
Abstract
Individuals bereaved by violent death have a higher risk of developing psychopathology. Consistent data concerning the subjective experience during the traumatic event of the death are still scarce. This study aimed to explore the traumatic experience of the violent death of a loved one. Nine reports of patients bereaved by violence were selected and transcribed. Reports were analyzed using Bardin’s Content Analysis. Two final categories were generated. It was observed that most participants remembered details about the traumatic event or the time they were told about the violent death. There were two factors described as important when coping with the loss, social support during the traumatic event, and receiving detailed information from the authorities and others present in that moment. This study provides relevant data for future interventions during violent situations by health and security professionals.
Introduction
Violent deaths, which include the cases of homicide, accidents, and suicide, are characterized by external factors that differ from death by natural causes. The suddenness can result in heightened suffering and clinical symptoms such as feelings of disbelief, confusion, and outrage, possibly, more so than the grief process following natural deaths (Kristensen et al., 2012). Individuals bereaved by violent death are often called survivors in scientific literature.
Several studies have described common responses to violent losses. These include shock, difficulty in accepting and believing the loss (Alves-Costa et al., 2018; Sharpe et al., 2013; Smith & Patton, 2016), rumination about what caused the death and how it could have been avoided and prevented (Djelantik et al., 2018; Johnsen & Dyregrov, 2016; Kristensen et al., 2012), as well as difficulty in attributing meaning to the loss and to the bereaved’s own life (Currier et al., 2006). A loss usually shatters previous assumptions about the world and life, which can interfere to reconstruct a meaning to a life without the loved one, complicating the grief process (Janoff-Bulman, 1992). Intrusive memories and images of the death and how it occurred are common response of survivors who did not witness the moment of death (Alves-Costa et al., 2018; Johnsen & Dyregrov, 2016; Kristensen et al., 2017; Omerov et al., 2014; Smith & Patton, 2016).
Research on trauma and grief has been develop in the past decade and many advances have already been made concerning these areas, such as mapping and diagnosing Prolonged Grief Disorder (PGD) or Persistent Complex Bereavement Disorder (PCBD), Posttraumatic Stress Disorder (PTSD), Major Depressive Disorder (MDD), and their comorbidities among survivors (Boelen et al., 2015; Djelantik et al., 2018; Heeke et al., 2017; Hu et al., 2015; Lenferink et al., 2018; Nakajima et al., 2012; Simon et al., 2007). However, findings are mostly exploratory and descriptive, and few studies investigate how these reactions and symptoms are individually experienced during the grief process.
Qualitative studies with survivors of violent death investigate mainly the grief process, contemplating emotional reactions, coping strategies, and social support (Alves-Costa et al., 2018; Johnsen & Dyregrov, 2016; Kristensen et al., 2017; Smith & Patton, 2016). These studies contribute to the ones focused on the diagnoses of psychopathologies. Nevertheless, data concerning specifically the exact traumatic moment of the death and the repercussions for mental health are scarce. Deeply learning about this experience would increase the understanding of the variables that can interfere both positively and negatively in the outcome of the trauma, which could be extremely useful for planning primary care strategies.
In addition, there is a lack of literature regarding how grief is manifested in different cultures and populations. A systematic review of the effects of death by homicide on surviving family members noted that 36 out of the 40 included studies had been conducted in high-income countries (Connoly & Gordon, 2014). Therefore, studies with population from other countries, regions, and cultures are necessary.
Thus, the aim of this study is to understand and describe the traumatic experience of losing a loved one by violent death. Specifically, we seek to understand how the survivors describe their exposure to the violent death of their loved one, how they express their grief and posttraumatic symptoms, and how they experience this event subjectively.
Method
This study is an excerpt from an umbrella project that seeks to evaluate posttraumatic reactions and the effectiveness of Cognitive-Behavioral Therapy protocols for the treatment of Posttraumatic Stress Disorder, conducted at a facility specialized in treating and researching individuals who were exposed to traumatic and stressful events. This facility is located at the second most populated city in southern Brazil and offers free care for these victims, who usually are in extremely vulnerable situations, often experiencing traumatic events on a daily basis from the region where they live or within their family context. All authors contribute in some way to research and care in the facility.
Audios of patients bereaved by violent death were selected, and the content analysis method was chosen to analyze them. This method was considered the best way to raise the largest amount of information about exposure to violent deaths and the grieving process in these cases without disregarding each individual’s particular and subjective experience.
Participants
Participants Characteristics.
