
Abstract
This study surveys the differences of relatively healthy proponents of end-of-life choices and people with irremediable health conditions having already made the decision to hasten their deaths on what each group considers important in influencing a desire to hasten death. Psychosocial factors were more important than physical ones for both groups; but those contemplating what might influence them to hasten their deaths in the future thought pain and feeling ill would be much bigger factors than they turned out to be for those deciding to do so. Those having decided to hasten their deaths cited the lack of any further viable medical treatments and having to live in a nursing home as bigger factors. Identifying these psychosocial factors influencing a desire for a hastened death suggests that caregivers and medical providers may want to review what compassionate understanding and support looks like for people wanting to hasten their death.
Introduction
Since Derek Humphry’s best-selling book in 1991, Final Exit: The Practicalities of Self-Deliverance and Assisted Suicide, public opinion on terminally ill patients seeking a hastened death has moved from wildly controversial to enormous public support, including now the majority of physicians (Humphry, 1991; Kane, 2020). After initial concerns about potential harmful consequences for vulnerable populations proved unfounded (Lindsay, 2009; Albaladejo, 2019), more and more countries and states are passing legislation to support the public’s interest in being able to have control over the manner and timing of their own death when faced with irremediable health conditions. Final Exit Network (FEN) is one of the organizations in the United States, alongside ten (and growing) state approved medical-aid-in-dying options, and other domestic and international groups and countries, that support end of life options. Examples of these organizations include Compassion and Choices, Death with Dignity, Dignitas, Exit International, and the World Federation of Right to Die Societies. These programs continue to grow in number and provide resources for those seeking information about how to achieve a peaceful death rather than a drawn-out process of increasing frailty, violent gun options, or loss of quality of life and autonomy due to health conditions over which they otherwise have little or no control (Bellamy, 2017). Seniors ages 85 and older had the second-highest suicide rate in the United States in 2018, and firearms were used in 70.0% of them among seniors aged 65 and older (America'sHealthRankings, 2021; Mertens & Sorenson, 2012). State-sponsored physician-aid-in-dying programs and informational organizations like the ones we have mentioned above aim to offer elders and others with intractable health conditions peaceful options when it comes to controlling their deaths.
There have been multiple studies seeking information from doctors, families, and patients assessing why people who use state sanctioned physician-aid-in-dying programs have chosen to hasten their deaths as well as studies of people’s emotions who are dying of terminal illnesses without such choices (Ganzini et al., 2008b; Hendry et al., 2013; Hudson et al., 2006; Singer et al., 1999). Central to these investigations has been the value of a person’s autonomy over both their life and death decisions, complicated sometimes by mismatches between provider and patient knowledge, lack of effective communication, familial, financial, demographic and social factors, or outside constraints on patients’ real options (Meier & Morrison, 2002; Winzelberg et al., 2005). There have been efforts to identify cognitive, emotional, relational, and values-based needs that go into autonomous decision making at the end of life, and our current study further adds to that identification process (Callahan, 2002). Our current study further delineates the factors that go into what previous studies have generally concluded are the main reasons people wish they could hasten their deaths in the face of progressive illness or frailty. These factors included not only the sense of loss of self and dignity associated with autonomy, but also an inability to participate in activities that make life enjoyable and a generalized global feeling of intolerable or unbearable suffering (Chochinov et al., 2005; Dees et al., 2011; Ganzini et al., 2009; Rodríguez-Prat et al., 2017).
Our current study compares the view of relatively healthy people who are professed supporters of end-of-life options with irremediably ill people who have already decided to hasten their deaths. We wanted to know whether those who are actually suffering from intractable health conditions and faced with end-of-life decision making may differ in their views from relatively healthy people who are thinking about the questions hypothetically. We sought to understand what factors were most important to each of these groups by asking each group to rate the importance of several physical, cognitive, social, and emotional factors in influencing their current thoughts on why they would hasten their deaths.
Methods
Questionnaire Development
We devised a Quality-of-Life Impact Scale (QLIS) to inquire about physical, cognitive, emotional, and social issues that might be related to people wanting to hasten their death. These questions were informed by previous discussions the organization had with people seeking information from FEN about hastening their death. The QLIS consists of 13 questions: 4 regarding physical challenges and symptoms, 2 regarding cognition and memory, 3 regarding emotional perspective, and 4 questions regarding social and family support issues.
As a starting point, we used some of the metrics previously devised by frailty scales for our QLIS development (Drubbel et al., 2013; Gobbens et al., 2020; Rolfson et al., 2006). Historically, the focus of frailty scales has been to provide an overall rating of a person’s fitness, but have evolved in application primarily to predict future adverse medical events, functional decline and death, and used for the purpose of preventing those outcomes where possible through appropriate treatment strategies (Fehlmann et al., 2021; Juma et al., 2016; So et al., 2018).
