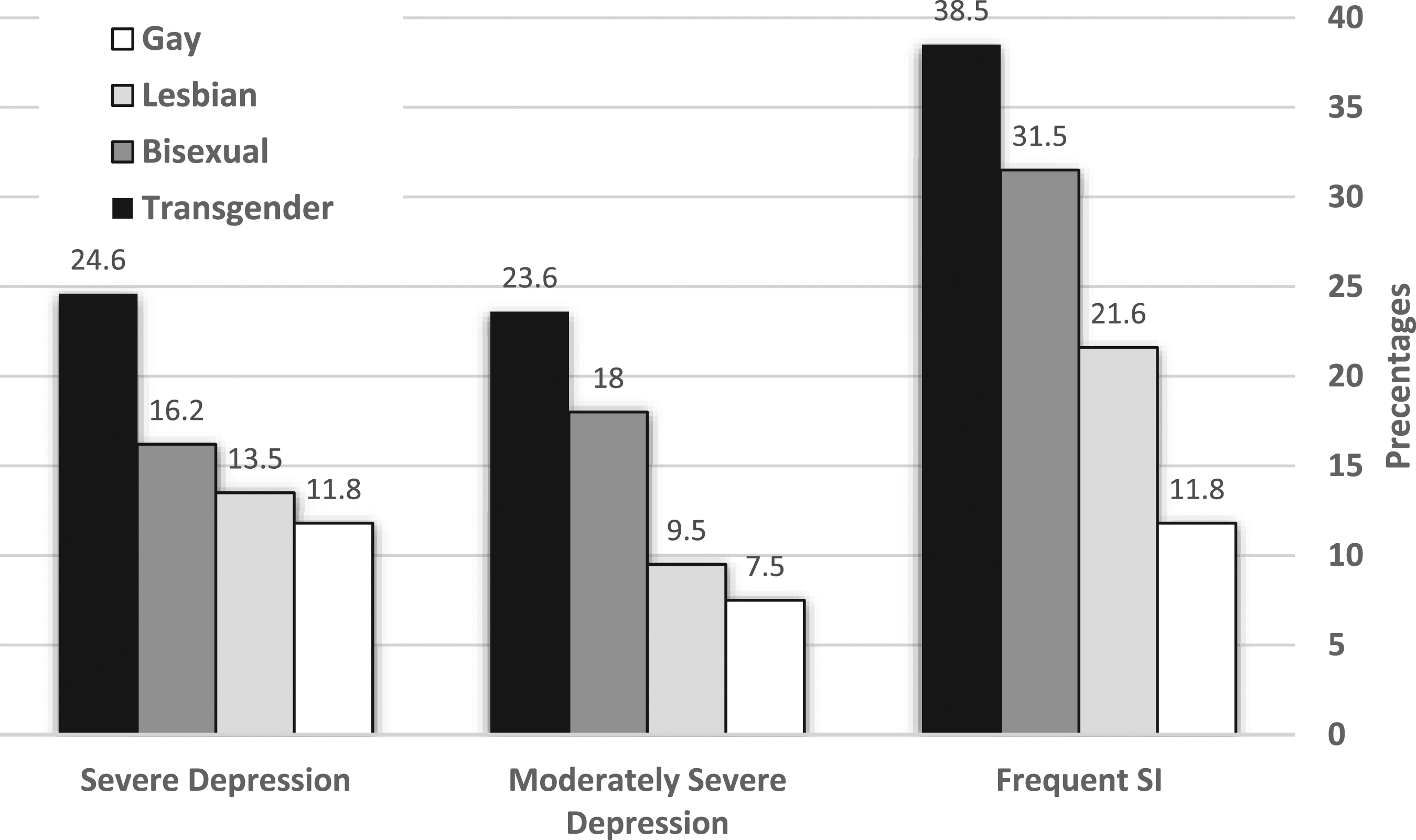
In general, as can be seen in Figure 1, 77.4% of the transgender respondents reported incidents of suicidal ideation throughout their lifetime, followed by bisexuals (69.4%), lesbians (50%), and gay respondents (41.9%). Regarding current suicidal ideation, as seen in Figure 2, 38.5% of the transgender people reported thinking about suicide often in the past year, followed by bisexuals (31.5%), lesbians (21.6%), and gay respondents (11.8%). Moreover, 39.5% of transgender respondents reported a lifetime suicide attempt, followed by bisexuals (36.0%), lesbians (29.7%), and gay respondents (16.1%). Regarding current depression characteristics, we found that moderately to