
Abstract
Those who are bereaved during the current COVID-19 pandemic are subject to restrictions on funeral sizes and practices. We conducted a rapid review synthesising the quantitative and qualitative evidence regarding the effect of funeral practices on bereaved relatives’ mental health and bereavement outcomes. Searches of MEDLINE, PsycINFO, KSR Evidence, and COVID-related resources were conducted. 805 records were screened; 17 studies of variable quality were included. Current evidence regarding the effect of funeral practices on bereaved relatives’ mental health and bereavement outcomes is inconclusive. Five observational studies found benefits from funeral participation while six did not. However, qualitative research provides additional insight: the benefit of after-death rituals including funerals depends on the ability of the bereaved to shape those rituals and say goodbye in a way which is meaningful for them. Findings highlight the important role of funeral officiants during the pandemic. Research is needed to better understand the experiences and sequalae of grief and bereavement during COVID-19.
Introduction
The coronavirus disease 2019 (COVID-19) has caused 383,000 deaths globally as of June 4th 2020, with c.106,000 deaths in the USA and 40,000 confirmed COVID-19 deaths in the UK (World Health Organization, 2020). In addition, there is an as-yet undetermined number of excess deaths associated with the pandemic; in the UK, overall figures since the start of the COVID-19 crisis are a fifth higher than usual (Office of National Statistics, 2020). To attempt to reduce infection rates and therefore mortality due to COVID-19, governments have implemented public health measures designed to reduce interactions between people. This includes restrictions on the number of mourners permitted to attend funerals as well as minimising interactions with the deceased during ceremonies, which affect all of those bereaved during the current crisis (Centers for Disease Control and Prevention, 2020; Public Health England, 2020). In the UK, for example, guidance for the foreseeable future states that the number of mourners is to be kept as low as possible to ensure a safe distance of at least 2 metres can be maintained between individuals (UK Government, 2020). Alongside funeral staff and an officiant (usually a non-denominational celebrant or a faith representative), permitted attendees are members of the deceased’s household, close family members, or, if these are unable to attend, close friends. While mourners unwell with symptoms of COVID-19 should not attend, those who are extremely clinically vulnerable can decide to do so despite the risk. Funeral venue managers are instructed to set caps on numbers to ensure social distancing can be maintained, consider how to manage the flow of attendees in and out of venues, ensure ventilation and regular disinfection of surfaces, and provide adequate handwashing stations. To ensure that organisations managing funerals are able to cope with the increased number of deaths, it is requested that funerals are not delayed.
In practice, these formal requirements mean mourners lack expressions of physical comfort (through hugs, handshakes or sitting next to each other during the funeral), are not able to touch the coffin, cannot hold a reception after the funeral to socialise and may not feel that they have said the farewells they would have wished for. The measures in place due to COVID-19 mean that funerals will most likely not resemble what the bereaved or the deceased would have wanted, and many mourners will be unable to attend funerals in person. Funerals are a fundamental component of cultural and religious mourning systems: they facilitate the offering of social and psychological support to the bereaved, and afford an opportunity to convey love and respect for the deceased (O’Rourke et al., 2011). It is consequently possible that being unable to participate in funerals, rituals, and ceremonies will have a detrimental effect on the bereaved, affecting their mental health and ability to cope with or process their grief. This rapid review therefore aims to synthesize evidence on the impact of funeral practices on bereaved friends and relatives’ mental health and experience of bereavement. We then consider implications for the COVID-19 pandemic.
Methods
Design
Rapid systematic review according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Online Appendix 1).
