
Abstract
This study aimed to investigate the effect of music on pain, anxiety, comfort, and functional capacity of cancer patients who received care in a palliative care unit. The population of this randomized controlled trial consisted of cancer patients hospitalized in the palliative care service between July 2018 and July 2019. The study included 60 patients (30 interventions/30 controls). The patients in the intervention group were given a total of six music sessions, 10 minutes each with the Turkish classical music in maqams of their choice (Hejaz or Rast accompanied by an expert tambour (drum) player). There was a significant difference between the mean total pain scores, anxiety, comfort, and functional capacity scores of the patients in the intervention and control groups before and after music therapy. Music therapy decreased the level of pain. It is demonstrated that Turkish classical music therapy improved the pain, anxiety, comfort, and functional capacity in the palliative care unit.
Introduction
There are several serious symptoms or conditions which cancer patients must deal from time of diagnosis to end of life. The palliative care begins at the time of diagnosis and aims to provide symptom control while preserving the quality of life (Rome, 2011). The palliative and end-of-life care is labeled as an essential component of cancer control by the World Health Organization (WHO). The WHO defines palliative care as an approach that improves the quality of life of patients (adults and children) and their families who are facing problems associated with a life-threatening illness. It prevents and relieves suffering through the early identification, accurate assessment, and timely management of pain and other problems either physical, psychosocial, or spiritual (Gwyther, 2011). In the palliative care, symptoms include pain, constipation, diarrhea, anorexia, dysphagia, nausea and vomiting, dehydration, depression, delirium, and fatigue. Pain is one of the most common symptoms that is encountered in the cancer patients (Ozcan et al., 2016). In previous studies, it was that 30% of cancer patients experienced pain at the diagnosis while 50–70% during treatment period and 60–80% at terminal period (Tuncer, 2012). In another study, it was found that 90% of patients had pain at time of admission to palliative care unit with >50% of patients with patient-reported pain severity ≥5 (Yılmaz, 2015).
Pharmacological agents are used in pain management as they are readily available with rapid action (Evans et al., 2016). In addition, non-pharmacological interventions are also important to improve quality of life and comfort and reduce symptom burden in the patient by relieving pain related to adverse effects of therapeutic interventions employed in the cancer patients receiving palliative care. As non-pharmacological intervention can reduce pain by either alone or in combination with drugs, they have been increasingly used in recent years (Gokhale & Gokhale, 2017). Music plus medicine was used as a non-pharmacological intervention in many health problems as a traditional treatment and psychosocial intervention (Baldısserın, 2020). In this study, it was aimed to investigate the effects of music and medicine on pain in cancer patients admitted to a palliative care unit.
Material and Methods
Required permissions to carry out the research was received. Research on palliative care permission was obtained from the hospital to be applied in the ward. The study was conducted at a Palliative Care Unit between July 2018 and July 2019 in XXX. The study population involves cancer patients admitted to the Palliative Care Unit between July 2018 and July 2019. The study sample included cancer patients fulfilling selection criteria. The sample size was calculated using Power analysis based on the data from pilot intervention. The sample size was evaluated with General Comfort Scale (GCS) scores. In the post-hoc sample calculation, the effect size was found to be .83 (large) with mean GCS scores of 2.77 ± .11 and 2.66 ± .15 for intervention and control groups, respectively. For inter-group comparison by independent samples t test, the power was calculated as 88.9% when the alpha error was .05 and 30 patients in each group (60 patients in total) (Faul et al., 2009).
