
Abstract
This study examined the effectiveness of dialectical behavior therapy intervention on emotion regulation and death anxiety in old women. This quasi-experimental study was conducted using a pretest-posttest design with a control group. The research population included elderly women aged 60–75 years who were members of the Tehran Municipality Retirees Association in 2020. A total of 30 women were assigned to intervention and control groups (15 persons in each group). The participants in the intervention group received the dialectical behavior therapy (DBT) intervention for 10 sessions while the participants in the control group did not receive any intervention. The results of the analysis of covariance (ANCOVA) showed that there was a significant difference between the women in the intervention and control groups in terms of cognitive emotion regulation and death anxiety on the posttest. This therapy can be used for the elderly living in nursing homes and aging associations and institutions.
Introduction
Population aging has undergone a growing trend in recent years and the multiplicity and variety of stresses that people face in old age have made it essential to pay attention to mental health in old age. Aging is a process that is associated with profound physiological, psychological, and sociological changes in people. In addition to the declining course of biological processes and the increase in the quantity and quality of stressors in old age, exposure to inevitable death and the anxiety associated with it play an important role in causing mental disorders in this period (Khodabakhshi-Koolaee & Froozani, 2018).
During old age, the physical strength and health of the elderly decrease, and as they retire from their jobs, they largely lose their income, and they are less likely to interact with their spouse, relatives, and friends over time. Along with these consequences, they also experience a decline in social status, which is associated with aging, and thus, feel passive and useless (Kampfe, 2015).
There is no cut-off point that everyone agrees on for old age. In developed countries, the age of 65, when a person qualifies for a pension, is considered the beginning of old age. In some countries, the age of 60 is an acceptable measure of old age. However, depending on working conditions and social welfare, this age is influenced by the economic and cultural factors of each society. The United Nations has also accepted the age of 60 as a cut-off point (Rosenthal & Moore, 2018; Hosseinzadeh & Khodabakhshi-koolaee, 2017).
Globally, there were 703 million older persons aged 65 or over in 2019. Eastern and South-Eastern Asia were home to the largest number of the world’s older population (260 million), followed by Europe and Northern America (over 200 million) (United Nations, 2019). Over the next three decades, the global number of older persons is projected to more than double, reaching over 1.5 billion persons in 2050 (United Nations, 2019).
According to the World Health Organization, more than 20% of the Iranian population will be elderly by 2030. The rapid increase in the number of elderly people relative to the general population in recent years, the so-called “graying” of the world, is the result of a process known as the “demographic transition.” The increase in the elderly population in the present age is so important that the World Health Organization has noted that a demographic revolution is about to take place in the world (Khodabakhshi-Koolaee & Froozani, 2018).
Due to its psychological, social, cultural, religious, and economic consequences, aging has turned into a serious and challenging issue for families in particular and society in general, in developing and developed countries. Economic problems, the bankruptcy of insurance companies, and the lack of social welfare in developing countries have worsened the problems and concerns of developing countries. On the other hand, aging reduces mobility, leads to inadequate care and low income, and increases the prevalence of physical and mental illness (Kampfe, 2015). Problems and worries of daily life along with social problems, isolation, loneliness, and depression in old age can ultimately reduce the mental health of the elderly and their quality of life (Orbach, 2003).
One of the consequences of approaching old age is understanding the occurrence of death. Signs that remind the elderly of death indicate entering the last stage of life (Hosseinzadeh & Khodabakhshi-Koolaee, 2017; Furer & Walker, 2008). Death anxiety is associated with worries and anxieties about one’s death. This anxiety is different from the anxiety associated with the death of others and makes the person afraid of his/her own death (Templer & Salter, 1971; Iverach et al., 2014).
Thoughts about death are an integral part of the process of living, and people’s preoccupation with death is inevitable. One of the most important human considerations about death is the fear or anxiety of death (Lehto & Stein, 2009; Neimeyer & Van Brunt, 2018).