Inclusion/Exclusion Criteria
Population – bereaved family members/friends
Intervention – funeral practices and rituals including burial rites and ceremonies
Context – N/A
Outcomes – mental health and bereavement outcomes assessed quantitatively (including but not limited to depression, prolonged grief disorder, PTSD symptoms, anxiety, grief intensity), and/or qualitative findings regarding experiences of grief and bereavement
Included
Original quantitative or qualitative studies or systematic reviews of the mental health or bereavement outcomes of bereaved families/friends, including children, in relation to funeral practices
Excluded
Non-English language study reports
Studies of health or social care staff or funeral directors
Studies related to bereavement after a pet’s death
Studies related to stillbirth, miscarriage, neonatal death or death of a child during the first year of life
Studies of bereaved people not examining mental health, bereavement outcomes or grief experiences
Opinion pieces, narrative reviews, dissertations, conference abstracts
Search Strategy
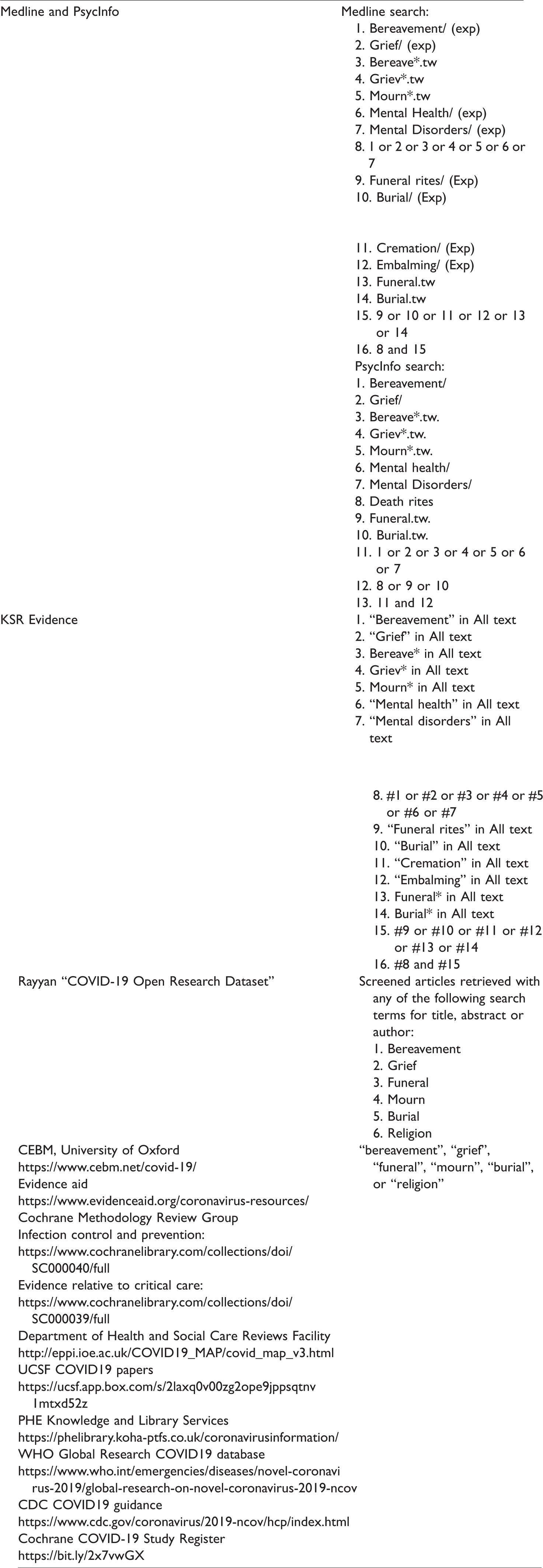
We searched for relevant articles using MEDLINE (Ovid) and PsycINFO databases with no date limits. We also searched KSR Evidence, Rayyan “COVID-19 Open Research Dataset” and other COVID-related resources. The search strategy comprised terms for funerals, bereavement, mourning, grief, and mental health outcomes (Table 1).
Search Strategy and Terms.
Study Selection
One author (L. S.) completed the MEDLINE (Ovid) and PsycINFO searches and deduplicated records. The other author (A. B.) completed the remaining searches. Article titles and abstracts were screened in EndNote (version X9, Clarivate Analytics, Philadelphia, PA) by A. B. The full-texts of articles not excluded on the basis of title and abstract were independently dual-screened by A. B. and L. S.
Data Extraction
Data were extracted into a bespoke results table. A. B. extracted the data, with extraction reviewed by L. S.
Analysis
Study findings are presented in Table 2 and synthesised narratively. Study quality and risk of bias were assessed using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools] and the Critical Appraisal Skills Programme Qualitative Checklist [https://casp-uk.net/casp-tools-checklists/] for quantitative and qualitative studies respectively. Quality appraisal was performed by A. B. and reviewed by L. S. with disagreements discussed and resolved. Quality assessments were tabulated, with limitations summarised and integrated into the narrative.
Results Table.

Results
All searches were performed on 24th April 2020. We identified 789 articles from MEDLINE and PsycINFO searches and 38 articles from other sources. After deduplication, 805 articles remained for screening. Searches of references from commentaries/narrative reviews identified were performed (n = 3) but resulted in no further relevant articles. Forty-four articles underwent full-text review, with 17 included in the analysis (Figure 1; Table 2).