Sample Selection Criteria
The selection criteria were as follows: age >18 years, capability to speak and understand Turkish language, volunteering to participate in the study, diagnosis of cancer and hospitalization to the palliative care unit, patient-reported “moderate” or “severe” pain (>3 Visual Analog Scale scores) despite opiate or analgesic use and not being in the terminal or bedridden status. In addition, the patients with no cognitive impairment, brain metastasis, and clinical diagnosis or findings of dementia, hearing problems, agitation, or delirium were also included. Overall, 78 patients were included in the study sample; however, some patients were excluded from the study after randomization by their request or were excluded from the study due to different reasons. Thus, there were 60 patients in the final study sample including 30 patients in the intervention group and 30 patients in the control group, who participated in the study. The number of patients in the sample over time is given in Figure 1. Diagram of the number of patients in the sample over time.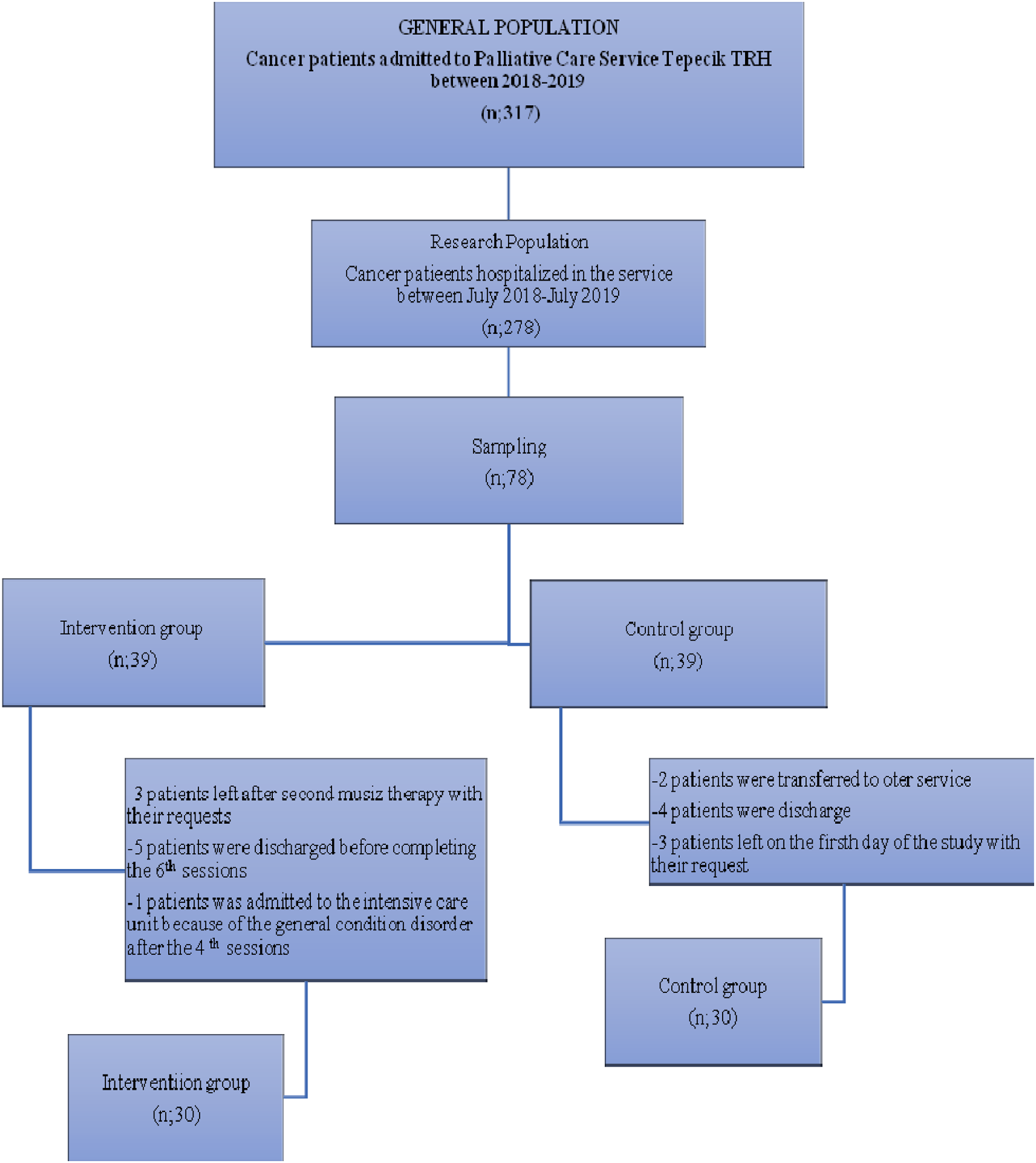
Dependent and Independent Variables
In the study, the dependent variables were pain level, comfort level, anxiety level, and performance level while independent variables were age, gender, diagnosis, stage of the disease, length of stay in palliative care unit, coping methods for pain, preference for musical genre as well as frequency, and duration of listening to music.
Data Collection Methods
A pre-treatment testing was performed on 10 cancer patients hospitalized in the Palliative Care Service to evaluate the usefulness of the form regarding the characteristics of the patients and to determine the applicability of the experimental research, and no problems were detected. Patients who received a pre-treatment testing were excluded.