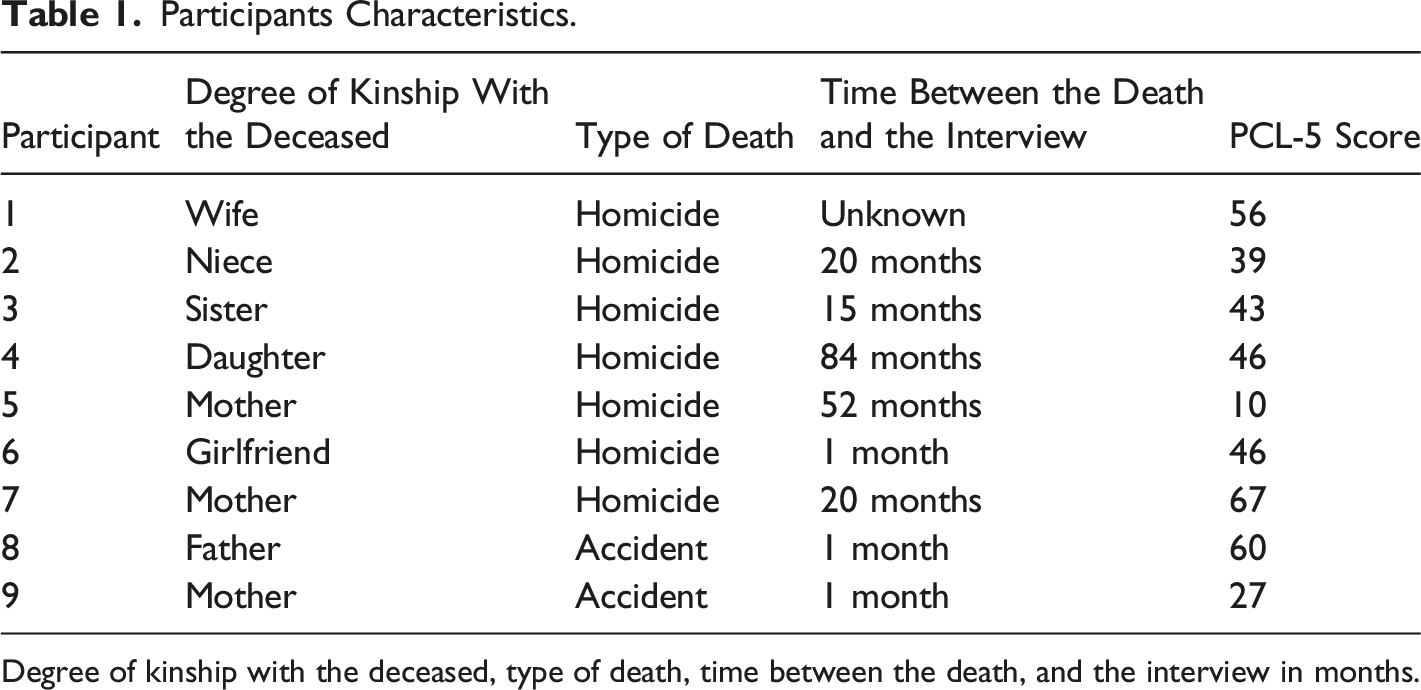
Degree of kinship with the deceased, type of death, time between the death, and the interview in months.
Data Collection Procedure
Upon entering the outpatient clinic, all patients underwent an assessment consisting of several instruments and inventories in order to assess symptoms of PTSD and other relevant information. Instruments selected for this study are described below.
Instruments
Trauma Interview: This semi-structured interview was developed for clinicians’ assessment in the aforementioned outpatient research clinic. It aims to investigate all lifetime exposure to traumatic situations. Also, individuals are asked to choose the worst event to answer questions about where the trauma occurred, who was with them, thoughts and feelings experienced in the time of the event, consequences for the individual’s health, and suicidal ideation. The interviewer asks the participant to report, in full detail, their traumatic event from start to finish, through a fixed statement: “Please describe the worst event in the most detailed way possible, identifying what you were feeling and thinking, your physiological reactions, and the worst part of it all”. This audio is recorded for later use during the treatment, especially if the patient goes on to receive prolonged exposure therapy. For this study, the audios of the selected patients were transcribed and subsequently analyzed.
Personal and Sociodemographic Data Sheet: The sheet consists of questions relating to age, sex, race, education, marital status, profession, and psychiatric history.