Our QLIS questionnaire incorporates some self-rating factors found in frailty scales, but includes more psycho-social factors, and it changes the purpose and framework for asking the questions (Table 1). It asks how strongly these physical, cognitive, emotional, and social factors influence people to want to hasten their death, rather than how these factors can lead to further treatment planning and the prolongation of life. While incorporating more psycho-social questions, the QLIS recognizes the inseparability and impact on each other of physical, emotional, cognitive, and social factors that lead to wanting to hasten one’s death rather than trying to measure primarily emotional impact alone (Julião et al., 2020; Rosenfeld et al., 2000).
Factors Influencing a Potential Desire to Hasten Death.
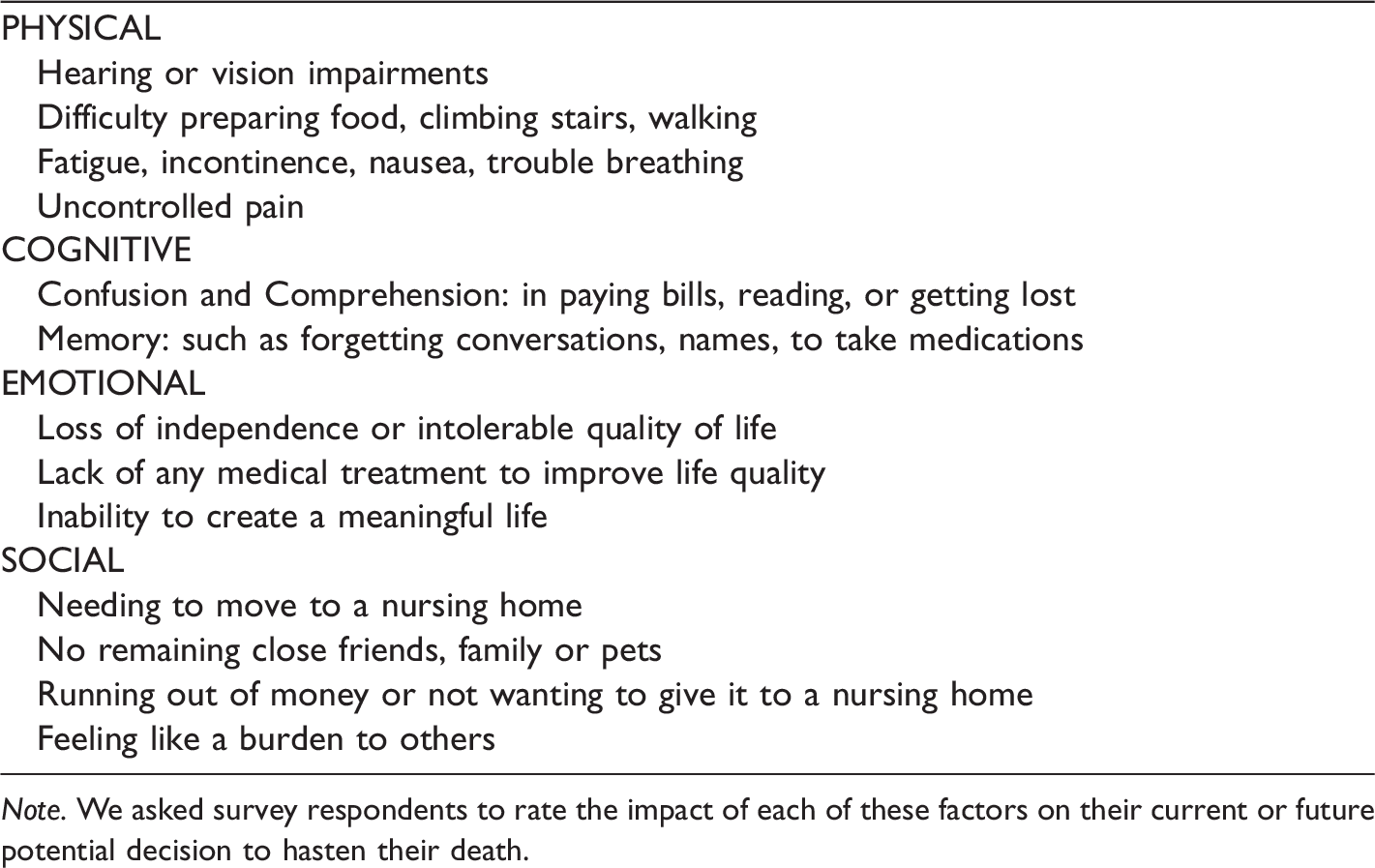
Note. We asked survey respondents to rate the impact of each of these factors on their current or future potential decision to hasten their death.
