
Abstract
This study investigated oncology nurses’ attitudes toward caring for dying patients, their principles of dying with dignity, and their views on good death. This descriptive study included 257 oncology nurses working at two university hospitals, an educational research hospital and a state hospital in Turkey. Data were collected using the descriptive characteristics information form, the Frommelt Attitudes toward Care of the Dying scale, the Assessment Scale of Attitudes toward the Principles of Dying with Dignity, and the Good Death Scale. The nurses obtained mean scores of 99.53 ± 7.76 on the Frommelt Attitudes toward Care of the Dying scale, 26.84 ± 12.45 on the Assessment Scale of Attitudes toward the Principles of Dying with Dignity, and 57.23 ± 7.48 on the Good Death Scale. The nurses’ personal and professional characteristics influenced their attitudes toward caring for dying patients, the principles of dying with dignity, and their views on good death.
Death is a universal reality for all living organisms (Banerjee et al., 2016; Khalaf et al., 2018). Despite advances in its diagnosis and treatment, cancer is the second most common cause of death after cardiovascular disease (Ahmad & Anderson, 2021; World Health Organization, 2019). According to Globocan 2018 data, one out of every six people die because of cancer worldwide (Bray et al., 2018). Attempts have been made to control cancer using modern treatment and care technology to extend the life expectancy of cancer patients. This increases the number of patients who are near death and in need of care. The majority of cancer patients die in the oncology clinics where they are being treated and cared for (Banerjee et al., 2016; Khalaf et al., 2018; Mohamed Ali & Ayoub, 2010).
Nurses who work in oncology clinics frequently care for dying patients and witness the death phenomenon because of the nature of their profession. Caring for a dying patient and witnessing the death of that patient is a stressful and challenging experience for nurses and requires a considerable amount of essential knowledge and skills (Andersson et al., 2016; Banerjee et al., 2016; Cevik & Kav, 2013; Khalaf et al., 2018). Caring for dying patients, lack of treatment options, difficulty controlling symptoms, being asked difficult questions by patients and their relatives, and increasing emotional and spiritual requirements make the caring process challenging. Furthermore, the death of a patient under the care of a nurse is a loss experience for the nurse. These difficulties experienced by nurses can negatively affect the quality of care provided to dying patients (Dong et al., 2016; Lancaster et al., 2017; Parry, 2011; Tait et al., 2015).
Nurses need to know the expectations and needs of their patients to provide them with a dignified death environment. These expectations and needs help shape nursing care. Often, patients want to say goodbye to life while maintaining their physical, emotional, and spiritual well-being; they want to have a high quality of life, good communication with healthcare personnel and maintain their dignity (Meier et al., 2016). Baillie and Matiti (2013) evaluated patients’ views on an honorable and respected death and noted that pain and suffering were alleviated when the death occurred at home, and the health personnel had sufficient knowledge and skills to ensure good death. Moreover, patients with advanced-stage cancer suffer from many physical, social, and psychological problems and often think about death. Therefore, it should be a priority for cancer patients to receive quality nursing care during the death process (Meier et al., 2016; Miyashita et al., 2007). When cancer patients’ views on good death were evaluated, they explained that good death was “freedom from pain,” “not being a burden to their families,” “the feeling that life was meaningful,” and “home or home‐like death” (Yun et al., 2018). In another study, cancer patients stated the components of good death as “not being a burden to others,” “preparation for death,” and “physical and psychological comfort” (Chindaprasirt et al., 2019).
Although there is no definitive standard for good death expectations, nurses need to understand how their knowledge and attitudes regarding terminal care affect the quality of care they provide to their patients. When planning the care of dying patients, nurses’ views on dying patient care and good and dignified death should be examined. Consequently, the quality of healthcare services for dying patients and patients’ satisfaction with the care provided will increase. Furthermore, instead of avoiding the subject, it is recommended that death—which is taboo in many cultures and often evokes negative feelings in oncology nurses who frequently witness it— should be treated as a natural part of life (Cevik & Kav, 2013; Kinoshita & Miyashita, 2011).
It is the most basic human right for cancer patients to have a dignified and respectable farewell as they wish (Becker et al., 2017; Ceyhan et al., 2018). Therefore, it is vital to determine nurses’ attitudes toward caring for dying patients and the principles of a dignified death and to gain insight into their views on death (Banerjee et al., 2016; Cevik & Kav, 2013; Choi et al., 2013; Zewdu et al., 2017).