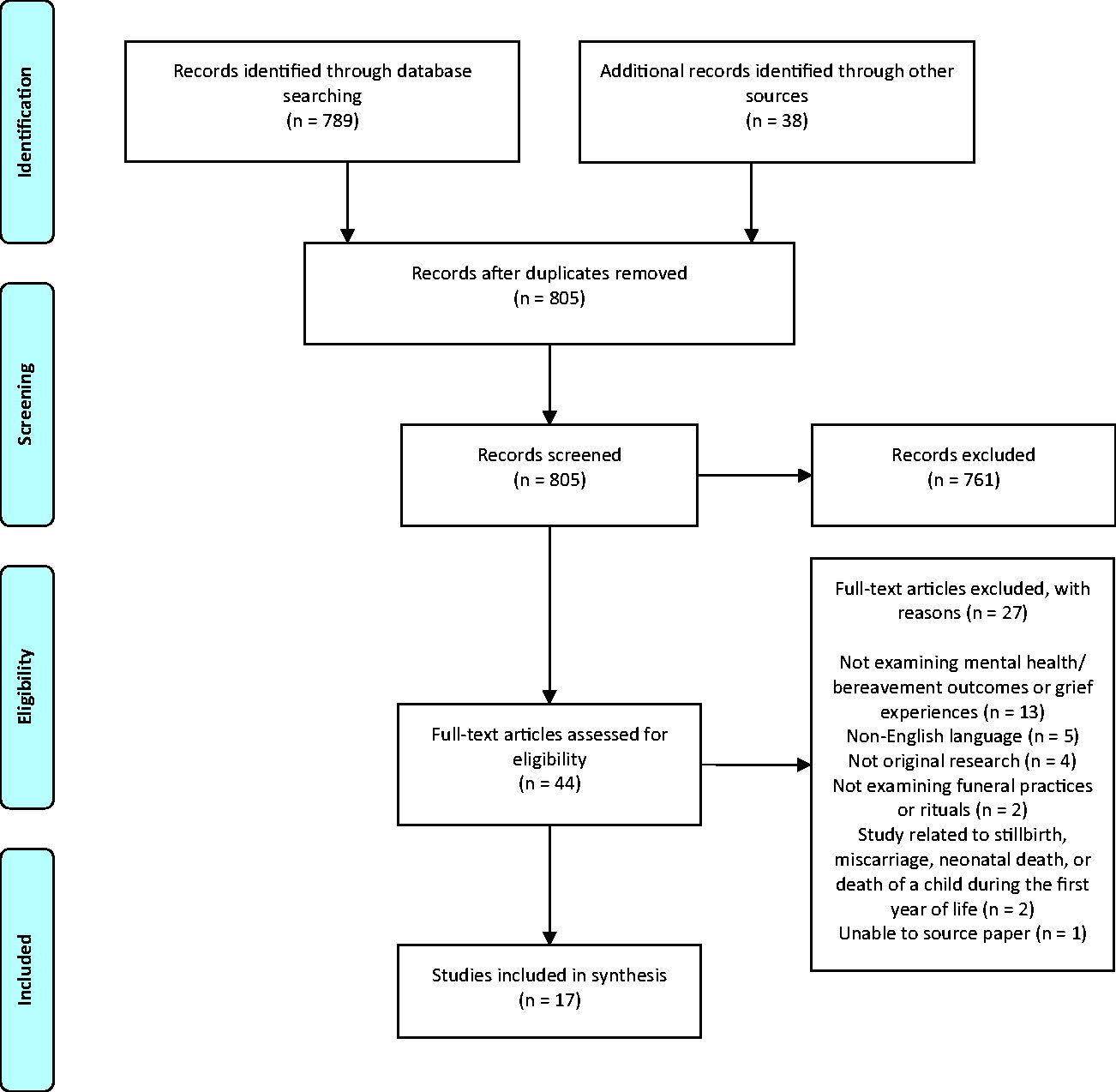
PRISMA Flow Diagram.
Eleven observational and six qualitative studies were identified.Most were conducted in the U.S. (Bolton & Camp, 1987; Doka, 1985; Fristad, et al. , 2001; Gamino et al., 2000; Grabowski & Frantz, 1993; Nesteruk, 2018; Saler & Skolnick, 1992; Silverman, 1987; Vandercreek & Mottram, 2009; Weller et al., 1988; Zisook & DeVaul, 1983) in White Christian populations.Other country settings were Hong Kong (Chan et al., 2005; Pang & Lam, 2002), Australia (Kissane et al., 1997), Netherlands (Mitima-Verloop et al., 2019), Rwanda (Schaal et al., 2010) and Turkey (Aksoz-Efe et al., 2018). The included articles, published between 1983 and 2019, were of variable quality (Tables 3 and 4). Participant numbers ranged from 50 to 552 in the observational studies.
Quantitative Study Quality—Assessed Using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.