We devised two forms of the questionnaire with slightly different language to reflect those who were predicting “What Factors Might Lead Me to Consider a Hastened Death” (the “supporter group”) and those who had already decided to hasten their death by going through the rigorous FEN medical screening process to obtain publicly available information on how to do so (the “decided group”). We asked respondents in the decided group to rate each factor as “Not a Problem”, “Mild or Moderate Problem”, or “Big Problem” based on their current symptoms and situation. We asked respondents in the supporter group about the same 13 factors with slightly different wording for those contemplating what issues they thought would influence their desire for a hastened death in the future. This supporter group was asked to rate each factor as of “Less Significance”, “Moderate Significance”, or High Significance”. We made these slight changes to the wording of the three response choices for each question in order to reflect the responder’s current situation in the applicant decided group and the future expected importance of each issue in the supporter group. The content of the questions remained the same, and we believe the two versions of the survey are equivalent and appropriate for each group’s time position, immediate or future, in relation to deciding to hastening their death. In addition to the QLIS we asked demographic questions including age, education level, religious/spiritual identification, and recorded general categories of medical diagnoses for those in the decided group.
Data Collection
Final Exit Network (FEN) is a 501(c)(3) non-profit organization founded in 2004, based in Florida and serving people throughout the US. The organization provides publicly-available information on peaceful and legal options to control one’s own death to those who are suffering from intolerable medical circumstances, are mentally competent, want to end their lives, and meet strenuous application criteria. The participants in this study are either supporters of the organization who receive its newsletter or those who have gone through the application process to receive information on hastening their deaths. Many of the individuals who eventually apply for specific information from the organization about options for hastening their deaths are already members of the organization.
We solicited participation in the QLIS survey from FEN members through the Summer 2020 Final Exit Newsletter, all of whom by their membership are presumed to be supporters of having choices about hastening their own death if their health conditions ever become intolerable. This supporter sample group is comprised of the 341 returns of the QLIS questionnaire that was included in the newsletter sent to the approximately 2,500 members of FEN. The decided sample group is comprised of the 59 people who had filled out the QLIS after deciding to hasten their own death and were seeking information on options for peacefully doing so by completing FEN’s extensive screening application process. We informed all participants that no personal identifying information would ever be published about their responses and used anonymized data in all subsequent analysis.