Theoretical Framework
This study presents a theoretical framework that defines the effect of the socio-demographic characteristics of nurses and their experiences caring for dying patients. It also explores nurses’ attitudes toward dying patient care, their principles of dying with dignity, and their views on good death (Figure 1). This theoretical framework is based on Benner’s from novice to expert theory. The theory argues that nurses should gain experience in exhibiting pected behaviors. According to Benner, nurses gain expertise in clinical practice by having a strong educational background and through experience (Benner, 1982). Conceptual model of factors that affect the care of dying patients (Benner, 1982; Dunn et al., 2005).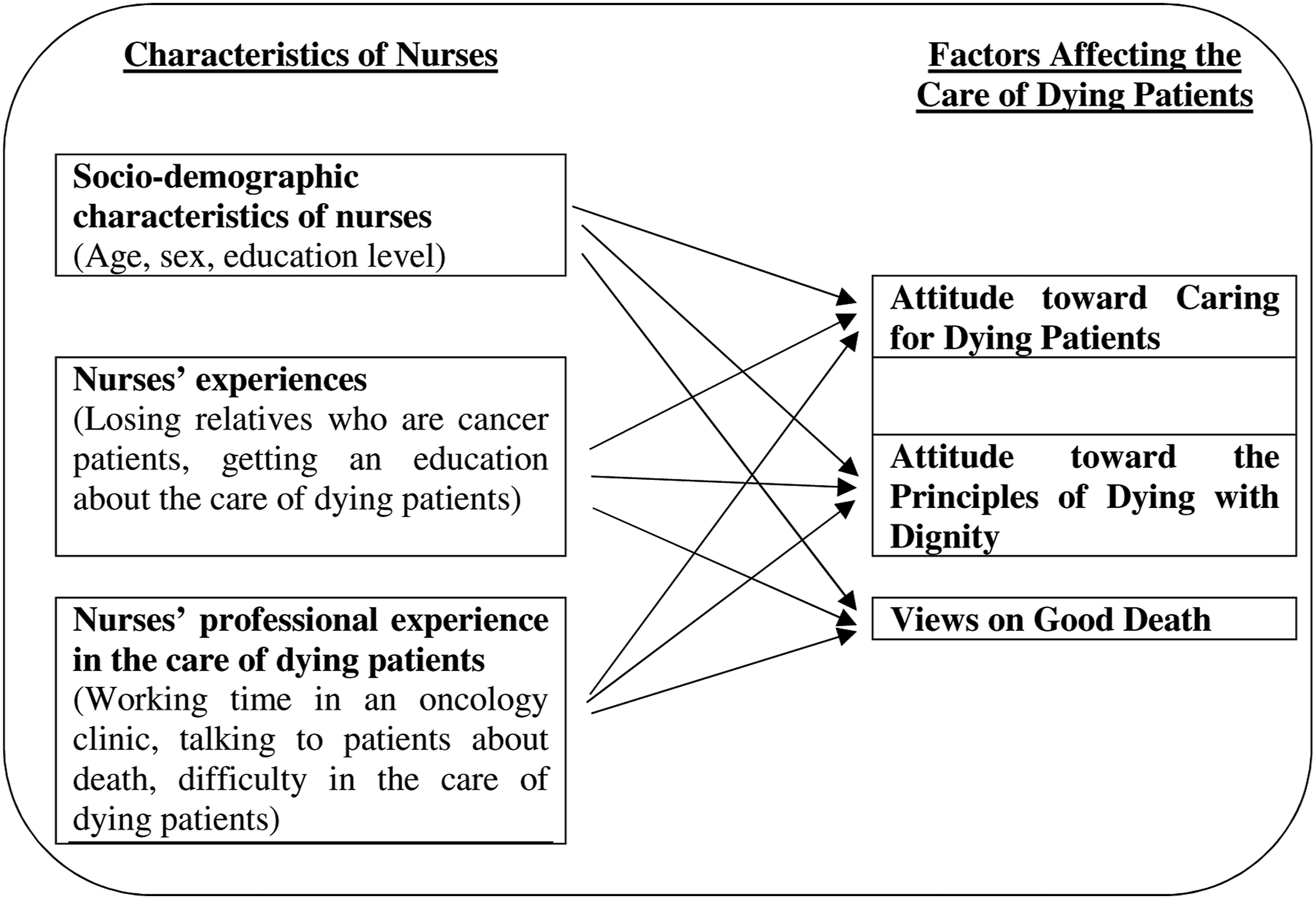
According to Benner’s skill acquisition theory, nurses’ attitudes toward dying patient care, their principles of dying with dignity, and their views on good death are affected by their socio–demographic characteristics and personal and professional experiences (Benner, 1982; Dunn et al., 2005). In this study, nurses’ specific personal and professional characteristics and their professional experiences in dying patient care were conceptualized based on their attitudes toward dying patient care, the principles of dying with dignity, and their views on good death (Figure 1).