severe major depression characteristics were experienced by 19.3% of the total sample. Transgender respondents experienced the highest percentage of severe depression, with 23.6% of them reporting moderately severe major depression symptoms and 24.6% reporting severe major depression symptoms (see Figure 2). Percentage of SIB Throughout Life among the LGBT Groups (N = 473). Percentage of Severe Depression and Current Suicidal Ideation among the LGBT Groups (N = 473). Note. SI = Suicidal Ideation.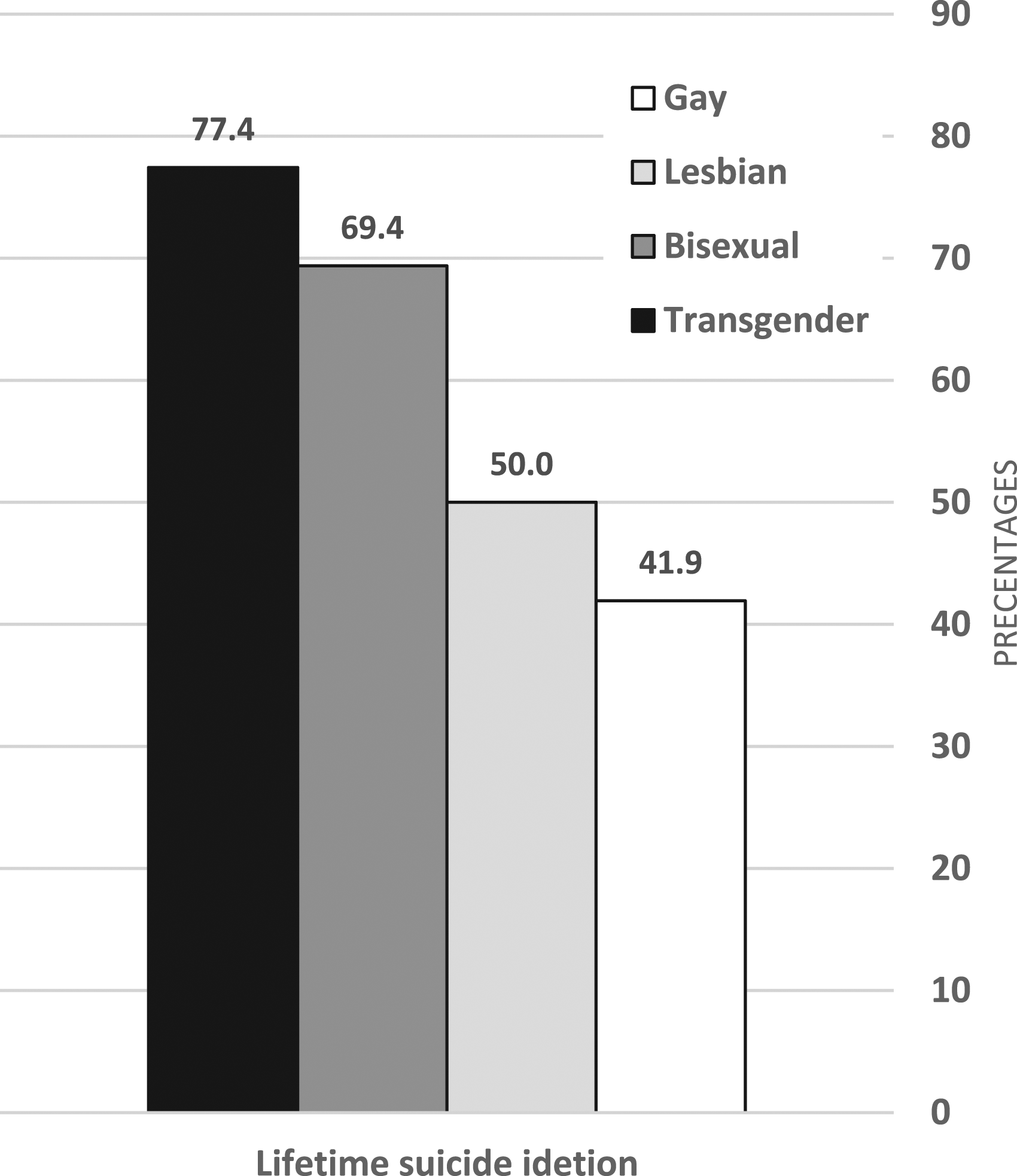
Differences Between the Groups on the Study Variables
Means, Standard Deviations, MANCOVA Results, and Post-Hoc Analysis of Dependent Measures in LGBT Identities (N = 473).