Statistical Analysis
In addition to the raw data from the QLIS survey we also calculated category scores for physical, cognitive, emotional, and social factors by dividing the sum of the respondents’ ratings for each section by the total possible score for each of these four sections, producing a value between 0 and 1 for each category. We also calculated total QLIS scores by adding responses for all 13 questions. We used logistic regression models to compare responses between the supporter and decided groups. We used Wilcoxon rank sum tests to compare QLIS category scores between groups. We conducted statistical analyses using JMP Pro 15.
Results
Our respondents ranged in age from 20 to over 100 for the supporter group and from 30 to 90 s for the decided group. For both groups 70–79 was the median age bracket, with respondents in their 70 s comprising 40% of the supporter group and 32% of the decided group. Both groups also tended to have a high level of education, with a large number of respondents possessing a graduate degree (supporter= 56%, decided= 49%).
As in previous studies, the religious or spiritual identification of both the supporter and decided groups were skewed heavily towards non-deist spiritual identifications or secular views (supporter= 69%, decided= 49%). For the decided group medical diagnoses included cancer (30%), serious kidney, pulmonary or heart disease (8.9%), chronic pain (5.3%), dementia (14%), neurodegenerative diseases (20%), and a constellation of diagnoses (20%).
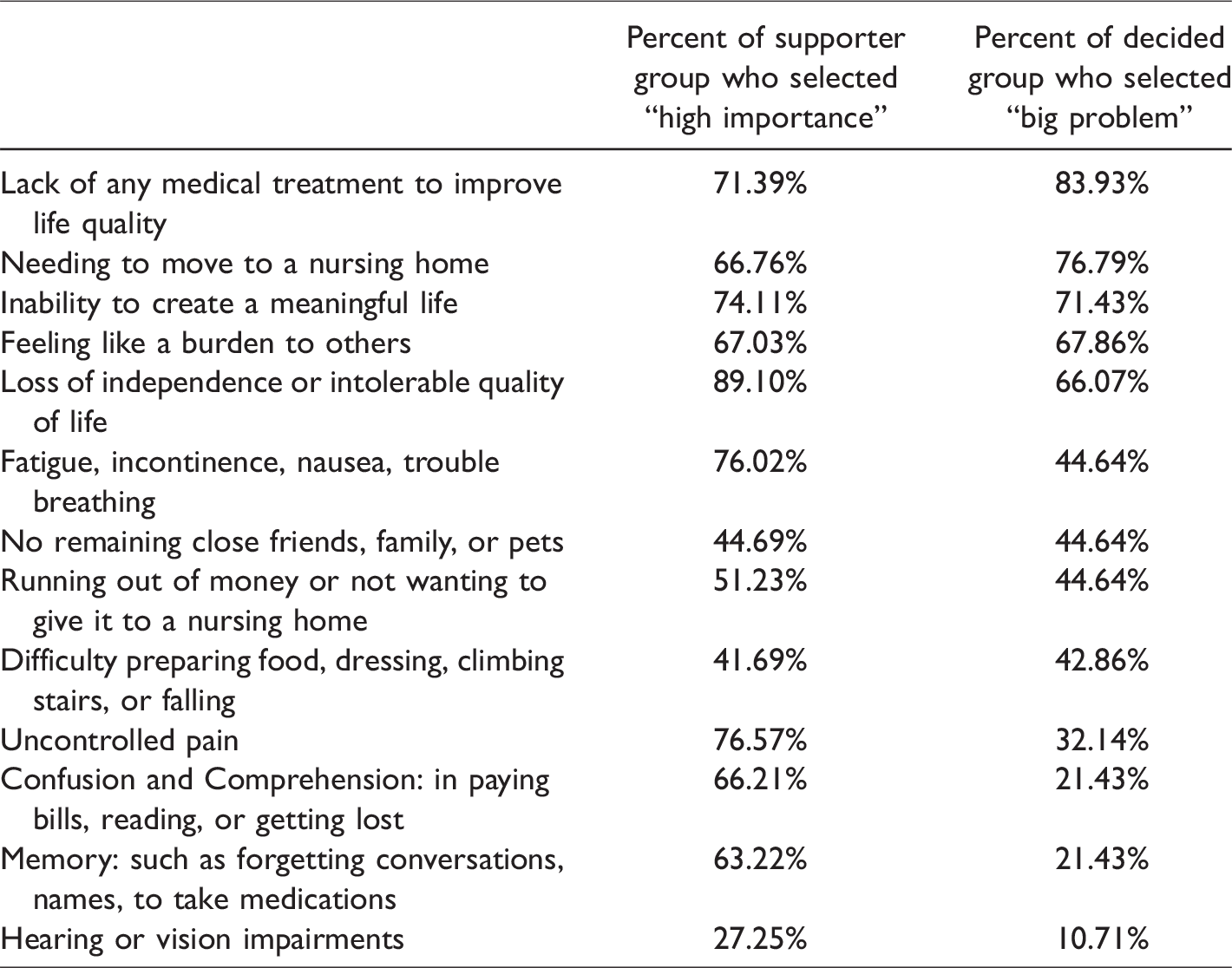
We found that lack of any further treatment to improve their quality of life was ranked as a big problem by more decided respondents than any other factor (Table 2). For the supporter group, more people rated loss of independence or an intolerable quality of life as of higher importance than any other factor they thought would lead to their decision to hasten their death. Of all the factors, impairments in hearing or vision was least often rated as very important, and this was true for both groups of respondents.
Importance of Various Factors in Considering a Hastened Death for Supporter and Decided Groups.
On the thirteen issues potentially affecting their decision to hasten their deaths there were no statistical differences between the supporter and decided group on five of the factors (Table 3). Both groups felt that decline in their vision and hearing was only mildly important in their decision making. There was also no statistical difference between the two groups on the importance of not having remaining friends and relatives, or on running out of money or not wanting to give it to a nursing home, with about half of both groups rating these as highly influential factors (Table 2). The inability to continue creating a meaningful life and feeling like a burden on loved ones was, important to more than two thirds of both groups, with no statistical difference between the groups (Table 2, 3).
Analysis of Differences in Survey Responses Between the Supporter and Decided Group.