Posttraumatic Symptoms Checklist – Clinician Version (PCL-5; Weathers et al., 2014; Brazilian version by Limas et al., 2016): The PCL-5 is a self-report checklist composed of 20 items on a Likert-type scale ranging from 0 = nothing to 4 = a lot. The instrument aims to measure the severity of PTSD symptoms and provide a diagnosis according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorder (DSM-5; American Psychiatric Association [APA], 2013). Individuals who score more than 44 points are considered to have high symptoms of posttraumatic stress, and individuals who score 44 or less show minor severity in symptoms. Studies that evaluate the psychometric properties of the PCL-5 present good results, both in the analysis of internal consistency (α = 0.94) and test–retest reliability (r = .82, p <0.05) as well as a satisfactory convergent validity when compared to other measures of posttraumatic symptoms.
Analysis
A content analysis of the transcribed recordings was carried out without aprioristic categories according to Bardin’s method (2011). Recordings occurred prior to the definition of the method of analysis. Descriptive analyses were not carried out until the end of the qualitative process to reduce research bias.
The analysis process was divided into three main stages: pre-analysis, creation of content units, and, finally, the grouping of data into initial and final categories. For all stages, the transcribed and printed reports were read and analyzed individually by four researchers familiarized with the field of study and then as a group. All researchers had access to the audio of the transcribed report if clarification was required.
The pre-analysis consisted of a first-impressions reading of the material, without the goal of finding units of content, plus a second reading to identify recurring patterns in the content of the reports. The separation of these patterns into units was the next step and was carried out through group meetings. Still, in this second stage, the content units were reread after being named and, when necessary, redistributed.
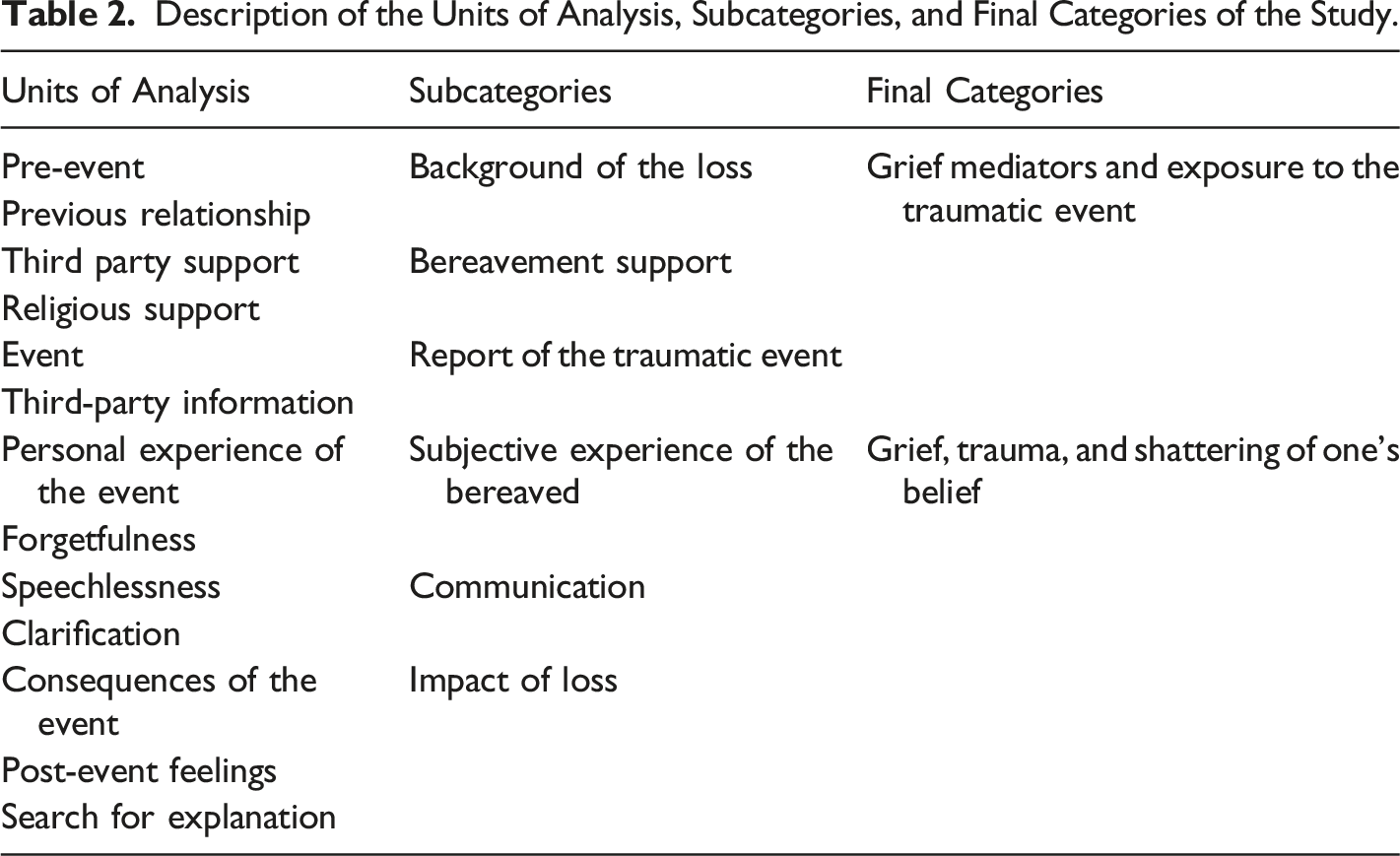
Description of the Units of Analysis, Subcategories, and Final Categories of the Study.