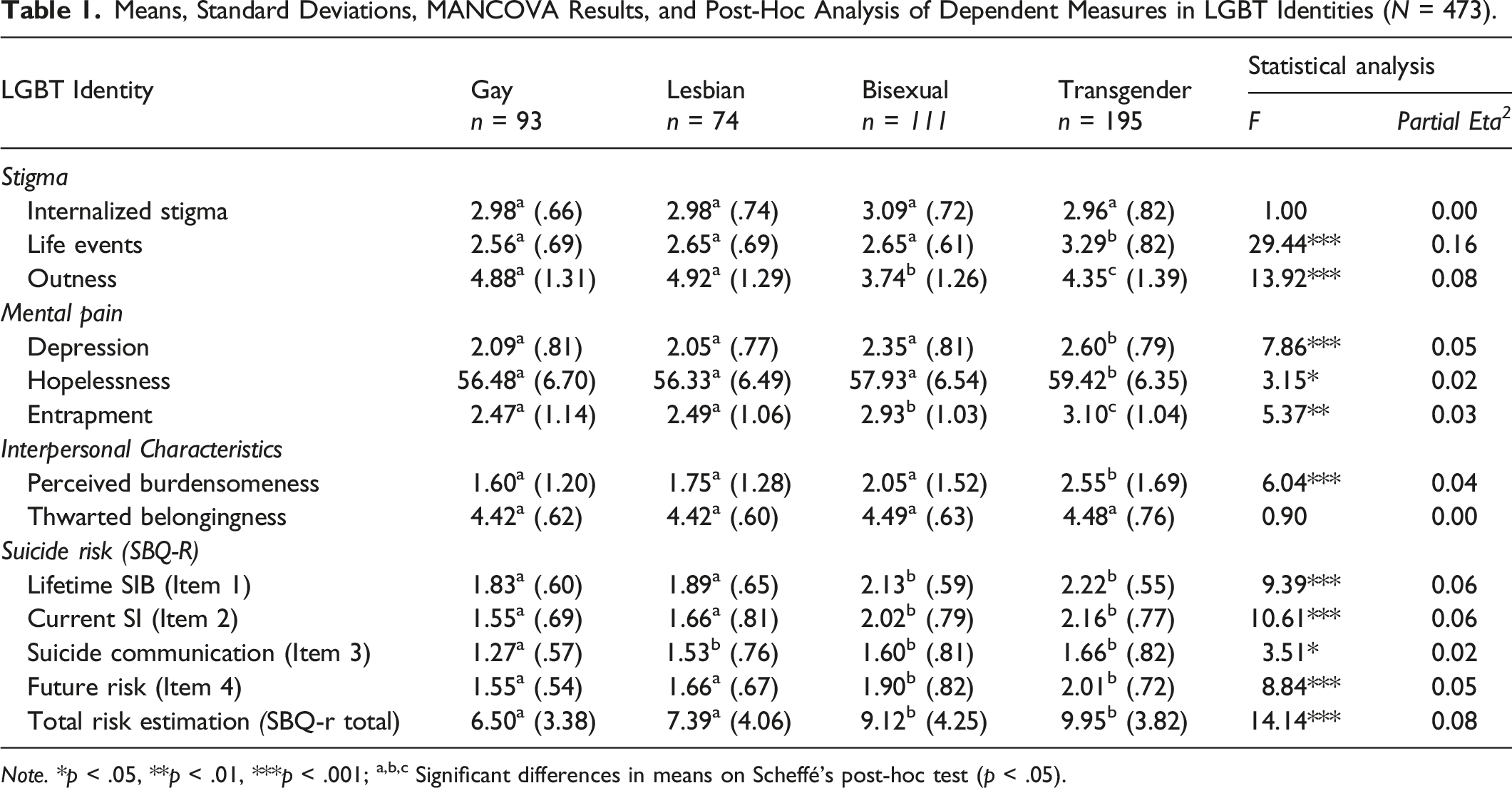
Note. *p < .05, **p < .01, ***p < .001; a,b,c Significant differences in means on Scheffé's post-hoc test (p < .05).
The suicide risk MANCOVA revealed a group effect of LGBT identity, Wilks’ F approximation (18, 1304) = 3.47, p < .001. Test of the between-subject effect revealed a significant group difference for lifetime SIB, as well as for current suicidal ideation, suicide communication, estimated future risk, and the total estimation of suicide risk. As shown in Table 1, the post-hoc analysis showed significant differences in all suicide risk variables, with bisexual and transgender respondents reporting higher suicide risk characteristics across most of the variables than gay and lesbian respondents.
The mental pain MANCOVA revealed a group effect of LGBT identity, Wilks’ F approximation (9, 1112) = 3.01, p < .001. Test of between-subject effect revealed significant group differences for depression, entrapment, and hopelessness. The post-hoc analysis showed significant differences in all measures, with the transgender group exhibiting the highest levels of depression, entrapment, and hopelessness compared with the other groups.
We also found a group effect of LGBT identity on interpersonal characteristics in a MANCOVA analysis, Wilks’ F approximation (9, 1129) = 2.37, p = .01. A significant group effect was found on perceived burdensomeness but not on thwarted belongingness. As shown in Table 1, a post-hoc analysis revealed that the transgender group reported higher levels of burdensomeness than the other groups.