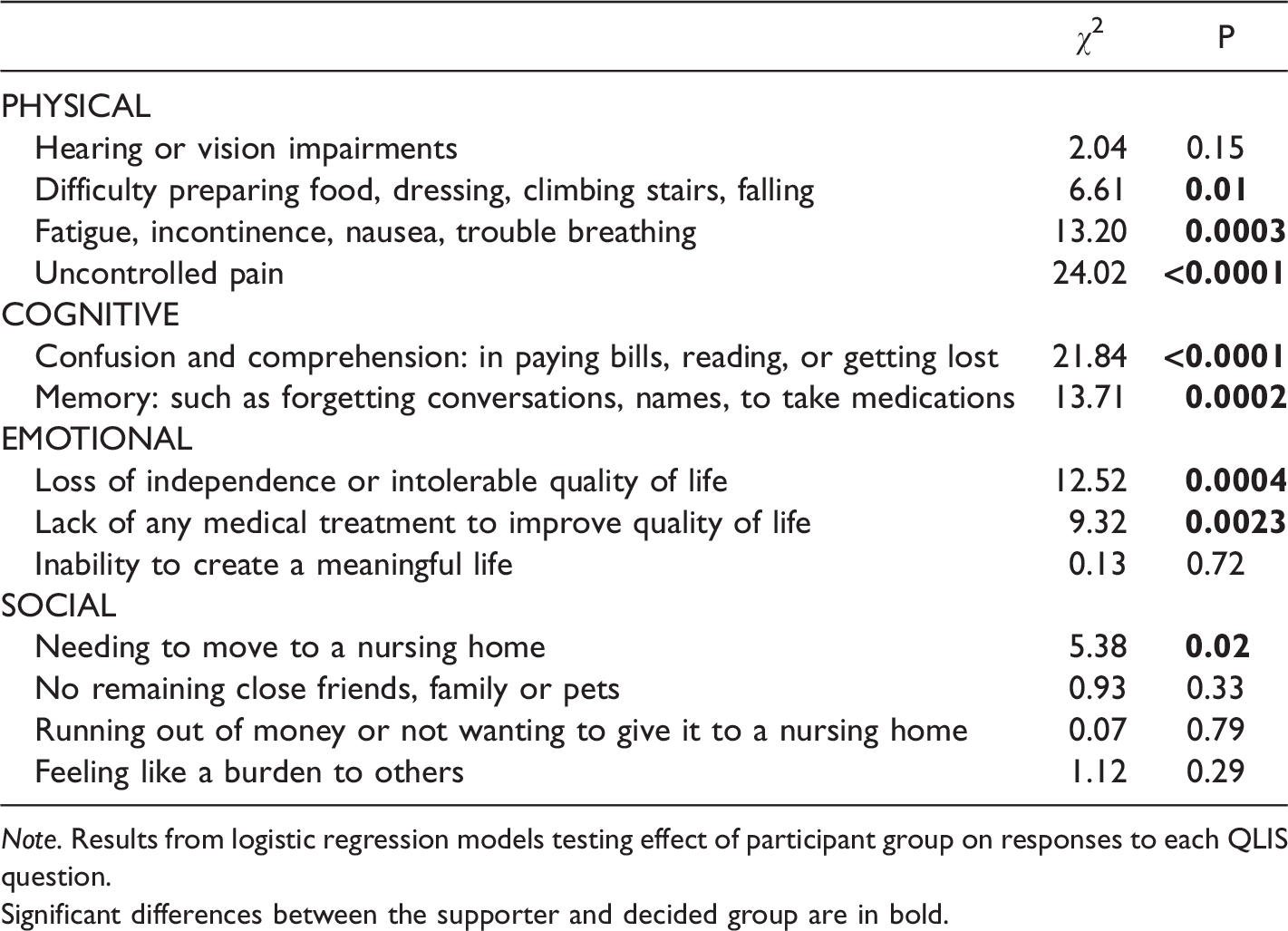
Note. Results from logistic regression models testing effect of participant group on responses to each QLIS question.
Significant differences between the supporter and decided group are in bold.
There were statistically significant differences between the supporter and decided group for the other eight factors (Table 3). People predicting what would be important to them in deciding to hasten their death in the future thought feeling ill on a daily basis (nausea, fatigue trouble breathing, and/or incontinence), uncontrolled pain, confusion, memory problems, and lack of independence and an intolerable quality of life would be more important than it turned out to be in the group of people who actually came to the decision to hasten their death. Even though 66% of the decided group still cited lack of independence and an intolerable quality of life as a “big problem”, 89% of the supporter group predicted this would be a major influencer when they made a decision about hastening their death.
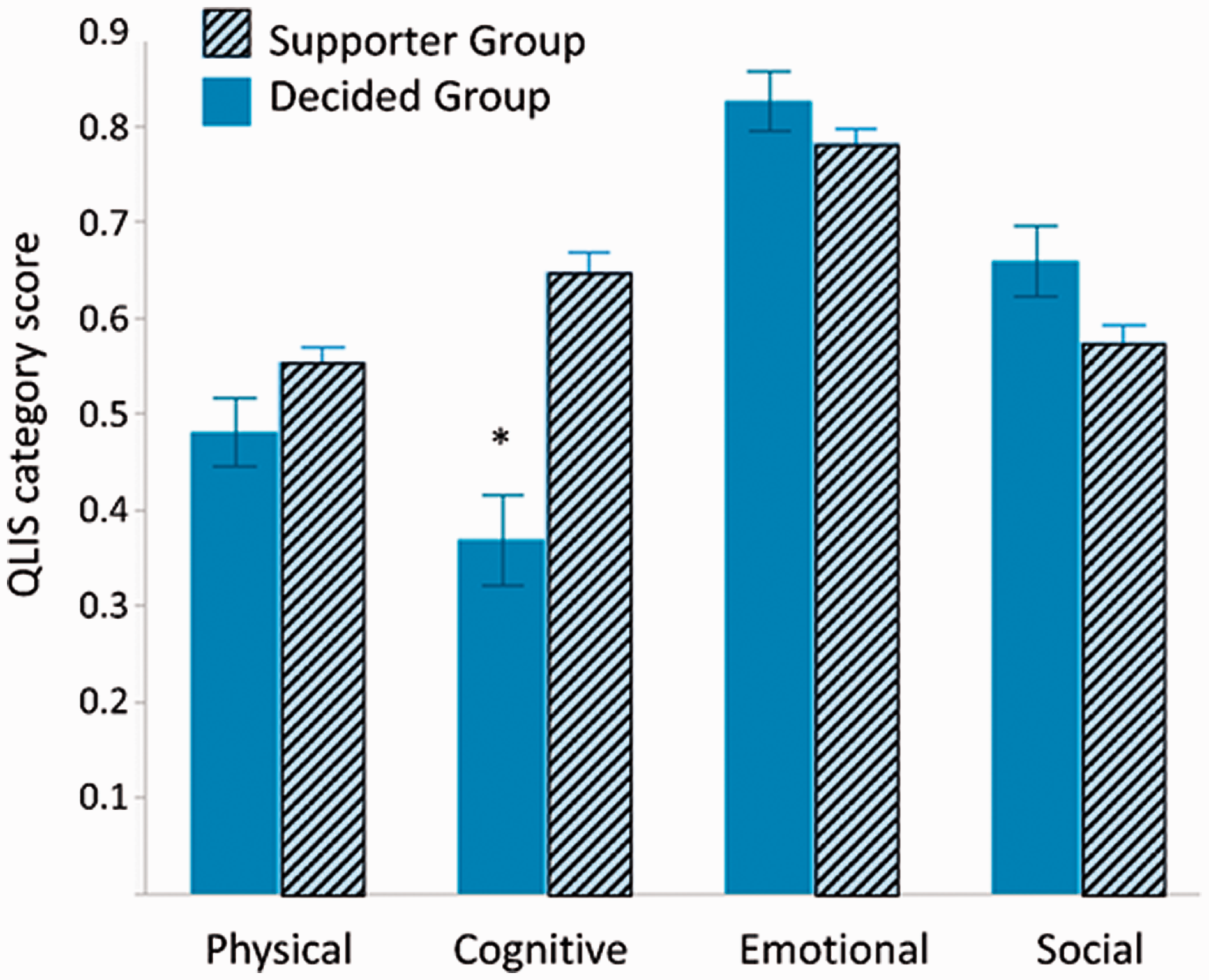
Importance of Different Categories of Factors for Supporter and Decided Group. Note: Mean scores for four categories of factors influencing a desire for a hastened death for the supporter and decided groups. The QLIS category scores are the sum of responses for each section divided by the maximum number of points possible for that section. *There was a significant difference in cognitive scores between the supporter and decided group (Z=-4.97, p<0.0001).
Nearly 84% of people who had decided to hasten their deaths cited the futility of further treatment to improve their current quality of life as a “big problem” as opposed to about 72% of those contemplating whether this would be of high significance. About 77% of the “decided group” cited the likelihood of ending up in a nursing home permanently was a” big problem” while 67% of the contemplating group felt that would be a big issue for them. There was a statistically significant difference in the responses to the question regarding difficulty with daily physical tasks such as dressing, food preparation, and climbing stairs, but this difference is largely due to differences in distribution of responses and there was actually little difference between the two groups in the percentage of respondents ranking this factor as of high importance (Table 3). One of the largest differences between the two groups was that 77% of the supporter group thought uncontrolled pain would be a big influence on wanting to hasten their deaths, while only 32% of the decided group said it was a big problem.
We also compared category scores for physical, cognitive, emotional and social factors between the two respondent groups. We saw that those in the supporter group thought that cognitive decline, evidenced by confusion and/or forgetting, would be a much greater factor in their decision making than it turned out to be for the decided group (Z=-4.97, p < 0.0001). Those in the decided group also cited cognitive issues as less important than the other factors (Figure 1). For both groups of respondents there were significant differences in the importance among the 4 categories, with emotional factors rated as most important by both the supporter (χ2=110.61, p < 0.0001) and decided group (χ2= 63.80, p < 0.0001).