The participants were randomized into two groups by stratification method (Özdemir, 2009). It was considered that three to four variables including age and gender were sufficient to assign the participants into the intervention and control groups (Büyüköztürk, 2016). Therefore, randomization process was stratified according to age, gender, and disease stage. The coin tossing method was used to determine intervention group. All patients continued to use all medications prescribed before, during and after the research without any intervention or change. All patients had pain score ≥3 and received narcotic analgesics.
Application Process of Intervention Group
A face-to-face interview was performed with the patient and information was provided about the research and the “Patient Information Form” was filled prior to the research. “Informed Consent Form” was signed to patients who met the criteria for inclusion in the study and accepted to participate in the study and group determined by randomization method (coin-tossing). In the control group, the patients received analgesic treatment alone while the patients received music (six sessions, 10 minutes per session) plus medicine with the support of a specialist from the Conservatory Department in an university using the Turkish classical music (Hejaz and Rast modes) accompanied by a tambour. The Patient Information Form, Informed Consent Form, Patient Follow-up Form, Short Form McGill Pain Questionnaire (SF-MPQ), General Comfort Scale (GCS), State-Trait Anxiety Inventory (STAI), and Karnofsky Performance Scale were applied to all patients before the intervention (music plus medicine). Following completion of forms, the patient was taken into intervention room (ventilated and set to 25–26°C) for music plus medicine.
In all patients, the pain level was recorded to the Patient Follow-Up Form before the intervention. The patient was asked to turn off mobile phone and to focus solely on the specialist and the duration of treatment before intervention. The specialist was instructed to not speak to the patient. The specialist asked the patient only two questions: “How are you?” and “Which modes do you want to listen?”. When the patient was ready to therapy, the music specialist was invited to the intervention room and the researcher left the room, leaving the patient and the specialist alone. Prior to musical therapy, the specialist asked the patient preference of classical music (Rast or Hejaz modes), and music (10 minutes) plus medicine was performed according to the patient’s preference. The patient was transferred to palliative care unit after the therapy. Clinical data and pain scores were obtained on minutes 5, 30, and 60 after music plus medicine. The music sessions (n = 6) and medicine were applied to the intervention group on different days. Patient Follow-up Form was recorded before and after each therapy during intervention period (six sessions of music). The GCS, the STAI, and the Karnofsky Performance Scale were assessed at baseline and on months three and six after intervention.
Application Process of Control Group
The control group included patients who received analgesic treatment alone and routine nursing care without any interventions. Again, a face-to-face interview was performed with the patient and information was provided about the research and the “Patient Information Form” was filled prior to the research. “Informed Consent Form” was signed to patients who met the criteria for inclusion in the study and accepted to participate in the study and group determined by randomization method (coin-tossing). Subsequently, the Patient Follow-Up Form, GCS, STAI, and Karnofsky Performance Scale were applied to patients. Six sessions of analgesic treatment were applied to all patients in the control group on different days. Throughout the study period, the Patient Follow-Up Form was completed before treatment and on minutes 5, 30, and 60 after analgesic treatment on each session (six sessions). The GCS, STAI, and Karnofsky Performance Scale were completed at baseline and on months three and six after the sessions completed. The Patient Information Form and SF-MPA were applied only once.
Instruments
1. Patient Information Form was developed by the researcher. The form included 16 items about patient characteristics such as age, educational status, place of residence, occupation, length of stay in palliative care, diagnosis and stage of disease, the history of chronic disease, coping methods for pain, preference for musical genre, frequency, and duration of listening to music. 2. Patient Follow-Up Form was developed by the researcher. In the intervention and control groups, the vital signs and pain level of the patients were recorded before and after the intervention in each session (n = 6 for each group). 3. Pain Scale-Short Form of McGill Pain Questionnaire (SF-MPQ) was developed by Melzack in 1987. It includes three items: the nature of the pain, its severity, and general pain intensity. The Turkish validity and reliability study was conducted by Yakut et al. and Cronbach Alpha value was calculated as .705 (Yakut et al., 2007). 4. GCS was developed to evaluate the individual’s comfort requirement and increased comfort with nursing interventions by Kolcaba in 1992 (Kolcaba, 1992). It includes three levels and four dimensions. Its adaptation to Turkish language and Turkish validity and reliability study was conducted by Kuğuoğlu and Karabacak in 2008 (Kuğuoğlu & Karabacak, 2008). The mean value is found by dividing the total scale scores by the number of scale items (Kolcaba, 1992; Kuğuoğlu & Karabacak, 2008). One point indicates the lowest comfort status while four points indicate the highest comfort status. 5. STAI is a self-assessment questionnaire consisting of short expressions. The questionnaire required patients to describe how they feel under certain conditions and to answer the scale with their feelings about these conditions. Translation and standardization of the scale into Turkish language was done by Öner and Le Compte in 1974–1977. The maximum score is 80 points while the minimum score is 20 points in the scale. Higher STAI scores indicate higher level of anxiety (Öner & Le Compte, 1985). 6. Karnofsky Performance Scale was developed to assess performance status of cancer patients by Karnofsky et al. in 1948. It allows score from 0 to 100 points and is prognostic marker for normal activities and functional capacity of a patient including working, the need for caregiver, and the level of dependence in medical care (Johnson et al., 2014).