The effects of death anxiety are either conscious or unconscious. Studies have shown that death anxiety is higher in the elderly, although gender differences are involved. For instance, Missler et al. (2012) found that older women who lost their husbands experienced higher rates of death anxiety than their male counterparts.
The experience of negative emotions and fear intensifies general anxiety in the elderly. Anxiety disorders are associated with emotions, and emotion regulation is one of the psychological components related to anxiety. Emotion regulation refers to strategies used to reduce, increase, or maintain emotional experiences (Gratz et al., 2018). Emotion regulation leads to effective coping strategies in individuals (Gratz et al., 2015). Older people are more likely than young people to use emotion-focused coping. The goal of emotion-focused coping strategies, sometimes called self-soothing coping, is to achieve a better feeling; that is, controlling or regulating the emotional response to a stressful situation to reduce its physical and psychological impacts (Papalia et al., 2007).
Dialectical behavior therapy (DBT) is a therapeutic approach that can align a balance in a person’s acceptance strategies with cognitive and behavioral change strategies and combine both changes in one therapy (Cheavns & Lynch, 2008). All DBT-modules (mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness) are intended to improve emotion regulation skills and patients are encouraged to learn and practice these skills regularly (Fassbinder et al., 2016).
In fact, DBT is an approach that integrates client-centered acceptance and empathy with problem-solving cognitive and social skills training. Some components of DBT are also taken from the perspective of emotionally experiential therapy and some oriental philosophical schools (Cheavns & Lynch, 2008).
In their study, Lynch et al. (2003) used dialectical behavior therapy for older adults and found that DBT treatment helped reduce depressive symptoms in the elderly (Lynch et al., 2003). Moreover, Helms & Ward (2017) used mindfulness-based cognitive therapy to reduce anxiety symptoms of older adults in residential care. They reported that after seven weeks of group intervention using the MBCT method, there was a significant reduction in anxiety symptoms in the elderly in residential care (Helms & Ward, 2017)
In another study, mindfulness-based stress reduction (MBSR) therapy was used to reduce emotional distress in older adults. The results showed that MBSR can significantly help reduce emotional distress. The older adults reported less depression and anxiety after 8 weeks of MBSR. MBSR intervention as a group therapy technique can help reduce psychological distress in the elderly (Young & Baime, 2010).
Given the psychological problems experienced by the elderly, it is very essential to address their mental health and quality of life. Previous studies have employed a variety of cognitive-behavioral therapies to treat depression, anxiety, and personality problems in the elderly. Following the previous findings, the present study tries to find out whether DBT-based group therapy intervention can be effective in regulating emotions and reducing death anxiety in Iranian women.
Method
Participants
The research population covered all women aged 60–75 who were members of the Tehran Municipality Retirees Association in 2020. A sample of 30 women (15 persons in each group) were selected using simple random sampling with the inclusion criteria: (1) Having no cognitive problems based on the Mini-Mental State Examination (MMSE; Folstein et al., 1975), (2) Having minimum literacy (at least ninth-grade school education) to answer the items in the questionnaires independently, and (3) Having no physical problem or acute illness upon a doctor’s diagnosis. Furthermore, the exclusion criteria were as follows: (1) The absence from more than three sessions of group therapy and (2) Simultaneous participation in other psychotherapy sessions. Finally, a total of 30 women who met the inclusion criteria were selected and placed in two intervention and control groups, each with 18 participants. The members of the intervention group received dialectical behavior group therapy for 10 weeks.
Instruments
This section introduces the instruments used in the study to collect the data:
Mini-Mental State Examination Folstein et al. (1975): The Mini-Mental State Examination (MMSE) was developed by Folstein et al. (1975) to screen for dementia. The prefix “Mini” in this test shows its important feature, which is its shortness. The items in this test assess different areas of cognitive function. According to Fulstein, it measures the ability to memorize without the need for tools and equipment. Cognitive functions that are evaluated in this test are orientation, registration, attention, and calculation, recall, language, and visual-spatial skills. Completing this test takes an average of 13–14 min. MMSE has 20 items and its total score is 30, with a score lower than 20 indicating the possibility of cognitive impairment. Cronbach’s alpha coefficients for the reliability and validity of the test were .81 and 095, respectively. The Persian version of the MMSE has good reliability and validity and with a cut-off point of 22 can differentiate people with dementia. However, some studies reported a score below 25 to be the beginning of cognitive impairment (Seyedian et al., 2008; Khodabakhshi-Koolaee & Froozani, 2018).