Discussion
As in previous studies, both the supporter group and the decided group trended toward social-emotional factors as more influential in why they would consider hastening their death than physical limitations in task activities of daily living or being in pain (Ganzini et al., 2008b; Rodríguez-Prat et al., 2017). Several of the factors rated highly by our study participants are similar to concerns identified in previous studies such as avoiding inappropriate prolongation of dying, achieving a sense of control, relieving burden on family, and strengthening relationships with loved ones (Singer et al., 1999). But lack of family or close social support was again found not to be a highly influential social problem in either group in wanting to hasten their death (Ganzini et al., 2009). The more important issues in the decided group were: having no further acceptable treatments to improve their condition or quality of life, having to move into a nursing home, the inability to have or create a meaningful life, feeling like a burden to family or loved ones, and an overall loss of independence and feeling life conditions were intolerable. Those who had reached a conclusion to end their life felt that having no further viable treatment options that would improve their quality of life and being faced with having to move into a nursing home were significantly more impactful on their decision making than those predicting what impact these factors would have in their future decision making. While important to both groups, these presumed emotional reactions to an unwelcomed perceived future, carried even more weight in the end than predicted, and apparently heavily influenced the decided group’s choosing not to go further down those paths.
Like the findings in other studies, uncontrolled pain was not a major factor in making the decision to hasten their death for those deciding to do so, while psychosocial factors were cited as more important (Ganzini et al., 2009; Shim & Hahm, 2011). In our study, only 32% of those who had decided to hasten their death cited uncontrolled pain as a big problem while 77% of those predicting what might cause them to choose a hastened death thought this would be of high significance. This difference may be partially related to the fact that palliative care has become much more effective and aggressive about treating pain–even if only at the very end of life–making uncontrolled pain less a problem than people fear it will be when there are no further curative options. And increasingly doctors are not seeing a patient’s request to hasten their death as a failure of pain control or of palliative care (al-Awamer, 2015). Unlike early hypotheses and critics of providing end of life options, this study again supports the conclusion that adequate pain control does not lesson people’s desire to hasten their own death when faced with health conditions that take away autonomy and meaningful existence (Mystakidou et al., 2005).