Data Analysis and Evaluation
General Comfort scores were taken as basis in the sample calculation. In the post hoc sample calculation, the mean score and SD of the study group were taken as 2.77 ± .11 and that of the control group as 2.66 ± .15, and the effect width was found to be .83 (large). In order to compare the two groups with the t-test in independent samples, the power of the analysis to be done is 88.9% when there are 30 people in each group (60 people in total), with an alpha error of .05 (Faul et al., 2009).
Statistical analyses were performed using the SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). Data are expressed as number, percentage, mean, and SD. Power analysis was conducted to determine the sample size. The normal distribution of data was evaluated with skewness coefficients. The variables were compared between groups using the chi-squared test, independent samples t-test, or Mann–Whitney U test. ANOVA and Pearson correlation analysis were used to compare repetitive measurements over time between groups. Statistical significance level was set as p < .05.
Results
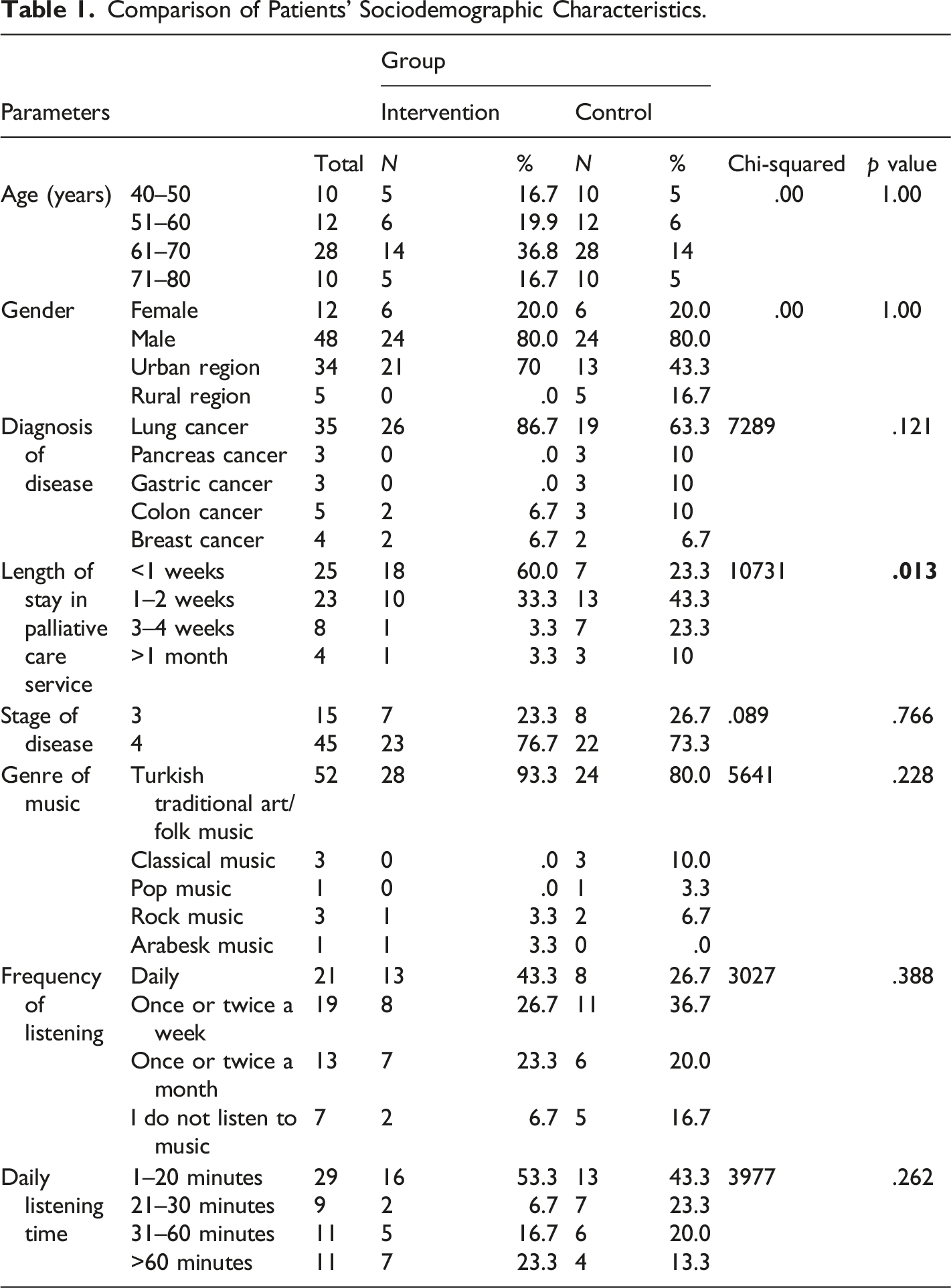
Comparison of Patients’ Sociodemographic Characteristics.
