
Abstract
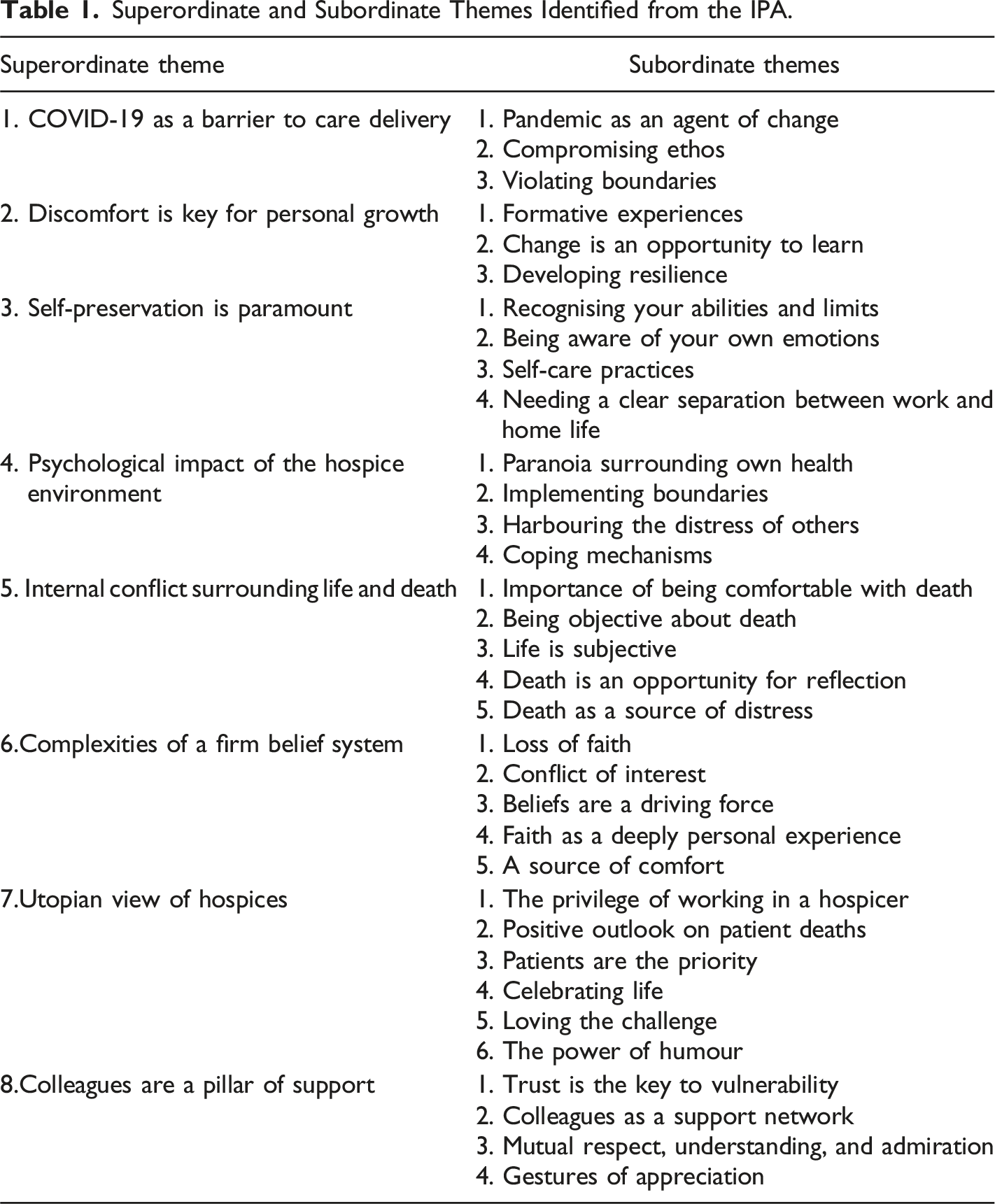
Current research surrounding the experiences of hospice staff is significantly underdeveloped. Additionally, the stigmatisation of death in Western society has formed delusions of hospice care amongst the general public. These findings gained an insight of the lived experiences of six hospice staff across England and Wales, through an interpretative phenomenological analysis. Eight superordinate themes were identified; ‘COVID-19 as a barrier to care delivery’, ‘Discomfort is key for personal growth’, ‘Self-preservation is paramount’, ‘Psychological impact of hospice environment’, ‘Internal conflict surrounding life and death’, ‘Complexities of a firm belief system’, ‘Utopian view of hospices’ and ‘Colleagues are a pillar of support’. All narratives shared overarching themes on growth, acceptance, and morality. These findings have future implications at the organisational level, identifying areas for adjustment for employee wellbeing. Furthermore, this may also educate aspiring end-of-life care staff in preparation for the reality of hospice environments.
Introduction
A hospice is where medical, spiritual and psychological professionals provide care to ameliorate the suffering of patients with life-limiting illnesses (Casarett & Quill, 2007; Linton & Feudtner, 2008). Palliative care aims to relieve unpleasant symptoms throughout a patient’s treatments, whereas end-of-life care is given in the later stages of a terminal illness and is crucial in providing comfort during a patient’s final stages of living (Hui et al., 2013; Izumi et al., 2012). Such care is motivated towards delivering emotional support for the patient and their loved ones, whilst managing their physical deterioration, providing them with a graceful death (Izumi et al., 2012). People may be perplexed by those entering a death-oriented career, but hospice staff believe this general aversion and fear of death is due to a lack of understanding (Goranson et al., 2017; Bell, 2020). Hospice care is widely standardised in Western society with approximately 25,000 UK residents being supported annually, which is continually increasing and creating strain on resources due to an ageing population (Hospice UK, 2015; Walker, 2018). Understanding the nation’s dependency on such care, this study will be focusing on hospice staff across the UK.