Method
Participants and Procedure
This descriptive study was performed at two university hospitals, one research and training hospital and one state hospital in Ankara, Turkey. Three hundred and twenty-five nurses worked in the oncology clinics of the four participating hospitals. Of these 325 nurses, 68 (21%) were excluded for the following reasons: maternity leave (31 nurses), medical leave (two nurses), leaving the institution (two nurses), non-clinical assignments (two nurses), unpaid leave (eight nurses), annual leave (seven nurses), and refusal to participate in the study (16 nurses). The final sample comprised 257 (79%) nurses. After the nurses signed informed consent forms, they completed the data collection tools in the nursing room. The completion of the forms required approximately 15–20 minutes.
Data Collection Tools
The data were collected using the descriptive characteristics information form, Frommelt’s Attitude toward Caring of the Dying scale (FATCOD), the Assessment Scale of Attitudes toward the Principles of Dying with Dignity (ASAPDD), and the Good Death Scale (GDS).
Descriptive Characteristics Information Form
This form was prepared by reviewing the literature on the topic (Cevik & Kav, 2013; Khader et al., 2010; Kinoshita & Miyashita, 2011; Lange et al., 2008; Mohamed Ali & Ayoub, 2010; Tait et al., 2015), and the opinions of three experts in the relevant fields were obtained. The form comprised 10 questions; these questions included information about the nurses’ age, sex, marital status, education level, working time in the profession, working year in an oncology clinic, training for the care of dying patients, the loss of a relative to cancer, talking to patients about death, and difficulty in caring for dying patients.
FATCOD
FATCOD was used to evaluate nurses’ attitudes toward the care of dying patients. This five-point Likert scale comprises 30 items. The Turkish validity and reliability study of the scale was performed by Cevik and Kav (2013), who found that the Cronbach’s alpha coefficient of the scale was .73. The rates of negative and positive attitudes were equal in the scoring of the scale. In the scoring of these negative and positive attitudes, scores with negative items were reversed, resulting in a total score ranging from 30–150. The higher the total score, the more positive the nurses’ attitudes toward the care of dying patients (Cevik & Kav, 2013). In our study, the Cronbach’s alpha reliability coefficient of the FATCOD scale was .69.
ASAPDD
The ASAPDD was used to evaluate nurses’ attitudes toward the principles of dying with dignity. This is a five-point Likert scale, which was included in The Future of Health and Care of Older People and prepared based on 12 principles by the Debate of the Age Health and Care Study Group in 1999. The Turkish validity and reliability study of the scale was assessed by Duyan (2014), who determined that the Cronbach’s alpha coefficient was .893. The total score on the scale ranged from 12–60. Higher scores indicate that adopting the principles of dying with dignity is high and lower scores indicate that adopting the principles of dying with dignity is low (Duyan, 2014). In our study, the Cronbach’s alpha coefficient of the ASAPDD scale was .94.
GDS
GDS was used to determine nurses’ views on good death. This four-point Likert scale comprises 17 questions. The Turkish validity and reliability study of the scale was assessed by Fadiloglu and Aksu (2013), who determined that the Cronbach’s alpha reliability coefficient was .91. The total score on the scale ranged from 17–68. The higher the scores on the scale, the more positive the nurses’ perception of death (Fadiloglu & Aksu, 2013). In our study, the Cronbach’s alpha reliability coefficient of the GDS was .87.
Ethical Issues
To conduct this study, approval was obtained from the relevant hospitals and the university ethical committee (number: 16969557-1328, GO 15-640), and informed written consent was obtained from the nurses who volunteered to participate in the study. Additionally, permission was obtained by email from the authors who conducted the Turkish adaptation study of the scales used in the study.
Statistical Analysis
The Statistical Package for the Social Sciences software version 20 (SPSS-20) (IBM Corp., Armonk, New York, USA) was used for statistical analysis. Descriptive statistical tests of the variables were performed, and the Kolmogorov–Smirnov test was used to determine the normal distribution of the data. The non-parametric Mann–Whitney U test (Z table value) and Kruskal–Wallis H test (χ2 table value) were used to evaluate the data that were not normally distributed. The parametric independent t-test for two samples (t table value) and the ANOVA test (F table value) were used to evaluate the normally distributed data. Additionally, Bonferroni correction was used for binary comparisons. The analysis regarding the direction, significance, and degree of the relationship between measurement values was performed using the Spearman correlation method. The results were evaluated at a 95% confidence interval and a significance level of p < .05.