Lastly, a MANCOVA analysis revealed a group effect on the stigma variables, Wilks’ F approximation (9, 1126) = 14.90, p < .001. Specific ANOVA tests revealed significant group effects on stigma-related life events as well as on outness. Post-hoc analysis showed that the transgender group reported significantly higher levels of stigma-related life events than all other groups. The post-hoc analysis also revealed that gays and lesbians reported the highest levels of outness, followed by transgender people, then bisexuals, who reported the lowest levels. No significant differences were found between the LGBT groups on internalized stigma.
An integrated model of the study variables’ contribution to suicide risk among LGBT identities
Preliminary Analysis
Descriptive Statistics and Bivariate Correlations Between Study Variables (N = 473).
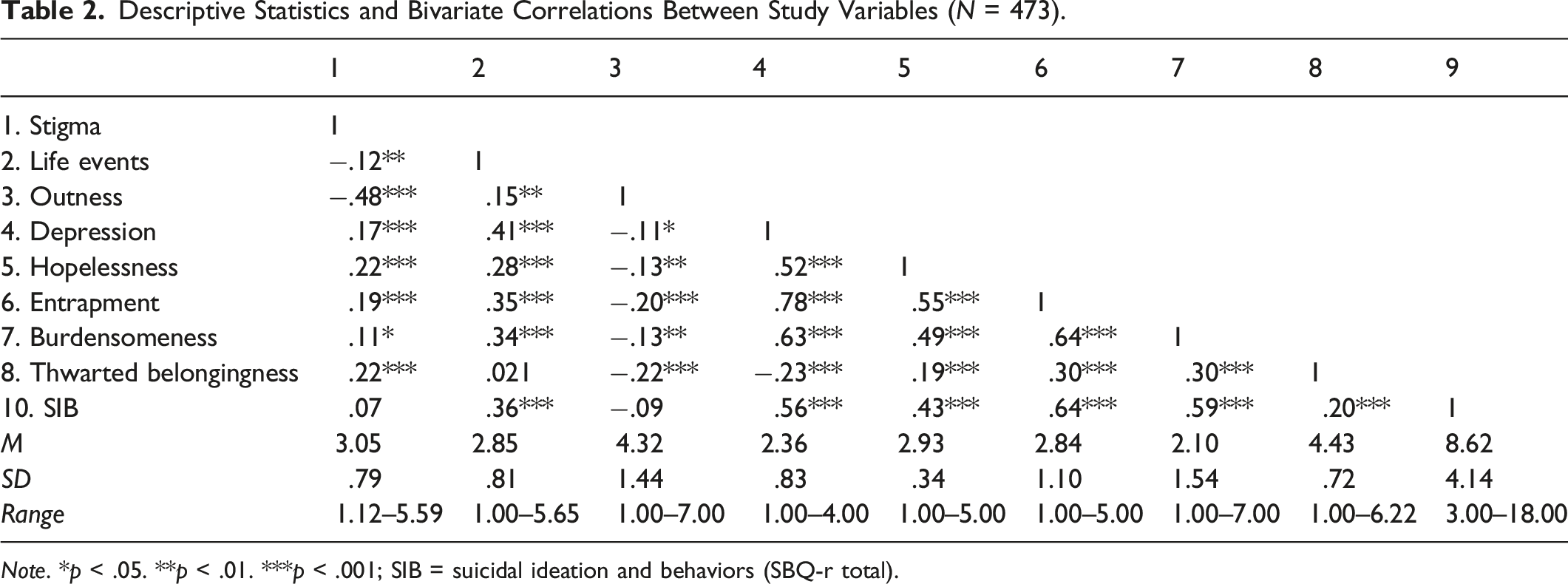
Note. *p < .05. **p < .01. ***p < .001; SIB = suicidal ideation and behaviors (SBQ-r total).
Structural Equation Modeling
To fully understand the mediational role of mental pain and interpersonal characteristics in the relationship between stigma-related life events and suicide risk (as measured by the SBQ-r), an SEM analysis was employed. The SEM analysis facilitated examining the nature of contributions and relationships between the psychological factors predicting suicide risk among LGBT respondents. The exploratory analysis included seven variables: stigma-related life events, outness, internalized stigma, entrapment, depression, perceived burdensomeness, and SIB. Hopelessness and thwarted belongingness were found to be non-significant as mediators in the first tested model and, thus, were not entered into the final model. The high intercorrelations between depression and hopelessness and between thwarted belongingness and perceived burdensomeness indicate that these two sets of variables tap proximal theoretical constructs; thus, only one of each set of variables was entered into the model. Importantly, however, a model containing depression and burdensomeness rather than hopelessness and thwarted belongingness was found to yield a considerably better fit with the data.