The literature presents the significant impact of stress on hospice staff health, wellbeing, and consequently their ability to deliver such crucial care. Their workplace environment needs to be thoroughly understood in order to develop support for staff, and enabling them to thrive in a field that depends on their nurturing. Existing qualitative research has used thematic or discourse analyses to identify broad themes within the staff experiences. An IPA has previously explored how palliative nurses attach purpose to their role (Smith & Shinebourne, 2012; Ablett & Jones, 2007). However, Ablett and Jones (2007) suggest that further qualitative research is needed to allow hospice employees to discuss their experiences and coping mechanisms. Therefore, this study aims to support the underdeveloped research by engaging with a deep, meaningful analysis of hospice staff experiences, contributing to a greater understanding of their livelihoods, needs, and stressors in their workplace. The study objectives were to take a qualitative stance, conducting individual semi-structured interviews on hospice staff from across the UK. An Interpretative Phenomenological Analysis (IPA) has been used on a discreet sample of six participants to determine themes surrounding how they make sense of the experiences, strains, and challenges of this niche phenomenon (Smith & Shinebourne, 2012). The findings will be beneficial for educating the general public, who may be curious and would like an insight to some staff experiences of hospice work. Additionally, this study may inform organisational psychologists to produce interventions, or amend policies to improve the livelihood of hospice workers. From this, the research question being posed will be asking ‘how do hospice staff make sense of, and adapt to working in a hospice environment?’
Literature Review
A study found hospice social-workers that demonstrated concrete beliefs about death showed lower levels of self-reported anxiety, and were more likely to continue or expand on their roles within a hospice (Quinn-Lee et al., 2014). Deci and Ryan’s (2012) Self-Determination Theory suggests those individuals remain positively committed to their field due to an innate need for personal development, satisfying internal psychological own goals. Additionally, Pezet (2018) states that when an individual establishes answers to the foundations of their needs, including existential questions, they begin to satisfy their internal goals. Subsequently, hospice carers may remain motivated within their careers as their experiences may contribute to their personal belief systems surrounding death (Sinclair, 2011). Additionally, Herzberg’s Two-Factor Theory implies that a workplace has ‘motivators’ and ‘hygiene factors’ (workplace expectations which may reduce motivation when not present) that account for the motivation to continue a career in hospice care (Herzberg et al., 1966). Interestingly however, contingency theories grounded in behaviourism suggest job satisfaction and productivity is situation dependent, rather than believing in set methods to best organise the workplace (Hamann, 2017). Such theories explain the correlation where the more concrete their belief systems surrounding death, the more comfortable and resilient end-of-life staff are when maintaining hospice careers.
A National Health Service (NHS) survey identified that healthcare staff exhibited a greater prevalence of mental illness than other areas of employment (Wall et al., 1998). Moreover, a correlational study highlighted a relationship between psychological burnout, with a decrease in quality of care delivered; treatment, communication, and support (Kennedy, 2005). Zimmermann’s (2012) discourse analysis found that caring for those younger than themselves or those they could personally resonate with, was a large contributing factor to the distress of palliative care workers. Alongside this, staff have also discussed the internal conflict they face within the early stages of their career; being confronted to think of their own mortality (Crawford et al., 2008).
Hospice carers are regularly confronted by change and pressure to provide sincere end-of-life care, which has been noted to cause physical and psychological exhaustion (Keidel, 2002). Interestingly, Abraham (2020) reported the acceptance of stress as being part of a typical working day within care-based roles. Heavy workloads, understaffing, and regular changes in unclear policies, were all emphasised as more stressful than their employment role itself (Abraham, 2020). A survey on 547 hospice staff in Minnesota found a relationship between workplace stress and symptoms of compassion fatigue and psychological burnout (Whitebird et al., 2013). Supporting this, further quantitative literature has shown that organisational changes lead to a decline in employee wellbeing and physical health (Papadopoulos et al., 2010). A deterioration in physical health as a result of stress is often exhibited through high blood pressure, frequent headaches, and digestive sensitivity, which may lead to more serious implications such as a heart attack or stroke (Larzelere & Jones, 2008; VanItallie, 2002). The detriment of this issue can be explained through Maslow’s (1943) hierarchy of needs theory, where an individual must satisfy the lower-level needs such as their health, before striving for higher needs such as recognition, and the ability to reach their full potential. In the context of hospice employees, their psychological and physical demands must be fulfilled before they feel confident to work effectively. Not only to reduce risks to physical health and burnout, but this is also necessary for them to have the capacity to provide their best possible care. Supporting this, a systematic review identified that the stress experienced by hospice carers was predominantly due to inadequate resources from the organisation for social, emotional, or psychological support (Vachon, 1995). Though the plethora of quantitative studies provides data where inferences can be drawn, the field requires more qualitative research in order to gain a deeper insight and thorough understanding of staff experiences.
Method
Design
This study took a qualitative approach, conducting semi-structured individual interviews that included a series of predetermined open-ended questions. An IPA was used to analyse the transcripts.
Participants
The participants were six hospice employees over the age of 18, with no set gender criteria as it was not relevant to the study. As part of the inclusion criteria, participants needed to be employed (not volunteering) at a hospice, and have a minimum of 1 year’s experience working directly alongside end-of-life/palliative patients.