Results
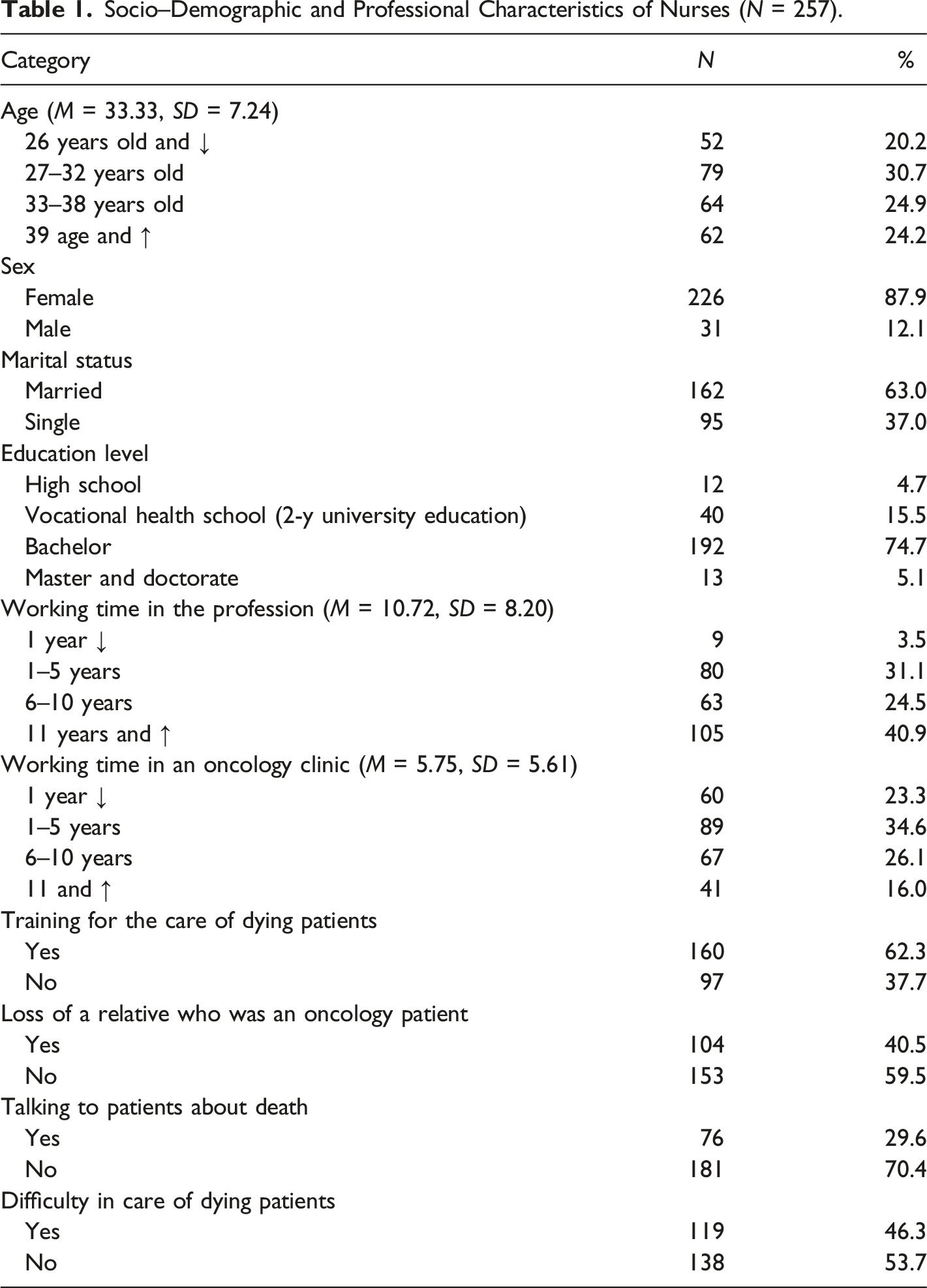
Socio–Demographic and Professional Characteristics of Nurses (N = 257).
Mean Scores of FATCOD, ASAPDD, and GDS.