Similarly, the group who had already decided to end their lives did not report chronic physical issues of feeling ill with nausea, fatigue, incontinence, and trouble breathing and physical problems such as preparing food, dressing, climbing stairs and falling as nearly as big an influence in their decision making as the supporter group thought it might. While it is possible that the decided group did not have these symptoms very often, that seems unlikely since the number of people in the decided group who had serious diseases that produce these symptoms and limitations, comprised the vast majority of the group. It seems more likely that anticipatory fear of loss of autonomy and control may help explain why uncontrolled pain, continuously feeling sick from chronic physical conditions, and diminished capacity for activities of daily living were anticipated as bigger issues ahead of time for the supporter group but not as significant factors for those actually having decided to hasten their deaths.
The supporter group thought that the overall feeling of loss of independence and intolerable quality of life would be a higher factor in wanting to hasten their death than the decided group reported it being a big problem. A gradual acceptance of and accommodation to chronic illness or old age related decline, including increased physical symptoms and limitations as well as decreased cognitive function, may help explain why loss of independence and feeling life was intolerable turned out to be less burdensome and less odious in reality to those in the decided group as opposed to those fearing these developments in the supporter group (Sarkisian et al., 2001; St John & Montgomery, 2013). There are lots of people who “just live with” physical circumstances and conditions that when described to others, especially younger people, they can’t imagine how they would cope with them. This “disability paradox”, where people report having a good life with what others might imagine as intolerable physical decline or limitations has been noted before (Albrecht & Devlieger, 1999; Ubel et al., 2005).
But gradual acceptance of the reality of and physical accommodation required for chronic illness or old age related diminished personal capacity may also come with an increased unwillingness to put up with it. The longer we have lived an active and enjoyable life before becoming significantly physically, cognitively, and socially limited, the less unexpected and emotionally devastating it may be when diminished abilities inevitably come. But the accompanying increasing awareness of actuarial time running out and/or the inability to regain previous autonomy, may equally lessen the need to endure, accept, or wish to burden others with our diminished autonomy and quality of life. This shift of attitude is referenced in the death with dignity movement as having had a “completed life” (van Wijngaarden et al., 2015).
“Unbearable suffering” has also previously been used as another global description of why people want to hasten their death, with “hopelessness” being an essential element of that suffering (Dees et al., 2011). In our study the identification of the lack of any further medical treatments to improve one’s quality of life was of even more importance than the supporter group thought it would be when it came to making a decision to end their life. It was endorsed most often as the biggest problem in the decided group. The abstract contemplation of what it might be like to be told “there is nothing more we can do”, while a potential big influence in the supporter group’s minds (71%), does not likely have as powerful an emotional impact, as when it is an actuality in a person’s life (84% in the decided group). Measuring the emotional impact of this development, as we did in the QLIS, as “the futility of further treatment”, “loss of independence and an intolerable quality of life”, and “a current inability to create a meaningful life” provides a description unrelated to traditional psychological diagnoses and may help prevent those from deciding to hasten their death under these circumstances from being labeled “depressed”. We posit that accepting the hopelessness of further medical treatment to produce an acceptable quality of life, rejecting the stress of further futile medical treatments, and wanting to have control over, or even hasten, one’s death in the face of irremediable medical conditions, are not symptoms of depression. Rather these are the reactions of emotionally healthy individuals, who are fully in control of their decision making, and want to remain in control even through their dying experience. We further suggest that along with embracing a life well lived, this acceptance of the inevitability of death without options to improve one’s quality of life, and the ability to have control over it by hastening one’s own death, is what leads many people to a significant and welcome emotional relief from what could otherwise be “unbearable suffering”.
This contextual placement of hopelessness as a medical reality rather than a symptom of depression or a failure of inadequate medical treatment is in concert with previous findings that show people who acknowledge they have no treatments to save them from dying, are actually less likely to be diagnosed as depressed by classical definition of depression than people who are denying the inevitability of their condition(Chochinov et al., 2000; Olden et al., 2009). Although there has been much concern from critics that a desire to hasten death in the face of irremediable health conditions is the result of unidentified or untreated clinical depression, previous studies have shown that the majority of those seeking physician aid in dying do not meet the criteria for depression (Ganzini, 2014; Ganzini et al., 2008a; Levene & Parker, 2011). Even if patients do have a diagnosable mental disorder, that does not make them incapable either legally or psychologically to make a rational and competent decision about whether they want to hasten their death in the face of irremediable health conditions (Cholbi, 2013).