The model’s chi-square goodness-of-fit index presented an excellent fit with the data [χ2 (7) = 16.97; p = .02; CMIN/DF = 2.42; NFI = .98; CFI = .99; RMSEA = .03]. The statistically significant path coefficients are provided as standardized estimates in Figure 3. As shown in Figure 3, stigma variables contributed indirectly to SIB through entrapment, while stigma-related life events also contributed to SIB through depression and perceived burdensomeness. The analysis shows the substantial role of entrapment in predicting SIB among LGBT identity respondents. Entrapment contributes significantly to SIB, both directly, as a mediator for stigma variables, and indirectly, through depression and perceived burdensomeness. A Serial Mediational Integrated Model for Suicide Risk Among LGBT Individuals (N = 473). Note. Rectangles indicate measured variables, and small circles reflect residuals (e). Numbers above or near endogenous variables represent the variance explained (R2). Unidirectional arrows depict hypothesized directional links. Standardized maximum likelihood parameters are used. Non-significant paths are not presented.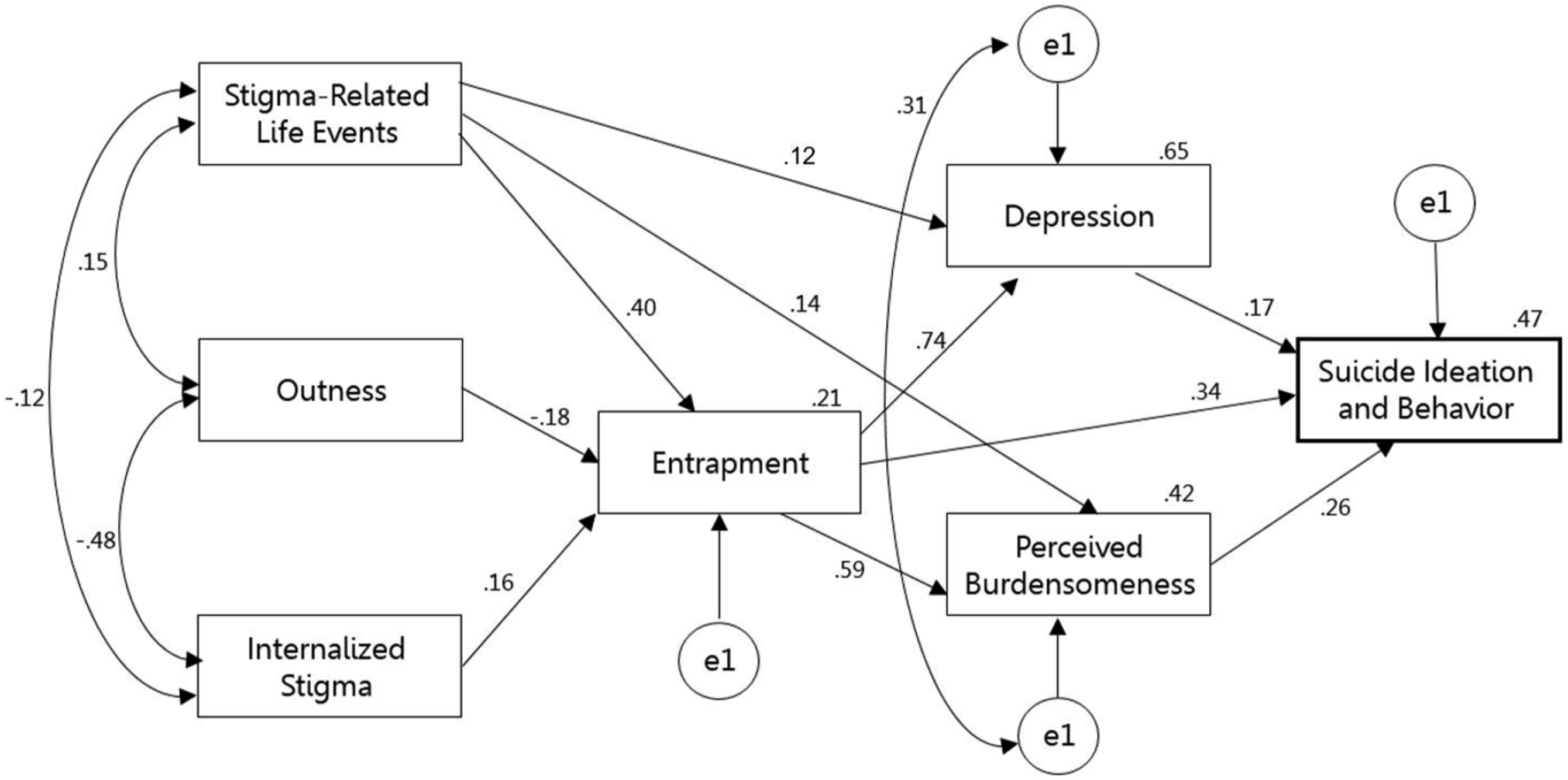
Discussion
This study aimed to understand differences in SIB levels among LGBT individuals in Israel and examine an integrative psychological model of risk factors in the LGBT population. To our knowledge, this is the first effort to understand the SIB characteristics of LGBT individuals in Israel and explore the psychological pathways and mechanisms of social stigma, mental pain, and interpersonal characteristics as facilitators of SIB in this population.