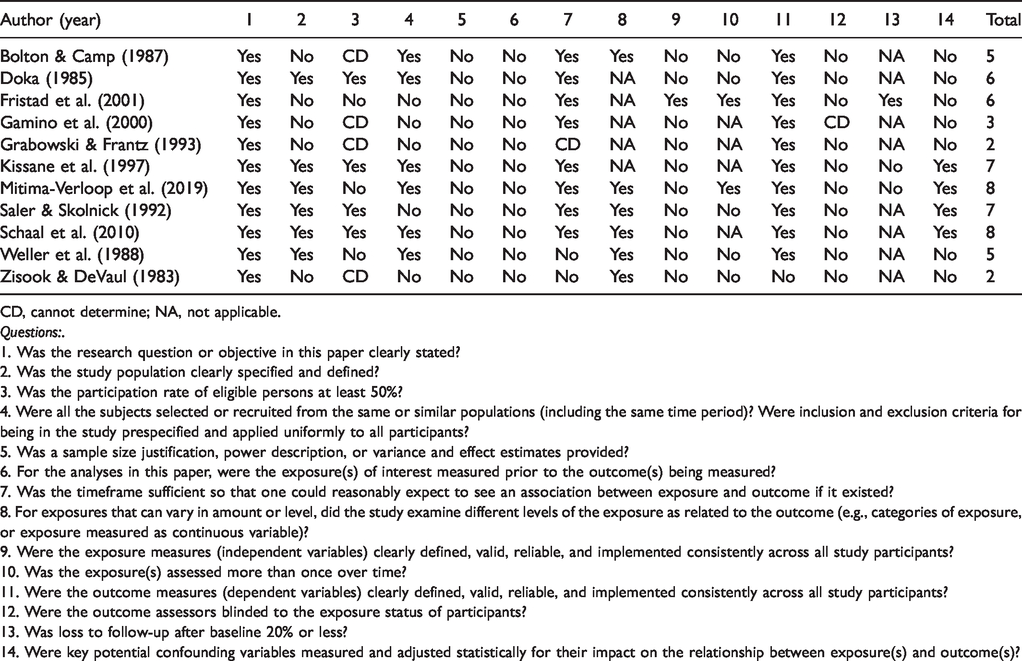
CD, cannot determine; NA, not applicable.
Questions:.
1. Was the research question or objective in this paper clearly stated?
2. Was the study population clearly specified and defined?
3. Was the participation rate of eligible persons at least 50%?
4. Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants?
5. Was a sample size justification, power description, or variance and effect estimates provided?
6. For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured?
7. Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed?
8. For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)?
9. Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?
10. Was the exposure(s) assessed more than once over time?
11. Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants?
12. Were the outcome assessors blinded to the exposure status of participants?
13. Was loss to follow-up after baseline 20% or less?
14. Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?
Qualitative Study Quality—Assessed Using Critical Appraisal Skill Programme Qualitative Checklist.
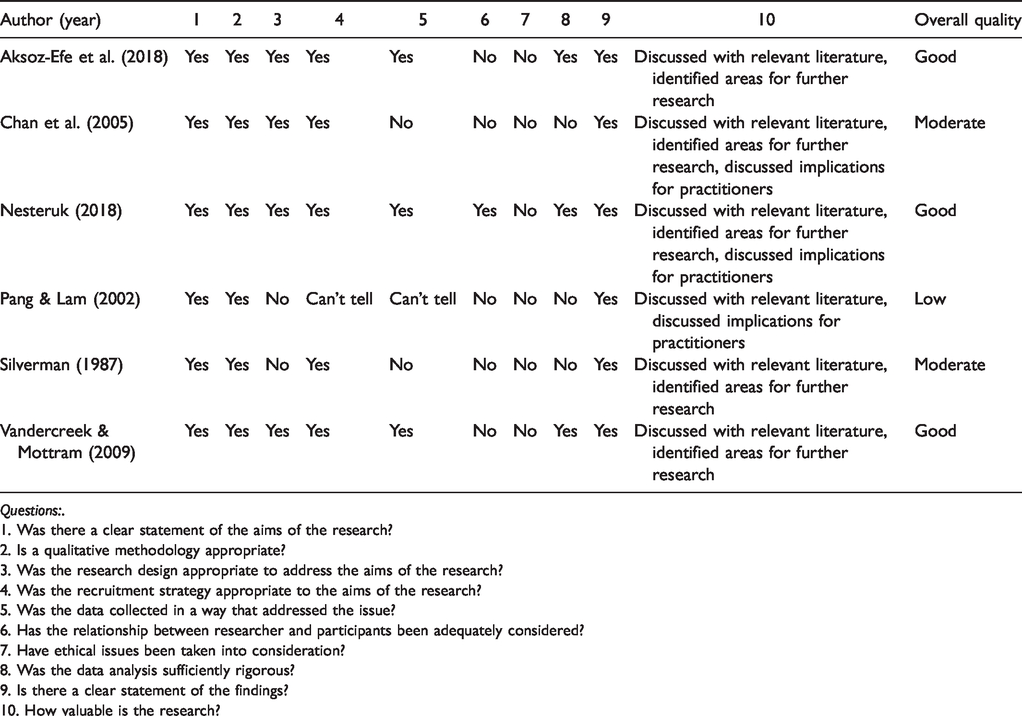
Questions:.
1. Was there a clear statement of the aims of the research?
2. Is a qualitative methodology appropriate?
3. Was the research design appropriate to address the aims of the research?
4. Was the recruitment strategy appropriate to the aims of the research?
5. Was the data collected in a way that addressed the issue?
6. Has the relationship between researcher and participants been adequately considered?
7. Have ethical issues been taken into consideration?
8. Was the data analysis sufficiently rigorous?
9. Is there a clear statement of the findings?
10. How valuable is the research?
Overall, evidence of the effect of funeral participation on mental health or bereavement outcomes was inconclusive. Five observational studies found funerals were associated with significant benefits to bereaved participants; the positive impact on grief experiences are described further in the six qualitative studies. However, the remaining six observational studies found no measurable associations.