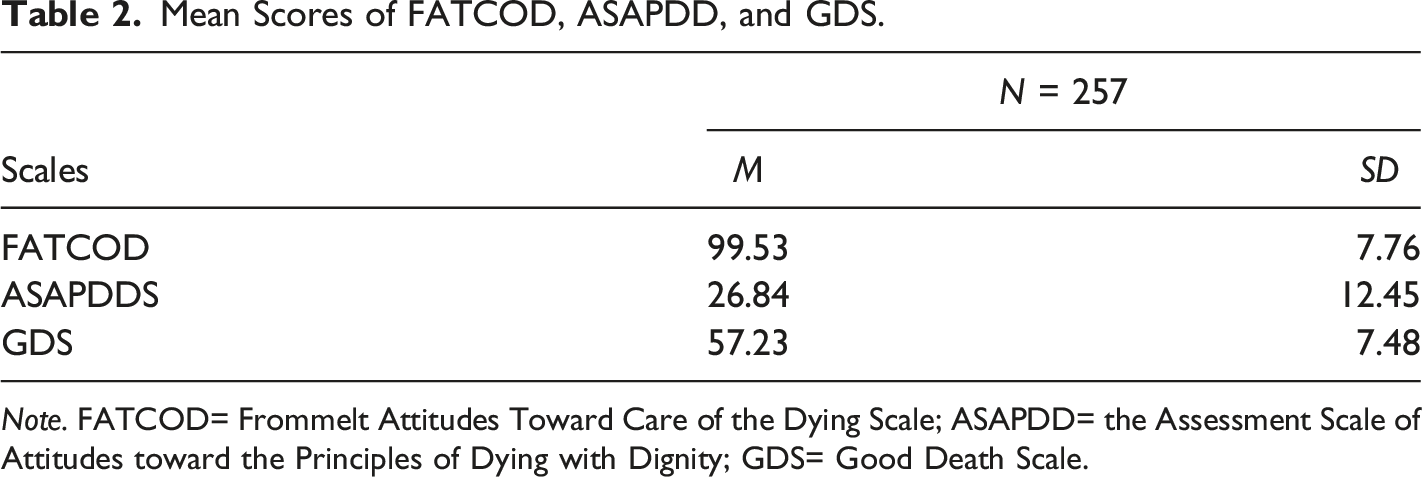
Note. FATCOD= Frommelt Attitudes Toward Care of the Dying Scale; ASAPDD= the Assessment Scale of Attitudes toward the Principles of Dying with Dignity; GDS= Good Death Scale.
Comparison of the Scale Scores According to the Socio-Demographic and Professional Characteristics of the Nurses.
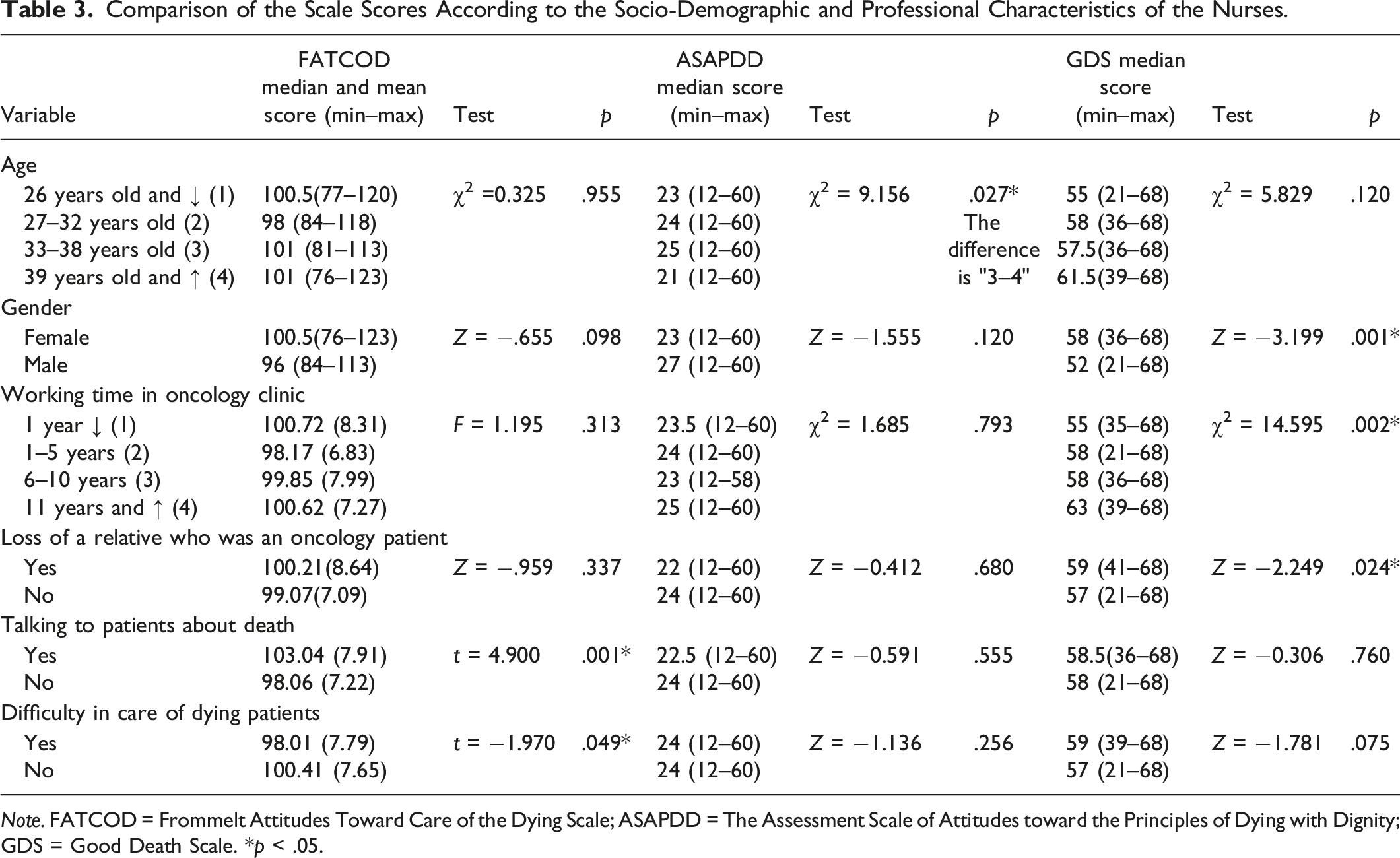
Note. FATCOD = Frommelt Attitudes Toward Care of the Dying Scale; ASAPDD = The Assessment Scale of Attitudes toward the Principles of Dying with Dignity; GDS = Good Death Scale. *p < .05.
Mean scores of ASAPDD were statistically significantly higher for nurses in the 33–38 age group than those in the 27–32 age group, under age 26, and above age 39 (χ2 = 9.156; p = .027) (Table 3).