Templer Death Anxiety Scale Templer & Ruff (1971): The Templer Death Anxiety Scale was developed by Templer (1970). It contains 15 items that measure respondents’ attitudes toward death. Each item is rated on a dichotomous scale of yes or no. The answer yes indicates the presence of anxiety in the person. Thus, the scores on this scale vary from 0 to 15, and a higher score indicates a higher level of death anxiety. Previous studies reported that this scale has high validity. In the original culture, the test-retest reliability coefficient of the scale was .83 and its concurrent validity was reported to be .27 by correlating it with the state Anxiety Scale and 0.40 with the Depression Scale (Templer and Ruff, 1971). Rajabi and Bohrani (2001) examined the reliability and validity of this scale for use in Iran and reported a split-half reliability coefficient of 0.60 and an internal consistency coefficient of .73. To evaluate the validity of the Death Anxiety Scale, the State Anxiety Scale was used and the correlation between the two scales was .34 (Rajabi and Bohrani, 2001). The reliability of the scale was recalculated for the elderly and its Cronbach’s alpha was reported to be .78 (Khodabakhshi-Koolaee & Froozani, 2018).
Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004): The Difficulties in Emotion Regulation Scale developed by Gratz & Roemer (2004) has six subscales: (a) lack of emotional awareness, (b) lack of emotional clarity, (c) difficulty regulating behavior when distressed, (d) difficulty engaging in goal-directed cognition and behavior when distressed, (e) unwillingness to accept certain emotional responses, and (f) lack of access to strategies for feeling better when distressed. The DERS (Gratz & Roemer, 2004) is a 36-item self-report measure of six facets of emotion regulation. Items are rated on a scale of 1 (“almost never [0–10%]”) to 5 (“almost always [91–100%]”). Higher scores indicate more difficulty in emotion regulation. Gratz & Roemer (2004) showed that this scale has high internal consistency (.93). The results showed that the scale has good construct and predictive validity. This scale was translated by Alavi for use in Iran and the internal consistency of the Persian version of the whole scale was .86. In this study, the scale was administered to a group of elderly and its reliability was reported as .91 using Cronbach’s alpha.
Design
This quasi-experimental study was conducted using a pretest-posttest design with a control group. Following previous studies and taking a 95% confidence interval and 80% test power, the sample size was estimated as 30 persons (15 persons for each group). Finally, the participants were selected based on the inclusion criteria and were randomly assigned to the intervention and control groups (15 persons in each group). After administering the pretest (the Difficulties in Emotion Regulation Scale and Templer Death Anxiety Scale) to the participants in both groups, the members of the intervention group attended 10 dialectical behavior therapy sessions by the researcher once a week for about 70–75 min per session. One week after the completion of the intervention, the posttest was administered to the members of both groups.