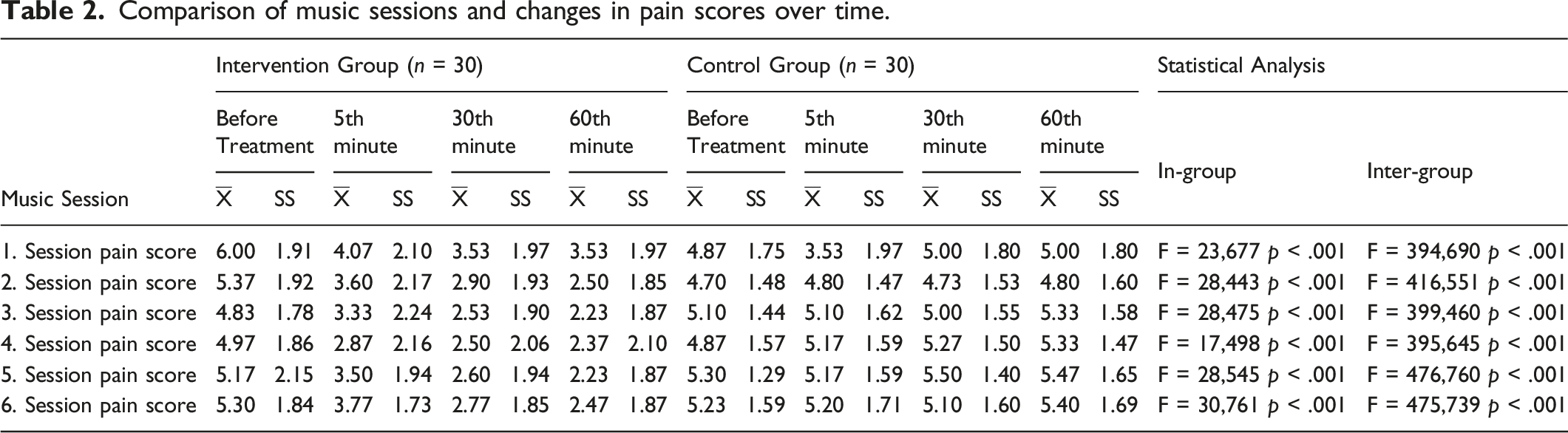
Comparison of music sessions and changes in pain scores over time.
Comparison of changes between music sessions and scale scores over time.