Ethical Considerations
This study was approved by the Ethics and Research Committee of the –[blinded for peer review] (protocol no. 1.438.437). Before starting evaluation, all patients from the facility signed an informed consent form in addition to a statement authorizing the audio recordings and agreeing to have their data and audio archived for future research.
Results
Due to the small size of the transcriptions, the path taken to the final categories used subcategories instead of initial and intermediate separately. Table 2 describes the analysis process conducted in the study.
Participant’s Scores in the PCL-5.
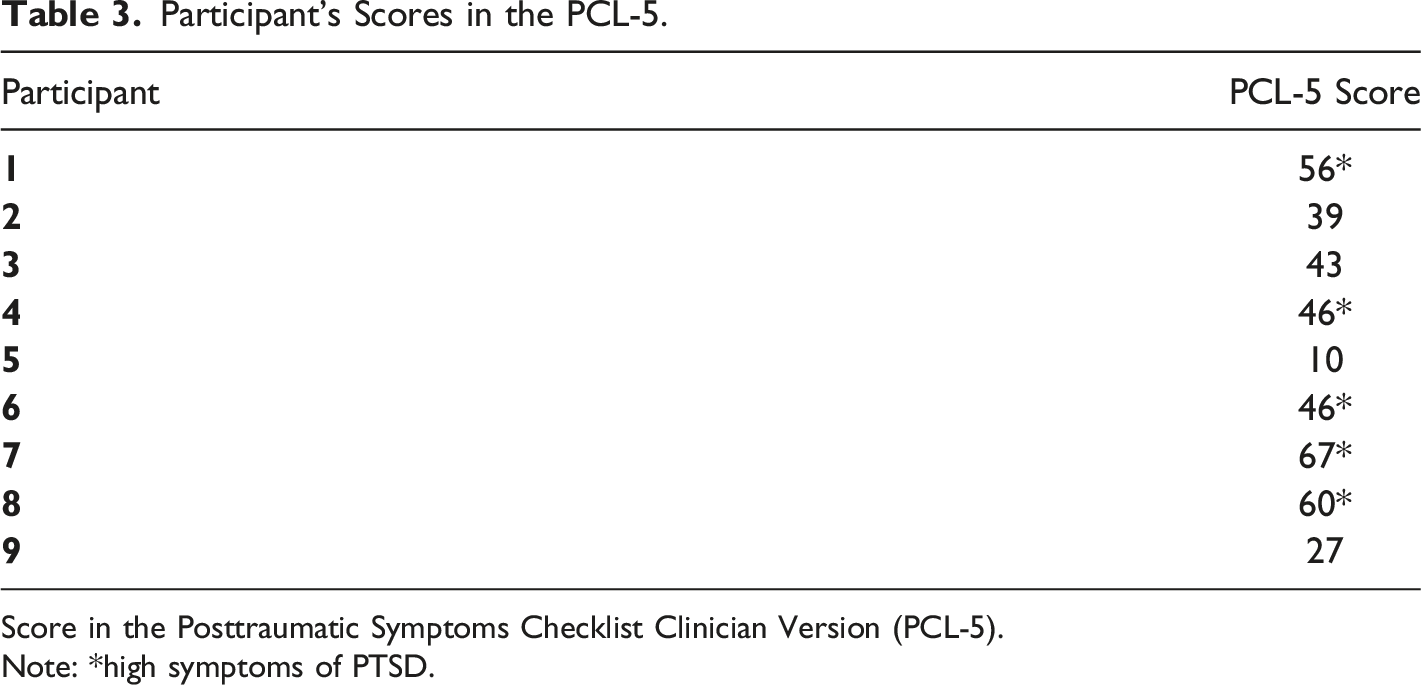
Score in the Posttraumatic Symptoms Checklist Clinician Version (PCL-5).