Before discussing this study’s findings, it is critical to note that, given the cross-sectional nature of the data derived from a non-representative sample having a high risk of self-selection biases, the findings should be interpreted with caution. For example, the directionality of the associations found among the variables remains undetermined. Thus, only future prospective studies with a representative sample would substantiate causal inferences regarding the associations among the variables.
In line with our hypothesis, we found group differences between lesbian, gay, bisexual, and transgender respondents in characteristics of SIB and mental pain. Transgender people reported the highest levels of depression, entrapment, hopelessness, perceived burdensomeness, and stigma-related life events relative to other LGBT identities. Bisexual individuals reported the second-highest levels of these variables. These findings are congruent with studies showing transgender individuals to be at higher risk for SIB (Bockting et al., 2005; Tebbe & Moradi, 2016) and with studies demonstrating bisexuals to be at higher suicide risk for SIB relative to gays and lesbians (Blosnich & Bossarte, 2012; Kann et al., 2016; Robin et al., 2002). Indeed, studies have shown that bisexuals may suffer from discrimination and prejudice from both the general population as well as from other sexual minorities (Zivony & Lobel, 2014), receiving less social support than their gay and lesbian counterparts (Shilo & Savaya, 2012). This social disadvantage may result in worse mental health and higher SIB relative to gays and lesbians.
Thus, our examination of the LGBT identities further highlights the transgender and bisexual populations as specific risk groups within an already vulnerable minority group. Notably, we also found that transgender and bisexual respondents presented comparable features of SIB on several measures, significantly differing from those reported by gay and lesbian respondents. Furthermore, following previous findings (Ifrah et al., 2018), the bisexual group presented the lowest levels of outness as compared with the other groups. Together, this pattern highlights the value of examining all LGBT groups rather than the traditional approach to LGBT study that has focused chiefly on lesbians, gays, and bisexuals as a single sexual minority population, while studying transgender respondents separately (Haas et al., 2010). In recent years, studies of the entire LGBT population have become more common (Bird et al., 2012; Mustanski & Liu, 2013). Findings from these studies are in line with the current findings, indicating that bisexuals and transgender people may have more shared features than previously thought, with both reporting relatively high rates of SIB.
As expected, we found that social stigma contributed to mental pain and SIB in our sample. Specifically, we found that stigma-related life events contributed to increased mental pain and distress, indirectly contributing to the manifestation of SIB. This finding is congruent with previous findings that related LGBT-phobic life events to SIB (Haas et al., 2010; Irwin et al., 2014). Our finding of life events’ predictive contribution indicates the critical role society plays in LGBT suicides, as the degree to which one is exposed to hostile, hurtful, and discriminatory societal treatment may dramatically affect their mental health and subsequently affect their desire to live. The individual could internalize this external stigmatization, and indeed, according to our findings, an internalized sense of stigma also predicted mental pain and SIB, in line with previous findings (Grossman & D'Augelli, 2007; Reyes et al., 2017; Skerrett et al., 2016). Seemingly, this means LGBT persons who internalize LGBT-phobic stigma and maintain negative thoughts and feelings toward their own identity are at graver risk of experiencing distress and suicidal ideation.
Exposure to social stigma could also result in these persons’ fear of disclosing their sexual/gender identity, thus remaining “in the closet” (low levels of outness). We found concealment could have a deleterious impact on mental health, as outness was negatively associated with mental pain and SIB. The more LGBT individuals discuss their identity openly, the less likely they will experience mental pain and SIB. Previous studies on the matter of outness have been inconclusive, as some found outness to be a protective factor for suicide, while others found it to be a risk factor, especially in studies conducted on youths living at home (Bouris et al., 2010; Michaels et al., 2016; Rivers et al., 2018). As our respondents were adults above age 18, our findings support studies revealing higher outness levels to be a protective factor for adults. In contrast to adolescents, who may suffer severe consequences following the disclosure of their sexual minority status (e.g., family rejection, homelessness), our findings indicate that for adults, outness contributes to better mental health and may serve as a protective factor against suicide.