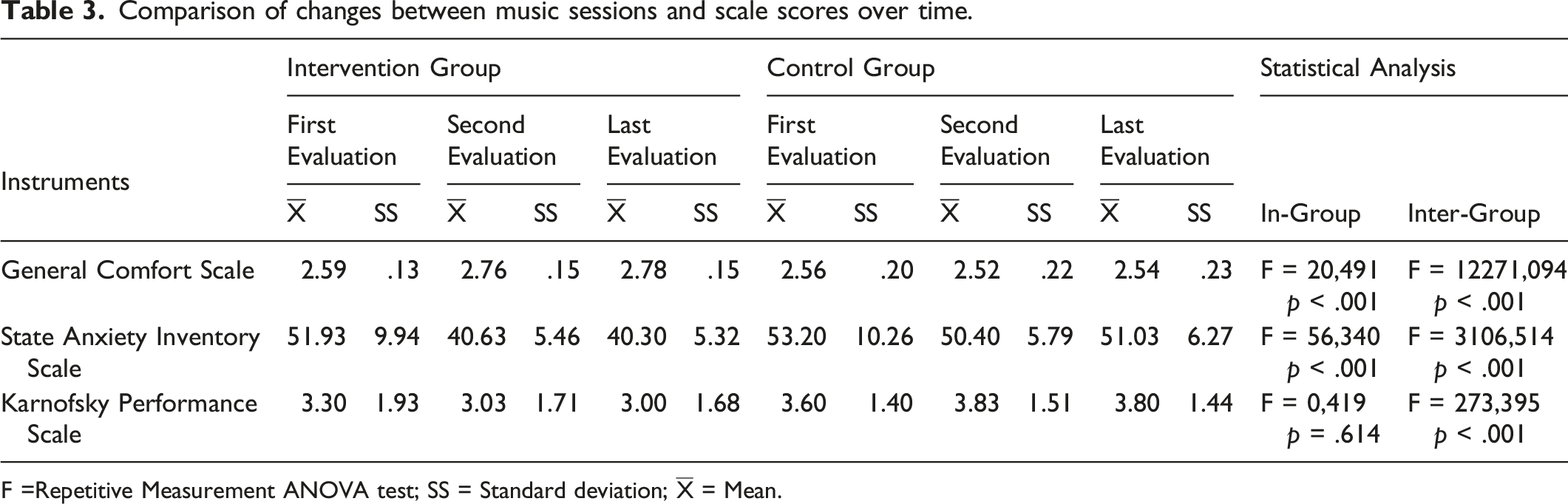
F =Repetitive Measurement ANOVA test; SS = Standard deviation;
Correlations between First and Last Evaluation Scores of Pain and Scores of State Anxiety Inventory, General Comfort Scale, and Karnofsky Performance Scale in the Intervention and Control Group.
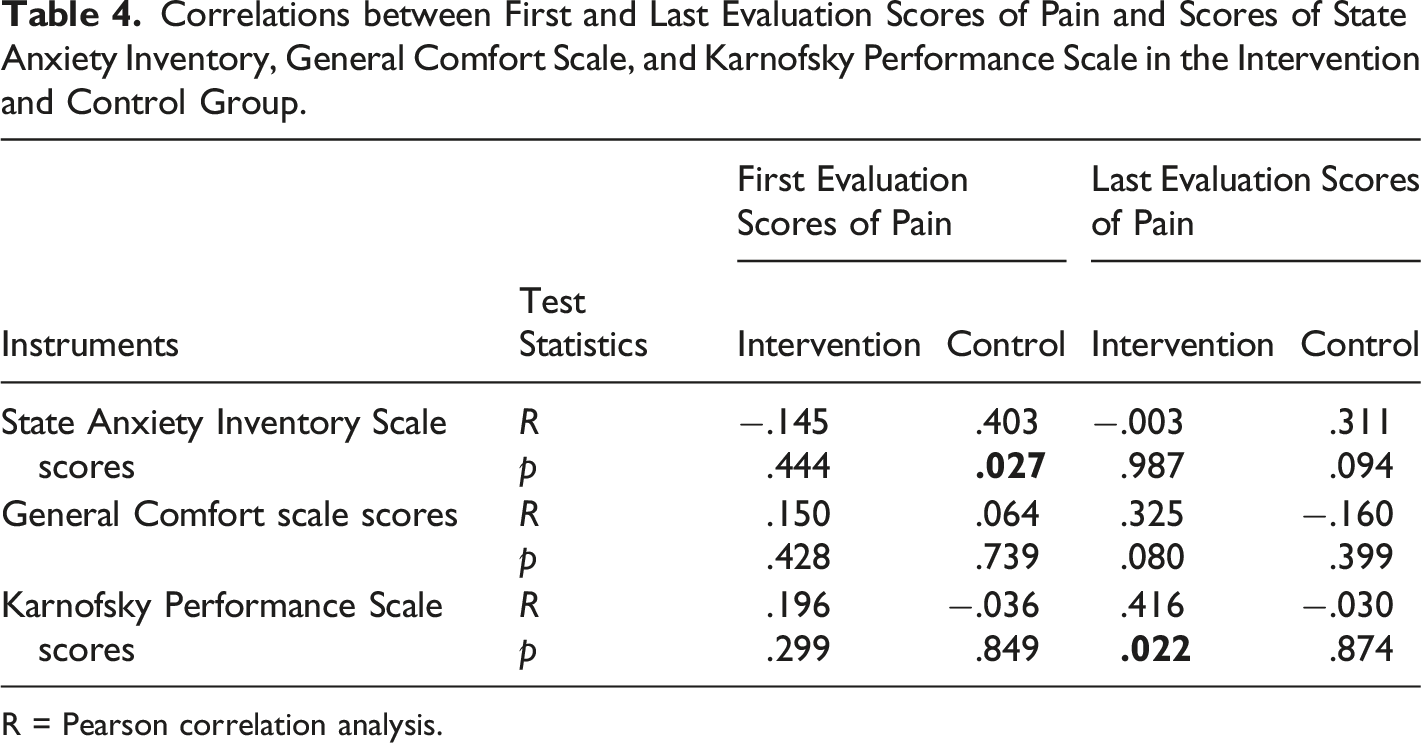
R = Pearson correlation analysis.