Procedure
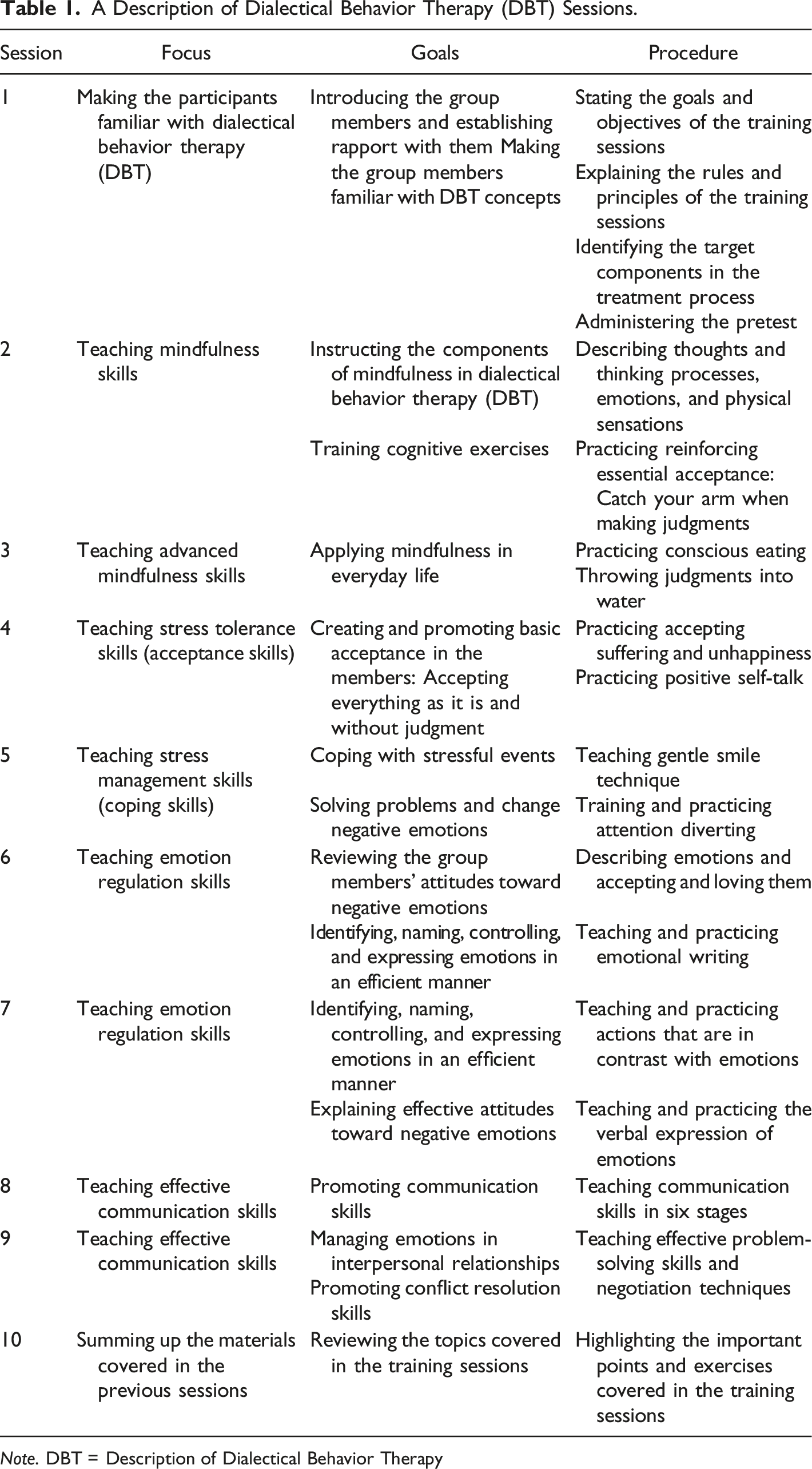
Before conducting the study, a written permit was obtained from the Khatam University Ethics Committee and the necessary arrangements were made. The participants were randomly assigned to either control or intervention group using a random number table by an independent researcher with 30 participants per group (Figure 1). Besides, informed written consent was obtained from them. The participants were assured that their transportation costs would be paid by the researcher. The training sessions were held for the participants in the intervention group for 10 weeks in a hall prepared for this purpose in Tehran Municipality Retirees Association. Each session was about 70–75 min. The intervention was implemented only for the participants in the intervention group. They participated in ten sessions (one session per week). The therapeutic intervention program was performed following the guidelines proposed in previous studies and dialectical behavior therapy textbooks (Koerner, 2012; Lynch et al., 2003; Peprah & Argáez, 