Involvement in planning a funeral was not associated with grief adjustment at one year in a study of 50 white, middle-to-upper class Americans. In another component of this mixed-methods study, 57% felt planning a funeral helped with their grief, 28% were unsure, and 15% felt it was unhelpful and viewed funeral planning as a routine duty (Doka, 1985). Gamino et al. (2000) reported that bereaved individuals who participated in planning the funeral reported significantly lower depersonalisation (p = 0.001) and social isolation (p = 0.05) than those who did not. In a qualitative study of immigrants in the U.S., participants who were able to attend funerals in their countries of origin reported gaining a sense of belonging and comfort from participating in funeral preparations with their loved ones (Nesteruk, 2018).
Funeral attendance was associated with less unresolved grief in one U.S. study (Zisook & DeVaul, 1983), with participants who were found to have “definitely unresolved grief” significantly less likely to have attended the funeral of their relative or close friend (p < 0.05). These findings should be interpreted with caution as this study had a number of methodological limitations: there was no clear definition of the study population, no application of inclusion or exclusion criteria, and no description of methods used for data analysis; the measure used for unresolved grief was also unvalidated and its development was not described in detail. In a study of widows who had experienced the 1994 Rwandan genocide, funeral attendance did not significantly contribute to the severity of prolonged grief reactions in a multiple regression analysis (Schaal et al., 2010). This is clearly a unique setting and these results may not be generalisable to other scenarios. A U.S. study found no significant differences in grief intensity between those who did and did not attend a funeral in Latino and Anglo-American samples. In the Latino sample, there was no significant difference in grief intensity between those who had and had not participated in a novena, a post-funeral practice involving prayer and support that generally takes place in the home of the bereaved (Grabowski & Frantz, 1993). In contrast, in qualitative studies, participants perceived funeral participation positively as a chance to say goodbye (Chan et al., 2005), and those unable to participate due to geographical distance reported distress (Nesteruk, 2018; Pang & Lam, 2002): “Everybody is there together and they are there for each other to give comfort. Here, we are the only ones. [All we can do] is just cry, that’s it. So, it is hard.” (Nesteruk, 2018, p. 9)
A participant in Nesteruk’s study of immigrants in America described her experience of virtually attending her father’s funeral in India: “We were on Skype and whatever was going on—I was there. The whole night, sitting online, praying and seeing my daddy until the last moment when they took him away. So, I felt that I was there with him all the time.” (Nesteruk, 2018, p. 10)
Post-death rituals: In Bolton and Camp’s (1987) study, the number of self-reported pre-, during-, and post-funeral rituals performed after a death was not associated with grief adjustment, although no interpretative statistical data are provided to support this statement. An Australian longitudinal study found that 6 weeks after a death, viewing the body was associated with fewer depressive symptoms (p < 0.001) and less intense grief (p < 0.01), and saying goodbye as wished with better social adjustment (p < 0.01), but these associations were not evident at 6 months or 13 months (Kissane et al., 1997).
In a qualitative study of Muslim participants in Turkey, traditional post-death rituals were perceived as helpful or unhelpful in the grieving process, with their reported helpfulness dependent on participants’ sense of control over and involvement in them. In particular, the practice of not leaving the bereaved alone was perceived by participants who retained a sense of personal space and control as supportive, while others perceived the same ritual to be difficult or even disturbing. Participants who felt a lack of control were generally older and financially dependent on others (Aksoz-Efe et al., 2018).
In two studies in Hong Kong, rituals were generally viewed positively and provided meaning, easing grief and reinforcing bonds with the deceased (Chan et al., 2005; Pang & Lam, 2002). The exception was a group of widows describing their pain at the Taoist ritual of ‘breaking the comb’, performed before covering the coffin to symbolize the end of the marriage between the bereaved and deceased (Chan et al., 2005).
Funeral experience: In a recent longitudinal study from the Netherlands, funerals were perceived as contributing to processing the loss by >70% of participants at 6 months (T1) and 3 years (T2) post bereavement, and a positive evaluation of the funeral and funeral director was associated with positive affect at T1 (p < 0.001). A regression analysis including grief, general evaluation of the funeral and evaluation of the funeral director at T1 predicted grief at T2 (p < 0.001), however when looking at individual components of the model, only grief at T1 explained a unique proportion in variance of grief at T2 (p < 0.001). Of note, participants were recruited via a funeral service’s satisfaction survey and there was a high dropout rate from T1 to T2 (552 to 289 participants), with significant differences between those who withdrew and those who did not (Mitima-Verloop et al., 2019).