Participants were recruited by opportunity sampling through emailing hospices across the UK, attaching a poster advertisement and requesting their human resources department to forward it to the relevant staff. This would directly invite potential participants to contact the researcher to express an interest in taking part. Participants were then chosen according to their experience, in relevance to the duration of their employment in hospice settings.
Methodological Theory
Interpretative Phenomenological Analysis grants the opportunity for a deeper understanding of lived experiences, so a small sample size between four to six participants is adequate (Eatough & Smith, 2008; Baker & Edwards, 2012). Interpretative Phenomenological Analysis takes an idiographic approach; focusing on the unique phenomenon experienced by the participants and providing comprehension that would not be achieved through other methods (Tuffour, 2017). This is the most appropriate methodology for the study as it explicitly focuses on the individual experiences, as opposed to generalising the findings (Reid et al., 2005). Moreover, IPA takes a double hermeneutic approach; the qualitative researcher is making sense of the participant’s efforts to interpret and make sense of their own phenomena (Shinebourne, 2011).
Data Collection
Semi-structured interviews open the research question to wide interpretation, enabling the participant to cover areas of interest which may not have been considered, due to their inclusion of follow-up and open-ended questions (Smith, 2017; Kallio et al., 2016). Subsequently, risk of bias in potentially forming leading questions may need to be addressed during analysis. Smith (2004) suggests that the flexibility of a semi-structured approach would by highly effective in sourcing a rich dataset from a niche sample size; providing further justification for using this technique in this study.
Procedure
When determining the research question, a review of the literature identified a significant lack of qualitative studies surroundings the thoughts and feelings of hospice staff in their work environment. An interview schedule was formulated and then submitted alongside complete ethical documentation for approval. Upon approval, the researcher began recruiting participants through emailing hospices with a pre-approved recruitment message and poster. Due to the COVID-19 pandemic, there were no in-person interactions between researcher and participant. Prior to online interviews, participants were sent copy of the participant information sheet and consent form which they needed to electronically sign and return to the researcher; reminding them of the study, their involvement, and their right to withdraw. Each online interview lasted between 45 and 60 minutes at an agreed date and time of the participant’s convenience, and concluded with an additional reminder to participants of their right to withdraw their data up to 6 weeks after the interview had taken place.
Ethical Considerations
In accordance with the British Psychological Society (BPS) guidelines (2017), rigid ethical considerations were implemented to ensure the ethicality of the study. A complete ethics application had been submitted for approval prior to recruitment.
Ensuring participant anonymity and confidentiality, participants decided their own pseudonym which would be used throughout transcription and when presenting the analysis. Any names of individuals/locations would be deleted during transcription so participants/organisations would not be identifiable from the dataset. However, anonymity cannot be entirely guaranteed since the participants would need email the researcher to request for their data to be withdrawn.
Confidentiality was ensured by having all data being handled by the researcher, with any audio/transcript/consent form documents being stored on a password protected university OneDrive account. However, these files would be made available exclusively to the researcher’s dissertation supervisor, by sharing them in a OneDrive folder. Any audio/video recordings were permanently deleted from the password protected recording device once the files had been transferred to the OneDrive account.
Prior to, and after their participation, all participants were reminded of their right to withdraw their data up to 6 weeks after their interview date. Participants were also reminded that they could terminate the interview at any point if they wished to do so without penalty. The researcher also had this ability to terminate the interview. Abiding to the BPS guidelines and maintaining valid ethicality, the researcher provided a list of resources on the participant information sheet and was able to signpost participants to the relevant support once the interview had concluded. In accordance with the government and university guidelines, the study was carried out virtually, and so eliminating the risk surrounding the researcher’s lone worker policy.