Note: *high symptoms of PTSD.
Grief Mediators and Exposure to the Traumatic Event
The category Grief Mediators and Exposure to the Traumatic Event covers the background of the loss, the support received and perceived by the mourner, and the report of the loved one’s violent death. The category received this name because, according to Worden (2013), both the past relationship between the mourner and the beloved and the perception of support received are important mediators of the grieving process. Exposure to the death, to the location where the death occurred, to mental image or to the news, photos, and information from third parties about the death can also impact on the reactions experienced by survivors (Kristensen et al., 2012; Smid et al., 2015). Thus, these subcategories were combined into a single final category.
Among the recorded audios, four participants reported on how their relationship with the deceased was before their death. One mother reported that even though her son was admitted to a clinic for substance abuse, they were very close to each other. When speaking about their last contact by telephone before the death, which happened after her son ran away from the clinic for drug addicts, Participant 5 recalls their dialogue: “I said to him, ‘Oh my son, all you do is bother’. Then he said to me: ‘Mom, I love you, mom I’ll never bother you again’ and then he didn’t call me anymore (...)”. Another mother also talked about her relationship with her son: “People ask me: didn’t you have any other purpose in your life besides your children? No, I didn’t. My children were my life’s purpose. The phrase that I used the most in my entire life was: my life comes down to before them and after them. I had no life before them”. (Participant 7, her son was murdered)
Participant 6, a young woman, mentioned the beginning of the relationship with her boyfriend, which was interrupted by his murder only a few months later. Another participant recounted the history of aggressions she experienced with her late husband, who was also murdered.
Four participants included in their report the support received at the time of the loss. Participant 3 witnessed the shooting in which her brother was killed and described the support she received from friends during the shooting, when taking her brother to the hospital, as well as when recounting the incident to her parents: “They tried to calm me down until the shooting passed a little. (...) Then, with my friends’ help, we managed to take him to the emergency room, but I didn't go with him, it was just my husband and my friends (...).”
Support was also perceived by a participant during the funeral, in which her brother helped with deciding the method of final disposition of the body. Religious support was also mentioned in two audios. Participant 1 sought out help in her church in the face of her domestic violence situation and, subsequently, after her husband’s death. Participant 5 mentioned her devotion to Saint Jorge: “Oh, I’m a devotee of Saint George (...)And always go (to visit the tomb), I made a beautiful panel for him, with Saint George, his photo”.
Only one participant (no. 2) reported the lack of support at the time of the death of her uncle, who was murdered by members of a drug trafficking faction: “I remember that nobody wanted to lift him off the floor, just me and my family”. In her case, her uncle was murdered with a firearm in the street in front of her house and no help was provided by neighbors due to the fear of retaliation by the faction: “I ran away, my mother told me to ask for help, I ran to ask for help to all neighbors, nobody wanted to help because it was the drug dealers who had killed him (…)”.
Only one participant (no. 9) did not have any memory from the moment of death, a car accident she suffered which resulted in the death of her four-year-old son. The traumatic event of death was recalled by eight participants in detail, including the time of the day, what they were doing, and who they were with when they witnessed the death or when they were informed of it. Participant 7 recalls that she was with her husband when she learned that her son had been murdered by mistake at a bus stop. “I was at home with my husband. Asleep. On a Sunday and ... my friend arrived, ok, telling me ... then, crying, uh, that he had died, that he had been murdered at a bus stop and ... that I needed to go to... (city where he died)”.
Three participants detailed the danger they were exposed to in the situation in which their family members died. All were exposed to gunshots: “Then I went with the people at Uxxx ... a couple who took a friend, as soon as we got there, you know, there was a fight and ... and then the shots ... And then I was in the middle of the crossfire”. (Participant 1, whose companion was shot and killed). “It was on a ... on a Sunday... we were… everyone was happy in my little sister’s birthday, so my uncle went to get more soda (...) then right after, there was a bunch of gunshots, one after the other, and everyone thought it was a bomb. When I went out to the street, I came across them shooting at my uncle (...) ". (Participant 2, uncle was murdered in front of her home). “It happened around 2 am, hum ... all I can remember is that a boy tapped my shoulder and said that my brother had been shot (...) we managed to get out of the club, except the shootout was still going on. Then we went out, we managed to see him there... and then my friends and my husband told me that we were going to have to go back to the club, because they’re still shooting, because if we didn’t (go back) they were going to kill us. Then we went back to the club” (Participant 3, brother was murdered in front of a club).