In a U.S. study, mourners who described a funeral as ‘comforting’ reported significantly less overall grief (p = 0.01), social isolation (p = 0.005), despair (p = 0.01), anger/hostility (p = 0.02) and guilt (p = 0.05), although the nature of these associations (and in particular what causal mechanisms might be at play) is unclear. Adverse events during the funeral service – for example conflicts among survivors, discrepancies between the wishes of the deceased and the bereaved, and problems with cremation – were associated with higher overall grief (p = 0.05) and other poor outcomes including somatisation (p = 0.001), loss of control (p = 0.02), and depersonalisation (p = 0.05) (Gamino et al., 2000).
In qualitative research, low funeral attendance was perceived by relatives as a lack of social support (Pang & Lam, 2002), while high funeral attendance was supportive, and remained helpful for years afterwards: “Even now, I think back to that day and it gives me strength because there were so many people who supported us.’’ (Vandercreek & Mottram, 2009, p. 751)
In Hong Kong, some negative memories were reported of the ritual viewing of the body before the final covering of the coffin: “Whenever I close my eyes, the image of my father pops up obsessively. His eyes were half opened, and so was his mouth. His face was white like a cement wall, contrasting with the lips with lip-stick as if he was bleeding. I cannot wash away this awful memory.” (Chan et al., 2005, p. 16)
Children’s bereavement outcomes and experiences: A U.S. study of 38 children with restrictive inclusion criteria (see Table 2) found no association between a child’s funeral participation and depression or anxiety as reported by parent or child 2 months post-death, although no specific data were provided to support this statement (Weller et al., 1988). Fristad et al. (2001) studied parent-bereaved children in the U.S., and found less opportunity to participate in funeral-related activities was associated with higher rates of depressive symptomatology at 13- and 25- months post-loss. This was, however, in an analysis that was not pre-specified: nearly all children whose families had visitations, funerals and burials attended these, therefore comparison was instead made between participants whose families did and did not have a visitation. In the same study, children were asked open-ended questions regarding what they did and didn’t like about the funeral and associated rituals. The most common responses regarding what they liked related to aspects of the ritual (e.g. music such as the deceased’s favourite song, flowers, prayers, poems, or the act of putting something into the casket), the support of others, and the eulogy. Children also appreciated the finality of death represented by the funeral and burial. Aspects of the funeral children did not like included the behaviour of others (e.g. friends, relatives); seeing the deceased or their physical appearance (e.g., “did not like their smell and their lips sealed”, Fristad et al., 2001, p. 7); not liking the preacher or minister (“the minister did not know my father”, p. 8) or the lowering of the casket during the burial.
In a study of adults bereaved as a child (Saler & Skolnick, 1992), having less opportunity to participate in mourning activities as a child was associated with higher rates of depressive symptomology and likelihood of being prone to self-criticism. In qualitative research, however, U.S. college-age women who were teenagers at the time of bereavement had varying views: some resented being involved in the funeral and reported more difficulty coping, whilst others felt their participation brought the family closer (Silverman, 1987).
Discussion
This review is the first to synthesise evidence regarding the effect of funeral practices on bereaved friends’ and relatives’ mental health and bereavement outcomes. We found no systematic reviews in this area and the only quantitative studies were observational in nature, examining associations between funeral practices and bereavement/mental health outcomes rather than establishing causal relationships, which would require randomised designs unethical in this context. Across observational studies of variable quality, some found benefits associated with funeral participation while others did not. However, the qualitative research identified provides useful additional insight: for both adults and children, the benefit of after-death rituals including funerals depends on the ability of the bereaved to shape those rituals and say goodbye in a way which is meaningful for them, and on whether the funeral demonstrates social support for the bereaved.
In the context of COVID-19, these findings suggest that restrictions to funeral practices do not necessarily entail poor outcomes or experiences for the bereaved: it is not the number of attendees or even the type of funeral which determines how supportive it is, but rather how meaningful the occasion is, and how connected it helps mourners feel. Similarly, a research study published since our searches were conducted found no association between type nor elaborateness of cremation service and levels of grief (Birrell et al., 2020), although these participants chose their funeral arrangements as opposed to having restrictions imposed. The review findings also highlight the crucial role played by funeral directors and officiants in helping the bereaved to create funerals which are personal, meaningful and expressive of collective grief and support despite the current restrictions associated with COVID-19. Creating a funeral in this context requires sensitivity, creativity and skill, especially since it may be harder to create an emotional connection with the bereaved when arranging a funeral service virtually; however, there are resources to support this process (Table 5). Our findings suggest that ‘template’ services where the funeral officiant takes a leading role might be less appropriate than personalised services in which families take the lead and the officiant facilitates, supporting people to create and perform their own rituals (Kuyvenhoven, 2020). The latter approach also reflects the role funeral providers play in bereavement support: in an Australian survey, their support was perceived as very/quite helpful by 91.30% of respondents, second only to family support (Aoun et al., 2018). With social support from family and friends limited during the pandemic, funeral providers’ and officiants’ part in bereavement support is particularly relevant.
. Resources for Meaningful Funerals During COVID-19.