In line with our hypotheses, we found that mental pain contributed substantially to LGBTs’ SIB. According to our findings, the association between stigma and SIB was mediated by the feeling of entrapment. In other words, social stigma predicted suicidality indirectly through the impact on mental pain and entrapment. We found that stigma-related variables, particularly stigma-related life events, predicted stronger feelings of entrapment in LGBT individuals. Subsequently, entrapment was linked to higher suicidal ideation, as death could be viewed as the only possible escape from severe mental pain (Williams, 2001). This finding is congruent with theoretical models specifying entrapment’s role in suicide formation in the general population (O'Connor et al., 2016; O'Connor & Kirtley, 2018) and with empirical studies in the general population that found entrapment to have a facilitating role in the path to suicidality (Littlewood et al., 2016; O’Connor & Kirtley, 2018; Teismann & Forkmann, 2017). Within LGBT studies, our results support and broaden the recent finding that involuntary subordination, a psychosocial mechanism related to defeat and entrapment, is associated with suicidal ideation among gay and bisexual men (Li et al., 2016). However, to our knowledge, the current study is the first to demonstrate an association between LGBTs’ feelings of entrapment and their suicidality.
The Role of Entrapment in SIB in the LGBT Population
The integrated motivational-volitional model of suicidal behavior delineates the critical role of entrapment in facilitating the initial motivation for suicide (O'Connor et al., 2016; O’Connor & Kirtley, 2018), and our findings suggest that these feelings of entrapment comprise a specific risk factor for the LGBT population. LGBT individuals commonly realize from a young age that they are a part of a minority group that is often shamed, victimized, and treated as inferior. This perception is particularly relevant to the Israeli context, where religion is influential and masculine stereotypes prevail (Kaplan & Ben-Ari, 2000), forming ample ground for anti-LGBT social norms. These social norms could generate feelings of humiliation and resentment toward their identity, along with efforts to hide it or even change it (e.g., conversion therapy; D'Augelli & Grossman, 2001; Meyer, 2003), all to ultimately find that they cannot escape who they are. LGBT individuals also often experience stigmatic life events, such as discrimination, harassment, and family rejection throughout life, promoting the belief that society’s negative perception and treatment of them comprise an inescapable reality (D'Augelli & Grossman, 2001; Mustanski & Liu, 2013). Subsequently, LGBT individuals, especially those who have experienced higher levels of LGBT-phobia around them, could eventually feel trapped within the identity to which they were born, as well as trapped in and unable to control society’s and their loved ones’ negative perceptions of it. Alongside elevations of depressive symptoms and other mental pain characteristics in this population, the feeling of being trapped in a painful situation with no ability to escape could trigger a line of thinking offering only two possible options: life with inescapable suffering or a state of no suffering through death (Williams, 2001). The framing of this dilemma can create the perception that suicide is the only bearable outcome (Taylor et al., 2011).
The importance of interpersonal difficulties as a mediator between entrapment and SIB among LGBT individuals
Beyond the contribution of mental pain and stigma to the formation of SIB, we found that interpersonal qualities contributed significantly to suicide risk in this population. Indeed, studies have demonstrated the key role of interpersonal connection and social support in LGBT mental health and suicide risk (Baams et al., 2015; Hill & Pettit, 2012; Wichstrøm & Hegna, 2003). Specifically, the exploratory model examined in this study revealed that the relationship between mental pain and SIB was mediated by perceived burdensomeness. However, entrapment predicted SIB directly, it had another indirect impact on SIB through its association with interpersonal characteristics and, specifically, with perceived burdensomeness: The more LGBT individuals feel inescapably trapped within their inner identity and social situation, the more they feel that their presence is a burden and an affliction to those close to them. This perception of burdensomeness increases the likelihood of suicidal ideation due to the individual’s belief that those around them would be better off without them (Joiner et al., 2009).
This latter finding is congruent with the interpersonal theory of suicide, specifying the important and empirically founded role of burdensomeness in forming suicidal ideation (Van Orden et al., 2008, 2010). It also supports studies on LGBT populations, showing that perceived burdensomeness has a facilitating role in forming LGBT suicidal ideation (Cramer et al., 2014; Hill & Pettit, 2012). Interestingly, thwarted belongingness did not significantly contribute to SIB in the SEM model. Given the equivocal nature of research in this field, this finding may validate several studies that examined the interpersonal theory in LGB populations and did not find thwarted belongingness associated with SIB (Baams et al., 2015; Hill & Pettit, 2012). However, it is noteworthy that in the current study, thwarted belongingness was found to correlate positively with SIB, and the non-significant results in the mediation model may be due to the correlation between thwarted belongingness and perceived burdensomeness (Van Orden et al., 2010; Levi-Belz & Aisenberg, 2021).