Female nurses had a more positive perception of good death than male nurses (Z = −3.199; p = .001). Nurses working in the oncology clinic for 11 years or longer had a more positive perception of good death than nurses who had been working for less than 1 year, 1 to 5 years, and 6 to 10 years (p < .05). The median GDS of the nurses who had lost a relative to cancer were significantly higher than those of the nurses who did not lose a relative to cancer (p < .05) (Table 3).
Correlation Between FATCOD, ASAPDD, and GDS (N = 257).
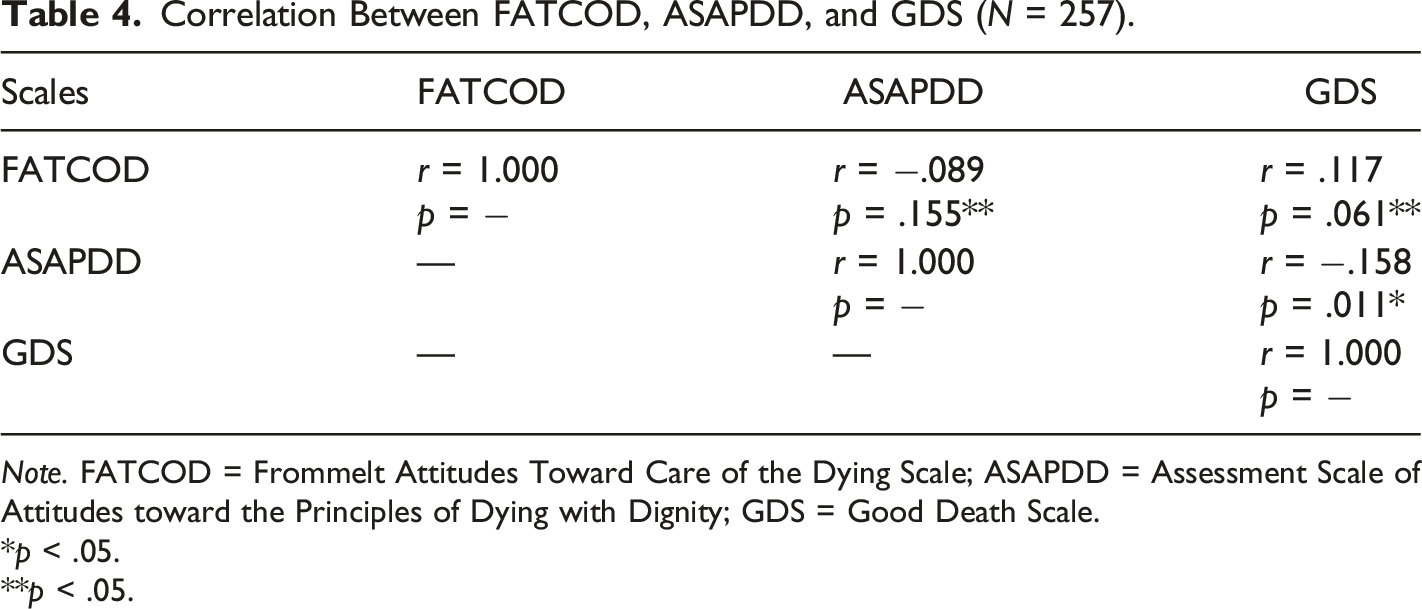
Note. FATCOD = Frommelt Attitudes Toward Care of the Dying Scale; ASAPDD = Assessment Scale of Attitudes toward the Principles of Dying with Dignity; GDS = Good Death Scale.