2017). Finally, the collected data were analyzed using analysis of covariance (ANCOVA) with SPSS software (version 24). Table 1 summarizes the content of the intervention sessions: The CONSORT flow diagram of the data process. A Description of Dialectical Behavior Therapy (DBT) Sessions. Note. DBT = Description of Dialectical Behavior Therapy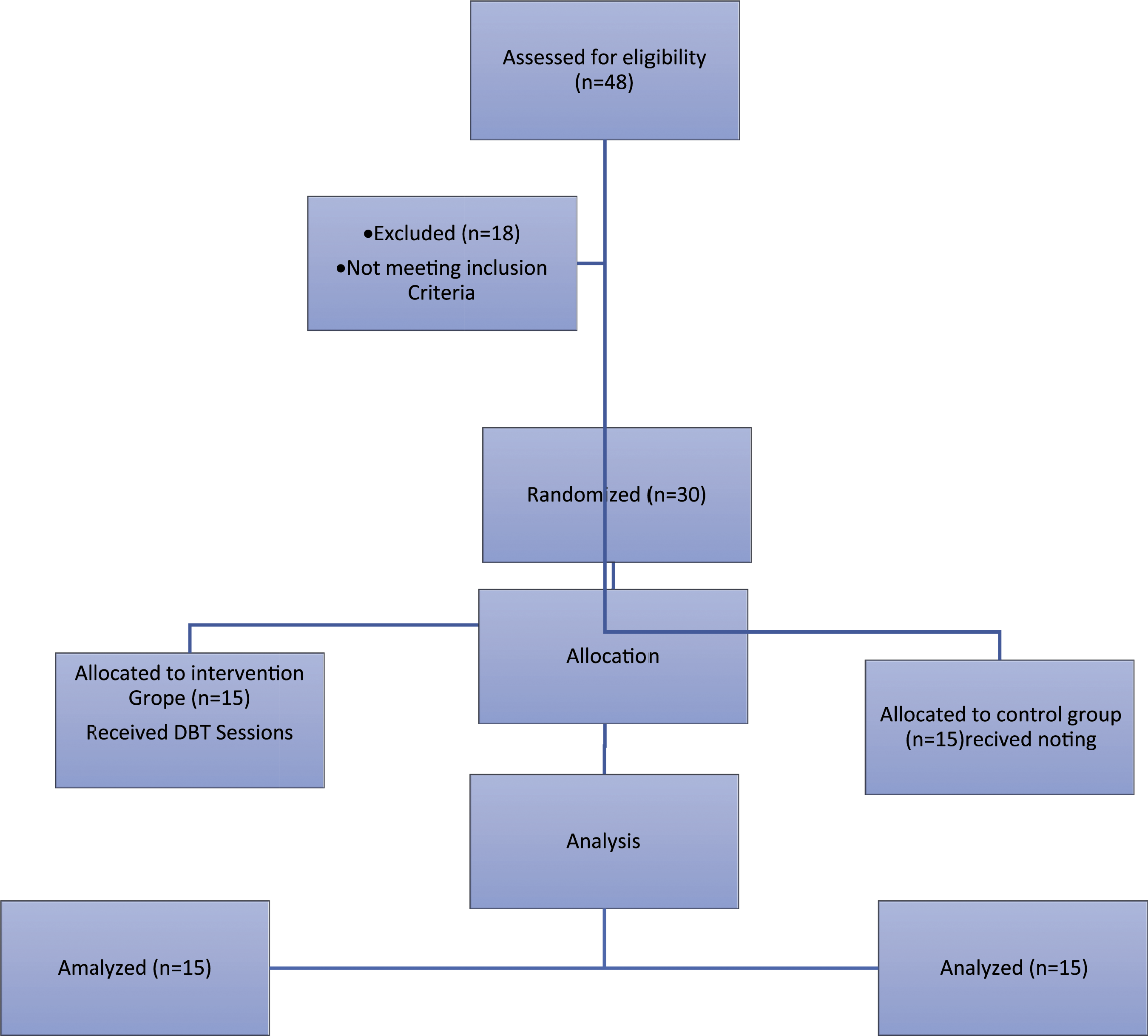
Results
Analysis of the Demographic Data
Analysis of the demographic data suggested that the age of the participants in the two groups (M = 63.01 ± SD = 3.16) years old. Besides, five participants (33.3%) held a high school diploma degree. Moreover, a majority of the participants (seven persons; 46.7%) were women who lived with their husbands. It was also shown that a majority of the participants in the control group (eight persons; 50%) were 60–64 years old and six participants (37.5%) held a high school diploma degree. Furthermore, a majority of the participants (seven persons; 43.8%) were the women who lived with their husbands and also the women (seven persons; 43.8%) whose husbands had passed away.