Data Analysis
The IPA procedure eventually leads to a hermeneutic and idiographic analysis of each transcript (Hefferon & Gil-Rodriguez, 2011). Initial descriptive coding identified topics of significance, as displayed by the extract in Figure 1. From this, interpretative codes were then developed and noted within another column of the transcript (see Figure 1). With this data, emerging subordinate themes were established and clustered in discreet groups to distinguish superordinate themes. The subsumption technique was used where individual interpretative codes were linked together to form subordinate themes, which were then clustered according to relativity to form an overarching superordinate theme. The researcher used the novel technique of using sticky notes for clustering themes, which is a method that has been commended by previous literature to visually engage with the data (Christensen & Friis-Olivarius, 2020). Transcript analysis table with descriptive and interpretative coding columns.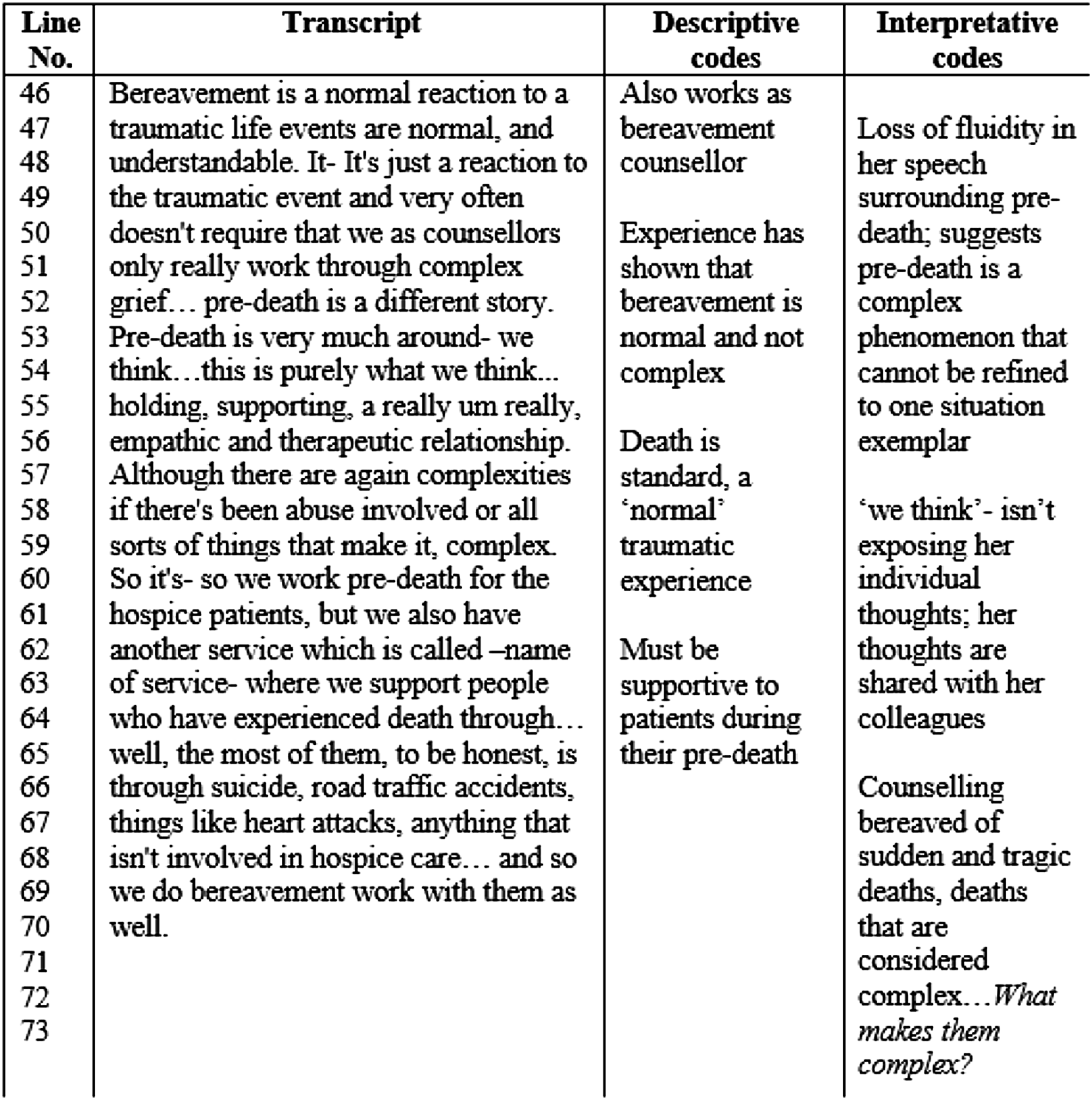
Reflexivity and Validity
An adaptation of the Gibbs (1988) reflective cycle was utilised by the researcher in a reflexive journal, providing the opportunity to enhance the rigidity and ethical delivery of the study (Smith, 1999). Conducting a literature review, maintaining a journal, and conversing with the research supervisor ensured the validity of this study. This provided opportunities to explore different perceptions and give a profound insight into the research topic (Vicary et al., 2016). Conversely, complete transparency and recorded thoughts have been partially compromised to safeguard confidentiality and protect the anonymity of participants/organisations involved.
Qualitative research results in the researcher having a direct impact on the dataset, through their influence during interviews and analysis. Though having experience, the researcher may not be strongly proficient in delivering the interviews, which may have had an impact on the quality of the dataset. However, the semi-structured approach enabled the researcher to flexibly ask questions that may conjure longer and elaborative responses from the participants. The interviews were planned to last no longer than an hour. This decision had been informed by the relevant literature that suggests an hour would be most effective in collecting enough substantial data for an IPA (Larkin et al., 2019).
Analysis
Superordinate and Subordinate Themes Identified from the IPA.
‘Discomfort is Key for Personal Growth’
This theme was central to each of the participants’ narratives. Participants conveyed these formative experiences of personal loss or illness as a catalyst for their epiphany to change. Subsequently, this personal growth proved to be fundamental in their abilities to adapt and thrive when working within the hospice environment. Within this theme, there are three subordinate themes that will be discussed; ‘formative experiences’, ‘change is an opportunity to learn’ and ‘developing resilience’.
Though all participants gave accounts of how their personal grief served as inspiration for their career path, Rosie provided a deep insight on the impact of losing her father and how it shaped her perspective; ‘My dad died in this hospice…it helped me knowing what I knew, but having someone close to me die also helped me in my work with people, because you get it’. (Rosie, 221–225)
In stating this, Rosie demonstrated the multi-faceted influence that a personal loss had on her, and its unconventional benefits. By expressing how these experiences have ‘helped’ her, there is a sense of symbiosis between herself and her workplace as she has been able to reflect on client experiences for guidance in her own struggles. Additionally, Rosie maintains that this experience has provided her with an authentic sense of empathy towards her client circumstances as she can relate to their distress. Though Rosie clearly highlights the distress her father’s death caused her, it seems she has optimistically taken away the lessons she gained from the trauma. However, an interpretation by Funk et al.(2017) suggests that such optimism may be a means of self-preservation amongst end-of-life staff, who are unable to communicate their grief due to the restrictions against expressing emotions for the sake of professionalism. Though Molly depicts an understanding of her growth as a result of her personal distress, she presents a more morose outlook on her personal grief; ‘I don’t think I’m any happier for it. I think I would’ve been happier if I hadn’t gone through bereavement myself, but yeah… Life is more meaningful for me now though’. (Molly, 624–627).