Participant 5 learned that her son was dead 3 days after his murder. For that, she was exposed to details of the death by third party, like Participant 7, who learned about the details of her son’s murder by witnesses of the scene. “The inspector left the room and I pulled out the folder and looked at the photos. He was prone, like this, collapsed, prone and sprawled out. (...) he was murdered on a drug den because, at the police station, they said it was because of 15 reais (a very small amount of money in Brazil), that he owed to that den, so he went in another one to buy the drug and they saw him and had him killed” (Participant 5, son ran away from a psychiatric clinic and was murdered in a drug den).
Participant 8 was in the car accident, along with his wife, which resulted in the death of their 4-year-old son. Participant 8 does not remember the whole accident, but he reports the following: “And then I woke up to the accident, they were tearing the door out of my car, right, and then I woke up and ran out of my car, I got up and ran out, I circled the car and saw them trying to resuscitate F(son), ok, on the side of the road on the ground and then trying to revive him ... I could see from that, that he was already ... already, already dead (...) I remember everything, you know ... we were talking inside the car and he was sleeping in the car seat ... everything, the crash, the pressure of the impact, everything. I remember everything (...)”.
Grief, Trauma, and the Shattering of One’s Belief
The category of Grief, Trauma, and Shattering of One’s Belief covers aspects of the subjective experience when witnessing or learning about a loved one’s violent death, how the participant communicates, and the impact of the loss on their lives. The name of the category was chosen based on the knowledge that death is a potentially traumatic event, especially a violent death, and that it can significantly impact on previously held conceptions about how the world and life operated (Alves-Costa et al., 2018; Dyregrov et al., 2016; Kristensen et al., 2017; Kristensen et al., 2012; Neimeyer, 2002; Worden, 2013).
Two participants reported the need to understand what happened and find explanations for the death of their loved ones. Along with this search for answers, feelings of anger, guilt, and regret for what was and was not said were displayed: “I felt really bad about it. That’s what hurts me the most, like, it’s ... Hum ... that ... I feel guilty. Extremely guilty. It’s a guilt that I want to resolve. I need to resolve this. It’s a very big pain” (Participant 1). “Then we carry that ... that outrage, that ‘why’, that ‘if’ and ... it’s something that we have no explanation for. We don’t understand why it happened since we did nothing wrong and then that self-demanding and thoughts it’s, this is .... It’s unfair (…)” (Participant 9).
The absence of a loved one is also recalled as an important part of the traumatic event: “The worst part is, it’s the day-to-day, it’s sleeping and waking up and not being together, it’s doing things that remind me of him” (Participant 9).
Another interesting aspect of the reports was the difficulty in expressing the traumatic experience of the death in words. Many participants found it challenging to complete sentences: “I ... ah, talking about it, it gives me ah ... it’s complicated” (Participant 1). Others expressed not being able to find words that could describe their experience: “(...) like, I don’t know, I can’t explain” (Participant 4). In addition, two participants found it difficult to remember important parts of the event: “I, I don't know, like, details, exactly hum, what to remember, you know?” (Participant 9) and “(...) as I told you before, I kind of deleted this part, you know, I forgot this part” (Participant 7).
The subjective experience of personally witnessing the death was felt by five participants intensely. Participant 3 who saw her brother being shot in front of a party says that: “then I was in shock, how was I going to tell my mom and dad? (...) but it was really ... really ... really horrible like... a horrible feeling”. Participant 1 also reported about the experience of witnessing her husband’s death: “that, when I saw that, I was very frightened. I even thought I was going to die with him, right. Then, when I saw him fallen on the ground, I wanted to ask for help and I couldn't do it”.
Those bereaved who did not directly witness the death recalled their experience when hearing the news. Participant 6, whose boyfriend was murdered, mentioned the shock and difficulty in accepting the loss and believing it was real. “So, like, I felt like I needed to just stay in a corner, like in a square meter like that and do not leave that corner because it seemed that if I moved, I don't know, I would live more in that story (...) I couldn’t believe he died, you know? I needed to see it (…) I wanted more people to tell me that he had died because I couldn't believe it”.
The importance of having information about how the death occurred to be able to construct a memory of the sequence of events was also mentioned by Participant 6: “(..) so I keep wondering how he died. Because nobody wanted to show me the photo, so I wondered what the photo was like. And, it’s really awful because, then, all I could think was like some tragic scenes, like that, and I think I wanted to see the photo (...) I wondered how he was in the photo and wondered if, I don't know, if he had suffered, if it was quick”.