Discussion
Majority of cancer patients experience significant pain in palliative care and at end of life. In the cancer patients, the quality of life was significantly impaired due to the nature of cancer, as well as the many side effects of cancer treatment. Therefore, health professionals have been attempted to provide symptom control in cancer patients using pharmacological and non-pharmacological interventions. The non-pharmacological interventions have been increasingly used to promote comfort in palliative care settings. The non-pharmacological interventions are valuable regarding avoidance from drug side-effects. In our study, we evaluated the effects of music plus medicine on pain, anxiety, comfort scores, and functional capacity of the intervention group in comparison with the control group.
Evaluation of Patients’ Characteristics
No statistical difference was found between two groups regarding gender, age, diagnosis, and stage of disease (p > .005). Our study revealed that both groups were homogeneous regarding descriptive characteristics. It was found that 75% of patients had lung cancer in the study sample. In a study, Gallagher et al. (2018) demonstrated that the most common diagnosis was lung cancer by 16% (Peng et al., 2019). In similar studies, the study sample generally consisted of cancer patients (Preissler et al., 2016; Teut et al., 2014; Warth et al., 2015). In our study, 75% of the patients had stage 4 cancer. It is noteworthy that the studies were performed in patients with advanced cancer in the literature (Hilliard, 2003; Preissler et al., 2016; Teut et al., 2014).
Among our patients, the most preferred music genre was Turkish traditional folk and Turkish art music by 86.7%. In a study on patients receiving outpatient chemotherapy, Çokmert et al. showed that 21 of 56 patients (38%) preferred to listen to “Classical Turkish Music” and 18 patients (32%) “Turkish Traditional Folk Music” (Çokmert et al., 2011). In similar studies from different countries, it was found that patients generally preferred genres of religious music, classical music, or instrumental relaxing music (Aker & Akar, 2020; Gallagher et al., 2018; Hilliard, 2005; Sales et al., 2011). The intervention using music based on patient preference was identified as an important factor that increased the effectiveness of the study with provision of highest level of benefit and better compliance to the therapy (Gutgsell et al., 2013). In consistent with our study, similar results were reported in previous studies when patients allowed to select the type of music and preferred music that appealed to the society and culture to which they belong. In our study, the patients in the intervention group were allowed to select the modes of Hejaz or Rast in each music session. After music plus medicine, the pain scores were decreased significantly by both modes.
In our study, music (10 minutes per session) plus medicine was given to the patients in the intervention group with the recommendation of the music specialist. A tambour, which is a stringed Turkish music instrument, was used in our study. The music plus medicine intervention was performed with tambour using the improvisation method with rhythm-free. It was found that the duration of listening to music was 1–20 minutes in 48.3%, 21–30 minutes in 15%, 31–60 minutes in 18.3%, and more than 60 minutes in 18.3% of our patients. Therefore, 10 minutes of music plus medicine performed with a tambour were sufficient regarding duration. However, the duration of music plus medicine intervention was highly variable in similar studies in the literature.
In the study by Hilliard, music plus medicine intervention was given using 15-minute sessions in hospitalized and palliative care patients, whereas using 3–13-minute sessions in palliative care patients by Teut et al., 30-minute sessions by Warth et al., and 30–to 45-minute sessions by McConnell et al. (Hilliard., 2005; McConnell et al., 2016; Teut et al., 2014; Warth et al., 2015). The duration was left to the patient’s preference, and they listened as much as they wanted between 20 and 90 minutes (Preissler et al., 2016). Since the music plus medicine had a variable duration in other studies, it was observed that previous results did not show similar characteristics with our outcomes.