The repetition of ‘think’ highlights how highly reflective her formative experiences have made her, though the sorrowful undertone suggests that Molly believes that ignorance would have been bliss; though necessary for her growth, her wellbeing has been indefinitely compromised.
The ability to adapt to change was also widely discussed across all interviews. The superordinate theme of ‘COVID-19 as a barrier to care delivery’ depicts the negative impact change had on the hospice staff participants, predominantly due to the changes at the institutional level in accordance with the national lockdown restrictions. Referencing prior to the pandemic, numerous participants indicated that they had become accustomed to constant change and had developed their own organisational skills to maintain a sense of stability within their working day. Leigh talks of their willingness to take change in their stride; ‘I like to sort of embrace change, I think that’s who I am as a person. I appreciate the challenge and how it’s not a bad thing’ (Leigh, 146–149).
Leigh alludes to her belief that her enthusiasm towards accepting change is an innate quality, and her appreciation for the struggles further highlights the power of a positive outlook. Through recognising the significance of optimism and positive emotion within employees, the Appreciative Inquiry Model encourages the perception of change being an opportunity to learn within the workplace (Cooperrider & Whitney, 2001). Reinforcing the narrative of using change as a chance to learn, Leigh reiterates; ‘The people we are looking after are changing, so I think it’s important that we change with them’. (Leigh, 154–157).
Leigh recognises end-of-life care as a fluid situation, which suggests the importance of being accommodating when working in palliative care as a relatively new sector of the healthcare industry (Miller et al., 2010). Ultimately, Leigh’s experience can be seen as an example of how the strain of change can be used to her advantage, and equip her with knowledge to carry through her career path.
Interestingly, distressing experiences within the hospice environment also enabled participants to develop resilience as part of their personal growth. Again, this was an experience shared among all participants where they continually demonstrated a sense of sorrow for patient deaths. However, few gave deep emotional accounts of their first patient death and could recall the turmoil they felt. In her interview, Rosie’s talk suggests a baseline resilience which, as a hospice employee, she experienced early in her career; ‘I remember one of my first clients going home at the weekend and I literally cried all weekend, because I just couldn’t- I was just so so so sad’. (Rosie, 297–300).
This extract shows Rosie’s struggle with emphasising the extent of her initial distress and illuminates the power of client deaths. Rosie later addresses how she would not have the capacity to mourn every patient death, and identifies this distress as essential in her process of developing resilience to grow into her role. This supports the literature that suggests that resilience is developed after continual exposure to trauma (Francis & Bulman, 2019).
Furthermore, Robin can reflect on his years of experience and illustrates how this discomfort was a mediator in his personal growth, which was key for him to remain competent at work; ‘Not uh- being completely robotic, but being emotionally resilient and responding to patient and families’ emotions appropriately…but I don’t think you can get too tied up in that because it would just completely drain you’. (Robin, 180–187).
This perspective shows the progress of his personal development, acknowledging that it was necessary to become less affected by the narratives of his clients. Robin has established the niche grey area where himself and his colleagues must be mindful of self-preservation, whilst simultaneously delivering the quality of care that aligns with their moral obligations. Coinciding with the findings from Black and Honeyman (2020), the participants of this study shared the importance of finding a boundary between resilience and complete dissociation when preserving their personal growth journey, as a palliative care professional.
‘Utopian view of Hospices’
Within this ‘utopian view’, participants all communicated their lived experiences positively, though each participant presented their individuality by having appreciation for different aspects of their work life. Its subordinate themes create a flowing narrative surrounding honour and enthusiasm within their sense-making of their work environment, fortifying the extent of the public’s misconceptions surrounding hospice care (see Table 1).
‘Celebrating life’ is a concept that has been clearly portrayed among all transcripts, founded on the realisation where participants have used client experiences as a tool of reflection. By witnessing the harsh realities of their clients’ terminal diagnoses, participants have reported a shared epiphany of needing to appreciate the fortunes within their own lives. Kim and McGill (2018) stress the importance of how affirming the detriment of others’ situations enables a person to be grateful for their own circumstances. In celebrating life, these participants have collectively demonstrated the skill of placing a positive twist on their personal narratives. Participants indicated that this is a common phenomenon within their colleague networks and with this layer of relatability, Alex states; ‘There’s a very unique camaraderie with working in a hospice that you probably don’t get in many other places’. (Alex, p.222–225).
The use of the word ‘camaraderie’ suggests how these communal experiences create a safe space and common ground in which end-of-life/palliative care staff are being brought closer together. This has also been elaborated on in the other superordinate theme of ‘colleagues are a pillar of support’ (see Table 1). The sense of inclusion within this ‘camaraderie’ supports Alex’s utopian view of his workplace. Supplementary to this, previous research has identified that such exclusive ‘in-group’ experiences are a key mediator in strengthening connections with others (Patel et al., 2021). This agrees with the previous literature which identified a strong positive correlation between good colleague relationships and wellbeing (Zhai et al., 2020).