Descriptive Analysis of the Research Variables
Descriptive Analysis of the Research Variables.
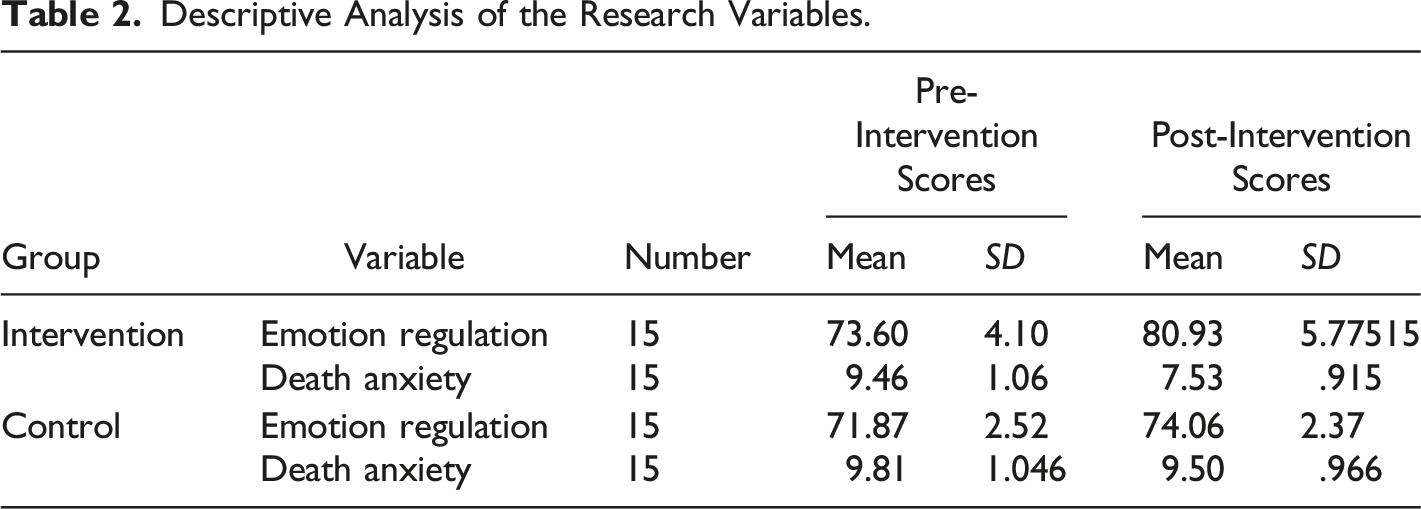
As can be seen in Table 2, the mean score of emotion regulation for the participants in the intervention group increased after the intervention compared to the pre-intervention stage. In contrast, the mean score of death anxiety for the participants in the intervention group decreased after the intervention compared to the pre-intervention stage.
The Results of Analysis of Covariance (ANCOVA) for the Effect of the Intervention on Emotion Regulation.