Evaluation of the Instruments of the Patients
The changes in pain score over time with interventions were statistically significant between two groups. While the mean pain scores were decreased by music plus medicine in the intervention group, there was no change in the pain score of the control group. Based on these data, the research hypothesis was accepted. Gallagher et al. showed that the pain levels decreased from 2.7 to 2.1 after music plus medicine in palliative care patients (Kara & Açer, 2012) In the study by Gutgsell et al., it was found that the pain level was decreased from 2.38 to 1.76 in the intervention group and from 2.30 to 2.19 in the control group from (Gutgsell et al., 2013). In hospice patients, Krout et al. demonstrated that one-session music and medicine significantly reduced pain (Krout, 2001). In our study, the pain level was evaluated at baseline and on minutes 5, 30, and 60 after intervention. In the intervention group, all patients received a total of six music plus medicine sessions (10 minutes per session) on different days. The follow-up frequency and the number of sessions differed in previous studies. Our study presented more detailed data than other studies with its higher follow-up frequency and greater the number of interventions (Gallagher et al., 2018; Gutgsell et al., 2013; Kim, 2006; Krout, 2001).
The comfort is one of the important concepts that significantly affects the quality of life in patients. The mean comfort score was significantly increased by treatment in the intervention group with treatment while it was significantly lower in the control group. Previous studies showed that patient comfort level was affected positively by the music plus medicine (Krout, 2001; Preissler et al., 2016; Teut et al., 2014). Overall, 11 studies were reviewed by Hilliard who found that the physical comfort was among the dependent variables that were positively affected by music and medicine and improved well-being of patients (Hilliard, 2005)
In the intervention group, the anxiety levels were significantly decreased by music plus medicine. Although the anxiety levels were also decreased in the control group, the difference did not reach statistical significance when compared to intervention group. State anxiety is defined as anxiety in response to a specific situation that is perceived as threatening or dangerous (Kara & Açer, 2012). Anxiety levels negatively affected blood pressure and could cause relative changes in heart rate. We found decreased heart rate after the music plus medicine, with a significant difference between the intervention group and the control group regarding heart rate. In a meta-analysis, Koelsch et al. demonstrated that music plus medicine reduced the level of anxiety by reduction in the heart rate (Koelsch & Jäncke, 2015). It was emphasized that there is paucity in the studies in this field and should be examined by researchers. Our study presented new data on the effects of music and medicine on anxiety status for palliative care patients.
We used the Karnofsky Performance Scale to assess functional capacity, as it provides a broader assessment and has a higher sensitivity to minimal differences. There was a statistically significant difference between functional capacity before and after music in both interventions and control groups. No difference was found between time points (minute 5, 30, and 60) after the therapy in the intervention group, but some patients were transferred to the intervention room by a wheelchair and preferred to walk to their rooms after the music plus medicine. This indicates that the music may have positive effects on the patients, leading improved functional capacity. Some patients chose to spend time in the garden after therapy, while others preferred to talk to other patients instead of staying in the room. This positive affect in patients also affected their physical capacities positively. In the literature, only one study using music plus medicine with Karnofsky Performance Scale in cancer patients was identified, which demonstrated improvement in the quality of life and KPS after music plus medicine (Liao et al., 2013). In a study on 301 patients with terminal cancer in a hospice center, Santiago-Palma showed that 239 patients reported having difficulties in their daily life activities (Santiago‐Palma & Payne, 2011). Our study revealed that palliative care patients benefit from non-pharmacological interventions that could be applied to increase their functional capacities. It is important to increase the number of studies in this area.
Conclusion
Our study demonstrated that Turkish music and medicine was effective on pain, anxiety, comfort, and functional capacity in patients with cancer in the palliative care service. Music plus medicine was one of the non-pharmacological interventions and supported an effective care that nursing could also achieve independently.
Music and medicine were one of the complementary and integrative methods that can be applied to patients with pain after receiving professional training by nurses and other healthcare professionals, and the results can be evaluated with clinicians. Since the genre of music preferred by patients affects the results, it will be useful to pay attention to the music genre in the treatment. New music and medicine studies can be performed in different sample groups or in larger sample groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.