‘The power of humour’ also became a prominent subtheme across participants who continually reiterated its role and benefits within the workplace. Corroborating with this, Robalo Nunes et al. (2018) acknowledged the significant relationship between dark humour and overcoming grief, identifying humour as a widely used coping mechanism in end-of-life care. Supporting this, Rosie captures its efficacy; ‘With the humour though, it’s more kind of comments that we make that are really inappropriate. Oh god… But they’re funny because it diffuses sometimes a really difficult situation’. (Rosie, 350–354).
In stating this, Rosie recognises that the arguably poor taste of humour is necessary for herself, and her colleagues to use when comprehending the morbid reality they are faced with.
Contrary to this need to get along with colleagues, Leigh states; ‘I’m…I’m naturally a rather introverted person. I am very self-sufficient um, so I think my need to go and get along with people differs, I guess, from other people’. (Leigh, 528–532)
The following suggests she gains her sense of contentedness through different means aside from colleague interactions. Leigh provides an interesting contrast to the consensus of the other participants, as she implies that her introverted nature makes her less dependent on social support than the rest. Though the other superordinate theme of ‘colleagues are a pillar of support’ illuminates the importance of positive interactions within workplace dynamics, introverts have also been presented as an asset to work teams for not being emotionally reliant on their peers (Chang, 2020). Rather than focusing on the support network of her peers, Leigh discussed the extent to which she places her patients on what seems to be a metaphorical pedestal, for example; ‘You’re working in a way that actually… you’re trying to bring elements of- a little bit of control back to that person’. (Leigh, 269–273).
Through this, Leigh has captured the need for understanding within the hospice, as her ability to appreciate the perspective of her clients enables her to acknowledge the importance of what she is doing for them. This experience teaches a way of thinking from a staff perspective, exemplifying the qualities they need in forming strong connections with terminally ill patients. Elaborating on this, Robin uses religious imagery in stating ‘It’s almost like giving a heaven for the few’. (Robin, 70–71). This statement illustrates Robin’s recognition of the impact of his work and in referring to ‘heaven’, he alludes to wanting to provide the ultimate standard of care. This agrees with the body of literature that has previously depicted the innate need to care for patients, and how having a genuine concern was key to lasting careers within hospice environments (Al-Abdin et al., 2020).
Adding to this nurturing tone, Leigh states; ‘Sometimes I think actually it’s a positive thing, when you witness someone suffering you know, you can see the change of the patient and their family when actually –that release of death is there’. (Leigh, 788–793).
Leigh’s talk provides a sense that she anticipates a client death as a liberating endpoint for herself, the client and their loved ones. Similarly, Ceri recalls a positive client-death experience, in which his tone is almost celebratory; ‘There was a lot of banter going on and it was quite fun. And again, there’s another piece of spiritual care for somebody’. (Ceri, 323–325).
In relevance to the research question, this perspective suggests that through interpreting their workplace surroundings with a positive lens, the end-of-life staff can make sense of these regular deaths. It could be inferred that this is an adaptive trait that they have gained by developing their world views and becoming emotionally hardened (Trylińska-Tekielska, 2020). Interestingly, surrounding research has expanded on this, and found that family of the bereaved perceive the death as a relief from the distress of watching a loved one’s deteriorating condition (Bainbridge et al., 2018).
Participants portray a sincere sense of gratitude and privilege when talking about their job roles, contradicting the common misconceptions within the public view (Dixe et al., 2020). People who are not involved with palliative care/hospice settings have continually perceived hospices as a morbid place where people go to die, and any hospice-based role as a depressing last resort career (Grant et al., 2021). Challenging this, Rosie says; ‘I feel lucky to work there because of the caring nature of the place, but also because it fulfils me. It’s almost a bit of a selfish thing- I get massive pleasure from working with someone and watching the change’. (Rosie, 495–498).
From this, Rosie presents a sense of guilt where she loves her job so much that she feels selfish for having such an exclusive opportunity to gain personal growth, and seeing the inconceivable vulnerability of her patients. Rosie alludes to the job satisfaction she receives from her career, and it is satisfying her innate need to care for others. This supports the previously discussed ‘hierarchy of needs’, which illustrates that an individual’s lower-level needs must be met in order for them to thrive and achieve complex needs and fulfilment (Maslow & Lewis, 1987). In application to this theory, Rosie’s ‘utopian view’ would be enabled due to satisfying her psychological needs of belonging and accomplishment (McLeod, 2007). This ability to recognise their impact on others has been a common theme. Leigh states; ‘As miserable as every day might be, you will come home and think “okay everybody I saw yesterday has died – I’m not going to see them again.” But then you reflect on it and think “well I made a change to that person’s life in a time that was really important”.’ (Leigh, 1027–1033).
In Leigh’s talk she recognises death as a loss of life, and there is an element of sadness in this. However, her tone is optimistic when narrating her reflective process and the self-reassurance she provides herself; recognising she is doing a good job is significantly important in contributing to her positive world view. Again, in relevance to the research question, this highlights the essential need for Leigh to positively reinforce herself when making sense of the loss of life. Interestingly, this also highlights how Leigh holds herself accountable for the quality of living that her client endures in their end-of-life stages. This serves as a contradiction to other subthemes, as it suggests that she has enabled herself to become personally involved and is solely responsible for making a positive impact on the client (see Table 1). Though presenting themselves as positive and in a strong frame of wellbeing, previous literature has highlighted the negative impact of accountability within the healthcare industry (Myers, 2017).