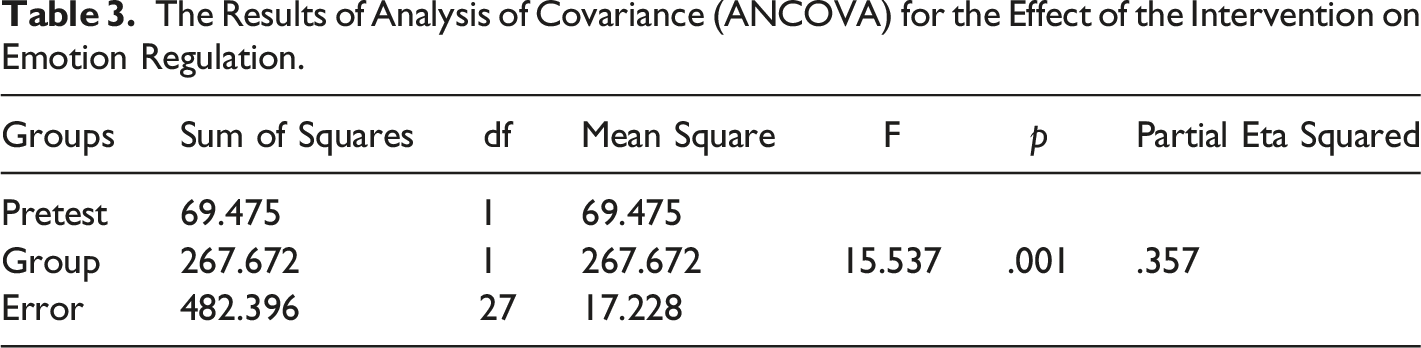
As shown in Table 3, upon controlling the effect of the pretest, there was a significant difference between the intervention and the control groups in terms of the mean scores of cognitive emotion regulation after the intervention (F = 15.537; p = .01). In other words, group dialectical behavior therapy was effective in improving cognitive emotion regulation in older women. Since the post-intervention score of cognitive emotion regulation increased significantly for the participants in the intervention group but did not change significantly in the control group, it can be concluded that group dialectical behavior therapy improved the cognitive emotion regulation in the older adult females. The effect size for cognitive emotion regulation is .357, implying the 35.7% of individual differences in the post-intervention scores of cognitive emotion regulation can be attributed to group dialectical behavior therapy.
The Results of Analysis of Covariance (ANCOVA) for the Effect of the Intervention on Death Anxiety.
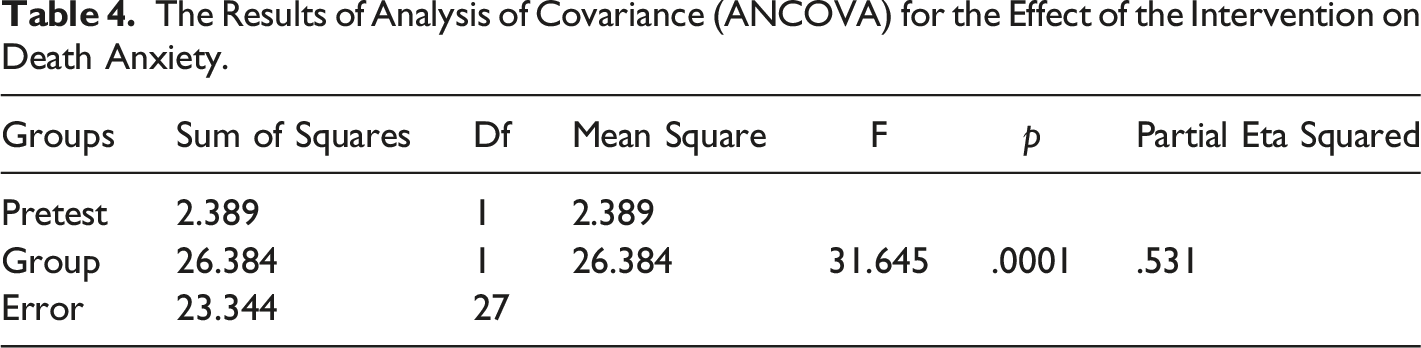
As can be seen in Table 4, after controlling the effect of the pretest, there was a significant difference between the intervention and the control groups in terms of the mean scores of death anxiety after the intervention (F = 31.645; p = .01), indicating that group dialectical behavior therapy was effective in reducing death anxiety in older women. Since the post-intervention score of death anxiety decreased significantly for the participants in the intervention group but did not change significantly in the control group, it can be concluded that group dialectical behavior therapy improved death anxiety in the older adult females. Moreover, the effect size for death anxiety is .531, suggesting the 53.1% of individual differences in the post-intervention scores of death anxiety can be attributed to group dialectical behavior therapy.