There was also greater concern in the decided group about having to move into a nursing home (the second highest issue identified as a big problem) than in the supporter group. Along with having no viable medical treatment options to improve their quality of life, and a high desire not to be a burden on others, the impact of these emotional and social factors may be magnified beyond their individual weights. The identification of and combined effect of these individual factors seem to help make up and define the global reason of “loss of autonomy” or “existential distress” that is often cited in previous studies as a central reason for people wanting to hasten their death in the face of irremediable health conditions and consequently being treated with palliative sedation (Li et al., 2017; Rodrigues et al., 2018).
Future Research and Policy Implications
One constraint on our study was the limited sample size for those already having decided to end their lives. A larger sample size in the future would allow further testing of our initial finding that cognitive factors are less important in hastening one’s death than people predicted. Further, this suggests there could be merit in exploring the accompanying hypothesis that when people actually start to have more serious cognitive decline, they aren’t aware how bad it is and aren’t distressed by it. Unsolicited spontaneously hand-written additions on the QLIS questionnaire suggested there could be particular influence of the death of a spouse, life companion, or children on deciding to hasten one’s death, and this could be an important area for future studies to delineate as well.
In our study, we asked a single question regarding loss of independence and having an intolerable quality of life rather than separating these two ideas. For some people, they are highly correlated and for others, an argument strongly made by a portion of the long-term disabled community, they are not correlated. For example, people living with disabilities may rely on assistive technology and caregivers, but experience a satisfying quality of life. Some people with long-term disabilities fear the worth and dignity of their lives may be disrespected by health conditions that others find “intolerable” and would lead them to hasten their deaths (Gill, 1992). Some in the disability-rights community have expressed concerns with aid in dying laws because of fears that disabled people won't receive the in home and medical resources they need and be inadvertently pushed to consider hastening their deaths (Weir, 2017). This is a more concrete example of the larger “slippery slope” argument, the idea that people from more vulnerable groups may be offered euthanasia too easily, instead of being offered more helpful improvements to their quality of life (Burgess, 1993; Verbakel & Jaspers, 2010). This argument is often promoted by those whose values and religious beliefs are against any form of self-intentional ending of (human) life and seek to restrict wider application of the principle of self-autonomy by opposing any self-directed or physician aid in dying. Importantly, evidence suggests that while vulnerable people may fear them, abuses, pressures, and inequities in application are not actually transpiring in areas where aid-in-dying is available (Albaladejo, 2019; Battin et al., 2007; Lindsay, 2009). At this time it is not so much a “slippery slope” but rather an “intentional slope” toward more and more self-autonomy and self-control at the end of life. Support for more autonomous choice was even more pronounced in our decided study group when people are actually face to face with issues such as not having any acceptable treatment to improve their quality of life and forced to live the rest of their life in a nursing home.
Our findings have possible implications for policy as more governments begin to consider how to legalize and regulate aid-in-dying for irremediably ill citizens. As highlighted in our results, the factors that may make the life of an ill person untenable include social and emotional factors as well as physical ones that may be difficult to capture fully in a medical chart. Yet all state laws in the US require a six-month terminal prognosis from a doctor based on a medical diagnosis as a legal necessity to access aid-in-dying options. In contrast, a Belgian law passed in 2002 requires only “constant and unbearable physical or mental suffering that cannot be alleviated”, not a physical terminal illness with six months or less to live as the condition for medical aid in dying ("The Belgian act on euthanasia of May, 28th 2002," 2003). Canadian law requires only “a grievous and irremediable medical condition…that cannot be relieved under conditions that you consider acceptable”("Medical Aid in Dying (MAID)," amended 2020). And as of March 17, 2023, an irremediable mental illness, without any other medical conditions, will be included as a qualifying condition for medical aid in dying. These recent 2021 amendments to Canada’s medical-aid-in-dying law show what policy looks like when more weight is given to autonomous decision making and when medical aid in dying policy weighs physical and psycho-social factors more equally. Insights from our study could be relevant as Canada and others consider how carefully to address people with chronic irremediable mental illness who wish to hasten their death.
Our research highlights that those who are actually dealing with severe, progressing intractable illness and intolerable decline in quality of life, think about specific factors affecting their desire to hasten their death somewhat differently than those who are supportive but not yet in that position in their own lives. Along with our finding that social and emotional factors are as or are more important than physical ones in influencing people to want to hasten their death, our study suggests that loved ones, caregivers, policy makers, and medical providers may want to again review what compassionate understanding and support looks like for people wanting to hasten their death because of irremediable health conditions.
Footnotes
Authors’ Contribution
R Blake conceptualized and supervised this study, including managing the investigation and writing the initial draft of the manuscript. C Blake curated the data, conducted formal analyses, created tables and figures, and edited the manuscript. Funding for analysis and support for data collection was provided by the Final Exit Network. We also thank Carol Ballou for her assistance in development of the survey and data collection.
Ethical Approval
This research design and methods were reviewed under Protocol #19-BLA-101 by the Pearl Institutional Review Board in December 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:Funding for statistical analysis was provided by the Final Exit Network.