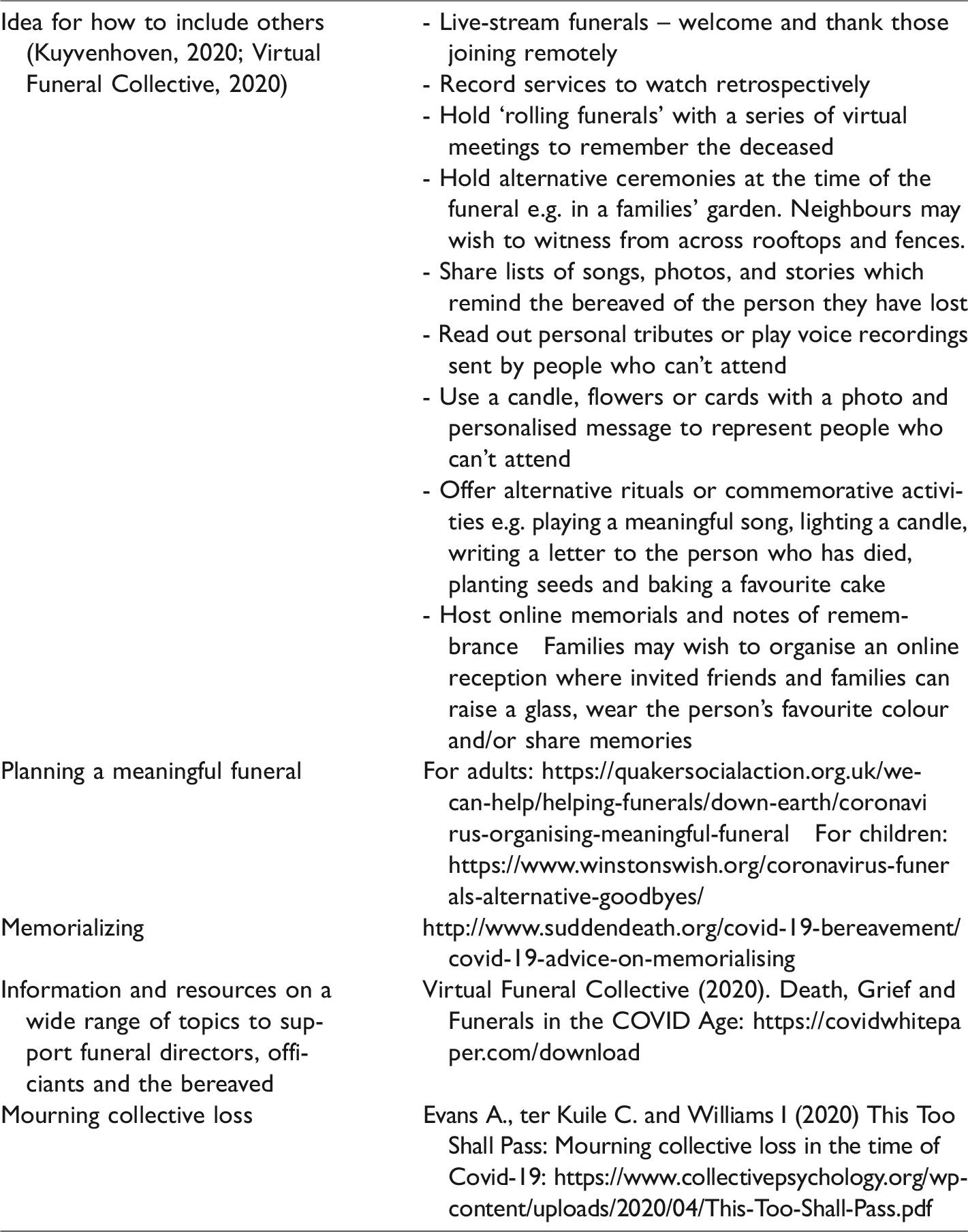
Emerging evidence suggests that during the pandemic, the bereaved and the funeral providers and officiants supporting them have shown remarkable resilience, finding novel alternatives to usual practices and traditions. A U.K. report published since our literature searches describes positive experiences of smaller funerals during the pandemic, with those able to attend appreciating their intimate and personal nature (Bear et al., 2020). When physical funeral attendance isn’t possible, virtual attendance has been facilitated through live-streaming or other means, including integrating the presence of those who are absent in other ways (Table 5) (Bear et al., 2020; Walter et al., 2011). In non-academic literature published during the pandemic, religious leaders and attendees have praised live-streamed funeral services for widening access – for example, enabling Muslim women to experience the burial – and enabling private emotional expression not possible at public ceremonies (Wood, 2020). Our review did not find any literature examining whether or how virtual attendance impacts mental health or bereavement outcomes, although one participant’s experiences of virtual funeral attendance were described positively by Nesteruk (2018). Comparing the grief and bereavement outcomes of virtual attendance to both physical attendance and not being able to attend a funeral at all is a recommended avenue for exploration.