Discussion
The results of the present study showed that DBT was effective in improving emotion regulation and reducing death anxiety in old female adults. Similarly, Farb et al. (2014) found that mindfulness training (MT) was very effective in adaptive emotion regulation. They integrated mindfulness concepts and the Buddhist contemplative theory and concluded that mindfulness could be used as an effective strategy for regulating emotions (Farb et al., 2014). Moreover, Gratz et al. (2005) examined the effectiveness of different intervention techniques including cognitive behavioral therapy and mindfulness-based cognitive behavioral therapy and found that acceptance and commitment therapy (ACT) and mindfulness were effective techniques to reduce a variety of anxiety disorders including generalized anxiety disorder, panic disorder, post-traumatic stress disorder (PTSD), and obsessive-compulsive disorder (OCD). DBT therapy helps people to develop an emotional acceptance of their emotions and not to suppress them. DBT skills teach the patient to reduce unwanted and negative emotions (Gratz et al., 2005).
Malivoire also reported that dialectical behavioral therapy (DBT) skills training is likely to be an effective alternative treatment for generalized anxiety disorder (GAD). DBT intervention is especially effective for people who have difficulty regulating their emotions. DBT skills training can improve emotional disorders and help the individual learn acceptance-based strategies and DBT skills (Malivoire, 2020). Furthermore, a meta-analysis of third-wave mindfulness-based cognitive-behavioral therapies for older people showed that the third wave mindfulness-based CBT could be effective in reducing depressive symptoms in older adults (Kishita et al., 2017). In their review study of the effectiveness of mindfulness therapy on the physical and mental health of the elderly, Geiger et al. (2016) concluded that third-wave therapies, including mindfulness, can help increase the physical and mental well-being of the elderly.
The older women who participated in this learned how to communicate with themselves and practice the gentle smile technique so that they could be happy. They also learned to perform mental exercises and physiological regulation to feel relaxed when experiencing anxiety and negative emotions. They were also trained to accept and love their emotions and learned how to resolve problems easily and reinforce their communication and interpersonal skills. The participants were able to relax and better cope with their losses, wrong decisions, illnesses, and physical disabilities by learning emotional strategies, practicing the empty chair technique, and verbally expressing their emotions. Thus, they were able to adjust their emotions and avoid negative emotions such as death anxiety. Following these observations, it can be concluded that by employing dialectical strategies, accreditation, problem-solving, cognitive styles, and patient management and by reducing daily behaviors that interfere with the treatment and training of behavioral skills (interpersonal skills, anxiety tolerance skills, emotion regulation skills, and mindfulness skills) dialectical behavior therapy helps individuals to extend these skills to their life situations. Given the obvious effectiveness of DBT in treating emotional and anxiety disorders, this intervention technique can be used for reducing other anxieties and stressful issues such as death, accepting life problems, and coping with them. The results of the present study showed that DBT training sessions helped older people to pay less attention to negative life events and manage their negative emotions. They also managed to control their death anxiety by using emotion adjustment strategies since the use of ineffective strategies in individuals predisposes them to anxiety and as a result, instead of responding effectively to stressful and stressful events such as anxiety they are more likely to experience negative reactions and emotions.
The present study was conducted with some limitations. First, the research sample was limited to older adult women referring to the Tehran Municipality Retirees Association in the Spring of 2020. Moreover, given the prevalence of the COVID-19 pandemic, the intervention sessions were held in full compliance with health protocols, and it was not possible to perform a follow-up test to evaluate the retention effects of the intervention program.
Following the findings of the present study, future studies can examine the effectiveness of DBT intervention when implemented with other CBT and third wave techniques including mindfulness in reducing stress in the elderly, and perform follow-up procedures to examine the retention effects of the intervention on participants.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.