Survivors whose first contact with the death of a loved one happened at the funeral focused their report on this experience. Participant 7 saw her son’s body for the first time during the wake, and retells the shocking experience: “I wasn’t thinking about anything, I didn't think, I couldn't reason, I couldn't stop seeing one of them in the coffin and the other one (youngest son) crying and kissing his brother desperately, I couldn't see that”.
The effects of exposure to a trauma were reported by some participants. Participant 5 comments the following: “There are certain things that stun me, people’s voices stun me (…)”.
Faced with re-experiencing symptoms, such as memories of the death, Participant 1 comments the following: “If I could, I would erase it from my head, if I could I’d erase it”. Participant 8 talks about nightmares and triggers that elicit the same experience, making him relive the traumatic moment: “From then up until today, I feel at night the impact of the car crash, right ... and I see ... I see him on the floor there, being resuscitated, I see that image, sleeping, and I... and in the impact, I wake up with the impact of the crash at night. (...) If I see a car on the street the color of that truck I... I already think about the accident, If I see a car of the brand that I had, I already think about the accident, anything there is, that happened on the day of the accident, the accident comes back immediately, like that”.
Discussion
The main purpose of the study was to understand how the participants lived their traumatic experiences. The content analysis conducted on the reports provided two final categories that contained important data about losing a loved one by violent death, such as the vivacity of the remembered details, even after a long time since the death, the importance of getting information about the death, and receiving social support during the event. It is important to notice that the participants were struggling with the violent loss, which led them to seek professional help in a specialized service.
Exposure to the event that culminated in the death of a loved one or to the news and information about the death was reported in detail by eight participants. This factor points to the relevance of the way the exposure occurs in each traumatic experience, which is in line with previous findings regarding the association of the exposure to the event that led to the death and third parties' reports, as well as images of the traumatic event, with the development of PTSD (Baddeley et al., 2015; Boelen et al., 2018; Nickerson et al., 2014; Smid et al., 2015). Other qualitative studies with bereaved by violent death have also pointed to the presence of intrusive memories of how the death occurred, even with those who were not directly exposed to the incident. (Alves-Costa et al., 2018; Kristensen et al., 2017; Smith & Patton, 2016).
Participant 8, who was driving the car in which his son died and saw him being resuscitated, scored 60 points on the PCL-5. This elevated score is in line with his story, marked by nightmares, intrusive memories, and frequent symptoms of re-experiencing the trauma caused by triggers associated with the day of the accident, such as cars. These are classic symptoms of PTSD (APA, 2013), which can arise as comorbidity with grief and CG (Kristensen et al., 2012; Lenferink et al., 2018). It is important to notice that grief involves longing symptoms, yearning, and emotional pain, while in PTSD, symptoms are associated with the circumstances of the death, such as the exposure to the moment of the death or to the death scene or the body, or even after third party reports and images from the media (Baddeley et al., 2015; Heeke et al., 2017; Kristensen et al., 2012; Neria et al., 2007; Omerov et al., 2014). In the case of participant 8, intrusive thoughts and memories are related to the exposure to the death of his son and, thus, characterizing a PTSD condition.
Significant PTSD symptoms related to the child’s wake were manifested by Participant 7 (score 67 on the PCL-5), especially related to seeing and being exposed to the body of her son. This was also observed in a study with parents who lost their children to suicide, which found that those who viewed the body in a formal setting were significantly more at risk of having nightmares and intrusive memories than those who only viewed at the site of the death and those who chose to not see it at any time (Omerov et al., 2014). The relationship between seeing the body in different settings and the outcome of CG and PTSD is still unknown, as few studies had dedicated to this investigation (Badenhorst & Hughes, 2007; Hu et al., 2015; Ogata et al., 2009; Omerov et al., 2014). However, these findings contribute to the reflection about the need of primary care interventions in formal situations related to death
Similarly, participants who did not personally witness the death reported ruminative and intrusive thoughts about how it occurred and whether their loved one suffered, expressing the need to obtain more information to be able to firmly believe that the loss occurred, as it was the case of Participant 6, who mentioned her desire in seeing photos taken of her boyfriend’s dead body. This pattern was also observed in a study of Kristensen et al. (2017) with families who lost their children in a terrorist attack. This reinforces the importance of receiving information for constructing a narrative and a memory about what happened and caused the death.
The difficulty in constructing the memories in order to understand how the death occurred seems to connect with the feeling of unrealness, which was emphasized in some reports, such as the one of Participant 6. This feeling is common in sudden deaths, which may be accompanied by extreme outrage because of the violent and abrupt way the separation occurred (Worden, 2013), which was demonstrated by Participant 9, who described her outrage when faced with the death of her 4-year-old son in a car accident. The particularities of violent death, such as the suddenness and the exposure to violence, tend to shatter assumptions about the world and life more strongly, which make this type of loss incredibly painful and difficult to find a meaning for this experience (Alves-Costa et al., 2018; Bellet et al., 2018; Janoff-Bulman, 1992; Sharpe et al., 2013; Smith & Patton, 2016).