We found that in qualitative research, a sense of control was a key determinant of whether participants identified funeral practices and rituals as helpful or unhelpful. Given the social restrictions and economic uncertainty during the COVID-19 pandemic, many people will be experiencing a sense of lack of control over their lives. This may be particularly true in Black, Asian and Minority Ethnic (BAME) groups which are underrepresented in research in this area, overrepresented in lower socioeconomic groups and have a markedly higher mortality risk from COVID-19 (Razaq et al., 2020). Calls for governments to provide financial support for funeral costs to communities disproportionately affected by the pandemic are therefore appropriate (Bear et al., 2020). To further support vulnerable communities, we recommend engaging with community and religious leaders to provide culturally sensitive information and support regarding local bereavement services and funerals.
Only one of the studies we identified explicitly examined ethnic, cultural, or religious differences in funeral practices and mental health, grief, or bereavement outcomes (Grabowski & Frantz, 1993). Funeral practices vary widely between groups along all of these axes and different faith and cultural groups will be affected to varying degrees by current restrictions (Bear et al., 2020; Uzell, 2018). Washing the body of the deceased, for example – an important ritual in Islam, Judaism and Sikhism – is currently restricted in the U.K. to either only being carried out in full personal protective equipment with supervision, or not at all (Public Health England, 2020). COVID-19 has also disrupted the Jewish ritual of shiva, seven days of intense mourning in which the community provides meals, prayer and comfort, as well as has the Irish tradition of the wake and the Baptist repast that follows a funeral (Schuck et al., 2020). While every individual will be affected differently by restrictions to their mourning process, these losses may be a source of communal as well as individual distress (Bear et al., 2020). An improved understanding of the impact of restrictions on funeral practices on different communities’ bereavement outcomes and experiences could help funeral officiants in adapting services and inform the advice bereavement service providers give to families. Technology is being used to accommodate gatherings of friends and family for prayer, recitation of the rosary or a wake, to coordinate virtual shiva visits, and to hold the nine night ceremonies traditional across the Caribbean diaspora (Schuck et al., 2020; White, 2020); however the acceptability and impact of these adaptations is not yet known.
The quantitative studies identified used a range of grief, social adjustment, and psychological symptomology outcome measures. There was, however, a notable lack of research on how these outcomes may impact on subsequent psychiatric and psychological diagnosis, treatment and service use, be that primary care, specialist bereavement services, or psychiatric care. Clinical correlates should be explored in future research to enable service providers to anticipate demand and allocate resources accordingly.
Limitations
This review excluded non-English language reports and may therefore have omitted relevant articles. As with any review, there is a risk of publication bias impacting the outcome of literature searches. The evidence identified was published from 1983 to 2019; during this time there have been considerable changes in how funerals are designed and conducted. In particular, in recent years, celebrant-led, person-centred services have grown in popularity. These changes should be taken into account when considering the external validity of our findings, and future research should reflect the diversity of the current funeral landscape. While existing evidence on funeral practices and bereavement outcomes provides useful indicative guidance, its generalisability to the unprecedented funeral restrictions currently in place are unknown.
Conclusion
The prevalence of mental health conditions is likely to increase during and immediately after the COVID-19 pandemic (Nobles et al., 2020), with those who have lost a family member at particular risk of psychiatric distress (Chew et al., 2020). The social support available to those who are bereaved is limited, and social isolation is known to exacerbate psychological morbidity in bereavement (Selman et al., 2020).Based on this review, it is unclear how funeral restrictions will contribute to this on a population level. However, qualitative research highlights the importance of meaningful and supportive funerals for the bereaved; enabling relatives to achieve a sense of control and social support despite current restrictions is crucial, especially among BAME communities most vulnerable at this time. As well as access to bereavement support and sign-posting to specialist services, palliative care and bereavement teams should provide locally-relevant information regarding the creation of meaningful, culturally appropriate funerals. As people continue to find new ways to grieve and commemorate their loved one, the impact of these alternative modalities should be explored. Becoming bereaved during COVID-19 presents challenges at every stage of the funeral process, from planning to post-funeral rituals and memorialisation. Understanding the personal and public health effects of this will take time and sensitive, methodologically robust research.
Supplemental Material
sj-pdf-1-ome-10.1177_0030222820941296 - Supplemental material for How do Funeral Practices impact Bereaved Relatives' Mental Health, Grief and Bereavement? A Mixed Methods Review with Implications for COVID-19
Supplemental material, sj-pdf-1-ome-10.1177_0030222820941296 for How do Funeral Practices impact Bereaved Relatives' Mental Health, Grief and Bereavement? A Mixed Methods Review with Implications for COVID-19 by Alexander Burrell and Lucy E. Selman in OMEGA–Journal of Death and Dying
Footnotes
Acknowledgements
We would like to thank Dr Jo Hartland for requesting a review on this topic to inform clinical practice, Lara Edwards at NIHR ARC West for inviting us to conduct it, and Rosalie Kuyvenhoven, celebrant at Rituals Today, for her valuable comments on a draft of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.