*p < .05.
**p < .05.
Discussion
Cancer is the most fatal disease after cardiovascular system diseases, and the mortality rate is high in oncology clinics that treat and care for cancer patients. Therefore, nurses who work in oncology clinics frequently face death and care for dying patients. To provide professional care, nurses need to understand their attitudes toward the care of dying patients. They should recognize the factors that affect their attitudes, reinforce their positive attitudes, and gain insight into changing negative attitudes to enable them to provide dying patients with a dignified and good death environment (Abudari et al., 2014; Andersson et al., 2016; Cevik & Kav, 2013; Choi et al., 2013; Gurdogan et al., 2017; Kinoshita & Miyashita, 2011). This study evaluated the attitudes of nurses working in oncology clinics toward dying patient care, the principles of dying with dignity, their views on good death, and the factors affecting them.
Our results showed that oncology nurses’ attitudes toward caring for dying patients were less positive than nurses’ attitudes reported in other studies (Abudari et al., 2014; Kinoshita & Miyashita, 2011; Tait et al., 2015) conducted using FATCOD. One possible reason for the higher scores in attitudes towards dying patient care in other studies is that these studies were conducted in different clinics using different samples such as palliative care and intensive care nurses. Henoch et al. (2014) demonstrated that the attitudes of hospice and palliative care nurses toward caring for dying patients are more positive than those of oncology and surgery nurses.
Nurses’ attitudes toward caring for dying patients influence the level of care they provide. Various factors have been reported to affect nurses’ attitudes toward caring for dying patients (Cevik & Kav, 2013; Dunn et al., 2005; Jeong et al., 2020; Khader et al., 2010; Lange et al., 2008). Our study reported that nurses who spoke to patients about death had more positive attitudes toward dying patient care than nurses who did not speak to patients about death. Cevik and Kav (2013) reported that nurses who did not talk to their patients about death and were unwilling to provide care for dying patients had negative attitudes toward dying patients. Further, Feudtner et al. (2007) reported that nurses who talk more comfortably about death with their patients provide better palliative care, and their patients had higher levels of hope.
Our study showed that nurses who had no difficulty caring for dying patients had more positive attitudes than nurses who had difficulty providing care for dying patients. Rooda et al., 1999 showed that nurses who did not avoid caring for dying patients had more positive attitudes than their counterparts. In the literature, it is emphasized that nurses who can talk about death while caring for dying patients and who do not have difficulty in caring for these patients have more positive attitudes toward providing care for dying patients (Cevik & Kav, 2013; Feudtner et al., 2007; Hasheesh et al., 2013; Mohamed Ali & Ayoub, 2010).
It is important for every individual to maintain their dignity during the last period of life. Therefore, nurses should provide attentive care to protect patients’ dignity (Demir et al., 2017; Gurdogan et al., 2017). In our study, the level of nurses’ adoption of dying with dignity principles was low. In other studies conducted with physicians and nurses working in intensive care units (Kose et al., 2019) and nurses working in internal, surgical, and intensive care units (Gurdogan et al., 2017) using the same scale, the level of adoption of dying with dignity principles by nurses was high. Nursing experience plays an important role in supporting the dignity care dimension of nurses’ roles, increasing dignity awareness, and gaining competence and confidence in this field (Cura, 2020; Gurdogan et al., 2017). This result is thought to be because nurses are less experienced in oncology clinics and providing care to dying patients.
In our study, nurses in the 33–38 age group highly adopted the principles of dying with dignity. Hasheesh et al. (2013) and Lange et al. (2008) found that nurses in the 20–29 age group were had a high fear of death and had negative thoughts about death, while nurses aged 40 and over showed an accepting approach to death. They showed that nurses in the 30–39 age group neither feared death nor accepted it. This result obtained from our study can be explained by the fact that nurses in the 33–38 age group do not have a negative view of death as in the younger age group, are not accepting death as in older age groups, but are more neutral perspective towards death, so they have a higher level of adopting the principles of respectable death.