The perception of being a burden on loved ones could relate to lifetime experiences of alienation among LGBT individuals, who are often perceived as outsiders to social norms, different from those close to them, and, in many instances, subverting normative expectations, such as gender presentation and heterosexual marriage (Valentine et al., 2003). Consequently, family members of LGBT individuals frequently experience this identity negatively since family members now have to adjust their expectations and perceptions to a new situation, often dealing with their own stigmatic perceptions of LGBT identities (Valentine et al., 2003; Waldner & Magrader, 1999). Such experiences could promote LGBT individuals’ misperception that their whole existence is a burden on loved ones and that their lives are inconsequential. High levels of mental pain and distress in this population could further aggravate perceptions of burdensomeness, as the individual may begin to believe that a persistent negative mood or the subjective severity of problems may be too intense for loved ones to handle (Stellrecht et al., 2006). Aside from the dangerous perception that others would welcome the person’s death, perceptions of burdensomeness could also promote the idea that reaching out for support and assistance in times of distress would burden others (Stellrecht et al., 2006). These perceptions would likely lead to additional isolation, impairing interpersonal connections, and distancing the individual from possible resiliency effects against suicide.
More generally, our findings indicate that, given a state of entrapment and distress, interpersonal characteristics (i.e., perceived burdensomeness) could comprise some of the factors determining whether this distress escalates into SIB. Indeed, interpersonal skills could avert isolation and loneliness, factors that could exacerbate mental pain (Gvion & Levi-Belz, 2018). When a person feels as though they are alone, isolated within their pain, they are less likely to be exposed to an array of experiences, perspectives, and possibilities that other people might share regarding various strategies they adopted to cope with similar situations (Brown & Heimberg, 2001; Levi-Belz et al., 2014). Thus, the lack of interpersonal connectedness within a situation of mental pain could promote cognitions of “tunnel vision” (Orbach, 1994) and the feeling that no option remains besides suicide. Social contact would thus seem to be vital for LGBT individuals, as the experience of forming an LGBT identity may, at times, lead to social isolation (Garnets et al., 2003).
Limitations
Several limitations of this study should be noted. As noted, due to the cross-sectional and non-representative nature of the data gathered in this study, the directionality of the associations found among the variables remains undetermined. This shortcoming was partly overcome by using SEM analysis, enabling a deeper understanding of directionality among the study variables. However, prospective longitudinal studies are recommended for further research to safely infer causality in this field. Furthermore, the present study used path analyses with observed variables that could not control for measurement error. The final study model was built in an exploratory manner. Future studies that include latent variables in the SEM analyses may control for measurement error. Another important limitation is our use of a snowball sampling technique, which may have led to a sample not representative of the true extent of distress in the population. We partly addressed this limitation by including a relatively large sample of LGBT participants of diverse identities and characteristics. However, the present study did not address the various identities included under the transgender umbrella (e.g., possible combinations between different gender and sexual orientation identities among transgender individuals). Future studies could examine the current study’s model among different sub-groups among transgenders. The lack of a non-LGBT comparison group presents another limitation and calls for future studies to compare the reported model between the LGBT and the general populations.
A further limitation is that the data were obtained using retrospective self-report measures, which could introduce a well-known range of biases caused by factors such as mood-dependent recall, forgetting, cathartic effect, and social desirability. An additional shortcoming emerged from using self-report questionnaires, as fully estimating suicide risk is a clinically complex process. However, highly validated measures of suicidal ideation and behavior were used to address this limitation. Moreover, notwithstanding the common use of MANCOVA analysis in LGBT studies (e.g., Shenkman et al., 2021) and its theoretical justification in the present study (Warne, 2014), this analysis may have statistical limitations that should be considered in future studies (Huang, 2020). Lastly, due to the large samples required in SEM analyses, the present study did not compare the model fit between the LGBT groups (Kyriazos, 2018). Future studies should recruit larger samples for each LGBT group to compare the model fit between the groups.
Conclusions and clinical implications
Our work highlights the high suicide risk levels for SIB in Israel’s LGBT community. While this is a non-representative study, we can still recommend some steps that can be taken to enhance suicide awareness and prevention in this population. Designing intervention programs tailored to LGBT individuals in Israel would facilitate averting suicide behavior and suicide in this population, specifically among bisexuals and transgender people.
Our findings also suggest that when treating LGBTs in suicide crises, it may be advisable to recognize and assess their levels of entrapment and interpersonal difficulties, such as perceived burdensomeness, as they may comprise some of the underlying psychological mechanisms that contribute to suicide risk. Thus, in line with these recommendations, interventions targeting feelings of entrapment may be a promising direction in treating this population. For example, cognitive-behavioral therapy (CBT) and mindfulness-based cognitive therapy (MBCT) interventions have both been found to be highly effective in reducing suicide behavior, partly by addressing entrapment and other related experiences such as hopelessness (Tarrier et al., 2008; Williams et al., 2006).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “Path to life” association under Grant [No. 122] in memory of Dafna Westreich.