‘Psychological Impact of Hospice Environment’
Overall, the identified superordinate themes create a narrative of the complex barriers hospice staff must face when adapting to the workplace. Though these themes demonstrate the strength and resilience of participants, this theme suggests that inevitably, the hospice environment takes a considerable toll on them. Within this theme, four subordinate themes have been identified; ‘Paranoia surrounding own health’, ‘implementing boundaries’, ‘harbouring the distress of others’ and ‘cognitively adapting to deal with stress’ (see Table 1).
Though there are themes surrounding the general awareness of their own mortality, Alex presented a theme that was unique to his own experience; ‘On the occasions where I’ve been ill, you always immediately think the worst because- because everybody you speak to starts with a “well it was just a dull ache, and I didn’t think anything and then BOOM’ (Alex, 69–73).
Alex’s experience as an end-of-life worker illuminates the issue of being exposed to a relentless, constant flow of terminal diagnosis stories. Coinciding with the findings of Gleeson and Higgins (2009), Alex’s interview presents the contradiction in being aware that he must remain objective and place client circumstances within context, whilst taking their experiences to inform his own. Though this IPA has demonstrated the benefits of reflexivity within staff who are able to learn from their patient’s lives, this theme highlights the adverse impact of this exposure. The need to implement boundaries was a particularly prominent topic of conversation among all participants, prior to, and particularly during the COVID-19 pandemic. In developing resilience and self-preservation to the morbidity of their careers, participants offered their different insights into how they place boundaries to keep work separate from their personal lives. Though all participants highlighted the importance of maintaining professionalism for themselves and their clients, Ceri provided a novel understanding of setting boundaries where he expresses concerns against getting emotionally involved within his job; ‘You have to recognise that when people are vulnerable, they can make you very vulnerable as well...If you don’t have the boundaries then you will get into trouble’. (Ceri, 578–580).
By recognising the potential impact of others’ emotions, Ceri has established the necessity of being empathetic, rather than sympathetic within this line of work. Previous literature has supported Ceri’s perspective, by stressing the fundamental role of empathy within nurturing care-based roles (Bloom et al., 2018). Alex also explained how objectivity was key to his boundaries, by recognising his job role and support as a metaphorical journey; ‘You’ve supported that person for a long time, and theres a beginning, theres a middle and an end to the support as well’. (Alex, 602–605).
Alex is holding himself accountable for the patient’s quality of living whilst it is within his role but can diminish himself of this responsibility once he has completed the process. Supporting this, previous literature has expressed the importance of acknowledging what responsibilities are legitimately their own within healthcare roles (Aguinis & Glavas, 2019).
Participants also discussed the ways in which they process the distress of others. Rosie presents the learning process of having to ignore the instincts of human nature that she has been raised with. Her role as a hospice patient counsellor serves as a huge strain on her mental wellbeing; ‘They’ve died before the next session…and we’re left with this impression of really vulnerable person that now is just gone, and they’ve dumped you with all this stuff’. (Rosie, 263–266).
The depiction of being ‘left with this impression’ indicates the complex layers of loss that Rosie faces after a client death. Aside from feeling that loss of a life, Rosie also alludes to a sense of abandonment where the client has left their relationship prematurely. This is also suggestive of Rosie’s deep involvement with her role, and the sincerity in the care and connections she creates with her clients. However, she continues to discuss her ability to adapt to this distress; ‘I have a vision of boxes around me, and I put things in boxes. Not all of them have lids that are shut, but when I know they’re not shut I must look and think “well what- what’s going on here?”’ (Rosie, 308–314)
Sivers (1998) refers to this coping mechanism and suggests that this may be a maladaptive quality if she is doing so to avoid dissecting her own feelings surrounding the situation. Furthermore, Sivers (1998) indicates that such regular ‘traumatic’ events may cause Rosie to question their world view, and the meaningful attachments associated with life and death, as previously identified in the other themes (see Table 1).
Conclusion
Main Findings
This study contributes to the underdeveloped literature surrounding the lived experiences of end-of-life/palliative care staff, through a qualitative lens. Particularly through utilising an IPA, this project is contributing to the current literature that chiefly uses thematic or discourse analysis.
Though condensed into eight superordinate themes, with most presenting dual qualities, the experiences of the participants presented themselves to be an intricate, complex phenomena. These findings are significant as they reveal the inner conflict surrounding participants’ shared experiences, whilst also addressing the misconceptions and stigma surrounding the hospice care industry (Herbstsomer & Stahl, 2020). Through an interpretation of their sense-making, this study highlights how these hospice workers hold self-care and a firm belief system as sacred to their evolved worldview. Additionally, five out of six participants spoke of colleague friendships as being a vital support, and the remaining participant also highlighted the necessity of having a compassionate network of friends outside of their workplace. Through this, the importance of companionship and belonging for wellbeing was a key finding to the study.
Some themes arose which were not anticipated by the interview schedule. Due to data collection taking place during the COVID-19 pandemic, there were discussions surrounding its impact on their industry, and on themselves as individuals. Interestingly, all participants suggested that their distress was the result of severing of social ties between colleagues who were forced to work at home or in solitude. This further reiterates the importance of socialising, to these participants. Furthermore, these discussions enacted as an opportunity for participants to also debunk the stigma surrounding an industry so heavily involved with death. It was deliberated that death has always been a staple to their career pre-pandemic, and thus their years of experience ensured that such strain was not necessarily felt within the hospices.