The most important factor that demonstrates the success of end-of-life care provided to cancer patient is to ensure a good death process. Nurses play a key role in improving the quality of patients’ remaining days and preparing them for good death. However, they need to know and manage their own perceptions regarding good death to reduce their patients’ anxiety about the good death process and to be able to provide patient-specific care with the awareness that they have gained about good death (Becker et al., 2017; Ceyhan et al., 2018; Yang et al., 2019). Our study showed that oncology nurses had high mean scores on the GDS. Similarly, Ceyhan et al. (2018) performed a study to determine the good death perceptions of nurses working in the intensive care unit and found that the nurses had high GDS scores. As the level of education of nurses increase, they can acquire knowledge, psychosocial skills, and cultural sensitivity about good care of dying patient (Ceyhan et al., 2018). In addition, when the literature is examined; it is stated that people who lost their first degree relatives care more about, want and adopt good death (Krikorian et al., 2020; Menekli et al., 2021). The result obtained from our research can be associated with the fact that the majority of oncology nurses participating in the research witnessed the deaths of their relatives and gained empathy skills, and that they were constantly beside their patients during the death process and their awareness of good death increased. Therefore, it can be concluded that the sensitivity shown by nurses in preparing dying patients for good death has positive results.
In the literature, it is emphasized that female sex (Demir et al., 2017) and longer duration of professional experience (Beckstrand et al., 2006; Steinhauser et al., 2000) positively affected the perception of a good death among healthcare professionals. Similarly, our study determined that female nurses and nurses with a working period of 11 years or longer had a better perception of good death. Parry (2011) explained that nurses experience fear, increased anxiety levels, and lack of knowledge and skills when they first encounter death. However, the increased frequency of encountering death and interacting with dying patients positively affects nurses’ perception of death and their response to death (Lange et al., 2008). As the professional experience of nurses caring for dying patients increases, their fear of death decreases, and the acceptance of death increases (Hasheesh et al., 2013; Mohamed Ali & Ayoub, 2010).
Nurses exhibit a more positive attitude toward caring for dying patients if they spend time with long-term oncology patients and witness the difficulties experienced by these patients during their care than if they did not (Kavas et al., 2012). In our study, the nurses who lost a relative who was an oncology patient have more positive perceptions of good death than those who did not. This result suggests that losing a relative to cancer contributes to nurses’ ability to cope with death and understand the lives of dying patients and their families.
Our study showed a weak negative correlation between nurses’ level of adopting principles about death with dignity and their perceptions about good death. Ozkiris et al. (2011, p. 92) conducted a study in which physicians’ attitudes toward death and dying patients were examined; the authors reported that 70.1% of the physicians agreed that “Regardless of the disease diagnosis and prognosis, good death can be achieved by healthcare workers.” Demir et al. (2017) conducted a study with nurses working in intensive care and oncology units to determine their perceptions and experiences on “dying with dignity principles.” The authors reported that 75% of the nurses stated that dying with dignity principles were not applied in hospitals. Accordingly, the nurses believed that while good death can be achieved, incidences of applying the dying with dignity principles are low.
Based on the results of our study, the age, sex, experiences, and professional experiences of oncology nurses who want to reach expert level in caring for dying patients are essential factors in Benner’s model (Benner, 1982; Dunn et al., 2005). In line with this model, we believe that this study’s results will guide new oncology nurses in the training and practices required to care for dying cancer patients.
Limitations
This study cannot be generalized to institutions other than the institutions where the study was conducted and to nurses working in other clinics except oncology clinics.
Conclusion
The study results showed that nurses’ characteristics and experiences influenced their attitudes toward dying patient care, adoption of the principles of dying with dignity, and good death perception. When caring for cancer patients in the last days of life, ensuring a good and dignified death process should be considered. Further, initiatives to increase good death awareness among male nurses working in oncology clinics should be supported. In addition, we recommend that future studies examine the reasons for the lower level of oncology nurses’ adoption of dying with dignity principles and nurses who are trained and experienced in caring for dying patients should be employed at oncology clinics.
Relevance to Clinical Practice
This study is unique in that it examines and correlates oncology nurses’ attitudes toward dying patient care, their level of adoption of the principles of dying with dignity, and their perceptions of good death. It is expected that this study will increase oncology nurses’ attitudes toward dying patient care, and their level of adoption of dying with dignity principles, to guide necessary training, care protocols, and research to discover and develop good death perceptions and to raise awareness.
Footnotes
Acknowledgments
We are grateful to the oncology nurses who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.