Some participants mentioned the received support in their reports of the traumatic event. Both people who provided emotional support as well as who provided directed support toward trying to rescue the deceased and taking charge of making difficult decisions about the wake were mentioned. Research studies show that the presence of social support from family and friends is essential for those bereaved by violent death, especially in homicide cases, as it helps in the face of stigma and feelings of guilt and shame (Englebrecht et al., 2016; Hibberd et al., 2010; Thompson, 2007). Religious support was also mentioned in two audios. The use of religion and spirituality as an adaptive coping strategy provides comfort and hope (Alarcao et al., 2008; Da Costa et al., 2017; Domingues et al., 2011). However, to our knowledge, our study is the first to investigate the support in the moment of the death, and reports demonstrated the positive impact of the support when it is received, and, also, the scars that the lack of support leaves.
It is relevant to consider the pattern of vulnerability in the sample of this study. The majority of participants have low education and low socioeconomic status, living in violent neighborhoods in a country known for its urban violence. These are subjects who continue to be exposed to situations of violence due to their environment, which makes them prone to use avoidance as their main coping strategy. All of these factors are known to pose a risk to the development of psychopathologies and complications in the grieving process (Burke & Neimeyer, 2013; Smith & Patton, 2016). Additionally, the violence that permeated some deaths, especially the ones linked to drug trafficking and/or use, may entail this grief to be disenfranchised by society and sometimes by the person itself who is suffering (Doka, 1989). The suffering experienced by the bereaved is stigmatized and strong feelings of shame and guilt can emerge. As a result of the stigma, these survivors tend to isolate themselves and avoid social interaction. The son of the Participant 5, a drug user, was killed in a drug den and, as a consequence, her grief is at risk of being disenfranchised by her community.
Last, the experience of having a loved one ding in a violent way is shown to be traumatic thought the speechlessness of the survivors in their audios including the inability to find or finish words and sentences. Witnessing the death or knowing how it happened, as well as the sudden absence of a loved one, made it difficult for the participants of the study to properly recount their experience, forcing them to use expressions such as “I don't even know what words to use to describe what I felt”.
Strengths and Limitations of the Study
Some limitations of this study must be discussed. First, this study was conducted only with a clinical sample. The small sample of survivors and its specificity limit the generalization of the findings, especially for those who did not seek professional help. The access to information about the participants’ experience was limited to the pre-recorded audios, as there was only one short report per individual, and the researchers could not supervise the interviews. The transcriptions were translated into English, in order to fit in the article. The authors made the greatest possible effort to adapt the language to English, but it is understood that slang and cultural expressions may have been lost. However, this is considered a minimal loss for understanding and discussing the data.
Furthermore, the sample only included bereaved by homicide and accidents, with no cases of suicide being reported. This factor, as well as the fact that most of the sample was composed by women with low degrees of education, drastically reduced variability. This study also did not focus on the traumatic experience of each specific type of death. However, this was not our aim; instead we sought to assess in general the traumatic experience of losing a loved one in a violent way. To the best of our knowledge, this is the first study in Brazil that intended to evaluate the traumatic experience of exposure to the site of the death, reports, images, and information about violent death in a qualitative way, and our findings may contribute to future studies with this population.
Conclusion
This article contributes to a better understanding of the experience of direct exposure to violent death as well as news and images about the event. The content analysis allowed looking at the subjective and individual experience of the trauma for each participant, punctuating differences, but also similarities.
The sample presented evidence that the social support of friends and family is extremely important at the time of a loss. This data is especially useful for professionals who are faced with these traumatic events in their line of work, since, with this knowledge, they can seek measures to make sure the victims receive the necessary support. Another essential lesson, which has already been reported in previous studies (Dyregrov et al., 2016; Kristensen et al., 2017), is the need for survivors to receive information about the death, an issue that should also be considered by professionals during their practice with situations of violent death. This information validates the importance of crisis interventions, such as Psychological First Aid, which aims to alleviate the impact of traumatic events and help mobilize adaptive coping strategies and social resources for the survivor as a supportive network (Castillo-Varela & Gil, 2019; Comisi n Nacional de Derechos Humanos, 2010). We also believe the study is relevant to discuss governmental policies of primary care for these survivors, especially in Brazil, where it was conducted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.