Additionally, the participant views on death were novel and unexpected. Previous literature has portrayed their resilience and emotional hardening as a means of self-preservation, with themes of this study thoroughly supporting this (Hart et al., 2014). Interestingly however, participants expressed a complete acceptance of death, and talked of a sense of relief and satisfaction felt when a client dies. Relevant research has portrayed a sense of optimism within hospice employees who face death, though the research observed that this positivity was a result of coping strategies such as memorial building (Montross-Thomas et al., 2016). Novel to this study, participants experienced their time within the industry as conditioning them to perceive the client death as an immediate act of emancipation. Upon deliberation, participants expressed how death was a symbolic release for the client and their surrounding circles, as well as providing a sense of closure for the staff.
Ultimately, these findings appropriately address the research question and captured the essence of the lived experiences of hospice staff. The identified themes present the trials and tribulations faced by those on the frontline of end-of-life care, though their reality of their strength, comradery and resounding optimism in life cannot be quantified.
Limitations
Interpretative Phenomenological Analysis was a suitable methodological approach as it enabled the researcher to address the complexities of a hospice work environment. In doing this, the reader should be mindful that the interpretative nature of this analysis means that the interview flow and observed themes may have been influenced as a result of a subjective socio-economic perspective (Castonguay et al., 2010). Through this lens, the perspectives of race, gender, sexuality, and religious values may be subjective and differ between each individual reader (Weis & Willems, 2017).
A limitation of the study could be the selectivity at both the researcher and participant level. The use of a semi-structured interview enabled the participant to be careful in what elements of their experiences they were willing to share. Furthermore, there is selectivity bias on part of the researcher, who determines what they deem to be significant themes within these interviews. Ultimately, qualitative research has an inevitable bias due to the researcher’s interpretation of events (Johnson et al., 2020). To avoid their own interpretation bias, the researcher reflected regularly on their own possible biases in the analysis.
Due to the COVID-19 national lockdown restrictions, all interviews were conducted virtually. Previous literature has made inferences that video calls should be identified as a study limitation due to the researcher’s inability to read the body language of the participant (Farooq & De Villiers, 2017). However, conflicting literature from Weller (2017) has identified that some individuals view video/phone interviews as an opportunity to be more open when commenting on sensitive topics than if placed within an in-person interview. Lastly, the reader must consider the unprecedented times caused by the pandemic in which this study was carried out. Though participants explicitly stated their comfort in handling the pressures of the deaths, they felt significant strain in other aspects of the workplace, and this should be considered when the research question was exploring their lived experiences and ability to adapt to the niche hospice environment.
Reflexivity
This research project has given the opportunity for reflection at every stage, which has been crucial to ensure that any risk of bias has been minimal. Johnson and Richard-Eaglin (2020) support this, and state that the reflective process plays a crucial role in developing research skills and processes, as the individual can determine the effectiveness of their current strategies. This research area was initially decided due to personal interest, and the use of the Gibbs (1988) reflective cycle facilitated a personal aspect of this process. This reflective framework provides the opportunity to examine the six stages of a specific experience, ranging from a descriptive recall of the experience to one’s own interpretation and sense-making of the situation (Markkanen et al., 2020; Gibbs, 1988).
Implications and Future Research
The outcomes of this meaningful analysis may be of benefit to the public, as these themes may be able to rectify the misunderstandings carried within the stigmatisation of hospice care and dying. Additionally, this study may provide reassurance and an understanding for individuals who are coming to terms with a personal loss that they have faced within a hospice. Surrounding literature has identified the significant positive affect understanding has on the anxiety of loved ones who are supported by hospice care (Duijn et al., 2018).
These findings may have organisational implications, providing relevant institutions and employers with insight of their employees’ wants and needs within their work life. Supporting this, previous literature has exemplified the importance of employers listening to employee needs, and its influence on staff wellbeing (Poulsen & Ipsen, 2017). Moreover, this study may inform decisions in scheduling across hospices as to when they implement their wellbeing activities, so their staff will not feel as though they are sacrificing personal time. This was a prominent dilemma among all six participants who would choose to leave work and attempt to deal with their wellbeing, rather than stay for an intervention after a long day in the environment that challenges them. Meissonnier and Richer (2021) also reinforce this as a common issue amongst employees within various shift-working industries, where staff are having to prioritise home life over wellbeing, though this is not the desired outcome of the institutions implementing such activities.
Furthermore, these themes may act to educate aspiring end-of-life/palliative care nurses on the reality and impact of working within a hospice environment. As previously mentioned by some participants, this insight would be invaluable to newcomers before thoroughly committing themselves to the potentially challenging career pathway. In relevance to staff implications, the identified themes also show the positive influence of having those strong colleague bonds within the hospice environment, and may encourage staff to pursue more opportunities to interact and develop those support systems.
From this study, numerous avenues for further research have been identified. Given that this study has been conducted during the peculiar time of the pandemic, it would be of interest for other qualitative researchers to recreate this study during normality and see if different themes emerge. Additionally, further research should be conducted to explicitly explore hospice staff thoughts and feelings surrounding death in both the workplace and personal life, as this was a strong recurrent topic of discussion amongst all participants. Though not the aim of this study, participants also presented novel insight to their relationships with their patients. These connections were portrayed as highly personal and complex, which contradicted other subthemes surrounding the participants’ need to remain objective. Therefore, it would be interesting if future research was to explore the perceptions of staff-client relationships within a hospice environment in specific detail.
Footnotes
Acknowledgements
I would like to express sincere gratitude for the guidance and encouragement I have received from my supervisor Dr. Alison Mackiewicz. Without her support and optimism, I would not have had the confidence in my abilities to pursue my passion for occupational psychology. I am especially thankful to the participants and their hospices, for contributing their valuable time and insights to this research.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.